1 bone marker-directed dosing of zoledronic acid for the...
TRANSCRIPT

Raje et al Z-MARK Study Primary Manuscript
1
Bone Marker-Directed Dosing of Zoledronic Acid for the Prevention of Skeletal 1
Complications in Patients With Multiple Myeloma: Results of the Z-MARK Study 2
3
Noopur Raje1, Robert Vescio2, Charles W. Montgomery3, Ashraf Badros4, Nikhil 4
Munshi5, Richard Orlowski6, Joseph T. Hadala7, Ghulam Warsi7, Eliza Argonza-Aviles7, 5
Solveig G. Ericson7, and Kenneth C. Anderson8 6
7
1Massachusetts General Hospital Cancer Center and Harvard Medical School, Boston, 8
Massachusetts, USA. 2Cedars-Sinai Samuel Oschin Comprehensive Cancer Center, 9
Los Angeles, California, USA. 3Hematology and Oncology Associates, Tupelo, 10
Mississippi, USA. 4University of Maryland – Baltimore, Marlene and Stewart 11
Greenebaum Cancer Center, Blood and Marrow Transplant Program, Baltimore, 12
Maryland, USA. 5Boston Veterans' Administration Healthcare System, Boston, 13
Massachusetts, USA. 6Carolina Oncology Specialists, Hickory, North Carolina, USA. 14
7Novartis Pharmaceuticals Corporation, East Hanover, New Jersey, USA. 8Dana-15
Farber/Partners Cancer Care Institute, Boston, Massachusetts, USA. 16
Funding Source: Financial support for this study and medical editorial assistance were 17
provided by Novartis Pharmaceuticals Corporation. 18
Running Title (≤ 50 characters): Zoledronic Acid and Skeletal-Related Events in MM 19
Research. on June 30, 2018. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on December 7, 2015; DOI: 10.1158/1078-0432.CCR-15-1864
Raje et al Z-MARK Study Primary Manuscript
2
Corresponding Author: Noopur Raje, Director, Multiple Myeloma Program, 20
Massachusetts General Hospital Cancer Center, 55 Fruit Street, POB216, Boston, 21
Massachusetts, 02114, USA. Phone: 617-726-0711; Fax: 617-724-6801; E-mail: 22
24
Previous Publication: Portions of these data were presented at the 54th American 25
Society of Hematology Annual Meeting and Exposition; December 8 to 11, 2012; 26
Atlanta, Georgia, USA (abstract 4077) and the 52nd American Society of Hematology 27
Annual Meeting and Exposition; December 4 to 7, 2010; Orlando, Florida, USA 28
(abstract 2971). 29
30
Trial Registration: ClinicalTrials.gov:NCT00622505 31
(http://clinicaltrials.gov/ct2/show/NCT00622505) 32
33
Keywords: zoledronic acid, myeloma, bone lesion, skeletal-related event, 34
bisphosphonate 35
Word Count (limit 4000): 3072 36
Figures/tables (limit 6, not counting consort): 5 (3 tables, 2 figures) 37
References (no limit): 24 38
39
Research. on June 30, 2018. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on December 7, 2015; DOI: 10.1158/1078-0432.CCR-15-1864
Raje et al Z-MARK Study Primary Manuscript
3
Author Disclosures 40
Noopur Raje: Received consulting fees from Millenium, Celgene, Amgen, and Onyx, 41
and research funding from Acetylon and Eli Lilly 42
Robert Vescio: Received honoraria as member of Novartis Speaker's Bureau 43
Charles W. Montgomery: None 44
Ashraf Badros: None 45
Nikhil Munshi: Received consulting fee for Celgene, Janssen, and Onyx 46
Richard Orlowski: None 47
Joseph T. Hadala: Novartis employee 48
Ghulam Warsi: Novartis employee 49
Eliza Argonza-Aviles: Novartis employee 50
Solveig G. Ericson: Novartis employee 51
Kenneth C. Anderson: Received consulting fees from Millennium, Celgene, Gilead, 52
Sanofi-Aventis and Onyx; scientific founder of Acetylon and Oncopep 53
54
Research. on June 30, 2018. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on December 7, 2015; DOI: 10.1158/1078-0432.CCR-15-1864

Raje et al Z-MARK Study Primary Manuscript
4
Authors’ Contributions 55
Conception and design: N Raje, K C Anderson, Novartis authors 56
Collection and assembly of data: R Orlowski, R Vescio, C Montgomery, A Badros, N 57
Munshi, Novartis authors 58
Data analysis and interpretation: N Raje, K C Anderson, Novartis authors 59
Administrative support: Novartis authors 60
Provision of study materials or patients: N Raje, K C Anderson, N Munshi, R Vescio, C 61
W Montgomery, A Badros, R Orlowski 62
Manuscript writing: All authors 63
Final approval of manuscript: All authors 64
Research. on June 30, 2018. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on December 7, 2015; DOI: 10.1158/1078-0432.CCR-15-1864

Raje et al Z-MARK Study Primary Manuscript
5
Translational Relevance 65
Zoledronic acid is indicated for the treatment of patients with multiple myeloma in 66
conjunction with standard antineoplastic therapy. Although standard monthly infusions 67
are effective in reducing the risk of skeletal complications, patients with normal bone 68
metabolism may not require as intense a treatment schedule as patients with 69
accelerated bone resorption. A reduced dosing schedule of every 12 weeks may be 70
adequate for patients with normal bone metabolism and may mitigate long-term toxicity. 71
This study evaluated a tailored approach to zoledronic acid therapy that aimed at 72
maximizing the benefit-risk ratio and allowing an effective, less frequent dosing based 73
on bone turnover marker, urinary N-telopeptide of type I collagen (uNTX). In this study, 74
the low skeletal-related event (SRE) rate maintained with for every 12-week dosing 75
support the efficacy of less frequent zoledronic acid dosing in patients with multiple 76
myeloma who have already received 1 to 2 years of prior intravenous bisphosphonate 77
therapy. 78
79
Research. on June 30, 2018. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on December 7, 2015; DOI: 10.1158/1078-0432.CCR-15-1864

Raje et al Z-MARK Study Primary Manuscript
6
Abstract 80
Background: Zoledronic acid (ZOL) given every 3 to 4 weeks can reduce skeletal-81
related events (SREs) in patients with bone lesions from multiple myeloma. This study 82
evaluated efficacy and safety of less-frequent ZOL dosing based on bone turnover 83
markers in patients with 1 to 2 years of prior bisphosphonate therapy. 84
Methods: Patients received ZOL (4 mg) every 4 or 12 weeks based on urinary N-85
telopeptide of type 1 collagen (uNTX) levels (every 4 weeks if uNTX ≥50 nmol/mmol 86
creatinine, every 12 weeks if uNTX <50). 87
Results: Of 121 patients enrolled (mean age, 63.8 years; median follow-up, 21 88
months), 4 patients started ZOL every 4 weeks and 117 received ZOL every 12 weeks 89
based on uNTX at study entry. All 4 patients who initiated ZOL every 4 weeks switched 90
to every 12 weeks due to decreased uNTX. Thirty-eight of 117 patients who initiated 91
ZOL every 12 weeks switched to ZOL every 4 weeks due to disease progression 92
(n=20), increased uNTX (n=14), and SREs (n=4). Overall SRE incidence was low; 7 93
(5.8%) and 5 (4.9%) patients experienced an SRE during years 1 and 2, respectively. 94
Mean (SD) SRE rate at year 2 was 0.01 (0.03) per person-year. The 2-year incidence 95
rate for osteonecrosis of jaw was 3.3%. Four deaths were reported, none related to 96
ZOL. 97
Conclusion: Less frequent ZOL dosing (every 12 weeks over 2 years) maintains a low 98
SRE rate and can be safely administered for up to 4 years. 99
ClinicalTrials.gov registration: NCT00622505 100
Word Count (limit 250): 238 101
Research. on June 30, 2018. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on December 7, 2015; DOI: 10.1158/1078-0432.CCR-15-1864

