006 - wilson wbh molpath for jdw final - laboratory home dna symposiu… · – liposarcoma 16.5%...
TRANSCRIPT

10/16/2014
1
Molecular Pathology of Soft Tissue Sarcomas
Jon D. Wilson, MD
Disclosures
• Nothing to disclose.
Goals
• Soft tissue sarcomas– Background
– General principles of sarcomagenesis
• Selected examples to illustrate:– Molecular pathogenesis
– Molecular diagnostic techniques• Clinical utility
• Advantages
• Disadvantages
Soft tissue sarcoma• Uncommon tumors:
– ~1% of all cancers (all ages)– ~15% of cancers in childhood and adolescence (<20 y/o)
• Lifetime risk:– 1 out of 350 people
• Annual incidence, all ages (U.S. SEER data 2005‐2009): – Soft tissue and bone: 12,000 ‐ 15,000 new cases/year
– Undifferentiated pleomorphic sarcoma 30.2%– Liposarcoma 16.5%– Leiomyosarcoma 13.7%– Fibrosarcoma 6.3%– Synovial sarcoma 5%– Rhabdomyosarcoma 4.3%– Dermatofibrosarcoma protuberans 3.2%– Myxosarcoma 0.8%– Alveolar soft part sarcoma 0.5%– Other 19.5%
• 850‐900 new cases/year in children and adolescents (<20 y/o)– ~50% are rhabdomyosarcoma
Sarcomahelp.orgSEER.cancer.gov
• Self‐sufficiency in growth signals
• Insensitivity to growth‐inhibitory signals
• Evasion of programmed cell death
• Limitless replicative potential
• Sustained angiogenesis
• Tissue invasion and metastasis
Cancer “defined”
Hanahan D and Weinberg RA. The hallmarks of cancer. Cell 2000;100:57‐70
Sarcoma versus carcinoma
• Similar “cancer” criteria for sarcoma…..but• Multistep tumorigenesis seen in epithelial neoplasia (carcinomagenesis) has been more difficult to document– Example: translocation associated sarcomas
• No pre‐neoplastic cell identified• Translocation may be the only genetic alteration; sufficient for the development of mesenchymal cancer
• Cell type specificity appears to be important in sarcomagenesis– Same translocation may be found in different tumors

10/16/2014
2
Mesenchymal stem cells (MSC)• Mouse MSCs undergo spontaneous tumorigenic transformation after long
term ex‐vivo culture– This does not happen with human MSCs
• Transformation can also be induced by inserting fusion genes, targeted gene mutations, drug or chemical treatment– Human MSCs are more reluctant to transform than mouse MSCs
• Specific tumor types appear to depend not only on the pathway targeted, but also the tissue of origin
• Recent evidence suggests a perivascular cell (PVC) origin for MSCs– In long term culture human PVC
• Display stem cell markers and markers of their tissue of origin• Do not display endothelial, hematopoietic or myogenic markers• Under proper culture conditions, PVCs can differentiate into adipocytes, chondrocytes or
osteocytes
Crisan M, et al. A perivascular origin for mesenchymal stem cells in multiple human organs. Cell Stem Cell 2008;3:301‐313Rodriguez R, et al. Modeling sarcomagenesis using multipotentmesenchymal stem cells. Cell Res 2012;22:62‐77
Chondrocytes
Adipocytes
Osteocytes
MSC
potency
Stem cell
Committed progenitors
Mature MSC derivatives
Differentiation impairment Oncogenic hit A1 Oncogenic hit A2 Oncogenic hit A3 Oncogenic hit A4
Oncogenic hit B1
Oncogenic hit B2
Oncogenic hit B4
Sarcoma differentiation
Proliferationanti‐Apoptosis
Oncogenic hit B3
Rodriguez R, et al. Cell Res 2012;22:62‐77
DevelopmentalMesenchymalCompartment
Classification of gene mutations
• Driver mutations– Directly or indirectly confer a selective growth advantage to the cell in which it occurs
• Passenger mutations– No direct or indirect effect on the selective growth advantage of the cell in which it occurs
Vogelstein B, et al. Cancer Genome Landscapes. Science 2013;339:1546‐1558
Classification of cancer genes
• Mechanistic classification– Tumor suppressor genes
• Deactivation: deactivating mutation, deletion, or reduced expression
– Oncogenes• Activation: activating mutation or amplification
– Caretaker genes• More likely to develop mutation(s) in tumor suppressor genes or oncogenes
• Functional classification– Protein kinases
• Can function as oncogenes or tumor suppressor genes
– Transcription factors• Can function as oncogenes or tumor suppressor genes
– DNA maintenance and repair proteins• Caretaker genes
Molecular classification of soft tissue sarcomas
1. Variable & complex abnormal karyotype 50%– Spindle cell/pleomorphic sarcoma, NOS– Leiomyosarcoma– Myxofibrosarcoma– Pleomorphic liposarcoma– Pleomorphic rhabdomyosarcoma– Other
2. Reciprocal translocations 15‐30%– Ewing sarcoma (EWSR1‐FLI1)– Synovial sarcoma (SS18‐SSX)– Other
3. Specific mutations– Gastrointestinal stromal tumors (KIT & PDGFRA activating mutations)– Other
4. Amplifications– Well‐differentiated liposarcoma/atypical lipomatous tumor (12q13‐15 ring
chromosome; MDM2)– Other
Guillou L, et al. Soft tissue sarcomas with complex genomic profiles. Virch Arch 2010;456:201‐217Fisher C. Soft tissue sarcomas with non‐EWS translocations: molecular genetic features and pathologic and clinical correlations. Virch Arch 2010;456:153‐166Jain S, et al. Molecular classification of soft tissue sarcomas and its clinical applications. Int J Clin Exp Pathol 2010;3:416‐429
Why test?
• Potential type(s) of information obtained:
– Diagnostic: Aid in rendering a morphologic diagnosis
– Prognostic: Educated guess at a tumor’s behavior without the influence of treatment
– Predictive: Response of tumor to therapy

10/16/2014
3
Method Advantages Disadvantages
CytogeneticsDNA
Global viewPrimary and secondary abnormalities identified
Does not require knowledge of abnormality or diagnosisMay detect abnormalities not seen by FISH or PCR
Requires fresh tissue (dividing cells)Low resolution
Cryptic rearrangementsLower sensitivitySlower TAT
FISHDNA or RNA
More targeted viewRequires prior knowledge of abnormality or diagnosisDiagnostically specific and sensitiveModerate resolutionModerate analytic sensitivityMultiple tissue types can be used
FFPE, frozen, cytology or cultured cells (FISH or iFISH)Can localize abnormality to specific cellsFaster TAT
Need for fluorescence microscopeSignals fadeDoes not work on decal tissue
RT‐PCR(reverse transcriptase)RNA
High resolution (very targeted view)High sensitivity and specificity, and quantifiable (MRD)Multiplexing possibleCan use FFPE, frozen sections, cytology, or freshFaster TAT
Requires knowledge of abnormalityDoes not work on decal tissueFFPE may have degraded RNAPCR inhibitors
IHCProtein
Can use FFPE, frozen sections or cytologyMorphologic correlationRapid TATRelatively inexpensiveMutation specific antibodies available
Interlab variablility
NGSDNA or RNA
High throughput (huge multiplex capability)High resolution (individual nucleotide level)
Cost of equipment (decreasing)Need and cost of bioinformatics
MRI: Large 10.5 x 8.7 x 6.5 cm lobulated extraperitoneal mass in the posterolateral mid and upper right abdomen, showing heterogeneous enhancement and multiple enhancing septations surrounding nodular areas with variable degrees of enhancement. It displaces the adjacent liver medially and the outer layer of adjacent thoracic/abdominal wall musculature laterally. It surrounds portions of the lower right ribs, and appears to be arising from the lower aspect of the intercostal muscles, suggesting a sarcoma.
• 17 y/o female, 30 weeks pregnant, presenting with right flank pain.
CD99
NSECD45, CD20, CD3, desmin, and myogenin
Image from Dr. Mark Micale, William Beaumont Hospital, Royal Oak, MI
• Ewing sarcoma/Primitive NeuroectodermalTumor (ES/PNET)
– Lung and bone metastases present
• Delivered healthy 33‐week‐old baby
• Treated
Diagnosis:

10/16/2014
4
ES/PNET
• Definition:
– Malignant small round blue cell sarcoma with variable neuroectodermal differentiation as assessed by light microscopy, immunohistochemistry, and EM
• Recurrent translocations:– EWSR1 22q12 fusions with a variety of fusion partners (promiscuous)
• EWSR1‐FLI1 t(11;22)(q24q12) 85‐90%
• EWSR1‐ERG t(21;22)(q21;q12) 5‐10%
• Other
Reciprocal translocations in sarcomas
• RNA‐binding protein genes
– FUS, EWSR1, TAF15 (FET family of genes)
• Receptor tyrosine kinase (RTK) genes
– ALK
• Growth factor genes
– PDGFB
• Other
– SS18 (formerly SYT)
General principles of translocations
• Frequency of specific translocations appears to be a random event related to gene size, average intron length, length of longest intron– Exons comprise only 1‐2% of human genome
– Recombinogenetic DNA sequences not more frequent in commonly translocated genes
• Additional factors: – Accessibility of DNA for rearrangement (open/actively transcribed > close/silent)
– Proximity in nucleus (nuclear domains)
• Because translocations occur within introns (now, “not so junk DNA”)– Difficult to detect due to variability of break points using PCR for DNA
• Because RNA splicing joins chimeric mRNA exons– Easier to detect with RT‐PCR (cDNA) due to more consistent splicing of exons
Exons 1 2 3 4 5 6 7
http://static.wikidoc.org/6/6e/PLoSBiol3.5.Fig1bNucleus46Chromosomes.jpg
Ewing sarcoma breakpoint region 1 (EWSR1)
• RNA‐binding protein– FET (TET) family of RNA‐binding proteins FUS(TLS), EWSR1
(EWS), and TAF15(TAFII68)• N‐term activation domain (SYGQQS hexanucleotide repeat domain)
– serine, tyrosine, glycine, glutamine, glutamine, serine
• RNA‐binding domain (RRM: RNA recognition motif)• RG‐rich regions (arginine‐glycine‐glycine)• Cys2‐Cys2 Zinc finger nucleic acid binding site
• Locates predominantly in nucleus; shuttles to cytoplasm– Nucleolus and coiled body
• Functions– RNA transcription– mRNA processing (splicing)– DNA repair
Splicing
Transport
Stability
Transcription
Translation
RNAPolymerase
Pol‐II
DNA
pre‐mRNA
Ribonucleoproteins
mRNA decay
Nucleus Cytoplasm
RNA‐bindingprotein
RNA‐binding proteins
Key components of RNA metabolism
Regulate all aspects of RNA biogenesis• Maturation
• Surveillance
• Nucleocytoplasmic transport
• Translation
• Degradation

10/16/2014
5
ES/PNET• Native FLI1 transactivating domain (TAD) tightly regulated and lineage restricted• Native EWSR1 TAD is strongly and broadly activated
• EWSR1‐FLI1 fusion ‐> unrestricted high level expression of the fusion gene product– Structurally heterogeneous
• Up to 18 possible in‐frame chimeric transcripts• Two main types (85‐90%)
– Type 1: EWSR1 exon 7 fused to FLI1 exon 6– Type 2: EWSR1 exon 7 fused to FLI1 exon 5– Fusions always contain intact EWSR1 exons 1‐7 (TAD) and intact FLI1 exon 9 DNA‐binding domain– Type 1 fusions initially reported to show somewhat better survival than other types
• Other genetic alterations involving cell progression and apoptosis are commonly present (25%) and define a subset of more aggressive chemoresistant tumors– p16/p14ARF (CDKN2A gene)– p53 (TP53 gene)
Cytogenetic and molecular genetic pathology of soft tissue tumors. In Enzinger & Weiss’s Soft Tissue Tumors. 5th Ed. Mosby Elsevier 2008; pages 73‐102
AtlascytogeneticsoncologyKovar H. Sarcoma 2011
N‐terminus C‐terminusFusion region
R7BD: RPB7‐binding domainDHR: Degenerate hexanucleotide repeat domain (serine‐tyrosine‐glycine‐glutamine‐rich (SYGQQS)ZFM1: IQ binding domain (binds calmodulin)RGG1, 2 and 3: Arginine/Glycine/Glycine rich areasRRM: RNA recognition motifZF: Zinc finger domainNLS: Nuclear localization signal
EWSR1 protein
R7BD DHR ZFM1(IQ) RGG1 RRM RGG2 ZF RGG3 NLSEWS activation domain RNA‐binding domain
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17
Breakpoint region in intron 7
EWSR1 (22q12.2)
Exon
Fusion partner’s DNA‐binding domain
EWSR1‐fusion partner oncoprotein
ES/PNET translocations
• EWSR1‐FLI1 t(11;22)(q24q12) ~90%– EWSR1 exons 7 to 11 fused to FLI1 exons 3 to 8– Usually EWSR1 exons 7 or 8 fused to FLI1 exons 5 or 6
• Type 1: EWSR1 exon 7 to FLI1 exon 6 (51%)• Type 2: EWSR1 exon 7 to FLI1 exon 5 (27%)
• EWSR1‐ERG t(21;22)(q21;q12) ~5%• EWSR1‐ETV1 t(7;22)(p22;q12)• EWSR1‐ETV4 t(17;22)(q21;q12) <1%• EWSR1‐FEV t(2;22)(q36;q12)
• FUS‐ERG t(16;21)(p11;q22) <1%• FUS‐FEV t(2;16)(q35;p21) rare
EWSR1 (22q12)
PBX1 (1q23)METERG (21q21)
ES/PNET/Other
PATZ1 (22q12)Undiff ES‐like
NFATC2 (20q13)Undiff ES‐like
ETV4 (17q21)ES/PNET
DDIT3 (12q13)M/RCLS
ATF1 (12q13)CCS/AFH/Other
ZNF384 (12p12)AL FLI1 (11q24)
ES/PNETWT1 (11p13)
DSRCT
NR4A3 (9q22)EMCS
ETV1 (7p22)ES/PNET
POU5F1 (6p21)HidradenomaMEC/Other
DUX4 (4q35)RMS
FEV (2q36)ES/PNET
CREB1 (2q34)CCS/AFH
SP3 (2q31)Other
Huret JL, et al. EWSR1, partners, and tumours. 2010
AFH: Angiomatoid fibrous histiocytomaAL: Acute leukemiaCCS: Clear cell sarcomaDSRCT: Desmoplastic small round cell tumorEMCS: Extraskeletal myxoid chondrosarcomaES/PNET: Ewing sarcoma/PNETMET: Myoepithelial cell tumorM/RCLS: Myxoid/round cell liposarcomaRMS: RhabdomyosarcomaUndiff ES‐like: Undifferentiated Ewing sarcoma‐like
Image from Dr. Mark Micale, William Beaumont Hospital, Royal Oak, MI
*
Ch 11 Ch 22
t(11;22)(q24;q12)
der(11)
der(22)
FLI111q24
EWSR122q12

