03 otong pages - delmarlearning.com
TRANSCRIPT
33
CHAPTER OUTLINE
Integration of Brain and Behavior
Kindling
Trauma
Major Paradigms of Psychiatric-Mental HealthNursing
Clinical and Practice Issues
Nursing Interventions
Psychiatric Nursing Education
The Role of the Nurse
The Generalist Nurse
The Advanced-Practice Psychiatric Registered Nurse
Related Research
History of the Biological-BehavioralDichotomy
Major Neurobiological Models
The Central Nervous SystemNeurodegenerative ProcessesNeurochemical Processes
Neuroendocrinology
Psychoneuroimmunology
GeneticsTwin, Adoption, and Family StudiesEnvironmental FactorsGenetics and AddictionGenetic Research
Major Behavioral Models
63
Interfacing Biological-
Behavioral Concepts into
Psychiatric Nursing PracticeDeborah Antai-Otong, MS, RN, CNS, PMHNP, CS, FAANMargaret Brackley, PhD, RN, CS

64 U N I T O N E Perspectives and Principles
CompetenciesUpon completion of this chapter, the learner should be able to:
1. Identify major paradigms of mental disorders.2. List major aspects of the central nervous system
and its relationship to mental disorders.3. Describe the role of genetics in the predisposi-
tion of mental disorders.4. Discuss brain function and its impact on human
behavior.
5. Understand the human response to acute andchronic stress.
6. Explain the interrelationships between mind,brain, and hormones.
7. Develop a plan of care using biological andbehavioral interventions.
Key TermsAmygdala: A nucleus in the limbic system or medialtemporal lobe that affects neuroendocrine andbehavioral functions. It also plays a role in behaviors,including eating, drinking, and sexuality, and theemotions linked to these behaviors. It plays a role inthe emotional significance of events or memoriesand governs the level of hippocampal activity accord-ingly. Consequently, a traumatic or overwhelmingevent is permanently etched into the memory,whereas irrelevant events are immediately ignored.
G-proteins: Part of the cell’s second messenger system in the plasma involved in sending signalsfrom regulatory chemicals such as hormones andneurotransmitters to target cells.
Genetic Vulnerability: The relationship betweengenetic and enzymatic defects and vulnerability tomental illness. Genetic function is influenced by pre-natal and environmental factors that activate intri-cate biochemical processes and affect behavior. Anumber of researchers have attempted to explorethe relationship between genetic factors and mentaldisorders using twin, adoption, and family studies.
Hippocampus: Located in the medial temporal lobe,it is an important site for the formation and storage ofimmediate and recent memories, and it is influencedby the amygdala emotional rating of an event. Thispart of the brain is damaged by Alzheimer’s disease.
Hypothalamus: Combined with the pituitary gland,thyroid gland, adrenal glands, gonads, and the pan-creas, the hypothalamus forms the major regulatorysystem and is involved in the biological aspects ofbehavior. The hypothalamus-pituitary-adrenal axis(HPA) is important in understanding certain mentaldisorders. The hypothalamus regulates autonomic,endocrine, and visceral integration and is surmisedto be the foundation of the limbic system and the
brain center for emotions and certain behaviors such as eating, drinking, aggression, and sexuality.Information in the hypothalamus is modulated by ascending sensory pathways, hormones, anddescending pathways of the cerebral cortex.
Kindling: The electrophysiological process that overtime produces an action potential after repetitivesubthreshold stimulation or progressive sensitizationof a neuron. This concept is thought to play a role in recurrent mood disorders.
Neuroendocrinology: The study of how the neuraland endocrine systems work together to maintainhomeostasis. Communication between these systems is involved in biological and behavioralresponses. Major organs of the neuroendocrine system are the hypothalamus, the pituitary, thyroid,and adrenal glands; the gonads; and the pancreas.
Protein Kinase C (PKC): A group of enzymes thatactivate other enzymes.
Psychoneuroimmunology: The study of the role ofthe immune system in health and illness in the faceof biological and psychosocial stress. This field is adeveloping knowledge about the interconnectednessof the nervous system and the immune system.
Reinforcers: Personal, complex, learned, and bio-chemical rewards that are used to modify maladap-tive behavior. Reinforcers can be positive, negative,or punishing, and are personally determined.
Twin Studies: Researchers attempt to explore therelationship between genetic factors and mental disorders using these studies that usually includemonozygotic or single ovum and dizygotic or two ova twins. Twin studies are helpful in isolatinggenetic and environmental influences and determin-ing preventive and precipitating factors.

When the U.S. Congress proclaimed the 1990s to bethe “Decade of the Brain,” the families of mentally
ill clients welcomed this new perspective of mental disor-ders. In the past, parents and siblings were thought to beresponsible for many mental illnesses, during which timeclinicians sought to explain these disorders solely in abehavioral context. As a consequence, family members feltdemoralized and were blamed for their loved one’s ill-nesses. Recently, however, neurobiological and geneticresearch findings have helped clinicians and researchersbegin to understand the biological component of mental illness, particularly in terms of brain function and dysfunc-tion, genetics, immunology, and endocrinology. Clients,families, and mental health professionals are hopeful aboutthe potential impact of neurobiological studies on mental ill-nesses. These studies are also likely to improve quality oflife and provide possible cures for serious mental disorders(U.S. Congress, 1989).
Advances in neurobiology and neuroendocrinologyreflect the sweeping biotechnological findings of brain map-ping, imaging, and scanning. Studies have demonstrated theunderlying biological bases of schizophrenia, bipolar dis-order and other mood disorders, anxiety disorders, dementia,and the aging process. Likewise, the use of psycho-pharmacologic agents has produced remarkable results,such as decreased side effects, decreased exacerbation ofsymptoms, improved quality of life, and increased treatmentadherence in clients with severe schizophrenia, bipolar dis-order, pervasive developmental disorder, depression, andanxiety disorders.
More importantly, advances in neurobiology and neuro-science offer unprecedented opportunities for the expan-sion and strengthening of the scientific underpinnings ofmental health research. Presently, researchers are usingmolecular and genetic mechanisms to identify genes and proteins that give rise to mental illness. They are also discovering that they can modify these neurobio-logical alterations by using psychopharmacologic and environmental interventions. These data provide novel targets for the development of pharmacologic agents andpsychotherapies for mental disorders. They also affordclients with a plethora of interventions (Hyman, 1998;NIMH, 1998).
Many symptoms or behaviors observed in people withmental illness are linked to underlying biological factors.Disturbances in mood, cognitions, sensory-perceptualresponses, aggression and other impulse control, and socialinteractions are examples of behaviors that have beenlinked to biological abnormalities or disruption.
The purpose of this chapter is to explore major conceptsof the biological-behavioral interface and its impact on psy-chiatric nursing practice. The chapter also identifies clientoutcomes from nursing interventions that meet the complexneeds of the mentally ill.
HISTORY OF THEBIOLOGICAL-BEHAVIORALDICHOTOMYNovel expansion of neurobiological technology emphasizesthe need to explain the biological-behavioral phenomenaand its relationship to mental illness. The interrelatedness ofbiology and behavior is not a new concept. It has its begin-nings as far back as the fourteenth century stemming fromthe works of Hippocrates, who explained the concept ofmental illness as a process of the brain rather than a spiri-tual event. He surmised that the brain gave rise to pleasure,joy, sorrow, pain, and grief and contributed to disturbancesin affect or mood. Although his early description of the ten-uous balance of four humors (blood, phlegm, and yellowand black bile) and their relationship to mood disordersproved inaccurate, his premise that maladaptive behaviorsarise from complex biological processes was accurate.
In more recent times, Sigmund Freud contributed to neu-robiology in the late 1800s through the phase of his workknown as the neurological phase. Freud sought to establisha relationship between neural mechanisms, behavior pat-terns, and cognitive distortions. Freud and others sought tounderstand psychopathology in relation to disturbances ofspecific areas of brain dysfunction. Ultimately, this work hasled to the recent plethora of neurobiological research anddiscoveries.
The search for the ideal treatment for mental illnessfound a major breakthrough in the discovery of tranquiliz-ers in the 1950s. These agents relieved clients with variedsymptoms of mental illness such as intense anxiety, agita-tion, delusions, and hallucinations. Some of the tranquiliz-ing agents uncovered during this era included thephenothiazines, such as chlorpromazine (Thorazine), thefirst of the medications that was effective in treating behav-ioral manifestations of schizophrenia. Other tranquilizersinduced major behavioral and biological changes in thementally ill, thus generating further clues to the biologicalaspects of mental illness.
Newer psychotropics have emerged since the 1950s thathave proven effective in the treatment of various mental dis-orders, such as schizophrenia and mood, anxiety, andaddictive disorders (see Chapter 28, PsychopharmacologicTherapy). Over the past decade the effectiveness of theseagents has increased because of improvements made intheir ability to target behavioral manifestations of the com-plex neurobiological processes, such as those located in thehypothalamus and other regions in the limbic system.Psychotropics appear to act on neurochemical mechanismsthat modify or alter or interfere with behavioral patterns.Examples include selective serotonergic reuptake blockingagents such as fluoxetine (Prozac) and sertraline (Zoloft),which are used to treat major depression, eating, impulsiv-ity, and anxiety disorders, and atypical neuroleptics such as
C H A P T E R 3 Interfacing Biological-Behavioral Concepts into Psychiatric Nursing Practice 65

clozapine (Clozaril) and quetiapine (Seroquel), which areused to treat schizophrenia. Research and trial studies havedrastically reduced the disabling side effects of some ofthese agents and have improved the quality of life and pro-vided hope and relief for clients and their families. Geneticand genome research offer even greater hope for clients byidentifying the phenotypes for mental disorders and furtherlinking behavior, brain, and genetics and providing molecu-lar targets for more effective therapies (Cowan, Kopnisky, &Hyman, 2002)
MAJOR NEUROBIOLOGICALMODELSTo understand the neurobiological models of mental ill-nesses and their implications for nursing, one must be famil-iar with the structure and function of the central nervoussystem (CNS) and its neurochemical processes. One alsoneeds some basic knowledge of neuroendocrinology, psy-choneuroimmunology, and genetics. Each of these modelshas widespread implications for behavioral and psycho-pharmacologic and non-pharmacologic interventions rele-vant to nursing practice.
The Central Nervous SystemThe central nervous system acts as the body’s primary infor-mation processing system, gathering data about the internaland external environments. It is the most complex of humansystems, governing emotional and behavioral as well as biological processes. It consists of the brain, the spinal cord,and the peripheral nervous system. Highly developed net-works of specialized cells work together to integrate a vari-ety of stimuli to respond appropriately to internal andexternal needs.