Raje et al Z-MARK Study Primary Manuscript
7
Introduction 102
Approximately, 80% of patients with newly diagnosed multiple myeloma (MM) 103
have skeletal involvement and are at increased risk for skeletal complications (1,2). The 104
increased rate of bone resorption and suppressed bone formation associated with 105
myeloma bone lesions severely impairs normal skeletal homeostasis. This often results 106
in debilitating skeletal-related events (SREs) including pathologic fracture of bone, 107
spinal cord compression, hypercalcemia of malignancy (HCM), and the need for 108
radiation therapy or surgery to bone (3-5). These SREs have a negative effect on quality 109
of life and significantly increase morbidity and mortality. 110
Current treatment guidelines recommend intravenous (IV) bisphosphonate 111
therapy to delay the onset and reduce the risk of SREs (6-8). Although not routinely 112
used in clinical practice, the pharmacological effect of IV bisphosphonate therapy can 113
be assessed by measuring circulating levels of bone resorption markers, including urine 114
N-telopeptide of type 1 collagen (uNTX). Several studies have demonstrated that NTX 115
levels correlate significantly with the extent of bone involvement in MM (9,10), wherein 116
higher levels are associated with increased risk for skeletal complications and disease 117
progression. 118
To date, zoledronic acid is the only bisphosphonate with widespread regulatory 119
approval for reducing the risk and delaying the onset of SREs across a variety of tumor 120
types, including MM. The results of MRC myeloma IX trial support the use of zoledronic 121
acid in patients with newly diagnosed MM regardless of bone disease status at baseline 122
(11). In this setting, zoledronic acid infusions (4 mg, every 3-4 weeks) significantly 123
reduced the risk of SREs, demonstrating a low SRE incidence rate of 27% after a 124
Research. on June 30, 2018. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on December 7, 2015; DOI: 10.1158/1078-0432.CCR-15-1864
Raje et al Z-MARK Study Primary Manuscript
8
median follow-up of 3.7 years (11). In addition, there is clinical evidence to support 125
monthly zoledronic acid dosing to prevent SREs and improve survival, and these data 126
are reflected in current guidelines (6,12). Treatment with zoledronic acid also 127
significantly improved progression-free survival and overall survival by 5.5 months vs 128
clodronate in patients with MM (13). 129
Currently, monthly zoledronic acid therapy is recommended for at least 2 years in 130
patients with active bone disease (6-8); however, there is no guidance regarding the 131
optimum zoledronic acid dosing schedule after the 2-year treatment period. The 132
Zoledronic Acid - Bone MARKer-Directed Dosing (Z-MARK) study evaluated whether 133
patients with MM, who had received 1 to 2 years of prior IV bisphosphonate therapy, 134
would continue to benefit from IV zoledronic acid infusions and if bone turnover markers 135
such as uNTX could guide the frequency of treatment, on a schedule of zoledronic acid 136
every 4 weeks or every 12 weeks. 137
138
Research. on June 30, 2018. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on December 7, 2015; DOI: 10.1158/1078-0432.CCR-15-1864
Raje et al Z-MARK Study Primary Manuscript
9
Methods 139
Z-MARK was a prospective, single-arm, open-label, multicenter study conducted 140
to evaluate clinical benefits of bone marker-directed zoledronic acid dosing in patients 141
with advanced MM (14). This study was conducted in accordance with the Declaration 142
of Helsinki, and all patients gave written informed consent. The protocol was reviewed 143
and approved by an appropriate institutional review board or ethics committee at each 144
participating center. 145
Patients 146
The study included patients (aged ≥18 years) with confirmed diagnosis of MM 147
and life expectancy of ≥9 months. Patients were eligible for enrollment if they were on 148
standard monthly IV bisphosphonate (zoledronic acid or pamidronate) treatment, having 149
received a minimum of 4 doses within 52 to 104 weeks of study entry. Previous 150
standard monthly bisphosphonate treatment had been initiated for treatment of 151
osteolytic lesion, bone fracture, spinal compression, or osteopenia. Patients with an 152
Eastern Cooperative Oncology Group (ECOG) performance status ≤2, serum creatinine 153
<3 mg/dL, and calculated creatinine clearance ≥30 mL/min at screening were included. 154
Key exclusion criteria were known hypersensitivity to zoledronic acid or other 155
bisphosphonates, use of investigational drugs with a significant effect on bone turnover, 156
or a concurrent malignancy or history of a malignancy in the past 2 years except for 157
basal cell or squamous cell skin cancer, cervical carcinoma, or treated early stages of 158
prostate or breast cancer. Patients with current dental issues, recent or planned 159
dental/jaw surgery, and current or prior osteonecrosis of the jaw (ONJ) were excluded. 160
Patients with peripheral blood stem cell/bone marrow transplantation within 2 months 161
Research. on June 30, 2018. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on December 7, 2015; DOI: 10.1158/1078-0432.CCR-15-1864
Raje et al Z-MARK Study Primary Manuscript
10
before treatment or uncontrolled congestive heart failure, hypertension refractory to 162
therapy, with a diagnosis of metabolic bone disease other than osteoporosis, or a 163
diagnosis of primary amyloidosis and immunoglobulin M-related disorders were also 164
excluded. 165
Study Treatment and Assessments 166
Patients received IV zoledronic acid (4 mg) for 96 weeks on a schedule of every 4 167
weeks or every 12 weeks based on the patient’s most recent uNTX measurement. 168
Zoledronic acid administration was carried out on a schedule of every 4 weeks if uNTX 169
levels were ≥50 nmol/mmol creatinine and every 12 weeks if the levels were <50 170
nmol/mmol Cr. Patients could switch to the alternate zoledronic acid dosing schedule 171
while on study based on a change in uNTX level as described above. If patients 172
receiving zoledronic acid every 12 weeks developed an SRE or had disease 173
progression requiring change in antimyeloma therapy, then zoledronic acid was 174
administered every 4 weeks regardless of uNTX level. 175
The primary end point was the proportion of patients who experienced at least 1 176
SRE during study year 1. Secondary end points included the proportions of patients 177
experiencing each type of SRE and SRE rate per patient. SREs were defined as 178
pathologic fracture, radiation therapy to bone, surgery to bone, spinal cord compression, 179
or HCM. SREs were assessed at baseline and on study every 12 weeks during year 1, 180
and by clinical assessments throughout the study period. Other clinical assessments 181
included change from baseline in uNTX. uNTX and urine protein were analyzed by a 182
central laboratory and measured at baseline, every 12 weeks up to week 84, and at the 183
end of study visit (week 100). The dosing schedule was based upon urine NTX 184
Research. on June 30, 2018. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on December 7, 2015; DOI: 10.1158/1078-0432.CCR-15-1864