10/16/2014
6
Image from Dr. Mark Micale, William Beaumont Hospital, Royal Oak, MI
*
FISH dual color break apart probe for EWSR1
Ch 11 Ch 22
t(11;22)(q24;q12)
der(11)
der(22)
FLI111q24
EWSR122q12
3’‐EWSR1 – 5’‐FLI1 fusion
5’‐EWSR1 ‐ 3’‐FLI1 fusion*
FISH dual color break‐apart probe for EWSR1 rearrangement (in this case with FLI1)
Image from Dr. Mark Micale, William Beaumont Hospital, Royal Oak, MI
Image from Dr. Mark Micale, William Beaumont Hospital, Royal Oak, MI
t(11;22)(q24;q12)Ch 22
der(11)
der(22)
Ch 11
5’‐EWSR1 ‐ 3’‐FLI1 fusion*
FLI111q24
EWSR122q12
3’‐ EWSR1 – 5’‐FLI1 fusion
FISH dual‐color dual‐fusion probe for EWSR1‐FLI1 fusion

10/16/2014
7
RT‐PCR for EWSR1‐FLI1 fusions
1 2 3 4 5 6 7 6 7 8 9
EWSR1‐FLI1 t(11;22)(q24;q22)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17
EWSR1 22q12
breakpoint region
1 2 3 4 5 6 7 8 9
FLI1 11q24
breakpoint region
*
**
1 2 3 4 5 6 7 6 7 8 9
EWSR1‐FLI1 t(11;22)(q24;q22)
1 2 3 4 5 6 7 6 7 98
EWSR1
FLI1
1 2 3 4 5 6 7 6 7 98
EWSR1
FLI1
8 9 10 11 543
1 2 3 4 5 6 7 6 7 98
EWSR1
Other fusion partner
1 2 3 4 5 6 7 6 7 98
EWSR1
Other fusion partner
8 9 10 11 543
100bp ladder
Patient
Positive ctrl
Negative ctrl
RT‐PCR for EWSR1‐FLI1 fusions
Ewing sarcoma/PNET
• Utility of molecular diagnostics:– Diagnosis
– Minimal residual disease detection (MRD)
• Differential diagnosis:– Rhabdomyosarcoma
– Poorly differentiated synovial sarcoma t(X;18)(p11.2;q11.2) SS18‐SSX
– Lymphoblastic lymphoma
– Metastatic neuroblastoma
– Myxoid/round cell liposarcoma t(12;16)(q13;p11) FUS‐DDIT3, other
– Mesenchymal chondrosarcoma t(8;8)(q21;q13)/del(8)(q21‐q13) ) HEY1‐NCOA2
– Small cell osteosarcoma
– Ewing sarcoma‐like t(4;19)(q35;q13) CIC‐DUX4, other
Sampling
Fusion
Non‐ES/PNET sarcomas with EWSR1 rearrangements
• Desmoplastic small round cell tumor (DSRCT)– t(11;22)(p13;q12) EWSR1‐WT1 >95%
• Myxoid liposarcoma– t(12;16)(q13;p11) FUS‐DDIT3 >90%
– t(12;22)(q13;q12) EWSR1‐DDIT3 <10%
• Extraskeletal myxoid chondrosarcoma– t(9;22)(q22;q12) EWSR1‐NR4A3 75%
– t(9;17)(q22;q11) TAF15‐NR4A3 15%
• Clear cell sarcoma– t(12;22) (q13;q12) EWSR1‐ATF1 90%
– t(2;22)(q33;q12) EWSR1‐CREB1 10%
• Angiomatoid fibrous histiocytoma– t(2;22)(q34;q12) EWSR1‐CREB1 72%
– t(12;22)(q13;q12) EWSR1‐ATF1 21%
– t(12;16)(q13;p11) FUS‐ATF1 7%
Undifferentiated round cell sarcoma (Ewing sarcoma‐like)
• Definition: – Recently described highly aggressive undifferentiated round cell
sarcoma of children and young adults, morphologically similar to Ewing sarcoma/PNET but lacking fusions between EWSR1 and ETS (E‐twenty‐six) family of DNA binding transcription factors (FLI1, ERG, ETV1, ETV4, and FEV).
• Epidemiology:– Incidence: Rare– Age: children and young adults (median 24 years; range 6‐62)– Sex: slight male predominance [M:F = 1.4:1]
• Clinical:– Location:
• Superficial soft tissue– Extremities (50%)– Trunk– Head and neck
Kawamura‐Saito M, et al. Fusion between CIC and DUX4 up‐regulates PEA3 family genes in Ewing‐like sarcomas with t(4;19)(q35;q13) translocations. Hum Mol Genet 2006;15:2125‐2137Specht K, et al. Distinct transcriptional signature and immunoprofile of CIC‐DUX4 fusion‐positive round cell tumors compared to ESSR1‐rearranged Ewing sarcomas: Further evidence
toward distinct pathologic entities. Genes Chrom Canc 2014;7:622‐633
• Genetics:– Recurrent translocations between EWSR1 and a non‐ETS family genes
• NFATC2 (nuclear factor of activated T‐cells, cytoplasmic, calcineurin dependent 2) 20q13.2
– t(20;22)(q13;q12) EWSR1‐NFATC2» Activates some downstream targets similar to ETS family members
• PATZ1 (POZ [BTB] and AT hook containing zinc finger 1– inv(22)(q12q12) EWSR1‐PATZ1
– Recurrent translocations between non‐FET and non‐ETS families of genes• CIC (capicua transcriptional repressor) 19q13• DUX4 (double homeobox 4) 4q35 & 10q26 (two copies in the human genome!)
– t((4;19)(q35‐q13) CIC‐DUX4– t(10;19)(q26;q13) CIC‐DUX4
• BCOR (BCL6 co‐repressor) Xp11.4• CCNB3 (cyclin B3)
– inv(X)(p11.4p11.22) BCOR‐CCNB3 (paracentric inversion)
Kawamura‐Saito M, et al. Fusion between CIC and DUX4 up‐regulates PEA3 family genes in Ewing‐like sarcomas with t(4;19)(q35;q13) translocations. Hum Mol Genet 2006;15:2125‐2137Specht K, et al. Distinct transcriptional signature and immunoprofile of CIC‐DUX4 fusion‐positive round cell tumors compared to ESSR1‐rearranged Ewing sarcomas: Further evidence
toward distinct pathologic entities. Genes Chrom Canc 2014;7:622‐633
Undifferentiated round cell sarcoma (Ewing sarcoma‐like)

