06 nguyen duc lam
TRANSCRIPT

Anesthesia in obstetric haemorrhage
Nguyen Duc Lam PhD, MD, Hanoi Medical UniversityDepartment of anesthesia, HN Obstetric and Gynecology
Hospital

Percentage of postpartum bleedingAutors year location
Total
deliveryn percentage
TrÇn Ch©n Hµ 1996-2000National
hospital of OG
38801 247 0,63%
NguyÔn Đøc Vy 1996-2001National
hospital of OG
48528 264 0,54%
Ph¹m ThÞ Xu©n
Minh1999-2004
National hospital of
OG51807 332 0,64%
B¹ch ThÞ Cóc 2008-2009National
hospital of OG
38084 262 0,69%
NguyÔn ThÞ Ngäc
Phượng1991-1994
Tu Du
hospital44675 164 0.38%
F. Reyal 1992-1998 France 19182 44 0,23%
J. Lankoande 1993-1997 Burkina Faso 12175 200 1,6% Bạch Thị Cúc, thesis, HMU, 2012

Obstetric haemorrhage, the first cause of death and maternal complications
In Vietnam: 67.4% of all maternal deaths In French: = 30% of deaths from direct obstetric causes = 10 deaths / year Maternal complication rate = 6.7 / 1000 births (6.0 to 7.5): shock
bleeding, severe anemia, complications of large volume blood transfusions, kidney, pituitary necrosis.
Around the world: 140,000 deaths / year every 4 minutes with a maternal mortality.
Half of these deaths occur 24 hours after birth

Obstetric haemorrhage
0
5
10
15
20
1988-1990 1991-1993 1997-1999
UK France
The leading cause of direct maternal death (%)
Statistics on maternal mortality in the UK Statistics from the National Advisory Council on Maternal mortality France

Maternal deaths could be avoided
Statistics from the National Advisory Council on Maternal mortality France
Causes of maternal deaths N
Tử vong mẹ có thể tránh khỏi
Yes May be % evitable No Conclusion inevitable
Due to direct obstetric causes
92 30 12 51,6 26 19
hemorragie 30 15 4 73,3 3 5
Amniotic fluid embolism 10 0 0 0,0 9 1
Hypertention 16 4 3 43,7 4 5
MTE ? 14 2 3 35,7 7 2
Infection 7 3 2 71,4 2 0
Obstetric complications 5 3 1 80,0 0 1
Anesthesia complications 1 0 1 100,0 0 0
Another causes 9 2 1 37,5 1 5
Due to indirect obstetric causes
49 6 8 28,6 28 7
Total causes 141 35 25 43,6 54 26

Definition
• Physiological blood loss
- Vaginal delivery <500 ml
- C-section: 500 - 1000 ml
• Haemorrhage
- When normal delivery: 500 - 1000 ml
- In cesarean section:> 1000 mL
- Severe haemorrhage > 1500 mL

Causes
• Hematome retro-placenta
• Placenta previa
• Uterine rupture
• Postpartum coagulopathy
• Postpartum bleeding (45%)

Cause of obstetric haemorrhage according Lariboisier
Uterine atony
Genital trauma
Retained placenta
Anormalplacenta
TrombusPlacental abruption
Anothercauses

The cause bleeding after birth in National hospital of OG
Total Percentage %Group Causes
Atonie Uterine atony 59 22,5
Retained placenta 18 6,9
Vaginal traumaGenital trauma 33 12,6
perineal hematoma 4 1,5
Placenta
Placenta previa 51 19,5
Placenta abruption 12 4,6
Placenta accreta 15 5,7
Placenta increta 4 1,5
Complication of cesareansection
Vaginal trauma 10 3,8
Hematome abdominal 5 1,9
infection 11 4,2
Postpartum bleeding at the National Hospital of OG at 2008-2009 (Thesis, Bach Thi Cuc, HMU)

Factors related to postpartum bleeding and vaginal delivery
Case-control study (USA) 9598 vaginal delivery374 postpartum bleeding
(= 3.9%)
Risk Factors
Factors OR
Prolonged labor 7,56
preeclampsia 5,02
Episiotomy 4,67
History of obstetric haemorrhage
3,55
multiple pregnancy 3,31
Labor induction 2,91
Soft tissue injury 2,05
Forceps 1,66
race 1,58-1,73
first pregnancy 1,45
Epidural anesthesia 1,00Combs CA et al. Obstet Gynecol 1991;77:69-76
Hight risks
Normal risks