Raje et al Z-MARK Study Primary Manuscript
11
measurement that is performed every 12 weeks. The patient’s most recent urine NTX 185
measurement was used to determine the next dosing schedule to be implemented. SRE 186
rate per patient was calculated as the number of SREs divided by the time on study for 187
the patient. Bone fractures or vertebral compressions occurring in year 2 were analyzed 188
by a local reader. A bone survey was performed as soon as possible if an SRE occurred 189
(eg, fracture or spinal cord compression) between bone survey visits that were 190
conducted at screening and every 12 weeks during year 1. 191
Safety assessments included recording of adverse events (AEs) and serious AEs 192
(SAEs), collection of clinical laboratory data for hematology and blood chemistry, vital 193
signs, physical condition, electrocardiogram, and pregnancy. 194
Statistical Analysis 195
Sample size determination and power calculation were based on the primary 196
efficacy variable, which was the proportion of patients with ≥1 SRE including HCM at 197
the end of year 1. Assuming that approximately 37% of patients on the bone marker-198
directed dosing schedule would have at least 1 SRE as ascertained by bone surveys 199
during the first year, the sample size required to estimate the proportion using a 95% 200
confidence interval with a half-width of 10% was 90. Assuming a dropout rate of about 201
25%, 31 additional patients were enrolled bringing the total sample size to 121 patients. 202
For each patient, the SRE rate was first calculated as the number of SREs divided by 203
the exposure time in years. The efficacy variables were analyzed in the intent-to-treat 204
population, which included all enrolled patients who received at least 1 dose of study 205
drug and had at least 1 postbaseline assessment. All safety analyses were performed 206
on the safety population, which included all enrolled patients who received at least 1 207
Research. on June 30, 2018. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on December 7, 2015; DOI: 10.1158/1078-0432.CCR-15-1864
Raje et al Z-MARK Study Primary Manuscript
12
dose of study drug. Sample size estimation was performed using nQuery Advisor® 4.0 208
(Statistical Solutions, Boston, MA). 209
210
Research. on June 30, 2018. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on December 7, 2015; DOI: 10.1158/1078-0432.CCR-15-1864
Raje et al Z-MARK Study Primary Manuscript
13
211
Results 212
Patients 213
This study was conducted at 67 centers in the United States. The first patient was 214
enrolled in November 2007; the last patient completed the study in April 2012. Among 215
the 121 patients enrolled, 84% (n=102) and 57% (n=69) completed the first and second 216
year of treatment, respectively (Fig. 1). The reasons for study discontinuation prior to 217
the planned 2-year duration include withdrawal of consent (14%), AEs (13%), elevated 218
serum creatinine levels (7%), administrative problems (5%), death (3%), and abnormal 219
test procedure results consistent with progressive disease (1%). 220
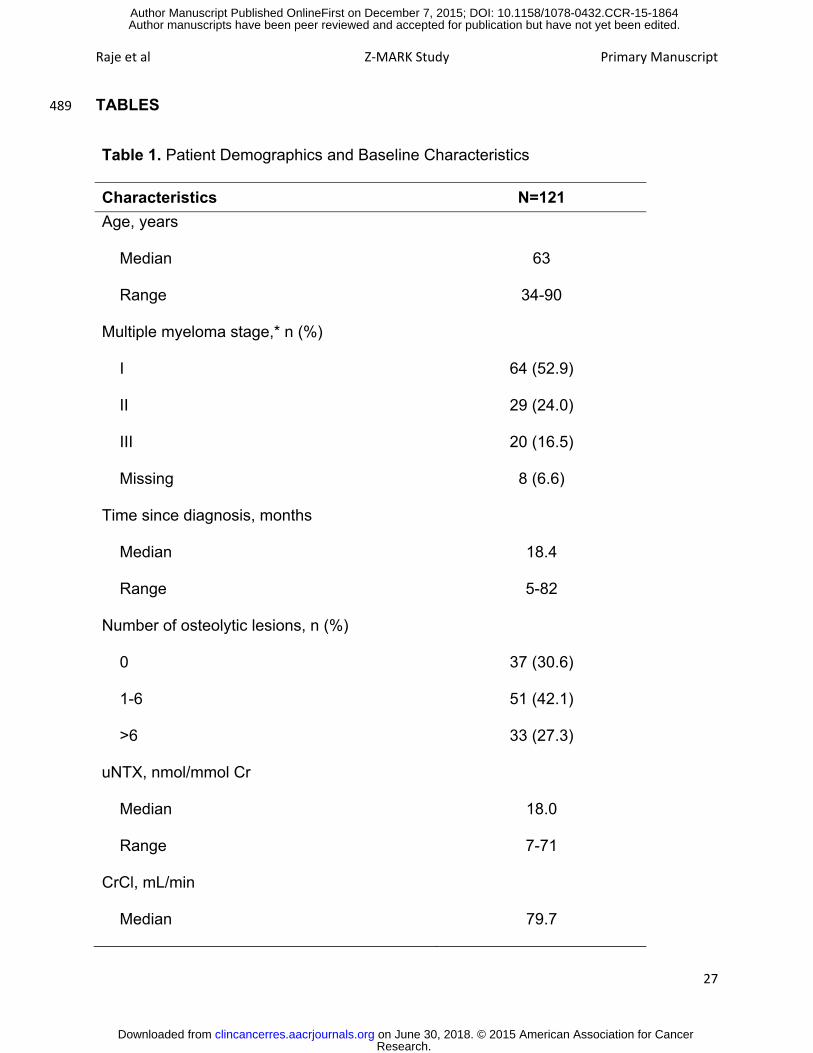
The baseline demographics and clinical characteristics of all enrolled patients are 221
shown in Table 1. Approximately, half of the patients were male (52.9%) and the 222
majority were Caucasians (76.9%), with a mean age of 63.8 years. Half of the patients 223
(52.9%) had stage I MM by the International Staging System. At baseline, 27% of 224
patients had more than 6 osteolytic lesions localized predominantly to the femur (43%), 225
humerus (40.5%), and skull (40.5%). The median duration of prior bisphosphonate 226
therapy was 14 months (range, 1-36 months). Approximately, 86% of patients had 227
received prior zoledronic acid therapy. Overall, 74.4% of patients had experienced ≥1 228
prior SRE, with vertebral fracture reported in 41.3% of patients. 229
At study entry, 4 patients initiated zoledronic acid every 4 weeks and 117 230
patients initiated zoledronic acid every 12 weeks. The median dose per zoledronic acid 231
infusion for both treatment schedules was 4.0 mg (range, 3.9-4.0). All patients received 232
at least 1 zoledronic acid dose, with 87.6% (n=106) of patients receiving at least 11 233
Research. on June 30, 2018. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on December 7, 2015; DOI: 10.1158/1078-0432.CCR-15-1864
Raje et al Z-MARK Study Primary Manuscript
14
zoledronic acid doses (Table 2). Overall, 38 of the 117 patients (32.5%) initially 234
assigned to 12-week dosing switched to 4-week dosing, and the remaining 79 patients 235
continued the 12-week dosing schedule until study completion. The reasons for a 236
change in initial zoledronic acid administration frequency included disease progression 237
(n=20), increased uNTX (n=14), and SREs (n=4). Disease progression was a 238
prespecified protocol criteria for every 4-week dosing. No patient had progressive 239
disease at study entry. Patients who switched to 4-week dosing remained on this 240
schedule for the duration of the study regardless of their subsequent uNTX 241
measurements. 242
Incidence of SREs 243
During the first year on study, 7 of 121 patients (5.8%) experienced at least 1 244
SRE (Fig. 2). Some patients experienced more than 1 SRE, which included pathologic 245
fractures (n=3), spinal cord compressions (n=3), radiation to bone (n=4), surgery to 246
bone (n=1), and HCM (n=1). During the second year on study, 5 of 101 patients (4.9%) 247
experienced at least 1 SRE including 1 event of pathologic fracture and 4 events of 248
radiation to bone. The mean (standard deviation; SD) SRE rate per patient during year 249
1 and 2, including hypercalcemia of malignancy or prior fracture, were 0.01 (0.049) and 250
0.01 (0.031). Of the 11 patients, who had an SRE on study, 6 had SREs while on every 251
12 weeks treatment. 252
Among the 11 patients, who experienced at least 1 on-study SRE, 5 patients had 253
stage I MM, 5 patients had stage II MM, and 1 patient had stage III MM at the time of 254
study entry. Prior antineoplastic therapies reported for these patients included 255
bortezomib, dexamethasone, thalidomide, cyclophosphamide, melphalan, doxorubicin, 256
Research. on June 30, 2018. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on December 7, 2015; DOI: 10.1158/1078-0432.CCR-15-1864