10/16/2014
8
• Pathology
– Microscopic:
• Small round blue cell tumor
• Immunohistochemistry (CIC‐DUX4 tumors)
– Positive membranous staining for CD99 (86%)
– Positive nuclear staining for WT1 and FLI1 (100%) and ERG (18%)
– Absence of EWSR1 rearrangement with FISH
Specht K, et al. Distinct transcriptional signature and immunoprofile of CIC‐DUX4 fusion‐positive round cell tumors compared to EWSR1‐rearranged Ewing sarcomas: Further evidence toward distinct pathologic entities. Genes Chrom Canc 2014;7:622‐633
Undifferentiated round cell sarcoma (Ewing sarcoma‐like)
MRI T2
MRI T1
MRI T1
2 y/o male with soft tissue mass in proximal right forearm. He underwent biopsy, followed by neoadjuvent chemotherapy and radical resection.
Cytokeratin AE1/3
BCL2 CD99
Image from Dr. Mark Micale, William Beaumont Hospital, Royal Oak, MI Image from Dr. Mark Micale, William Beaumont Hospital, Royal Oak, MI

10/16/2014
9
Synovial sarcoma (SS)• Definition:
– Sarcoma with variable epithelial differentiation. May arise at any site, and despite its name does not arise from or differentiate towards synovium.
• Recurrent translocations:– t(X;18)(p11.2;q11.2) SS18‐SSX
• SSX1 & SSX2 (synovial sarcoma X breakpoints 1 & 2)– Only 13 amino acids difference (homology: 81% nucleic acid; 78% aa)
• SS18 (synovial sarcoma translocation, chromosome 18)– SS18‐SSX1 biphasic 35‐50%– SS18‐SSX2 biphasic <10% (reported more favorable prognosis)– SS18 to SSX4 rare
– Differ in that neither SSX or SS18 (SYT) have DNA‐binding domains; appear to be transcriptional regulators working through protein‐protein interactions (favored to be housekeeping genes, but exact function is unknown)
Biphasic
Monophasic spindle cell
Monophasic with HPC‐like vessels
Poorly differentiated
Spindle (SFT‐like)
Other (adenomatoid)
S100 protein
• Malignant spindle cell neoplasm, favor metastatic melanoma
• FISH which had been previously ordered, returns positive for SS18 rearrangement, consistent with synovial sarcoma
Diagnosis:
Synovial sarcoma, poorly differentiated, lung primary Synovial sarcoma, poorly differentiated, lung primary

10/16/2014
10
Synovial sarcoma CD99 BCL2
S100 protein EMA
Synovial sarcoma TLE‐1
Synovial sarcoma (SS)
• Utility of molecular diagnostics:– Diagnosis
• Differential diagnosis:– Poorly differentiated (small round blue cell tumor)
• Ewing sarcoma/Primitive neuroectodermal tumor• Rhabdomyosarcoma• Neuroblastoma• Cellular solitary fibrous tumor (hemangiopericytoma)• Mesenchymal chondrosarcoma• Lymphoblastic lymphoma
– Biphasic• Carcinosarcoma• MPNST with glandular differentiation
– Monophasic fibrous• Fibrosarcoma• Leiomyosarcoma• Cellular solitary fibrous tumor (hemangiopericytoma)• Malignant peripheral nerve sheath tumor (MPNST)• Spindle cell carcinoma• Malignant peripheral nerve sheath tumor
– Monophasic epithelial• Carcinoma
TLE1
Extragastrointestinal stromal tumor (EGIST)• Description:
– Spindle cell proliferation arising from gut wall, with phenotypic features of interstitial cell of Cajal. Spectrum of biologic behavior from benign to malignant. They are the most common mesenchymal tumor of the gastrointestinal tract. A small number of GISTs arise from mesentery, omentum, or retroperitoneum and show no connection with the gut (EGISTs).
• Recurrent mutations:– Activating mutations of receptor tyrosine kinase
• KIT 70‐80%
• PDGFRA 5‐8%
Mutually exclusive
– Other 12‐15%• SDH
• BRAF
• HRAS
• NRAS
• KIT is expressed in >95% of GISTs, including those without KIT or PDGFRA mutations.
GIST spindle
CD117 (cKIT)
GIST epithelioid
CD117 (cKIT)

10/16/2014
11
kit oncogene KIT (AKA CD117)• Member of type III receptor tyrosine kinase (RTK) family
– Other members: PDGFRA, CSF1R, and FLT3
• Critical to normal development & function of interstitial cells of Cajal
• Also involved in hematopoiesis, gametogenesis, and melanogenesis.
• Activating KIT mutations identified in multiple tumors: seminomas, mast cell tumors, acute myelogenous leukemia, and melanoma.
Platelet derived growth factor‐alpha (PDGFRA)• RTK closely related to KIT (homologue)
• PDGFRA mutated GISTs– Tend to arise in stomach, have epithelioid morphology, variable to
absent KIT IHC staining, and more indolent behavior
Gastrointestinal stromal tumor (GIST)
• KIT and PDGFRA mutated GISTs– Sporadic = Majority (solitary tumors)– Familial = Rare (often multiple tumors and background ICCH)
• Wild‐type GISTs (no KIT or PDGFRA mutations identified)– 10% of adult GISTs and 85% of pediatric GISTs– Most are associated with hereditary syndromes
• Neurofibromatosis type 1 (NF1)• Carney triad (CT): SDHA, SDHB, SDHC, SDHD deficient (mutation unknown)• Carney‐Stratakis syndrome (CSS): SDHA, SDHB, SDHD germline mutations• Hereditary paraganglioma/pheochromocytoma syndrome (HPGL/PCC):
germline mutations of SDHA, SDHB, SDHC, SDHD
– BRAF V600E in 13% of cases – HRAS– NRAS
TK1
TK2
TK1
TK2
Stem cell factor
Extracellular domain5 Ig‐like loops
Juxtamembrane domain
Transmembrane domain
Tyrosine kinase #1(ATP binding)
Tyrosine kinase #2Phosphotransferase
P
P
P
P
TK1
TK2
TK1
TK2
PDGFs PDGFs
P
P
P
P
KIT Ch 4q12
PDGFRACh 4q12
Stem cell factor
Modified from Lasota J & Miettinen M. Clinical significance of oncogenic KIT and PDGFRA mutations in gastrointestinal stromal tumors. Histopathology 2008;53:245‐266
YY
Y Y
YY
Y Y
Exon 8Exon 9 (~9%)
Exon 11 (~70%)
Exon 13
Exon 14
Exon 15
Exon 16
Exon 17
Exon 12
Exon 14
Exon 18 (~8%)
most frequent
ReceptorRegulatorydomains
Enzymaticdomains
Evolved from common ancestral gene?Signaling cascade:1) Ligand binding2) Receptor dimerization3) Phosphorylation of tyrosine residues4) Leads to activation downstream signaling
‐RAS/RAF/MEK/ERK‐PI3K/AKT‐STAT
COOH
NH2
Asp842ValResistant to imatinib*
*Respond well to imatinib
Gene mutation Frequency Site Familial
KIT 75‐80%
Exon 8 Rare Small bowel One kindred
Exon 9 insertion AY502‐503 10% Small bowel & colon None
Exon 11 (del, sub, ins) 67% All sites Several kindreds
Exon 13 K642E 1% All sites Two kindreds
Exon 17 D820Y, N822K and Y823D 1% All sites Five kindreds
PDGFRA 5‐8%
Exon 12 (such as V561D) 1% All sites Two kindreds
Exon 14 N659K <1% Stomach None
Exon 18 D842V 5% Stomach, mesentery & omentum None
Exon 18 (ex: del IMHD p.842‐846 IMHD)
KIT & PDGFR wild‐type 12‐15%
BRAF V600E ~7‐15%
SDHA, SDHB, SDHC, SDHC ~2% Stomach & small bowel Carney‐Stratakis
HRAS or NRAS <1%
Sporadic pediatric ~1% Stomach Not heritable
Carney triad with GISTs ~1% Stomach Not heritable
NF1 with GISTs Rare Small bowel Numerous
Corless C, et al. Gastrointestinal stromal tumours: origin and molecular oncology. Nature Reviews Cancer 2011;11:865‐878
imatinib
imatinib mesylate for GIST
• Imatinib mesylate is a selective tyrosine kinaseinhibitor (TKI) whose targets included KIT, PDGFRA, PDGFRB and ABL
– Partial or stable response in 80% of patients
– Complete lasting responses are rare
• ~ 50% of initial responders develop drug resistance
– Most commonly a second KIT mutation in the kinase domain
– Disrupts imatinib binding by stabilizing the receptor in a constitutively active formATP
TYR
Substrate
KIT
Exon 13
Exon 14
Exon 17
Exon 18
Secondary KIT mutations
Mutations imatinib sunitinib sorafenib nilotinib
V654A Resistant Sensitive Sensitive Intermediate
T670I Resistant Sensitive Sensitive Resistant
D816A/G/H/V Resistant Resistant Resistant Resistant
D820A/E/G/Y Resistant Resistant Sensitive Unknown
N822H/K Intermediate Resistant Sensitive Resistant
Y823D Resistant Resistant Unknown Unknown
A829P Intermediate Resistant Unknown Unknown
Modified from: Corless C, et al. Gastrointestinal stromal tumours: origin and molecular oncology. Nature Reviews Cancer 2011;11:865‐878