Factors related to bleeding and cesarean section
Case-control study (USA) 3052 cesarean section196 bleeding (= 6.4%)
Risk Factors
Factors OR
General anesthesia 2,94
Chorioamnionitis 2,69
Preeclampsia 2,18
Labor dirigee prolongee 2,40
Cervical not progress 1,90
Race 1,58-1,73
Epidural anesthesia 1,00
Combs CA et al. Obstet Gynecol 1991;77:69-76
Hight risks Normal risks

May prevent obstetric haemorrhage?The risk factors for antenatal period Age of women Race Marital status Living standards and education levels No follow-up pregnancy Multiple pregnancy Preeclampsia Uterus had a previous caesarean scar +++ Placenta previa +++ Caesarean sectionHistory of bleeding Prehistoric yourself or a history of high-risk obstetric
Did not find any risk factor in 50% of cases

Abnormal placental
Location
• Placenta implants in low grip
• Placenta previa
The level of adherent placenta • Placenta accreta
• Placenta increta
• Placenta percreta
0
5
10
15
1985-1887 1988-1990 1991-1993
Postpartum hemorrhage
Placenta previa
placenta abruption
Deaths
Statistics from the National Advisory Council on Maternal mortality France

Uterine incision and anormal placenta
Clark SL et al. Obstet Gynecol 1985;66:89-
0
2
4
6
8
10
0 1 2 3 > 3
Số lần mổ đẻ trước đó
accreta
0
20
40
60
80
100
0 1 2 3 > 3
Số lần mổ đẻ trước đó
praevia + accreta
Time of cesarean section in hystory
Time of cesarean section in hystory
Time of cesarean section in hystory

Placenta previa
The proportion of Placenta accreta / placenta previa: 3.7% by Xa Thi Minh Hoa, Hanoi Hospital of OG in 2012 5.4% by Le Thi Huong Tra, National Hospital of OG in 2007-2011

Placenta accreta
Abnormally adherent placenta
• Scale: 1/2000 - 1/7000 births
• Classify
- Placenta accreta vera: adherence to the myometrium without invasion of uterine muscle
- Placenta increta: invasion uterine muscle.
- Placenta percreta: invasion of the uterine serosa or other pelvic structures
• Risk: a fulminant bleeding in surgery, can be life-threatening

Placenta acreta
Research on the periode of 2007-2011, Placenta accreta in the National Hospital of Obstetric and Gynecology
•100 cases
•60% had a history of cesarean section
•83% had placenta previa
•76% hysterectomy, ligation uterus artery 25%, 3% Blynch suture
•57% had a blood transfusion, in which 35% transmission> 5 units of packed red blood cells (1 case 9 units of packed red blood cells )
(Le Thi Huong Tra, thesis of master, HMU, 2012)

Placenta acretaReport 8 cases of Placenta percreta bladder in Central hospital of Hue
•7 patients require blood transfusion (87.5%)
•2 patients transfusion 5800 ml and 7500 ml of red blood cells
•100% total hysterectomy
(Bach Cam An)
Reported 1 case of Placenta accreta in patient had 2 times cesarean section at Tu Du Hospital
•Operation time of 200 minutes, mobilizing 20 people
•6500 ml blood loss
•26 units of packed red blood cells, 12 Plasma, 16 Cryo, 1 packed of platelete
(Ma Thanh Tung)

Placenta acretaAttention of anesthesia
• Common in women with placenta previa, multiple previous caesarean
• Color Doppler diagnosis: sensitivity 96.8%, specificity 87.5% (Tran Danh Cuong)
• Scheduled surgery plans
• 2 large intravenous lines, invasive blood pressure
• General anesthesia
• Packed red blood cells (PRBC)availability expected, plasma, Cryo, platelete
• 2 units of PRBC available in the operating room before incision
• Request obstetrician clamp and cut the uterus immediately after delivery

Placenta abruption

Haemorrhage post deliveryUterine atony 80%
- Multiparity
- Placenta previa
- Urinary retention
- Precipitous labor or prolonged labor
- Chorioamnionitis
- Halogen anesthetics, tocolytic therapy, MgSO4

Haemorrhage post deliveryAccumulation in the uterus 10%
• Retained placenta
• Hematoma in the uterus
• Placenta accreta
• Fibroids uterus, uterus anomaly
• Uterine leiomyomas

Haemorrhage post deliveryanother causes 10%
• Obstetric trauma (cervical, vaginal, perineal tears…)
• Vaginal hematomas
• Uterine inversion
• Coagulopathy (placenta abruption, amniotic fluid embolism, intrauterine fetal death)

Haemorrhage post delivery
• 30-50% of cases do not see a clear risk factors (to think of amniotic fluid embolism)
• Well tolerated in terms of hemodynamic, can not change the loss of 1,500 ml of blood
• There coagulopathy in 50% of cases
• Incorrect or lately management caused 70% mortality

