基础分物学 - bio.pku.edu.cn
TRANSCRIPT


Chapter 9 - Outline❖ 9.1 Molecular Mechanism of Disease_Pathology Perspective
❖ Cell Death❖ Acute & Chronic Inflammation❖ Infection & Host Response❖ Neoplasia
❖ 9.2 Molecular Mechanism of Disease_Molecular Biology Perspective❖ 9.3 Molecular Pathology of Disease
❖ Cancer❖ Infectious Disease❖ Inherited Disease❖ Metabolic Disease
❖ 9.4 Practice of Molecular Medicine❖ Molecular Diagnosis❖ Pharmacogenomics & Personal Medicine
2

Acquired Capabilities of Cancer
3

Sustaining Proliferative Signaling
4

Seven Types of Proteins that Participate in Controlling Cell Growth and Proliferation
Oncoproteins❖ Extracellular signaling molecules (I)❖ Signal receptors (II)❖ Signal-transduction proteins (III)❖ Transcription factors (IV)
Tumor suppressors❖ Cell cycle control proteins (VI)❖ DNA-repair proteins (VII)
❖ Apoptotic proteins (V) include tumor suppressors that promote apoptosis and oncoproteins that promote cell survival.
❖ Virus encoded proteins that activate signal receptors (Ia) also can induce cancer.
Lehninger, Principles of Biochemistry, 4th Edition5

Lehninger, Principles of Biochemistry, 4th Edition6

Evading Growth Suppressors
7

Cell Cycle and Loss of Cell Cycle Control
Burger’s Medicinal Chemistry and Drug Discovery, 6th Edition, Vol. 5. ISBN 0-471-37031-2, 2003.8

Loss of p53 Abolishes the DNA-Damage Checkpoint
9
Resisting Cell Death
10

Apoptosis and Reduced Sensitivity to Apoptosis
Burger’s Medicinal Chemistry and Drug Discovery, 6th Edition, Vol. 5. ISBN 0-471-37031-2, 2003.11

Brown, C.J., Lain, S., Verma, C.S., Fersht, A.R., and Lane, D.P. (2009). Awakening guardian angels: drugging the p53 pathway. Nat Rev Cancer 9, 862-873.
p53 Tumor Suppressor
12

Activating Invasion and Metastasis
13

Cancer Tends to Involve Multiple Mutations
Malignant cells invade neighboring tissues, enter blood vessels, and metastasize to different sites
More mutations, more genetic instability, metastatic disease
Proto-oncogenes mutate to oncogenes
Mutations inactivate DNA repair genes
Cells proliferate
Mutation inactivates suppressor gene
Benign tumor cells grow only locally and cannot spread by invasion or metastasis
Time
14

15
Linear Progression Model of Cancer
❖ A sequence of events must occur before a normal cell becomes malignant.
❖ At least three tumor suppressor genes and one oncogene must be mutated in sequence for an epithelial cell in the colon to become metastatic.
❖ Although the likelihood of this happening to any given cell is small, the colon has millions of cells that divide constantly in the presence of carcinogens.

❖ Histologic and molecular changes in the development of pulmonary squamous cell carcinoma. These changes occur in a stepwise fashion, beginning in histologically normal epithelium.
16
Linear Progression Model of Cancer

Cancer Tends to Corrupt Surrounding Environment
Growth factors = proliferation
Blood vessel
Proteases
Cytokines
Matrix
Fibroblasts, adipocytes
Invasive
Cytokines, proteases = migration & invasion17

Cancer Metastasis
18

Inducing Angiogenesis
19

Tumor Growth Requires Formation of New Blood Vessels
❖ Tumors, whether primary or secondary, require recruitment of new blood vessels in order to grow to a large mass. In the absence of a blood supply, a tumor can grow into a mass of about 106 cells, roughly a sphere 2 mm in diameter.
❖ Most tumors induce the formation of new blood vessels that invade the tumor and nourish it, a process called angiogenesis.
❖ This complex process requires several discrete steps: degradation of the basal lamina that surrounds a nearby capillary, migration of endothelial cells lining the capillary into the tumor, division of these endothelial cells, formation of a new basement membrane around the newly elongated capillary.
20
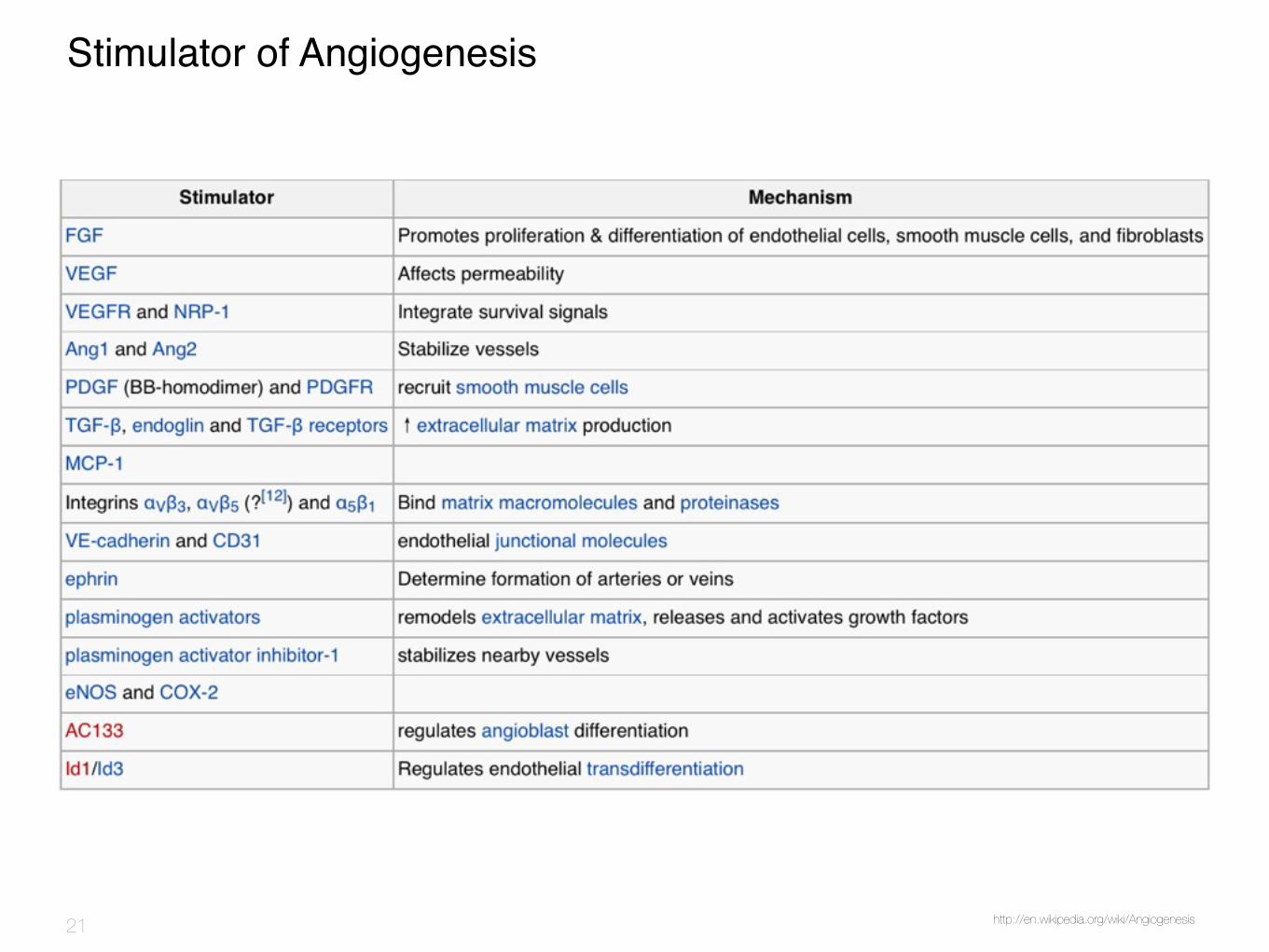
Stimulator of Angiogenesis
http://en.wikipedia.org/wiki/Angiogenesis21

