1 interprofessional approaches to chronic and episodic disability: connecting interprofessional...
TRANSCRIPT
1
Interprofessional Approaches to Chronic and Episodic Disability:
Connecting Interprofessional Education and Practice
Le-Ann Dolan, BSW (MSW in process)
Lynne Sinclair, BScPT, MA(Ad Ed)
Elisse Zack, MMgt, MEd
Julie Hard, MScPT
Overview
• Background on HIV / CWGHR
• In-person and on-line courses
• Course IPE components
• Integration into IP practice
• Lessons Learned
• Practical strategies for sustainability
• Next steps
2
Background HIV as a chronic and episodic condition
• Can - Est 65,000 living with HIV in 2008/Est 55-75,000 living with MS • HIV - complex, multi system Involvement • 1996 –new HIV treatments– people living longer but increasing
impairments, activity limitations, participation restrictions • Unpredictable cycles (episodes) and degrees of wellness/functioning
and illness/disability• Similarities - HIV and other lifelong conditions with episodic
components – e.g. MS, arthritis, lupus, forms of cancer, mental illness• Increasing comorbidities with HIV (arthritis, cancer, neurocognitive,
cardiovascular (stroke); osteoporosis/ other bone and joint disease)
3
Canadian Working Group on HIV and Rehabilitation (CWGHR)
• National, multi-sector, multi-disciplinary organization• Disability and rehab in context of HIV - Bridging HIV, disability & rehab• Cross-disability and interprofessional• Priorities - integrated approach - research, education, policy and
practice
• Awareness of and access to rehab services and resources for people living with HIV and other episodic disabilities - cross disability/ pan disease collaboration
• IP learning / education - link to IP practice • Promote effective policies to respond to needs • Address the needs and concerns of families, caregivers, communities
and people living with HIV-related disabilities
Development of Interprofessional Learning Course
Why an interprofessional course?
Respond to gaps between identified need and capacity of service providers
•Prevalence study 2002-3 High level of disability/Providers survey 2004
•86% of therapists (OT, PT and SLP), indicate their profession is somewhat or very important to the care of people living with HIV
•19% agree they have adequate knowledge or skills to provide these services
•50% agree - rehab professionals are uncomfortable with idea of working with people with HIV
Course Goals: increase knowledge and skills related to HIV among rehab professionals, increase capacity of rehab professionals to respond to needs of people with HIV, enhance IP practice among rehab and other professionals
•Course curriculum for 1.5 days – can be modified as needed
5
IPL in Rehab in the Context of HIV
In-person course - Why an on-line course?
Delivery – key principles•Interprofessional•Engaging people living with HIV as educators•Providing useable information in a practical interactive format•Problem based (e.g. case studies)
Promoting Sustainability •In-person workshops, in-person course, mentorship and on-line format•On-line increases scope and accessibility •Create opportunities for collaboration in in-person and on-line formats
6
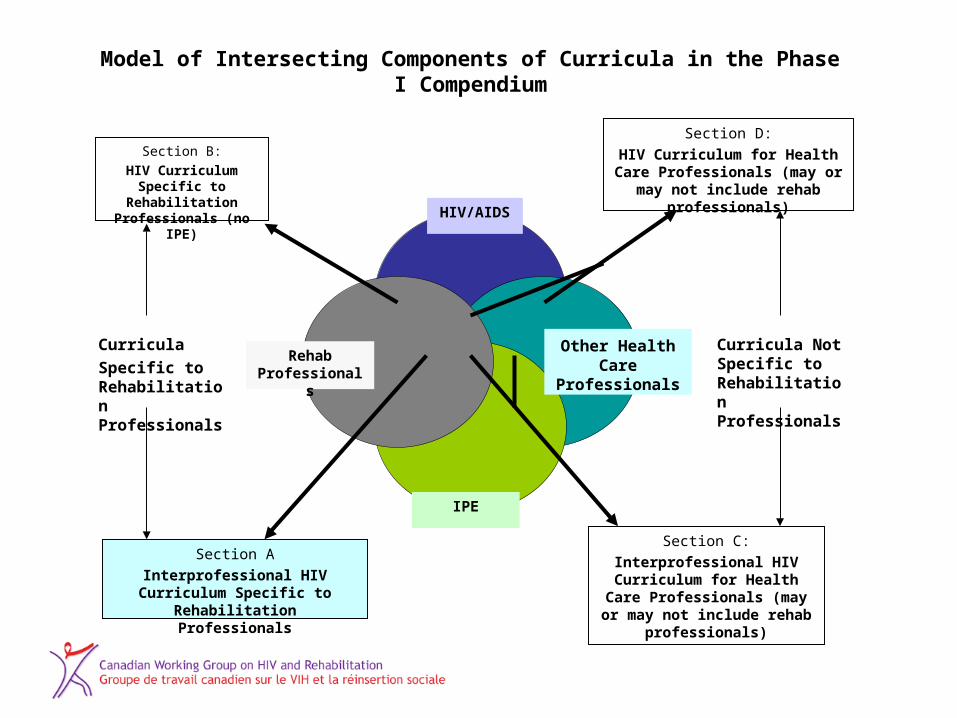
Section A
Interprofessional HIV Curriculum Specific to Rehabilitation
Professionals
Section C:
Interprofessional HIV Curriculum for Health Care
Professionals (may or may not include rehab professionals)
Other Health Care
Professionals
Section D:
HIV Curriculum for Health Care Professionals (may or may not include rehab professionals)
Model of Intersecting Components of Curricula in the Phase I Compendium
Curricula
Specific to Rehabilitation Professionals
Curricula Not Specific to Rehabilitation Professionals
Section B:
HIV Curriculum Specific to Rehabilitation
Professionals (no IPE)
Rehab Professionals
HIV/AIDS
IPE
Developing an On-line course
• Research - Increasing role for rehab professionals in HIV care; only a minority currently serve people with HIV
