대한소아마취학회 -...
TRANSCRIPT
소아마취의 최신 지견
1) Anesthesia for neonate and ex-premature infants ··················141
인제의대 방시라
2) 소아를 위한 심폐소생술 ···············································································145
서울의대 김진태
대한소아마취학회
제89차 종합학술대회
프로그램 및 초록
대한소아마취학회

제89차 종합학술 회 로그램 록 □ 세부 공학회발표 □
141
한
소
아
마
취
학
회
Anesthesia for neonate and ex-premature infants
인제 학교 의과 학 해운 백병원 마취통증의학과
방 시 라
산과학과 신생아학의 발 은 신생아 생존, 특히 preterm
neonate의 생존 증가에 많은 기여를 하 다. 많은 수의 생존
미숙아들은 생애 기에 크고 작은 수술이 필요한 경우가
많아 이에 마취과 의사들은 다양한 신생아 수술을 경험하
게 되어 신생아 생리와 미숙아들의 합병증 등에 한 이해
와 주의가 필요하게 되었다.
Neonatal physiology
Pulmonary
A. Transition phase and persistent pulmonary hypertension of
the neonate
At birth - 략 35 ml의 양수가 폐에서 배출되며 폐확장
이 이루어지며 호흡이 시작됨.
기에 폐는 매우 stiff (compliance very low):
first breath require negative forces > 70 cm H2O.
Pulmonary vascular resistance (PVR) 이 빠르게 감소하며
ductus arteriosus가 출생 후 1−15 hours 사이에 닫힘. PVR
정상화는 진 인 과정이며 3−4일 정도가 소요. ductus ar-
teriosus와 foramen ovale의 해부학 폐쇄는 몇 달이 소요.
출생 후 normal tidal ventilation은 10분 내에 normal FRC
는 20분 내에 도달하게 됨.
Persistent pulmonary hypertension of the neonate (PPHN):
hypoxia, hypercarbia, or acidosis can cause a sudden increase
in PVR and a return to a fetal circulatory pattern. PPHN is an
acute, life-threatening condition, as shunt fraction increases to
70% to 80%, and profound cyanosis results. Many factors dur-
ing anesthesia can affect this transitional state. Anesthetic agents
can markedly diminish systemic vascular resistance (SVR), re-
sulting in right-to-left shunt. Hypoxia or hypercarbia and acido-
sis from inadequate ventilation can increase PVR, with similar
effects on shunt.
Summary of Pulmonary differences with adults
1. Higher O2 Consumption
2. Higher closing volume
3. Higher MV:FRC
4. Compliant ribs and less Type 1 muscle in the diaphragm
B. Airway anatomy
Head: much larger compared with body size than that of
older children
Short neck, larger tongue
Higher and anterior larynx: cords located at C4 in the infant
compared with C5 or C6 in an adult.
Epiglottis: soft and folded
At the cricoids ring, 1 mm of edema results in a 60% re-
duction in the cross-sectional area of the airway, causing in-
creased airway resistance and increased work of breathing.
Laryngomalacia is also common in premature infants and can
result in obstruction.
Cardiovascular
Reduced ventricular compliance and less ability to increase
contractility → relatively dependent on heart rate to increase
cardiac output.
According to Barash, the neonatal heart is only capable of
increasing CO by about 30% (the adult, by contrast, can in-
crease CO by 300%).
Bradycardia: particularly dangerous in the neonate.
Hypoxemia, which can precipitate bradycardia, should be
vigorously avoided.
Diminished baroreceptor response to hypotension, and have
difficulty mounting a tachycardiac response.
Renal
Nephronogenesis: complete at 34 weeks’ gestation
Term neonate: as many nephrons as an adult, although they
are immature, with a glomerular filtration rate (GFR) approx-
imately 30% of the adult’s GFR.

제89차 종합학술 회 로그램 록
142
With increasing cardiac output and decreasing renal vascular
resistance, renal blood flow and GFR increase rapidly over the
first few weeks of life, and reach adult levels by about 1 year
of life. The diminished function over the first year is well bal-
anced to the infant’s needs because much of the neonate’s sol-
ute load is incorporated into body growth, and excretory load
is smaller.