Enabling Replicative Immortality
22

23

Changes in telomere length over time during tumour progression, compared with changes in normal tissue
Blasco, M.A. (2005). Telomeres and human disease: ageing, cancer andbeyond. Nat. Rev. Genet. 6, 611–622.24

25

26

Chapter 9 - Outline❖ 9.1 Molecular Mechanism of Disease_Pathology Perspective
❖ Cell Death❖ Acute & Chronic Inflammation❖ Infection & Host Response❖ Neoplasia
❖ 9.2 Molecular Mechanism of Disease_Molecular Biology Perspective❖ 9.3 Molecular Pathology of Disease
❖ Cancer❖ Infectious Disease❖ Inherited Disease❖ Metabolic Disease
❖ 9.4 Practice of Molecular Medicine❖ Molecular Diagnosis❖ Pharmacogenomics & Personal Medicine
27

Chapter 9 - Outline❖ 9.3 Molecular Pathology of Disease
❖ Cancer❖ Infectious Disease
❖ General Concepts❖ Viral Infection: HIV, HBV & HCV❖ Bacterial Infection
❖ Inherited Disease❖ Metabolic Disease
28

Chapter 9 - Outline❖ 9.3 Molecular Pathology of Disease
❖ Cancer❖ Infectious Disease
❖ General Concepts❖ Viral Infection: HIV, HBV & HCV❖ Bacterial Infection
❖ Inherited Disease❖ Metabolic Disease
29

Disease Categories
❖ Infectious Disease Organisms that cause disease inside the human body are called pathogens
❖ Bacteria and Viruses are the best known pathogens❖ Fungi, protozoa and parasites can also cause disease❖ Diseases are said to be infectious or communicable if pathogens
can be passed from one person to another
❖ Non-infectious Disease: Diseases that are not caused by pathogens
30
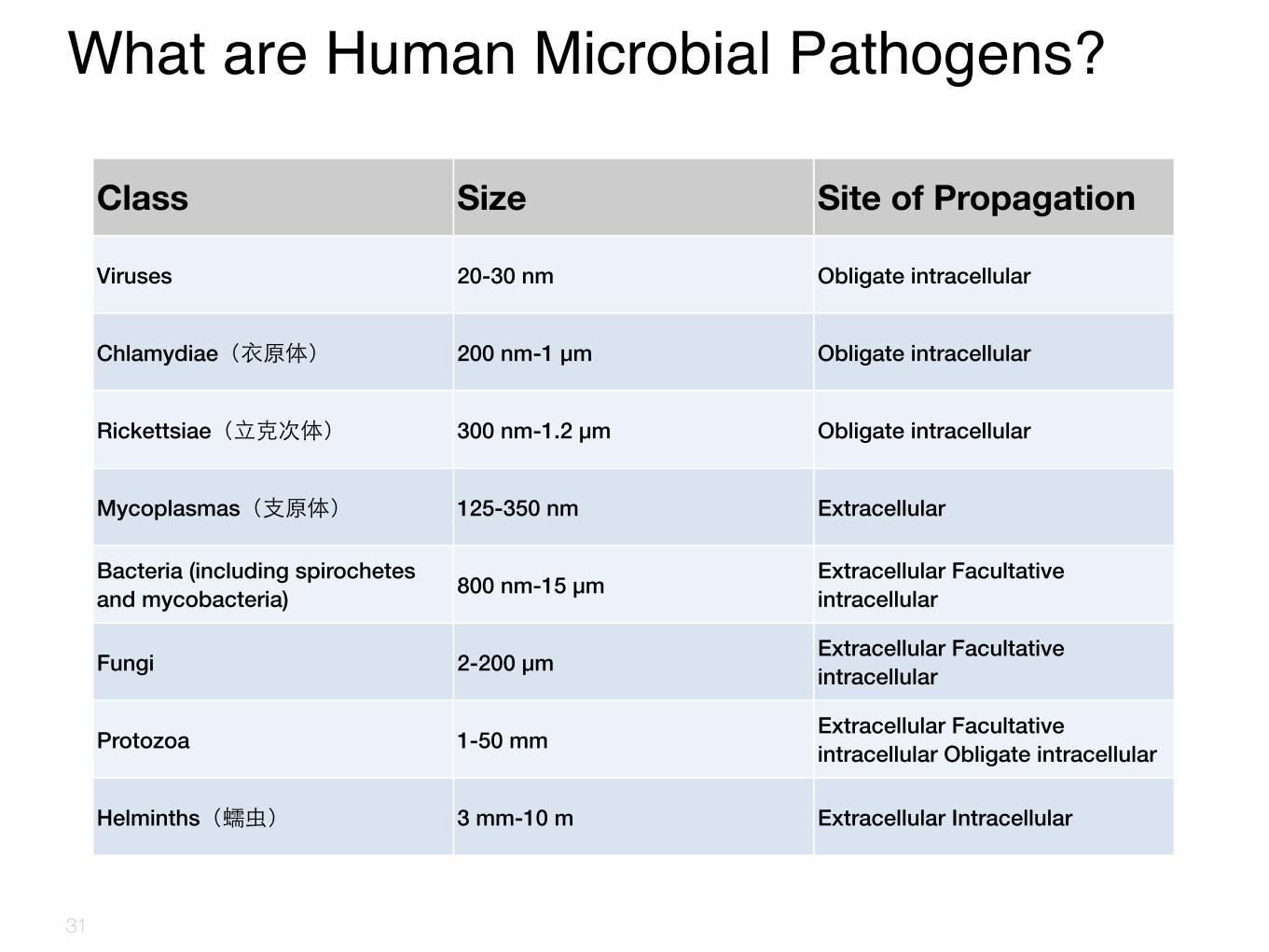
What are Human Microbial Pathogens?
31
Class Size Site of Propagation
Viruses 20-30 nm Obligate intracellular
Chlamydiae(⾐衣原体) 200 nm-1 μm Obligate intracellular
Rickettsiae(⽴立克次体) 300 nm-1.2 μm Obligate intracellular
Mycoplasmas(⽀支原体) 125-350 nm Extracellular
Bacteria (including spirochetes and mycobacteria) 800 nm-15 μm Extracellular Facultative
intracellular
Fungi 2-200 μm Extracellular Facultative intracellular
Protozoa 1-50 mm Extracellular Facultative intracellular Obligate intracellular
Helminths(蠕⾍虫) 3 mm-10 m Extracellular Intracellular

