1 improving referring provider communication performance improvement leadership development program...
Post on 19-Dec-2015
215 views
TRANSCRIPT

1
Improving Referring Provider Communication
Performance Improvement
Leadership Development Program
Center for Health Care Quality
University of Missouri – Columbia

2
Team• Provider Champion/Coach/Facilitator
– Kevin Dellsperger, MD– Kristin Hahn-Cover, MD
• Team Members– Cindy Feutz, RN, Clinical Nurse Specialist (Cardiology)– Jordan Magdits, Assistant Manager (Admissions)– Sherry Rickard, RN , Case Manager (Family & Community Medicine)– Tracy Riecke, RN, Case Manager (Orthopaedic Surgery)– Krista Romanetto, Supervisor (Medical Records)– Matt Wilp, Manager (Provider Relations)
• Resources– Candice Monnig (Cardiology) – Joanne Burns (IT)– Colette Nolin (Admissions) – John Guyton (IT)– Becky Morton (Medical Records) – Scott Barger (IT)– Carol Toliver (Finance) – Doug Garrison (Admissions)
• Executive Sponsor – Marty McCormick, Director, Planning

3
Focus Area & Aim• Problem
– Over the past 12 years, communication has consistently ranked as the leading cause of dissatisfaction for referring/primary care providers.
• Timeliness of communication• Quality of communication
– Poor communication has a negative impact on:• Patient safety and outcomes• Referral volumes
• Aim Statement - we aim to improve communication within one business day of discharge to external referring and primary care providers whose patients receive in-bed services at University Hospital by increasing successful transmission of discharge documentation from 28% to 100% by April 1, 2011.

4
Timeline• August 2010 – Project Began• September - November 2010 – Diagnostic Journey• November 2010 – Interventions chosen – reintroduce
scripting & pursue automation• November 2010 – Admissions/Registration reinforces
scripting to staff• December 2010 – Dr. Hahn-Cover presents recommended
changes to Executive Committee; approved by Executive Committee
• December 2010 - February 2011 – Rapid Cycle PDSA• February 2011 – Pilot process of faxing Depart Summary to
referring and primary care provider• February 2011 – Dr. Hahn-Cover presents updated
recommendations to Executive Committee

5
Relationship to Strategic Goals• Service Column of Excellence
– FY15• Goal - To become the provider of choice through exceptional patient-
and family-centered care • Targets/measures - referring provider satisfaction mean score of 80
– FY11• Objective/tactics
– Develop and implement a process to provide communication within one to two business days of discharge to the referring/primary care provider
– Develop a succinct discharge summary that meets the needs of referring providers and improves coordination of care and outcomes
• Targets/measures– Implementation of inpatient discharge notification process; 80% of
external referring physicians receive a phone call within two business days of patient discharge
– Development of discharge summary

6
Fishbone Diagram
Referring providers/PCP not getting information
At discharge
Internal System
Medical Records
Patient
Admissions
Knowledge
Incorrect faxing
Patients don’t have PCP
Establish new PCP
Internal communication with
PCP disconnect
Staff not verifying
Patients don’t know definition of PCP
scripting
Cerner/IDX not talking
Depart Summary
Physician Referral fax number not correct
Timely discharge summary by
Residents
Timely signature on discharge summary
by attending
PCP not Identified on emergent/
urgent admissions
Referring physician not identified on emergent/
urgent admissions
Elective identified
10/13/10

7
Stakeholders
• External referring/primary care providers • Patients• Patient care staff (e.g. physicians, fellows, residents,
nurses, case managers, discharge planners, etc.)• Revenue cycle• Information technology• Provider relations

