· web viewthe drug product—episcleral topotecan—consists of a sustained-release formulation...
TRANSCRIPT

SUSTAINED RELEASE TOPOTECAN PERIOCULAR CHEMOTHERAPY VIA EPISCLERAL IMPLANT (CHEMOPLAQUE) for RETINOBLASTOMA
The Retinoblastoma ProgramDepartments of Ophthalmology and Vision Science & Pediatric Oncology
The Hospital for Sick Children (SickKids)Toronto, Ontario, CANADA

Episcleral Toptecan Chemoplaque Phase I–II Trial 2
Targeted Therapy Technologies, LLC (DBA: 3T Ophthalmics) supports this clinical trial.
IND number assigned: 112785
ClinicalTrials.gov Identifier:

Episcleral Toptecan Chemoplaque Phase I–II Trial 3
TERMINOLOGY AND NAMING OF DRUG PRODUCTThe drug product—Episcleral Topotecan—consists of a sustained-release formulation of topotecan hydrochloride—drug substance—contained within an episcleral implant at various ascending doses. The Episcleral Implant in various publications and in this protocol is referred variously as an Episcleral Device, Episcleral Topotecan, Episcleral Sustained Release Topotecan, Episcleral Reservoir, Episcleral Exoplant, Episcleral Implant, and Targeted Transscleral Delivery System (TTDS).
In the current protocol we use the term Chemoplaque. All these terms refer to the same drug product and are interchangeable. Episcleral Topotecan clinical supplies will be shipped from the manufacturer (Targeted Therapy Technologies, LLC/DBA 3T Ophthalmics) ready for use and require no further manipulation before ocular placement.
A full brochure with the drug product details provided by the manufacturer is Appendix I.

Episcleral Toptecan Chemoplaque Phase I–II Trial 4
PARTICIPATING CENTERS
Hospital for Sick Children (SickKids)
555 University Avenue
Toronto, Canada

Episcleral Toptecan Chemoplaque Phase I–II Trial 5
RESEARCH TEAM:Hospital for Sick ChildrenPrincipal Investigator
Brenda L. Gallie, MD, FRCSC
Co-Investigator
Furqan Shaikh, MD, FRCPC
Co-Investigator
Helen Dimaras, PhD
Co-Investigator
Sameh Soliman, MD, PhDmed

Episcleral Toptecan Chemoplaque Phase I–II Trial 6
ABSTRACT

Episcleral Toptecan Chemoplaque Phase I–II Trial 7
EXPERIMENTAL DESIGN SCHEMA

Episcleral Toptecan Chemoplaque Phase I–II Trial 8
1.0 HYPOTHESES AND OBJECTIVES Primary Hypothesis
Sustained release topotecan delivered by Chemoplaque will achieve complete remission (CR) of small volume of retinoblastoma and facilitate appropriate focal therapy in the event of small volume residual/recurrent disease.
Secondary Hypothesis
Sustained release topotecan delivered by Chemoplaque will reduce the burden of systemic treatment, anaesthetics, number of focal treatments and time from diagnosis to CR for retinoblastoma.
Objectives
Primary Objectives
To determine effectiveness of sustained release topotecan topotecan delivered by Chemoplaque to achieve CR of small volume retinoblastoma.
Secondary Objectives:
To quantify total treatment burden (duration to CR, rate of recurrence, number of EUAs, economic impact, eye salvage rate, mortality)
To identify tumor characteristics that correlate with response to Topotecan (i.e. vitreous seeds, subretinal seeds, multifocality, tumor height …etc.)
2.0 BACKGROUNDManagement of retinoblastoma
Retinoblastoma is the most common pediatric malignant intraocular tumor that originates from the retina (the innermost layer of the ocular wall). Retinoblastoma arises when both copies the retinoblastoma tumor supressor gene, RB1, are pathogenic (non-functional) in a developing retinal cell. It affects one or both eyes, depending on the developmental timing of the first RB1 pathogenic variant: if RB1 is damaged in all cells of the person usually both eyes are independently affected by retinoblastoma when the second RB1 gene is damaged in a specific susceptible developing retinal cell. If both RB1 genes are damaged only in the developing retinal cell that becomes a tumor, only one tumor is formed, affecting one eye.
The primary goal of therapy is prevention of tumor spread outside the eye to save the child’s life. If the tumor is advanced (with a potential to spread outside the eye), removal of the eye (enucleation) is the safest option. However, if the tumor is less advanced and the optic nerve is visible, vision and eye salvage become the priorities.
In unilateral children with poor visual potential, treatment burden is weighed against potential outcome in informed discussion with the parents. For advanced, high risk disease, enucleation is a good choice that avoids invasive proceedures that might not control disease, but consume a large part of the child’s early experience. On the other hand, in bilateral disease threatens both eyes and blindness.
Cancer Staging

