06212016 evidence live presentation
TRANSCRIPT

Rapid creation of GRADE-labeled recommendations before
guidelines are available using a systematic multi-expert process
Peter Oettgen MD FAHA, FACCSheila Bond MD FACP
DynaMed, EBSCO HealthIpswich, MA

Outline• Review example of making recommendation
in DynaMed Plus (10-15 minutes)
• Background on asymptomatic bacteruria during pregnancy (10-15 minutes)
• Breakout groups (30 minutes)
• Discussion (20 minutes)

Rationale
• There is often a delay or gap between when practice-changing studies are published and when changes in clinical practice guidelines are made. Delay may be months to years
• Examples:– A new heart failure drug (e.g. Sacubitril-valsartan recently shown
to reduce hospitalization rates and mortality this year)– A new class of cholesterol lowering drugs (PCSK9 inhibitors
shown to reduce cardiovascular events by >50% in selected patients at high risk of or with known CAD)
What is DynaMed Plus?
DynaMed Plus is a point-of-care tool designed to provide the busy physician with the information they need with a focus on rapid time-to-answer

Mission of DynaMed Plus
“To provide health care professionals with the most useful information at the point of care.”

DynaMed Plus recommendation process
• Step 1 – The need for a new or modified recommendation is identified• Step 2 – Clinical questions are formulated using the PICO framework for all
outcomes of interest related to the recommendation to be developed• Step 3 – Systematic search for evidence in support of the clinical questions• Step 4 – Evidence is summarized for each outcome, the relative importance of the
outcome, the estimated effects comparing intervention and comparison, the sample size, and overall quality rating for the body of evidence
• Step 5 - Recommendation panel members are selected to include at least three members that together have sufficient
– clinical expertise for the subject(s) pertinent to the recommendation, – methodological expertise for the evidence being considered, and– experience with guideline development
• Step 6 – Potential panel members must disclose conflicts of interest (COI) and if significant COIs exist must recuse themselves of being on the review panel
• Step 7 – Panel reviews evidence and makes Strong, Weak, or no recommendation• Step 8 - All steps in the process are transparent

GRADE

Evidence summary for Sacubitril-valsartan
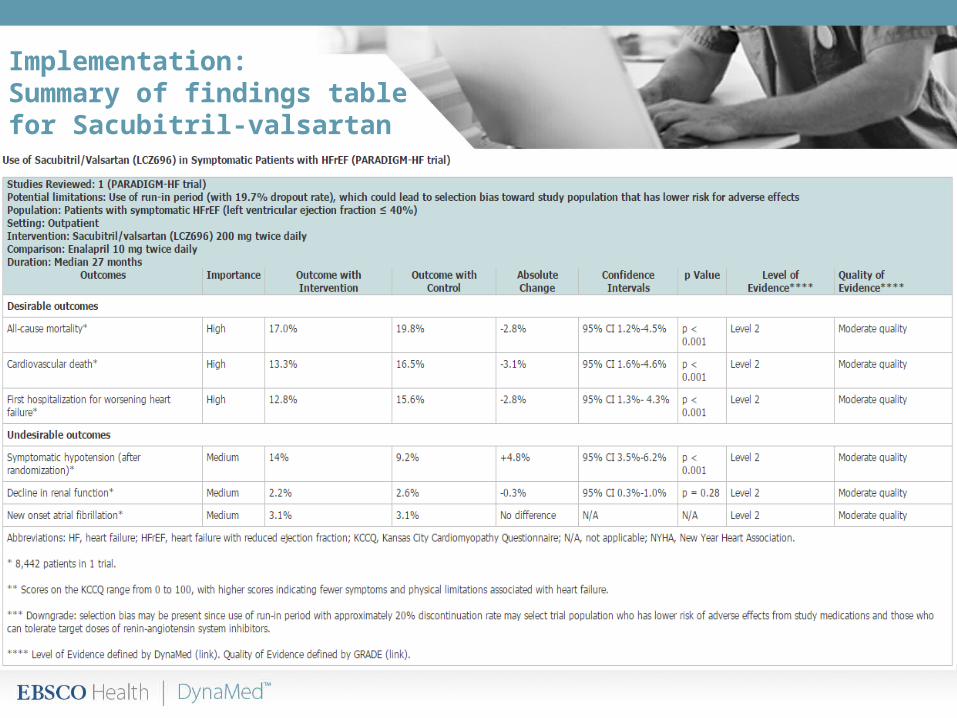
Implementation:Summary of findings tablefor Sacubitril-valsartan








Workshop:
Should women be screened and treated for asymptomatic bacteruria during early pregnancy?
What do you recommend?