Temperature regulation
Given a large surface area, small body volume, and minimal
insulation, neonates are extremely prone to heat loss. Any de-
gree of cold stress is detrimental and increases metabolic de-
mands in the neonate.
Preterm mortality
Intensive medical care should be initiated at 26 weeks of
gestation, aggressive resuscitation: not widely recommended for
infants born before 23 weeks gestation ‘grey zone’: gestational
age - play a role in influencing outcome.
Infants born at 22−25 weeks gestation
: in addition to gestational age, four factors as important in
the outcome of extreme prematurity.
Higher birth weight,
Female sex,
Use of antenatal steroids,
Singleton birth
Morbidity and mortality: remains high (one study estimating
a mortality rate of 89% for infants weighing 401−500 g)
Almost all the survivors in this extremely low birth weight
group suffered from considerable morbidity
Preterm morbidity
A. short-term morbidity
respiratory distress syndrome,
bronchopulmonary dysplasia,
persistent patent ductus arteriosus,
intraventricular hemorrhage,
periventricular leukomalacia,
retinopathy of prematurity,
necrotizing enterocolitis.
B. long-term morbidity
neurodevelopmental sequelae [cerebral palsy (CP), cognitive
delay, blindness, deafness,
chronic lung disease,
feeding difficulties,
subglottic stenosis following prolonged endotracheal intubation.
Brain development: particularly vulnerable during the second
and third trimesters.
Infants born at 22−26 weeks gestation :
high risk for hypoxic/ischemic brain injury
intraventricular hemorrhage,
→ frequently result in subsequent neurodevelopmental
sequelae.
Anesthetics and neurodevelopment
The current controversy can perhaps be summarized in sev-
eral points, as follows:
A. Exposure to anesthetic agents, at clinically appropriate
doses, at the peak of synaptogenesis can cause widespread
neuroapoptosis in several species of animals, including pri-
mates. A clinically appropriate dose is the minimum necessary
to induce anesthesia in the species. In some species, and with
some agents, this dose also results in significant mortality, in-
creasing the difficulty of interpreting the significance.
B. Synaptogenesis in rats occurs postnatally over the first 2
weeks of life. An analogous period in humans would range
from the third trimester of pregnancy through the first 3 years
of life. Whether the child might be susceptible to anesthetic
toxicity during this entire period is unknown. Other studies
looking specifically at neurodevelopment suggest that a post-
natal 7-day-old rat more closely corresponds to the human fetus
between 17 and 22 weeks of gestation. Elucidation of the crit-
ical period is of prime importance in anesthetic management.
C. The animal studies of apoptosis involve anesthesia with-
out surgery. There is some indication that the presence of sur-
gical stress may alter the response to anesthetics.
D. Abnormal behaviors and learning have also been shown
in animal studies after anesthetic exposure.

방시라:Anesthesia for neonate and ex-premature infants
143
한
소
아
마
취
학
회Fig. 1. Post-operative monitoring of the former preterm infant with a post-conceptual age (PCA) < 60 weeks. Acta Anaesthesiol Scand. 2006;
50(7): 888-93.
E. Initial extremely limited studies of children after anes-
thetic exposure as infants are suggestive, but difficult to
interpret. It is impossible to separate the effects of anesthesia
from the effects of surgery; the fact that in Wilder and col-
leagues study an effect was seen only with multiple anesthetics
might be related to dose, but could be related to other con-
founding effects, such as more severe illness.
F. The effects under examination are subtle, and difficult to
categorize and measure. The effects of fetal ethanol exposure
were first elucidated because of marked craniofacial abnormal-
ities, rather than more subtle developmental problems.
G. As has been proposed, the careful multicenter FDA ini-
tiative may be needed to determine the clinical impact of the
problem.