8
Driver Diagram
•
Referring providers/PCP not getting information
At discharge
Internal System
Medical Records
Patient
Admissions
Knowledge
Incorrect faxing
Patients don’t have PCP
Establish new PCP
Internal communicatio
n with PCP disconnect
Staff not verifying
Patients don’t know
definition of PCP
scripting
Cerner/IDX not talking
Depart Summary
Physician Referral fax number not
correct
Timely discharge
summary by Residents
Timely signature on
discharge summary
by attending
PCP not Identified on emergent/
urgent admissions
Referring physician not identified on
emergent/urgent admissions
Elective identified
10/13/10
III - 3
II - 2
I - 1
IIII - 4
II - 2
III - 3
9
Interventions Chosen
• Immediate/Short-term– Reinforce scripting for registration/admissions staff to better
clarify what a referring and primary care provider is to patients– Fax Depart Summary to referring and primary care provider by
next business day after patient discharge
• Long-term– Develop an automated process to send out all communication
(admission note, operative notes, succinct discharge summary, clinician summary) within timeframe outlined in Medical Staff Bylaws
– Roll out this process to all areas at University Hospital as well as all other MUHC facilities (WCH, MUPC, EFCC, clinics, etc.)
10
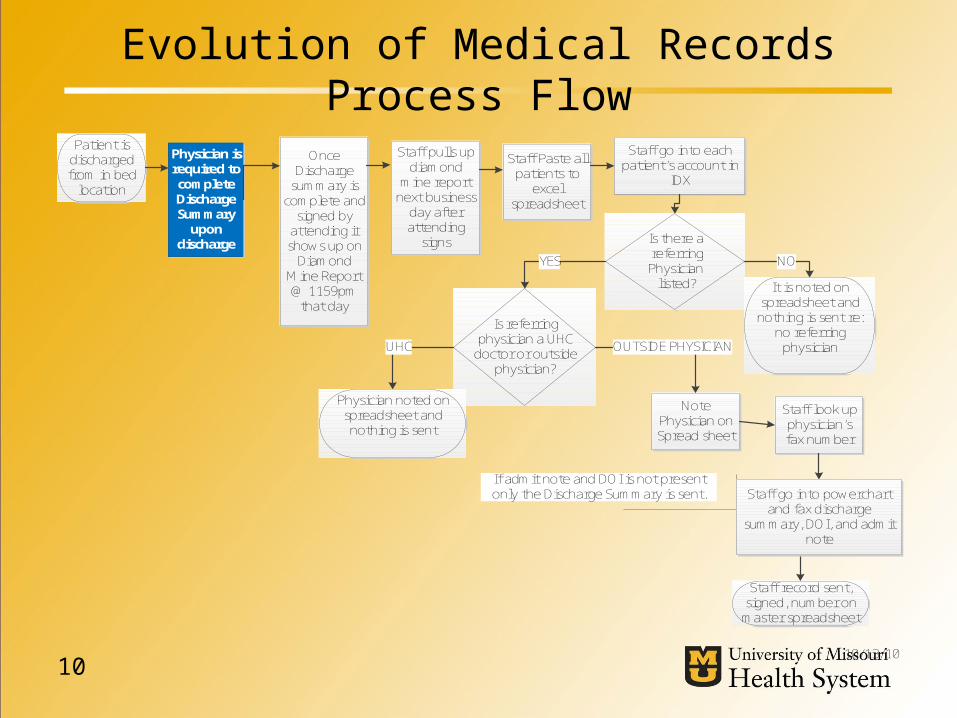
Evolution of Medical Records Process Flow
Patient is discharged from in bed
location
Physician is required to complete Discharge Summary
upon discharge
Once Discharge
summary is complete and
signed by attending it shows up on
Diamond Mine Report @ 1159pm
that day
Staff pulls up diamond
mine report next business
day after attending
signs
Staff Paste all patients to
excel spreadsheet
Is there a referring Physician listed?
Staff go into each patient’s account in
IDX
It is noted on spreadsheet and
nothing is sent re: no referring
physician
Is referring physician a UHC
doctor or outside physician?
Note Physician on Spread sheet
NOYES
OUTSIDE PHYSICIANUHC
Physician noted on spreadsheet and nothing is sent
Staff look up physician’s fax number
If admit note and DOI is not present only the Discharge Summary is sent.
Staff record sent, signed, number on
master spreadsheet
10/13/10
Staff go into powerchart and fax discharge
summary, DOI, and admit note

11
Evolution of Medical Records Process Flow

12
Measurement
• Measure the percentage of external referring and primary care providers who are sent follow-up communication
• Key measures for this process include:– Primary care provider complete– Referring provider complete– Proportion of providers that are external– Time interval between date of discharge and date documentation is faxed– Fax sent successfully

13
Baseline Data• 429 discharges measured in November 2010
63
366
External Referring Provider
Internal Provider, Self Referred, Provider Not In Dictionary

14
0-3 Days 4-6 Days 7-9 Days 10+ Days0
5
10
15
20
25
30
26
18
811
Days Until Discharge Summary Signed By Attending
Baseline Data• 63 External Referring Providers