✤ Stomach Cancer: 555,000 new cases per year due to Helicobacter pylori
✤ Cervical Cancer: increased risk due to human papilloma virus
✤ Liver Cancer: 8 in 10 cases due to Hepatitis B or C
✤ Hodgkin’s Disease: can be caused by Epstein-Barr virus
✤ Atherosclerosis: Chlamydia pneumoniae may contribute to its progression
Sources: American Society for Microbiology. New and Reemerging Infectious Diseases: A Global Crisis and Immediate Threat to the Nation’s Health, The Role of Research. Washington, D.C.: ASM, 1997. Cited in Emerging Crisis in Infectious Diseases.Volume 70: Epstein-Barr virus and Kaposi’s sarcoma herpesvirus/human herpesvirus 8. IARC monographs on the Evaluation of Carcinogenic Risks to Humans. 1997. Cited in Emerging Crisis in Infectious Diseases.Bahrmand AR, Bahadori M, et al. Chlamydia pneumonia DNA is more frequent in advanced than in mild atherosclerosis lesions. Scand J Infect Dis. 2004;36:119-123. Cited in Emerging Crisis in Infectious Diseases.
Diseases Caused by Pathogen Infection




Prion – the Mad Cow Disease

Death by Misfolding: The Prion Diseases❖ The infectious agent has been traced to a single protein (Mr 28,000), which Prusiner dubbed prion (from
proteinaceous infectious only) protein (PrP). ❖ Illness occurs only when the normal cellular PrP, or PrPC, occurs in an altered conformation called PrPSc (Sc
denotes scrapie). The interaction of PrPSc with PrPC converts the latter to PrPSc, initiating a domino effect in which more and more of the brain protein converts to the disease-causing form.
❖ In inherited forms of prion diseases, a mutation in the gene encoding PrP produces a change in one amino acid residue that is believed to make the conversion of PrPC to PrPSc more likely.
37 Lehninger Principles of Biochemistry, Fourth Edition

Chapter 9 - Outline❖ 9.3 Molecular Pathology of Disease
❖ Cancer❖ Infectious Disease
❖ General Concepts❖ Viral Infection: HIV, HBV & HCV❖ Bacterial Infection
❖ Inherited Disease❖ Metabolic Disease
38

What are HIV and AIDS?
❖ HIV is the human immunodeficiency virus. It is the virus that can lead to acquired immune deficiency syndrome, or AIDS.
❖ HIV infects primarily vital cells in the human immune system such as helper T cells (to be specific, CD4+ T cells), macrophage, and dendritic cells.
❖ AIDS is the late stage of HIV infection, when a person’s immune system is severely damaged and has difficulty fighting diseases and certain cancers.
❖ From its discovery in 1981 to 2006, AIDS killed more than 25 million people. HIV infects about 0.6% of the world's population. In 2005 alone, AIDS claimed an estimated 2.4–3.3 million lives.
❖ At this time, there is no cure for HIV infection. Despite major advances in diagnosing and treating HIV infection, in 2007, 35,962 cases of AIDS were diagnosed and 14,110 deaths among people living with HIV were reported in the United States.
http://www.cdc.gov/

Scanning Electron Micrograph of HIV-1 (in green) Budding from
40 http://en.wikipedia.org/wiki/HIV

Comparison of HIV Species
❖ There are two types of HIV, HIV-1 and HIV-2. Unless otherwise noted, the term “HIV” primarily refers to HIV-1.
❖ Both types of HIV damage a person’s body by destroying specific blood cells, called CD4+ T cells, which are crucial to helping the body fight diseases.