Raje et al Z-MARK Study Primary Manuscript
15
and vincristine. Two of the patients who experienced SREs were subsequently found to 257
have disease progression approximately 4 months after presenting with SREs. 258
Change in uNTX 259
Overall, mean uNTX values generally decreased from baseline throughout the 260
study period. The mean (SD) percentage change from baseline in uNTX was –13.36 261
(47.36) at the end of study (P < 0.001) (Fig. 3). Throughout the study, only 14 patients 262
had uNTX ≥50, and these were observed during the first year of the study and these 263
uNTX levels were moderate to high (range, 50-82 nmol/mmol creatinine). The majority 264
of uNTX shifts observed were from normal to low levels or maintenance of low levels. 265
Analysis using a Cox regression model demonstrated that baseline uNTX level was not 266
predictive of SREs during the first year on study. 267
Safety 268
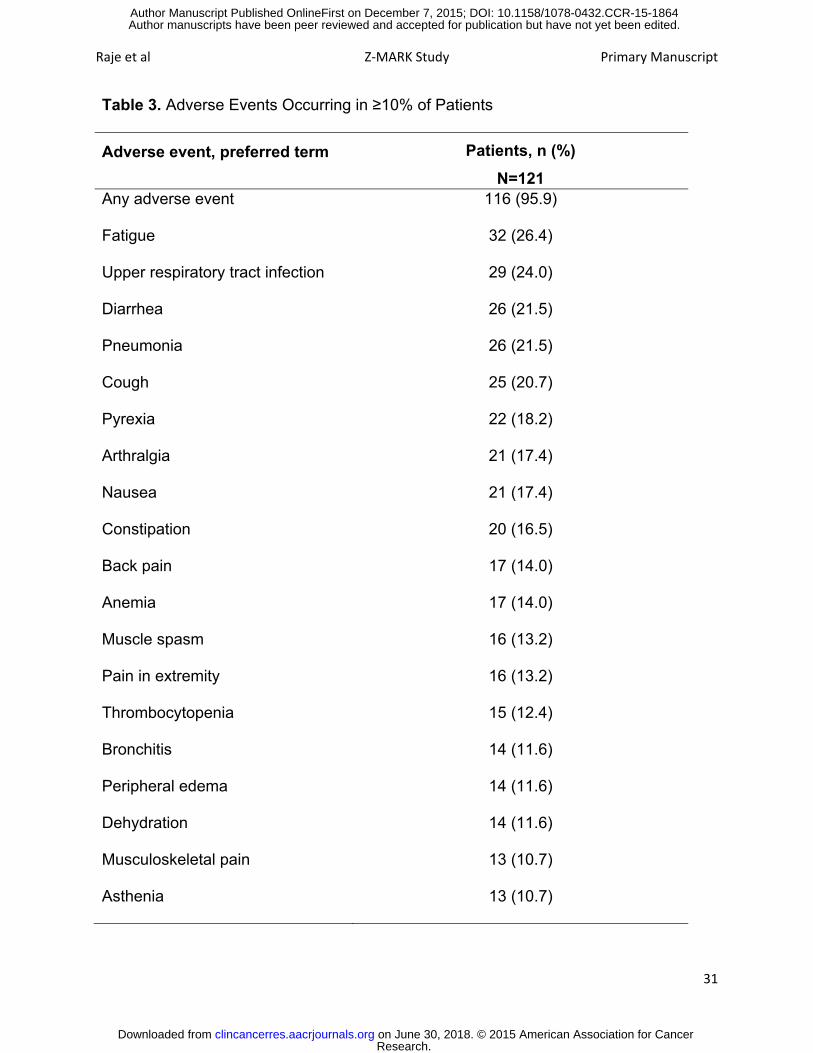
The most frequently reported AEs (all grades) included fatigue (26.4%), upper 269
respiratory tract infection (24.0%), diarrhea (21.5%), and pneumonia (21.5%) (Table 3). 270
Grade 4 AEs were reported in 10.7% of patients and included thrombocytopenia (n=6), 271
neutropenia (n=4), respiratory failure (n=3), cardiac failure (n=3), and leukopenia (n=2). 272
However, only 17 patients (14%) experienced at least 1 AE that was suspected to be 273
related to the study drug. 274
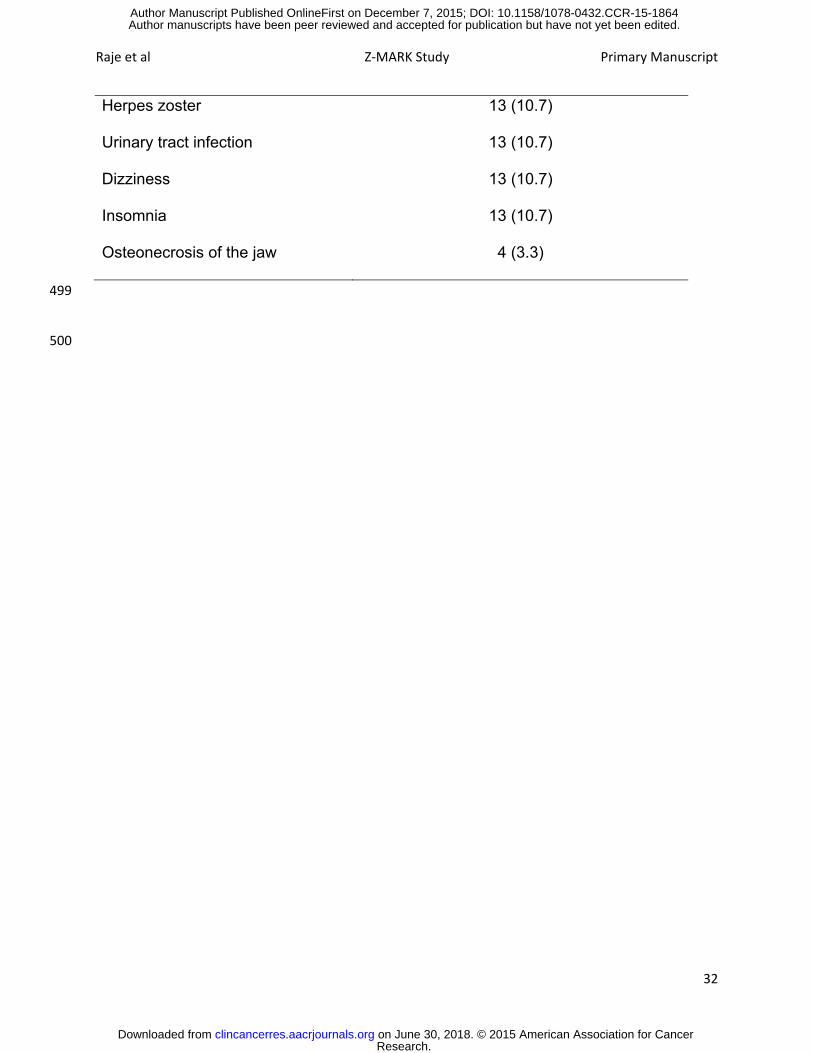
Adverse events leading to zoledronic acid discontinuation occurred in 19.8% of 275
patients, the most common being serum creatinine increase (5%), ONJ (3.3%), and 276
acute renal failure (3.3%). Eleven patients required delay of zoledronic acid 277
administration due to renal function deterioration, as indicated by changes in serum 278
creatinine levels. Mean (SD) urine protein level at baseline was 14.43 (27.64) mg/dL. 279
Research. on June 30, 2018. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on December 7, 2015; DOI: 10.1158/1078-0432.CCR-15-1864
Raje et al Z-MARK Study Primary Manuscript
16
The mean (SD) urine protein change increased from baseline to 34.02 (80.10) mg/dL at 280
study end. The mean (SD) corrected calcium at baseline was 9.36 (0.40) mg/dL. At 281
study end, the mean change in corrected calcium from baseline was 34.02 (80.10) 282
mg/dL. No specific trend was observed in changes over time or shift from baseline to 283
higher or lower corrected calcium levels. 284
Overall, 39.7% of patients had at least 1 SAE during the study. The most 285
common SAEs were pneumonia (9.9%), acute renal failure (4.1%), anemia (3.3%), ONJ 286
(3.3%), and congestive heart failure (3.3%). Fourteen patients (11.6%) discontinued 287
from the study due to SAEs, the most common SAEs resulting in discontinuation of 288
study drug was ONJ (3.3%, n=4) and acute renal failure (3.3%; n=4). The rate of ONJ 289
was 3.3% at the end of 2 years; 1 patient had grade 3 and 3 patients had grade 2 290
events. Except for ONJ, none of the SAEs were suspected to be related to zoledronic 291
acid treatment. Four deaths were reported on study, none of which were suspected to 292
be related to zoledronic acid: 2 from disease progression, 1 from pneumonia, and 1 of 293
unknown cause. 294
295
296
Research. on June 30, 2018. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on December 7, 2015; DOI: 10.1158/1078-0432.CCR-15-1864