결론 으로 신생아 마취에 해 신경학 손상을 최소화
하기 한 방안을 고려해 보면,
A. The benefits versus the risk of delay in surgical proce-
dures, particularly if performed in premature infants, should be
carefully considered. Similar concerns could be raised in older
children if the procedure is elective.
B. It seems reasonable to perform a “simple” anesthetic.
There is virtually no extensive experience with many anesthetic
agents in neonates. This lack of extensive experience is not
unusual in neonates or pediatrics in general, but may be of in-
creased importance given the small therapeutic margin of most
anesthetics. There would seem to be little utility in the combi-
nation of agents, such as midazolam, propofol, and isoflurane,
when a single agent could be as easily used. Whether the use
of multiple agents could decrease the required dose of each,
and whether this would be beneficial is impossible to answer.
One preference is to use a predominant narcotic technique in
premature infants who may be most at risk, when appropriate.
Fentanyl has little, if any, activity as either an NMDA antago-
nist or GABA agonist. It is well tolerated hemodynamically,
and effective at preventing the surgical stress reaction. This
particular technique may prevent extubation, but in this gen-
erally ill population, this is not usually a consideration. The
possibility of recall with a pure narcotic technique can be
raised, but with a dose adequate to prevent the stress response,
this may not be important.
Summary of recommendations for the anesthetic
care of the expremature patient
ㆍDelay nonessential surgery until apnea risk is reduced:
Post-pone surgery until PCA _ 60 weeks
ㆍWhen surgery cannot be delayed, plan for overnight admis-
sion and monitoring (at least 18 hours (?) in those still at
risk for apnea.
ㆍOptimize medical conditions, including reactive airway dis-
ease and gastroesophageal reflux, prior to surgery.
ㆍRecognize limitations of all expremies, even those that are
not obvious (pulmonary function, developmental): Assessment
of comorbidity or anaemia.
ㆍConsult with the patient’s physicians regarding ongoing med-
ical problems.

제89차 종합학술 회 로그램 록
144
ㆍChoose appropriate anaesthesia technique
ㆍPlan for intraoperative bronchospasm.
ㆍConsider postoperative intensive care unit admission prior to
surgery to ensure availability, should it become necessary.
ㆍDecide level of post-operative monitoring (see Fig. 1)
References
1. Martin RJ, Fanaroff AA, Michele C. WalshFanaroff and Martin’s
Neonatal-Perinatal Medicine: Diseases of the Fetus and Infant, 9th
ed. pp 597-614.
2. Laura S. Seminars in Anesthesia, Perioperative Medicine and Pain
(2006) 25, 117-123.
3. Walther-Larsen S, Rasmussen LS. The former preterm infant and
risk of post-operative apnoea: recommendations for management.
Acta Anaesthesiol Scand. 2006; 50(7): 888-93.
4. Davis P, Cladis F, Motoyama E. Smith’s Anesthesia for infancts
and children, 8th ed. 512-588.
5. Wilder RT, et al: Early exposure to anesthesia and learning
disabilities in a population-based birth cohort, Anesthesiology 110:
796, 2009.