How AIDS Affects the Body
42

HIV Genome and Structure
❖ HIV is composed of two copies of positive single-stranded RNA that codes for the virus's nine genes enclosed by a conical capsid composed of 2,000 copies of the viral protein p24.
❖ The single-stranded RNA is tightly bound to nucleocapsid proteins, p7 and enzymes needed for the development of the virion such as reverse transcriptase, proteases, ribonuclease and integrase.
❖ A matrix composed of the viral protein p17 surrounds the capsid ensuring the integrity of the virion particle.
❖ Viral envelope: two layers of fatty molecules (phospholipids) taken from the human cell.
❖ Env: a cap (three glycoprotein (gp) 120) and a stem (three gp41).
❖ The RNA genome consists of at least 7 structural landmarks (LTR, TAR, RRE, PE, SLIP, CRS, and INS) and nine genes (gag, pol, and env, tat, rev, nef, vif, vpr, vpu, and sometimes a tenth tev, which is a fusion of tat env and rev) encoding 19 proteins.
❖ gag, pol, and env, contain information needed to make the structural proteins for new virus particles.
43

HIV-I: Genome Structure & its Major Encoded Proteins
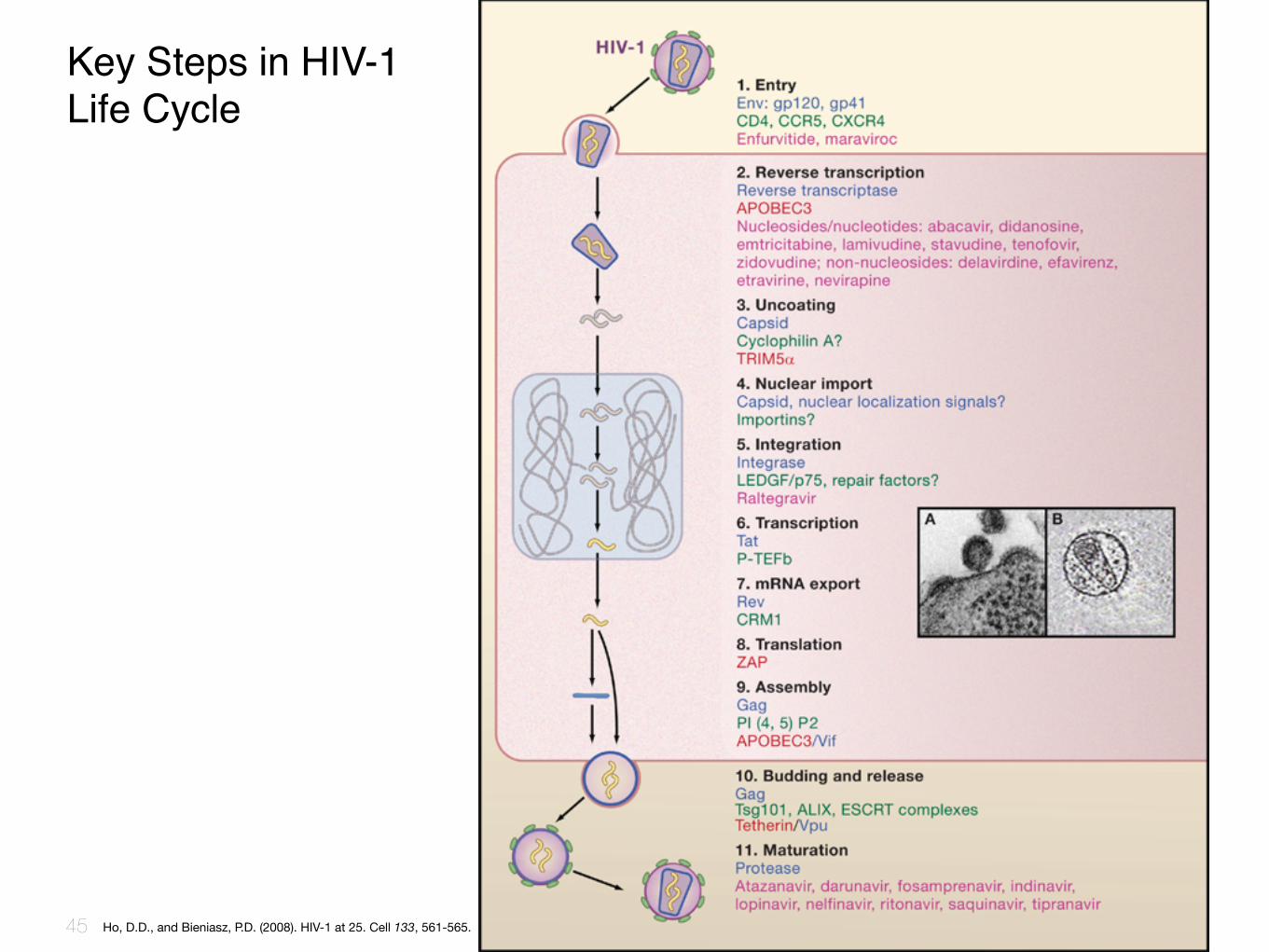
Key Steps in HIV-1 Life Cycle
45 Ho, D.D., and Bieniasz, P.D. (2008). HIV-1 at 25. Cell 133, 561-565.

Entry to the cell❖ HIV enters macrophages and CD4+ T cells by the adsorption of glycoproteins on its surface to receptors
on the target cell followed by fusion of the viral envelope with the cell membrane and the release of the HIV capsid into the cell.
❖ Entry to the cell begins through interaction of the trimeric envelope complex (gp160 spike) and both CD4 and a chemokine receptor (generally either CCR5 or CXCR4, but others are known to interact) on the cell surface.
❖ gp120 binds to integrin α4β7 activating LFA-1 the central integrin involved in the establishment of virological synapses, which facilitate efficient cell-to-cell spreading of HIV-1. The gp160 spike contains binding domains for both CD4 and chemokine receptors.
❖ After HIV has bound to the target cell, the HIV RNA and various enzymes, including reverse transcriptase, integrase, ribonuclease, and protease, are injected into the cell.
❖ During the microtubule based transport to the nucleus, the viral single strand RNA genome is transcribed into double strand DNA, which is then integrated into a host chromosome.
❖ HIV can infect dendritic cells (DCs) by this CD4-CCR5 route, but another route using mannose-specific C-type lectin receptors such as DC-SIGN can also be used. DCs are one of the first cells encountered by the virus during sexual transmission. They are currently thought to play an important role by transmitting HIV to T-cells when the virus is captured in the mucosa by DCs. The presence of FEZ-1, which occurs naturally in neurons, is believed to prevent the infection of cells by HIV.
46
Key Steps in HIV-1 Life Cycle
Replication and transcription
❖ Shortly after the viral capsid enters the cell, an enzyme called reverse transcriptase liberates the single-stranded (+)RNA genome from the attached viral proteins and copies it into a complementary DNA (cDNA) molecule.
❖ The process of reverse transcription is extremely error-prone, and the resulting mutations may cause drug resistance or allow the virus to evade the body's immune system.
❖ The reverse transcriptase also has ribonuclease activity that degrades the viral RNA during the synthesis of cDNA, as well as DNA-dependent DNA polymerase activity that creates a sense DNA from the antisense cDNA.
❖ Together, the cDNA and its complement form a double-stranded viral DNA that is then transported into the cell nucleus. The integration of the viral DNA into the host cell's genome is carried out by another viral enzyme called integrase.
47
Key Steps in HIV-1 Life Cycle