Raje et al Z-MARK Study Primary Manuscript
17
Discussion 297
In the Z-MARK trial, only 5.8% of patients experienced at least 1 SRE during the 298
first study year, which was well below the initially expected 37%, despite the fact that 299
the majority of patients received zoledronic acid every 12 weeks. The low incidence of 300
SREs observed in Z-MARK compared with historical controls may be in part due to 301
recent improvements in antimyeloma therapies, which are also known to have bone-302
protective effects. Overall, approximately 32% of patients who started on zoledronic 303
acid dosing every 12 weeks switched to standard monthly dosing. The patients who had 304
disease progression were switched to standard zoledronic acid dosing (every 4 weeks). 305
These data suggest that patients who have already received 1 to 2 years of IV 306
bisphosphonate therapy continue to derive SRE protective effects from less frequent 307
zoledronic acid dosing. This is the first prospective study in patients with MM where the 308
relationship between prolonged therapy with zoledronic acid treatment (3-4 years) and 309
cumulative SRE incidence has been established. However, there is limited data on 310
estimation of SRE reduction rates in patients with multiple myeloma with this duration of 311
bisphosphonate therapy. Low SRE incidence during long-term zoledronic acid therapy 312
has been previously reported in a retrospective claims analysis on 4546 patients with 313
bone metastases from a single tumor type (breast, lung, or prostate cancer) (15). The 314
monthly SRE rate decreased with increased durations of zoledronic acid therapy, with 315
approximately 1 SRE occurring every 9 months in patients receiving zoledronic acid 316
4 mg every 3 to 4 weeks for longer than 1 year (15). 317
Changes in bone turnover markers may provide potential insight into bone 318
destruction rates in patients with malignant bone disease. High baseline NTX serum 319
Research. on June 30, 2018. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on December 7, 2015; DOI: 10.1158/1078-0432.CCR-15-1864