Screening and Treatment forAsymptomatic Bacteruria in Pregnancy
• Asymptomatic bacteruria (ASB) is common in pregnant and nonpregnant women
• ASB in pregnancy is associated with an increased risk of pyelonephritis, which most often occurs in the 2nd trimester
• ASB and pyelonephritis may be associated with an increased risk of preterm labor
• A screen-and-treat strategy is recommended by many medical societies for pregnant women in the 1st trimester
• A recent new study (the 1st since 1987) calls this strategy into question and has lead the European Association of Urology to rescind its prior strong recommendation on the matter

Asymptomatic Bacteruria in Pregnancy: The Guidelines
Organization Date Recommendation GradeInfectious Diseases Society of America (IDSA) 2005 Screen all pregnant women by urine culture at least
once early in pregnancy (around 12-16 weeks) and treat if culture positive
IDSA Grade A-I
United States Preventive Services Task Force (USPSTF)
2008 Screen all pregnant women for asymptomatic bacteriuria using urine culture at 12-16 weeks gestation
USPSTF Grade A
National Institute for Health and Care Excellence (NICE)
2008 Offer routine screening for asymptomatic bacteriuria by midstream culture early in pregnancy, as identification and treatment reduces risk of pyelonephritis
No rating applied
American Academy of Pediatrics (AAP) and American College of Obstetricians and Gynecologists (ACOG)
2012 If urine culture performed early in pregnancy, treat asymptomatic bacteriuria and do test of cure
No rating applied
Society of Obstetricians and Gynaecologists of Canada (SOGC)
2012 Treat any bacteriuria with colony counts 100,000 ≥ CFU/mL in pregnancy with appropriate antibiotics
SOGC Grade II-2A
Scottish Intercollegiate Guidelines Network (SIGN) 2012 Treat asymptomatic bacteriuria detected in pregnant women with an antibiotic
SIGN Grade A
European Association of Urology (EAU) 2015 No recommendation made Not applicable
References - EAU 2015 Mar, AAP and ACOG 2012, J Obstet Gynaecol Can 2012 May;34(5):482, SIGN 2012 Jul PDF, Ann Intern Med 2008 Jul 1;149(1):43, NICE 2008 Mar, Clin Infect Dis 2005 Mar 1;40(5):643

Should women be screened and treated with a 3 – 7 day course of antibiotics for asymptomatic bacteruria (ASB) during early pregnancy?
Background: ASB is associated with an increased risk of maternal pyelonephritis, and may be associated with preterm labor
Perspective: A screen and treat strategy for ASB may prevent maternal pyelonephritis and associated adverse neonatal outcomes. Recommendations vary among major medical societies. Most trials addressing the efficacy of this intervention are older and may not be generalizable to the present day. A new study challenges the efficacy of the intervention but is limited by small size.
Population: Asymptomatic, healthy women in the 1st trimester of pregnancy
Intervention: 1st trimester screening by urine culture with 3-7 days of antibiotic treatment for positive results
Comparison Placebo/no intervention
Setting: Outpatient
Step 1:
Identify the need for a new or modified recommendation

Desirable Outcomes:
• Does screening and antibiotic treatment for ASB in early pregnancy prevent
1. maternal pyelonephritis?2. preterm labor?3. perinatal death?
Undesirable Outcomes:
• Is screening with antibiotic treatment associated with any adverse maternal or neonatal outcomes?
Step 2:
Formulate a clinical question using the PICO framework for all outcomes of interest

Step 3:
Perform a systematic search for evidence
Smaill FM, Vazquez JC. Antibiotics for asymptomatic bacteriuria in pregnancy. Cochrane Database Syst Rev. 2015 Aug 7;(8):CD000490. doi: 10.1002/14651858.CD000490.pub3. Review.
BM, Koningstein FN, Schneeberger C, et al. Maternal and neonatal consequences of treated and untreated asymptomaticbacteriuria in pregnancy: a prospective cohort study with an embedded randomised controlled trial. Lancet Infect Dis. 2015 Nov;15(11):1324-33.
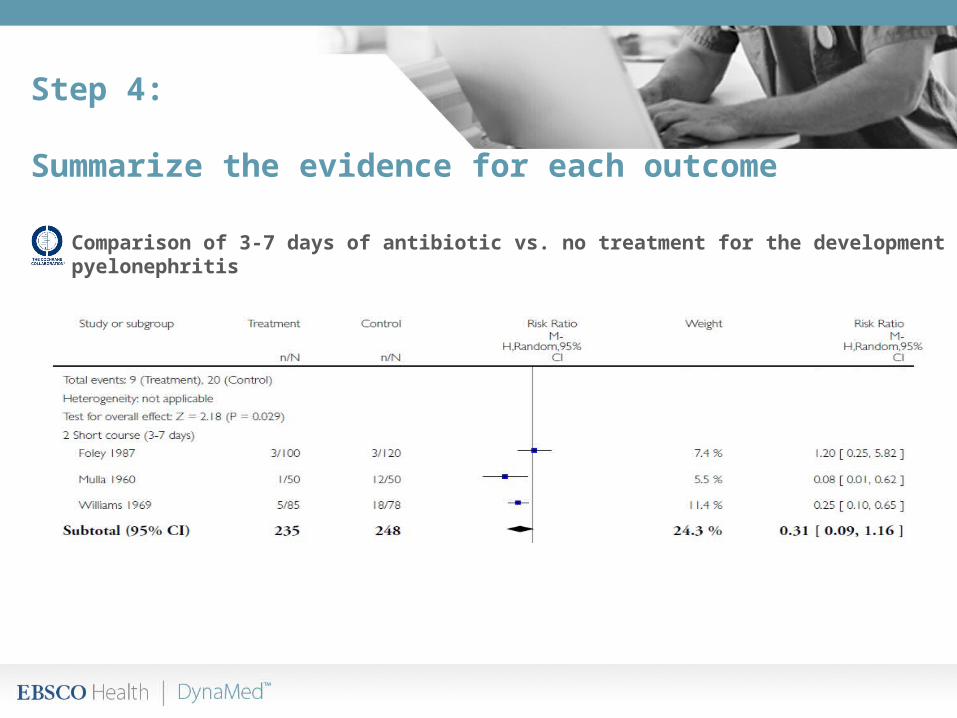
Step 4:
Summarize the evidence for each outcome
Comparison of 3-7 days of antibiotic vs. no treatment for the development of pyelonephritis