Haemorrhage post deliveryTreatment
- Alert obstetrician and midwife
- Examination of uterus
• Removal and inspection of the placenta
• Currettage and surgical repair
• Evaluation of circulating volume
• Antibiotics

Measurement of blood loss

Medical uterotonic therapy• Uterine massage
• These drugs increase the contraction of uterus
• * Oxytocin: Do not exceed 30 UI
• * Sulproston (Nalador): 30 minutes
• - Initial doses of 500 mcg for 1 hour, then 500 mcg / 6 hours
• - CI: asthma, coronary, severe hypertension
• - How to use: dilution 50 ml, perfusion 10 ml / hour. Add 10 ml / hr every 10 minutes for up to 50 ml / hour
• Maintenance dose of 10 ml / h for 6 hours

Baumgarten K et al. Eur J Obstet Gynecol 1983;16:181-92
0 15 30 45 60 120 min
%methylergometrinesulprostone
oxytocinplacebo
101 women with normal pregnancies Measuring the pressure in the chamber TC TC contraction taking 3 different medications
Onset of efficacity sulpr. >
methylerg. ou oxytocine.
Time methylerg. > sulpr. >
oxytocine.
The pressure intra - uterus

Early drug use Nalador®
50
40
30
20
10
0
100
90
80
70
60
Treatment failure Treatment efficace
> 30 mn
< 30 mn
%
OR=8,3 ; IC à 95% : 2,2-31,7
Goffinet F. J Gynecol Obstet Biol Reprod 1995 ; 24 : 209-16

Management of severe postpartum bleeding by PGF2
Hayashi RH, Obs Gyn 1984
• 18 000 births in 3 years
• 900 cases of postpartum bleeding
• 54 cases uterine atony with oxytocin and treated with PGF2a
- Success: 86%
- Fever: 6%
- Sides effects on the digestive system: 9%

Why mothers die 1997-1999
Spinal anesthesia for caesarean section - direct intravenous oxytocin 5 UI

Blood transfusion
• Rarely, <1% of all births
• The risk of immune complications secondary to blood transfusion: need to prepare for future pregnancies
Research across France in 2003: 4% of the scientific production time for a transfusion of> 30 minutes

Control of blood transfusion
• Set the 2 line large diameter peripheral vein • Try FBCBilan fluid and blood
Surveillance hémoglobinTest hemoglobin, use the HemoCue ou Radical 7 Masimo
Coagulation testLabo, Vitro test dry, TEG
2 dry test tubes: Tubes 1/3 blood volume in each tube Tube 1: Tilt the tube every minute / time
When blood clot tube = recorded clotting time of tube 1 How well do the 2nd tube. Then add the clotting time of 2 tubes back - Normal <7 minutes - Sure, coagulopathy when> 20 min

Practice of blood transfusion in trauma of war

The mortality rate related to the transmission rate Plasma / globulin

Reanimation
• Antithrombin III và Aprotinin
• Fibrinogen
• Role of Transamin• Activated factor VII (Novo seven - FVII exogene)

• Evaluation• Number of units of plasma transfusion (PFC) • Percentage of AT> 70%
Result• clinical condition improved• XN (TC number and percentage of prothrombin (TP) increased significantly since firt day• But the efficiency is very low• Mortality rates did not differ between the 2 groups
Maki M. Gyn Obst Invest 1987
Disseminated intravascular coagulation (CIVD): Specific treatment
Antithrombine in CIVD heamorrage During labor and birth

Reduce the number Fibrinogen is a marker for early severity of postpartum bleeding
Fibrinogen concentration index is the only independent related to the progression of postpartum bleeding
Prognostic value of these results focus between The first hour to hour 4

Anti-fibrinolytic
•Randomized multicenter • Measure the volume of blood loss during and after cesarean • 180 nulliparous women with no risk factors • Tranexamique acid injection before incision: •1g then transmit 3 g / 3 hours • 20% reduction in bleeding in the period from • when taken during pregnancy through the first 2 hours after surgery

Tissue factor and factor VII activation essential for blood clotting
Important step is Moving from prothrombin to Thrombin
independently of FVIIIand FIX.
This step is independentof TF.
The thrombin burst leadsto the formation ofa stable clot

Temporary treatment regimen
•After obstetric interventions (constriction of RESERVED, circuit nodes) •- If the blood continues to flow mauchay •- Before you decide to cut styptic TC (if possible)
Dose
Second dose
Temperature normal
platelete