제89차 종합학술 회 로그램 록 □ 세부 공학회발표 □
145
한
소
아
마
취
학
회
소아를 위한 심폐소생술
서울 학교 의과 학 마취통증의학교실
김 진 태
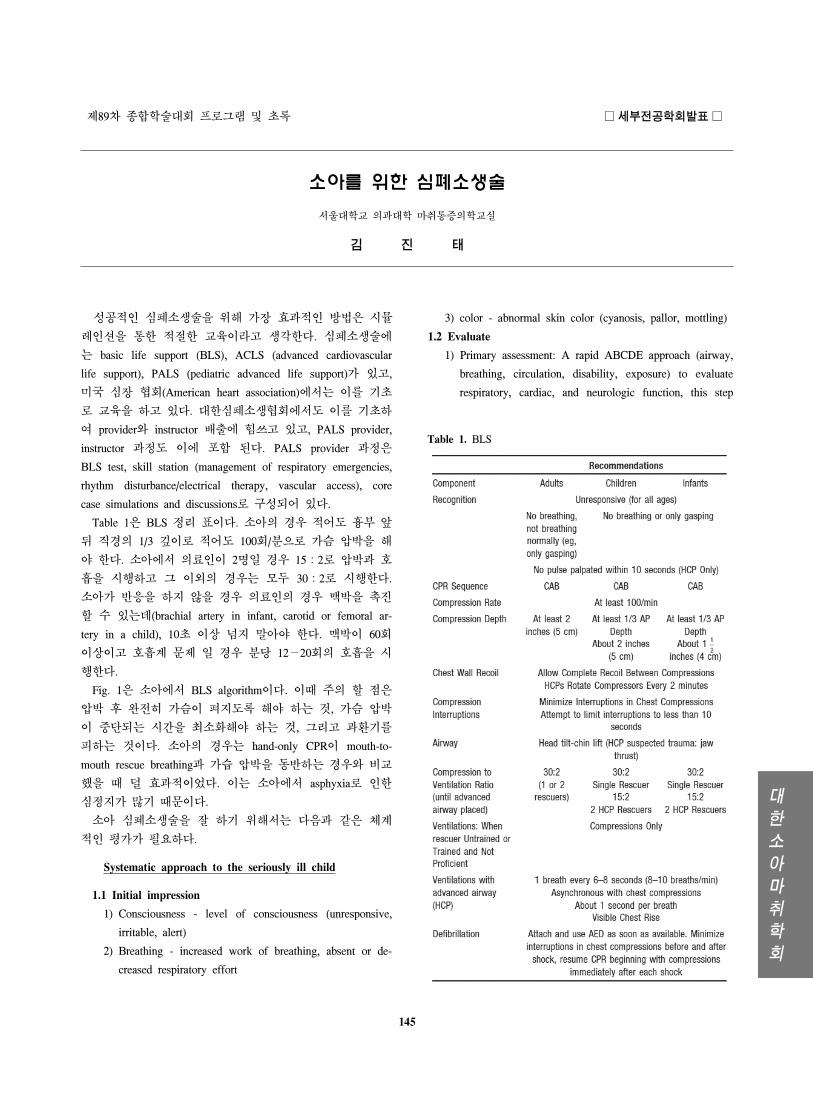
Table 1. BLS
성공 인 심폐소생술을 해 가장 효과 인 방법은 시뮬
인션을 통한 한 교육이라고 생각한다. 심폐소생술에
는 basic life support (BLS), ACLS (advanced cardiovascular
life support), PALS (pediatric advanced life support)가 있고,
미국 심장 회(American heart association)에서는 이를 기
로 교육을 하고 있다. 한심폐소생 회에서도 이를 기 하
여 provider와 instructor 배출에 힘쓰고 있고, PALS provider,
instructor 과정도 이에 포함 된다. PALS provider 과정은
BLS test, skill station (management of respiratory emergencies,
rhythm disturbance/electrical therapy, vascular access), core
case simulations and discussions로 구성되어 있다.
Table 1은 BLS 정리 표이다. 소아의 경우 어도 흉부 앞
뒤 직경의 1/3 깊이로 어도 100회/분으로 가슴 압박을 해
야 한다. 소아에서 의료인이 2명일 경우 15:2로 압박과 호
흡을 시행하고 그 이외의 경우는 모두 30:2로 시행한다.
소아가 반응을 하지 않을 경우 의료인의 경우 맥박을 진
할 수 있는데(brachial artery in infant, carotid or femoral ar-
tery in a child), 10 이상 넘지 말아야 한다. 맥박이 60회
이상이고 호흡계 문제 일 경우 분당 12−20회의 호흡을 시
행한다.