Diverse conditions, such as mental illness, trauma, aging,and degenerative processes, influence brain function.Abnormalities in neurotransmitter production or absorption,neuroendocrine response, immunology responses, andgenetic predisposition all appear to contribute to mental dis-orders. It has not been clearly established whether neuro-transmitter or neuroendocrine abnormalities cause mentalillness or vice versa; that is, underlying functional or struc-tural disorders contributing to mental illness may cause neu-rotransmitter and neuroendocrine abnormalities.
Neurodegenerative Processes
Degenerating processes may occur at any age, leading tocognitive and affective impairment. More importantly, theseprocesses may arise from underlying general medical con-ditions or their treatments. For example, many medicationsused to treat medical conditions contribute to a depressedmood. Also, for years health providers have recognized thatcognitive impairment may be linked to depressive disorders,particularly among older adults. Researchers also submit thatcognitive impairment is strongly associated after left hemi-
spheric stroke and intellectual impairment (Downhill &Robinson, 1994; Kase et al., 1998). Finally, the link betweenmood disturbances, such as depression and adverse out-comes in heart disease, specifically myocardial infarction, is well documented and accounts for half of the cases inthose recovering from myocardial infarctions (Glassman &Shapiro, 1998; Ziegelstein, 2001).
The brain shrinks with age and loses a considerable num-ber of neurons after the fifth decade of life. Despite theseneuronal changes, there is no definitive evidence of mentalor cognitive decline associated with aging. Some researcherssuggest that the brain adapts to aging by preserving anabundance of nerve cells rich in acetylcholine in neuro-transmitter pathways between the hippocampus and thecerebral cortex. These maturational changes are linked withhigher cortical function (e.g., “wisdom”). Deterioration ofthese neurons is linked with degenerative processes such asthose found in dementia associated with Alzheimer’s disease(AD) (Mesulam & Geula, 1991; Pickering-Brown et al., 2002).
Contemporary data suggest that these neurons die morerapidly than normal neurons and become sensitive to bio-chemical stress, which often leads to proteins that adheretogether and form damaging clumps called fibrils and freeradicals. Eventually, the concentration of fibrils and free rad-icals—the cumulative theory—increases and destroys thecells (Heintz, 2000). Recently, researchers exploring the causeof neurodegenerative diseases, such as Alzheimer’s disease,questioned the cumulative death or “one-hit” or single-eventhypothesis and submit that neuronal death occurs ran-domly. The “one-hit” model or theory suggests that a singleevent activates a mutant steady on the neuron that results incellular death. Random cell death supposedly arises fromgenetic mutations that alter proteins. These proteins havenot been identified at this time (Clarke et al., 2000).
Other researchers have explained Alzheimer’s diseaseand other frontal lobe dementia as a degeneration of cholin-ergic fibers that arise from the nucleus basalis of structuresinnervating the cortex and hippocampus and ultimatelycausing neuronal death. Death of cortical neurons in thehippocampus, cortex, and parietal and temporal lobes inter-rupts pathways and loss of information storage and retrieval.Eventually, these structural alterations correlate with cog-nitive decline and produce classic symptoms of AD.Prominent behavioral changes and symptoms of AD includeexecutive deficits, language difficulties, and inattentiveness.
Although AD is probably the most well-described neu-rodegenerative disease, other non-Alzheimer’s forms ofdementia are associated with progressive degenerativeprocesses of the frontal and temporal lobes. Frontotemporaldementia (FTD) is characterized by personality and behav-ioral changes. Major symptoms are similar to AD andinclude impaired word comprehension and naming; recog-nition disorders, including facial and object; progressivespeech difficulties (aphasia), particularly when it affects theleft frontotemporal lobe primarily (Pickering et al., 2002;Snowden, Neary, & Mann, 1996) (See Chapter 16).
66 U N I T O N E Perspectives and Principles
Managing and searching for a cure for AD and otherneurodegenerative disorders is complex owing to a lack ofknowledge about their exact etiology. Recent data (de laTorre, 2002) indicate that it should be classified as a vascu-lar disorder rather than a neurodegenerative disorder. Moredata are needed to understand the etiology of these com-plex conditions. No drug on the market is totally effective inthe treatment of AD or in altering its progressive course.Drugs that prolong the life of existing cholinergic neurons,such as donepezil (Aricept) or galantamine hydrobromide(Reminyl) may delay clinical decline in clients who sufferfrom AD (Othmer, Othmer, & Othmer, 1998; Wahlund, 1996).
Neurochemical Processes
Neural regulation is based on a complex network of trans-mitter pathways that are sensitive to fluctuation of transmit-ter and hormonal balance. Neurotransmitters initially interactwith receptor terminals of the postsynaptic cell membrane,resulting in either inhibitory or excitatory response. Thetype of neurotransmitter and receptors determine the natureof the response. Norepinephrine, dopamine, acetylcholine,and serotonin are examples of excitatory transmitters,whereas amino acids, such as gamma-aminobutyric acid, areexamples of inhibitory transmitters. Abnormal concentrationsof these substances are associated with impulsivity and men-tal disorders such as depression, anxiety, addictive disorders,and schizophrenia. Antidepressants, neuroleptics, anxio-lytics, and other pharmacologic agents act on the neuro-transmitters to increase or decrease their release, ultimatelymodifying relative concentration to improve the symptomsof mental disorders (see Chapter 28, PsychopharmacologicTherapy). Nurses must understand the neurochemical andsystemic impact of the medication they administer whethertreating mental or concurrent medical illnesses. In this way,optimal responses will more often be achieved.
NeuroendocrinologyNeuroendocrinology, the study of neural and endocrinesystems, indicates that these systems work together to main-tain normal body function or homeostasis. These systemscommunicate through biofeedback mechanisms to establisha basis for all biological and behavioral responses. The neu-roendocrine system contains the hypothalamus, pituitarygland, thyroid gland, adrenal glands, gonads, and pancreas.The hypothalamic-pituitary-adrenal (HPA) axis is particularlyimportant in the response to threat or stress. The HPA axisprovides a cascade of processes governing positive and neg-ative control at various areas, consequently modulatingenergy and cellular activity throughout the body (Campeau,Day, Helmreich, Kollack-Walker, & Watson, 1998). Abnor-malities in the HPA axis are known to contribute to, and arediagnostic of, functional psychosis, phobias, bipolar disor-der, and depressive and anxiety disorders (Coryell &Tsuang, 1992; Kessler, 1997; Nelson & Davis, 1997;Wolkowitz & Reus, 1999) (see Chapter 11 and Figure 11–1).
It is important for nurses to be aware of the endocrine-neural influences of mental disorders to better assess for andunderstand underlying pathology and potential treatment.
PsychoneuroimmunologyThe immune system plays a key role in the development ofinfections and tumors when it is underactive, and in thedevelopment of allergies and autoimmune diseases when itis overactive (Borysenko, 1987; Solomon, 1987). It is nowbecoming clear that the immune system plays a role inhealth and illness in the face of biological and psychosocialstress as well. This relatively new field of psychoneuro-immunology is a developing knowledge concerned withthe interconnections between the nervous system and theimmune system.
Each cell in a human body contains a marker that iden-tifies the cell as part of “self.” Any material that does notcontain this marker is identified as foreign antigen. Theimmune system serves the body by first detecting and pro-tecting it from invasion of antigens. One way in which itmay do this is through humoral immunity by producingantibodies to destroy or neutralize the foreign body. Thecharacter of the antigen and the specific antibody are storedin the memory of the immune cells, so that response toanother attack is more rapid and rigorous.
The immune system may be chronically activated asoccurs in a stress response, or it may fail to recognize theself-marker and attack itself such as in autoimmune dis-eases. An attack is mounted against “non-self” material, andwhen the immune system fails to differentiate self from non-self, it can attack itself such as in autoimmune diseases likesystemic lupus erythematosus (SLE).
The manner in which the immune system works hasmany implications for psychiatric nurses. Research has longshown that negative life events and stress affect health(Monroe & Simons, 1991). Recently, psychiatric illnesses,notably affective disorders and panic disorders (Brambilla etal., 1992) have been linked to immune dysfunction.Continued research in this area is critical. The NationalInstitute of Nursing Research has called for research devel-opment in the area of immunoincompetence as well as forinterventions that bolster appropriate immune response.
GeneticsNumerous research studies confirm the relationshipbetween genetic and enzymatic defects and genetic vulnerability to mental illness. For most mental disorders—schizophrenia, bipolar disorder, and pervasive developmen-tal disorder—the site involving genes, acting at distincttimes in brain development in vast regions of the brain,interfaces with epigenetic and environmental influences.Clearly, genetic function is influenced by prenatal and envi-ronmental factors that activate intricate biochemicalprocesses, which may, in turn, affect behavior and increasethe likelihood of mental disorders (Cowan, Kopinsky, &
C H A P T E R 3 Interfacing Biological-Behavioral Concepts into Psychiatric Nursing Practice 67

Hyman, 2002; Hyman, 1998). These patterns are oftenapparent in families with positive histories of various men-tal disorders, such as depression and suicidal behavior. Forexample, children whose parents are depressed are geneti-cally vulnerable to depression and may also experiencecompromised parental caregiving by the depressed parent.Consequently, the child is more vulnerable to depressionbecause of both genetic and environmental modes of trans-mission (Field, 1998; Francis, Caldji, Champagne, Plotsky, & Meaney, 1999; Gorwood, Batel, Ades, Hamon, & Boni,2000).
Twin, Adoption, and Family Studies
A number of researchers have attempted to explore the rela-tionship between genetic factors and mental disorders usingtwin, adoption, and family studies. Twin studies are help-ful in isolating genetic and environmental influences and indetermining preventive and precipitating factors. Thesestudies usually include monozygotic (MZ) or single-ovumand dizygotic (DZ) or two-ova twins. Adoption studies try todetermine the impact of environmental factors on geneticexpression. These studies generally examine and comparebiological and adoptive parents of affected subjects andthose of healthy biological and adoptive control subjects.Family studies contrast the occurrence of mental disorderamong relatives of affected subjects and assess the relevanceof heredity (Kaplan & Sadock, 1998; Lohr & Bracha, 1992).
Genetic theories regarding the cause of schizophreniadate back to Kraepelin in the early 1900s, who observed thatbizarre behavior was commonly found in families of clientswith schizophrenia. Twin, adoption, and family studies con-sistently link genetic, individual vulnerability, and psycho-social stressors with manifestations of schizophrenia; pervasivedevelopmental disorders; mental retardation; dementias; andaffective, addictive, and other disorders (Amir et al., 1999;Kendler & Prescott, 1999; Lyons et al., 1998; Sullivan, Neale,& Kendler, 2000; Tsuang, Stone, & Faraone, 2000).