10/16/2014
12
Modified from :RiemenschneiderMJ & Reifenberger G. Molecular Neuropathology of Gliomas. Int J Mol Sci 2009;10:184‐212
MDM4
p53
p21waf1
p15INK4b
p16INK4a
p15INK4c
MDM2
p14ARF
RAS
PTEN PI3K
AKT
RB1E2F
Cell proliferation
Apoptosis
RAS signalingRB signaling
p53 signaling PTEN/PI3K/AKT pathway
Cdk4 and Cdk6
Cyclin D
ALK
OTHERNF1
RAF
MEK
ERK
PDK1
mTOR
RB1
E2F
‐P03
Growth factorreceptor signaling
TSC1
TSC2
EGFR
KIT
PDGFRA
SDH in GIST• Multi‐subunit complex of nuclear encoded genes • Component of mitochondrial Krebs cycle and ETS• Inactivating mutations affect global epigenomicmethylation pattern– Failure in DNA methylation maintenance (hypermethylation)– Succinate accumulation inhibits TET2 dioxygenase which converts 5‐MC to 5‐hMC (initial step in demethylation)
– Similar to IDH1/2 in gliomas– Can use IHC to detect SDH‐null GISTs (SDHA & SDHB) and decrease in 5‐hMC
• SDH mutant GISTs have more stable genomes– Do not have the numerous chromosomal gains and losses (CNVs) seen in KIT and PDGFR GISTs
Janeway KA, et al. Defects in succinate dehydrogenase in gastrointestinal stromal tumors lacking KIT and PDGFRA mutations. Proc Natl Acad Sci USA 2011;108:314‐318Killian JK, et al. Succinate Dehydrogenase Mutation Underlies Global Epigenomic Divergence in Gastrointestinal Stromal tumors. Canc Disc 2013; June Epub
Malzkorn B, et al. Unraveling the Glioma Epigenome – From Molecular Mechanisms to Novel Biomarkers andTherapeutic Targets. Brain Pathology 2011;21:619‐632
Succinate
Fumarate
FADFADH2
SDHWT
TET2 5‐methylcytosine dioxygenase:5‐hydroxymethylcytosineCIMP (hypermethylation)
SDHmut
INACTIVATING/LOSS OF FUNCTIONMUTATIONS
Krebs cycle and electrontransport chain (ETS)
SDHA 5p15SDHB 1p36.1‐p35SDHC 1q23.3SDHD 11q23
Gastrointestinal stromal tumor (EGIST)
• Utility of molecular diagnostics:
– Diagnosis
– Prognostic (specific mutations)
– Predictive (targeted therapy available)
• Differential diagnosis:
– Spindle cell and epithelioid neoplasms, including:
• Schwannoma
• Leiomyoma
• Leiomyosarcoma
Well‐differentiated and de‐differentiated liposarcoma (WDLPS & DDLPS)
• Definition:– Locally aggressive sarcoma showing variably‐developed
adipocytic differentiation, variation in cell size, nuclear atypia, and variable numbers of lipoblasts. Morphology categorized into adipocytic, sclerosing, spindle cell and inflammatory subtypes.
– May progress to de‐differentiated liposarcoma (low & high grade)• Retroperitoneal tumors >20%• Limbs <2%
• Recurrent genetic abnormality:– Amplification of 12q13‐15 within ring and/or supernumerary
chromosomes• Potential oncogenes
– MDM2, CDK4, HMGA2, TSPAN31, OS1, OS9, CHOP and GLI1– Most evidence for MDM2, CDK4, HMGA2, TSPAN31
• MDM2 most consistently amplified (99%)

10/16/2014
13
Well‐differentiated liposarcoma
Dedifferentiated liposarcoma
High grade dedifferentiated liposarcoma p16 IHC
Image from Dr. Mark Micale, William Beaumont Hospital, Royal Oak, MI
Atlasgeneticsoncology.orgZhang H, et al. Am J Surg Path 2010;34:1304‐1311Bridge J, et al. Molecular Diagnostics of Soft Tissue Tumors. 2011;135:588‐601
metaphase FISHMDM2 SOCDK4 SG
Interphase FISHMDM2 SOCEP SG
Giant marker/supernumerary chromosome
Ring chromosome
MDM2 oncogene, E3 ubiquitin protein ligase
• Ch 12q14.3‐q15
• Negative regulator of p53
–Negative feedback loop:
• Elevated p53 levels activate MDM2 transcription
• MDM2
–Binds to transcriptional activating domain of p53, blocking p53 dependent transcription
–Acts as a ubiquitin ligase, targeting p53 for degradation
Modified from :RiemenschneiderMJ & Reifenberger G. Molecular Neuropathology of Gliomas. Int J Mol Sci 2009;10:184‐212
MDM4
p53
p21waf1
p15INK4b
p16INK4a
p15INK4c
MDM2
p14ARF
RAS
PTEN PI3K
AKT
RB1E2F
Cell proliferation
Apoptosis
RAS signalingRB signaling
p53 signaling PTEN/PI3K/AKT pathway
Cdk4 and Cdk6
Cyclin D
PDGFRA
ALK
OTHERNF1
RAF
MEK
ERK
PDK1
mTOR
RB1
E2F
‐P03
Growth factorreceptor signaling
TSC1
TSC2
EGFR
KIT

