© 2011 pearson education, inc. 11 nutrients involved in bone health
TRANSCRIPT

© 2011 Pearson Education, Inc.
11Nutrients Involved
in Bone Health

© 2011 Pearson Education, Inc.
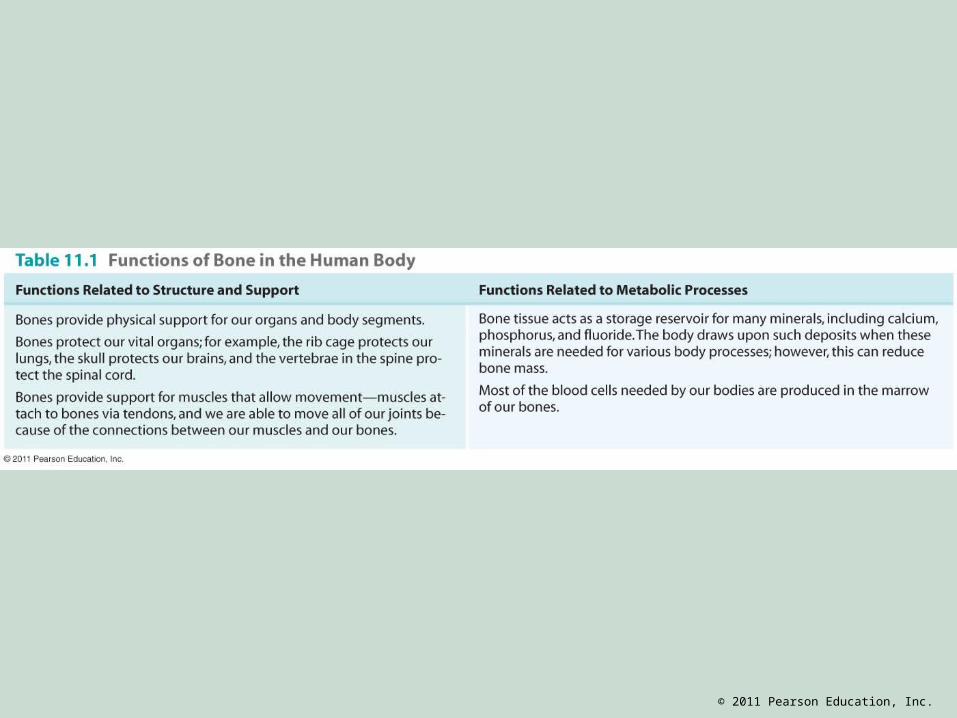
Bones
• Bones are living organs that contain • Bone tissue• Nerves• Cartilage• Connective tissue
• Blood vessels supply nutrients to bone to support its activities

© 2011 Pearson Education, Inc.
Bones
• Bone provides strength and flexibility• Contains about 65% minerals, providing the
hardness of bone• Contains 35% organic structures for strength,
durability, and flexibility• Collagen: fibrous protein in bone tissue• Hydroxyapatite: mineral crystals around collagen
designed to bear weight
© 2011 Pearson Education, Inc.

© 2011 Pearson Education, Inc.
Bone Tissues
• Cortical bone (compact bone) 80% of the skeleton Outer surface of bone
• Trabecular bone (spongy bone) 20% of the skeleton Inside of bones (scaffolding) Supports outer cortical bone Faster turnover rate (sensitive to hormonal
changes and nutritional deficiencies)

© 2011 Pearson Education, Inc.

© 2011 Pearson Education, Inc.
Bone Development
• Bone growth: increase in bone size• Complete by age 14 in girls; age 17 in boys
• Bone modeling: shaping of bone• Complete by early adulthood
• Exercise and overweight increase thickness • Bone remodeling: recycling of bone tissue

© 2011 Pearson Education, Inc.