Environmental Factors
Genetic factors do not account for all variances betweenheredity and mental illness. Such studies suggest that envi-ronmental factors are just as relevant as molecular-basedgenetic processes. Twin, adoption, and family studies tendto support this premise. Environmental factors includeparental treatment or caregiving patterns, family structures,age spacing, and gender. These factors may buffer or pro-tect genetically vulnerable clients (Berrittini, 2000; Field,1998; Kendler, Kessler, Neale, Heath, & Eaves, 1993), so thatpeople with a predisposition to a particular mental illnessmay not develop it because of exposure to protective envi-ronmental factors.
Genetics and Addiction
A leading area of concern for nurses is identifying clients at risk for alcoholism and other addictions. One possible
explanation for substance abuse perhaps lies in themesolimbic-mesocortical areas in the brain, which enhancedopamine and generate reward and reinforcement behav-iors. A blend of biological and psychosocial factors placescertain individuals at risk for addictive behaviors.
The role of genetic factors and alcoholism has generallybeen well supported by twin, family, and adoption studies.Biological or gene markers are found in dopamine receptors(Persico, Bird, Gabbay, & Uhl, 1996; Smith et al., 1992).More recent studies also implicate dysfunction of serotoner-gic transmission as a risk factor for excessive alcohol con-sumption and dependence (Gorwood et al., 2000; Heinzet al., 1998). In addition, certain behaviors are commonlyseen in clients who abuse substances (Hill, Shen, Lowers, &Locke, 2000). Many people who have genetic predispositionfor substance abuse may adhere to cultural or religious prin-ciples, or both, that never allow substance use; therefore,addiction will not occur even though the person has a vul-nerability marker. Religious groups, such as Muslims andMormons that forbid use of alcohol are believed to havefewer alcoholics than other religious groups. However, thisfinding does not mean that predisposition for addiction isnot present in their genetic makeup. Researchers continue toexplore the impact of genetics on mental illness and humanbehavior. The implications for finding clinical markers anddetecting biological and psychosocial factors include search-ing for the cause of mental illness, identifying clients at risk,developing effective treatment, and preventing exposure tonoxious factors that produce illness.
Genetic Research
Scientific studies involve identifying genes and proteins thatappear to cause mental disorders and are clearly altered bypsychopharmacologic agents and the environment. A keypurpose of this clinical evidence is the development ofnovel pharmacologic agents. Efforts to hasten the develop-ment of novel treatment have necessitated the establishmentof partnerships between biotechnology and pharmaceuticalindustries. The National Institute of Mental Health’sMammalian Genetics and Genome studies are already mak-ing great strides in genetic research, and studies are beingconducted that manipulate the mouse genome. These stud-ies are allowing scientists opportunities to take genes out,alter them, and replace them, and through brain probing,understand brain function relevant to behaviors, cognition,and emotions with precision (Hyman, 1998, 1999; NIMH,1998). Researchers are currently ambitiously involved in dis-covering “vulnerability genes” and in identifying the neuralpathways that regulate mood, emotion, energy, and othermechanisms that are affected by bipolar disorder and othermental disorders. They also propose that these discoverieswill be the bases of novel and clinical trials that integratepharmacologic and psychosocial interventions that improvethe quality of care and provide clients and insurers with evi-denced-based outcomes (Hyman, 2000).
68 U N I T O N E Perspectives and Principles

Newer technological advances in stem cell research thatinvolve culturing brainstem cells have the potential forreplacing any cell in the body. The great hope of medicineis that stem cells will one day be used as universal donorcells and offer cures to incurable diseases such as childhooddiabetes, Alzheimer’s disease, and spinal cord injury. Ofcourse, these studies are controversial, but in the near futurewill offer cures for clients, families, and communities suffer-ing from mental and physical disorders.
MAJOR BEHAVIORALMODELSBehavior represents an array of responses to internal andexternal stimuli. The behavioral approach to human activityassumes that behavior is influenced by specific interconnec-tions between complex neural processes, heredity, environ-ment, instinct, conditioning, and reinforcement. Behavior isdirected toward meeting basic human needs. Most humanbehavior is voluntary and related to avoiding negative expe-riences—behavior is not simply stimulus-response interac-tions. Behaviors are generally reinforced by rewards fordoing the right thing or punishment for doing the wrongthing. Human responses are directed either at goal attain-ment, such as asking for another piece of cake, or objectavoidance, such as avoiding crowds or elevators. Theseresponses are labeled either approach or avoidance ofstimuli.
Reinforcers are used to modify maladaptive behaviorand can be positive or negative. Reinforcers are personallydetermined. For example, it may be difficult to predictwhether two people at a party where alcohol is served willdrink: One may drink beer after beer regardless of themorning-after consequences, whereas the other may avoidalcohol altogether. Reinforcers account for the difference.One student may have a biochemical predisposition to alco-hol and thus will gain reinforcement directly from it.Another student may avoid alcohol because parental drunk-enness resulted his taking an oath not to drink. Or perhapsone of the people agreed to serve as the designated driverat this party and will be rewarded by drinking at the next.Perhaps both have a heavy workload the next day and can-not face the consequences of drinking. Good job perform-ance is the reinforcer in this example. Evidently, reinforcersare personal, complex, learned, and may be biochemical.
Behavior is observable and offers clues about the brain’sfunctioning in relation to internal and external stimuli.Internal stimuli include complex biological changes or dis-turbances, personality traits, perception, or temperament.Examples of external stimuli include developmental transi-tions, seasonal or circadian cycle changes, or other psy-chosocial stressors. Major behavioral theorists includeSkinner, Bandura, and Walters (see Chapter 2, Concepts ofPsychiatric Nursing).
INTEGRATION OF BRAINAND BEHAVIORThe interrelatedness of human behavior and brain functionis complex. Neural processes that govern thirst, hunger, sexdrive, aggression, and motivation are located in the hypo-thalamus and other areas in the limbic system. The brainanalyzes internal and external stimuli as either irrelevant or threats, and this process is the basis of perception.Perceptions generate neural signals that either inhibit orarouse cellular innervations. Motor commands arise fromthese signals. Complex nerve cell activity along the spinalcord governs motor and behavioral patterns. Lesions oralterations in the limbic system or sensory-perceptual mech-anisms generate maladaptive behavioral patterns, such asthose seen in psychosis. Psychosis is believed to arise frombiochemical and anatomical abnormalities that are mani-fested by vast behavioral responses, such as agitation, sensory-perceptual alterations, and social withdrawal.
Determining the origins and influences of behavior is difficult, but researchers continue to demonstrate more con-clusive evidence of biological bases for mental illness.Determinants of various behavioral responses include psy-chosocial stress and neurobiological, genetic, and culturalfactors. Appreciating the intricate link between psychosocialand neurobiological factors as causes of mental illness iscritical to developing effective interventions, participating inresearch that integrates these concepts, and understandingthe magnitude of technological advances.
KindlingNeurochemical changes are surmised to be associated withpsychosocial stressors. Kindling is an example of a neuro-biological response that is activated by significant early stressand losses. Kindling is the electrophysiological process thatover time produces an action potential after repetitive subthreshold stimulation or progressive sensitization of aneuron. Clinical studies over the past 40 years have soughtto discover the underpinnings of unipolar and bipolar disorders. Most findings suggest that monamine signalingand HPA axis dysregulation play integral roles in the patho-physiology of both mania and depression. Kindling andprogressive sensitization to seizures come from the epilepsyliterature and is a useful premise that explains neuro-biological processes at the molecular and cellular levels andthe genetic predisposition of mood dysregulation. Kindlingappears to produce dramatic increases in membrane-associated protein kinase C and certain G-proteins (Post &Weiss, 1999).
Protein kinase C (PKC) is a group of enzymes that acti-vate other enzymes. G-proteins are part of the cell’s plasmamembrane and are involved in sending signals from regula-tory chemicals such as hormones and neurotransmitters totarget cells. Collectively, PKC and G-proteins trigger a cascade
C H A P T E R 3 Interfacing Biological-Behavioral Concepts into Psychiatric Nursing Practice 69

of chemical reactions that produce target cells’ responses,and play roles in cellular proliferation, enzymatic reactions,and regulation of certain genes. Lithium and valproate acidregulate PKC activities and have efficacy in the treatment ofacute mania (Berretini, 2000; Manji & Lenox, 2000; Post &Weiss, 1999). Early losses and trauma are examples of stres-sors that result in mood dysregulation and its chronic andrecurrent course.
Early losses and traumas are thought to increase sensitiv-ity at some receptor sites by activating biochemicals thatimpair responsiveness and increase vulnerability to futuremood disorders. In other words, in early life, a psychosocialstressor, like the death of a parent, may precipitate a depres-sive episode. The next time a major psychosocial stressoroccurs, depression is experienced again. At some point, afterrepeated recurrences, depressive episodes begin to occurwithout a precipitating stressor. The basis of this premise is
encoding of a “long-standing trait marker” to affective illnessthat increases susceptibility to stress (Post, 1992). Feelings ofhelplessness are marked in people who have experiencedrepeated trauma (Maier & Seligman, 1976).
TraumaTraumatic events across the life span are also tied to neurobi-ological and behavioral changes, frequently seen in clientswith borderline personality, post-traumatic stress disorder,depression, and dissociative identity disorder. Responses totrauma are generally behavioral and biological. Clients experi-encing trauma often experience flashbacks, intrusive thoughts,“being in a daze” numbing, anxiety, startle reactions, night-mares, and fatigue (American Psychiatric Association, 2000).
Traumatic events involve activation of brain regionsrelated to perceiving and responding to a threat in which
70 U N I T O N E Perspectives and Principles
In The NewsWill Complementary Therapies Threaten the Use of ConventionalPsychotherapeutic Biological and Behavioral Treatment Approaches?From Fugh-Berman, A., & Cott, J. M. (1999). Dietary supplements and natural products as psychotherapeutic agents.
Psychosomatic Medicine, 61, 712–728.
Complementary and alternative therapies are chal-lenging nurses and other health care providers togain an appreciation for unconventional treatment ofpsychiatric disorders. Studies show that consumerinterest in complementary therapies was up 34 per-cent in 1997 from 1991 and continues to climb.Herbal medicine use has risen sharply over the pastdecade from 3 to 12 percent, and the majority ofconsumers use these therapies for chronic, ratherthan life-threatening, conditions. Many consumersmay not inform their health care providers of suchuse. A number of herbs and nutritional supplementshave observable effects on mood, memory, andsleep disturbances.
The surge of complementary therapies crosses allsocioeconomic, age, culture, gender, and ethnicgroups. The most cited health problems are chronicpain, anxiety, arthritis, chronic fatigue syndrome,and headaches. Psychiatric treatment appears to bea target of treatment, particularly anxiety and depres-sion. The skyrocketing use of these therapies amongthe mentally ill has prompted the National Institute ofHealth Office of Alternative Medicine and the NationalInstitute of Mental Health to fund a $4.3 million studyto determine the efficacy of these therapies on majordepression, biological, and behavioral therapies.Many clients consume these agents and use various
complementary therapies because they are readilyaccessible on the Internet, pharmacies, and healthfood stores. Critics worry that consumers will abandonconventional therapies and experience deleteriousconsequences. Do these consumer patterns reflectthe need for people to take charge of their lives in aseemingly out-of-control society, or does it reflectconsumers’ need for immediate gratification?