10/16/2014
14
Well‐differentiated and de‐differentiated liposarcoma (WDLPS & DDLPS)
• Utility of molecular diagnostics:– Diagnosis
• Differential diagnosis:– Lipoma
– Pleomorphic sarcoma infiltrating adipose tissue
– Normal adipose tissue
– Fat necrosis
– Atrophy of fat
– Localized massive edema
Summary• Molecular diagnostics can provide diagnostic, prognostic and predictive types of information in the clinical work‐up of soft tissue sarcomas.
• Each method has its own strengths and weaknesses.
• Appropriate triage of tissue while the specimen is fresh allows for potential access to the full array of diagnostic testing.
Summary• The field of molecular diagnostics is rapidly evolving, both in the area of new methodologies and discovery of recurrent genetic abnormalities in cancer.
• Molecular testing will increasingly become standard of care with further development and availability of targeted therapies.
• Immunohistochemical methods to detect protein products of chimeric gene fusions or mutated genes can provide a cost effective way to screen for well‐characterized genetic alterations in the setting of cancer.
IHC screening for genetic alterations and/or downstream pathway activation
• FLI1 for EWSR1‐FLI1 in Ewing/PNET• ERG for EWSR1‐ERG in Ewing/PNET• WT1 for EWSR1‐WT1 in DSRCT• TFE3 for ASPL‐TFE3 in alveolar soft part sarcoma (overexpression of c‐terminal
TFE3)• ALK in inflammatory myofibroblastic tumors• β‐Catenin for fibromatosis (nuclear localization)• SMARCB1 (INI1) for malignant rhabdoid tumors and epithelioid sarcoma (loss
of normal nuclear staining)• MDM2, cdk4, and p16 in atypical lipomatous tumor/well‐differentiated
liposarcoma and dedifferentiated liposarcoma (amplification and overexpression)
• STAT6 for NAB2‐STAT6 in solitary fibrous tumor (nuclear localization)
• AP2‐beta and P‐cadherin for alveolar rhabdomyosarcoma (overexpression)• TLE1 as a screen for synovial sarcoma (overexpression)
– Sensitive but not specific for synovial sarcoma
• MUC4 as a screen for low grade fibromyxoid sarcoma (overexpression)
Suggestions• Submit tissue for cytogenetic analysis. You can always cancel the testing, and incur only the charge for setting up the culture.
• Make air dried cytology preparations of tumor samples prepared at the time of frozen section and/or the grossing of fresh tissue. They are easier and faster to process, avoid the problem of nuclear truncation inherent to FISH performed on paraffin block tissue, and provide excellent quality DNA and/or RNA for molecular testing modalities.
• In the setting of partially bony or mineralized tissue, consider submitting non‐decalcified tissue for processing into FFPE to preserve DNA and RNA integrity to allow for possible later genetic testing.
?Thank you.

10/16/2014
15
Case 1MRI COR T1 FSE MRI COR STIR FSE
38 y/o male with left calf mass; initial core biopsy performed
Core biopsy CD99Core biopsy
FLI1TLE1
• Core biopsy diagnosis:
– Limited sample of small round blue cell tumor with background myxoid stroma.
– Comment:
• Suspect Ewing sarcoma
• Additional sampling suggested.
Excisional biopsy specimen

10/16/2014
16
p53
KI‐67
Excisional biopsy specimen
• Excisional biopsy diagnosis:
– Myxoid/round cell liposarcoma.
• DDIT3 rearrangement identified by FISH
• p53 positive; tend to behave more aggressively
– TLE1 reactivity reported in other tumors within differential diagnosis for small round blue cell tumor, including myxoid/round cell liposarcoma, and rhabdomyosarcoma.
Kosemehmetoglu K, Vrana JA, and Folpe AL. TLE1 expression is not specific for synovial sarcoma: a wholesection study of 163 soft tissue and bone neoplasms. Mod Pathol 2009;22:872‐878
Myxoid/round cell liposarcoma (MLPS/RCLPS)
• Definition:– Malignant sarcoma comprised of monotonous non‐lipogenic cells, variable numbers of small signet‐ring cell‐like lipoblasts, and branching “chicken‐wire” capillaries in a background myxoid stroma.
• Recurrent translocations– t(12;16)(q13;p11) FUS‐DDIT3 (CHOP) 95%
• Type 1: FUS exon 7 to DDIT3 exon 2 20%• Type 2: FUS exon 5 to DDIT3 exon 2 65%• Type 3: FUS exon 8 to DDIT3 exon 2 10%
– t(12;22)(q13;q12) EWSR1‐DDIT3 5%
• Secondary alterations – p53 mutations sometimes present and are associated with more aggressive behavior
Myxoid liposarcoma Round cell liposarcoma
Image from Dr. Mark Micale, William Beaumont Hospital, Royal Oak, MI Image from Dr. Mark Micale, William Beaumont Hospital, Royal Oak, MI

10/16/2014
17
Myxoid/round cell liposarcoma (MLPS/RCLPS)
• Utility of molecular diagnostics:
– Diagnosis
• Differential diagnosis:
– Extraskeletal myxoid chondrosarcoma t(9;22)(q22;q12) EWSR1‐NR4A3
– Myxofibrosarcoma (low grade myxoid MFH)
– Ewing sarcoma/primitive neuroectodermal tumor t(11;22)(q24;q12) EWSR1‐FLI
– Rhabdomyosarcoma
– Poorly differentiated synovial sarcoma t(X;18)(p11.2;q11.2) SS18‐SSX
– Myxoid well‐differentiated liposarcomas of the retroperitoneum
Return
Case 2
CT without and with contrast
23 y/o female with sinus mass 23 y/o female with sinus mass
MRI T1 FLASH SAG
MRI T1 FLASH COR MRI TSE AX FS
Extraskeletal mesenchymal chondrosarcoma CD99
BCL2 CD56
PAS PASd

10/16/2014
18
Resection specimen
• Definition:– Malignant biphasic tumor characterized by components of
undifferentiated small round blue cells and islands of relatively well‐differentiated hyaline cartilage. Soft tissue primary site seen in about 20% to 35% of case.
• Recurrent translocation:– t(8;8)(q21;q13)/del(8)(q21‐q13) HEY1‐NCOA2
– 10Mb apart– HEY1 exon 4 to NCOA2 exon 13
• HEY1 (hairy/enhancer‐of‐split related with YRPW motif 1– DNA‐binding domain– Downstream effector of NOTCH pathway
• NCOA2 (nuclear receptor coactivator 2)– Member of p160 nuclear hormone transcriptional co‐activator family– Transcriptional activation domains (AD1/CID and AD2) recruit histone acetyltransferases
and histone methyltransferases to specific enhancer/promoter regions, thereby facilitating chromatin remodeling and transcription of nuclear receptor target genes
– NCOA2 fusions identified in other tumors» MYST3‐NCOA2 inv(8)(p11q13) rare AML subset» ETV6‐NCOA2 t(8;12)(q13;p13) few ALL cases» PAX3‐NCOA2 t(2;8)(q35;q13) rare alveolar rhabdomyosarcoma
Wang L, et al. Identification of a Novel, Recurrent HEY1‐NCOA2 Fusion in Mesenchymal Chondrosarcoma Based on a Genome‐wide Screen of Exon‐level Expression Data. Genes Chromosomes & Cancer 20132;51:127‐139
Extraskeletal Mesenchymal Chondrosarcoma (EMCS)
Extraskeletal Mesenchymal Chondrosarcoma (EMCS)
• Utility of molecular diagnostics:– Diagnosis
• Differential diagnosis:– Ewing sarcoma/PNET t(11;22)(q24;q12) EWSR1‐FLI1
– Poorly differentiated synovial sarcoma t(X;18)(p11.2;q11.2) SS18‐SSX
– Extraskeletal chondrosarcoma
– Neuroblastoma
– Rhabdomyosarcoma
– Cellular solitary fibrous tumor (hemangiopericytoma)
– Small cell osteosarcoma
Return
Case 3
Clear cell sarcoma (CCS)
• Definition:– Soft tissue sarcoma with melanocytic differentiation, typically arising in tendons and
aponeuroses of young adults.
• Recurrent translocation:– t(12;22)(q13;q12) EWSR1‐ATF1 (90% soft tissue tumors; 10% GI tract)
• ATF1 (activating transcription factor‐1)– Member of bZIP transcription factors, which includes cAMP‐response‐element‐binding protein (CREB1)– RNA‐binding domain of EWSR1 replaced by a basic DNA binding and leucine zipper dimerization (bZIP) DNA
binding domain of ATF1.– Variation in fusion
» Type 1: EWSR1 exon 8 joined to ATF1 exon 4» Type 2: EWSR1 exon 7 joined to ATF1 exon 5» Type 3: EWSR1 exon 10 joined to ATF1 exon 5» Some cases express two different fusion transcripts derived from same fusion gene
– t(2;22)(q33;q12) EWSR1‐CREB1 (10% soft tissue tumors; 90% GI tract)• CREB1 (cAMP responsive elements binding protein 1• Common theme: Closely related gene family members can substitute for each as translocation
partners• This translocation appears to preferentially be present in CCS in gastrointestinal locations
– Relationship to melanoma?• Different tumors
– CCS lacks BRAF– Melanomas do not have EWSR1‐ATF1 or EWSR1‐CREB1 fusions
Clear cell sarcoma

