1 fig. 5-1, “toxic triangle”, epidemiologic triad environmental factors host factors agents
TRANSCRIPT

1
Fig. 5-1, “Toxic Triangle”, Epidemiologic Triad
Environmental Factors
Host Factors
Agents

2
Epidemiologic Triad
• Organisms• Chemicals
– exogenous– endogenous
• Nutrients• Physical
forces• Psychological
factors• Genetic
• Immunity• Immunologic
response• Host behavior
– diet
• Physical– hot, cold – altitude
• Biologic• Social
– economic
Source: Smith, Theobald, 1934
Agents Host Factors EnvironmentalFactors
Agents have characteristics such as infectivity, pathogenicity, virulence

3
Pathogens are also toxic agents that can cause cancer
• HP - Gastric; Mucosal-associated lymphoid tissue• Schistosoma haematobium - Bladder cancer• HTLV-I - Adult T-cell leukemia/lymphoma• HBV - Liver cancer• HHV-8 - Kaposi’s sarcoma• EBV - Lymphoproliferative disorders;
Nasopharyngeal; Burkitt’s lymphoma• HPV - Anogenital carcinoma; cervical cancer
• HP = Helicobacter pylori V.; HTLV = Human T-cell Leukemia/lymphoma V.; HHV = Hepatitis B V.; EBV = Epstein-Barr V.; HPV = Human papilloma V.

4
Classes of Xenobiotics
Pollutants (Air, Water, Soil)
Pesticides
Pharmaceuticals
IndustrialChemicals
FoodAdditives
Cosmetics

5
Dose - ResponseA is more toxic than B
• LD50
0
100
50
Response
Dose mg/kg
AB
6
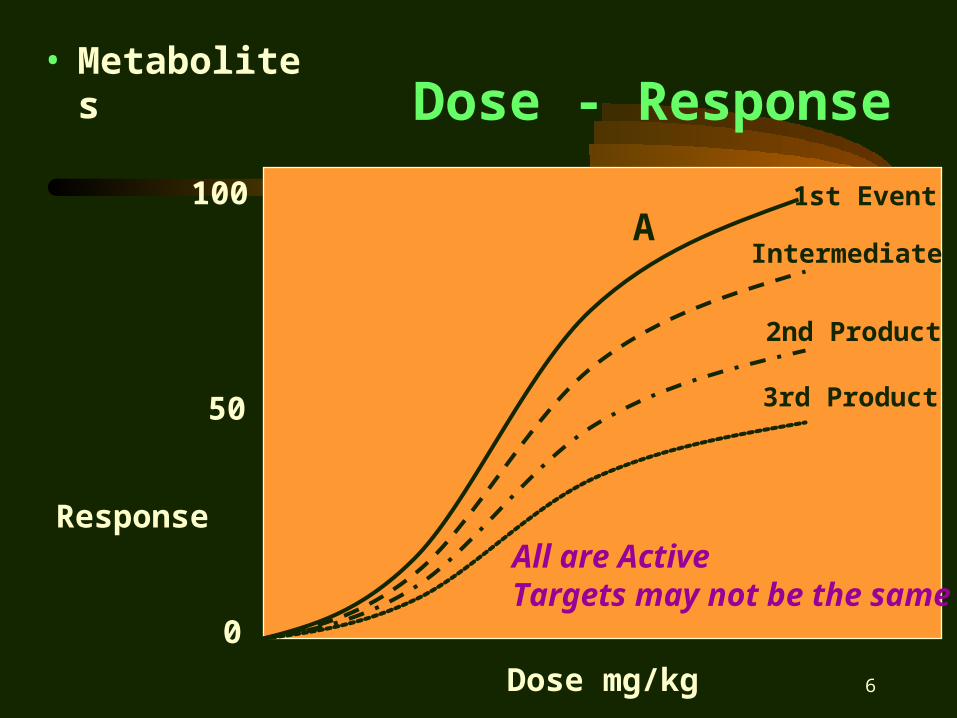
Dose - Response• Metabolites
0
100
50
Response
Dose mg/kg
A1st Event
Intermediate
2nd Product
3rd Product
All are ActiveTargets may not be the same

7
Dose - Response• Dose related
Toxicity
0
100
50
Response
Dose mg/kg
Parathion
DDT
50080

8
Dose - Response• Modes of
Action
0
100
50
Response
Dose mg/kg
Same LD50
A
A >> Toxic at Low Dose

9
Factors Governing Toxicity
• Age– very young or old
• Strain– e.g. skin color & UV
• Gender
• Weight• Exercise and
Physical Stress• Health Status
– immune deficiencies
• The outcome of exposure to a toxin depends on a number of factors that may include:

10
Dr. Robson’s Medical Terms
Artery The study of fine painting
BariumWhat you do after CPR fails
Benign What you are after you be eight
Dilate To live longer
Morbid A higher offer
Nitrate Lower than the day rate
Tumor An extra pair
Urine The opposite of you’re out

11
ProblemContext
Risks
OptionsActions
Decisions
Evaluation
EngageStakeholdersCommunication
Throughout
The New Risk Assessment Paradigm
MostImportantStep

12
Benefits of Engaging Stakeholders
• Supports Democratic decision-making
• Ensures public values are considered
• Develops the understanding needed for better decision-making
• Improves knowledge base for decision-making
• Can reduce time & expense involved in decision-making
• May improve credibility of agencies managing risk
• Should generate better accepted, more readily implemented risk management decisions

13
Three “Laws” of Toxicology
• Dose makes the Poison– everything can create toxic effects
• Chemicals have specific effects– structure relationships, subtle changes
can mediate toxicity
• Human is an animal– animals can be used as “human”
surrogates, choice is important

14
Dose ResponseLD50
ToxicityA > ToxicityB
0
100
50
Response
Dose mg/kg
AB
15
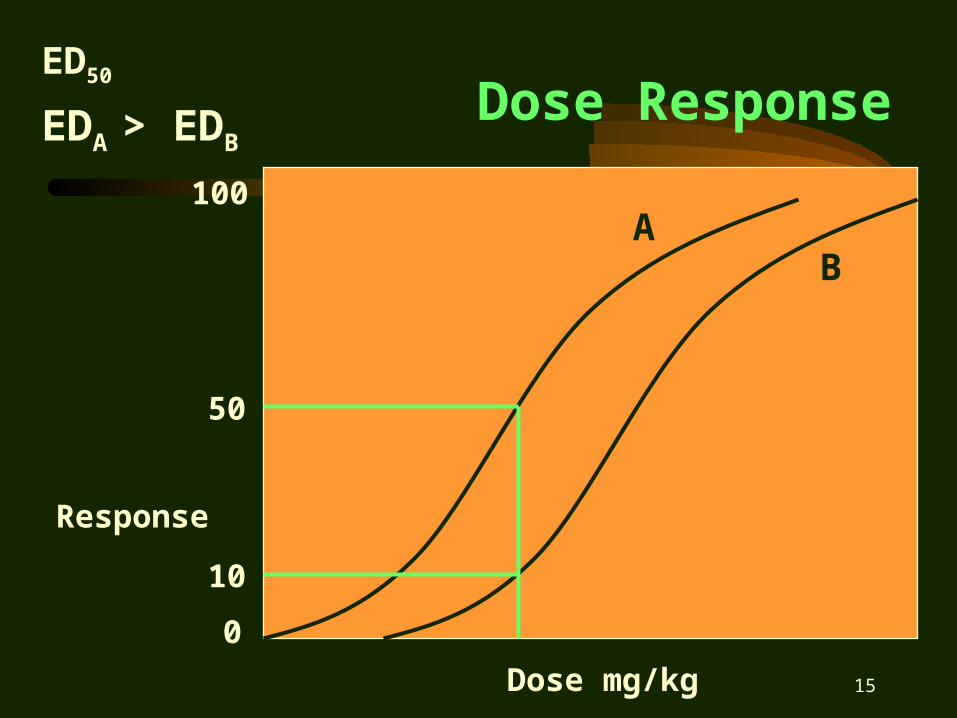
Dose ResponseED50
EDA > EDB
0
100
50
Response
Dose mg/kg
AB
10

16
Dose ResponseNOAELNo Observable Adverse Effect Level
0
5
2
Response
Dose mg/kg7
10
50 100
Dose Response
0 0/10
7 0/10
50 2/10
100 5/10
500 10/10
500
NOAEL

17
Dose ResponseLOAELLowest Observable Adverse Effect Level
0
5
2
Response
Dose mg/kg7
10
50 100
Dose Response
0 0/10
7 0/10
50 2/10
100 5/10
500 10/10
500
LOAEL

