# 293 measuring prevalence and incidence of antimicrobial
TRANSCRIPT
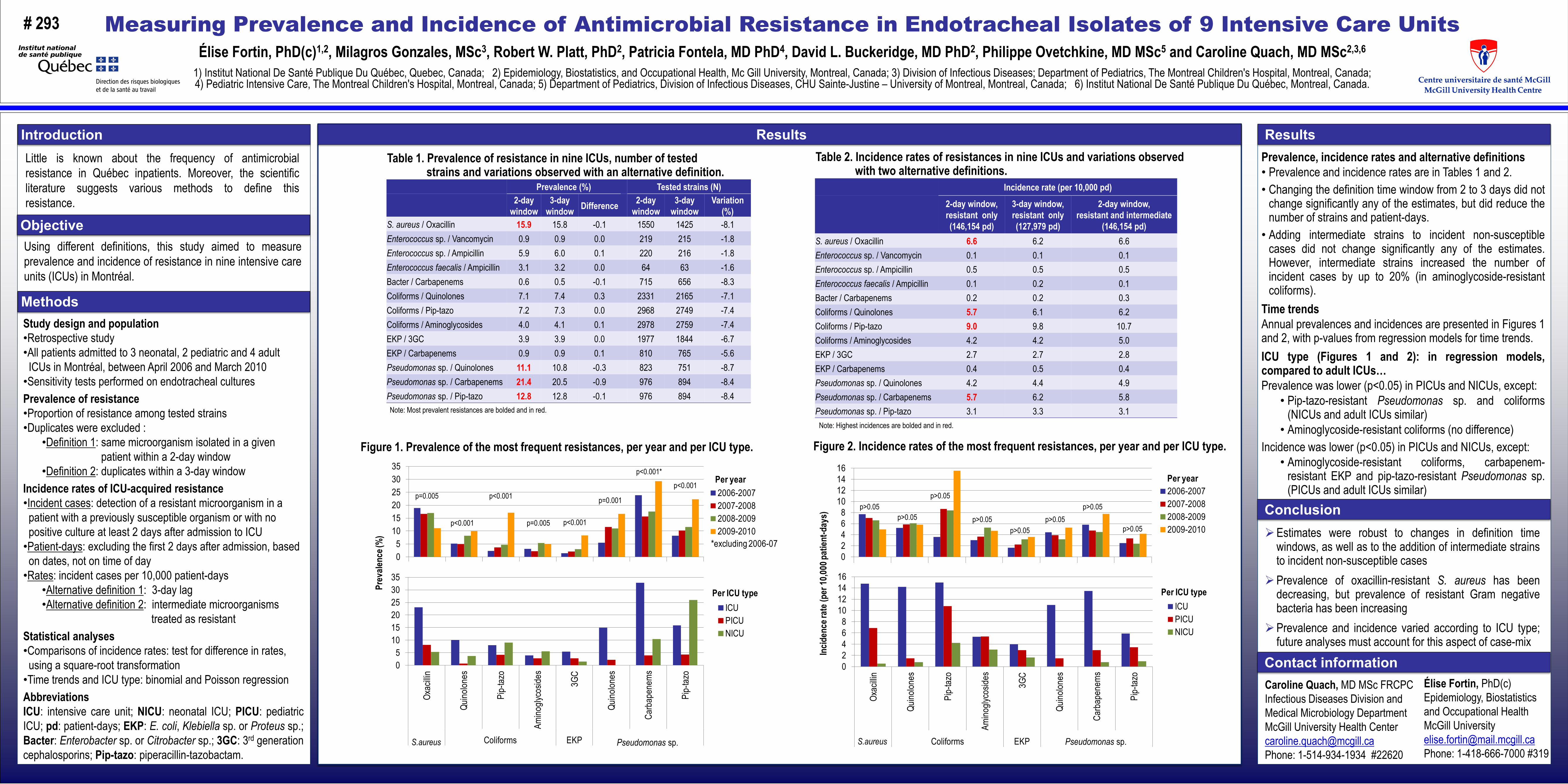
Table 2. Incidence rates of resistances in nine ICUs and variations observed with two alternative definitions.