Regardless of the bases of this lucrative market ofcomplementary therapies, psychiatric nurses mustapprise themselves of these diverse treatments. It isimportant for nurses to be aware of data availableon herbs and dietary supplements that consumersare likely to be using. Likewise, although theseagents have demonstrable effects on clients’ mood,memory, and energy levels, they are not regulated.Health education is an integral part of psychiatricnursing care. Controversies prevail about the safetyof drug and herbal interactions and the lack of regu-lation of complementary therapies. The reality is thatconsumers will continue to take control over theirlives by using complementary and conventionaltreatment. Understanding the effects of diverseherbs, dietary supplements, and other complemen-tary therapies provides opportunities to assess, edu-cate the consumer, and integrate various therapieswith conventional interventions to promote health.

the HPA axis has a principal role. The HPA axis is primarilyresponsible for the secretion of the two main stress hor-mones, cortisol and norepinephrine (NE). These mecha-nisms orchestrate a cascade of complex responses thatinclude brain nuclei determining facial expression and therate and depth of cardiac and respiratory patterns. Theseneurobiological and behavioral responses are modulated bythe principal nucleus of the amygdala, which also acts as apowerful modulator of fear responses (Davis, 1994).Together the amygdala and hippocampus play “crucialroles” in the encoding and retrieval of memories, eventuallyactivating neurochemicals that give rise to dissociativeamnesia (Grillon, Southwick, & Charney 1996). The braincircuits involved in fear parallel a rapid and transitoryresponse to environmental stimuli. The identification of neural substrates of fear have made it possible to appreciatethe underpinnings of anxiety disorders (Coplan & Lydiard,1998; Fanselow & LeDoux, 1999). This premise also under-scores the biological and behavioral responses to traumathat are likely to be intense and goal-directed social isola-tion or withdrawal, startle response, alienation, irritability,and agitation.
In addition, trauma interferes with modulation of anxietyand aggression because of hyperarousal of the autonomicnervous system and heightened sensitivity to feelings orenvironmental stimuli. Persistent, severe distress is associ-ated with increased risk for certain cancers and immuno-suppressive disorders, such as autoimmune deficiencysyndrome, biochemical changes in neurotransmitters, andendogenous opioid (endorphin) production and release.Presumably, during sustained stressful periods, immensequantities of neurotransmitters such as norepinephrine anddopamine are secreted, increasing the risk of chronic stress-related illnesses. With prolonged stimulation, repletion of
neurotransmitters occurs, leading to receptor hyperstimula-tion and depletion of cortisol, consequently increasing therisk of post-traumatic stress disorder (Adamec, 1997;Anisman, Ritch, & Sklar, 1981; Shalev, 2000; Yehuda,McFarlane, & Shalev, 1998). In other words, when the stressresponse is turned on too long or too often, it cannot beturned off. This area of research has potential for nursingpractice in the area of preventive health care. See Table 3–1for the bioneurochemical and behavioral responses tosevere stress.
Acute trauma or stress increases dopamine release andmetabolism in certain brain centers, particularly the pre-frontal cortex. Moreover, activated dopaminergic systemsappear to be directly involved in mobilizing copingresponses and play a major role in the development of post-traumatic stress disorder (Antelman, 1988; Charney, Deutch,Krystal, Southwick, & Davis, 1993). This may explain whytrauma leads to lifelong consequences in susceptible per-sons. It also validates the consideration of both psychosocialstressors and neurobiological and behavioral responses in aholistic view of nursing.
Behavioral responses to dysregulation of certain neuro-transmitters include social isolation, startle reactions, irrita-bility, paranoia, distrust, and agitation. Serotonin is thought tomodulate the activity of other neurotransmitters, resulting inbehavioral and emotional responses (Blier & de Montigney,1985).
Adaptation to trauma is related to a number of factors(van de Kolk, 1987a), including:
a. severity of stressor
b. genetic vulnerability
c. developmental stage
d. available support system
C H A P T E R 3 Interfacing Biological-Behavioral Concepts into Psychiatric Nursing Practice 71
Table 3–1
Biochemical and Behavioral Responses to StressPOSSIBLE BEHAVIORAL
BIOCHEMICAL RESPONSES COGNITIVE APPRAISAL RESPONSES
Forebrain
Screens emotional responses to Irrelevant stimuli Ignored, no responsesinternal and external stimuliLinks hypothalamus to environment Perceived danger, threat Anxiety, sweating, restlessness,to activate proper neurochemical agitation, avoidance/social isolation, responses (i.e., autonomic nervous anger, aggressionsystem, neuroendocrine)
Hypothalamus
Acts as principal ganglion Reappraisal of threat or danger Calmness, decreased anxiety, fear, Activates proper neurochemical restlessnessresponses (e.g., anterior pituitary to adrenal coA1ex)
e. history of trauma
f. ego function (personality traits)
Similarly, adaptation to stress is generally related to a per-son’s repertoire of coping behaviors. The severity of a stressor is determined by individual perception of theevent.
The developmental stage during which the trauma is experienced influences the impact of the trauma. For instance,adults with adequate coping behaviors and support systems are likely to be less vulnerable to trauma than a child would be. Social systems during traumatic or stressful events act asbuffers to sustain trust, security, and safety (Hendin, 1984; van der Kolk, 1987b). The emotionally abused 1-year-old child is more likely to experience difficulty forming trusting and healthy interpersonal relationships throughout the remain-der of the life span than the battered housewife. Besides thedevelopmental stage, other factors influence a child’s responseto trauma. Early traumatic experiences also interfere with normal growth and development tasks such as learning trust,self-esteem, and autonomy; influence adaptive responsesthroughout the life span; and increase the risk for biological and behavioral morbidity. These risk factors include being a female, being in close proximity or exposure to the event, the degree of personal injury, injury or death of a family member, parental psychopathology, lack of quality support system, and the degree of life threat (Lipschitz, Rasmusson, & Southwick, 1998; Shaw, 1997; Shaw, Applegate, & Schoor,1996).
Neurological damage has also been detected in a numberof abused children who have no symptoms of traumaticbrain injury. Psychosocial factors such as chaotic and abusive environments are tied with delayed impaired CNSmaturation such as attention deficit disorder (ADD) (Fish-Murray, Koby, van der Kolk, 1987).
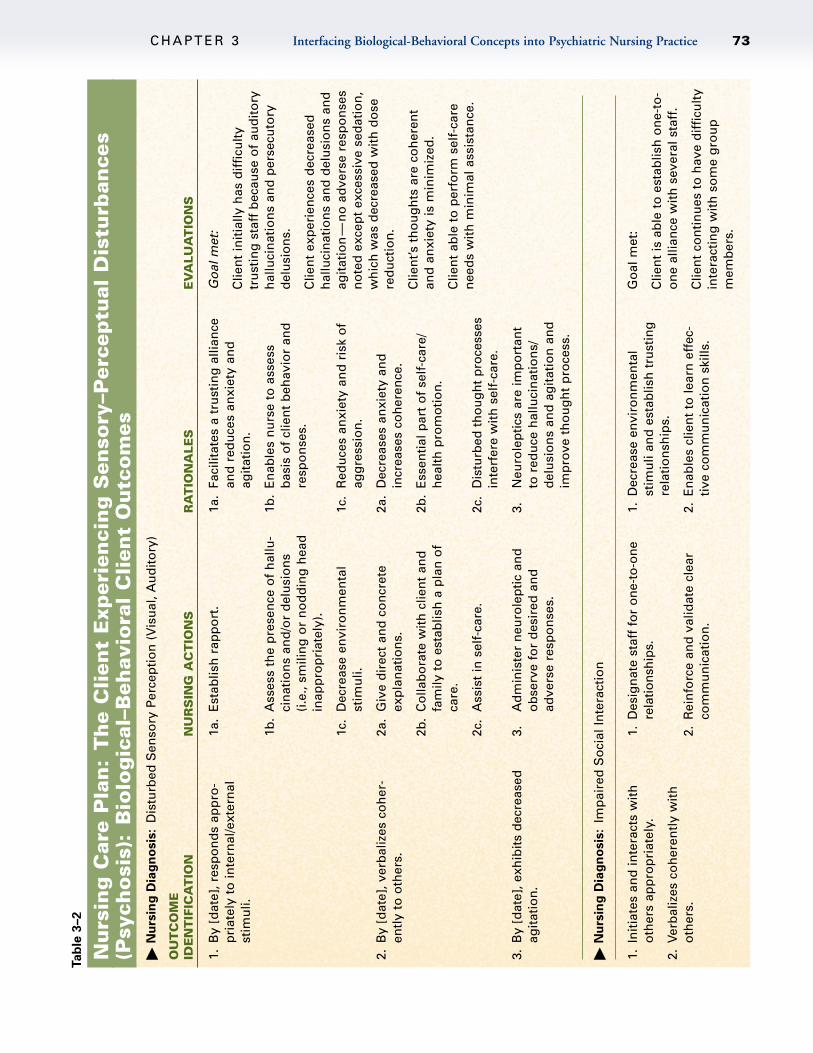
Bowlby (1973) believed that early attachments and rela-tionships with primary caregivers mediate maturation of theCNS, and that abuse impairs emotional and intellectual devel-opment. He noted the effect of early emotional bonding andformation of endorphins or endogenous opiates. Endorphinsplay a major role in managing severe stress, producingcalmness, and buffering one from emotional pain (van derKolk, Greenberg, Boyd, & Krystal, 1985; Kraemer, 1985). SeeTable 3–2 for biological-behavioral client outcomes, asincorporated into a nursing care plan. Understanding humanresponse to trauma and other psychosocial stressors is criti-cal to health maintenance. Pseudoseizures, abnormal elec-troencephalograms (EEGs), and clients with dissociativeidentity disorder have been associated with neurologicaltrauma (Brende, 1984). Interventions that provide emotionalsupport and empathy, modulate feelings, create trust, reduceanxiety, and promote a sense of control and power includevarious psychotherapies, cognitive-behavioral therapy, crisisintervention, stress management, and psychotropics. (SeeChapter 30, Chapter 11, and Chapter 28 for in-depth discus-sions of these interventions.)