Lancet Infect Dis 2015 Nov;15(11):1324
cohort study with embedded randomized trial
• 4,283 women with singleton pregnancy in 8 hospitals and 5 ultrasound centers in the Netherlands screened for asymptomatic bacteriuria with single dipslide between 16 and 22 weeks gestation were followed to 6 weeks postpartum
• 248 women (5.8%) had asymptomatic bacteriuria
• 85 women with asymptomatic bacteriuria randomized to nitrofurantoin 100 mg twice daily for 5 days vs. placebo
• 163 women with asymptomatic bacteriuria who chose not to participate in trial were followed without treatment (94% refused participation because they did not want to receive antibiotics during pregnancy for asymptomatic condition)
• pyelonephritis occurred in 29 women (0.7%) overall
• preterm birth (< 37 weeks) occurred in 220 women (5.1%) overall

Step 4:
Summarize the evidence for each outcome
Comparison of 5 days of antibiotic vs. placebo/no treatment for the development of pyelonephritis
0 1 (2.2%) -2.2 ( - 23.4 to 19.0)
1 (2.2%) - 2.2 (-23.4 to 19.0)

Step 4:
Summarize the evidence for each outcome
Outcome Cochrane Review* Lancet Cohort** Quality of Evidence Effect Estimate (95%CI) Control Event Rate Effect Estimate (95%CI) Control Event Rate
Pyelonephritis 0.31 ( 0.09-1.16) 13% (33/248) 0.46 (0.03-8.22) 2.9% (6/208) Very LowPreterm labor (<37 weeks) 0.14 (0.03 - 0.60) 38% (12/32) 0.95 (0.22-4.1) 5.3% (11/208) Very LowPreterm labor (<34 weeks) NA NA 2.6 (0.24-28) 1.0% (2/208) Very Low
Perinatal death NA NA 2.6 (0.24-28) 1.0% (2/208) Very LowAdverse antibiotic effects NA NA NA NA
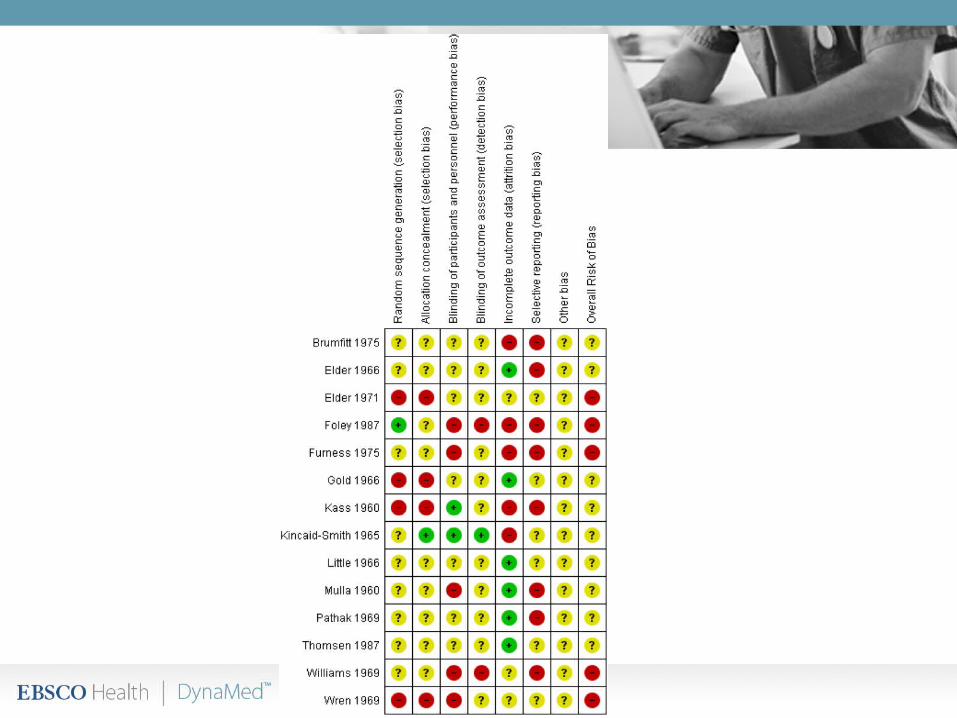
* Each of the 3 included randomized trials evaluating pyelonephritis was performed between 1960 and 1987 when standardized testing, methods of gestational data and access to care differed limiting generalizability to modern day. The 1 randomized trial evaluating preterm birth focused only on Group B streptococcus which may have different clinical implications. All included trials had several methodologic limitations including lack of blinding, incomplete descriptions of methods, selective and/or incomplete reporting.** Trial was underpowered to detect these outcomes
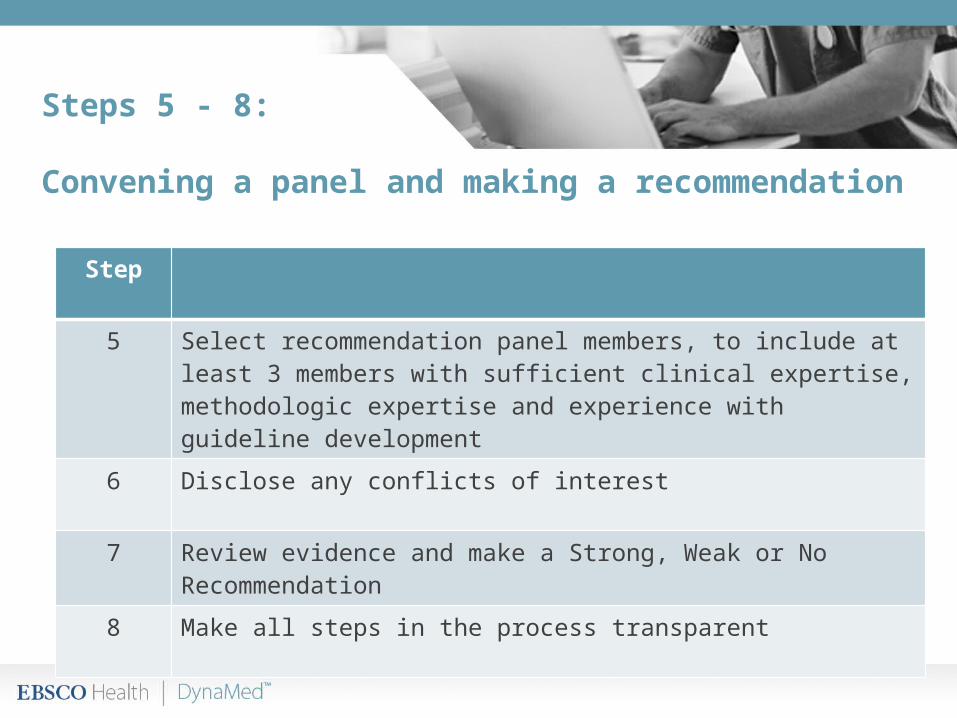
Steps 5 - 8:
Convening a panel and making a recommendation
Step
5 Select recommendation panel members, to include at least 3 members with sufficient clinical expertise, methodologic expertise and experience with guideline development
6 Disclose any conflicts of interest
7 Review evidence and make a Strong, Weak or No Recommendation
8 Make all steps in the process transparent