Episcleral Toptecan Chemoplaque Phase I–II Trial 9
Staging at initial diagnosis determines treatment and prognosis. Two staging schemes to predict eye salvage have caused significant confusion in the literature, preventing proper comparison between studies.1 The International Intraocular Retinoblastoma Classification (IIRC) staged eyes as Group A (very low risk) through E (very high risk).2 A subsequent modification of this classification3 resulted in severely advanced eyes being classified with less-affected eyes, so that “Group E” did not indicate the danger of extraocular disease.4-6
The 2017 American Joint Committee on Cancer (AJCC) 8th edition TNMH (tumor, node, metastasis, heritable trait) (Table 1) clinical and pathological staging system is the first evidence-based system to predict prognosis of both eye(s) and patients.1 It is informed by an international survey of 1728 eyes with retinoblastoma comparing all the previous classifications and best separates features of eye disease predictive of the likelihood to save the eye without use of external beam irradiation.
Current Retinoblastoma Treatment
Removal of the eyePrimary eye removal (enucleation) remains the definitive treatment for advanced unilateral retinoblastoma (TNMH1 cT3 and IIRC2 Group E eyes), allowing the child to return to normal life and enabling histopathological determination of risk of extraocular tumor.7 For unilateral retinoblastoma, enucleation is the definitive treatment when the optic nerve is not visible and in the presence of retinal detachment (TNMH1 cT2a and IIRC2 Group D eyes) or extensive vitreous seeds (TNMH1 cT2b and IIRC2 Group D eyes) that otherwise require invasive treatments over several years that are costly to the child and family, to save an eye with poor vision. Enucleation is strongly recommended when orbital or optic nerve involvement is suspected, there is anterior segment invasion, neovascular glaucoma, intraocular hemorrhage, orbital cellulitis, and no potential for useful vision.8
Systemic chemotherapySystemic chemotherapy is effective to reduce size of intraocular retinoblastoma tumors. Systemic chemotherapy alone is insufficient to control tumor and focal therapy (laser, cryotherapy) consolidation therapy are added subsequently to control tumor.9 Handheld OCT is excellent to accurately assess tumor activity related to focal therapy scars.10
The most common protocol world-wide includes Vincristine, Etoposide and Carboplatin (VEC) on a 3-weekly schedule for 4 to 6 cycles. The main indication for systemic chemotherapy is bilateral and trilateral retinoblastoma. Second line regimens for refractory retinoblastoma have been used. The St. Jude group combined Topotecan with Carboplatin and Vincristine followed by focal consolidation (details....).10
Intra-arterial chemotherapy (IAC)Direct delivery of one or multiple chemotheraoeutic agents (Melphalan, Toptecan) into the ophthalmic artery is currently used to treat eyes with retinoblastoma.6 First described by the Japanese and revisited by the Memorial Sloan-Kettering Cancer Center group,11-13 ocular salvage is reported to be high as both primary and salvage therapy. 11,14-26 The reported data of efficacy and ocular and periocular complications is still missing important details regarding metastasis, second cancers, visual outcome and choroidal health.27 IAC is an expensive modality that is not available in many centers even in developed countries. Published evidence on efficacy or safety of IAC compared to other treatment modalities is limited, and its relative benefits and harms are not known. The published non-comparative data is voluminous, but difficult for readers to critically assess.
Episcleral Toptecan Chemoplaque Phase I–II Trial 10
Radiotherapy28,29 Therefore radiotherapy is now only used if all other eye salvage options have failed for the last eye of a bilateral retinoblastoma patient. At the cost of doubling the second câncer risk, the eye can be saved with useful vision.
Consolidation with focal laser photocoagulation or cryotherapyConsolidation with local laser photocoagulation or cryotherapy following chemotherapy (systemic or IAC) is highly effective for cT1 (Groups A and B) eyes with intraretinal disease.30,31 32,33
Periocular ChemotherapyChemotherapy has been delivered locally to the eye. Direct injection of carboplatin into the subconjunctival or subtenon space was associated with complications including optic atrophy with profound vision loss,34 ocular motility problems,35 and periorbital cellulitis. COG ARET0321 (single arm trial of systemic and subtenon chemotherapy for Groups C and D retinoblastoma) nt of patients into ARET0321 was slower than expected and necessitated early closure of the study, in part, of the acute inflammatory response and complications of of rectus muscle fibrosis causing restrictive strabismus.
Subtenon injections of Topotecan in fibrin sealant reduced small volume intraocular retinoblastoma, combined with focal therapy.36 Doses ranged from 2.01-4.62mg/m2. Ocular toxicity was minimal and motility restriction was observed. Systemic effects included CTCAE grade 1-4 hematologic toxicity that improved after one week and did not require intervention. 37
Vitreous seeds are generally resistant to systemic and intra-arterial chemotherapy Intravitreal chemotherapy (melphalan and/or topotecan) now often controls the most difficult form of intraocular retinoblastoma to cure.38 usually repeated monthly depending on clinical response. The main complications include vitreous hemorrhage, retinal tears/detachment, damage to the lens leading to cataract, endophthalmitis and direct retinal toxicity when the drug is not well dispersed through the vitreous.39,40 A recent retrospective study of intravitreal chemotherapy injections in 10 retinoblastoma treatment centers worldwide found no extraocular extension of tumor when used with the described precautions, including selection of eyes where the source of seeds is controlled, preinjection lowering of intraocular pressure, and postinjection cryotherapy to the needle and needle track.38,41
Oncolytic vírus therapyOne recent publication42 describes the basic science of engineering an oncolytic vírus that targets cancer cells that have lost RB1, which targets RB1-deficient cells. Two patients were treated with intravitreal injections: boths eye showed very significant inflammation; one eye was enucleated with remaining active tumor on pathology.

Episcleral Toptecan Chemoplaque Phase I–II Trial 11
DEPICT HEALTH
DEPICT HEALTH (depictrb.technainstitute.com/username:demo-user/password:Demo1234) is a retinoblastoma-specific communication service that collections life-long retinoblastoma point-of-care data displayed visually on a timeline. Deep details are accessible in real-time by the circle of care, including patients, families and clinicians.6-8 DEPICT HEALTH has supported retinoblastoma care in SickKids since 2003, and in 2019 will be available to SickKids and Alberta patients to using Cloud computing.
The entry and eligibility criteria will be in the details of each encounter and treatment. The key summary criteria will clear in DEPICT HEALTH for each child assessed for eligibility. Outcome data for evaluation of outcomes will be supported by deep details of each tumor in each eye over many years in depict, as routinely collected in quality care irrespective of the Chemoplaque Trial.
3.0 Importance of this TrialImprove outcomes
Reduce treatment burden
Reduce cost
Deep eligibility and outcome data through DEPICT HEALTH
4.0 Preclinical evidenceAnimal studies
Purpose: To determine the safety, tolerability, and the pharmacokinetics (ocular and plasma) of various dosages of topotecan hydrochloride (TPT) formulated in the Targeted Transscleral Delivery Systems (TTDS) designed as Episcleral Implants (Episcleral Topotecan) and implanted onto the sclera of New Zealand White rabbits.
Methods: Female rabbits (n=87) assigned to toxicity (n=5 per dose group) or pharmacokinetics (n=3 per time point) groups, were implanted in the right eye with the test article TTDS Episcleral Implant containing doses ranging from 0.3 mg to 0.9 mg topotecan HCl. For the pharmacokinetic arm of the study, rabbits were euthanized after 24 hours, 48 hours, and 7, 14, 21, 28, 42, and 56 days (n=3 per time point). Plasma, ocular tissues (that were divided into distal and proximal sections relative to the implant site), and the test articles were collected from each animal during necropsy.
Ocular tolerability and toxicity were assessed by ocular examination (slit lamp biomicroscopy and indirect ophthalmoscopy), applanation tonometry (pneumatonometer), and electroretinography (ERG). Retinal findings were documented by fundus photography. Systemic tolerability was assessed by weight progression and observations for signs of toxicity.
Topotecan was assayed in the plasma and ocular tissue samples using a validated high-pressure liquid chromatography (HPLC) method for the detection and quantification of total topotecan and its lactone isoform (LLOQ = 1 ng/ml or ng/gram). Drug distribution is reported as Cmax (maximum concentration), Tmax (time when it reached maximum concentration), TLC90 (time above topotecan LC90 in retinoblastoma cell lines, 5 ng/ml or gram) and AUC (area under the time concentration curve).