Note: Highest incidences are bolded and in red.
Table 1. Prevalence of resistance in nine ICUs, number of tested strains and variations observed with an alternative definition.
Note: Most prevalent resistances are bolded and in red.
Measuring Prevalence and Incidence of Antimicrobial Resistance in Endotracheal Isolates of 9 Intensive Care UnitsÉlise Fortin, PhD(c)1,2, Milagros Gonzales, MSc3, Robert W. Platt, PhD2, Patricia Fontela, MD PhD4, David L. Buckeridge, MD PhD2, Philippe Ovetchkine, MD MSc5 and Caroline Quach, MD MSc2,3,6
1) Institut National De Santé Publique Du Québec, Quebec, Canada; 2) Epidemiology, Biostatistics, and Occupational Health, Mc Gill University, Montreal, Canada; 3) Division of Infectious Diseases; Department of Pediatrics, The Montreal Children's Hospital, Montreal, Canada; 4) Pediatric Intensive Care, The Montreal Children's Hospital, Montreal, Canada; 5) Department of Pediatrics, Division of Infectious Diseases, CHU Sainte-Justine – University of Montreal, Montreal, Canada; 6) Institut National De Santé Publique Du Québec, Montreal, Canada.
Methods
Results
Contact information
Conclusion
IntroductionLittle is known about the frequency of antimicrobialresistance in Québec inpatients. Moreover, the scientificliterature suggests various methods to define thisresistance.
Objective
Study design and population•Retrospective study•All patients admitted to 3 neonatal, 2 pediatric and 4 adult
ICUs in Montréal, between April 2006 and March 2010•Sensitivity tests performed on endotracheal culturesPrevalence of resistance•Proportion of resistance among tested strains•Duplicates were excluded :
•Definition 1: same microorganism isolated in a givenpatient within a 2-day window
•Definition 2: duplicates within a 3-day windowIncidence rates of ICU-acquired resistance•Incident cases: detection of a resistant microorganism in a
patient with a previously susceptible organism or with nopositive culture at least 2 days after admission to ICU•Patient-days: excluding the first 2 days after admission, based
on dates, not on time of day•Rates: incident cases per 10,000 patient-days
•Alternative definition 1: 3-day lag•Alternative definition 2: intermediate microorganisms
treated as resistantStatistical analyses•Comparisons of incidence rates: test for difference in rates,
using a square-root transformation•Time trends and ICU type: binomial and Poisson regressionAbbreviationsICU: intensive care unit; NICU: neonatal ICU; PICU: pediatricICU; pd: patient-days; EKP: E. coli, Klebiella sp. or Proteus sp.;Bacter: Enterobacter sp. or Citrobacter sp.; 3GC: 3rd generationcephalosporins; Pip-tazo: piperacillin-tazobactam.
Using different definitions, this study aimed to measureprevalence and incidence of resistance in nine intensive careunits (ICUs) in Montréal.
Caroline Quach, MD MSc FRCPCInfectious Diseases Division and Medical Microbiology Department McGill University Health [email protected]: 1-514-934-1934 #22620
# 293
Estimates were robust to changes in definition timewindows, as well as to the addition of intermediate strainsto incident non-susceptible cases
Prevalence of oxacillin-resistant S. aureus has beendecreasing, but prevalence of resistant Gram negativebacteria has been increasing
Prevalence and incidence varied according to ICU type;future analyses must account for this aspect of case-mix
Prevalence, incidence rates and alternative definitions• Prevalence and incidence rates are in Tables 1 and 2.• Changing the definition time window from 2 to 3 days did not
change significantly any of the estimates, but did reduce thenumber of strains and patient-days.
• Adding intermediate strains to incident non-susceptiblecases did not change significantly any of the estimates.However, intermediate strains increased the number ofincident cases by up to 20% (in aminoglycoside-resistantcoliforms).