MAJOR PARADIGMS OFPSYCHIATRIC-MENTALHEALTH NURSINGThe recent explosion of research and knowledge in the areaof neurobiology—involving advances in genetics brainmapping, imaging, and scanning—has opened up a fasci-nating world concerning the human brain and behavior.Psychiatric nursing educators and clinicians are challengedin their ability to integrate traditional psychiatric nursing andneurobiological concepts into nursing curricula and prac-tice. Psychiatric nursing continues to struggle with integrat-ing biological concepts into undergraduate and graduatecurricula despite advances in neurobiology, neuroscience,and genetics. Overall, technological advances in neurobio-logical discoveries and other psychiatric nursing challengesoffer vast opportunities to integrate biological and behav-ioral concepts into holistic interventions and improve thequality of life for the mentally ill.
Clinical and Practice IssuesRecent discoveries in the field of neurobiology continue torevolutionize the understanding and treatment of mental ill-ness. Because psychiatric nurses work collaboratively forthe most part, they cannot help but to be influenced bythese advances and must continually stay abreast of newfindings to communicate knowledgeably with other mentalhealth professionals. Likewise, evidenced-based researchshould guide nursing practice. Obviously, nursing must notlose sight of its holistic tradition, taking all aspects of theclient into consideration, including the spiritual, cultural,psychosocial, as well as the biological.
In spite of technological advances in neurobiology inunderstanding and treating mental illness, there has beensome controversy and doubt over its relevance to psychi-atric nurses. Peplau (1989) noted that specific mental dis-orders are difficult to explain as a “global or single entity”(p. 26) and determined that psychiatric nurses need toexplore the basis of impaired behavioral patterns rather thanthe biological aspects, and focus on human responses tostress and societal changes. At the same time, Peplaustrongly encouraged psychiatric nurses to value and appre-ciate the biological components of mental illness, as well asthe psychosocial concepts such as caring. Application ofbiological interventions does not negate the effectiveness ofother treatment modalities. Besides, psychosocial interven-tions such as psychoeducation, psychotherapy, stress man-agement, relaxation, and cognitive therapy continue to beviable treatment options.
Nursing InterventionsHistorically, one of the major biological interventions usedby psychiatric nurses involved assessing the need for pre-scribing and administering psychotropics to calm agitated
72 U N I T O N E Perspectives and Principles
C H A P T E R 3 Interfacing Biological-Behavioral Concepts into Psychiatric Nursing Practice 73
Tab
le 3
–2
Nu
rsin
g C
are
Pla
n:
Th
e C
lien
t E
xper
ien
cin
g S
enso
ry–P
erce
ptu
al D
istu
rban
ces
(Psy
cho
sis)
:B
iolo
gic
al–B
ehav
iora
l C
lien
t O
utc
om
es�
Nu
rsin
g D
iag
no
sis
:D
istu
rbed
Sen
sory
Per
cep
tio
n (
Vis
ual
, Au
dit
ory
)
OU
TC
OM
EID
EN
TIF
ICA
TIO
NN
UR
SIN
G A
CT
ION
SR
AT
ION
ALE
SE
VA
LUA
TIO
NS
1.B
y [d
ate]
, res
po
nd
s ap
pro
-p
riat
ely
to in
tern
al/e
xter
nal
stim
uli.
2.B
y [d
ate]
, ver
bal
izes
co
her
-en
tly
to o
ther
s.
3.B
y [d
ate]
, exh
ibit
s d
ecre
ased
agit
atio
n.
1a.
Est
ablis
h r
app
ort
.
1b.
Ass
ess
the
pre
sen
ce o
f h
allu
-ci
nat
ion
s an
d/o
r d
elu
sio
ns
(i.e
., sm
ilin
g o
r n
od
din
g h
ead
inap
pro
pri
atel
y).
1c.
Dec
reas
e en
viro
nm
enta
lst
imu
li.
2a.
Giv
e d
irec
t an
d c
on
cret
eex
pla
nat
ion
s.
2b.
Co
llab
ora
te w
ith
clie
nt
and
fam
ily t
o e
stab
lish
a p
lan
of
care
.
2c.
Ass
ist
in s
elf-
care
.
3.A
dm
inis
ter
neu
role
pti
c an
do
bse
rve
for
des
ired
an
dad
vers
e re
spo
nse
s.
1a.
Faci
litat
es a
tru
stin
g a
llian
cean
d r
edu
ces
anxi
ety
and
ag
itat
ion
.
1b.
En
able
s n
urs
e to
ass
ess
bas
is o
f cl
ien
t b
ehav
ior
and
resp
on
ses.
1c.
Red
uce
s an
xiet
y an
d r
isk
of
agg
ress
ion
.
2a.
Dec
reas
es a
nxi
ety
and
incr
ease
s co
her
ence
.
2b.
Ess
enti
al p
art
of
self
-car
e/h
ealt
h p
rom
oti
on
.
2c.
Dis
turb
ed t
ho
ug
ht
pro
cess
esin
terf
ere
wit
h s
elf-
care
.
3.N
euro
lep
tics
are
imp
ort
ant
to r
edu
ce h
allu
cin
atio
ns/
del
usi
on
s an
d a
git
atio
n a
nd
imp
rove
th
ou
gh
t p
roce
ss.
Go
al m
et:
Clie
nt
init
ially
has
dif
ficu
lty
tru
stin
g s
taff
bec
ause
of
aud
ito
ryh
allu
cin
atio
ns
and
per
secu
tory
del
usi
on
s.
Clie
nt
exp
erie
nce
s d
ecre
ased
h
allu
cin
atio
ns
and
del
usi
on
s an
dag
itat
ion
—n
o a
dve
rse
resp
on
ses
no
ted
exc
ept
exce
ssiv
e se
dat
ion
,w
hic
h w
as d
ecre
ased
wit
h d
ose
red
uct
ion
.
Clie
nt’s
th
ou
gh
ts a
re c
oh
eren
tan
d a
nxi
ety
is m
inim
ized
.
Clie
nt
able
to
per
form
sel
f-ca
ren
eed
s w
ith
min
imal
ass
ista
nce
.
� N
urs
ing
Dia
gn
osis
:Im
pai
red
So
cial
Inte
ract
ion
1.In
itia
tes
and
inte
ract
s w
ith
oth
ers
app
rop
riat
ely.
2.Ve
rbal
izes
co
her
entl
y w
ith
o
ther
s.
1.D
esig
nat
e st
aff
for
on
e-to
-on
ere
latio
nsh
ips.
2.R
ein
forc
e an
d v
alid
ate
clea
rco
mm
un
icat
ion
.
1.D
ecre
ase
envi
ron
men
tal
stim
uli
and
est
ablis
h t
rust
ing
rela
tio
nsh
ips.
2.E
nab
les
clie
nt
to le
arn
eff
ec-
tive
co
mm
un
icat
ion
ski
lls.
Go
al m
et:
Clie
nt
is a
ble
to
est
ablis
h o
ne-
to-
on
e al
lian
ce w
ith
sev
eral
sta
ff.
Clie
nt
con
tin
ues
to
hav
e d
iffi
cult
yin
tera
ctin
g w
ith
so
me
gro
up
mem
ber
s.

clients experiencing hallucinations and delusions. Recentneurobiological findings have promoted the creation of newpsychopharmacologic agents that target specific areas of thebrain to reduce symptoms and modify behaviors. Otherresearch findings link gender, culture, and genetic andfamilial factors to the efficacy of these agents. Selective sero-tonin reuptake inhibitors such as sertraline (Zoloft) andserotonin-norepinephrine reuptake inhibitors such as ven-lafaxine (Effexor) are examples of these new antidepres-sants. The use of electroconvulsive therapy (ECT) is gainingrenewed acceptance as an effective treatment modality forsevere depression and various schizophrenic disorders.Electroconvulsive and other biological therapies also helpseverely depressed clients suffering from psychomotor retar-dation, social withdrawal, and suicidal ideations. Otherexamples of biological therapies include complementarytherapies, such as St. John’s Wort for mild depression, rest-sleep manipulation for bipolar disorder, music or touch ther-apy in dementia, administration of full-spectrum lighting forseasonal affective disorder, and nutritional alterations inalcoholism.
Health promotion and primary prevention remain majornursing goals. These goals parallel managed health careconcepts that emphasize cost-effective and evidenced-basedhealth care. Prevention minimizes maladaptive behaviorsand chronicity in high-risk clients and groups. The domainof psychiatric nurses lies in recognizing and assessing age-appropriate responses to developmental tasks, biologicaldysregulation, and changes that define health and illnessacross the life span. Understanding the realm of normal oradaptive responses to stress helps nurses identify abnormalor maladaptive responses and formulate evidenced-basedoutcomes and interventions that incorporate biological andbehavioral concepts.
Client symptoms or behaviors allow the nurse to discernthe client’s inner world that comprises biological and behav-ioral processes activated by internal and external stressors.Active listening and astute observation of verbal and non-verbal cues are key aspects of assessing client responses.For instance, the psychotic client may smile or talk inap-propriately and have a disheveled appearance. These non-verbal cues link the nurse with complex neurobiologicalprocesses that affect the client’s behavior and effective treat-ment modalities.
Major treatment modalities include providing psychother-apy, behavioral modification, cognitive therapy; assessingthe need for medications; administering, prescribing, andmonitoring client responses to psychotropics; and facilitat-ing sleep-rest, light-dark, exercise-relaxation, and nutritionalaspects of care. These interventions integrate the biologicaland behavioral aspects of mental illness.
Psychiatric Nursing EducationThe National League of Nursing has long stipulated thatschools provide psychiatric nursing experiences for accred-
itation. Core areas of curricula focused on holistic conceptsand health promotion and prevention, and major conceptshave included caring and psychosocial needs of clients(American Nurses Association [ANA], 1984; McBride, 1990;Pothier, Stuart, Puskar, & Babich, 1990). A wealth of psychi-atric nursing literature has permitted faculty to define thescope and character of this specialty. Over the years educatorshave become leaders in directing psychiatric nursing prac-tice and generating specialization. These changes have par-alleled with the ANA specialization and scope of practice.
During the 1990s psychiatric nurses began to definemajor biological and behavioral concepts, integrating theminto nursing practice. McBride (1990) suggested that balanc-ing these concepts with care and caring to collaborate withother disciplines to develop effective client outcomes mightaccomplish this.
Some educators and clinicians have already defined out-comes that integrate biological and behavioral concepts intonursing practice. Additionally, undergraduate baccalaureatestudents were expected to gain knowledge of studiesregarding the brain and neuroscience and their impact onhuman adaptation to stress. Vast advances of the twenty-firstcentury in neurobiology and the information system provideeven greater opportunities for educators and clinicians togain a greater understanding of neurobiological researchand its impact on human behavior and the treatment ofmental illness. These efforts are likely to help nurses furtherdefine their roles and individualize mental health care moreprecisely than ever before.
