· web viewmr. fischer is a 55-year-old patient with small cell lung cancer (sclc). he was...
TRANSCRIPT
Enhancing Registered Nurse Job Readiness and Patient Safety Outcomes Through Clinical Simulation
Simulation Scenario Template
Adaptation of California Simulation Alliance (CSA)
Feb 23, 2014Revised April 2014
University of OttawaAlgonquin College
CSA REV template (12/15/08; 5/09; 12/09; 4/11; 1/14)Revised COUPN January 2014
TABLE OF CONTENTSii
SECTION I SCENARIO OVERVIEW
A. TitleB. SummaryC. Evidence Base
SECTION II CURRICULUM INTEGRATION
A. Learning Objectives1. Primary2. Secondary3. Critical Elements
B. Pre-scenario learner activities
SECTION III SCENARIO SCRIPT
A. Case SummaryB. Key Contextual DetailsC. Scenario CastD. Patient/Client ProfileE. Baseline patient/client simulator stateF. Environment / equipment / essential propsG. Case flow /triggers / scenario development
SECTION IV APPENDICES
A.B.C.
Health Care Provider OrdersB. Digital Images of Manikin / Milieu
Debriefing Guide
CSA REV template (12/15/08; 5/09; 12/09; 4/11; 1/14)Revised COUPN January 2014

1
SECTION I: SCENARIO OVERVIEW
Scenario Title: Mark Fisher (Part A) – End of life careOriginal Scenario Developer(s): Diane Alain, Valerie Fiset, Frances Bourbonnais-Forthergill and Susan
Brajtman, University of OttawaDate - original scenario February, 2014Validation: Revision Dates: Draft for peer review, week of Feb 24thPilot testing:QSEN revision:
Estimated Scenario Time: 20 min Debriefing time: 30-40 min
Target group: 4th year BScN students
Core case: Palliative Care/End of Life care CNA
Position Statement: Providing Nursing Care at the End of Life (2008)
CNO Practice Guideline “Authorizing Mechanisms (updated 2014)” (2014) re: delegation. Practice Guideline “Consent” (2009) Practice Guideline “Guiding decisions in End of Life care” (2009) Practice Standard “Documentation” (2008) Practice Standard “Medication” (2014)
RNAO: Best Practice Guidelines End of Life Care During the Last Days and Hours (2011)
CHPCA A Model to Guide Hospice Palliative Care: Based on National Principles and Norms of Practice.
Revised and Condensed (2013).
CASN Palliative and End-of-Life Care: Entry-to-Practice Competencies and Indicators for Registered Nurses
(2011)
Standardized Tools Edmonton Symptom Assessment System (ESAS). Cancer Care Ontario. Palliative Performance Scale (2005) Cancer Care Ontario. Frommelt Attitude Toward Care of the Dying Scale (Frommelt, K. (1991). The effects of death
education on nurses' attitudes toward caring for terminally ill persons and their families. American Journal Of Hospice & Palliative Medicine, 8(5), 37. As cited in RNAO BPG (2011))
CSA REV template (12/15/08; 5/09; 12/09; 4/11; 1/14) SECTION I
ALL DATA IN THIS SCENARIO IS FICTICIOUS

2
Brief Summary of Case:
This is the part A of a two part unfolding scenario that can be used as a single, stand-alone scenario.
Part A: Mr. Fischer is a 55-year-old patient with small cell lung cancer (SCLC). He was diagnosed 15 months ago. He received chemotherapy (Cisplatin and Etoposide) and some thoracic radiation therapy. In the last two weeks the disease has recurred, the patient has lost weight and is experiencing general weakness, dyspnea, chronic cough and hemoptysis. His pain is not well controlled at this stage. The prognosis is poor, his current Palliative Performance Scale (PPS) is 50% (Cancer Care Ontario, 2005; Wilner & Arnold, 2006) and the doctor is transferring the patient from oncology to the palliative service. He wants to die at home; a plan for this has been established and is will be enacted by the palliative discharge team. In this scenario the patient is prepared to switch their resuscitation status to “Do Not Resuscitate (DNR)”, and declaring his spouse power of attorney and substitute decision maker. He is anxious about having a conversation about this change with his spouse.
He has been married for 30 years and has 2 children and 3 grand-children that live out of town.
Spouse is present in hospital, but not currently with patient.
Part B: 55 year old male client is imminently dying of lung cancer with a PPS of 10%. He is married and spouse is at the bedside in the home. Client has 2 adult children and 3 grand-children who live out of town. One of which arrives at the home just after her/his father passes away. Nurses must provide comfort measures to the dying client and support the spouse during final breaths of life, in addition to breaking bad news to the child who arrives too late to say goodbye.
EVIDENCE BASE / REFERENCES (APA Format)Canadian Association of Schools of Nursing (CASN) (2012). Palliative and end-of-life care: A faculty guide for nursing education. Ottawa: CASN.Canadian Association of Schools of Nursing (CASN) (2011) Palliative and end-of-life care entry-to-practice competencies and indicators for registered nurses. Ottawa: CASNCanadian Interprofessional Health Collaborative (2010). A national interprofessional competency framework. Retrieved Feb. 3, 2014 from http://www.cihc.ca/files/CIHC_IPCompetencies_Feb1210.pdfCanadian Nurses Association (2008). Position Statement. Providing nursing care at the end of life. Retrieved Feb 3, 2014, from https://www.cna-aiic.ca/~/media/cna/page%20content/pdf%20en/2013/07/26/10/43/ps96_end_of_life_e.pdf A classic in field.Canadian Patient Safety Institute (2008). The safety competencies. Retrieved Feb. 3, 2014 from http://www.patientsafetyinstitute.ca/English/toolsResources/safetyCompetencies/Documents/Safety%20Competencies.pdf A classic in the Field.Cancer Care Ontario (2005). Edmonton Symptom Assessment System. Retrieved Feb 23, 2014 from https://www.cancercare.on.ca/common/pages/UserFile.aspx?fileId=13262 A classic in the Field.Cancer Care Ontario (2005). Palliative Performance Scale. Developed by the Victoria Hospice. Retrieved Feb 18, 2014 from https://www.cancercare.on.ca/toolbox/pallcaretools/ -A ClassicCollege of Nurses of Ontario (2009). Practice guideline. Guiding decisions about end-of-life care, 2009. Toronto: College of Nurses of Ontario. A classic in the Field.College of Nurses of Ontario (2008). National competencies: in the context of entry-level Registered Nurse practice. Toronto: College of Nurses of Ontario. Retrieved Feb. 3, 2014 from
CSA REV template (12/15/08; 5/09; 12/09; 4/11; 1/14) SECTION I
ALL DATA IN THIS SCENARIO IS FICTICIOUS
3
http://www.cno.org/Global/docs/reg/41037_EntryToPracitic_final.pdfFrommelt, K. (1991). The effects of death education on nurses' attitudes toward caring for terminally ill persons and their families. American Journal of Hospice & Palliative Medicine, 8(5), 37. doi:10.1177/104990919100800509 A classic in the Field.Kissane, D., Clarke, D., & Street, A. (2001). Demoralization syndrome -- a relevant psychiatric diagnosis for palliative care. Journal Of Palliative Care, 17(1), 12-21. A classic in the Field.Jones, J. (2007). Do not resuscitate: reflections on an ethical dilemma. Nursing Standard, 21(46), 35-39. A classic in the Field.Murray, M.A., Miller, T., Fiset, V., O’Connor, A., & Jacobsen, M.J. (2004). Decision support: Helping patients and families to find balance at the end of life. International Journal of Palliative Nursing, 10(6): 270-277. A classic in the Field.Wilner, L., & Arnold, R. M. (2006). The Palliative Performance Scale #125. Journal Of Palliative Medicine, 9(4), 994. doi:10.1089/jpm.2006.9.994 A classic in the Field.
CSA REV template (12/15/08; 5/09; 12/09; 4/11; 1/14) SECTION I
ALL DATA IN THIS SCENARIO IS FICTICIOUS

4SECTION II: CURRICULUM INTEGRATION
A. SCENARIO LEARNING OBJECTIVESDo What With What For What
Uses requisite relational skills to support decision-making and negotiate modes of palliative and end-of-life care on an ongoing basis.
Demonstrates knowledge of grief and bereavement
to support others from a cross-cultural perspective.
Demonstrates Knowledge and skill in holistic, family-centred nursing care
of persons at end-of-life who are experiencing pain and other symptoms.
Identifies the full range and continuum of palliative and end-of-life care services, resources and the settings in which they are available.