Reverse transcription of the HIV genome into double strand DNA
❖ This integrated viral DNA may then lie dormant, in the latent stage of HIV infection. To actively produce the virus, certain cellular transcription factors need to be present, the most important of which is NF-κB (NF kappa B), which is upregulated when T-cells become activated. This means that those cells most likely to be killed by HIV are those currently fighting infection.
❖ During viral replication, the integrated DNA provirus is transcribed into mRNA, which is then spliced into smaller pieces. These small pieces are exported from the nucleus into the cytoplasm, where they are translated into the regulatory proteins Tat (which encourages new virus production) and Rev.
❖ As the newly produced Rev protein accumulates in the nucleus, it binds to viral mRNAs and allows unspliced RNAs to leave the nucleus, where they are otherwise retained until spliced.
❖ At this stage, the structural proteins Gag and Env are produced from the full-length mRNA. The full-length RNA is actually the virus genome; it binds to the Gag protein and is packaged into new virus particles.
❖ HIV-1 and HIV-2 appear to package their RNA differently; HIV-1 will bind to any appropriate RNA, whereas HIV-2 will preferentially bind to the mRNA that was used to create the Gag protein itself. This may mean that HIV-1 is better able to mutate (HIV-1 infection progresses to AIDS faster than HIV-2 infection and is responsible for the majority of global infections).
48
Key Steps in HIV-1 Life Cycle

Reverse Transcription
49
1. A specific cellular tRNA acts as a primer and hybridizes to a complementary part of the virus genome called the primer binding site or PBS
2. Complementary DNA then binds to the U5 (non-coding region) and R region (a direct repeat found at both ends of the RNA molecule) of the viral RNA
3. A domain on the reverse transcriptase enzyme called RNAse H degrades the 5’ end of the RNA which removes the U5 and R region
4. The primer then ‘jumps’ to the 3’ end of the viral genome and the newly synthesized DNA strands hybridizes to the complementary R region on the RNA
5. The first strand of complementary DNA (cDNA) is extended and the majority of viral RNA is degraded by RNAse H
6. Once the strand is completed, second strand synthesis is initiated from the viral RNA
7. There is then another ‘jump’ where the PBS from the second strand hybridizes with the complementary PBS on the first strand
8. Both strands are extended further and can be incorporated into the hosts genome by the enzyme integrase

Assembly and release
❖ The final step of the viral cycle, assembly of new HIV-1 virons, begins at the plasma membrane of the host cell. The Env polyprotein (gp160) goes through the endoplasmic reticulum and is transported to the Golgi complex where it is cleaved by protease and processed into the two HIV envelope glycoproteins gp41 and gp120.
❖ These are transported to the plasma membrane of the host cell where gp41 anchors the gp120 to the membrane of the infected cell. The Gag (p55) and Gag-Pol (p160) polyproteins also associate with the inner surface of the plasma membrane along with the HIV genomic RNA as the forming virion begins to bud from the host cell.
❖ Maturation either occurs in the forming bud or in the immature virion after it buds from the host cell. During maturation, HIV proteases cleave the polyproteins into individual functional HIV proteins and enzymes.
❖ The various structural components then assemble to produce a mature HIV virion. This cleavage step can be inhibited by protease inhibitors. The mature virus is then able to infect another cell.
50
Key Steps in HIV-1 Life Cycle
Retrovirus reverse transcripiton
51

HIV Attenuates Host Immune Response
❖ HIV粒⼦子表⾯面的gp120蛋⽩白脱落,与正常细胞膜上CD4受体结合,使该细胞被免疫系统误认为病毒感染细胞⽽而遭杀灭。
❖ 因T细胞CD4受体被gp120封闭,影响了其免疫辅助功能。
❖ HIV的gp120蛋⽩白可刺激机体产⽣生抗CD4结合部位的特异性抗体,阻断T细胞功能。
❖ 带有病毒包膜蛋⽩白的细胞可与其他细胞融合形成多核巨细胞⽽而丧失功能。
52

HIV Treatment
❖ HAART: protease inhibitor-based treatment initially became available since 1996. Current options are combinations (or "cocktails") of at least three drugs belonging to at least two types, or "classes," of antiretroviral agents. Typically, these classes are two nucleoside analogue reverse transcriptase inhibitors (NARTIs or NRTIs) plus either a protease inhibitor or a non-nucleoside reverse transcriptase inhibitor.
❖ HAART neither cures the patient nor does it uniformly remove all symptoms; high levels of HIV-1, often HAART resistant, return if treatment is stopped.
❖ In July 2010, a vaginal gel containing tenofovir, a reverse transcriptase inhibitor, was shown to reduce HIV infection rates by 39 percent in a trial conducted in South Africa.
❖ Research to improve current treatments includes decreasing side effects of current drugs, further simplifying drug regimens to improve adherence, and determining the best sequence of regimens to manage drug resistance.
❖ However, after over 20 years of research, HIV-1 remains a difficult target for a vaccine.
53

Key Steps in HIV-1 Life Cycle
54 Ho, D.D., and Bieniasz, P.D. (2008). HIV-1 at 25. Cell 133, 561-565.