Techniques in surgical hemostasis
• Manual removal and inspection of the placenta
• Clamp pulling / twisting Cervix
• Examination of uterus, surgical repair
• Other measures

Hemostasis by ballon
•
•
•
sonde of Foley
sonde of Rüsch
Sonde ofBlakemore
• sonde of Linton-Nachlas
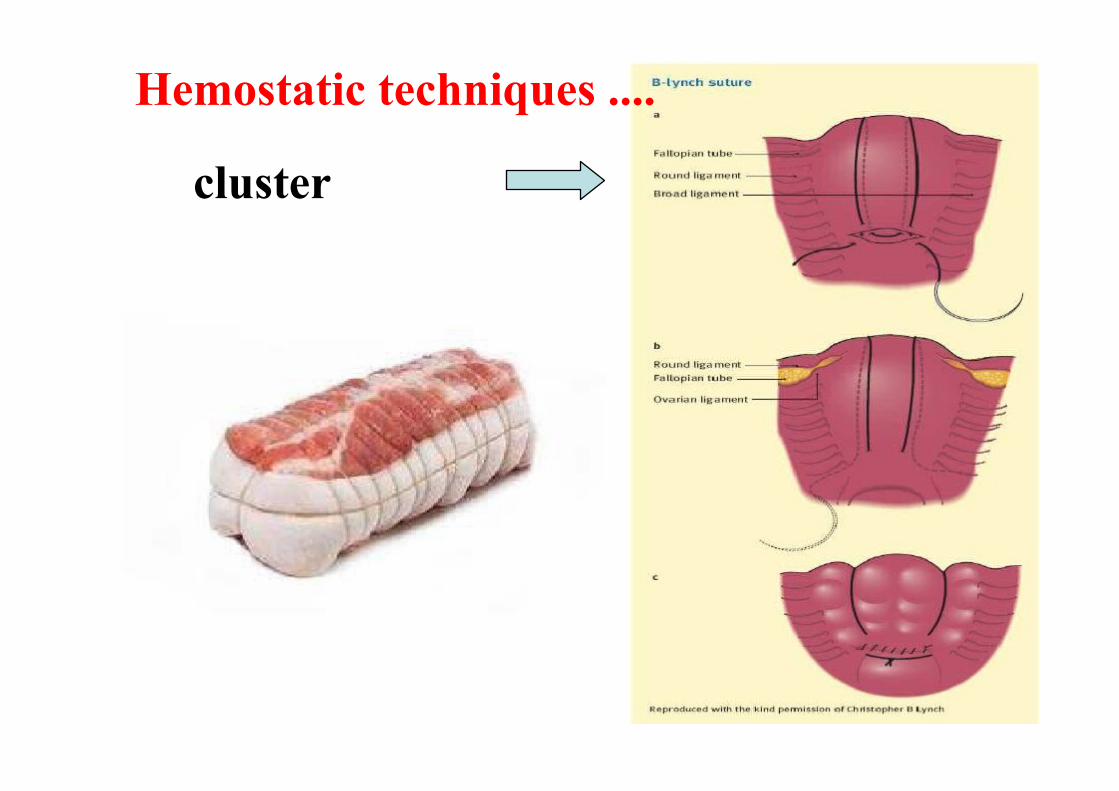
cluster
Hemostatic techniques ....