Raje et al Z-MARK Study Primary Manuscript
18
concentrations have been shown to be associated with an increased risk of SREs and a 320
negative effect on survival (16). In this study, mean uNTX values generally decreased 321
throughout the study period. The low levels of uNTX obtained at baseline in patients 322
who had received 1 to 2 years of prior bisphosphonate treatment is consistent with the 323
antiresorptive activity of standard monthly zoledronic acid dosing for 1 to 2 years in 324
patients with advanced disease (17,18). Hence, monthly dosing of zoledronic acid may 325
be needed to suppress aggressive bone resorption as indicated by high NTX levels 326
during initial therapy for bone lesions (19). In patients who had received 1 to 2 years of 327
prior bisphosphonate therapy in Z-MARK, baseline uNTX levels were generally low, with 328
levels above 50 nM in only 4 patients. The low measurements of uNTX obtained as a 329
baseline at study entry for these patients who had had 1 to 2 years of prior ZOL 330
treatment was consistent with reports demonstrating antiresorptive activity of ZOL 331
standard dosing for 1 year [Rosen et al, Cancer. 2001]. These low levels, suggestive of 332
adequate bone suppression, may have contributed to baseline uNTX levels not being 333
predictive of future skeletal complications. Consistent with our findings, a recent 334
exploratory analysis suggests that increases in NTX levels may not precede SREs in 335
zoledronic acid-treated patients with normal baseline NTX levels (20). In addition to the 336
open-label study design, the study has limitations in that uNTX assessments were 337
performed only every 3 months, which may not be frequent enough to capture a rapid 338
increase in uNTX level that may precede an SRE. Of note, the uNTX measurements 339
were not performed at the time of an SRE but were performed at the prespecified every 340
3-month interval. It may be that low-grade bone destruction occurred over several 341
years, resulting in the SREs observed in our study, and that increases in uNTX are not 342
Research. on June 30, 2018. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on December 7, 2015; DOI: 10.1158/1078-0432.CCR-15-1864
Raje et al Z-MARK Study Primary Manuscript
19
detectable even with more frequent monitoring in patients who have been on previous 343
bone antiresorptive therapy. Therefore, the utility of bone resorption markers such as 344
uNTX as a predictive marker after prolonged antiresorptive therapy is questionable and 345
underscores the need to study other novel biomarkers. Another limitation was the fact 346
that patients with progressive disease were switched to a more frequent dosing 347
schedule based on the prespecified protocol requirements. It is therefore unclear if 348
these patients would have done just as well with less frequent dosing of zoledronic acid. 349
The incidence of AEs and SAEs in this trial is consistent with that previously 350
reported for this patient population. Overall, the rate of acute renal failure was low, and 351
no events were suspected to be related to zoledronic acid treatment. In this study, 352
zoledronic acid dose adjustment guidelines based on creatinine clearance appeared to 353
be sufficient to maintain renal tolerability with long-term zoledronic acid treatment. This 354
is consistent with relative renal safety demonstrated in other long-term studies of 355
zoledronic acid in patients with MM (13,20). 356
ONJ has been reported as a complication in patients receiving 357
nitrogen-containing bisphosphonates such as pamidronate and zoledronic acid. In 358
Z-MARK, the prospective analysis of ONJ revealed an incidence rate of 3.3% beyond 3 359
years. This result is consistent with the ONJ incidence (≤5%) reported in long-term 360
studies in patients receiving monthly zoledronic acid treatment for more than 2 years 361
(20,21). ONJ incidence has been shown to increase with longer duration of zoledronic 362
acid exposure and is often triggered by invasive dental procedures or tooth extraction 363
(22). Per treatment guidelines, patients are advised to proactively monitor and maintain 364
Research. on June 30, 2018. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on December 7, 2015; DOI: 10.1158/1078-0432.CCR-15-1864

Raje et al Z-MARK Study Primary Manuscript
20
good oral hygiene by regular dental examinations with preventive dentistry to reduce 365
ONJ risk while receiving zoledronic acid therapy (23,24). 366
In conclusion, Z-MARK is the first trial to provide prospective clinical evidence to 367
support the efficacy of less frequent zoledronic acid dosing during years 3 and 4 in 368
patients who have already received 1 to 2 years of IV bisphosphonate therapy. Although 369
uNTX levels were not predictive of SREs in this patient population, this study provides 370
information about the use of zoledronic acid beyond 2 years of therapy, and it shows 371
that a low SRE rate can be maintained in patients receiving zoledronic acid every 12 372
weeks. The overall low incidence of SREs clearly demonstrates that less frequent ZOL 373
dosing beyond 1 to 2 years continues to provide SRE-prevention benefits and may 374
reflect changing treatment patterns in the context of newer antimultiple myeloma 375
therapies with some bone-protective effects. It, however, also highlights important 376
information demonstrating continued risk of SREs in a patient’s lifetime albeit very low. 377
Further studies will be required to identify other bone turnover markers that can be used 378
as surrogates for predicting SREs and to tailor bone-directed therapy. 379
380
Acknowledgments 381
We thank the patients who took part in this study and the staff at the participating 382
clinical centers. We thank Lakshmi Kasthurirangan, PhD, Novartis Healthcare Pvt. Ltd. 383
and Michael Hobert, PhD, ProEd Communications, Inc, for medical editorial assistance 384
with this manuscript. 385
386
387
Research. on June 30, 2018. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on December 7, 2015; DOI: 10.1158/1078-0432.CCR-15-1864
Raje et al Z-MARK Study Primary Manuscript
21
Disclaimer: The Editor-in-Chief is an author on this article. In keeping with the AACR’s 388
editorial policy, the peer review of this submission was managed by a senior member of 389
Clinical Cancer Research’s editorial team; a member of the AACR Publications 390
Committee rendered the final decision concerning acceptability. 391
392
Research. on June 30, 2018. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on December 7, 2015; DOI: 10.1158/1078-0432.CCR-15-1864

Raje et al Z-MARK Study Primary Manuscript
22
References 393
1. Terpos E, Morgan G, Dimopoulos MA, Drake MT, Lentzsch S, Raje N, et al. 394
International Myeloma Working Group recommendations for the treatment of multiple 395
myeloma-related bone disease. J Clin Oncol 2013;31:2347–57. 396
2. Raje N, Roodman GD. Advances in the biology and treatment of bone disease in 397
multiple myeloma. Clin Cancer Res 2011;17:1278–86. 398
3. Saad F, Lipton A, Cook R, Chen YM, Smith M, Coleman R. Pathologic fractures 399
correlate with reduced survival in patients with malignant bone disease. Cancer 400
2007;110:1860–67. 401
4. Abrahm JL. Assessment and treatment of patients with malignant spinal cord 402
compression. J Support Oncol 2004;2:377–88, 391; discussion 391–73, 398, 401. 403
5. Jacofsky DJ, Haidukewych GJ. Management of pathologic fractures of the 404
proximal femur: State of the art. J Orthop Trauma 2004;18:459–49. 405
6. National Comprehensive Cancer Network: NCCN Clinical practice guidelines in 406
oncology: Multiple myeloma. V2. 2016. 407
http://www.nccn.org/professionals/physician_gls/pdf/myeloma.pdf 408
7. Kyle RA, Yee GC, Somerfield MR, Flynn PJ, Halabi S, Jagannath S, et al. 409
American Society of Clinical Oncology 2007 clinical practice guideline update on the 410
role of bisphosphonates in multiple myeloma. J Clin Oncol 2007;25:2464–72. 411
8. Durie BG. Use of bisphosphonates in multiple myeloma: IMWG response to 412
Mayo Clinic consensus statement. Mayo Clin Proc 2007;82:516–17; author reply 517–413
18. 414
Research. on June 30, 2018. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on December 7, 2015; DOI: 10.1158/1078-0432.CCR-15-1864