Episcleral Toptecan Chemoplaque Phase I–II Trial 12
Results: All studied doses of Episcleral Topotecan were well tolerated systemically. No measurable concentrations of topotecan—either total topotecan or its lactone isoform—were found in the plasma after implantation of any dose of Episcleral Topotecan. All rabbits gained weight during the study period of 84 days. There was no evidence of a systemic response to topotecan treatment in the body weight data or daily health observations.
After implantation with Episcleral Topotecan 0.3 mg (containing 0.3 mg topotecan HCl), the proximal ocular tissues with therapeutically relevant exposure to topotecan’s active (lactone) isoform (Cmax, Tmax, TLC90) were: Choroid (2.7 ug/g, day 2, 14 days), sclera (1.3 ug/g, day 2, 21 days), retina (0.86 ug/g, day 2, 14 days). Topotecan (lactone isoform) also reached therapeutic concentrations in the distal sclera on days 2 and 14.
After implantation with Episcleral Topotecan 0.6 mg (containing 0.6 mg topotecan HCl), the proximal ocular tissues with therapeutically relevant exposure to topotecan’s active (lactone) isoform (Cmax, Tmax, TLC90) were: Choroid (10.6 ug/g, day 2, 21 days), retina (1.1 ug/g, day 1, 21 days), sclera (1 ug/g, day 21), and vitreous humor (8.2 ng/ml, day 21). In addition, topotecan lactone isoform was also detected at relevant concentrations in the distal tissues—sclera (126.3 ng/g on day 21), retina (50 ng/g on day 2), and vitreous (30 ng/ml on day 2).
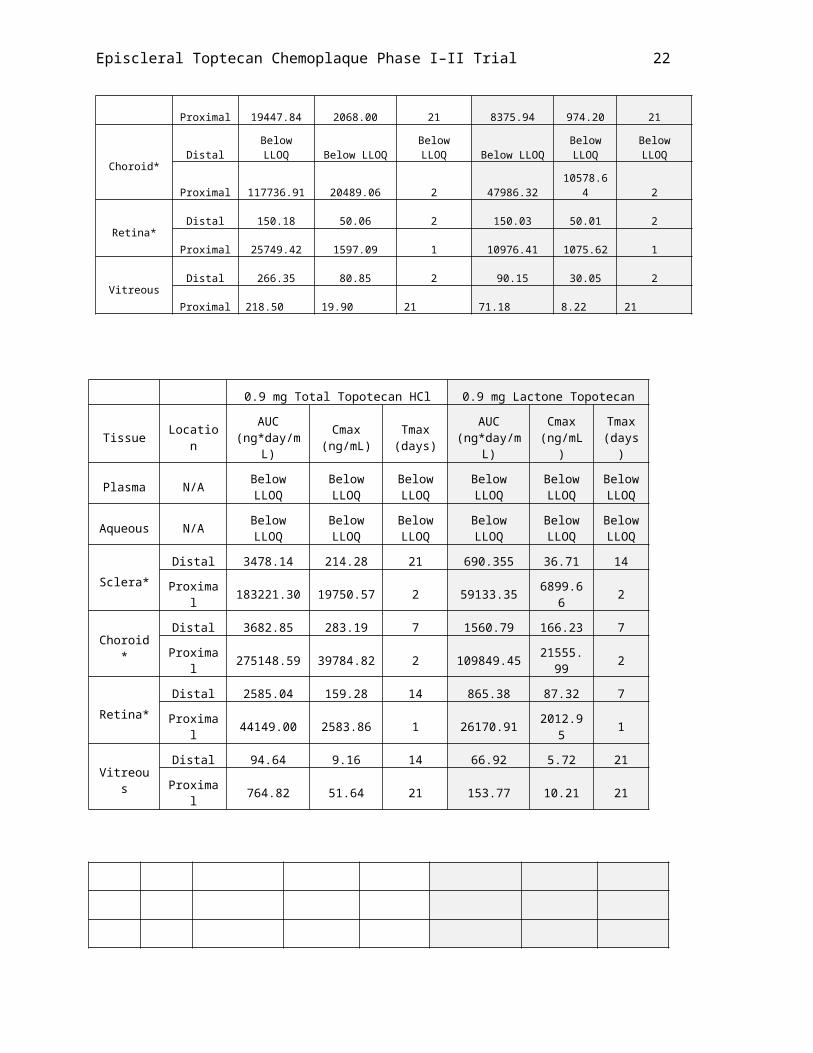
After implantation with Episcleral Topotecan 0.9 mg (containing 0.9 mg topotecan HCl), the proximal ocular tissues with therapeutically relevant exposure to topotecan’s active (lactone) isoform (Cmax, Tmax, TLC90) were: Choroid (21.6 ug/g, day 2, 21 days), retina (2 ug/g, day 1, 28 days), sclera (6.9 ug/g, day 2, 21 days), and vitreous humor (10.21 ng/ml, day 21). In the distal tissues relevant distribution of topotecan lactone was found in the sclera (36.71 ng/g, day 14, 21 days), choroid (166.23 ng/g, day 7, 21 days), retina (87.32 ng/g, day 7, 21 days) and vitreous (5.72 ng/ml on day 21).
Between days 1 and 7 after the implantation of any dose of Episcleral Topotecan (0.3, 0.6 and 0.9 mg of Topotecan HCl) a mild discharge, congestion and swelling of the conjunctiva, predominantly near the implantation site, was observed.
Between days 1 and 14, peaking on day 7, some degree of hyperemia of the choroid was noticed in all the eyes exposed to Episcleral Topotecan. It was predominantly mild (decrease of the white reflex between the mid-to-large choroidal vessels), but appeared to increase in extension and slightly in intensity from mild to moderate (blurred delineation of the mid-to-large choroidal vasculature) as a function of the dose.
Serous exudative retinal detachment was observed in eyes exposed to any dose of Episcleral Topotecan starting on day 7 and subsiding before day 21—mostly between days 7 and 14. Spontaneous and complete resolution occurred before day 28 in all cases. It was mostly located in the quadrant directly exposed to the test article, superior-temporal, but it was also sporadically found in the adjacent inferior quadrant (inferior-temporal) in the 0.6-mg and 0.9-mg dose groups.
Atrophy of the choroid was observed as mild starting at day 21 and it evolved up to day 42 to moderate (grade II) in dose groups 0.3-mg and 0.6-mg, or to severe (grade III) in dose group 0.9-mg. It invariably stabilized between days 56 and 83. The presence of atrophy in the adjacent inferior-temporal quadrant, was more frequent in eyes exposed to higher doses.
In animals implanted with Episcleral Topotecan 0.3 mg, there was no substantial difference in the intraocular pressure between the right eye (implanted) and the left eyes (controls) during the follow-up period. After Episcleral Topotecan 0.6 mg implantation, implanted eyes demonstrated a significant decrease in the intraocular pressure on days 7 (9 mmHg, CI 95% 2.4-15.6) and 14 (7.6 mmHg, CI 95% 2.2-13) compared to the control eyes. In the Episcleral Topotecan 0.9 mg

