1 chapters 12 motor system – cerebellum chris rorden university of south carolina norman j. arnold...
Post on 21-Dec-2015
219 views
TRANSCRIPT

1
Chapters 12 Motor System – Cerebellum
Chris RordenUniversity of South CarolinaNorman J. Arnold School of Public HealthDepartment of Communication Sciences and DisordersUniversity of South Carolina

2
Function of Cerebellum
Error Control Device - Monitor, Quality Control– Monitors outputs to muscles from motor cortex and
sensory signals from receptors– Compares the efferent project plan with execution
at motor action site– Considers related factors and makes adjustments

3
Cerebellum
50% of brain’s neurons, 10% of volumeCan change movements as necessary
– E.G. Walking or talkingDoes not reach conscious awarenessMuscle synergy or coordination monitored Important in running, speaking - all fluid
movements

4
tentorium cerebelli
"tent of the cerebellum" dura mater that
separates the cerebellum from the inferior portion of the occipital lobes.

5
Posterior Cranial Fossa
Fossa is a depression or cavity in the bone
Cerebellum, pons, and medulla oblongata sit in the Posterior cranial fossa

6
Cerebellar Anatomy
Located dorsal to pons and medulla
In posterior fossa under tentorium cerebelli
Lobes– Floccular Nodular(small
fluffy mass)– Anterior– Posterior
Seen from feet
Posterior lobe (I)
Anterior lobe (H)

7
Flattened Cerebellum
Longitudinally separated into hemispheres and cortices– Median (Vermal)
Vermis=worm– Paramedian
(Paravermal)– Lateral

8
Cerebellum
Median Paramedian PrimaryFissure
PosteriorSuperiorFissure
HorizontalFissure
Posterolateral Fissure
Prepyramidal Fissure

9
Cerebellar Nuclei (Nuclei = deep cluster of neurons)
Dentate nucleus– Largest, communicates through cerebellar peduncle – Carries information important for coordination of limb
movements (along with the motor cortex and basal ganglia)
Emboliform nucleus (medial side of the nucleus dentatus)
– Regulates movements of ipsilateral extremity Globose nucleus
– Regulates movements of ipsilateral extremity Fastigial nucleus
– Regulates body posture– Is related to the flocculo nodular lobe
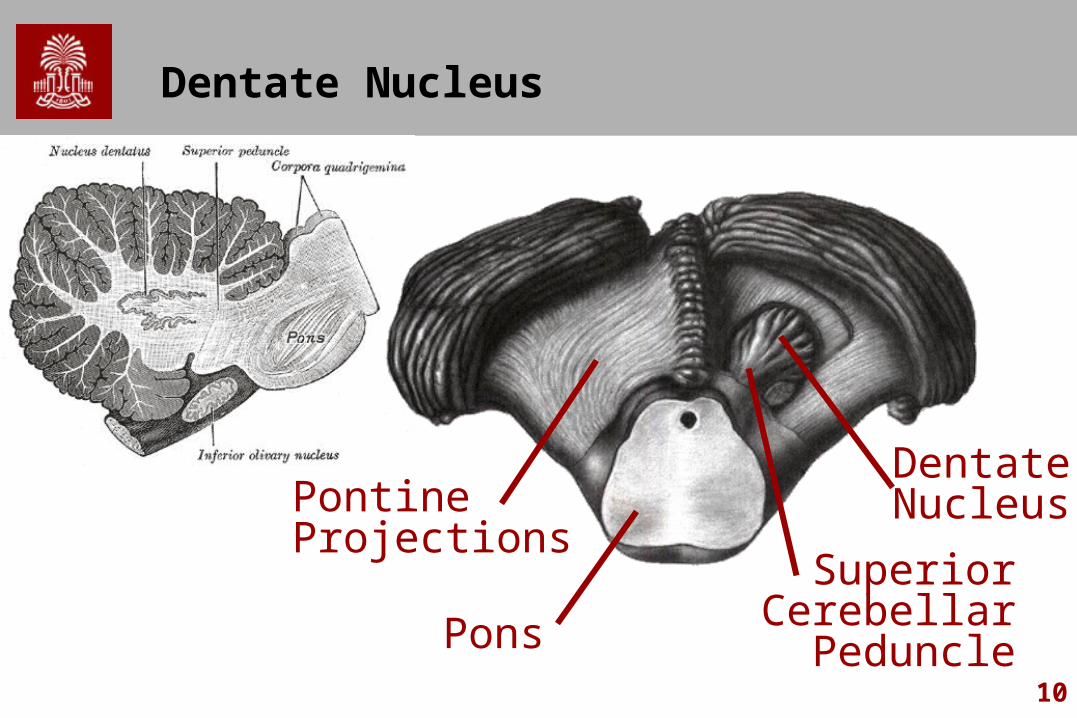
10
Dentate Nucleus
Pons
PontineProjections
DentateNucleus
SuperiorCerebellarPeduncle