Competency
CASN Competencies
Demonstrated Attributes Align With Competency
CASNIndicators of competencies
Demonstrated Attributes Need Some
Improvement To Align
Demonstrated Attributes Need Major
Improvement To Align
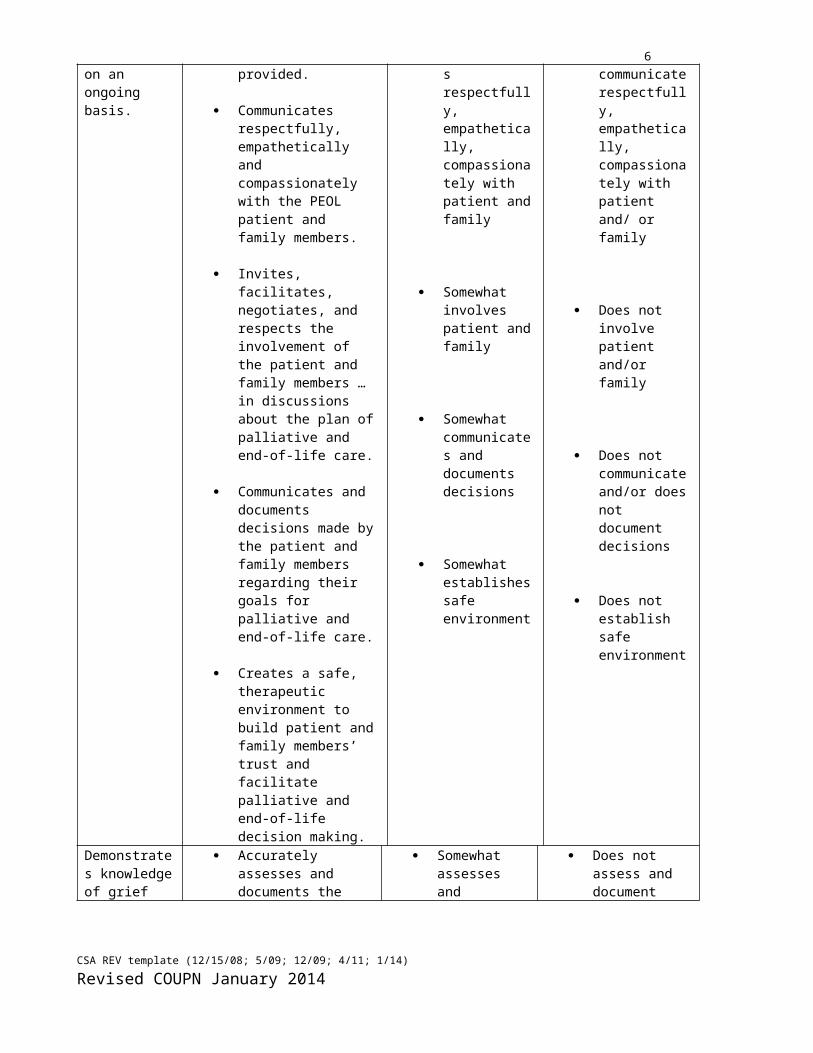
Uses requisite relational skills to support decision-making and negotiate modes of palliative and end-of-life care on an ongoing basis.
Provides information and assurance to the patient and family members regarding comfort measures during the last hours/minutes of living, and documents the information provided.
Communicates respectfully, empathetically and compassionately with the PEOL patient and family members.
Invites, facilitates, negotiates, and respects the involvement of the patient and family members … in discussions about the plan of palliative and end-of-life care.
Somewhat provides information and assurance
Somewhat communicates respectfully, empathetically, compassionately with patient and family
Somewhat involves patient and family
Does not/ avoids providing information and assurance
Does not communicate respectfully, empathetically, compassionately with patient and/ or family
Does not involve patient and/or family
CSA REV template (12/15/08; 5/09; 12/09; 4/11; 1/14)Revised COUPN January 2014
5 Communicates and
documents decisions made by the patient and family members regarding their goals for palliative and end-of-life care.
Creates a safe, therapeutic environment to build patient and family members’ trust and facilitate palliative and end-of-life decision making.
Somewhat communicates and documents decisions
Somewhat establishes safe environment
Does not communicate and/or does not document decisions
Does not establish safe environment
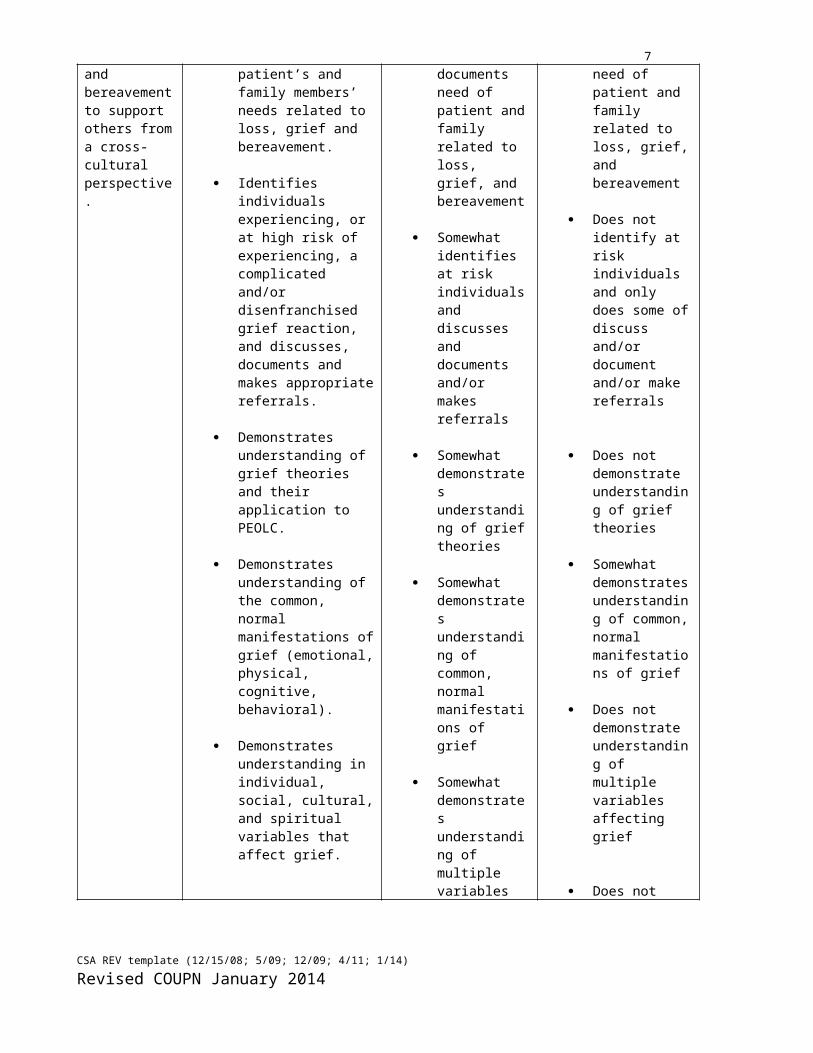
Demonstrates knowledge of grief and bereavement to support others from a cross-cultural perspective.
Accurately assesses and documents the patient’s and family members’ needs related to loss, grief and bereavement.
Identifies individuals experiencing, or at high risk of experiencing, a complicated and/or disenfranchised grief reaction, and discusses, documents and makes appropriate referrals.
Demonstrates understanding of grief theories and their application to PEOLC.
Demonstrates understanding of the common, normal manifestations of grief (emotional, physical, cognitive, behavioral).
Demonstrates understanding in individual, social, cultural, and spiritual variables that affect grief.
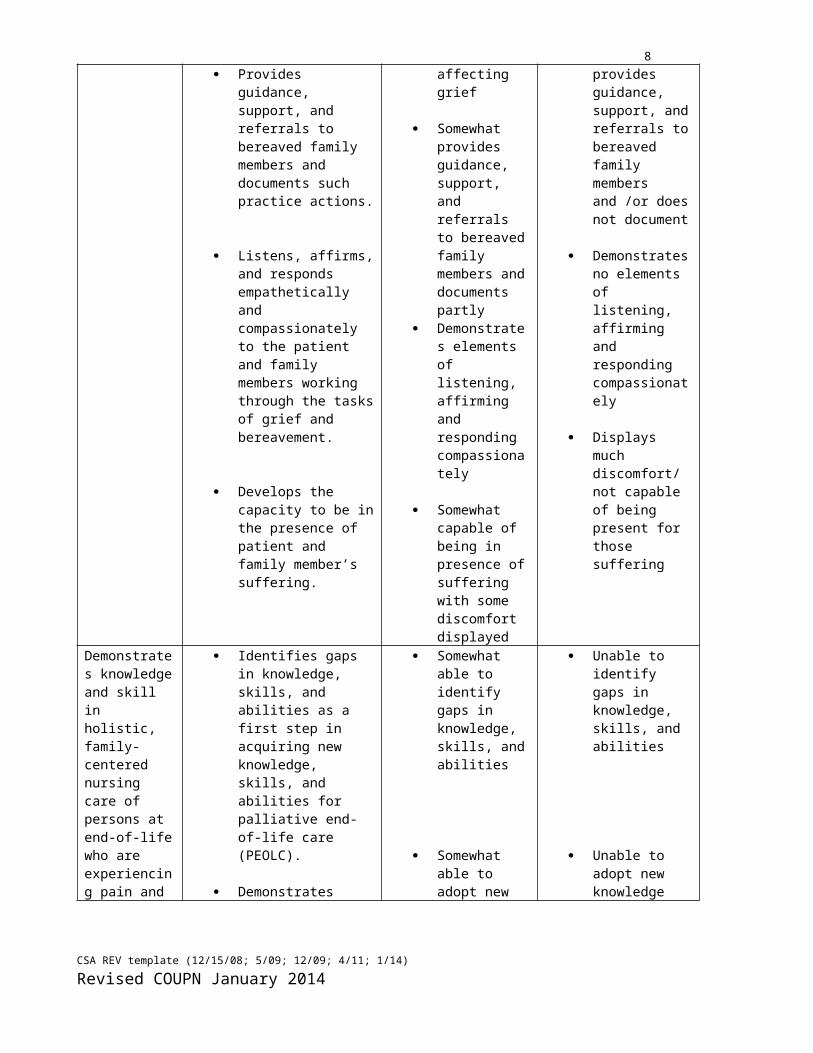
Provides guidance, support, and referrals to bereaved family members and
Somewhat assesses and documents need of patient and family related to loss, grief, and bereavement
Somewhat identifies at risk individuals and discusses and documents and/or makes referrals
Somewhat demonstrates understanding of grief theories
Somewhat demonstrates understanding of common, normal manifestations of grief
Somewhat demonstrates understanding of multiple variables affecting grief
Somewhat provides guidance, support, and
Does not assess and document need of patient and family related to loss, grief, and bereavement
Does not identify at risk individuals and only does some of discuss and/or document and/or make referrals
Does not demonstrate understanding of grief theories
Somewhat demonstrates understanding of common, normal manifestations of grief
Does not demonstrate understanding of multiple variables affecting grief
Does not provides guidance, support, and referrals to
CSA REV template (12/15/08; 5/09; 12/09; 4/11; 1/14)Revised COUPN January 2014

6documents such practice actions.