Episcleral Toptecan Chemoplaque Phase I–II Trial 13
group the average decrease in the IOP in tested vs. control eyes was also significant on day 7 (10.6 mmHg, CI 95% 2.17 to 19.03).
After implantation of 0.3-mg, 0.6-mg or 0.9-mg Episcleral Topotecan, due to the large variability inherent to the measured ERG responses in normal and control eyes, mostly non-significant changes were detected in either the amplitude or the implicit time of the studied parameters under the different stimuli conditions. On day 84, although mostly within the 95% confidence intervals of the control eye ERG readouts, a trend in the implanted eyes was observed towards a decrease of approximately 20 to 40% in the amplitude of a and b waves in scotopic and photopic conditions.
Non-significant decrease (within 95% confidence intervals of the ERG responses between tested and control eyes) were seen in both directions and mostly within the 95% confidence intervals. Significant but sporadic findings included changes after exposure to doses of topotecan at 0.3 mg in b-wave amplitude (scotopic 10 on day 84), and at 0.6 mg in the b-wave implicit time (photopic 3000 on day 14). Significant and consistent differences across different stimuli parameters were seen after 0.9 mg of topotecan on day 84, in the a-wave amplitude (scotopic 10000) and the b wave amplitude (scotopic 10 and 10000, and photopic 3000).
Explanted episcleral implants were completely depleted of topotecan at day 28 in all dose groups. Assay of the implant content of the 0.3 and 0.9 mg doses collected at necropsy on Day 21 showed that the content of the implant had decreased by 100%. The 0.6mg dose decreased by 97% on day 21 and 100% by Day 28.
HISTOLOGY
In general the implants appeared to be well tolerated. Both globes, the implant site, bulbar conjunctiva, both eyelids and the lacrimal glands were examined histopathologically. There was a small amount of chronic inflammation and mineralization in the wall of the implant pocket in some animals in all groups. Similarly, there was mild subacute inflammation in the bulbar conjunctiva in the right eye of some animals in all groups, probably nonspecific and secondary to the surgical and handling procedures. There was no meaningful difference between the three treatment groups. The left eye was normal in all animals.
Figures. Intraocular pressure (IOP) progression before and after implantation of Episcleral Topotecan containing 0.3, 0.6, or 0.9 mg of topotecan HCl. Tested eye: OD. Control eye: OS.
Base-line
Day 7 Day 14 Day 21 Day 28 Day 42 Day 56 Day 830.0
5.0
10.0
15.0
20.0
25.0
0.3 mg TPT: Mean IOP (CI 95%)
0D0S
IOP
(mm
Hg)

Episcleral Toptecan Chemoplaque Phase I–II Trial 14
Base-line
Day 7 Day 14 Day 21 Day 28 Day 42 Day 56 Day 830.0
5.0
10.0
15.0
20.0
25.0
30.0
0.6 mg TPT: Mean IOP (CI 95%)
0D0S
IOP
(mm
Hg)
Base-line
Day 7 Day 14 Day 21 Day 28 Day 42 Day 56 Day 830.0
5.0
10.0
15.0
20.0
25.0
30.0
0.9 mg TPT: Mean IOP (CI 95%)
0D0S
IOP
(mm
Hg)
Figures. Electroretinography implicit time and amplitude 84 days after implantation of episcleral topotecan containing 0.3, 0.6 or 0.9 mg topotecan HCl (TPT). Tested eye: OD. Control eye: OS.

Episcleral Toptecan Chemoplaque Phase I–II Trial 15

Episcleral Toptecan Chemoplaque Phase I–II Trial 16

Episcleral Toptecan Chemoplaque Phase I–II Trial 17

Episcleral Toptecan Chemoplaque Phase I–II Trial 18
Tables. Pharmacokinetics of topotecan (total and lactone) after implantation of Episcleral Topotecan containing 0.3, 0.6 or 0.9 mg of topotecan HCl: Area under the time-curve (AUC), maximum concentration (Cmax) and time to maximum concentration (Tmax) (*ng/g).
0.3 mg Total Topotecan HCl 0.3 mg Lactone Topotecan
Tissue LocationAUC
(ng*day/mL)Cmax
(ng/mL) Tmax (days)AUC
(ng*day/mL)Cmax
(ng/mL)Tmax (days)
Plasma N/A Below LLOQ Below LLOQBelow LLOQ Below LLOQ
Below LLOQ
Below LLOQ
Aqueous N/A 62.73 20.91 2 11.10 3.70 2
Sclera*Distal 1253.75 214.13 2 205.99 26.29 2
Proximal 29647.65 3563.05 2 8432.57 1304.18 2
Choroid* Distal 243.42 81.14 2 Below LLOQBelow LLOQ
Below LLOQ
Proximal 55170.19 8436.24 2 14787.60 2667.81 2
Retina* Distal Below LLOQ Below LLOQBelow LLOQ Below LLOQ
Below LLOQ
Below LLOQ
Proximal 9688.91 2322.07 2 3178.36 858.41 2
VitreousDistal Below LLOQ Below LLOQ
Below LLOQ Below LLOQ
Below LLOQ
Below LLOQ
Proximal 14.04 2.34 7 Below LLOQBelow LLOQ
Below LLOQ
0.6 mg Total Topotecan HCl 0.6 mg Lactone Topotecan
Tissue LocationAUC
(ng*day/mL) Cmax (ng/mL) Tmax (days)AUC
(ng*day/mL)Cmax
(ng/mL) Tmax (days)
Plasma N/A Below LLOQ Below LLOQ Below LLOQ Below LLOQBelow LLOQ Below LLOQ
Aqueous N/A Below LLOQ Below LLOQ Below LLOQ Below LLOQBelow LLOQ Below LLOQ
Sclera*Distal 4903.13 532.55 21 1351.65 126.35 21
Proximal 19447.84 2068.00 21 8375.94 974.20 21
Choroid* Distal Below LLOQ Below LLOQ Below LLOQ Below LLOQBelow LLOQ Below LLOQ
Proximal 117736.91 20489.06 2 47986.32 10578.64 2
Retina*Distal 150.18 50.06 2 150.03 50.01 2
Proximal 25749.42 1597.09 1 10976.41 1075.62 1
VitreousDistal 266.35 80.85 2 90.15 30.05 2
Proximal 218.50 19.90 21 71.18 8.22 21