© 2011 Pearson Education, Inc.
Bone Development
• Bone density: compactness of bones• Peak bone density: when bones are
strongest• Factors associated with a lower peak bone
density: • Late pubertal age in boys• Late onset of menstruation in girls• Inadequate calcium intake• Low body weight• Physical inactivity during the pubertal years

© 2011 Pearson Education, Inc.
Bone Remodeling
• Resorption: surface of bones is broken down by osteoclasts (cells that erode the surface of bones)
• New bone matrix formed by osteoblasts (bone builders)• Synthesize new bone matrix by laying down
collagen-containing component of bone

© 2011 Pearson Education, Inc.

© 2011 Pearson Education, Inc.
Bone Remodeling
• Bone resorption and formation are equal in young, healthy adults
• Resorption exceeds new bone formation after age 40: density begins to decrease
• High peak bone mass through proper nutrition and exercise: stronger skeleton • Protective against osteoporosis

© 2011 Pearson Education, Inc.
Bone Health
• Dual energy x-ray absorptiometry (DXA)• Measures bone density • Results are compared with average peak bone
density of 30-year-old healthy adult• T-score is used to assess a person’s risk for
fracture and diagnose osteoporosis• Recommended for postmenopausal women

© 2011 Pearson Education, Inc.

© 2011 Pearson Education, Inc.
Nutrients for Bone Health
• Calcium is the most recognized nutrient associated with bone health
• Also essential for bone health: • Vitamins D and K• Phosphorus• Magnesium• Fluoride

© 2011 Pearson Education, Inc.
Calcium
• Calcium absorption • Is enhanced in an acid environment• Requires 1,25-dihydroxyvitamin D
Calcium Metabolism

© 2011 Pearson Education, Inc.
Functions of Calcium
• Provides structure for bones and teeth• Assists with acid−base balance• Transmission of nerve impulses• Assists in muscle contraction• Maintains healthy blood pressure• Initiates blood clotting• Regulates hormones and enzymes

© 2011 Pearson Education, Inc.

© 2011 Pearson Education, Inc.
Calcium Intake
• Adequate Intake (AI) varies with age and gender: 1,000 mg to 1,300 mg/day
• Upper Limit (UL): 2,500 mg• Bioavailability: body’s ability to absorb and
utilize calcium depends on• Individual’s age and calcium need • Dietary calcium and vitamin D• Binding factors (phytates, oxalates) in foods

© 2011 Pearson Education, Inc.

© 2011 Pearson Education, Inc.
Sources of Calcium
• Excellent sources include milk products • Skim milk, low-fat cheese, nonfat yogurt
• Other good sources include • Green leafy vegetables (kale, collard greens,
broccoli, and cabbage are low in oxalates)• Fortified foods (orange juice, soy milk)• Fish with edible bones (sardines, salmon)

© 2011 Pearson Education, Inc.

© 2011 Pearson Education, Inc.

© 2011 Pearson Education, Inc.
Excess Dietary Calcium
• Excess dietary calcium is excreted in feces• Mineral imbalances from supplements• Hypercalcemia (high blood calcium)• Cause: cancer or parathyroid hormone (PTH)
overproduction• Symptoms: fatigue, appetite loss, constipation,
mental confusion, calcium deposits in soft tissues

© 2011 Pearson Education, Inc.
Calcium Deficiency
• Osteoporosis from long-term calcium deficiency
• Hypocalcemia (low blood calcium) • Causes: kidney disease, vitamin D deficiency, or
diseases that inhibit the production of PTH • Symptoms: muscle spasms and convulsions

© 2011 Pearson Education, Inc.
Vitamin D
• Fat-soluble vitamin• Excess is stored in liver, adipose tissue• Can be synthesized by the body from
exposure to UV rays from the sun• Considered a hormone: synthesized in one
location and regulates activities in other parts of the body

© 2011 Pearson Education, Inc.