Steps 5 - 8:
Workshop and Discussion
Step
5 Break into small groups and use the 3 worksheets provided to help in the deliberation process
6 Ask any questions
7 Review evidence and make a Strong, Weak or No Recommendation
8 Discussion
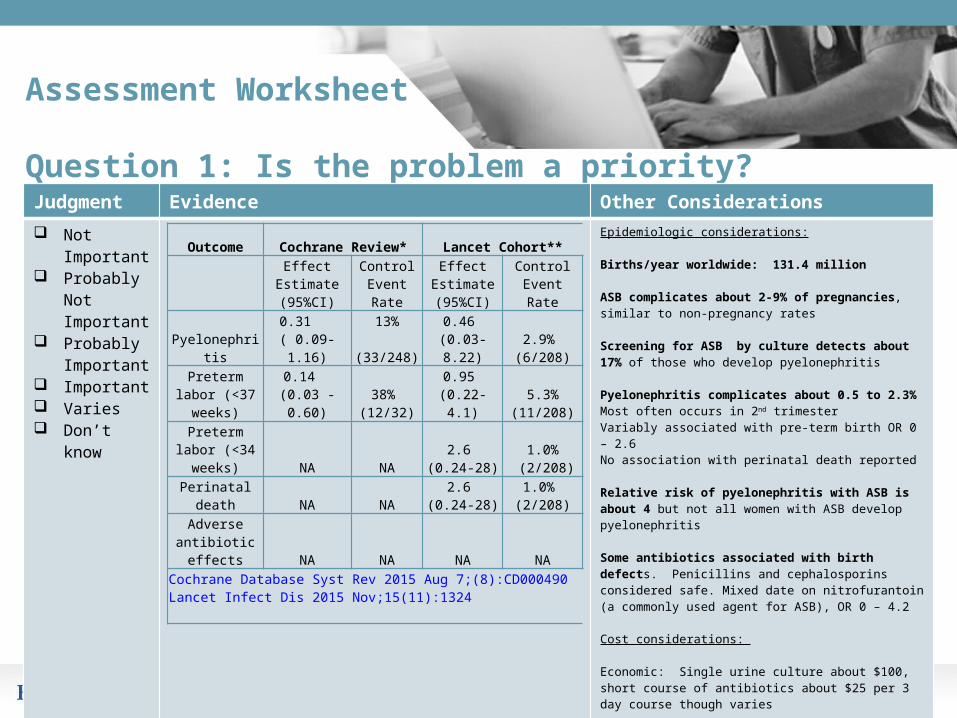
Assessment Worksheet
Question 1: Is the problem a priority? Judgment Evidence Other Considerations Not
Important Probably Not
Important Probably
Important Important Varies Don’t know
Epidemiologic considerations:
Births/year worldwide: 131.4 million
ASB complicates about 2-9% of pregnancies, similar to non-pregnancy rates
Screening for ASB by culture detects about 17% of those who develop pyelonephritis
Pyelonephritis complicates about 0.5 to 2.3%Most often occurs in 2nd trimesterVariably associated with pre-term birth OR 0 – 2.6No association with perinatal death reported
Relative risk of pyelonephritis with ASB is about 4 but not all women with ASB develop pyelonephritis
Some antibiotics associated with birth defects. Penicillins and cephalosporins considered safe. Mixed date on nitrofurantoin (a commonly used agent for ASB), OR 0 – 4.2
Cost considerations:
Economic: Single urine culture about $100, short course of antibiotics about $25 per 3 day course though varies
Ecologic: ASB treatment is associated with higher rates antibiotic resistant bacteria
Outcome Cochrane Review* Lancet Cohort**
Effect Estimate (95%CI)
Control Event Rate
Effect Estimate (95%CI)
Control Event Rate
Pyelonephritis 0.31
( 0.09-1.16)13%
(33/248)0.46
(0.03-8.22)2.9%
(6/208)
Preterm labor (<37 weeks)
0.14 (0.03 - 0.60)
38% (12/32)
0.95 (0.22-4.1)
5.3% (11/208)
Preterm labor (<34 weeks) NA NA
2.6 (0.24-28)
1.0% (2/208)
Perinatal death NA NA2.6
(0.24-28)1.0%
(2/208)Adverse antibiotic effects NA NA NA NA
Cochrane Database Syst Rev 2015 Aug 7;(8):CD000490Lancet Infect Dis 2015 Nov;15(11):1324
Assessment Worksheet
Questions 2 & 3: How substantial are the anticipated desirable and undesirable effects?Judgment Evidence Other Considerations
Large Moderate Small Trivial Varies Don’t know
Desirable outcomes:Prevention of pyelonephritisPrevention of preterm laborPrevention of perinatal death
Undesirable outcomes:Adverse effects of antibiotic use