Episcleral Toptecan Chemoplaque Phase I–II Trial 19
0.9 mg Total Topotecan HCl 0.9 mg Lactone Topotecan
Tissue Location AUC (ng*day/mL)
Cmax (ng/mL)
Tmax (days)
AUC (ng*day/mL)
Cmax (ng/mL)
Tmax (days)
Plasma N/A Below LLOQ Below LLOQ
Below LLOQ
Below LLOQ
Below LLOQ
Below LLOQ
Aqueous N/A Below LLOQ Below LLOQ
Below LLOQ
Below LLOQ
Below LLOQ
Below LLOQ
Sclera*Distal 3478.14 214.28 21 690.355 36.71 14
Proximal 183221.30 19750.57 2 59133.35 6899.66 2
Choroid*Distal 3682.85 283.19 7 1560.79 166.23 7
Proximal 275148.59 39784.82 2 109849.45 21555.99 2
Retina*Distal 2585.04 159.28 14 865.38 87.32 7
Proximal 44149.00 2583.86 1 26170.91 2012.95 1
VitreousDistal 94.64 9.16 14 66.92 5.72 21
Proximal 764.82 51.64 21 153.77 10.21 21

Episcleral Toptecan Chemoplaque Phase I–II Trial 20
Figures. Ocular and plasma distribution of topotecan lactone after implantation of Episcleral Topotecan containing 0.3, 0.6, or 0.9 mg of topotecan HCl. Plasma concentrations < LLOQ. LLOQ for plasma and ocular tissues: 1 ng/ml or 1 ng/gram.

Episcleral Toptecan Chemoplaque Phase I–II Trial 21
5.0
Episcleral Toptecan Chemoplaque Phase I–II Trial 22
6.0 PILOT COMPASSIONATE USE Two patients have been treated with the Chemoplaque. Both were close to losing their last eye to retinoblastoma and the remaining treatment options were judged to be more dangerous to vision or to have serious lifelong implications of increasing second cancer risk to close to 50%. Each patient experienced no eye or systemic toxicity. Both eyes had a rapid regression of small volume disease. Both patients had recurrence of disease requiring further treatments at Day 135 and Day 110. At present time both eyes remain with good vision.
Patient ONE
A child with a constitutional RB1 gene pathogenic variant was diagnosed with both eyes stage1 cT2b (Group D murphree classification2) retinoblastoma. After 4 months treatment with systemic chemotherapy his left eye was removed because extensive refractory retinoblastoma threatened the optic nerve and choroidal invasion (Figure 1).
His right eye received systemic chemotherapy (2 different regimens, 8 total cycles, partial response, then recurrence) and intra-arterial chemotherapy (2 cycles, no response). After 8 months, there was still refractory multiply-recurrent extensive disease (Figures 1, 2). The large nasal tumor (paritally calcified, 6.5 mm elevation adjacent but not contiguous to the optic disc) showed growth of the main tumor in every direction with adjacent “greasy” vitreous seeds. Throughout the retina were 23–30 laser- and chemo-resistant tumors. The foveal pit was intact (excellent visual potential) but detached by new serous retinal detachment related to the active large nasal tumor. The only remaining conventional treatments were i) plaque radiotherapy, ii) external beam irradiation and iii) removal of his only eye.
Health Canada authorized the first human application compassionate use of the Chemoplaque.
A Chemoplaque (0.6mg Topotecan) was inserted in the inferonasal quadrant and glued to sclera on day 0. Blood tests and pain scores were normal (no pain). No local or systemic toxicities were observed. Vision improved by Day 12 (fóvea center of vision reattached). At examinations under anesthesia (EUAs) at days 12, 28, 42, 70 no ocular toxicity was detected. Vitreous seeds and all but one of the small retinal recurrent tumors disappeared by day 12; all disappeared by day 28 (Figure 3). The nasal calcified tumor showed shrinkage and on day 70 laser therapy to consolidate and flatten the surrounding tumor was started. Minimal superficial vitreous hemorrhage was seen over of the central mass shrinking-edge, that disappeared at day 70 and is more likely due to tumor necrosis than Chemoplaque toxicity.
The Chemoplaque was removed on Day 70, with no evidence of local toxicity. Ultarsound biomicroscopy showed normal scleral thickness where the chemoplaque had been placed (Figure 3). At day 98, there were no tumor recurrences and 20/80 vision.
On Day 135, the nasal calcified tumor showed tumor regrowth while the peripheral tumors remained scarred. At Day 156, the nasal calcified tumor continued growing and a ruthenium plaque was placed Day 175. The small tumors all remain scarred. At removal of the ruthenium plaque, vitreous seeds were noted and vitreous hemorrhage was evident partially obscuring fundus view, and vision decreased. On Day 185 intravitreal chemotherapy was given.
On Day 197 pars plana vitrectomy43 of vitreous blood and seeds was performed, in order to facilitate observation and focal treatment for recurrent tumor and control of vitreous seeds. Cytopathologic evaluation of the vitreous washout identified no tumor cells. Seven months after insertion of the Chemoplaque there has been no Chemoplaque-related toxicity. The small-volume multiply resistant tumors have not recurred. Vision is 20/100.