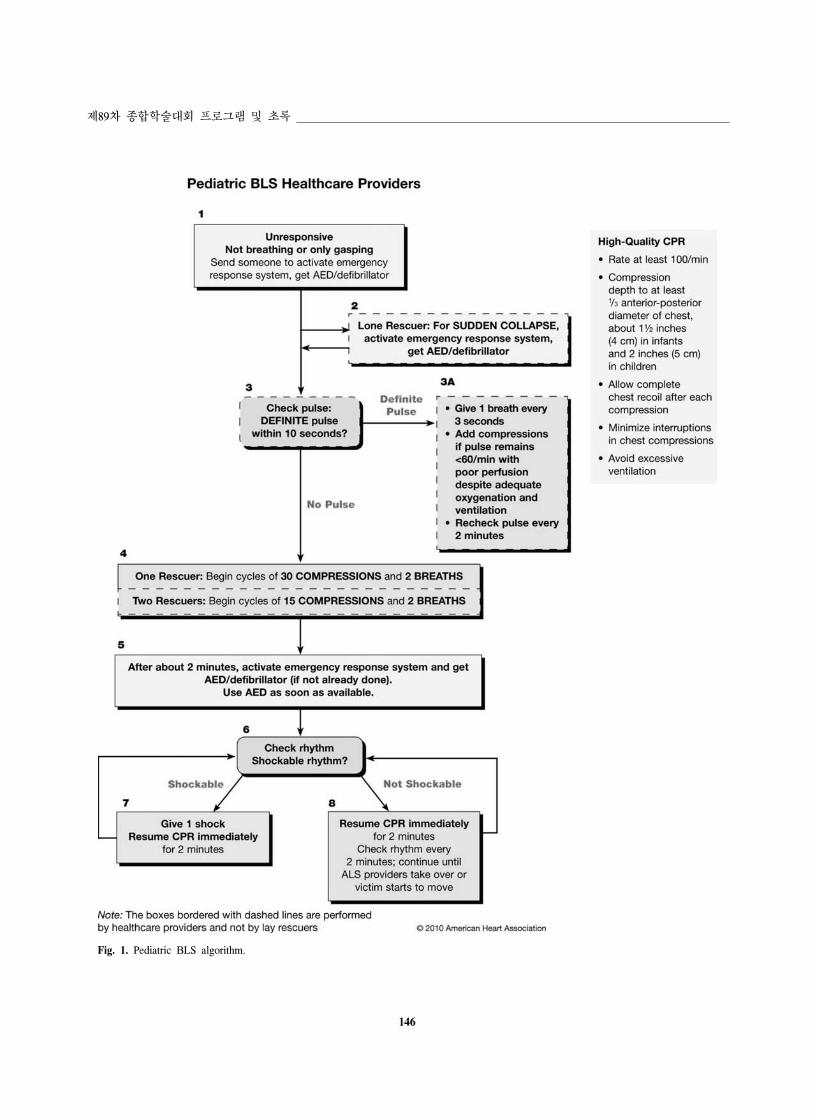
Fig. 1은 소아에서 BLS algorithm이다. 이때 주의 할 은
압박 후 완 히 가슴이 펴지도록 해야 하는 것, 가슴 압박
이 단되는 시간을 최소화해야 하는 것, 그리고 과환기를
피하는 것이다. 소아의 경우는 hand-only CPR이 mouth-to-
mouth rescue breathing과 가습 압박을 동반하는 경우와 비교
했을 때 덜 효과 이었다. 이는 소아에서 asphyxia로 인한
심정지가 많기 때문이다.
소아 심폐소생술을 잘 하기 해서는 다음과 같은 체계
인 평가가 필요하다.
Systematic approach to the seriously ill child
1.1 Initial impression
1) Consciousness - level of consciousness (unresponsive,
irritable, alert)
2) Breathing - increased work of breathing, absent or de-
creased respiratory effort
3) color - abnormal skin color (cyanosis, pallor, mottling)
1.2 Evaluate
1) Primary assessment: A rapid ABCDE approach (airway,
breathing, circulation, disability, exposure) to evaluate
respiratory, cardiac, and neurologic function, this step
146
제89차 종합학술 회 로그램 록
Fig. 1. Pediatric BLS algorithm.