Assessment Worksheet
Question 4: What is the overall certainty of the evidence?
Judgment Evidence Other Considerations
Very Low Low Moderate High No included
studies
Cochrane: Each of the 3 included randomized trials evaluating pyelonephritis was performed between 1960 and 1987 when standardized testing, methods of gestational data and access to care differed limiting generalizability to modern day. The 1 randomized trial evaluating preterm birth focused only on Group B streptococcus which may have different clinical implications. All included trials had several methodologic limitations including lack of blinding, incomplete descriptions of methods, selective and/or incomplete reporting..
Lancet Infectious Diseases: This trial was underpowered to detect significant differences in outcomes
Assessment Worksheet
Question 5: Is there uncertainty about or variability in how much people value the outcomes ?Judgment Evidence Other Considerations
Yes Probably not Possibly No No known
undesirable outcomes
The strategy to screen and treat has been widely employed in the United States and has been traditionally accepted by most obstetricians and infectious disease specialists.
By contrast, in the 2015 Lancet Infectious Diseases cohort study, performed in the Netherlands, 163 women with asymptomatic bacteriuria chose not to be a part of the randomized trial. 94% of these women refused participation because they did not want to receive antibiotics during pregnancy for asymptomatic condition

Assessment Worksheet
Question 6: Does the balance between desirable and undesirable effects favor the intervention or comparison?Judgement Evidence Other Considerations
Favors comparison
Probably favors comparison
Does not favor either
Probably favors intervention
Varies Don’t know

Assessment Worksheet
Question 7: Is the intervention acceptable to key stakeholders?Judgment Evidence Other Considerations
Unacceptable Probably not
acceptable Probably
acceptable Acceptable Varies Don’t know
Assessment Worksheet
Question 8: Is the intervention feasible to implement?
Judgment Evidence Other Considerations
Not feasible Probably not
feasible Probably
feasible Feasible Varies Don’t know

Worksheet 2:
Summary of JudgmentsJudgments
ImportanceNot important Probably
not importantProbably important Important Varies Don't know
Desirable effectsTrivial Small Moderate Large Varies Don't know
Undesirable EffectsLarge Moderate Small Trivial Varies Don't know
Certainty of EvidenceVery low Low Moderate High No
included studies
Important uncertainty of variability Yes Possibly Probably Not No
No known undesirable outcomes
Balance of Effects
Favors comparison
Probably favors
comparison
Does not favor either
Probably favors
intervention
Favors intervention Varies Don't know
AcceptabilityUnacceptable Probably
not acceptableProbably
acceptable Acceptable Varies Don't know
Feasibility Not feasible Probably not feasible
Probably feasible Feasible Varies Don't know

Worksheet 3:
Conclusions
Should women be screened and treated with a 3 - 7 day course of antibiotics for pyelonephritis in early pregnancy?
Type of recommendation
Strong recommendation
against intervention
Conditional recommendation
against intervention
Conditional recommendation
either for or against intervention
Conditional recommendation
for the intervention
Strong recommendation
for the intervention
No recommendation
Recommendation
Justification
Implementation considerations
Other considerations

Questions?