Episcleral Toptecan Chemoplaque Phase I–II Trial 23
Figure 1: DEPICT HEALTH graphic display of treatments since diagnosis of retinoblastoma in Patient One.
Figure 2: Retinoblastoma in right eye from Day 0 (Chemoplaque insertion), Day 98, and follow-up treatments (ruthenium plaque, vitectomy) related to Day 156 recurrence in calcified nasal tumor.

Episcleral Toptecan Chemoplaque Phase I–II Trial 24
Patient Two
This child had bilateral retinoblastoma, both eyes treated with systemic chemotherapy (2 different regimens, 10 total cycles, partial responses), IAC (2 cycles, non-responsive) and external beam irradiation therapy over one year (Figure 3). Four months later there was massive recurrence in both eyes. The right eye was removed.
The left eye had dispersed tumor recurrences with vitreous seeding and vitreoretinal fibrous proliferation. The fovea was detached with a serous retinal detachment. The tractional retinal detachment was covered with highly active retinoblastoma (Figure 4). There were no more conventional options for this last eye except removal of the child’s last eye. Health Canada authorized compassionate use of the Chemoplaque (0.6mg Topotecan)
On Day 0 the Chemoplaque was glued to sclera under conjunctiva. Blood tests and pain scores were normal (no pain). No local or systemic toxicities were observed. No ocular toxicity was noted under EUAs at any time.
Dispersed small tumors showed 50% reduction and marked reduction of vitreous seeds Day 28. No active-appearing tumors or seeds were visible by Day 48 and the fovea had re-attached. No signs of local or systemic toxicity were observed. Minimal superficial vitreous hemorrhage was seen over of the shrinking masses of tumor that disappeared by Day 48, perhaps related to tumor necrosis rather than chemoplaque toxicity. The Chemoplaque was removed at Day 77 (Figure 5). At day 103, there were no tumor recurrences vision 20/65. Day 110 pars plana vitrectomy with melphalan irrigation was performed to release the retinal traction. Although no active tumor was visible, the cytology from the vitrectomy fluid showed active retinoblastoma tumor clumps.
Figure 5: DEPICT HEALTH graphic display of treatments since diagnosis Patient Two.

Episcleral Toptecan Chemoplaque Phase I–II Trial 25
Figure 6: Recurrent retinoblastoma in left eye Patient Two on Day 0 (Chemoplaque insertion), and at removal on Day 77, but the pre-existing circumferential vitreous traction was increasing. The fovea remained attached and vitrectomy was done to reduce retinal traction Day 110.

Episcleral Toptecan Chemoplaque Phase I–II Trial 26
7.0 SCREENING AND STUDY ENROLLMENT PROCEDURES7.1 Inclusion Criteria
7.1.1 Primary therapy: Small volume active tumors (< 6mm in any dimension/tumor)
An eye with retinoblastoma classified as cT1b (IIRC group B) (location threatens fovea) in a child not receiving systemic chemotherapy for the other eye (bilateral or unilateral).
A unilateral cT2 (IIRC group C ) (visible optic nerve)7.1.2 Salvage therapy:
Any eye with refractory retinoblastoma that shows a visible optic disc, vision potential and no imminent risk for tumor spread.
7.1.3 Palliative therapy: for vision with incurable systemic retinoblastoma metastases
7.2 Exclusion Criteria7.2.1 Any eye with tumor touching the optic nerve rim. 7.2.2 Any suggestion of high-risk histopathology7.2.3 Reported allergy to topotecan, camptothecin or derivatives thereof.7.2.4 Eyes with spreading tumors:7.2.5 Extra-ocular extension into orbit or brain, or7.2.6 Metastatic retinoblastoma with or without CNS involvement, or7.2.7 Neuroimaging (MRI) showing suspicion of, or true optic nerve invasion.
7.3 Informed ConsentThe trial objectives, procedures and treatments (potential risks and complications, and alternative therapies) will be meticulously explained to the patient’s parents or guardian and a signed informed consent will be obtained according to institutional guidelines. A dated road map follow up schedule specific for the child will be presented to the parents and signed prior to enrollment. Upon signing necessary consent forms, a specific study screening number will be assigned to each patient.
7.4 Screening ProceduresDocumentation of the informed consent for screening will be maintained in the patient’s research chart. Studies or procedures that were performed for clinical indications (not exclusively to determine eligibility) may be used for baseline values even if the studies were done before informed consent was obtained. All clinical and laboratory studies to determine eligibility must be performed within 7 days prior to enrollment unless otherwise indicated. Before the patient can be enrolled, the responsible institutional investigator must sign and date the completed eligibility checklist.
8.0 Study EnrollmentPatients are cleared to be enrolled in the study once all eligibility requirements for the study have been met. The date protocol therapy is projected to start must be no later than fourteen (14) calendar days after the date the subject is cleared to be enrolled. Once enrolled, a patient-specific enrollment number will be assigned to each patient.

Episcleral Toptecan Chemoplaque Phase I–II Trial 27
9.0 TreatmentDay 0: Surgical chemoplaque insertion:
After performing a routine examination under anesthesia with emphasis on the intraocular pressure, Retcam imaging and any relevant imaging procedures (optical coherence tomography, ultrasound biomicroscopy or B-scan ultrasonography), the Chemoplaque will be inserted.
Under aseptic technique, an inferior 90° conjunctival periotomy will be performed. Depending on the chosen location for the Chemoplaque, inferior and medial / lateral recti will be identified and held by 4/0 silk threads for globe manipulation. The quadrant will be exposed and bare scleral clean of an hemorrhage will be prepared for the bed on the Chemoplaque.
The Chemoplaque will be held with the T-groove facing up and one drop of surgical glue will be applied to the groove only. The chemoplaque will be applied directly on the sclera in the exposed quadrant by placing the side opposite the glue on the dry sclera and gently lowering the Chemoplaque until the glue in the groove contacts the sclera. The Chemoplaque will be held in position on the sclera for 3 minutes without movement to ensure that it is being properly glued to the sclera. The conjunctiva is closed using 7/0 Vicryl sutures. A transparent eye shield will be applied for immediate postop protection in the recovery room.
Postoperative antibiotic/steroid eye drops will be prescribed for 2 weeks. No hospitalization is required and the child will be sent home. A pain chart will be provided to the parents to be filled.
Day 1 and 8:
Examine the child in the clinic to assess eye opening, lid swelling and vision if applicable.
Day 8, 21 and 35:
Examine in the oncology clinic for blood tests.
Day 15, 29, 50, 71:
EUA to assess tumor response and potential intraocular toxicity.
Days 50 or 71:
Plaque removal:
After performing a routine examination under anesthesia with emphasis on the intraocular pressure, Retcam imaging and any relevant imaging procedures (optical coherence tomography, ultrasound biomicroscopy or B-scan ultrasonography), the Chemoplaque will be removed.
Under aseptic technique, an inferior conjunctival periotomy will be performed. The quadrant where the Chemoplaque was inserted will be exposed and the anterior edge of the plaque will be identified and gently lifted off the globe. The conjunctiva is closed using 7/0 Vicryl sutures. Postoperative antibiotic/steroid eye drops will be prescribed for 2 weeks. No hospitalization is required and the child will be sent home.
The contents of the chemoplaque (if any left) will be studied for residual drug.
The chemoplaque removal will be removed earlier in the following situations:
Toxicity defined as grade 3 systemic or local. Tumor progression endangering tumor spread.
Post plaque follow up