HIV Replication
55


Viral Hepatitis❖ Hepatitis is an inflammation of the liver characterized by the presence of
inflammatory cells in the tissue of the organ.
❖ The condition can be self-limiting (healing on its own) or can progress to fibrosis (scarring) and cirrhosis.
❖ Hepatitis may occur with limited or no symptoms, but often leads to jaundice, anorexia (poor appetite) and malaise.
❖ Hepatitis is acute when it lasts less than six months and chronic when it persists longer.
❖ A group of viruses known as the hepatitis viruses cause most cases of hepatitis worldwide, and the most common types are Hepatitis A, Hepatitis B, and Hepatitis C.
❖ Viral hepatitis is the leading cause of liver cancer and the most common reason for liver transplantation.
57 http://www.cdc.gov/
Some Terminology
❖ Acute(急性)❖ Chronic(慢性)❖ Fulminant(爆发性)❖ Cirrhosis(肝硬化)❖ Jaundice(⻩黄疸): Yellowing of the skin, eyes, etc due to
raised levels of bilirubin in the blood due to liver damage.
❖ Anorexia (poor appetite) : 厌⾷食❖ Hepatocellular carcinoma(HCC, 肝细胞癌): is closely
associated with hepatitis B, and at least in some regions of the world with hepatitis C virus.
58
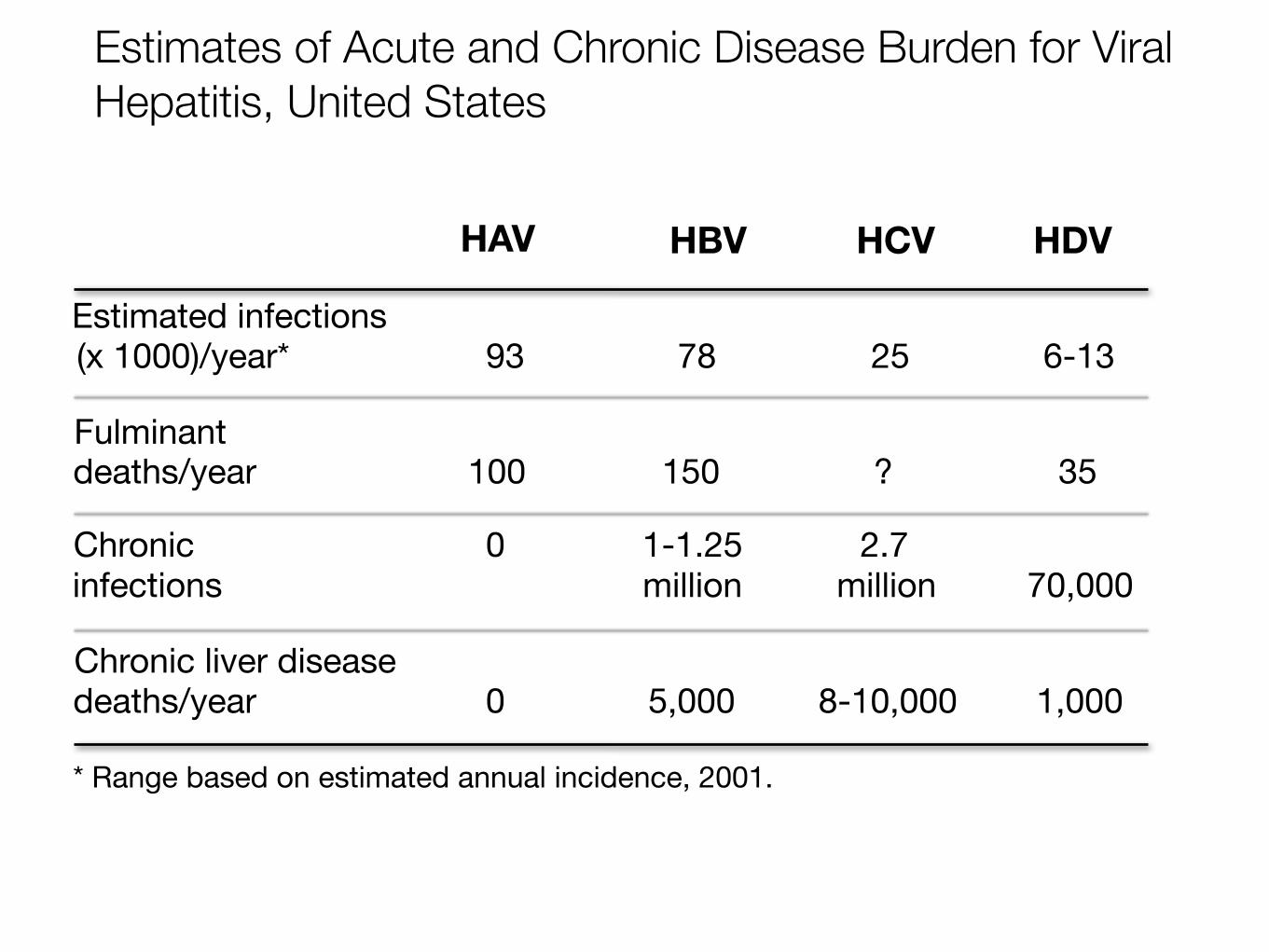
Estimates of Acute and Chronic Disease Burden for Viral Hepatitis, United States
Estimated infections(x 1000)/year* 93 78 25 6-13
Fulminant deaths/year 100 150 ? 35
Chronicinfections
0 1-1.25 million
2.7million 70,000
Chronic liver disease deaths/year 0 5,000 8-10,000 1,000
* Range based on estimated annual incidence, 2001.
HAV HBV HCV HDV
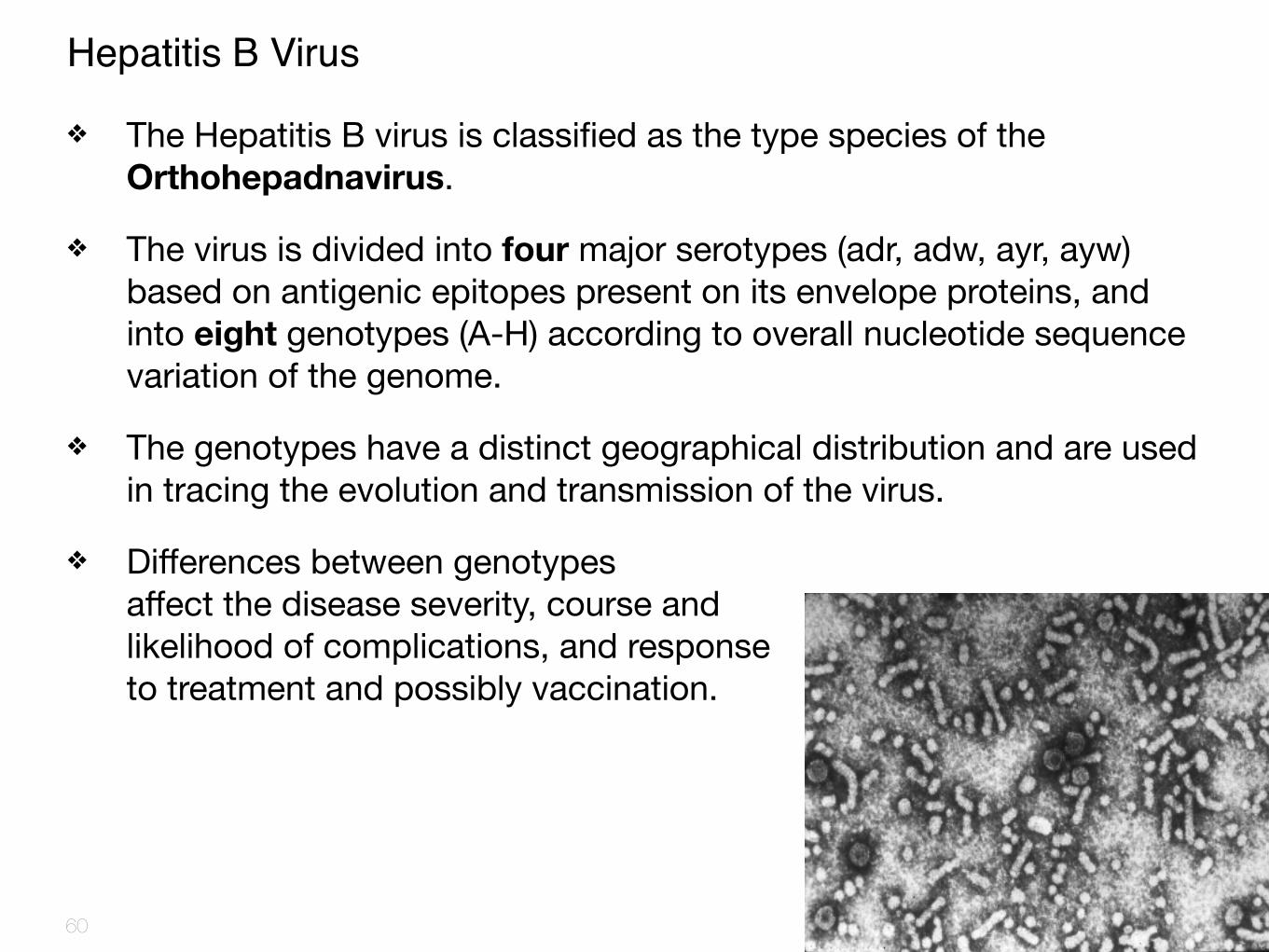
Hepatitis B Virus
❖ The Hepatitis B virus is classified as the type species of the Orthohepadnavirus.
❖ The virus is divided into four major serotypes (adr, adw, ayr, ayw) based on antigenic epitopes present on its envelope proteins, and into eight genotypes (A-H) according to overall nucleotide sequence variation of the genome.
❖ The genotypes have a distinct geographical distribution and are used in tracing the evolution and transmission of the virus.
❖ Differences between genotypes affect the disease severity, course and likelihood of complications, and response to treatment and possibly vaccination.
60