Thank you!And thanks to the DynaMed Editorial Team:
Brian Alper, MD, FounderKevin Loughlin, MD, CMO
Meghan Malone-Moses, MPHJill Angelosanto, PhD
Karen Clarke, PhD, MSPeter Lindgren, PhD
Christine Colpitts, MA, CRTTJames Forgione, PharmD
Catherine McQueen
BibliographyEpidemiologic Data:1. Farkash E, Wientraub AY, Sergienko R, et al. Acute antepartum pyelonephritis in pregnancy: a critical analysis of risk factors and outcomes. Eur J Obstet
Gynecol Reprod Biol. 2012;162:24–7. 2. Gravett MG, Martin ET, Bernson JD, et al. Serious and life-threatening pregnancy-related infections: opportunities to reduce the global burden. Plos
Med.2012;9:e1001324. 3. Mazor-Dray E, Levy A, Schlaeffer F, Sheiner E. Maternal urinary tract infection: is it independently associated with adverse pregnancy outcome? J Matern
Fetal Neonatal Med. 2009;22:124–324. Sharma P, Thapa L. Acute pyelonephritis in pregnancy: a retrospective study. Aust N Z J Obstet Gynaecol. 2007;47:313–59;22:124–325. Chen YK, Chen SF, Li HC, Lin HC. No increased risk of adverse pregnancy outcomes in women with urinary tract infections: a nationwide population-based
study. Acta Obstet Gynecol Scand. 2010;89:882–86. Conde-Agudelo A, Villar J, Lindheimer M. Maternal infection and risk of preeclampsia: systematic review and metaanalysis. Am J Obstet
Gynecol. 2008;198:7–22.7. Beck S, Wojdyla D, Say L, et al. The worldwide incidence of preterm birth: a systematic review of maternal mortality and morbidity. Bull World Health
Organ.2010;88:31–8.
Birth defects and antibiotic use:8. Crider KS, Cleves MA, Reefhuis J, et al. Antibacterial medication use during pregnancy and risk of birth defects. National Birth Defects Prevention Study. Arch
Pediatr Adolesc Med. 2009;163:978–85.9. Sulfonamides, nitrofurantoin, and risk of birth defects. Committee Opinion No. 494. American College of Obstetricians and Gynecologists. Obstet
Gynecol. 2011;117:1484–5.10. Nordeng H, Lupattelli A, Romøren M, Koren G. Neonatal outcomes after gestational exposure to nitrofurantoin. Obstet Gynecol. 2013;121:306–13.11. Kenyon S, Pike K, Jones DR, et al. Childhood outcomes after prescription of antibiotics to pregnant women with spontaneous preterm labour: 7-year follow-up
of the ORACLE II trial. Lancet. 2008;372:1319–27.
Antimicrobial resistance in the treatment of ASB:12. Rizvi M, Khan F, Shukla, et al. Rising prevalence of antimicrobial resistance in urinary tract infections during pregnancy: necessity for exploring newer
treatment options. J Lab Physicians. 2011;3:98–10313. Cai T, Nesi G, Mazzoli S, Meacci F, Lanzafame P, Caciagli P, Mereu L, Tateo S, Malossini G, Selli C, Bartoletti R. Asymptomatic bacteriuria treatment is
associated with a higher prevalence of antibiotic resistant strains in women with urinary tract infections. Clin Infect Dis. 2015 Dec 1;61(11):1655-61

GuidelinesOrganization Date Recommendation Grade
Infectious Diseases Society of America (IDSA) 2005 Screen all pregnant women by urine culture at least once early in pregnancy (around 12-16 weeks) and treat if culture positive
IDSA Grade A-I
United States Preventive Services Task Force (USPSTF)
2008 Screen all pregnant women for asymptomatic bacteriuria using urine culture at 12-16 weeks gestation
USPSTF Grade A
National Institute for Health and Care Excellence (NICE)
2008 Offer routine screening for asymptomatic bacteriuria by midstream culture early in pregnancy, as identification and treatment reduces risk of pyelonephritis
No rating applied
American Academy of Pediatrics (AAP) and American College of Obstetricians and Gynecologists (ACOG)
2012 If urine culture performed early in pregnancy, treat asymptomatic bacteriuria and do test of cure
No rating applied
Society of Obstetricians and Gynaecologists of Canada (SOGC)
2012 Treat any bacteriuria with colony counts 100,000 ≥ CFU/mL in pregnancy with appropriate antibiotics
SOGC Grade II-2A
Scottish Intercollegiate Guidelines Network (SIGN) 2012 Treat asymptomatic bacteriuria detected in pregnant women with an antibiotic
SIGN Grade A
European Association of Urology (EAU) 2015 No recommendation made Not applicableAbbreviation: CFU, colony-forming units.
References - EAU 2015 Mar, AAP and ACOG 2012, J Obstet Gynaecol Can 2012 May;34(5):482, SIGN 2012 Jul PDF, Ann Intern Med 2008 Jul 1;149(1):43, NICE 2008 Mar, Clin Infect Dis 2005 Mar 1;40(5):643

Appendix

Definitions
Asymptomatic bacteruria presence of bacteria in the urine in the absence of symptomsdiagnosis of ASB is made when ≥ 105 colony-forming units (CFU)/mL of a single bacterial strain isolated from 2 consecutive voided urine specimens
Pyelonephritis infection of kidney
Preterm Labor World Health OrganizationModerate to late preterm: 32 to <37 weeksVery preterm: 28 to <32 weeksExtremely preterm: <28 weeks
Centers for Disease Control and Prevention Preterm: <37 weeksLate preterm: 34 to 36 weeksEarly preterm: <34 weeks
34 weeks is the threshold at which perinatal morbidity and mortality are too low to justify the potential maternal and fetal complications and costs associated with inhibition of preterm labor, which only results in short-term delay in delivery