18
Dose ResponseReference Dose, RfD• Allowable daily dose
over a lifetime• = (NOAEL) / (UF)• Uncertainty Factors
– 10x, Animals to Man– 10x, Susceptibility– 10x, Only Acute Studies– 1-10x, Others
• In absence of NOAEL– = (LOAEL) / (10)– + UF as above
• Found in EPA’s IRIS database 0
2
Res
po
nse
Dose mg/kg7 50
LOAEL
NOAEL

19
Exposure Studies
• Animal Based (surrogate for human)– Acute (high dose)
• two weeks
– Subchronic (not as high as acute)• 30 - 90 days, some less
– Long term or Chronic (lower doses)• up to two years
– Maximum Tolerated Dose (MTD)• controversy

20
Non Cancer EndpointRisk = Exposure/ADI
• Exposure = Average Daily Dose– = [(C x IR x EF x ED) / (BW x AT)] x factor
• C = Concentration, e.g., soil = mg/kg• IR = Intake rate, e.g., soil = mg/day• EF = Exposure frequency, days/yr• ED = Exposure duration, years (chronic > 7)• BW = Body weight, 70 kg, child = 16 kg• AT = Averaging time, days
• ADI = Acceptable Daily Intake, RfD

21
Risk
• If ADD/ADI > 1, Risk of Adverse Health Effect
• If ADD/ADI < 1, No Adverse Health Effect Anticipated

22
Cancer Endpoints
• A similar approach is used– Slope Factor is used as the ADI
• = upper 95% CI of dose-response curve• e.g., for ingestion units of mg/kg-day
• Typically an acceptable risk is defined as < 1 x 10-6
– However, 10-4 to 10-5 may be acceptable
23
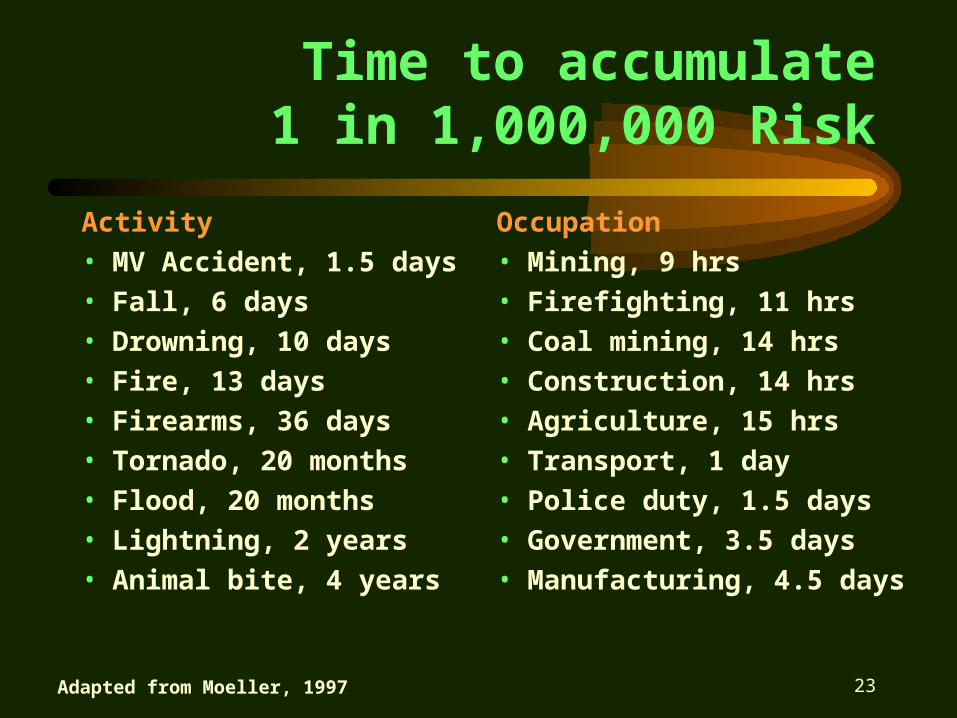
Time to accumulate 1 in 1,000,000 Risk
Activity
• MV Accident, 1.5 days
• Fall, 6 days
• Drowning, 10 days
• Fire, 13 days
• Firearms, 36 days
• Tornado, 20 months
• Flood, 20 months
• Lightning, 2 years
• Animal bite, 4 years
Occupation
• Mining, 9 hrs
• Firefighting, 11 hrs
• Coal mining, 14 hrs
• Construction, 14 hrs
• Agriculture, 15 hrs
• Transport, 1 day
• Police duty, 1.5 days
• Government, 3.5 days
• Manufacturing, 4.5 days
Adapted from Moeller, 1997