McCabe (2000) points out a daunting trend in nursingeducation, namely, reduced classroom and clinical experi-ences in psychiatric-mental health nursing. She also expressesconcerns about decreased enrollment in psychiatric-mentalhealth nursing graduate school. Despite these trends in thisspecialty, she offers recommendations to nurse educatorsand leaders to address these concerns, and they include the following:
• Reconceptualize what constitutes the core psychiatricnursing content (generalist and advanced).
• Identify critical clinical competencies that reflect thecore content, role, and scope of psychiatric-mentalhealth nursing.
• Identify and standardize measurable clinical outcomes,based on content and competencies.
• Establish a national research agenda that expands andbuilds on the psychiatric nurse’s unique knowledgebase.
McCabe (2000) also suggests that changes in nursing cur-ricula can be made by integrating core concepts, such asrelatedness, adaptation, regulation, vulnerability, integrity,and efficacy and integrating them in the care of clients whoare mentally ill. These core concepts provide a theoreticalframework that encompasses the educational needs of generalist and advanced-practice psychiatric nurses. Integrat-
74 U N I T O N E Perspectives and Principles
ing biological-behavioral concepts with present nursingeducation trends affords opportunities for novel approachesto psychiatric-mental health nursing education and clinicalpractice.
The ANA continues to support psychiatric nurses andadvocates the integration of biological and behavioral con-cepts into nursing practice. The newest edition of A State-ment on Psychiatric-Mental Health Nursing Practice (ANA,2000) addresses enormous changes in psychiatric nursingand the health care delivery system. The ANA stresses theimpact of rapid evolution of biological sciences and ad-vances in technology on psychiatric nursing practice. Thisstatement establishes that neurobiological advances anddevelopment of interventions promise more effectiveresponse for the mentally ill. Moreover, the ANA confirmsthe need for psychosocial interventions, such as psycho-therapy, cognitive therapy, psychoeducation, crisis interven-tion, and administration and prescribing of psychotropics to help clients develop effective coping patterns. Finally,this publication provides an in-depth discussion of theAdvanced-Practice Psychiatric Registered Nurse, which isuseful in helping the public, legislators, and other profes-sionals understand the role of the generalist and theadvanced-practice role in psychiatric-mental health nursing.
THE ROLE OF THE NURSEThe generalist and advanced-practice registered nurse canuse an array of biological and behavioral interventions tofacilitate adaptive responses to internal and external stres-sors. Psychiatric nurses are faced with providing complexcare that meets the holistic needs of clients in inpatient,ambulatory, primary care, and home health and communitysettings. These needs include psychosocial and biologicalfactors that affect client behavior. Aggression, suicide, irri-tability, noncompliance, and social withdrawal are commonbehavioral responses to stress, which often arise from psy-chosocial and biological alterations.
The Generalist NurseThe generalist or psychiatric-mental health nurse works withclients, families, groups, and communities and uses thenursing process to assess adaptive and maladaptiveresponses. This nurse understands the relationship betweenunderlying biological processes, facilitates and reinforcesadaptive coping patterns, and assesses and prevents furtherdisability. Specific interventions encouraging health promo-tion and maintenance include psychoeducation, administra-tion of psychotropic medications and monitoring clientresponse, milieu therapy, and crisis intervention. Theseinterventions occur during activities such as intake andscreening, telecare, case management, and in diverse set-tings such as community and mental health centers, dayhospitals, home health settings, and homeless shelters(ANA, 2000). Biological and psychosocial interventions
enable the generalist psychiatric-mental health nurse to alteror modify maladaptive responses seen in various mental dis-orders, such as attention deficit disorders, psychosis, anddepression.
A combination of biological and psychosocial interven-tions can be used in caring for a client who is experiencingpsychosis. The psychotic client experiences perceptual distur-bances, such as auditory hallucinations that lead to suspi-ciousness, and may result in irritability, social reclusiveness,and refusal to eat. Perceptual disturbances represent neuro-biological phenomenon that results in behavior in responseto this internal and external stimuli. The client may act onthe command of the hallucinations and step in front of a caror refuse to eat because “someone poisoned the food.”Assessing the nature of hallucinations is crucial to the clientand staff’s safety. Administering a typical neuroleptic such as haloperidol (Haldol) or an atypical agent such as olan-zapine (Zyprexa) are biological interventions that target cer-tain neurotransmitters, specifically dopamine, that give riseto psychotic symptoms. The psychosocial intervention is acalm, firm approach that conveys empathy and provides theclient with structure and limit setting. These interventionscan work together to decrease hallucinations, delusions, andanxiety, and increase the client’s impulse control, thusreducing the risk of violent, aggressive behaviors (see Table3–2 for the nursing care plan).
Behavioral patterns can be adaptive or maladaptive. Thedepressed adolescent may use maladaptive behavioral pat-terns such as alcohol, stealing, or quarreling, to manageinternal emotional pain and to deal with psychosocial stres-sors of family pressures and school. Conversely, anotheradolescent may use adaptive responses and seek out family,friends, or clergy to verbalize feelings about a stressful situation. The nurse must operate on the premise that all behavior has meaning and can be clarified. Therefore,assessing behavioral responses to internal and external stim-uli is a major nursing responsibility and involves collabo-rating with the client and other mental health professionalsto develop effective interventions and evidenced-based outcomes.
The Advanced-Practice PsychiatricRegistered Nurse The role of the advanced-practice psychiatric registerednurse encompasses that of the generalist in addition to pro-viding direct clinical care, such as psychotherapy and pre-scriptive authority. Advanced educational and clinicalpreparation enables the advanced-practice psychiatric regis-tered nurse to assess complex problems and employ knowl-edge, skills, and clinical experience to alter or modifymaladaptive responses in various clinical settings (ANA,2000).
Specific advanced-practice psychiatric registered nurseinterventions include prescribing, administrating psy-chotropics, and evaluating client responses to various bio-
C H A P T E R 3 Interfacing Biological-Behavioral Concepts into Psychiatric Nursing Practice 75
logical therapies such as psychotropics, electroconvulsivetherapy, complementary therapies, phototherapy, and integrating them with behavioral strategies. Furthermore,conducting research study to assess client responses tobehavioral and biological interventions is critical to evaluat-ing and developing evidenced-based care.
Behavioral interventions offered by the advanced-practicepsychiatric registered nurse include cognitive-behavioral ther-apy, progressive relaxation, guided imagery, psychotherapy,and psychoeducation. Various interventions depend onnurse-client collaboration that allows nurses to empowerclients in understanding the basis of mental illness and cre-ate interventions that can alleviate symptoms and promotehealth maintenance.
RELATED RESEARCHPsychiatric nurses are in the midst of a neurobiological explo-sion that provides vast opportunities to define and investigateclient outcomes that integrate biological and behavioral con-cepts. Studies that compare the effectiveness of biological andbehavioral interventions can also assist nurses in developingevidence-based outcomes that meet the complex needs of thementally ill (refer to the Research Abstract). Survival of psy-chiatric nurses depends on the ability of educators, clinicians,and researchers to integrate biological and behavioral con-cepts into academic curricula and scope of practices. Eval-uating student experiences that incorporate these conceptscan generate data that direct students and practicing nurses.
76 U N I T O N E Perspectives and Principles
RESEARCH ABSTRACT
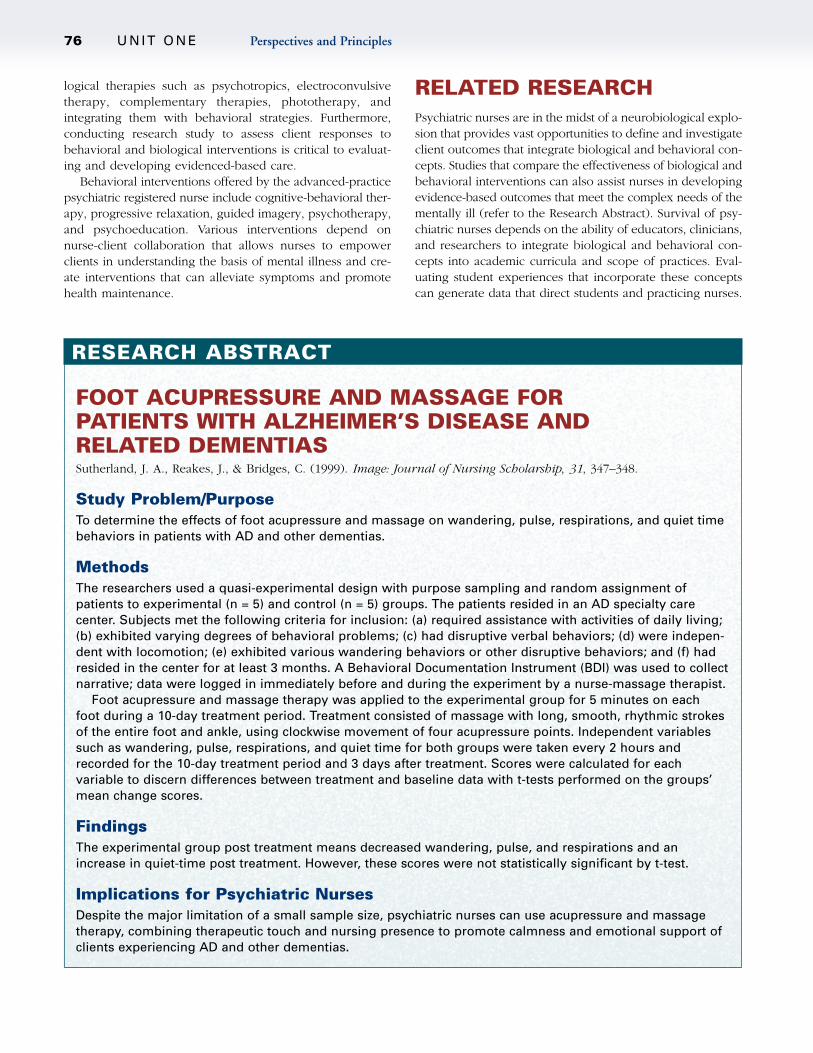
FOOT ACUPRESSURE AND MASSAGE FOR PATIENTS WITH ALZHEIMER’S DISEASE AND RELATED DEMENTIASSutherland, J. A., Reakes, J., & Bridges, C. (1999). Image: Journal of Nursing Scholarship, 31, 347–348.
Study Problem/PurposeTo determine the effects of foot acupressure and massage on wandering, pulse, respirations, and quiet timebehaviors in patients with AD and other dementias.
MethodsThe researchers used a quasi-experimental design with purpose sampling and random assignment ofpatients to experimental (n = 5) and control (n = 5) groups. The patients resided in an AD specialty care center. Subjects met the following criteria for inclusion: (a) required assistance with activities of daily living;(b) exhibited varying degrees of behavioral problems; (c) had disruptive verbal behaviors; (d) were indepen-dent with locomotion; (e) exhibited various wandering behaviors or other disruptive behaviors; and (f) hadresided in the center for at least 3 months. A Behavioral Documentation Instrument (BDI) was used to collectnarrative; data were logged in immediately before and during the experiment by a nurse-massage therapist.