Step 4:
Summarize the evidence for each outcome
Comparison of antibiotic vs. no treatment for the development of pyelonephritis
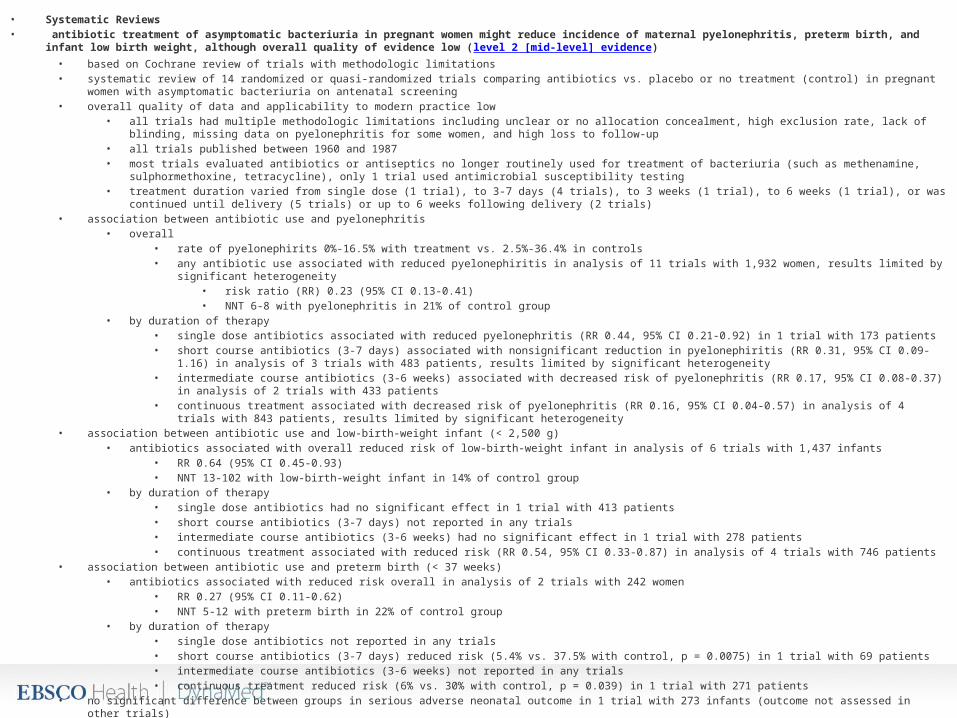
• Systematic Reviews• antibiotic treatment of asymptomatic bacteriuria in pregnant women might reduce incidence of maternal pyelonephritis, preterm birth, and infant low birth weight, although
overall quality of evidence low (level 2 [mid-level] evidence)• based on Cochrane review of trials with methodologic limitations• systematic review of 14 randomized or quasi-randomized trials comparing antibiotics vs. placebo or no treatment (control) in pregnant women with asymptomatic bacteriuria on
antenatal screening• overall quality of data and applicability to modern practice low
• all trials had multiple methodologic limitations including unclear or no allocation concealment, high exclusion rate, lack of blinding, missing data on pyelonephritis for some women, and high loss to follow-up
• all trials published between 1960 and 1987• most trials evaluated antibiotics or antiseptics no longer routinely used for treatment of bacteriuria (such as methenamine, sulphormethoxine, tetracycline), only 1 trial used
antimicrobial susceptibility testing• treatment duration varied from single dose (1 trial), to 3-7 days (4 trials), to 3 weeks (1 trial), to 6 weeks (1 trial), or was continued until delivery (5 trials) or up to 6 weeks
following delivery (2 trials)• association between antibiotic use and pyelonephritis
• overall• rate of pyelonephirits 0%-16.5% with treatment vs. 2.5%-36.4% in controls• any antibiotic use associated with reduced pyelonephiritis in analysis of 11 trials with 1,932 women, results limited by significant heterogeneity
• risk ratio (RR) 0.23 (95% CI 0.13-0.41)• NNT 6-8 with pyelonephritis in 21% of control group
• by duration of therapy• single dose antibiotics associated with reduced pyelonephritis (RR 0.44, 95% CI 0.21-0.92) in 1 trial with 173 patients• short course antibiotics (3-7 days) associated with nonsignificant reduction in pyelonephiritis (RR 0.31, 95% CI 0.09-1.16) in analysis of 3 trials with 483 patients,
results limited by significant heterogeneity• intermediate course antibiotics (3-6 weeks) associated with decreased risk of pyelonephritis (RR 0.17, 95% CI 0.08-0.37) in analysis of 2 trials with 433 patients• continuous treatment associated with decreased risk of pyelonephritis (RR 0.16, 95% CI 0.04-0.57) in analysis of 4 trials with 843 patients, results limited by
significant heterogeneity• association between antibiotic use and low-birth-weight infant (< 2,500 g)
• antibiotics associated with overall reduced risk of low-birth-weight infant in analysis of 6 trials with 1,437 infants• RR 0.64 (95% CI 0.45-0.93)• NNT 13-102 with low-birth-weight infant in 14% of control group
• by duration of therapy• single dose antibiotics had no significant effect in 1 trial with 413 patients• short course antibiotics (3-7 days) not reported in any trials• intermediate course antibiotics (3-6 weeks) had no significant effect in 1 trial with 278 patients• continuous treatment associated with reduced risk (RR 0.54, 95% CI 0.33-0.87) in analysis of 4 trials with 746 patients