© 2011 Pearson Education, Inc.
Functions of Vitamin D
• Regulates blood calcium levels (regulates calcium and phosphorus absorption from the small intestine)
• Stimulates osteoclasts when calcium is needed elsewhere in the body
• Required for bone calcification
Activation of Vitamin D

© 2011 Pearson Education, Inc.
Vitamin D Adequacy
• AI: assume sun exposure is inadequate• Inadequate sun in the winter (latitude of more
than 40°N or more than 40°S)• Darker skin (more melanin pigment) reduces
the penetration of sunlight• People >65 years: decreased capacity to
synthesize vitamin D from the sun • Obesity: lower circulating vitamin D levels

© 2011 Pearson Education, Inc.

© 2011 Pearson Education, Inc.
Vitamin D Adequacy
• AI: 5 to 15 µg/day depending on age• UL: 50 µg/day for all age groups • Controversy: recent evidence suggests that
the current AI is not sufficient to maintain optimal bone health and reduce the risks for diseases such as cancer

© 2011 Pearson Education, Inc.

© 2011 Pearson Education, Inc.
Sources of Vitamin D
• Ergocalciferol (D2)—plants, supplements
• Cholecalciferol (D3)—animal foods, sun
• Most foods naturally contain little vitamin D• Mostly obtained from fortified foods (e.g., milk)• High amounts: cod liver oil, fatty fish (salmon,
mackerel, and sardines)• Vegetarians not consuming milk products receive
vitamin D from the sun, fortified soy or cereal products, or supplements

© 2011 Pearson Education, Inc.

© 2011 Pearson Education, Inc.
Vitamin D
• What happens if you consume too much?• Results in hypercalcemia
• What if you don’t consume enough?• Loss of bone mass: from fat malabsorption• Rickets (children), osteomalacia (adults)• Medications alter vitamin D metabolism and
activity: glucocorticoids, phenobarbital

© 2011 Pearson Education, Inc.
© 2011 Pearson Education, Inc.
Vitamin K
• Fat-soluble vitamin stored in the liver• Phylloquinone—plant form of vitamin K• Menaquinone—animal form of vitamin K
produced by bacteria in the large intestine• Functions of vitamin K• Blood coagulation• Bone metabolism

© 2011 Pearson Education, Inc.

© 2011 Pearson Education, Inc.
Vitamin K
• “Gla” protein production• Osteocalcin: secreted by osteoblasts (bone
remodeling)• Matrix Gla protein: in protein matrix of bone,
cartilage, blood vessel walls, soft tissues

© 2011 Pearson Education, Inc.
Vitamin K
• Recommended intake• AI values are 120 µg/day for men and 90 µg/day
for women
• Sources of vitamin K• Synthesized by bacteria in the large intestine• Green leafy vegetables, vegetable oils

© 2011 Pearson Education, Inc.

© 2011 Pearson Education, Inc.
Vitamin K
• What if you consume too much?• No known side effects from large quantities
• What if you don’t consume enough?• Reduced blood clotting, excessive bleeding• Fat malabsorption (celiac disease, Crohn’s
disease, and cystic fibrosis) • Long-term use of antibiotics can lead to deficiency• Injection of vitamin K at birth for newborns

© 2011 Pearson Education, Inc.
Phosphorus
• Phosphorus (as phosphate) is the major intracellular negatively charged electrolyte
• Functions of phosphorus• Critical in bone formation• Required for proper fluid balance• Component of ATP, DNA, membranes

© 2011 Pearson Education, Inc.
Sources of Phosphorus
• High in protein-containing foods such as milk, meats, eggs
• In processed foods as a food additive: smoothness, binding, and moisture retention
• In soft drinks as phosphoric acid (milk-displacement effect)

© 2011 Pearson Education, Inc.
Phosphorus
• What if you consume too much?• Excessive vitamin D supplements or phosphorus-
containing antacids can cause high phosphorus levels (muscle spasms and convulsions)
• What if you don’t consume enough?• Deficiencies are rare in healthy adults• Can occur in alcohol abuse, premature infants,
and elderly people with poor diets