Foot acupressure and massage therapy was applied to the experimental group for 5 minutes on each foot during a 10-day treatment period. Treatment consisted of massage with long, smooth, rhythmic strokesof the entire foot and ankle, using clockwise movement of four acupressure points. Independent variablessuch as wandering, pulse, respirations, and quiet time for both groups were taken every 2 hours andrecorded for the 10-day treatment period and 3 days after treatment. Scores were calculated for each variable to discern differences between treatment and baseline data with t-tests performed on the groups’mean change scores.
FindingsThe experimental group post treatment means decreased wandering, pulse, and respirations and anincrease in quiet-time post treatment. However, these scores were not statistically significant by t-test.
Implications for Psychiatric NursesDespite the major limitation of a small sample size, psychiatric nurses can use acupressure and massagetherapy, combining therapeutic touch and nursing presence to promote calmness and emotional support ofclients experiencing AD and other dementias.
SUMMARY• Advances in neurobiological research offer clinicians
and researchers a greater understanding of the com-plexity of mental health and illness.
• The expansion of biological knowledge gives clients,families, communities, and psychiatric nurses hope formore effective treatment to improve their quality of life.
• The human experience arises from the complex inter-action of the person’s neurobiological mechanism andthe individual’s environment.
• The biological-behavioral interface of mental health andillness is complex and challenges nurses to integratethese concepts into practice, education, and research.
STUDY QUESTIONS
1. Mary, a 28-year-old college student, encounters a situ-ation during her class that reminds her of a previoustraumatic predicament. Her immediate reactioninvolves intense fear and immediately getting out ofthe situation. The most accurate description of herreactions reflects which neurobiological processes?
a. The hypothalamus-pituitary-adrenal axis and amygdala
b. Kindling, neurotransmitters
c. Genetic predisposition
d. Hippocampus
2. Mr. Murray presents in the mental health center com-plaining of “hearing voices,” and he is smiling andtalking to himself during the assessment. The mostappropriate explanation for his behavior involveswhich of the following?
a. Dysregulation of a neurotransmitter such asdopamine
b. Stressful home situation caused by frequent argu-ments with his mother
c. Dopamine dysregulation and interpersonal conflicts
d. Overmedication with neuroleptic and related sideeffects
3. You are assessing the new client who is brought in byher father, who reports that he is concerned about herbehavior. As her nurse, which of the following is criti-cal in making an appropriate assessment of this client?
a. What kind of pressure has she been under lately?
b. Describe her relationship with family members.
c. How long has she lived with you?
d. Is there a family history of mental illness?
4. Mikie, a 7-year-old boy is brought in by his parents, whoreport that he has been irritable and fearful since hewitnessed his friend being viciously attacked by a dogseveral days ago. Which of the following is the mostappropriate immediate response to the parents and child?
a. Reassure the child and parents about the normalcyof his behavior.
b. Encourage the parents to consider an antidepres-sant for their child.
c. Refer them to a trauma counselor so the child canexplain the impact on his life.
d. Educate them about normal stress reactions.
5. Health maintenance is an integral part of psychiatricnursing practice. Which of the following interventionsmost accurately depicts health maintenance?
a. The client who loses his job is seen in a crisis center.
b. The anxious pregnant client who is referred forstress management.
c. The client with acute psychosis is offered an injec-tion of haloperidol.
d. The client experiencing an acute panic attack istaught deep breathing exercises.
6. Mrs. Nelson, an 86-year-old woman who has beenrecently diagnosed with Alzheimer’s disease, is seenduring a home health visit and is very confused. Herdaughter explains that she does not recognize familymembers, and this has been very difficult to handle.Which of the following behaviors might you expectfrom Mrs. Nelson during this visit?
a. She will respond appropriately after the nurse reorients her.
b. She is likely to become calm and cooperative.
c. She is likely to be aggressive and verbally abusive.
d. She is likely to remember things that happenedyears ago, but not recent events.
RESOURCES
Please note that because Internet resources are of a time-sensitive nature and URL addresses may change or bedeleted, searches should also be conducted by associationor topic.
Internet Resources
1. National Association of Clinical Nurse Specialists(NACNS)3969 Green StreetHarrisburg, PA 17110(717) 234-6799http://www.nacns.org
2. American Nurses Association600 Maryland Ave, SWSuite 100 WWashington, DC 20024(202) 651-7000(800) 274-4262http://www.ana.org
C H A P T E R 3 Interfacing Biological-Behavioral Concepts into Psychiatric Nursing Practice 77

3. The American Nurse Online Journal of Issues in Nursing
(800) 274-4262www.nursingworld.org
4. American Psychiatric Nurses AssociationColonial Place Three2107 Wilson Boulevard, Suite 300AArlington, VA 22201(703) 243-2443http://www.apna.org/
5. The American Heart AssociationNational Center7272 Greenville AvenueDallas, TX 75231(800) 242-8721www.americanheart.org
6. Alzheimer’s Association919 North Michigan Ave., Ste 1000Chicago, IL 60611-1676(800) 272-3900http://www.alz.org
Professional Organizations Involved in Brain andGenetic Research
www.nimh.nih.gov National Institute of Mental Health
www.nature.com Nature
www.sciencemag.org/misc/e-perspectives.shtml Scienceon line
http://www.grb.nimh.nih.gov/gi.html Department ofHealth and Human Services NIMH, Human GeneticsInitiative
http://www.edc.gsph.pitt.edu/stepbd Epidemiology DataCenter. STEP-BD. Systematic Treatment EnhancementProgram for Bipolar Disorder
REFERENCES
Adamec, R. (1997). Transmitter systems involved in neural plastic-ity underlying increased anxiety and defense—implications forunderstanding anxiety following traumatic stress. NeuroscienceBiobehavior Review, 21, 755–765.
American Nurses Association. (1984). Distribution and utilizationof psychiatric and mental health clinical nurse specialists in theUnited States. Kansas City, MO: Author.
American Nurses Association. (2000). Statement on psychiatric-mental health nursing practice. Washington, DC: Author.
American Psychiatric Association. (2000). Diagnostic and statisticalmanual of mental disorders, 4th edition Revision (DMS-IV-TR).Washington, DC: Author.
Amir, R. E., Van den Veyver, I. B., Wan, M., Tran, C. Q., Francke,U., & Zoghbi, H. Y. (1999). Rett syndrome is caused by muta-tions in X-lined MECP2, encoding methyl-CpG-binding protein2. Nature and Genetics, 23, 185–188.
Anisman, H. L., Ritch, M., & Sklar, L. S. (1981). Noradrenergic anddopimanergic interactions of escape behavior. Psychopharma-cology, 74, 263–268.
Antelman, S. M. (1988). Time dependent sensitization is the corner-stone for a new approach to pharmacotherapy: Drugs as foreignor stressful stimuli. Drug Development (Research), 14, 1–30.
Berretini, W. H. (2000). Are schizophrenic and bipolar disordersrelated? A review of family and molecular studies. BiologicalPsychiatry, 48, 531–538.
Blier, P., & de Montigney, C. (1985). Short term lithium adminis-tration enhances serotonergic transmission. European Journalof Pharmacology, 112, 415–418.
Borysenko, M. (1987). Area review: Psychoneuroimmunology.Annals of Behavioral Medicine, 9 (2), 3–10.
Bowlby, J. (1973). Attachment and loss, Vol. II, Separation. NewYork: Basic Books.
Brambilla, F., Bellodi, L., Perna, G., Battagalia, M., Sciuto, G.,Diaferia, D., Petraglia, F., Panerai, A., & Sacerdote, P. (1992).Psychoimmunoendocrine aspects of panic disorder. Neuro-psychobiology, 26, 12–22.
Brende, J. O. (1984). The psychophysiologic manifestation of dis-sociation: Electrodermal responses in a multiple personalitypatient. Psychiatric Clinics of North America, 7, 41–50.
Campeau, S., Day, H. E. W., Helmreich, D. L., Kollack-Walker, S., & Watson, S. J. (1998). Principles of psychoneuroendo-crinology. The Psychiatric Clinics of North America, 21, 259–276.
Charney, D. S., Deutch, A. Y., Krystal, J. H., Southwick, S. M., &Davis, M. (1993). Psychobiological mechanisms of posttraumaticstress disorder. Archives of General Psychiatry, 50, 294–305.
Clarke, G., Collins, R. A., Leavitt, B. R., Andrews, D. F., Hayden,M. R., Lumsden, C. J., & McInnes, R. R. (2000). A one-hit modelof cell death in inherited neuronal degenerations. Nature, 406,195–199.
Coplan, J. D., & Lydiard, R. B. (1998). Brain circuits in panic dis-order. Biological Psychiatry, 44, 1264–1276.
Coryell, W., & Tsuang, D. (1992). Hypothalamus-pituitary-adrenalaxis by hyperactivity and psychosis: Recovery during an 8-yearfollow-up. American Journal of Psychiatry, 149, 1033–1039.
Cowan, W. M., Kopnisky, K. L., & Hyman, S. E. (2002). Thehuman genome project and its impact on psychiatry. AnnualReview of Neuroscience, 25, 1–50.
Davis, M. (1994). The role of the amygdala in emotional learning.International Review of Neurobiology, 36, 225–266.
Downhill, J. E., Jr., & Robinson, R. G. (1994). Longitudinal assess-ment of depression and cognitive impairment following stroke.Journal of Nervous and Mental Disorders, 182, 425–431.
Fanselow, M. S., & LeDoux, J. E. (1999). Why we think plasticityunderlying Pavlovian fear conditioning occurs in the basolateralamygdala. Neuron, 23, 229–232.
Field, T. (1998). Maternal depression affects infants and earlyinterventions. Preventive Medicine, 27, 200–203.
Fish-Murray, C. C., Koby, E. V., & van der Kolk, B. A. (1987).Evolving ideas: The effects on children’s thoughts. In B. A. vander Kolk (Ed.), Psychological trauma (pp. 89–126).Washington, DC: American Psychiatric Press.
Francis, D. D., Caldji, C., Champagne, F., Plotsky, P. M., &Meaney, M. J. (1999). The role of corticotropin-releasing factor-norepinephrine systems in mediating the effects of early experi-ence on the development and endocrine responses to stress.Society of Biological Psychiatry, 46, 1153–1166.
Glassman, A. H., & Shapiro, P. A. (1998). Depression and thecourse of coronary artery disease. American Journal ofPsychiatry, 155, 4–11.
Gorwood, P., Batel, P., Ades, J., Hamon, M., & Boni, C. (2000).Serotonin transporter gene polymorphisms, alcoholism, and suicidal behavior. Society of Biological Psychiatry, 48,259–264.