Listens, affirms, and responds empathetically and compassionately to the patient and family members working through the tasks of grief and bereavement.
Develops the capacity to be in the presence of patient and family member’s suffering.
referrals to bereaved family members and documents partly
Demonstrates elements of listening, affirming and responding compassionately
Somewhat capable of being in presence of suffering with some discomfort displayed
bereaved family members and /or does not document
Demonstrates no elements of listening, affirming and responding compassionately
Displays much discomfort/ not capable of being present for those suffering
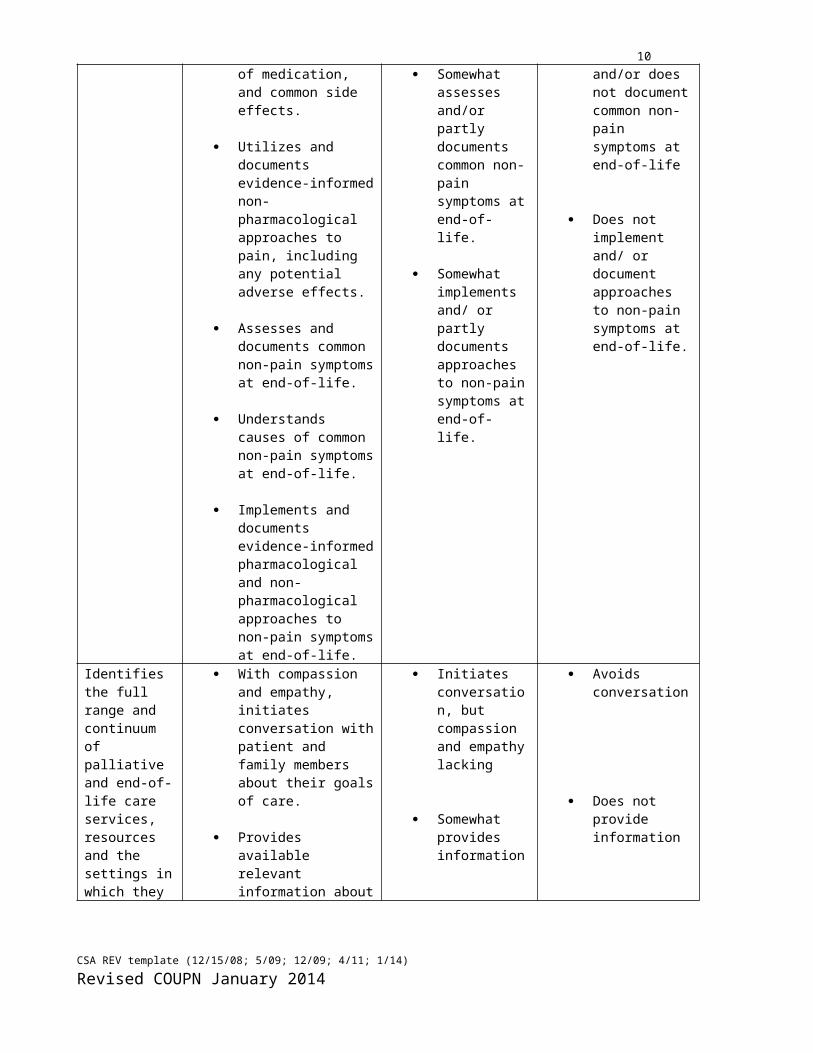
Demonstrates knowledge and skill in holistic, family-centered nursing care of persons at end-of-life who are experiencing pain and other symptoms.
Identifies gaps in knowledge, skills, and abilities as a first step in acquiring new knowledge, skills, and abilities for palliative end-of-life care (PEOLC).
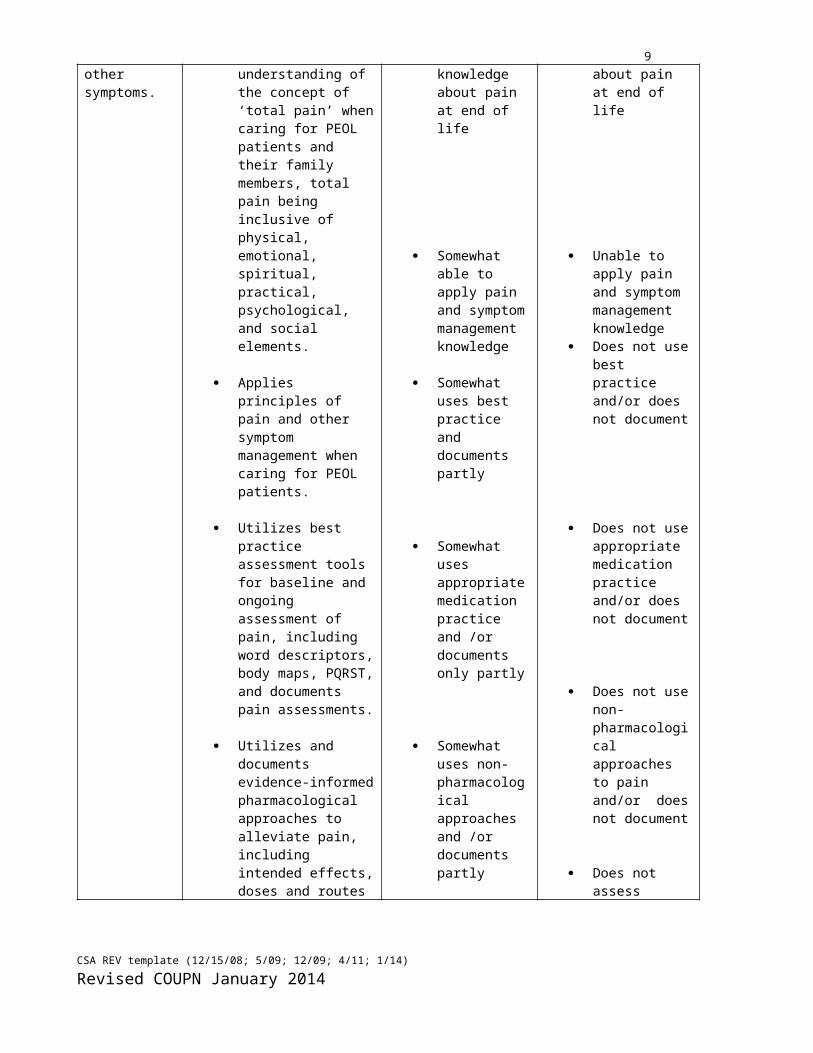
Demonstrates understanding of the concept of ‘total pain’ when caring for PEOL patients and their family members, total pain being inclusive of physical, emotional, spiritual, practical, psychological, and social elements.
Applies principles of pain and other symptom management when caring for PEOL patients.
Utilizes best practice assessment tools for baseline and ongoing assessment of pain, including word descriptors, body maps, PQRST, and documents pain assessments.
Utilizes and documents
Somewhat able to identify gaps in knowledge, skills, and abilities
Somewhat able to adopt new knowledge about pain at end of life
Somewhat able to apply pain and symptom management knowledge
Somewhat uses best practice and documents partly
Somewhat uses appropriate
Unable to identify gaps in knowledge, skills, and abilities
Unable to adopt new knowledge about pain at end of life
Unable to apply pain and symptom management knowledge
Does not use best practice and/or does not document
Does not use
CSA REV template (12/15/08; 5/09; 12/09; 4/11; 1/14)Revised COUPN January 2014
7evidence-informed pharmacological approaches to alleviate pain, including intended effects, doses and routes of medication, and common side effects.