© 2011 Pearson Education, Inc.
Magnesium
• Kidneys regulate blood magnesium levels• Functions of magnesium• Mineral found in bone structure• Cofactor for over 300 enzyme systems• Required for ATP, DNA, and proteins• Supports vitamin D metabolism, muscle
contraction, and blood clotting

© 2011 Pearson Education, Inc.
Magnesium
• Recommended intake• RDA varies based on age and gender• UL (pharmacological): 350 mg/day
• Sources of magnesium• Green leafy vegetables, whole grains, seeds,
nuts, seafood, beans, some dairy products• Dietary protein enhances absorption and retention

© 2011 Pearson Education, Inc.

© 2011 Pearson Education, Inc.
Magnesium
• What if you consume too much?• Excess supplements cause diarrhea, nausea,
cramps, dehydration, acid–base imbalances• Hypermagnesemia occurs in individuals with
impaired kidney function (antacid)
• What if you don’t consume enough?• Hypomagnesemia: results in hypocalcemia;
associated with osteoporosis, heart disease, high blood pressure, type 2 diabetes

© 2011 Pearson Education, Inc.
Fluoride
• Trace mineral• Stored in teeth and bones• Functions of fluoride• Develop and maintain teeth and bones• Combines with calcium and phosphorus to protect
teeth from bacteria

© 2011 Pearson Education, Inc.
Fluoride
• Recommended intake• AI varies by gender and increases with age,
ranging from 1 to 4 mg/day
• Sources of fluoride• Fluoridated dental products• Fluoridated water (not in bottled water)

© 2011 Pearson Education, Inc.
Fluoride
• What if you consume too much fluoride?• Fluorosis (excess fluoride) increases the protein
content of tooth enamel and makes teeth porous; teeth become stained and pitted
• What if you don’t consume enough?• Dental caries (cavities)

© 2011 Pearson Education, Inc.

© 2011 Pearson Education, Inc.
Osteoporosis
• A disease characterized by• Low bone mass• Deterioration of bone tissue• Fragile bones leading to bone-fracture risk• Compaction of bone: decreased height• Shortening and hunching of the spine: kyphosis
(dowager’s hump)

© 2011 Pearson Education, Inc.

© 2011 Pearson Education, Inc.

© 2011 Pearson Education, Inc.
Osteoporosis
• Risk factors for osteoporosis include:• Age • Gender• Smoking• Poor nutrition• Physical inactivity

© 2011 Pearson Education, Inc.

© 2011 Pearson Education, Inc.
Age
• Bone mass decreases with age• Age-related hormonal (estrogen and
testosterone) changes influence bone density• Decreased vitamin D metabolism with age

© 2011 Pearson Education, Inc.
Gender
• 80% of Americans with osteoporosis: women• Women have lower bone density than men• Low estrogen production increases bone loss:
postmenopausal women and adolescent girls (extreme dieting)
• At risk: Caucasian women of low body weight with first-degree relative (mother or sister) with osteoporosis

© 2011 Pearson Education, Inc.
Smoking and Poor Nutrition
• Cigarette smoking effects hormones that influence bone formation and resorption
• Alcoholism is associated with fractures• Caffeine increases urinary calcium loss• Dietary protein and calcium interaction• Low calcium and vitamin D intakes result in
low bone density

© 2011 Pearson Education, Inc.
Physical Inactivity
• Regular exercise stresses bone tissues, stimulates bone density
• Weight-bearing activities (walking, jogging) are helpful in increasing bone mass

© 2011 Pearson Education, Inc.
Female Athlete Triad
• Low energy availability (with or without eating disorders)
• Amenorrhea: hormonal changes (estrogen reduction) result in loss of menstruation
• Osteoporosis

© 2011 Pearson Education, Inc.
Treatment for Osteoporosis
• There is no cure for osteoporosis• These slow the progression of osteoporosis:• Adequate calcium and vitamin D intake• Regular exercise (weight-bearing)• Anti-resorptive medications