HBV Structure and Antigens
61
42 nm
HBsAg (4 phenotype: adw, adr, ayw, ayr)
HBcAg(Single serotype)
HBeAg (HBcAg splice varient, secreted protein)
(mostly dsDNA, 3200bp)

HBV Genome
❖ The genome of HBV is made of not-fully-double-stranded circular DNA.
❖ One end of the full length strand is linked to the viral DNA polymerase.
❖ The genome is 3020-3320 nucleotides long (for the full length strand) and 1700-2800 nucleotides long (for the short length strand).
62

HBV Genome
The negative-sense, (non-coding), is complementary to the viral mRNA.
❖ The partially dsDNA is rendered fully double-stranded by completion of the (+) sense strand and removal of a protein molecule from the (-) sense strand and a short sequence of RNA from the (+) sense strand. Non-coding bases are removed from the ends of the (-)sense strand and the ends are rejoined.
❖ There are four known genes encoded by the genome called C, X, P, and S.
63

Gene S Encodes HBV Envelope Protein
64

HBV GenotypesThere are eight known genotypes labeled A through H. Different genotypes may respond to treatment in different ways. The genotypes differ by at least 8% of the sequence and have distinct geographical distributions and this has been associated with anthropological history.
❖ Type A is prevalent in Europe, Africa and South-east Asia, including the Philippines.
❖ Type B and C are predominant in Asia.
❖ Type D is common in the Mediterranean area, the Middle East and India.
❖ Type E is localized in sub-Saharan Africa.
❖ Type F (or H) is restricted to Central and South America.
❖ Type G has been found in France and Germany.
❖ Genotypes A, D and F are predominant in Brazil and all genotypes occur in the United States with frequencies dependent on ethnicity.
❖ The E and F strains appear to have originated in aboriginal populations of Africa and the New World, respectively.
❖ Within genotypes 24 subtypes have been described which differ by 4-8% of the genome.
65

Steps of HBV Replication
66
Dienstag, J.L. (2008). Hepatitis B virus infection. N Engl J Med 359, 1486-1500.

HBV: Replication
❖ Reverse transcription: one of the mRNAs is replicated with a reverse transcriptase making the DNA that will eventually be the core of the progeny virion.
❖ RNA intermediate: HBV replicates through an RNA intermediate and produces and release antigenic decoy particles.
❖ Integration: Some DNA integrates into host genome causing carrier state
67

❖ Parenteral - drug abusers, health workers are at increased risk.
❖ Sexual - sex workers and homosexuals are particular at risk.
❖ Perinatal (Vertical) - mother (HBeAg+) →infant.
HBV: Modes of Transmission

Current Treatments
❖ Interferon alfa (Intron A) (干扰素)Response rate is 30 to 40%
❖ Lamivudine (Epivir HBV)(拉⽶米呋啶)Relapse, drug resistance
❖ Adefovir dipivoxil (Hepsera)(阿德福⻙韦酯)
69

Hepatitis C Virus
Schematic view of hepatitis C virus
Single-stranded RNA
http://www.cdc.gov/
❖ First identified in 1989
❖ Scientifically classified as Flavivirus
❖ Contains ribonucleic acid (RNA)

Hepatitis C❖ An estimated 3% of the world’s population - more than 170
million people – are infected by the hepatitis C virus (HCV).
❖ Hundreds of thousands of people die each year from liver failure and cancer caused by this infection. Chronic HCV infection is the most common cause of liver transplantation.
❖ Current medical treatment options are limited. There are safe and effective vaccines to prevent hepatitis A and B; however, there is no vaccine for hepatitis C. The available antiviral drugs are toxic, expensive and only partly effective.
❖ Despite the discovery of the virus more than 15 years ago, our knowledge of the virus is limited.