Utilizes and documents evidence-informed non-pharmacological approaches to pain, including any potential adverse effects.
Assesses and documents common non-pain symptoms at end-of-life.
Understands causes of common non-pain symptoms at end-of-life.
Implements and documents evidence-informed pharmacological and non-pharmacological approaches to non-pain symptoms at end-of-life.
medication practice and /or documents only partly
Somewhat uses non-pharmacological approaches and /or documents partly
Somewhat assesses and/or partly documents common non-pain symptoms at end-of-life.
Somewhat implements and/ or partly documents approaches to non-pain symptoms at end-of-life.
appropriate medication practice and/or does not document
Does not use non-pharmacological approaches to pain and/or does not document
Does not assess and/or does not document common non-pain symptoms at end-of-life
Does not implement and/ or document approaches to non-pain symptoms at end-of-life.
Identifies the full range and continuum of palliative and end-of-life care services, resources and the settings in which they are available.
With compassion and empathy, initiates conversation with patient and family members about their goals of care.
Provides available relevant information about resources to the PEOL patient and family members.
Initiates conversation, but compassion and empathy lacking
Somewhat provides information
Avoids conversation
Does not provide information
CSA REV template (12/15/08; 5/09; 12/09; 4/11; 1/14)Revised COUPN January 2014
8
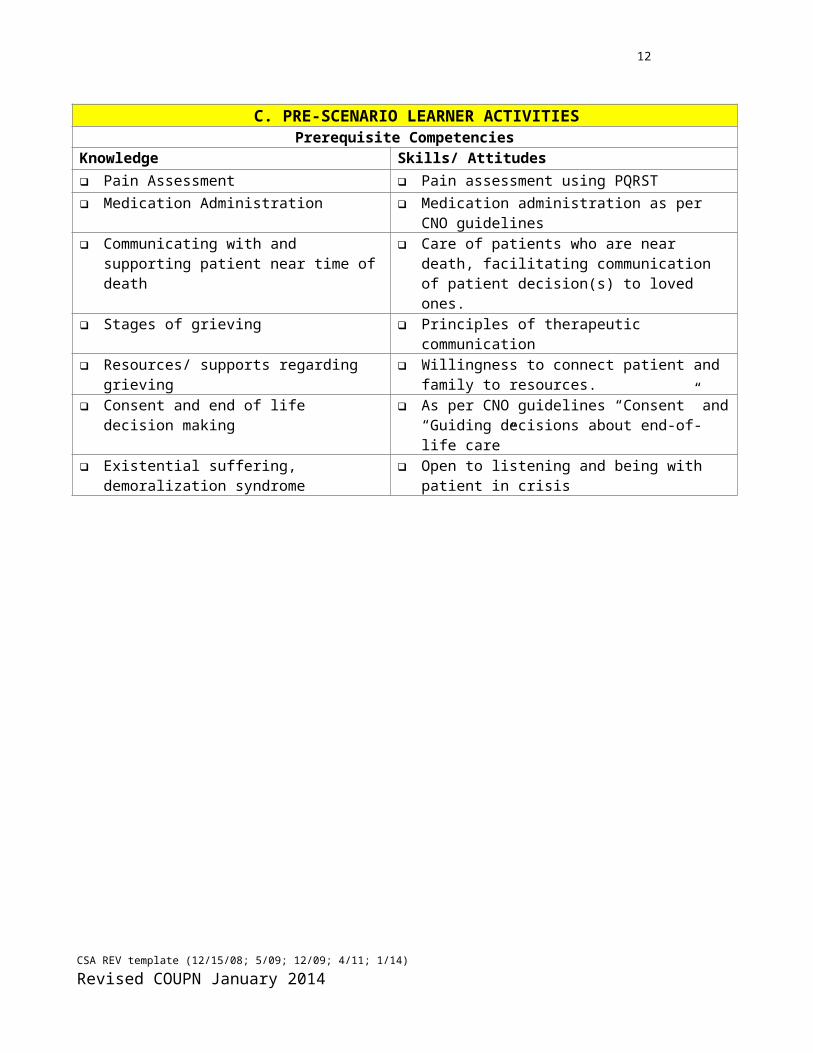
C. PRE-SCENARIO LEARNER ACTIVITIES Prerequisite Competencies
Knowledge Skills/ Attitudes Pain Assessment Pain assessment using PQRST Medication Administration Medication administration as per CNO guidelines Communicating with and supporting patient
near time of death Care of patients who are near death, facilitating
communication of patient decision(s) to loved ones. Stages of grieving Principles of therapeutic communication Resources/ supports regarding grieving Willingness to connect patient and family to
resources. Consent and end of life decision making As per CNO guidelines “Consent” and “Guiding
decisions about end-of-life care” Existential suffering, demoralization syndrome Open to listening and being with patient in crisis
CSA REV template (12/15/08; 5/09; 12/09; 4/11; 1/14)Revised COUPN January 2014
9SECTION III: SCENARIO SCRIPT
A. Case summaryPart A: Mr. Fischer is a 55-year-old patient with small cell lung cancer (SCLC). He was diagnosed 15 months ago. He received chemotherapy (Cisplatin and Etoposide) and some thoracic radiation therapy. In the last two weeks the disease has recurred, the patient has lost weight and is experiencing general weakness, dyspnea, chronic cough and hemoptysis. He was been readmitted to the oncology unit via ER yesterday. His pain was not well controlled overnight.
The prognosis is poor, his current Palliative Performance Scale (PPS) is 50% (Cancer Care Ontario, 2005; Wilner & Arnold, 2006) and the doctor is transferring Mr. Fischer from oncology to the palliative service. He wants to die at home; a plan for this possiblility has been established by Mr. Fischer, his wife and the oncology team in consultation with palliative services while Mr. Fischer was an outpatient. It will be enacted by the palliative discharge team. In this scenario, the patient is prepared to switch their resuscitation status to “Do Not Resuscitate (DNR)”, and declaring his spouse power of attorney and substitute decision maker. He is anxious about having a conversation about this change with his spouse.
B. Key contextual details
55 year old married man and father. The patient has lost weight and is experiencing general weakness, pain, dyspnea, chronic cough,
hemoptysis over the last 2 weeks. Came into the hospital through emergency yesterday, admitted under oncology and is being
transferred to palliative service with a plan to go home under community palliative care. Plan of treatment:
o In process to transfer patient from oncology service to palliative care service and from hospital inpatient palliative service to home/community palliative care.
This plan has been established and will be enacted by the palliative discharge team. The nursing student(s) do/does not need to undertake discharge planning responsibilities in this
scenario. Rather, they need to be able to re-assure Mr. Fischer that there is a plan and his and his family’s needs will be met by the new team taking over his care.
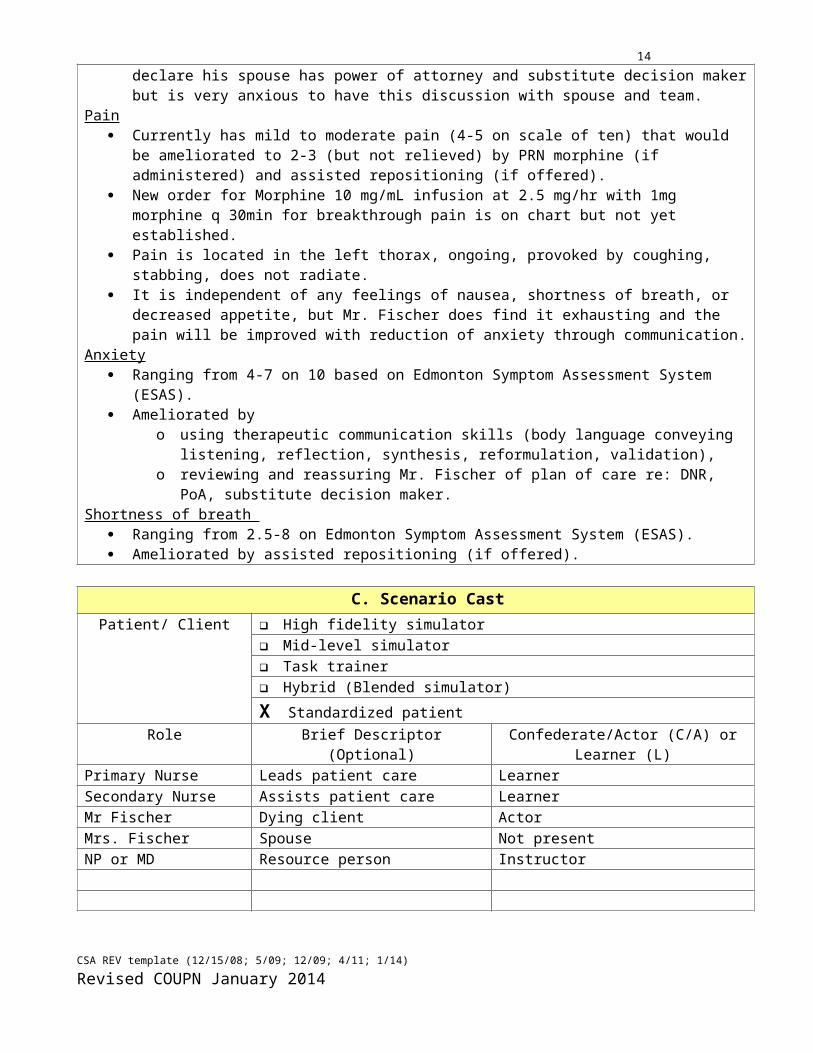
Mr. Fischer is ready to initiate “Do Not Resuscitate (DNR)” order and declare his spouse has power of attorney and substitute decision maker but is very anxious to have this discussion with spouse and team.