Raje et al Z-MARK Study Primary Manuscript
23
9. Tosi P, Zamagni E, Cellini C, Parente R, Cangini D, Tacchetti P et al. First-line 415
therapy with thalidomide, dexamethasone and zoledronic acid decreases bone 416
resorption markers in patients with multiple myeloma. Eur J Haematol 2006;76:399–04. 417
10. Terpos E, Dimopoulos MA, Sezer O, Roodman D, Abildgaard N, Vescio R, et al. 418
The use of biochemical markers of bone remodeling in multiple myeloma: A report of 419
the International Myeloma Working Group. Leukemia 2010;24:1700–12. 420
11. Morgan GJ, Child JA, Gregory WM, Szubert AJ, Cocks K, Bell SE, et al. Effects 421
of zoledronic acid versus clodronic acid on skeletal morbidity in patients with newly 422
diagnosed multiple myeloma (MRC Myeloma IX): Secondary outcomes from a 423
randomised controlled trial. Lancet Oncol 2011;12:743–52. 424
12. Bird JM, Owen RG, D'Sa S, Snowden JA, Pratt G, Ashcroft J, et al. Guidelines 425
for the diagnosis and management of multiple myeloma 2011. Br J Haematol 426
2011;154:32–75. 427
13. Morgan GJ, Davies FE, Gregory WM, Cocks K, Bell SE, Szubert AJ et al. First-428
line treatment with zoledronic acid as compared with clodronic acid in multiple myeloma 429
(MRC Myeloma IX): A randomised controlled trial. Lancet 2010;376:1989–99. 430
14. ClinicalTrials.gov: Zoledronic acid treatment (every 4 or 12 weeks) to prevent 431
skeletal complications in advanced multiple myeloma patients (Z-MARK). Identifier: 432
NCT00622505. http://clinicaltrials.gov/ct2/show/NCT00622505. 433
15. Hatoum HT, Lin SJ, Smith MR, Barghout V, Lipton A. Zoledronic acid and 434
skeletal complications in patients with solid tumors and bone metastases: Analysis of a 435
national medical claims database. Cancer 2008;113:1438–45. 436
Research. on June 30, 2018. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on December 7, 2015; DOI: 10.1158/1078-0432.CCR-15-1864

Raje et al Z-MARK Study Primary Manuscript
24
16. Terpos E, Berenson J, Cook RJ, Lipton A, Coleman RE. Prognostic variables for 437
survival and skeletal complications in patients with multiple myeloma osteolytic bone 438
disease. Leukemia 2010;24:1043–49. 439
17. Rosen LS, Gordon D, Kaminski M, Howell A, Belch A, Mackey J et al. Zoledronic 440
acid versus pamidronate in the treatment of skeletal metastases in patients with breast 441
cancer or osteolytic lesions of multiple myeloma: A phase III, double-blind, comparative 442
trial. Cancer J 2001;7:377–87. 443
18. Rosen LS, Gordon D, Kaminski M, Howell A, Belch A, Mackey J et al. Long-term 444
efficacy and safety of zoledronic acid compared with pamidronate disodium in the 445
treatment of skeletal complications in patients with advanced multiple myeloma or 446
breast carcinoma: A randomized, double-blind, multicenter, comparative trial. Cancer 447
2003;98:1735–44. 448
19. Lipton A, Cook R, Brown J, Body JJ, Smith M, Coleman R. Skeletal-related 449
events and clinical outcomes in patients with bone metastases and normal levels of 450
osteolysis: Exploratory analyses. Clin Oncol (R Coll Radiol) 2013;25:217–26. 451
20. Morgan GJ, Davies FE, Gregory WM, Szubert AJ, Bell SE, Drayson MT, et al. 452
Effects of induction and maintenance plus long-term bisphosphonates on bone disease 453
in patients with multiple myeloma: The Medical Research Council Myeloma IX Trial. 454
Blood 2012;119:5374–83. 455
21. Dimopoulos MA, Kastritis E, Bamia C, Melakopoulos I, Gika D, Roussou M, et al. 456
Reduction of osteonecrosis of the jaw (ONJ) after implementation of preventive 457
measures in patients with multiple myeloma treated with zoledronic acid. Ann Oncol 458
2009;20:117–20. 459
Research. on June 30, 2018. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on December 7, 2015; DOI: 10.1158/1078-0432.CCR-15-1864
Raje et al Z-MARK Study Primary Manuscript
25
22. Ripamonti CI, Maniezzo M, Campa T, Melakopoulos I, Gika D, Roussou M, et al. 460
Decreased occurrence of osteonecrosis of the jaw after implementation of dental 461
preventive measures in solid tumour patients with bone metastases treated with 462
bisphosphonates. The experience of the National Cancer Institute of Milan. Ann Oncol 463
2009;20:137–45. 464
23. Weitzman R, Sauter N, Eriksen EF, Tarassoff PG, Lacerna LV, Dias R, et al. 465
Critical review: Updated recommendations for the prevention, diagnosis, and treatment 466
of osteonecrosis of the jaw in cancer patients – May 2006. Crit Rev Oncol Hematol 467
2007;62:148–52. 468
24. Ruggiero SL, Mehrotra B. Bisphosphonate-related osteonecrosis of the jaw: 469
Diagnosis, prevention, and management. Annu Rev Med 2009;60:85–96. 470
471
472
Research. on June 30, 2018. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on December 7, 2015; DOI: 10.1158/1078-0432.CCR-15-1864
Raje et al Z-MARK Study Primary Manuscript
26
Figure Legends 473
Figure 1. Consort diagram. 474
*If a patient developed an SRE or had disease progression requiring a change in 475
antimyeloma therapy, zoledronic acid was administered every 4 weeks thereafter 476
regardless of uNTX level. †Adverse events that led to discontinuation include back pain, 477
dehydration, diarrhea, acute renal failure, respiratory failure, osteonecrosis of the jaw, 478
and disease progression. Abbreviations: AE, adverse event; Cr, creatinine; ITT, intent-479
to-treat; q, every; SRE, skeletal-related event; uNTX, urine N-telopeptide of type 1 480
collagen. 481
Figure 2. Proportion of patients with any skeletal-related events by year. 482
Abbreviations: N, number of patients; SRE, skeletal-related events. 483
Figure 3. Mean uNTX change from baseline. 484
Error bars are standard errors of the mean. Abbreviations: Cr, creatinine; uNTX, urinary 485
N-telopeptide of type 1 collagen. 486
487
488
Research. on June 30, 2018. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on December 7, 2015; DOI: 10.1158/1078-0432.CCR-15-1864
Raje et al Z-MARK Study Primary Manuscript
27
TABLES 489
Table 1. Patient Demographics and Baseline Characteristics
Characteristics N=121 Age, years
Median
Range
63
34-90
Multiple myeloma stage,* n (%)
I 64 (52.9)
II 29 (24.0)
III 20 (16.5)
Missing 8 (6.6)
Time since diagnosis, months
Median
Range
18.4
5-82
Number of osteolytic lesions, n (%)
0 37 (30.6)
1-6 51 (42.1)
>6 33 (27.3)
uNTX, nmol/mmol Cr
Median
Range
18.0
7-71
CrCl, mL/min
Median 79.7
Research. on June 30, 2018. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on December 7, 2015; DOI: 10.1158/1078-0432.CCR-15-1864

Raje et al Z-MARK Study Primary Manuscript
28
Range 29-228
Prior bisphosphonate therapy, n (%)
Zoledronic acid only 104 (86.0)†
Pamidronate only 12 (9.9)
Zoledronic acid and pamidronate 5 (4.1)
Duration of prior bisphosphonate therapy, months
Median
Range
14.0
1-36
≥1 SRE at enrollment, n (%) 90 (74.4)
Prior SRE type, n (%)
None
Pathologic vertebral fracture
Pathologic nonvertebral fracture
Spinal cord compression
Radiation to bone
Surgery to bone
Hypercalcemia of malignancy
31 (25.6)
50 (41.3)
30 (24.8)
28 (23.1)
30 (24.8)
35 (28.9)
7 (5.8)
Prior antineoplastic therapy, n (%)
Dexamethasone
Melphalan
Lenalidomide
Thalidomide
Cyclophosphamide
80 (66.1)
59 (48.8)
46 (38.0)
43 (35.5)
43 (35.5)
Research. on June 30, 2018. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on December 7, 2015; DOI: 10.1158/1078-0432.CCR-15-1864