15
• 139 discharges measured in January 2011– 94 external referring or primary care providers listed
• 28% (26 of the 94) of patients’ providers receive follow-up communication
• Low percentage due to current UH process of only sending documentation to referring provider
Baseline Data
16
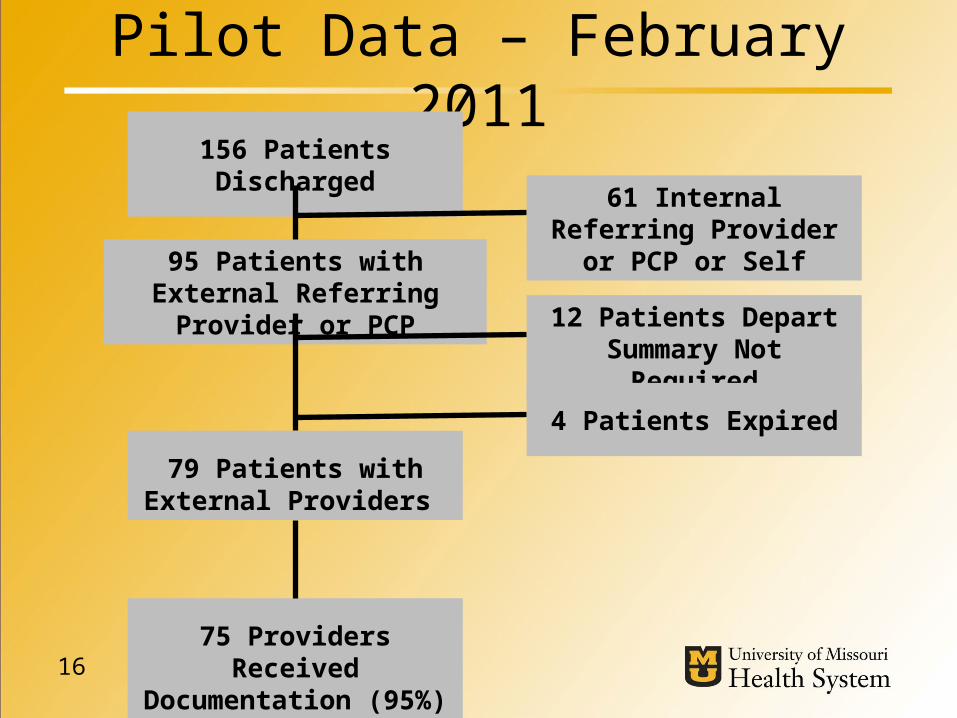
Pilot Data – February 2011156 Patients Discharged
12 Patients Depart Summary Not Required
95 Patients with External Referring Provider or PCP
79 Patients with External Providers
61 Internal Referring Provider or PCP or Self
75 Providers Received Documentation (95%)
4 Patients Expired
17
Process & Outcome Indicators• Process Indicators
– Registration Services to include the completion of referring and primary care provider field into daily QA process
– Medical Records to include QA process of recording verification of faxes sent to referring and primary care providers
• Outcome Indicators– Continuity of care for patient safety and decrease in avoidable
readmissions– number of referring and primary care providers receiving follow-
up communication– Referring physician satisfaction– Referrals volumes

18
Benefits• Quality – improving communication to referring physicians will enhance the
coordination of care and patient outcomes and prevent avoidable readmissions
• Service - increased referring physician and patient satisfaction• People – increased physician satisfaction and retention• Growth - the Advisory Board states that physicians are the most important
driver of market share: – 35% - primary physician is affiliated with hospital– 31% - hospital provides specialized services– 31% - advice/referral from physician– 21% - hospital is up-to-date with medical advances
• Finance – Reimbursement increasingly being tied to quality of care and outcomes– FY10 net revenue/adjusted case YTD (excl. FRA and retail pharmacy revenue)
• University Hospital - $13,712 • CRH (now W&CH) - $ 13,152

19
Anticipated ROI• MUHC has aggressive growth and financial targets
– FY10 actual discharges were 21,279 and the FY11 budgeted discharges are 23,064. This is an 8.4% (1,785) increase in discharges
– The FY11 budgeted change in net assets is $30.0 million
• Assuming average net revenue per adjusted case of $13,500, MUHC could experience the following improvement in performance:– 2% (425) increase in discharges would result in an additional $6.5 million in
net revenue– 6.5% (1,383) increase in discharges would result in an additional $18.6
million in net revenue– 10% (2,127) increase in discharges would result in an additional $28.7
million in net revenue
• Medical Records estimates a saving of at least 2 hours of employee time per day when implementing the process of faxing Depart Summaries
20
Lessons Learned • The situation is more complex than anticipated and requires collaboration on the
part of many• Patients need clarification of what a primary care physician is • Residents and attendings have ownership in completing discharge summaries
and signing off in a timely manner• A clear/concise discharge summary or Depart Summary for referring and
primary care providers needs to be developed • The provider dictionaries need to be combined and maintained and IT systems
need to interface• The process needs to be centralized to improve quality and reduce inefficiencies• Both the referring physician and the primary care physician should receive
communication• The reason that documentation was sent to only referring providers was
because years ago the referring provider field was the most filled out field• Sometimes change to hospital policy is needed and can be time consuming

21
Summary• We have only taken on a very small part in improving overall
communication to referring providers
• In an ideal world an automated process is the best answer, but the bottom line is it can only be as good as the data that is available to it; the goal is to achieve automation by July 2012
• With a major emphasis on outcomes and avoidable readmissions, improved coordination of care through communication to referring and primary care providers is essential
• Improving quality of care and outcomes and increasing the satisfaction of our referring providers will assist in achieving the volume growth needed to support MUHC’s strategic financial plan
• We feel our biggest accomplishment so far was discovering that primary care providers were not receiving communication and mirroring our current process to get communication to them