Pain Currently has mild to moderate pain (4-5 on scale of ten) that would be ameliorated to 2-3 (but not
relieved) by PRN morphine (if administered) and assisted repositioning (if offered). New order for Morphine 10 mg/mL infusion at 2.5 mg/hr with 1mg morphine q 30min for
breakthrough pain is on chart but not yet established. Pain is located in the left thorax, ongoing, provoked by coughing, stabbing, does not radiate. It is independent of any feelings of nausea, shortness of breath, or decreased appetite, but Mr. Fischer
does find it exhausting and the pain will be improved with reduction of anxiety through communication.
Anxiety Ranging from 4-7 on 10 based on Edmonton Symptom Assessment System (ESAS). Ameliorated by
CSA REV template (12/15/08; 5/09; 12/09; 4/11; 1/14)Revised COUPN January 2014
10o using therapeutic communication skills (body language conveying listening, reflection,
synthesis, reformulation, validation), o reviewing and reassuring Mr. Fischer of plan of care re: DNR, PoA, substitute decision maker.
Shortness of breath Ranging from 2.5-8 on Edmonton Symptom Assessment System (ESAS). Ameliorated by assisted repositioning (if offered).
C. Scenario CastPatient/ Client High fidelity simulator
Mid-level simulator Task trainer Hybrid (Blended simulator)
X Standardized patientRole Brief Descriptor
(Optional)Confederate/Actor (C/A) or Learner (L)
Primary Nurse Leads patient care LearnerSecondary Nurse Assists patient care LearnerMr Fischer Dying client ActorMrs. Fischer Spouse Not presentNP or MD Resource person Instructor
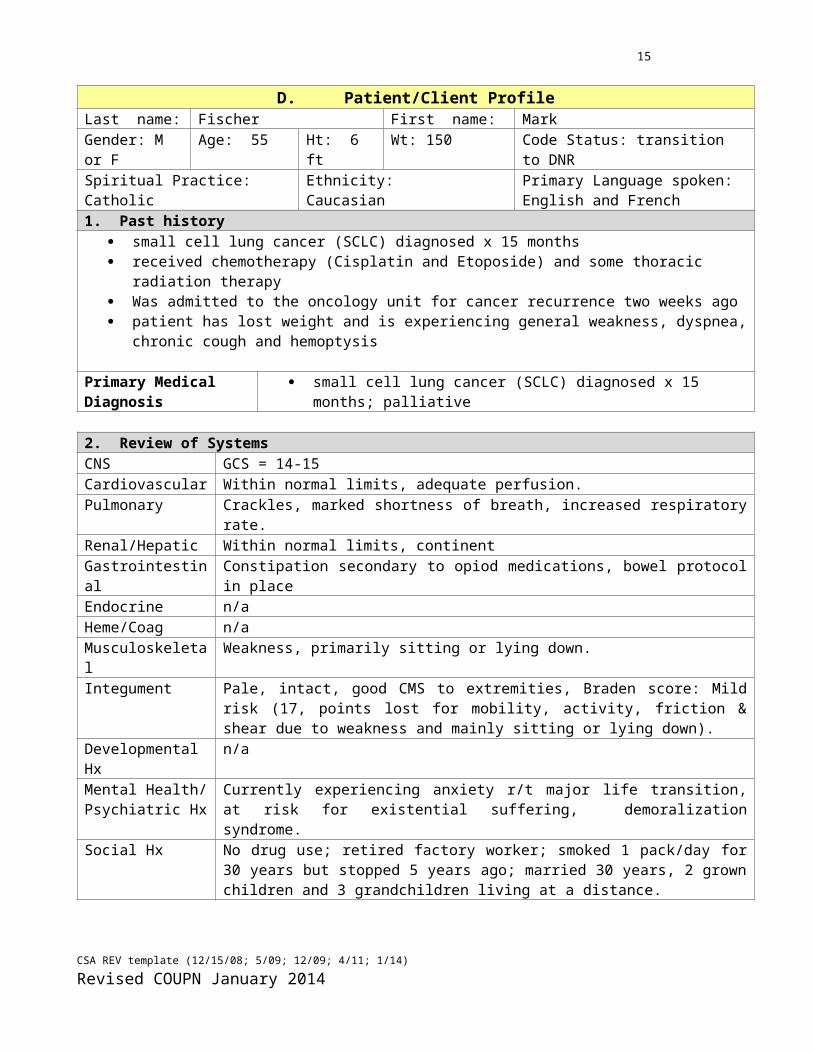
D. Patient/Client ProfileLast name: Fischer First name: MarkGender: M or F Age: 55 Ht: 6 ft Wt: 150 Code Status: transition to DNRSpiritual Practice: Catholic
Ethnicity: Caucasian
Primary Language spoken: English and French
1. Past history small cell lung cancer (SCLC) diagnosed x 15 months received chemotherapy (Cisplatin and Etoposide) and some thoracic radiation therapy Was admitted to the oncology unit for cancer recurrence two weeks ago patient has lost weight and is experiencing general weakness, dyspnea, chronic cough and hemoptysis
Primary Medical Diagnosis small cell lung cancer (SCLC) diagnosed x 15 months; palliative
2. Review of SystemsCNS GCS = 14-15Cardiovascular Within normal limits, adequate perfusion.Pulmonary Crackles, marked shortness of breath, increased respiratory rate.Renal/Hepatic Within normal limits, continentGastrointestinal Constipation secondary to opiod medications, bowel protocol in placeEndocrine n/aHeme/Coag n/aMusculoskeletal Weakness, primarily sitting or lying down.
CSA REV template (12/15/08; 5/09; 12/09; 4/11; 1/14)Revised COUPN January 2014
11Integument Pale, intact, good CMS to extremities, Braden score: Mild risk (17, points lost for
mobility, activity, friction & shear due to weakness and mainly sitting or lying down).Developmental Hx n/aMental Health/ Psychiatric Hx
Currently experiencing anxiety r/t major life transition, at risk for existential suffering, demoralization syndrome.
Social Hx No drug use; retired factory worker; smoked 1 pack/day for 30 years but stopped 5 years ago; married 30 years, 2 grown children and 3 grandchildren living at a distance.