10/16/2014
19
Angiomatoid fibrous histiocytoma (AFH)
• Definition:– Proliferation of histiocyte‐like cells, with multiple areas of cystic hemorrhage and chronic inflammation. Typically occurs in children and young adults. Excellent clinical prognosis after surgical excision.
• Recurrent translocations:– EWSR1 or FUS rearrangements
• EWSR1‐CREB1 t(2;22)(q34;q12) most common (72%)• EWSR1‐ATF1 t(12;22)(q13;q12) (21%)• FUS‐ATF1 t(12;16)(q13;p11) least common (7%)
– EWSR1 (EWS‐RNA‐binding protein 1)– FUS (Fused In Sarcoma)– CREB1 (cAMP Responsive Element Binding protein 1)– ATF1 (Activating Transcription Factor‐1)
Angiomatoid fibrous histiocytoma (AFH)
• Same EWSR1‐CREB1 and EWSR1‐ATF1 fusions also seen in:
– Clear cell sarcoma (CCS) of soft tissue
– Clear cell sarcoma‐like tumor of gastrointestinal tract (CCSLGT)
– Hyalinizing clear cell carcinoma of salivary gland
*Same translocation > different tumors!Related to specific site of mesenchymal stem cells and/or
epithelial tumor initiating cells?
Case
• Nineteen‐year‐old female, recurrent 3.7 cm right forearm soft tissue mass within the muscle. Re‐resection performed.
Angiomatoid Fibrous Histiocytoma
Angiomatoid Fibrous Histiocytoma
1 2 3 4 5 6 7 8 9
CREB1Chr 2q34
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17
EWSR1Chr 22q12
ATF1Chr 12q13 1 2 3 4 5 6 7
CCS Type 3CCS Type 2CCS Type 1
Clear cell sarcoma of tendon and aponeurosis
Least common in CCS‐soft tissue (10%); most common in CCS‐GI tract (90%)

10/16/2014
20
1 2 3 4 5 6 7 8 9
CREB1Chr 2q34
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17
EWSR1Chr 22q12
ATF1Chr 12q13 1 2 3 4 5 6 7
FUSChr 16p311 1 2 3 4 5 6 7CCS Type 2
Most common in AFH (72%); also seen in CCS (least common)
Angiomatoid fibrous histiocytoma (AFH)
• Utility of molecular diagnostics:
– Diagnosis
• Differential diagnosis:
– Melanoma
– Other melanin producing lesions
Clear cell sarcoma (CCS)
• Utility of molecular diagnostics:
– Diagnosis
• Differential diagnosis:
– Reactive process
Angiomatoid Fibrous Histiocytoma (AFH)
Case 4 Solitary fibrous tumor (SFT)
• Definition:– Fibroblastic sarcoma with morphologic spectrum ranging classical SFT
to hemangiopericytoma (HPC)/cellular SFT with hemangiopericytomatous blood vessels. Originally described as arising from lung pleura, but now known to have wide tissue distribution.
• Recurrent translocation:– NAB2‐STAT6 inv(12)(q13q13.3)
• Intrachromosomal inversion • NAB2 (NGFI‐A binding protein 2 [EGR1 binding protein 2]) 12q13.3
– Transcriptional repressor of zinc‐finger transcription factors EGR1 and EGR2
• STAT6 (signal transducer and activator of transcription 6, interleukin ‐4 induced ) 12q13
– Modulates IL4 and IL13 signaling
• Hypothesized that the fusion protein:– Homodimerization through NAB2 oligomerization domain– Translocates to nucleus to modulate STAT6‐dependent transcription
– Can detect by STAT6 IHC nuclear staining
Chmielecki J, et al. Whole‐exome sequencing identifies a recurrent NAB2‐STAT6 fusion in solitary fibrous tumors. Nature Genetics 2013; 45:131‐132Schweizer L, et al. Meningeal hemangiopericytoma and solitary fibrous tumors carry the NAB2‐STAT6 fusion and can be diagnosed by nuclear expression of STAT6 protein. Acta Neuropath 2013;125:651‐658
Solitary fibrous tumor Cellular solitary fibrous tumor (previously HPC)

10/16/2014
21
BCL2
CD99
CD34 CD34
NAB2 STAT6
NAB2 STAT6
Ch 12q13
Intact STAT6NAB2 Exonsvar I: 1‐4var II: 1‐7var III: 1‐3var IV: 1‐6
NAB2
WT
NAB2‐STAT6
Modified from: Chmielecki J, et al. Whole‐exome sequencing identifies a recurrent NAB2‐STAT6 fusion in solitary fibrous tumors. Nature Genetics 2013; 45:131‐132
Solitary fibrous tumor (SFT)
• Utility of molecular diagnostics:
– Diagnosis
• Differential diagnosis:
– Meningioma
– Synovial sarcoma
– Other fibroblastic tumors
Case 5Myxoinflammatory fibroblastic sarcoma (MIFS), Hemosideroticfibrolipomatous tumor (HFLT), and Pleomorphic hyalinizing
angiectatic tumor (PHAT) spectrum of tumors
• Definition:– MIFS (AKA inflammatory myxohyaline tumor of dital extremities with virocyte or Reed‐
Sternberg‐like cells; acral myxoinflammatory fibroblastic sarcoma): Rare low‐grade sarcoma with predilection for sub‐cutaneous tissue of distal extremities and propensity for local recurrence, but low likelihood of metastasis. Multinodular, poorly circumscribed lesion with alternating myxoid and fibrohyaline stroma, spindle to epithelioid cells, variable numbers of Reed‐Sternberg‐like cells with prominent nucleoli mimicking intranuclear viral‐inclusions (virocytes), and patchy prominent inflammatory infiltrate.
– HFLT: Rare low‐grade sarcoma with predilection for sub‐cutaneous tissue of middle‐aged women. Predominantly adipose, with admixture of bland fibroblastic spindle cells, multinucleate giant cells, lymphoid aggregates, and hemosiderin deposits. Resembles “early PHAT”. Initially interpreted as reactive in nature. Propensity for local recurrence, but not metastasis.
– PHAT: rare low‐grade sarcoma with predilection for superficial soft tissue of distal extremities. Lobulated growth pattern, scattered clusters of thin‐walled ectatic fibrin containing blood vessels and circumferential stromal hyalinization which emanate to trap pleomorphic stromal cells with prominent nucleoli. Early‐PHAT: Peripheral bland spindle cells infiltrate surrounding adipose tissue with some myxoid stromal change. Propensity for local recurrence, but not metastasis.
– Some “hybrid cases”