Episcleral Toptecan Chemoplaque Phase I–II Trial 28
Following completion of protocol therapy, vital status and disease status will be followed based on routine clinical visits for a minimum of one year. At each follow up period, status of patients will be categorized:
Patient alive, no active disease Patient alive, active disease requires further interventions Patient died, related to the disease Patient died, not related to the disease
Outcome measures:
Tumor control Salvage rates
Data management:
Sample size Study coding Data storage Data analysis Statistics
Data CollectionThe complexity of retinoblastoma has defeated most attempts to conduct meaningful clinical trials.
References1 Mallipatna, A. et al. in AJCC Cancer Staging Manual Vol. 8th Edition (eds M. B. Amin,
S. B. Edge, & F. L. Greene) Ch. 68, 819-831 (Springer, 2017).
2 Murphree, A. L. Intraocular retinoblastoma: the case for a new group classification. Ophthalmology clinics of North America 18, 41-53 (2005).
3 Shields, C. L. et al. The International Classification of Retinoblastoma predicts chemoreduction success. Ophthalmology 113, 2276-2280, doi:10.1016/j.ophtha.2006.06.018 (2006).
4 Novetsky, D. E., Abramson, D. H., Kim, J. W. & Dunkel, I. J. Published international classification of retinoblastoma (ICRB) definitions contain inconsistencies--an analysis of impact. Ophthalmic Genet 30, 40-44, doi:908192764 [pii] 10.1080/13816810802452168 (2009).
5 Mallipatna, A., Dimaras, H., Héon, E. & Gallie, B. Published International Classification of Retinoblastoma (Icrb) Definitions Contain Inconsistencies: An Analysis of Impact. Evidence-Based Ophthalmology 10, 183-185, doi:10.1097/IEB.0b013e3181b93c45 (2009).
6 Dimaras, H. et al. Retinoblastoma. Nat Rev Dis Primers 1, 15021, doi:10.1038/nrdp.2015.21 (2015).
7 Mallipatna, A. C., Sutherland, J. E., Gallie, B. L., Chan, H. & Heon, E. Management and outcome of unilateral retinoblastoma. J AAPOS 13, 546-550, doi:S1091-8531(09)00308-5 [pii] 10.1016/j.jaapos.2009.09.004 (2009).

Episcleral Toptecan Chemoplaque Phase I–II Trial 29
8 Kletke, S., Zhao, X. F., Hazrati, L.-N., Gallie, B. L. & Soliman, S. E. Clinical predictors of low histopathologic risk features in unilateral cT2b (Group D) retinoblastoma. (Submitted, 2019).
9 Dimaras, H. et al. Retinoblastoma. Lancet 379, 1436-1446, doi:10.1016/S0140-6736(11)61137-9doi:10.1016/S0140-6736(12)61446-9 (2012).
10 Soliman, S. E., VandenHoven, C., MacKeen, L. D., Heon, E. & Gallie, B. L. Optical Coherence Tomography-Guided Decisions in Retinoblastoma Management. Ophthalmology 124, 859-872, doi:10.1016/j.ophtha.2017.01.052 (2017).
11 Suzuki, S., Yamane, T., Mohri, M. & Kaneko, A. Selective ophthalmic arterial injection therapy for intraocular retinoblastoma: the long-term prognosis. Ophthalmology 118, 2081-2087, doi:10.1016/j.ophtha.2011.03.013 (2011).
12 Abramson, D. H., Dunkel, I. J., Brodie, S. E., Kim, J. W. & Gobin, Y. P. A phase I/II study of direct intraarterial (ophthalmic artery) chemotherapy with melphalan for intraocular retinoblastoma initial results. Ophthalmology 115, 1398-1404, 1404 e1391, doi:S0161-6420(07)01359-0 [pii] 10.1016/j.ophtha.2007.12.014 (2008).
13 Yamane, T., Kaneko, A. & Mohri, M. The technique of ophthalmic arterial infusion therapy for patients with intraocular retinoblastoma. Int J Clin Oncol 9, 69-73 (2004).
14 Gobin, Y. P., Dunkel, I. J., Marr, B. P., Brodie, S. E. & Abramson, D. H. Intra-arterial chemotherapy for the management of retinoblastoma: four-year experience. Arch Ophthalmol 129, 732-737, doi:10.1001/archophthalmol.2011.5 (2011).
15 Peterson, E. C., Elhammady, M. S., Quintero-Wolfe, S., Murray, T. G. & Aziz-Sultan, M. A. Selective ophthalmic artery infusion of chemotherapy for advanced intraocular retinoblastoma: initial experience with 17 tumors. Journal of neurosurgery, doi:10.3171/2011.1.JNS10466 (2011).
16 Munier, F. L. et al. Occurrence of sectoral choroidal occlusive vasculopathy and retinal arteriolar embolization after superselective ophthalmic artery chemotherapy for advanced intraocular retinoblastoma. Retina 31, 566-573, doi:10.1097/IAE.0b013e318203c101 (2011).
17 Muen, W. J. et al. Efficacy and Complications of Super-selective Intra-ophthalmic Artery Melphalan for the Treatment of Refractory Retinoblastoma. Ophthalmology 119, 611-616, doi:10.1016/j.ophtha.2011.08.045 (2012).
18 Thampi, S. et al. Superselective intra-arterial melphalan therapy for newly diagnosed and refractory retinoblastoma: results from a single institution. Clin Ophthalmol 7, 981-989, doi:10.2147/OPTH.S43398 (2013).
19 Venturi, C. et al. Superselective ophthalmic artery infusion of melphalan for intraocular retinoblastoma: preliminary results from 140 treatments. Acta Ophthalmol 91, 335-342, doi:10.1111/j.1755-3768.2011.02296.x (2013).
20 Shields, C. L. et al. Intra-arterial chemotherapy for retinoblastoma in 70 eyes: outcomes based on the international classification of retinoblastoma. Ophthalmology 121, 1453-1460, doi:10.1016/j.ophtha.2014.01.026 (2014).
21 Taich, P. et al. Clinical pharmacokinetics of intra-arterial melphalan and topotecan combination in patients with retinoblastoma. Ophthalmology 121, 889-897, doi:10.1016/j.ophtha.2013.10.045 (2014).