Alternative/ Complementary Medicine Hx n/a
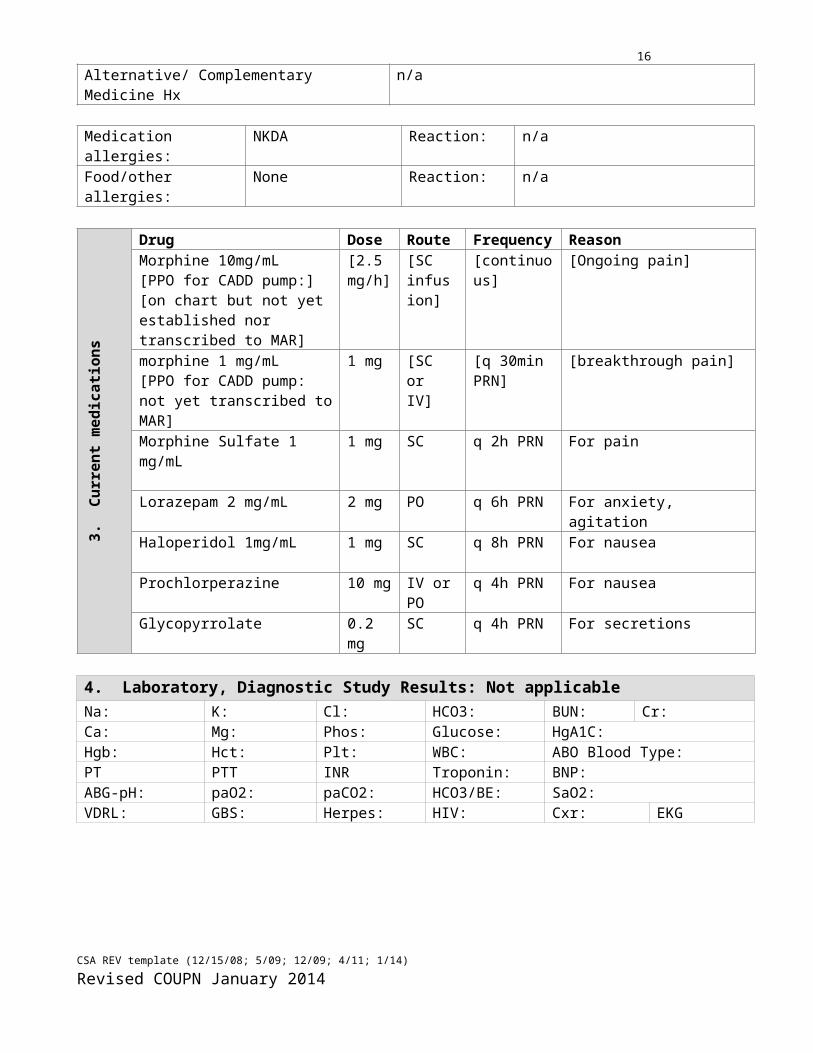
Medication allergies: NKDA Reaction: n/aFood/other allergies: None Reaction: n/a
3. C
urre
nt m
edic
ation
s
Drug Dose Route Frequency ReasonMorphine 10mg/mL[PPO for CADD pump:][on chart but not yet established nor transcribed to MAR]
[2.5 mg/h]
[SC infusion]
[continuous] [Ongoing pain]
morphine 1 mg/mL [PPO for CADD pump: not yet transcribed to MAR]
1 mg [SC or IV]
[q 30min PRN]
[breakthrough pain]
Morphine Sulfate 1 mg/mL 1 mg SC q 2h PRN For pain
Lorazepam 2 mg/mL 2 mg PO q 6h PRN For anxiety, agitation
Haloperidol 1mg/mL 1 mg SC q 8h PRN For nausea
Prochlorperazine 10 mg IV or PO q 4h PRN For nauseaGlycopyrrolate 0.2 mg SC q 4h PRN For secretions
4. Laboratory, Diagnostic Study Results: Not applicableNa: K: Cl: HCO3: BUN: Cr: Ca: Mg: Phos: Glucose: HgA1C:Hgb: Hct: Plt: WBC: ABO Blood Type: PT PTT INR Troponin: BNP:ABG-pH: paO2: paCO2: HCO3/BE: SaO2: VDRL: GBS: Herpes: HIV: Cxr: EKG
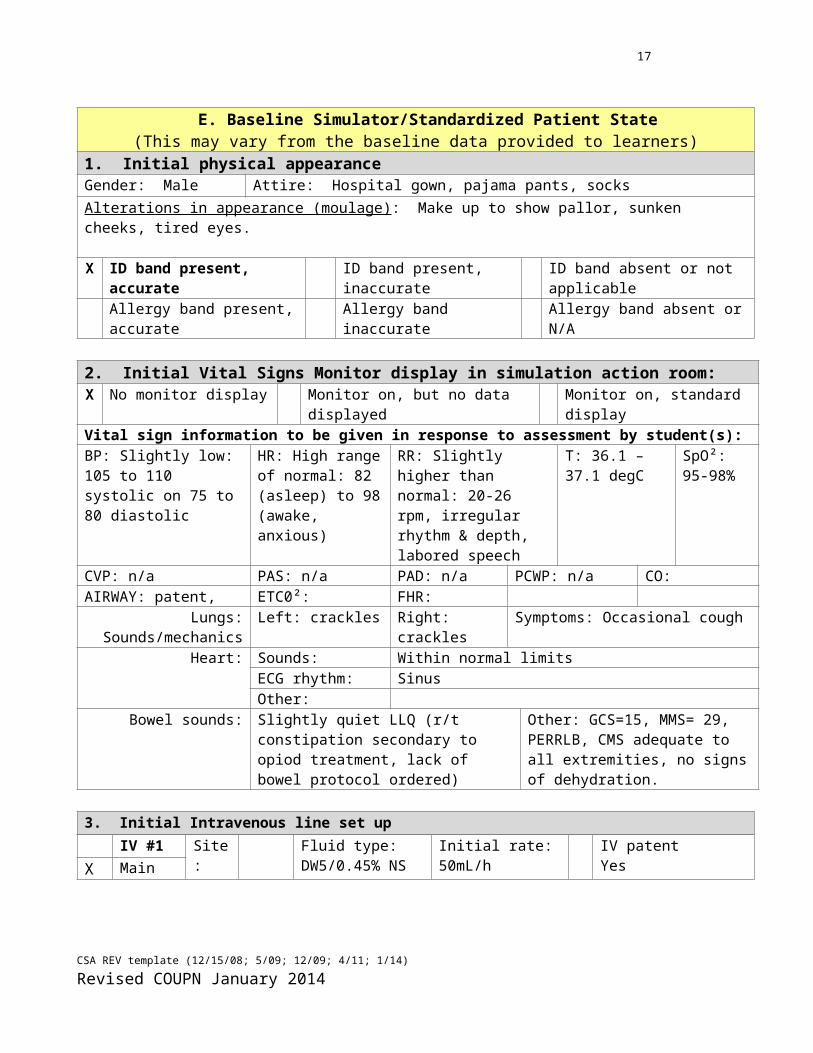
E. Baseline Simulator/Standardized Patient State(This may vary from the baseline data provided to learners)
1. Initial physical appearance
CSA REV template (12/15/08; 5/09; 12/09; 4/11; 1/14)Revised COUPN January 2014
12Gender: Male Attire: Hospital gown, pajama pants, socksAlterations in appearance (moulage): Make up to show pallor, sunken cheeks, tired eyes.
X ID band present, accurate ID band present, inaccurate ID band absent or not applicableAllergy band present, accurate Allergy band inaccurate Allergy band absent or N/A
2. Initial Vital Signs Monitor display in simulation action room:X No monitor display Monitor on, but no data displayed Monitor on, standard displayVital sign information to be given in response to assessment by student(s):BP: Slightly low: 105 to 110 systolic on 75 to 80 diastolic
HR: High range of normal: 82 (asleep) to 98 (awake, anxious)
RR: Slightly higher than normal: 20-26 rpm, irregular rhythm & depth, labored speech
T: 36.1 – 37.1 degC
SpO²: 95-98%
CVP: n/a PAS: n/a PAD: n/a PCWP: n/a CO:AIRWAY: patent, ETC0²: FHR:
Lungs:Sounds/mechanics
Left: crackles Right: crackles Symptoms: Occasional cough
Heart: Sounds: Within normal limits ECG rhythm: SinusOther:
Bowel sounds: Slightly quiet LLQ (r/t constipation secondary to opiod treatment, lack of bowel protocol ordered)
Other: GCS=15, MMS= 29, PERRLB, CMS adequate to all extremities, no signs of dehydration.
3. Initial Intravenous line set upIV #1 Site:
L hand
Fluid type:DW5/0.45% NS
Initial rate:50mL/h
IV patentYesX Main
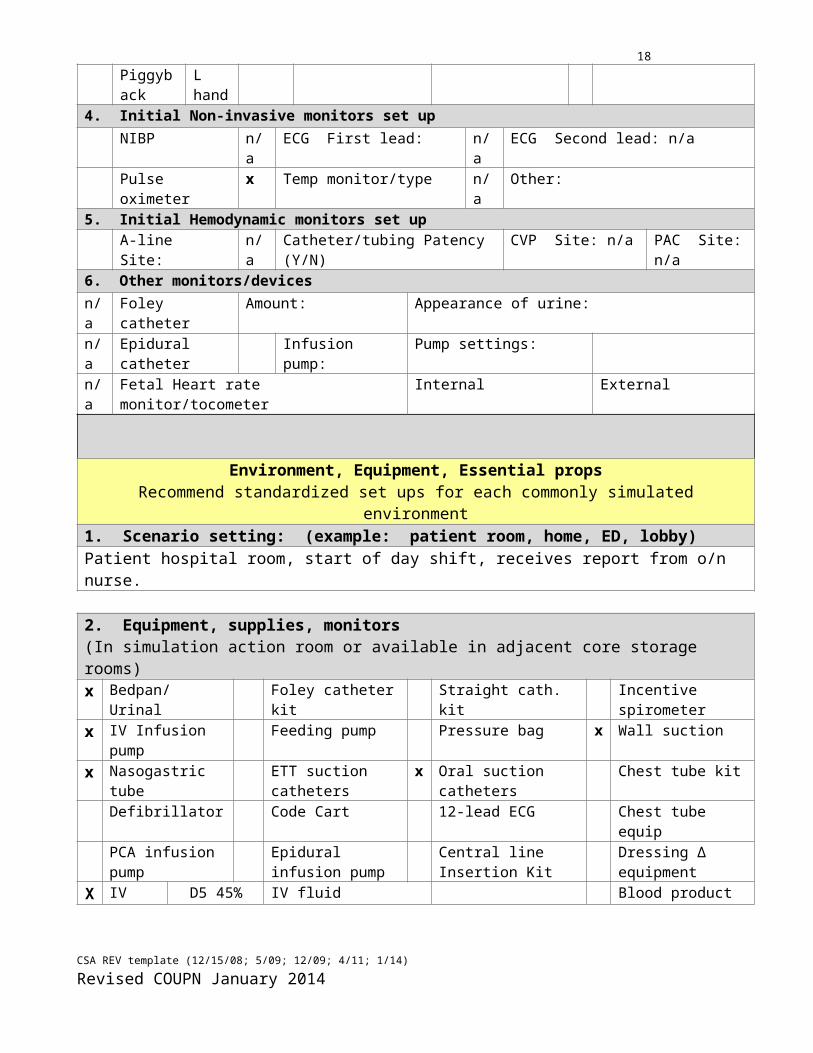
Piggyback4. Initial Non-invasive monitors set up
NIBP n/a ECG First lead: n/a ECG Second lead: n/aPulse oximeter x Temp monitor/type n/a Other:
5. Initial Hemodynamic monitors set upA-line Site: n/a Catheter/tubing Patency (Y/N) CVP Site: n/a PAC Site: n/a
6. Other monitors/devicesn/a Foley catheter Amount: Appearance of urine:n/a Epidural catheter Infusion pump: Pump settings: n/a Fetal Heart rate monitor/tocometer Internal External
Environment, Equipment, Essential props Recommend standardized set ups for each commonly simulated environment
1. Scenario setting: (example: patient room, home, ED, lobby)Patient hospital room, start of day shift, receives report from o/n nurse.