김진태:소아를 한 심폐소생술
147
한
소
아
마
취
학
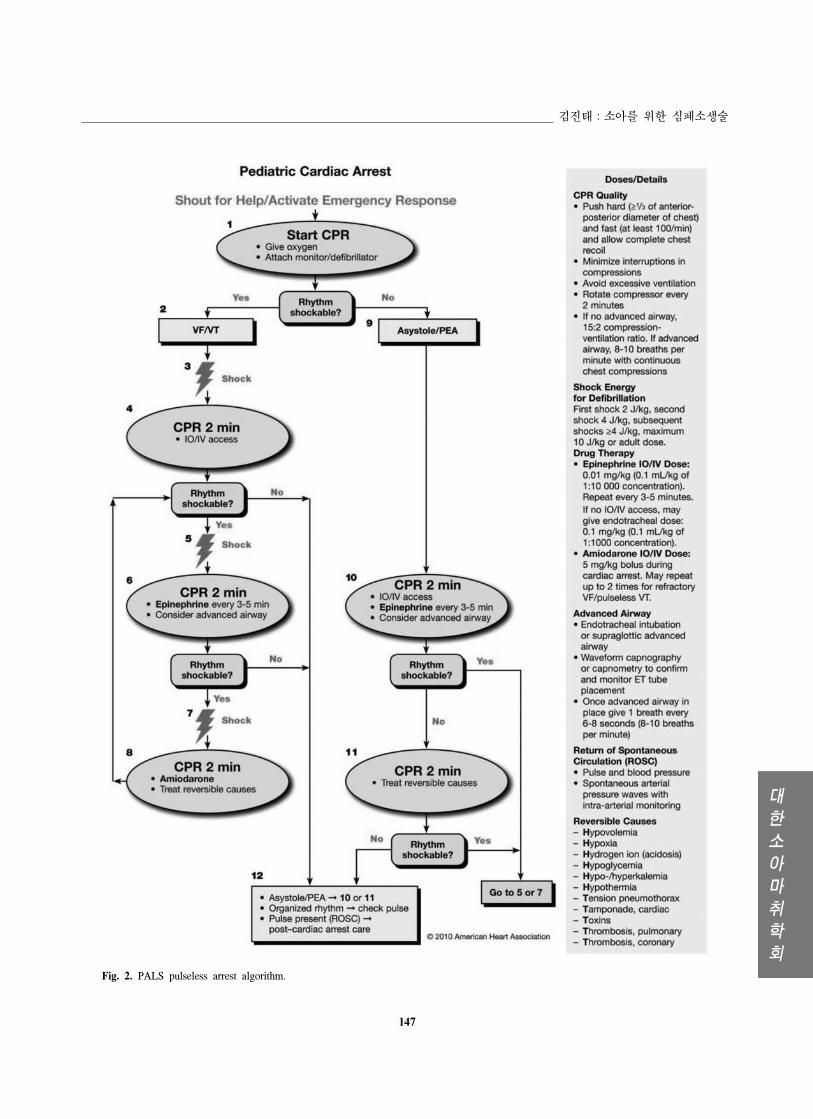
회Fig. 2. PALS pulseless arrest algorithm.