10/16/2014
22
MRI SAG T2 FSE fat sat MRI SAG T1 FSE
USR14‐512 MIFS HFLT63 y/o female with 4.0 x 3.7 x 1.4 cm left knee mass, T1 isointense, high T2 signal
USR14‐512 Myxoinflammatory fibroblastic sarcoma (MIFS) /hyalinizing fibrolipomatous tumor (HFLT)
USR14‐512 MIFS/HFLT USR14‐512 MIFS/HFLT
USR14‐512 MIFS/HFLT USR14‐512 MIFS/HFLT
10/16/2014
23
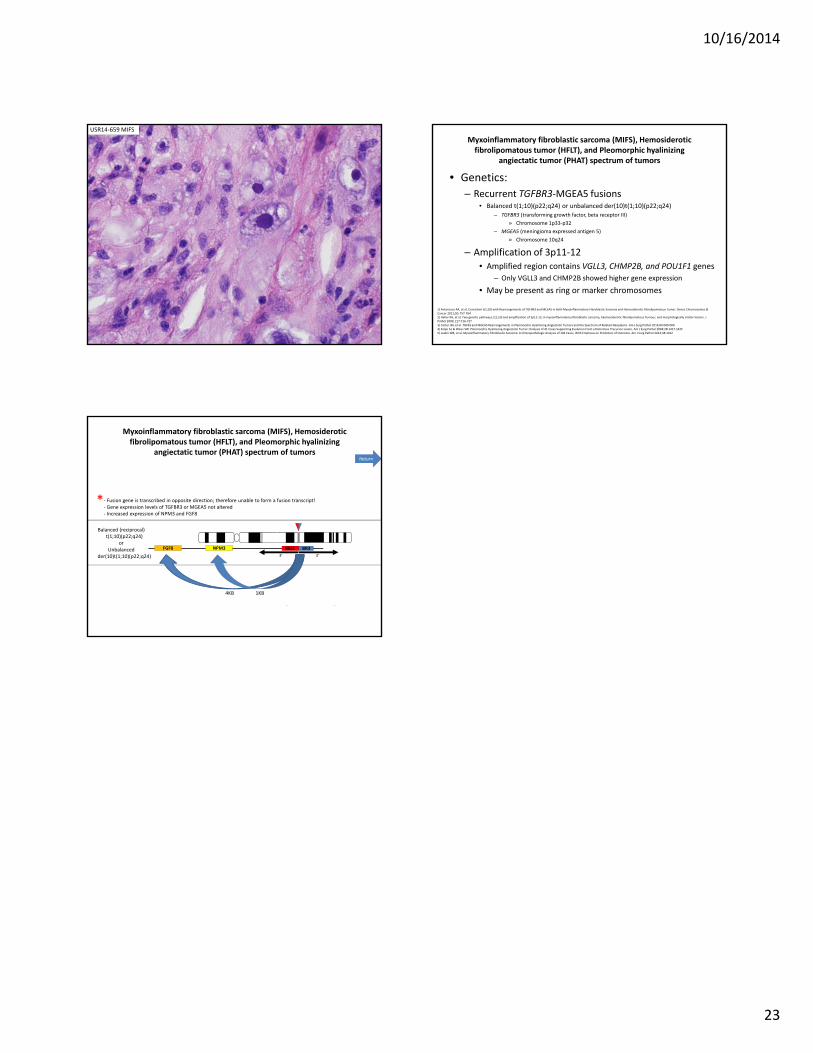
USR14‐659 MIFS
• Genetics:
– Recurrent TGFBR3‐MGEA5 fusions• Balanced t(1;10)(p22;q24) or unbalanced der(10)t(1;10)(p22;q24)
– TGFBR3 (transforming growth factor, beta receptor III)
» Chromosome 1p33‐p32
– MGEA5 (meningioma expressed antigen 5)
» Chromosome 10q24
– Amplification of 3p11‐12
• Amplified region contains VGLL3, CHMP2B, and POU1F1 genes
– Only VGLL3 and CHMP2B showed higher gene expression
• May be present as ring or marker chromosomes
1) Antonescu RA, et al. Consistent t(1;10) with Rearrangements of TGFBR3 and MEEA5 in Both Myxoinflammatory Fibroblastic Sarcoma and Hemosiderotic Fibrolipomatous Tumor. Genes Chromosomes & Cancer 2011;50: 757‐7642) Hallor KH, et al. Two genetic pathways, t(1;10) and amplification of 3p11‐12, in myxoinflammatory fibroblastic sarcoma, haemosiderotic fibrolipomatous Tumour, and morphologically similar lesions. J Pathol 2009; 217:716‐7273) Carter JM, et al. TGFB3 and MGEA5 Rearrangements in Pleomorphic Hyalinizing Angiectatic Tumors and the Spectrum of Related Neoplasms. Am J Surg Pathol 2014;00:000‐0004) Folpe AL & Weiss SW. Pleomorphic Hyalinizing Angiectatic Tumor: Analysis of 41 Cases Supporting Evolution From a Distinctive Precursor Lesion. Am J Surg Pathol 2004;28:1417‐14255) Laskin WB, et al. Myxoinflammatory Fibroblastic Sarcoma: A Clinicopathologic Analysis of 104 Cases, With Emphasis on Predictors of Outcome. Am J Surg Pathol 2014;38:1012
Myxoinflammatory fibroblastic sarcoma (MIFS), Hemosideroticfibrolipomatous tumor (HFLT), and Pleomorphic hyalinizing
angiectatic tumor (PHAT) spectrum of tumors
TGFGR3 (transforming growth factor, beta receptor III) Chr 1p33‐p32
MGEA5 (meningioma expressed antigen 5) Chr 10q24
TGFBR3
MGEA5NPM3FGF83’ 5’
Chr 1
Chr 10
3’ 5’
Balanced (reciprocal)t(1;10)(p22;q24)
orUnbalanced
der(10)t(1;10)(p22;q24)
MGENPM3FGF8
3’
BR3
3’
‐ Fusion gene is transcribed in opposite direction; therefore unable to form a fusion transcript! ‐ Gene expression levels of TGFBR3 or MGEA5 not altered‐ Increased expression of NPM3 and FGF8
*
1KB4KB
Myxoinflammatory fibroblastic sarcoma (MIFS), Hemosideroticfibrolipomatous tumor (HFLT), and Pleomorphic hyalinizing
angiectatic tumor (PHAT) spectrum of tumorsReturn