Grillon, C., Southwick, S. M., & Charney, D. S. (1996). The psy-chobiological basis of posttraumatic stress disorder. MolecularPsychiatry, 1, 278–297.
78 U N I T O N E Perspectives and Principles
Heinz, A., Ragan, P., Jones, D. W., Homner, D., Williams, W.,Knable, M. B., Gorey, J. G., Doty, L., Geyer, C., Lee, K. S.,Coppola, R., Weinberger, D. R., & Linnoila, M. (1998). Reducedcentral serotonin transporters in alcoholism. American Journalof Psychiatry, 155, 1544–1549.
Heintz, N. (2000). One-hit neuronal death. Nature, 406, 137, 139.Hendin, H. (1984). Combat never ends: The paranoid adaptation
to posttraumatic stress. American Journal of Psychotherapy, 38,121–131.
Hill, S. Y., Shen, S., Lowers, L., & Locke, J. (2000). Factors pre-dicting the onset of adolescent drinking in families at high riskof developing alcoholism. Society of Biological Psychiatry, 48,265–275.
Hyman, S. E. (1998). NIMH during the tenure of director StevenE. Hyman, MD (1996–present): The now and future of NIMH.American Journal of Psychiatry, 155, 36–40.
Hyman, S. E. (1999). Introduction to the complex genetics ofmental disorders. Biological Psychiatry, 45, 518–521.
Hyman, S. E. (2000). Goals for research on bipolar disorder: Theview from NIMH. Biological Psychiatry, 48, 436–441.
Kaplan, H. I., & Sadock, B. J. (1998). Synopsis of psychiatry:Behavioral sciences, clinical psychiatry (8th ed.). Baltimore,MD: Williams & Wilkins.
Kase, C. S., Wolf, P. A., Kelly-Hayes, M., Kannel, W. B., Beiser, A.,& D’Agostino, R. B. (1998). Intellectual decline after stroke: TheFarmington Study. Stroke, 25, 805–812.
Kendler, K. S., Kessler, R. C., Neale, M. C., Heath, A. C., & Eaves,L. J. (1993). The prediction of major depression in women:Toward an integrated etiologic model. American Journal ofPsychiatry, 150, 1139–1145.
Kendler, K. S., & Prescott, C. A. (1999). A population-based twinstudy of lifetime major depression in men and women.Archives of General Psychiatry, 56, 39–44.
Kessler, R. C. (1997). The effects of stressful life events on depres-sion. Annual Review of Psychology, 48, 191–214.
Kraemer, G. W. (1985). Effects of differences in early social expe-riences on primate neurobiological-behavioral development. InM. Reife & T. Field (Eds.), The psychobiology of attachmentand separation (pp. 135–161), Orlando, FL: Academic Press.
Lipschitz, D. S., Rasmusson, A. M., & Southwick, S. M. (1998).Childhood posttraumatic stress disorder: A review of neurobio-logic sequella. Psychiatric Annals, 28, 452–457.
Lohr, J. B., & Bracha, H. S. (1992). A monozygotic mirror-imagetwin pair with discordant psychiatric illness: A neuropsychiatricand neurodevelopmental evolution. American Journal ofPsychiatry, 1091–1095.
Lyons, M. J., Eisen, S. A., Goldberg, J., True, W., Lin, N., Meyer,J. M., Toomey, R., Faraone, S. V., Merren, J., & Tsuang, M. T.(1998). A registry-based twin study in males. Archives ofGeneral Psychiatry, 55, 468–472.
Maier, S. F., & Seligman, M. E. P. (1976). Learned helplessness:Theory and evidence. Journal of Experimental Psychology:General, 105, 3–46.
Manji, H. K., & Lenox, R. H. (2000). Signaling: Cellular insightinto the pathophysiology of bipolar disorder. Society ofBiological Psychiatry, 48, 518–530.
McBride, A. B. (1990). Psychiatric nursing in the 1990s. Archivesof Psychiatric Nursing, 4, 21–28.
McCabe, N. (2000). Bring psychiatric nursing into the twenty-firstcentury. Archives of Psychiatric Nursing, 14, 109–116.
Mesulam, M. M., & Geula, C. (1991). Acetylcholinesterase-richneurons of the human: Cytoarchitectonic and ontogenetic patterns of distribution. Journal of Comprehensive Neurology,306, 193–220.
Monroe, S. M., & Simons, A. D. (1991). Diathesis-stress theories in the context of life stress: Implications for the depressive disorders. Psychological Bulletin, 110, 406–425.
National Institute of Mental Health (1998). Genetics and mentaldisorders: Report of the National Institute of Mental Healthgenetics workgroup (NIH Publication No. 98-4268). Bethesda,MD: Author.
Nelson, J. C., & Davis, J. M. (1997). DST studies in psychoticdepression: A meta-analysis. American Journal of Psychiatry,154, 1497–1503.
Othmer, E., Othmer, J. P., & Othmer, S. C. (1998). Brain functionsand psychiatric disorders: A clinical view. The PsychiatricClinics of North America, 21, 517–566.
Peplau, H. E. (1989). Future direction in psychiatric nursing fromthe perspective of history. Journal of Psychosocial Nursing, 27,18–28.
Persico, A. M., Bird, G., Gabbay, F. H., & Uhl, G. R. (1996). D2
dopamine receptor gene TaqI and B1 restriction fragment lengthpolymorphisms: Enhanced frequencies in psychostimulant-preferring polysubstance abusers. Biological Psychiatry, 15,776–784.
Pickering-Brown, S. M., Richardson, A. M., Snowden, J. S.,McDonagh, A. M., Burns, A., Braude, W., Baker, M., Liu, W. K.,Yen, S. H., Hardy, J., Hutton, M., Davies, Y., Allsop, D., Craufurd,D., Neary, D., & Mann, D. M. (2002). Inherited frontotemporaldementia in nine British families associated with intronic mutations in the tau gene. Brain, 125 (Pt. 4), 732–751.
Post, R. M. (1992). Transduction of psychosocial stress in the neurobiology of recurrent affective disorder. American Journalof Psychiatry, 149, 999–1010.
Post, R. M., & Weiss, S. R. B. (1999). Neurobiological models ofrecurrent mood disorder. In D. S. Charney, E. J. Nester, & B. S.Bunney (Eds.), Neurobiology of mental illness (pp. 365–384).New York: Oxford University Press.
Pothier, P. C., Stuart, G. W., Puskar, K., & Babich, K. (1990).Dilemmas and direction for psychiatric nursing in the 1990s.Archives of Psychiatric Nursing, 4, 284–291.
Shalev, A. Y. (2000). Biological responses to disasters. PsychiatricQuarterly, 17, 277–288.
Shaw, J. A. (1997). Children of the storm: A study of school children and Hurricane Andrew. In C. S. Fullerton & R. J.Ursando (Eds.), Post-traumatic stress disorder: Acute and longterm responses to trauma and disaster (pp. 123–143).Washington, DC: American Psychiatric Press.
Shaw, J. A., Applegate, B., & Schoor, C. (1996). Twenty-onemonth follow-up study of school aged children exposed toHurricane Andrew. Journal of the American Academy of Childand Adolescent Psychiatry, 34, 359–364.
Smith, S. S., O’Hara, B. F., Persico, A. M., Gorelick, D. A., Newlin,D. B., Vlahov, D., Solomon, L., Pickens, R., & Uhl, G. R. (1992).Genetic vulnerability to drug abuse: The D2 dopamine receptorTaqI B1 restriction fragment length polymorphism appear more frequently in polysubstance abusers. Archives of GeneralPsychiatry, 49, 723–727.
Snowden, J. S., Neary, D., & Mann, M. N. A. (1996). Frontotemporallobar degeneration: Frontotemporal dementia, progressiveaphasia, semantic dementia. New York: Churchill-Livingstone.
Solomon, G. F. (1987). Psychoneuroimmunology: Interactionbetween central nervous system and immune system. Journalof Neuroscience, 18, 1–9.
Sullivan, P. F., Neale, M. C., & Kendler, K. S. (2000). Genetic epi-demiology of major depression: Review and meta-analysis.American Journal of Psychiatry, 157, 1552–1562.
de la Torre, J. C. (2002). Alzheimer disease as a vascular disorder.Stroke, 33, 1152–1174.
Tsuang, M. T., Stone, W. S., & Faraone, S. V. (2000). Towardreformulating the diagnosis of schizophrenia. AmericanJournal of Psychiatry, 157, 1041–1050.
U.S. Congress. (1989). Decade of the Brain-Proclamation. Pub. L.No. 101-58 [HJ Res. 174], 130 Stat. 152-154 (July 25, 1989).
C H A P T E R 3 Interfacing Biological-Behavioral Concepts into Psychiatric Nursing Practice 79

van der Kolk, B. A. (1987a). Psychological trauma. New York:American Psychiatric Press.
van der Kolk, B. (1987b). The trauma spectrum: The interactionof biological and social events in the genesis of traumaresponse. Journal Traumatic Stress, 1, 273–290.
van der Kolk, B. A., Greenberg, M., Boyd, H., & Krystal, J. (1985).Inescapable shock, neurotransmitters and addiction to trauma:Towards a psychobiology of post-traumatic stress. BiologicalPsychiatry, 20, 314–325.
Wahlund, L. O. (1996). Magnetic resonance imaging and com-puted tomography in Alzheimer’s disease. Acta NeurologicaScandinavica (Supplementation), 168, 50–53.
Wolkowitz, O. M., Reus, V. I. (1999). Treatment of depressionwith antiglucocorticoid drugs. Psychosomatic Medicine, 61, 698–711.
Yehuda, R., McFarlane, A. C., & Shalev, A. Y. (1998). Predictingthe development of post-traumatic stress disorder from acuteresponse to a traumatic event. Biological Psychiatry, 44,1305–1313.
Ziegelstein, R. C. (2001). Depression after myocardial infarction.Cardiolology Review, 1, 45–51.
SUGGESTED READINGS
Antai-Otong, D. (2000). The neurobiology of anxiety disorders:Implications for psychiatric nursing practice. Issues in MentalHealth Nursing, 21, 71–89.
Faraone, S. V., Tsuang, M. T., & Tsuang, D. V. (1999). Genetics of mental disorders: A guide for students, clinicians, andresearchers. New York: Guilford Publications, Inc.
Goldberg, S. (1996). Clinical physiology made ridiculously simple(3rd ed.). Miami, FL: MedMaster.
Kaplan, H. I., & Sadock, B. J. (1996). Pocket handbook of psychi-atric drug treatment (2nd ed.). St. Louis, MO: Williams & Wilkins.
van der Kolk, B. A., McFarlane, A. C., & Weisaeth, L. (1996).Traumatic stress: The effects of overwhelming experience onmind, body, and society. New York: Guilford Publications.
80 U N I T O N E Perspectives and Principles