148
제89차 종합학술 회 로그램 록
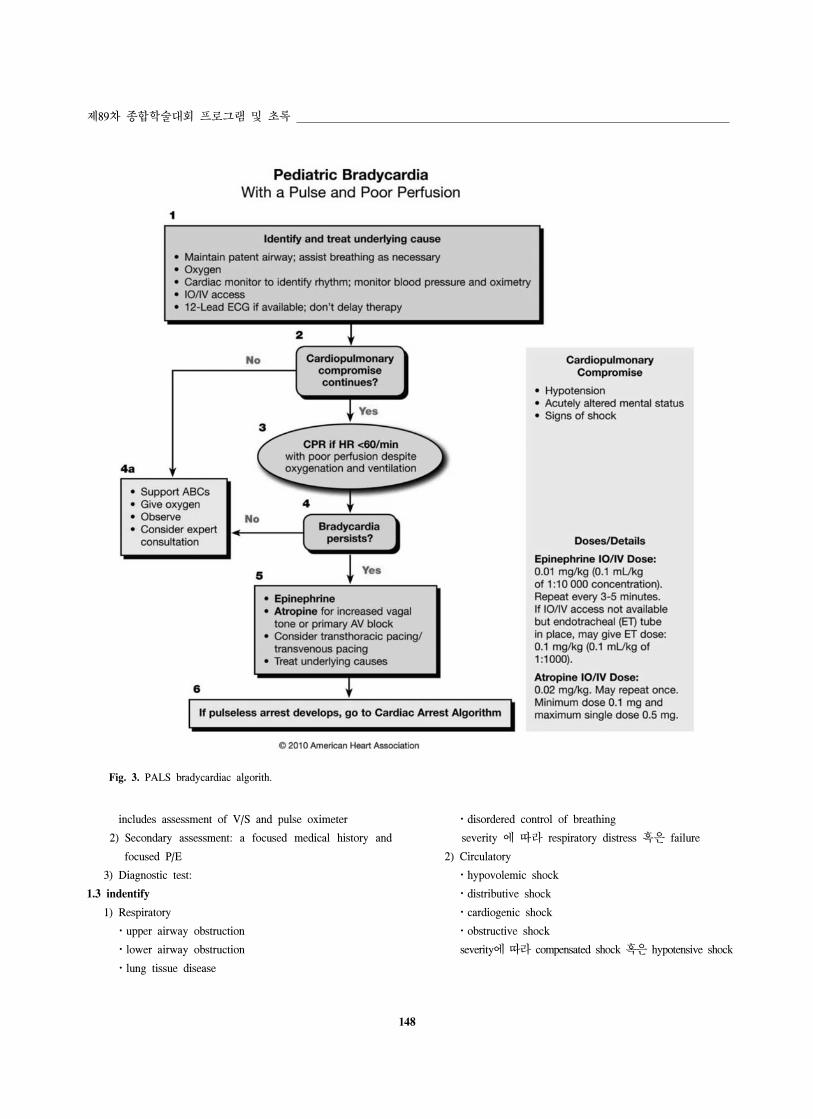
Fig. 3. PALS bradycardiac algorith.
includes assessment of V/S and pulse oximeter
2) Secondary assessment: a focused medical history and
focused P/E
3) Diagnostic test:
1.3 indentify
1) Respiratory
ㆍupper airway obstruction
ㆍlower airway obstruction
ㆍlung tissue disease
ㆍdisordered control of breathing
severity 에 따라 respiratory distress 혹은 failure
2) Circulatory
ㆍhypovolemic shock
ㆍdistributive shock
ㆍcardiogenic shock
ㆍobstructive shock
severity에 따라 compensated shock 혹은 hypotensive shock
김진태:소아를 한 심폐소생술
149
한
소
아
마
취
학
회
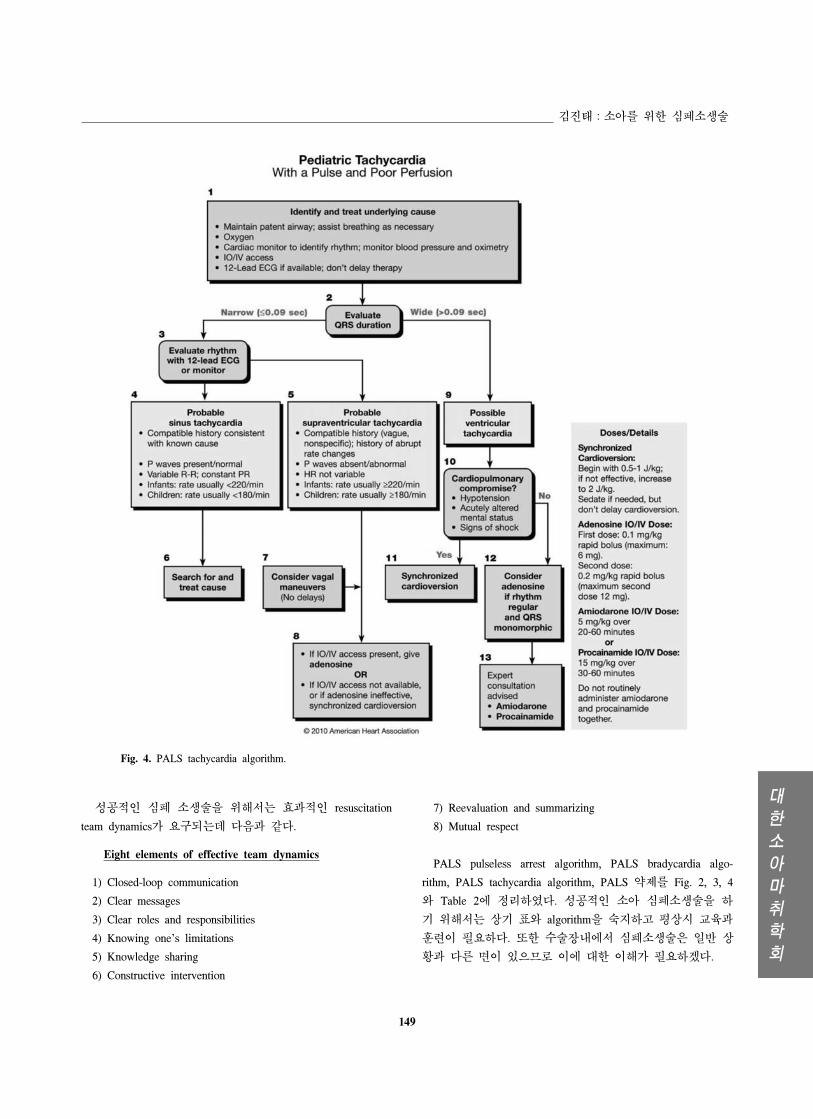
Fig. 4. PALS tachycardia algorithm.
성공 인 심폐 소생술을 해서는 효과 인 resuscitation
team dynamics가 요구되는데 다음과 같다.
Eight elements of effective team dynamics
1) Closed-loop communication
2) Clear messages
3) Clear roles and responsibilities
4) Knowing one’s limitations
5) Knowledge sharing
6) Constructive intervention
7) Reevaluation and summarizing
8) Mutual respect