Episcleral Toptecan Chemoplaque Phase I–II Trial 30
22 Parareda, A. et al. Intra-arterial chemotherapy for retinoblastoma. Challenges of a prospective study. Acta Ophthalmol 92, 209-215 (2014).
23 Ghassemi, F. & Amoli, F. A. Pathological findings in enucleated eyes after intravitreal melphalan injection. Int Ophthalmol 34, 533-540, doi:10.1007/s10792-013-9851-2 (2014).
24 Ong, S. J., Chao, A. N., Wong, H. F., Liou, K. L. & Kao, L. Y. Selective ophthalmic arterial injection of melphalan for intraocular retinoblastoma: a 4-year review. Japanese Journal Of Ophthalmology. 59, 109-117, doi:10.1007/s10384-014-0356-y (2015).
25 Francis, J. H. et al. Efficacy and Toxicity of Second-Course Ophthalmic Artery Chemosurgery for Retinoblastoma. Ophthalmology, doi:10.1016/j.ophtha.2014.11.029 (2015).
26 Shields, C. L. et al. Rescue intra-arterial chemotherapy following retinoblastoma recurrence after initial intra-arterial chemotherapy. Journal Francais D Ophtalmologie., doi:10.1016/j.jfo.2015.03.004 (2015).
27 Yousef, Y. A. et al. Intra-arterial Chemotherapy for Retinoblastoma: A Systematic Review. JAMA ophthalmology 134, 584-591, doi:10.1001/jamaophthalmol.2016.0244 (2016).
28 Kleinerman, R. A. et al. Variation of second cancer risk by family history of retinoblastoma among long-term survivors. Journal Of Clinical Oncology. 30, 950-957, doi:10.1200/JCO.2011.37.0239 (2012).
29 Temming, P. et al. Incidence of second cancers after radiotherapy and systemic chemotherapy in heritable retinoblastoma survivors: A report from the German reference center. Pediatr Blood Cancer 64, 71-80, doi:10.1002/pbc.26193 (2017).
30 Murphree, A. L. et al. Chemotherapy plus local treatment in the management of intraocular retinoblastoma. Archives of Ophthalmology 114, 1348-1356 (1996).
31 Soliman, S. et al. Precision laser therapy for retinoblastoma. Expert review of ophthalmology, 1-11, doi:10.1080/17469899.2018.1478729 (2018).
32 Berry, J. L. et al. Factors predictive of long-term visual outcomes of Group D eyes treated with chemoreduction and low-dose IMRT salvage: the Children's Hospital Los Angeles experience. Br J Ophthalmol 98, 1061-1065, doi:10.1136/bjophthalmol-2013-304411 (2014).
33 Munier, F. L. et al. First-line intra-arterial versus intravenous chemotherapy in unilateral sporadic group D retinoblastoma: evidence of better visual outcomes, ocular survival and shorter time to success with intra-arterial delivery from retrospective review of 20 years of treatment. Br J Ophthalmol, doi:10.1136/bjophthalmol-2016-309298 (2016).
34 Schmack, I., Hubbard, G. B., Kang, S. J., Aaberg, T. M., Jr. & Grossniklaus, H. E. Ischemic necrosis and atrophy of the optic nerve after periocular carboplatin injection for intraocular retinoblastoma. Am J Ophthalmol 142, 310-315, doi:10.1016/j.ajo.2006.02.044 (2006).
35 Mulvihill, A. et al. Ocular motility changes after subtenon carboplatin chemotherapy for retinoblastoma. Arch Ophthalmol 121, 1120-1124 (2003).
36 Mallipatna, A. C., Dimaras, H., Chan, H. S., Heon, E. & Gallie, B. L. Periocular topotecan for intraocular retinoblastoma. Arch Ophthalmol 129, 738-745, doi:10.1001/archophthalmol.2011.130 (2011).

Episcleral Toptecan Chemoplaque Phase I–II Trial 31
37 Murray, T. G. et al. Subconjunctival carboplatin therapy and cryotherapy in the treatment of transgenic murine retinoblastoma. Arch Ophthalmol 115, 1286-1290 (1997).
38 Munier, F. L. et al. Intravitreal chemotherapy for vitreous disease in retinoblastoma revisited: from prohibition to conditional indications. Br J Ophthalmol 96, 1078-1083, doi:10.1136/bjophthalmol-2011-301450 (2012).
39 Shields, C. L. et al. Intravitreal melphalan for persistent or recurrent retinoblastoma vitreous seeds: preliminary results. JAMA ophthalmology 132, 319-325, doi:10.1001/jamaophthalmol.2013.7666 (2014).
40 Aziz, H. A., Kim, J. W., Munier, F. L. & Berry, J. L. Acute Hemorrhagic Retinopathy following Intravitreal Melphalan Injection for Retinoblastoma: A Report of Two Cases and Technical Modifications to Enhance the Prevention of Retinal Toxicity. Ocul Oncol Pathol 3, 34-40, doi:10.1159/000448718 (2017).
41 Francis, J. H. et al. Risk of Extraocular Extension in Eyes With Retinoblastoma Receiving Intravitreous Chemotherapy. JAMA ophthalmology 135, 1426-1429, doi:10.1001/jamaophthalmol.2017.4600 (2017).
42 Pascual-Pasto, G. et al. Therapeutic targeting of the RB1 pathway in retinoblastoma with the oncolytic adenovirus VCN-01. Sci Transl Med 11, doi:10.1126/scitranslmed.aat9321 (2019).
43 Zhao, J. et al. Pars Plana Vitrectomy and Endoresection of Refractory Intraocular Retinoblastoma. Ophthalmology 125, 320-322, doi:10.1016/j.ophtha.2017.10.015 (2018).