CSA REV template (12/15/08; 5/09; 12/09; 4/11; 1/14)Revised COUPN January 2014
13
2. Equipment, supplies, monitors(In simulation action room or available in adjacent core storage rooms)x Bedpan/ Urinal Foley catheter kit Straight cath. kit Incentive spirometerx IV Infusion pump Feeding pump Pressure bag x Wall suction x Nasogastric tube ETT suction catheters x Oral suction catheters Chest tube kit
Defibrillator Code Cart 12-lead ECG Chest tube equipPCA infusion pump Epidural infusion
pumpCentral line Insertion Kit
Dressing ∆ equipment
XIV fluid Type: D5 45% N/S
IV fluid additives: Blood productABO Type:# of units:
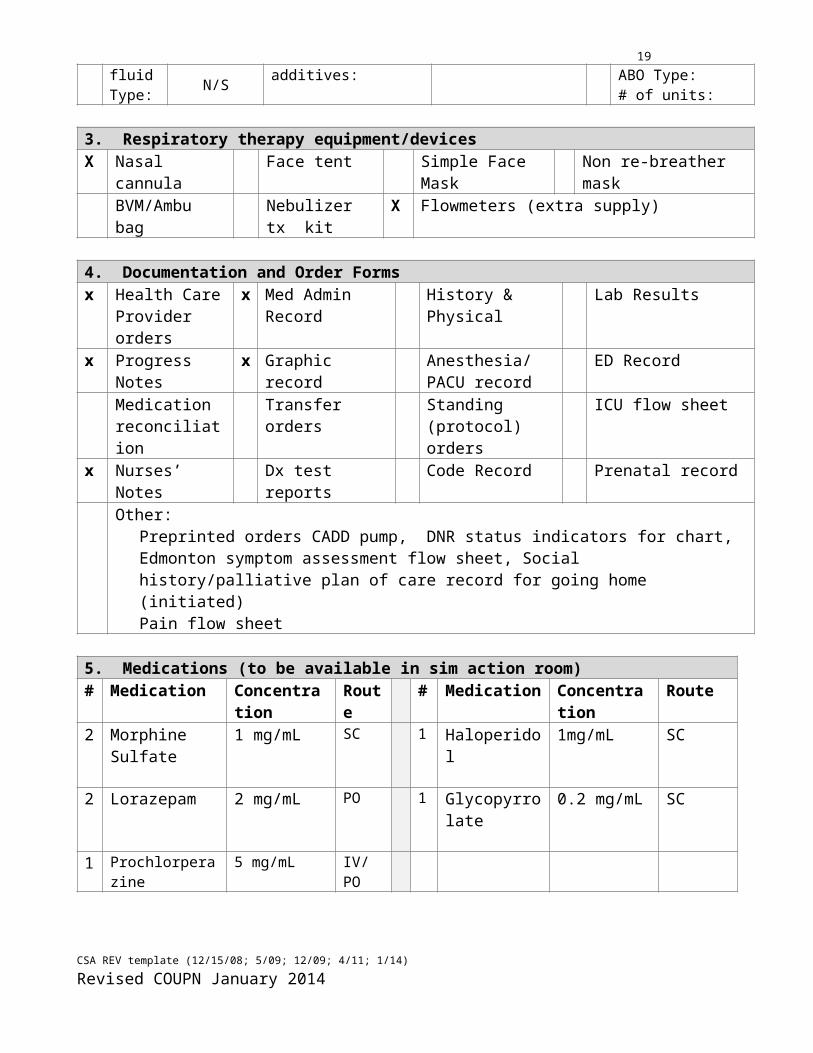
3. Respiratory therapy equipment/devicesX Nasal cannula Face tent Simple Face Mask Non re-breather mask
BVM/Ambu bag Nebulizer tx kit X Flowmeters (extra supply)
4. Documentation and Order Formsx Health Care
Provider orders x Med Admin
RecordHistory & Physical Lab Results
x Progress Notes x Graphic record Anesthesia/PACU record
ED Record
Medication reconciliation
Transfer orders Standing (protocol) orders
ICU flow sheet
x Nurses’ Notes Dx test reports Code Record Prenatal recordOther:
Preprinted orders CADD pump, DNR status indicators for chart, Edmonton symptom assessment flow sheet, Social history/palliative plan of care record for going home (initiated)Pain flow sheet
5. Medications (to be available in sim action room)# Medication Concentration Route # Medication Concentration Route2 Morphine
Sulfate 1 mg/mL SC 1 Haloperidol 1mg/mL SC
2 Lorazepam 2 mg/mL PO 1 Glycopyrrolate 0.2 mg/mL SC
1 Prochlorperazine 5 mg/mL IV/PO
CSA REV template (12/15/08; 5/09; 12/09; 4/11; 1/14)Revised COUPN January 2014

14
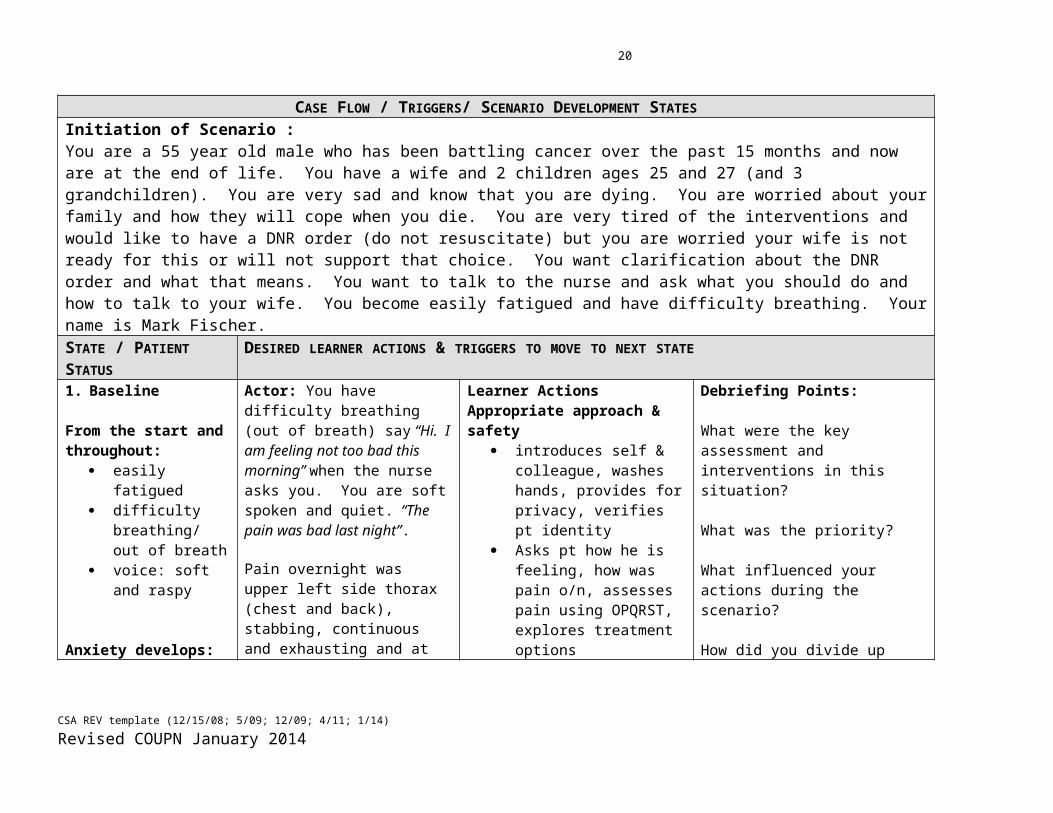
CASE FLOW / TRIGGERS/ SCENARIO DEVELOPMENT STATESInitiation of Scenario : You are a 55 year old male who has been battling cancer over the past 15 months and now are at the end of life. You have a wife and 2 children ages 25 and 27 (and 3 grandchildren). You are very sad and know that you are dying. You are worried about your family and how they will cope when you die. You are very tired of the interventions and would like to have a DNR order (do not resuscitate) but you are worried your wife is not ready for this or will not support that choice. You want clarification about the DNR order and what that means. You want to talk to the nurse and ask what you should do and how to talk to your wife. You become easily fatigued and have difficulty breathing. Your name is Mark Fischer.STATE / PATIENT STATUS DESIRED LEARNER ACTIONS & TRIGGERS TO MOVE TO NEXT STATE1. Baseline
From the start and throughout:
easily fatigued difficulty
breathing/ out of breath
voice: soft and raspy
Anxiety develops: fidgety, sighing, worried look, slightly inattentive to nurse
Actor: You have difficulty breathing (out of breath) say “Hi. I am feeling not too bad this morning” when the nurse asks you. You are soft spoken and quiet. “The pain was bad last night”.