Raje et al Z-MARK Study Primary Manuscript
29
Prednisone
Liposomal doxorubicin Doxil/Caelyx
Adriamycin
Vincristine
Other
10 (8.3)
9 (7.4)
3 (2.5)
1 (0.8)
56 (46.3)
Abbreviations: Cr, creatinine; CrCl, creatinine clearance; SRE, skeletal-
related event; uNTX, urinary N-telopeptide of type 1 collagen; zoledronic
acid.
*Based on the International Staging System. 490
†One patient received only one dose of zoledronic acid prior to study entry. This patient was 491
included in the analysis despite this protocol violation, which was documented as no change in 492
risk or outcome. This patient did not experience any SREs. The patient started with q 12 weekly 493
dosing and then switched to q 4 weekly dosing. The patient had prior antineoplastic therapies 494
such as cyclophosphamide, bortezomib, dexamethasone, thalidomide, doxorubicin, etoposide, 495
and melphalan. 496
Research. on June 30, 2018. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on December 7, 2015; DOI: 10.1158/1078-0432.CCR-15-1864

Raje et al Z-MARK Study Primary Manuscript
30
Table 2. Average Zoledronic Acid Dose per Infusion
N=121
Zoledronic acid dose, mg
Median*
25th, 75th percentile
4.0
3.9, 4.0
Number of doses, n (%)
1-5 21 (17.4)
6-10 72 (59.5)
11-15 21 (17.4)
≥16 7 (5.8)
Abbreviation: zoledronic acid, zoledronic acid.
*The median values were calculated based on the average dose per patient.
497
498
Research. on June 30, 2018. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on December 7, 2015; DOI: 10.1158/1078-0432.CCR-15-1864
Raje et al Z-MARK Study Primary Manuscript
31
Table 3. Adverse Events Occurring in ≥10% of Patients
Adverse event, preferred term
Patients, n (%) N=121
Any adverse event 116 (95.9)
Fatigue 32 (26.4)
Upper respiratory tract infection 29 (24.0)
Diarrhea 26 (21.5)
Pneumonia 26 (21.5)
Cough 25 (20.7)
Pyrexia 22 (18.2)
Arthralgia 21 (17.4)
Nausea 21 (17.4)
Constipation 20 (16.5)
Back pain 17 (14.0)
Anemia 17 (14.0)
Muscle spasm 16 (13.2)
Pain in extremity 16 (13.2)
Thrombocytopenia 15 (12.4)
Bronchitis 14 (11.6)
Peripheral edema 14 (11.6)
Dehydration 14 (11.6)
Musculoskeletal pain 13 (10.7)
Asthenia 13 (10.7)
Research. on June 30, 2018. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on December 7, 2015; DOI: 10.1158/1078-0432.CCR-15-1864
Raje et al Z-MARK Study Primary Manuscript
32
Herpes zoster 13 (10.7)
Urinary tract infection 13 (10.7)
Dizziness 13 (10.7)
Insomnia 13 (10.7)
Osteonecrosis of the jaw 4 (3.3)
499
500
Research. on June 30, 2018. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on December 7, 2015; DOI: 10.1158/1078-0432.CCR-15-1864

Remained on ZOL q 12 weeks(n=79)
Completed 2 years on study (n=50)
Discontinued (n=29)AE† (n=9)Withdrew consent (n=12)Abnormal laboratory values (n=3)Administrative problem (n=2)Death (n=2)Abnormal test procedure results (n=1)
Discontinued (n=23)AE† (n=7)Withdrew consent (n=5)Abnormal laboratory values (n=5)Administrative problem (n=4)Death (n=2)
ITT/Safety population (N=121)
Remained on ZOL q 4 weeks(n=42)
Completed 2 years on study(n=19)
Completed 1 year on study (n=63)
Completed 1 year on study (n=39)
uNTX <50 nmol/mmol CrAssigned to ZOL q 12 weeks*
(n=117)
uNTX ≥50 nmol/mmol CrAssigned to ZOL q 4 weeks
(n=4)
Figure 1
Switched to ZOL q 4 weeks Reasons for switch:
Disease progression Increased uNTXSREs
(n=38)
(n=20) (n=14)(n=4)
Assess baseline uNTX
*If a patient developed an SRE or had disease progression requiring a change in anti-myeloma therapy, ZOL was administered every 4 weeks thereafter regardless of uNTX level. †Adverse events that led to discontinuation include back pain, dehydration, diarrhea, acute renal failure, respiratory failure, osteonecrosis of the jaw, and disease progression. Abbreviations: AE, adverse event; Cr, creatinine; ITT, intent-to-treat; q, every; SRE, skeletal-related event; uNTX, urine N-telopeptide of type 1 collagen; ZOL, zoledronic acid.
Consort Diagram
Research. on June 30, 2018. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on December 7, 2015; DOI: 10.1158/1078-0432.CCR-15-1864

0.044
0.046
0.048
0.05
0.052
0.054
0.056
0.058
0.06
0.062
Figure 2
Year 1
5.8%
Year 2
4.9%
Prop
ortio
n of
pat
ient
s w
ith ≥
1 S
RE
N 121 101Proportion of Patients With any Skeletal-Related Events by Year.Abbreviations: N, number of patients; SRE, skeletal-related events.
Research. on June 30, 2018. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on December 7, 2015; DOI: 10.1158/1078-0432.CCR-15-1864

-8
-6
-4
-2
0
2
4Figure 3
12 24 36 48Weeks
Number of patients
60 72 84 100
115 113 105 100 91 86 78 84
Mea
n uN
TX (n
mol
/ mm
ol C
r)ch
ange
from
bas
elin
e
Mean uNTX Change From Baseline. Error bars are standard errors of the mean. Abbreviations: uNTX, urinary N-telopeptide of type-I collagen; Cr, creatinine.
Research. on June 30, 2018. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on December 7, 2015; DOI: 10.1158/1078-0432.CCR-15-1864
Published OnlineFirst December 7, 2015.Clin Cancer Res Raje Noopur, Robert Vescio, Charles W. Montgomery, et al. Myeloma: Results of the Z-MARK StudyPrevention of Skeletal Complications in Patients With Multiple Bone Marker-Directed Dosing of Zoledronic Acid for the
Updated version
10.1158/1078-0432.CCR-15-1864doi:
Access the most recent version of this article at:
Manuscript
Authoredited. Author manuscripts have been peer reviewed and accepted for publication but have not yet been
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/early/2015/12/07/1078-0432.CCR-15-1864To request permission to re-use all or part of this article, use this link
Research. on June 30, 2018. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on December 7, 2015; DOI: 10.1158/1078-0432.CCR-15-1864