PALS pulseless arrest algorithm, PALS bradycardia algo-
rithm, PALS tachycardia algorithm, PALS 약제를 Fig. 2, 3, 4
와 Table 2에 정리하 다. 성공 인 소아 심폐소생술을 하
기 해서는 상기 표와 algorithm을 숙지하고 평상시 교육과
훈련이 필요하다. 한 수술장내에서 심폐소생술은 일반 상
황과 다른 면이 있으므로 이에 한 이해가 필요하겠다.

150
제89차 종합학술 회 로그램 록
Table 2. 소아 심폐소생술 시 약제
참 고 문 헌
1. Berg MD, Schexnayder SM, Chameides L, Terry M, Donoghue
A, Hickey RW, Berg RA, Sutton RM, Hazinski MF. Part 13:
pediatric basic life support: 2010 American Heart Association
Guidelines for Cardiopulmonary Resuscitation and Emergency
Cardiovascular Care. Circulation 2010; 122(18 Suppl 3): S862-75.
2. Kleinman ME, Chameides L, Schexnayder SM, Samson RA,
Hazinski MF, Atkins DL, Berg MD, de Caen AR, Fink EL, Freid
EB, Hickey RW, Marino BS, Nadkarni VM, Proctor LT, Qureshi
FA, Sartorelli K, Topjian A, van der Jagt EW, Zaritsky AL. Part
14: pediatric advanced life support: 2010 American Heart
Association Guidelines for Cardiopulmonary Resuscitation and
Emergency Cardiovascular Care. Circulation 2010; 122(18 Suppl
3): S876-908.