HCV Genotypes
❖ Hepatitis C virus species is classified into six genotypes (1-6) with several subtypes within each genotype (represented by letters).
❖ Subtypes are further broken down into quasispecies based on their genetic diversity.
❖ In North America, genotype 1a predominates followed by 1b, 2a, 2b, and 3a.
❖ In Europe, genotype 1b is predominant followed by 2a, 2b, 2c, and 3a.
❖ Genotypes 4 and 5 are found almost exclusively in Africa.
❖ Genotype is clinically important in determining potential response to interferon-based therapy and the required duration of such therapy.
❖ Genotypes 1 and 4 are less responsive to interferon-based treatment than are the other genotypes (2, 3, 5 and 6).
72

HCV Genes and Gene Products
73

HCV Structure
74
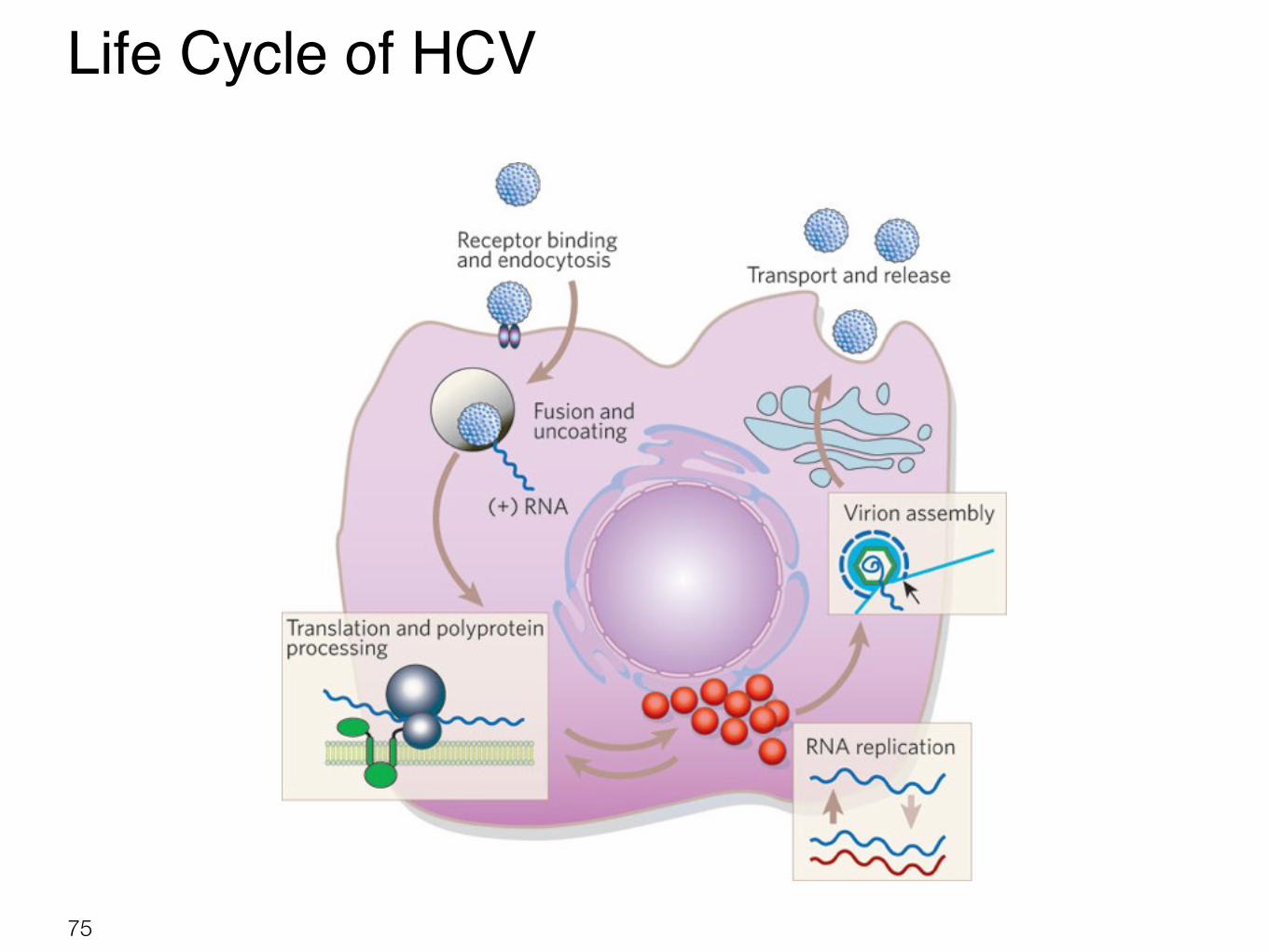
Life Cycle of HCV
75

HCV Life Cycle and Major Host Cell Defense Pathways.
76 Sklan, E.H., Charuworn, P., Pang, P.S., and Glenn, J.S. (2009). Mechanisms of HCV survival in the host. Nat Rev Gastroenterol Hepatol 6, 217-227.

Innate Immune Signaling Pathways Interdicted by HCV
77 Sklan, E.H., Charuworn, P., Pang, P.S., and Glenn, J.S. (2009). Mechanisms of HCV survival in the host. Nat Rev Gastroenterol Hepatol 6, 217-227.

HCV Factors Involved in Viral Evasion Strategies
78 Sklan, E.H., Charuworn, P., Pang, P.S., and Glenn, J.S. (2009). Mechanisms of HCV survival in the host. Nat Rev Gastroenterol Hepatol 6, 217-227.

HIV and HCV
❖ One out of every 4 people with HIV also has hep C. “Coinfection” with hep C and HIV is common because they share a similar route of transmission: exposure to infected blood. Unlike HIV, hep C is rarely transmitted during sexual activity. Thus, different people may be more or less likely to have both infections:
❖ Coinfection with HIV and hep C is common among people who became infected from injection drug use.
❖ HIV/hep C coinfection is also common among persons with hemophilia who received clotting factor concentrates (before 1987).
❖ For persons infected with HIV through sexual exposure, coinfection with hep C is no more common than it would be for anyone else.