Pain overnight was upper left side thorax (chest and back), stabbing, continuous and exhausting and at 8-9/10. Shortness of breath is helped by repositioning.
You answer the questions that the nurse will ask you. Hold your concern about the DNR status until the nurse asks you why you are anxious/upset.
Triggers: If the nurse does not ask you what is in your mind after 5 minutes you can go to Section 2.
Learner ActionsAppropriate approach & safety
introduces self & colleague, washes hands, provides for privacy, verifies pt identity
Asks pt how he is feeling, how was pain o/n, assesses pain using OPQRST, explores treatment options
Asks about shortness of breath, assesses, offers repositioning
Begins head to toe and vital sign assessments
At some point should ask about patient appearing anxious.
If student does not ask about anxiety, actor will proceed to section 2 after ca. 5 minutes
Primary delegates appropriately to secondary nurse.
Debriefing Points:
What were the key assessment and interventions in this situation?
What was the priority?
What influenced your actions during the scenario?
How did you divide up what needed to be done?
CSA REV template (12/15/08; 5/09; 12/09; 4/11; 1/14)Revised COUPN January 2014
15
STATE / PATIENT STATUS DESIRED ACTIONS & TRIGGERS TO MOVE TO NEXT STATEPart 2.
AnxiousAfraid
You are anxious, afraid of suffering if you decide for the DNR.
Teary
Operator/Actor
“Can I talk to you about something that has been bothering me?”
“I think I am close to the end and I am not sure how to tell my family this.”
“I don’t want anything done to prolong all of this...I just want to go peacefully but I am also scared of how painful this might be”
“The doctor talked about this possibility and we made a plan at the beginning, but I can’t believe it is happening to me”
“My wife will need to make decisions for me, but I don’t know if she is ready for me to be dying”
Triggers:
Either nurse asking you what is on your mind or by 4-5 minutes
Learner Actions:
Therapeutic communication: Shows active listening
through body language (arms uncrossed, leaning twds pt, eye level, looks at patient)
Uses techniques of communication such as reflection, synthesis, reformulation, validation.
Validates patient’s concerns & experiences
Reassures and creates/reviews plan
Explores stages of grief of patient and his perception of his wife’s grieving.
Restates and clarifies ambiguous statements to obtain clear information.
Provides accurate information about DNR, PoA, substitute decision making as per CNO Practice Guidelines, assigned journal articles.
Debriefing Points:
How did you let the patient know you were listening?
Do you think the patient felt heard/understood?
How did you assess what the patient already knew?
How did your pre-reading of CNO guidelines and journal articles help you with the factual information the patient needed?
CSA REV template (12/15/08; 5/09; 12/09; 4/11; 1/14)Revised COUPN January 2014
16
STATE / PATIENT STATUS DESIRED ACTIONS & TRIGGERS TO MOVE TO NEXT STATEPart 3.
Concerned, anxious, tearful
You are anxious because you think your wife/husband will not agree with your decision. It is not easy for you to open to the nurse.
Weary
Restrained/Taciturn/ Withdrawn
Operator/Actor:
“I don’t think my wife is okay with that (DNR order) She wants everything done. How can I tell her I don’t want that?”
“I just can’t do this anymore. I am so tired.”
“I want them to be okay, but I am afraid they won’t be, especially my kids…”
“I don’t want to drag them down”
Triggers: 6-7 min
Learner Actions:
Explores/assesses the possibility of existential suffering, depression, panic attack, demoralization syndrome
Provides reassurance Offers links to
assistance/resources available in hospital &/or community
Debriefing Points:
Are you comfortable with silence/ with being present for the patient in this scenario?
What members of the interprofessional team (in hospital or in the community) might be well prepared to deal with this depth of suffering?
CSA REV template (12/15/08; 5/09; 12/09; 4/11; 1/14)Revised COUPN January 2014
17
STATE / PATIENT STATUS DESIRED ACTIONS & TRIGGERS TO MOVE TO NEXT STATEPart 4.
Stock phrases can be used throughout:
Operator/Actor:
“Can you talk to her and tell her what I want?”
“She might understand better from you.”
Triggers: 6-10 minutes
“I am not sure why this happened to me.” “This is not what I expected.” “Can I ask: will I be in a lot of pain? (If this wasn’t addressed elsewhere)
Learner Actions:
Assures patient that they will be present as support for his conversation with his wife
Debriefing Points
Let’s discuss options for supporting this patient.
Scenario End Point: 20 minutes has passed or student & patient have exhausted the conversation.
Suggestions to decrease complexity: Suggestions to increase complexity: CADD pump set up
CSA REV template (12/15/08; 5/09; 12/09; 4/11; 1/14)Revised COUPN January 2014
18
CSA REV template (12/15/08; 5/09; 12/09; 4/11; 1/14)Revised COUPN January 2014
19
APPENDIX A: HEALTH CARE PROVIDER ORDERS
Patient Name: Mark Fischer
DOB/DDN: 1958-10-01Age: 56Weight: 69 kg MR#: 24516789Room: 20
Diagnosis: SCLC
[Affix label or stamp here]
No Known Allergies Allergies & SensitivitiesDate Time HEALTH CARE PROVIDER ORDERS AND SIGNATURE Transcribed by
(initials & signature):
Yesterday 1000 Lorazepam 2mg PO q 6h PRN if anxious NBMorphine sulfate 1mg SC q 2h PRN for pain NBProchorperazine 10 mg IV/PO q 4h PRN for nausea NBHaloperidol 1 mg SC/PO q 8h for nausea NBIV: D5W + 0.45NS at 50cc/h NBAAT, DAT NB
F. Quirran, MD R2Nathan Benoit, RN
Today 0800 Sub-Q set for PRN and PCA pain CD Morphine 10mg/mL by SC infusion via CADD pump at rate of 2.5 mg/h
CD
Morphine 1 mg q 30min for breakthrough pain CDDiscontinue previous morphine order CD
F. Quirran, MD R2Carole Deno RN
*Ideally, the orders for today would be done on a PPO See section 4, “Environment, Equipment, Props” on pg 12
CSA REV template (12/15/08; 5/09; 12/09; 4/11)Revised COUPN January 2014
20
APPENDIX B: Digital images of manikin and/or scenario milieu
CSA REV template (12/15/08; 5/09; 12/09; 4/11)Revised COUPN January 2014
Insert digital photo of initial scenario set up here
Insert digital photo here Insert digital photo here
Insert digital photo hereInsert digital photo here
21
APPENDIX C: DEBRIEFING GUIDE
General Debriefing PlanIndividual Group With Video Without Video
Debriefing MaterialsDebriefing Guide Objectives Debriefing Points QSEN
CPSI Competencies to consider for debriefing scenarios Culture Teamwork/Collaboration Identify safety risk
Communication Issues in environment Respond to safety risk
Sample Questions for Debriefing
Interprofessional Competencies to consider for debriefing scenariosRole Clarification Interprofessional Teamwork Functioning
Patient/Family /Client ? Community centred care
Collaborative Leadership
Interprofessional CommunicationSample Questions for Debriefing
General questions:
• What was the key assessment and interventions in this situation? What was the priority? What influenced your actions during the scenario?
• How do you think the simulation went? Were you comfortable in this role? Why or why not?
• What were your favorite and least favorite aspects of the simulation?
• What were some of your successes? What made you effective? Your difficulties? How could you become more effective? Give me specific examples.
Additional questions:
• What information did you have about this case?
• Was the student assessing knowledge of the disease state? Was the student assess the knowledge of prognosis
CSA REV template (12/15/08; 5/09; 12/09; 4/11)Revised COUPN January 2014

22
• Was the patient's pain well controlled, by the nursing interventions? What are non-pharmaceutical techniques we could use to help control pain? How and when should we re-evaluate the patient's pain?
• What type of questions should we ask pt to assess her pain with the use of the PQRST (Provoke = what causes the pain? Quality = is it dull, sharp, crushing, stabbing or burning? Radiates = where does the pain radiate? Severity = how severe is the pain on a scale of 1 to 10? Time = time pain started?)
• What kind of teaching needs to be done?
In summary (closing) :
These are the things you identified as going well, and these are the things you told me you need to work on...
The take home points include.... and finally I saw vast improvement in these areas...
What worked well:… Even better if:…
CSA REV template (12/15/08; 5/09; 12/09; 4/11)Revised COUPN January 2014