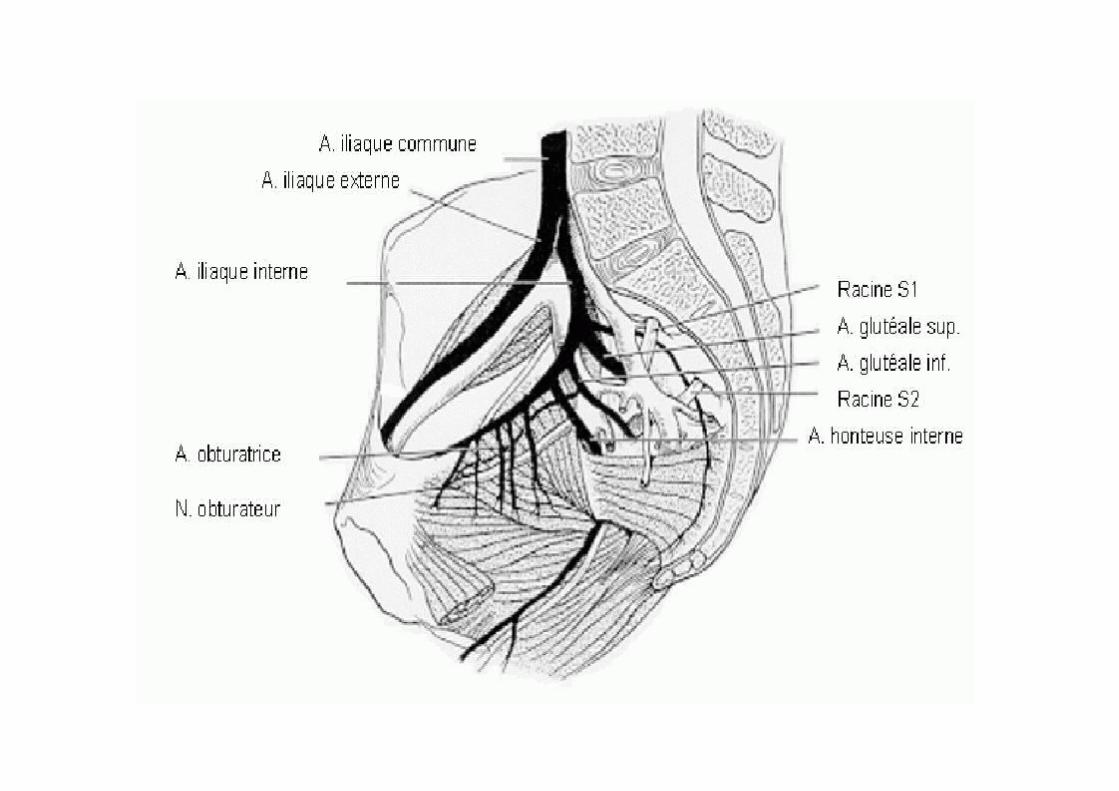
Hemostatic surgical techniques
Adominal way
• Uterine artery ligation• Hypogastric artery ligation
• Round ligamen artery ligation
• Measure the final:Hysterectomy hemostatic

Ligation nonselective

Selective ligation

Suc
cès
(%)
0Evans 1985 Clark 1985 Chatto 1990 O'Leary
1995Lédée 1996
Ligation external iliac arteries in obstetric haemorrhage
100
75
50
25
Successful%

Arterial embolization

Arterial embolization
• The center is equipped with• Button-screen circuit in the operating room through brightening due to radiologist do
Can proceed in the following cases:
• After cesarean section, after hemostatic suture lines under
• Can be conducted even when the patient has coagulopathy

(n) Succèsnombre (%)
Greenwood et al 6 83
Gilbert et al 10 100
Mitty et al 7 86
Yamashita et al 15 100
Merland et al 15 93
Pelage et al 37 89
Vandelet et al 15 73
Results of arterial embolization
successful(%)

Arterial embolizationResearch effective treatment of arterial embolization at
National hospital of OG 2009-2011 17 patients were node artery at Bach Mai Hospital and Vietnam Germany
(14: bleeding after cesarean section, postpartum usually 1, 1 to abortion, after cutting the TC 1)
100% stop bleeding, bleeding in 3 1/3 days off
No one hysterectomy
Not yet infected patients after occlusion of the vessel
1 Patients with lower extremity arthritis rules, medical treatment
100% return of menstruation
(Nguyen Phuong Tu, thesis of graduade Dr , HNU, 2012)

Dangerous if transfere
•State of shock not control: •- BP drops (had a blood transfusion / catecholamine) •- Need to control resuscitation of shock •Not only good for the circuit node: •- Shock bleeding during cesarean section •- Bleeding after cesarean •No blood and blood products •- A rare blood type, antibodies against the human erythrocyte •- Problem organizations •- Prognosis: deadline to stop bleeding

Pregnant women treated in the ICU, and maternal mortality
0
5
10
15
20
total transfere grade III
maternal death
Bouvier-Colle MH et al, Eur J Obstet Gynecol 1996,65:121-5
%

Classification of obstetric hospital
*Grade 1
•Get the patient has no risk factors
•Full-term newborn care
* Grade 2
•Get the care of patients requiring more complex
•Have neonatal department
* Grade 3
•Get the severely ill patients requiring intensive care
•Have neonatal ICU unit



Anesthesia
• Epidural anesthesia if available is sufficient for the
hemostatic surgical echniques
• Anesthetic when bleeding more
and surgery to stop bleeding
• Priority selection ketamine (1 mg / kg) or
Etomidat (0.3mg/kg)

Conclusion
• 87% of deaths due to bleeding that could have been avoided
• Pay attention to time detection, treatment usually late
• The discreet clinical sign
• Blood transfusion in proportion 1/1 - Fibrinogen - Transamin
• Keep progressing syndrome CIVD
• Position the insertion of the ballon, arterial embolization and circuit activates factor VII?

Thank for your attention!Thank for your attention!