• association between antibiotic use and preterm birth (< 37 weeks)• antibiotics associated with reduced risk overall in analysis of 2 trials with 242 women
• RR 0.27 (95% CI 0.11-0.62)• NNT 5-12 with preterm birth in 22% of control group
• by duration of therapy• single dose antibiotics not reported in any trials• short course antibiotics (3-7 days) reduced risk (5.4% vs. 37.5% with control, p = 0.0075) in 1 trial with 69 patients• intermediate course antibiotics (3-6 weeks) not reported in any trials• continuous treatment reduced risk (6% vs. 30% with control, p = 0.039) in 1 trial with 271 patients
• no significant difference between groups in serious adverse neonatal outcome in 1 trial with 273 infants (outcome not assessed in other trials)• Reference - Cochrane Database Syst Rev 2015 Aug 7;(8):CD000490
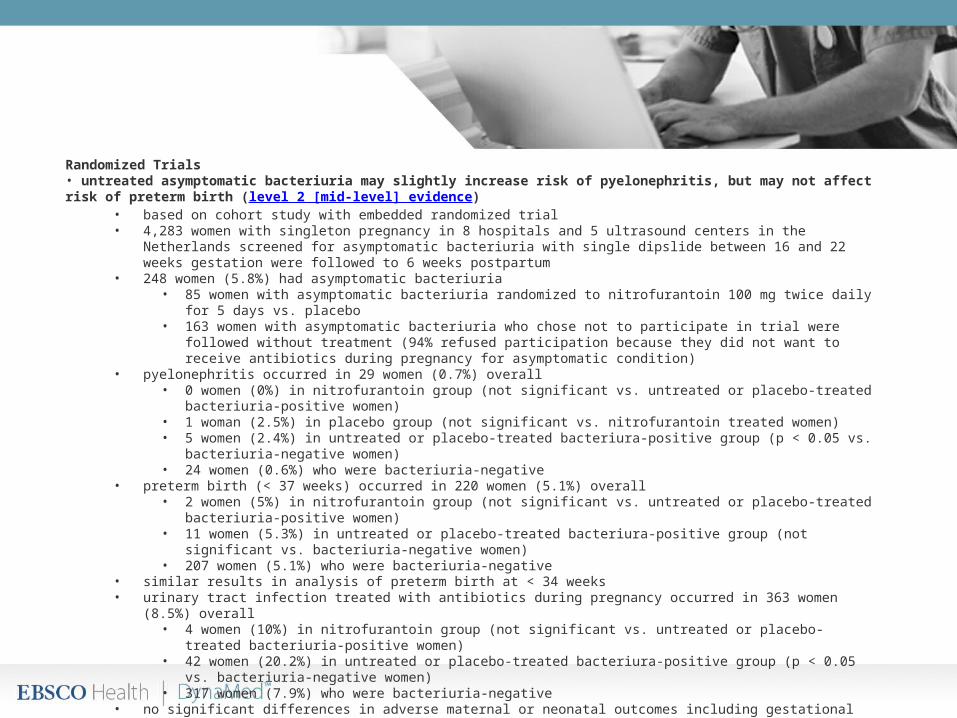
Randomized Trials• untreated asymptomatic bacteriuria may slightly increase risk of pyelonephritis, but may not affect risk of preterm birth (level 2 [mid-level] evidence)
• based on cohort study with embedded randomized trial• 4,283 women with singleton pregnancy in 8 hospitals and 5 ultrasound centers in the Netherlands screened for asymptomatic
bacteriuria with single dipslide between 16 and 22 weeks gestation were followed to 6 weeks postpartum• 248 women (5.8%) had asymptomatic bacteriuria
• 85 women with asymptomatic bacteriuria randomized to nitrofurantoin 100 mg twice daily for 5 days vs. placebo• 163 women with asymptomatic bacteriuria who chose not to participate in trial were followed without treatment (94%
refused participation because they did not want to receive antibiotics during pregnancy for asymptomatic condition)• pyelonephritis occurred in 29 women (0.7%) overall
• 0 women (0%) in nitrofurantoin group (not significant vs. untreated or placebo-treated bacteriuria-positive women)• 1 woman (2.5%) in placebo group (not significant vs. nitrofurantoin treated women)• 5 women (2.4%) in untreated or placebo-treated bacteriura-positive group (p < 0.05 vs. bacteriuria-negative women)• 24 women (0.6%) who were bacteriuria-negative
• preterm birth (< 37 weeks) occurred in 220 women (5.1%) overall• 2 women (5%) in nitrofurantoin group (not significant vs. untreated or placebo-treated bacteriuria-positive women)• 11 women (5.3%) in untreated or placebo-treated bacteriura-positive group (not significant vs. bacteriuria-negative
women)• 207 women (5.1%) who were bacteriuria-negative
• similar results in analysis of preterm birth at < 34 weeks• urinary tract infection treated with antibiotics during pregnancy occurred in 363 women (8.5%) overall
• 4 women (10%) in nitrofurantoin group (not significant vs. untreated or placebo-treated bacteriuria-positive women)• 42 women (20.2%) in untreated or placebo-treated bacteriura-positive group (p < 0.05 vs. bacteriuria-negative
women)• 317 women (7.9%) who were bacteriuria-negative
• no significant differences in adverse maternal or neonatal outcomes including gestational diabetes, pregnancy-induced hypertension, preeclampsia, kidney stones, mean birth weight, small for gestational age, perinatal death, or admission to neonatal intensive care unit
• Reference - Lancet Infect Dis 2015 Nov;15(11):1324