11
Somatotopic Organization
Tactile information– Ipsilateral anterior lobule – Bilateral paramedian lobules– Cerebral Cortex and
Cerebellum have similar representations
Motor representation– Same area as sensory
mapping– May have auditory and visual
processing

12
Transverse Cerebellar Regions
1. Floccular nodular lobe (Archicerebellum )– Oldest, related to vestibular part of CN VIII– Regulates equilibrium through vestibulospinal tract
2. Anterior lobe (Paleocerebellum)– Rostral to Primary Fissure– General Sensory Receptors– Concerned with muscle tone and walking
3. Posterior lobe (Neocerebellum)– Newest and Largest, Receives afferent projections from contralateral
sensorimotor cortex– Projects to contralateral motor cortex– Functions in coordination of fine and skilled movements
13
Longitudinal Cerebellar Regions
Vermis– Contributes to body posture
Paravermal region– Regulates movements of ipsilateral extremities
(e.g. walking) Lateral Zone
– Regulates skilled movements of ipsilateral extremity (e.g. tying your shoe)

14
Cerebellar Connection Three Peduncles
1. Inferior – afferent: mediate sensorimotor input to the cerebellum2. Middle – afferent: same as above3. Superior – efferent: transmit output from the cerebellum to the
brainstem and on to the thalamus, motor cortex, and spinal cord
Varied afferents to Cerebellum :– spinal cord– brainstem – motor cortex
Afferenet:Efferent Ratio = 40:1– For each going from cerebellum to body, 40 coming in

15
Afferent Pathways (Inferior)
Vestibulocerebellar Tract– Info From Semicircular Canals Through Inferior
Peduncle– Maintains Upright Posture
Dorsal Spinocerebellar Tract– Info From Reticular Nuclei (involved in regulation of
sleep, respiration, heartbeat, etc.)– Unconscious Proprioception From Muscle
Spindles, Golgi Tendons and Tactile Receptors

16
Afferent Pathways (Inferior 2)
Reticulocerebellar Tract– Info From Cerebral Cortices, Spinal Cord, Vestibular
Complex, and Red Nucleus
Olivocerebellar Tract– Info From Spinal Cord Through Olivary N to Contralateral
Cerebellar Hemisphere– Source of Climbing Fibers for Direct Input to Cerebellum
Cuneocerebellar Tract– Mediate Proprioception From Upper Limbs and Neck

17
Afferent and Efferent Projections
Superior CerebellarPeduncle
Red nucleus
Thalamus
Middle CerebellarPeduncle (pontocerebellar fibers)
Inferior Cerebellar Nucleus(olivocerebellar fibers)

18
Afferent Pathways (Middle)
Info From Pontine Nuclei From Opposite Cerebral Cortex, Visual and Auditory Inputs
To Opposite Cerebellar Hemisphere

19
Efferent Pathways
Arise From Cerebellar Nuclei– Dentate nucleus– Emboliform nucleus– Globose Nucleus
Through Superior Cerebellar Peduncle to – Red Nucleus (Brainstem)– Thalamus– Motor Cortex

20
Cerebellar Cortex
Structured in Three Parallel Layers– Molecular– Purkinje
Connecting Surface and Deep Cerebellar Nuclei
Source of All Efferent Fibers Cerebellar Cortex
– Granular Have Mossy Fiber Axons to
Purkinje Axons

21
Clinical Considerations
Signs of Dysfunction– Impaired Muscle Synergy– Reduced Muscle Tone– Evident in Skilled Tasks– Ataxia
Lack of Order and Coordination in Activities Slow Movement (Bradykinesia) Mild Muscular Weakness (Asthenia) Asynergia (Poor coordination of muscles: Dysdiadochokinesia) Speech difficulties (Ataxic Dysarthria)
– affects respiration, phonation, resonance and articulation, but most pronounced in articulation and prosody.

22
Clinical Considerations 2
Dysdiadochokinesia– Clumsiness in Alternating Movements
Switching between supination and pronation – e.g. screwing in a light buld
– Tapping, Speech Sound Dysarthria
– Ataxic Dysarthria– Poor articulation: Slurred and Disjointed Speech
Dysmetria– Error in Judgment of Range and Distance of Target– Undershooting or Overshooting

23
Clinical Considerations 3
Intentional Tremor– Accessory Movement During Volitional Task– vs. Parkinson’s Disease Where Tremor Lessens During
Volitional Movement Hypotonia
– Reduced Resistance to Passive Stretch Rebounding
– Inability to Predict Movement – Cannot Hold Back Movement
Disequilibrium– Unsteady Gait, Body Wavering

24
Cerebellar Pathologies
Cerebrovascular Accident (CVA)– Thrombotic, embolic or hemorrhagic– Vertebrobasilar Artery
Toxicity– Chronic Alcoholism
Progressive Cerebellar Degeneration– Friedrich's Ataxia: Autosomal Recessive Heredity
Degenerative Condition – Combined Sensory and Motor Dysfunctions
Poor coordination of Gait and speech