Time trendsAnnual prevalences and incidences are presented in Figures 1and 2, with p-values from regression models for time trends.ICU type (Figures 1 and 2): in regression models,compared to adult ICUs…Prevalence was lower (p<0.05) in PICUs and NICUs, except:
• Pip-tazo-resistant Pseudomonas sp. and coliforms(NICUs and adult ICUs similar)
• Aminoglycoside-resistant coliforms (no difference)Incidence was lower (p<0.05) in PICUs and NICUs, except:
• Aminoglycoside-resistant coliforms, carbapenem-resistant EKP and pip-tazo-resistant Pseudomonas sp.(PICUs and adult ICUs similar)
Results
Prevalence (%) Tested strains (N)2-day
window3-day
window Difference 2-day window
3-day window
Variation (%)
S. aureus / Oxacillin 15.9 15.8 -0.1 1550 1425 -8.1Enterococcus sp. / Vancomycin 0.9 0.9 0.0 219 215 -1.8Enterococcus sp. / Ampicillin 5.9 6.0 0.1 220 216 -1.8Enterococcus faecalis / Ampicillin 3.1 3.2 0.0 64 63 -1.6Bacter / Carbapenems 0.6 0.5 -0.1 715 656 -8.3Coliforms / Quinolones 7.1 7.4 0.3 2331 2165 -7.1Coliforms / Pip-tazo 7.2 7.3 0.0 2968 2749 -7.4Coliforms / Aminoglycosides 4.0 4.1 0.1 2978 2759 -7.4EKP / 3GC 3.9 3.9 0.0 1977 1844 -6.7EKP / Carbapenems 0.9 0.9 0.1 810 765 -5.6Pseudomonas sp. / Quinolones 11.1 10.8 -0.3 823 751 -8.7Pseudomonas sp. / Carbapenems 21.4 20.5 -0.9 976 894 -8.4Pseudomonas sp. / Pip-tazo 12.8 12.8 -0.1 976 894 -8.4
Incidence rate (per 10,000 pd)
2-day window, resistant only (146,154 pd)
3-day window, resistant only (127,979 pd)
2-day window, resistant and intermediate
(146,154 pd)S. aureus / Oxacillin 6.6 6.2 6.6Enterococcus sp. / Vancomycin 0.1 0.1 0.1Enterococcus sp. / Ampicillin 0.5 0.5 0.5Enterococcus faecalis / Ampicillin 0.1 0.2 0.1Bacter / Carbapenems 0.2 0.2 0.3Coliforms / Quinolones 5.7 6.1 6.2Coliforms / Pip-tazo 9.0 9.8 10.7Coliforms / Aminoglycosides 4.2 4.2 5.0EKP / 3GC 2.7 2.7 2.8EKP / Carbapenems 0.4 0.5 0.4Pseudomonas sp. / Quinolones 4.2 4.4 4.9Pseudomonas sp. / Carbapenems 5.7 6.2 5.8Pseudomonas sp. / Pip-tazo 3.1 3.3 3.1
Figure 2. Incidence rates of the most frequent resistances, per year and per ICU type. Figure 1. Prevalence of the most frequent resistances, per year and per ICU type.
Prev
alenc
e (%
)
05
101520253035
Oxac
illin
Quino
lones
Pip-
tazo
Amino
glyco
sides
3GC
Quino
lones
Carb
apen
ems
Pip-
tazo
S. aureus Coliforms EKP Pseudomonas sp.
ICUPICUNICU
Per ICU type
S.aureus Pseudomonas sp.
05
101520253035
2006-20072007-20082008-20092009-2010
Per year
*excluding 2006-07
p=0.005
p<0.001
p<0.001
p=0.005 p<0.001
p=0.001
p<0.001
p<0.001*
Élise Fortin, PhD(c)Epidemiology, Biostatistics and Occupational HealthMcGill [email protected]: 1-418-666-7000 #319
Incid
ence
rate
(per
10,00
0 pat
ient-d
ays)
02468
10121416
Oxac
illin
Quino
lones
Pip-
tazo
Amino
glyco
sides
3GC
Quino
lones
Carb
apen
ems
Pip-
tazo
S. aureus Coliforms EKP Pseudomonas sp.
ICU
PICUNICU
Per ICU type
S.aureus Pseudomonas sp.
02468
10121416
s o s s s o
2006-20072007-20082008-20092009-2010
Per year
p>0.05p>0.05
p>0.05
p>0.05p>0.05
p>0.05p>0.05
p>0.05