24
Lifestyle activities with1 in 1,000,000 Risk
Eating & Drinking• 0.5 liter wine• 6 # of peanut butter
(aflatoxin)• 180 pints of milk
(aflatoxin)• 200 gallons of
drinking water from Miami, New Orleans
• 90 # of broiled steak
Smoking• 2 cigarettes
Other• Paddling in canoe for 6
minutes• Traveling 10 miles by
bicycle• Traveling 30 miles by
car
Adapted from Moeller, 1997
25
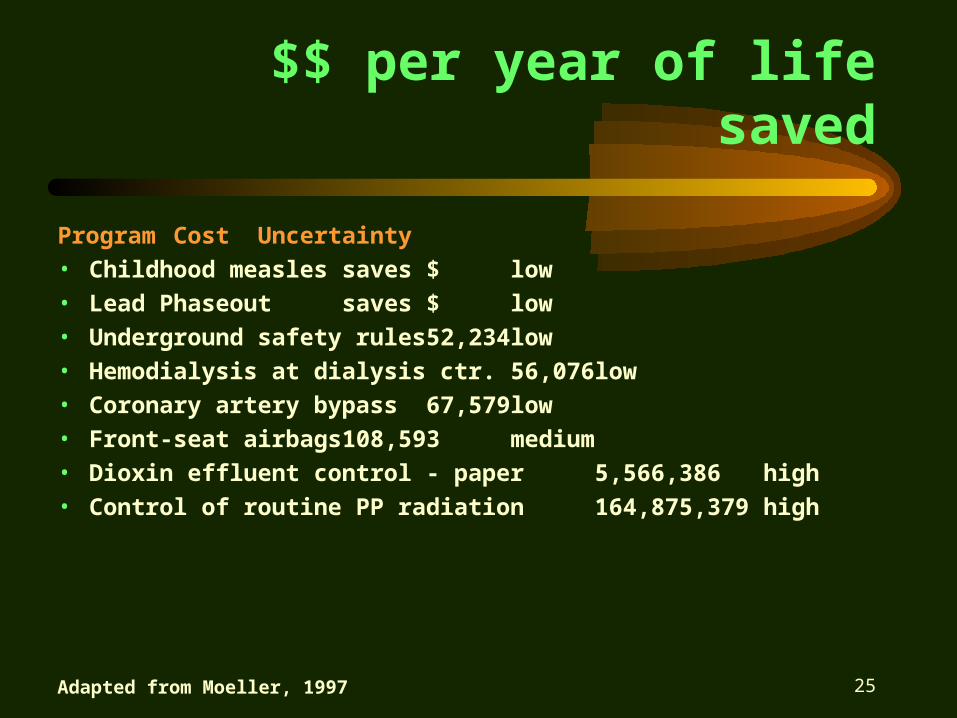
$$ per year of life saved
Program Cost Uncertainty• Childhood measles saves $ low• Lead Phaseout saves $ low• Underground safety rules 52,234 low• Hemodialysis at dialysis ctr. 56,076 low• Coronary artery bypass 67,579 low• Front-seat airbags 108,593 medium• Dioxin effluent control - paper 5,566,386 high• Control of routine PP radiation 164,875,379 high
Adapted from Moeller, 1997

26
“Typical” Risk Perceptions
“Acceptable” if:• Voluntary• Proximate Benefit• Known• Workplace• Natural• Self• Organ Damage• Distant (time, place)
“Unacceptable” if:• Involuntary• No Benefit• Unknown• Residential• Anthropogenic• Children• Cancer• Near

27
ProblemContext
Risks
OptionsActions
Decisions
Evaluation
EngageStakeholders
EPA’s Cardinal Rules of Risk Communication
• Accept & involve public as legitimate partner
• Plan carefully and evaluate your efforts
• Listen to public’s specific concerns
• Be honest, frank, & open• Coordinate & collaborate
w/other credible sources• Meet the media’s needs • Speak clearly and with
compassion

28
10 Key principles of risk assessment, John Graham, HSPS - CRA
• Use the best science for attributable health risk • Acknowledge scientific disagreements• Acknowledge assumptions, & sensitivity of results• Develop central estimates of risk and CI’s + uncertainty• Acceptable risk is policy that requires public involvement• No universally acceptable level of risk exists; context• Health risk decisions require consideration of values
– quality of life, equity, ecological health, choice, economic welfare
• Risk reduction programs should avoid side effects that risk• Programs should consider economic incentives + command c.• Context of risk may be as significant as the magnitude
– voluntary vs. involuntary risk