• HIV specialists currently provide or refer to limited rehabilitation-related programs
• Need further education–with HIV specialists and rehab professionals
• Process: Workshops >In-person curriculum > pilot in 3 locations > adapt for mentorship curriculum > adapt for online format > pilot on-line format > include in emodule update
• Case studies in online and mentorship formats
8
Evidence
Process for developing curriculum • Key principles - evidence informed and interprofessional (despite
funders’ recommendation for single profession)
Evidence• Literature review of HIV, Rehab and IPE models • Cochrane Reviews – Aerobic Exercise / HIV and Resistance
Exercise / HIV; “Module 7” (1998) and updated eModule (2010)• Focus groups and Key informant interviews across Canada
including: People with HIV, Rehab professionals, Curriculum experts, Academics, Placement coordinators, Policy makers, IPE networks
9
Examples from ProgramsMentorship (IPE and problem-based learning)
– Skilled IP clinicians as co-mentors with people living with HIV – capacity building with care givers new to HIV care
IPE curriculum - via CWGHR campus•HIV, disability and rehab; episodic disabilities; employment issues•Pharmacological implications for rehabilitation•Case studies for IP team response•Vulnerable populations (sensitive practice) •HIV as an episodic condition / links to arthritis, MS, cancer, MSK•Links to mental health challenges•Links to employment policies and programs/ workplace issues
10
IPE Essential Elements
• Communication – between and among
• Collaboration - integration
• Ethics and Values – sensitive care
• Health Care System - settings
• Learning continuum
• Evidence-based framework
11
IPE Components
• Interactive
• Self-directed
• Reflective practice
• Patient and family centred
• Delivered by variety of HCPs
• Patient cases – rehab goals
12

Sustainable Integration into IP Practice
• Focus on prevention, care, treatment and support
• Developed and delivered by clinicians, researchers and active patient involvement
• Across range of health care settings
• Across lifespan
• Across speciality and generalist areas
13
Working Collaboratively
• Target audience is primary rehabilitation and other health care providers
• Secondary audience includes psychosocial, vocational rehab and alternative therapies
• Provides info about referring to Rehab
• Modules cover Rehab roles
• Includes social support system
14
Integration into Daily Practice
• Applicable to other chronic illnesses and episodic disabilities
• Patient cases – primary or secondary HIV Dx– guiding questions– facilitator notes– pt-centred SMART goals– hyperlinked to content
15
Approaches to Integrate
• Answers questions such as;– How can you access Rehab services?– What can Rehab do?– How can your patients/clients benefit?
• Advocacy and sensitive practice
• Discipline specific and IP
• Return to Work
• Discussion board can be added16
Lessons Learned
• Broad multi-sector stakeholder input
• Meaningful patient content and involvement
• Different learning styles and learning tools
• Content based on clinical expertise AND lived experience
• Need ongoing (peer) support for sustainable IP learning
17
Sustainability Success
• Workshops, in-person and on-line formats
• Client focused and holistic care
• Across the continuum of care
• Safety for learning about sensitive care
• Address barriers (e.g. return to work)
• Include evaluation
• Employer support for integration into practice (including time for mentorship)
18
Next Steps
• New opportunities for rehab – research
• Education – broad curricula dissemination
• Partnerships – Clinical, Academic,
Professional Associations and Community
• Create more lateral inter-sectoral links
within regions and communities
19
Summary
• In-person and on-line courses
• Workshops
• Mentorship
• Multi-stakeholder input (meaningful patient)
• Evidence-based approach
• Problem-based learning with cases
20
Conclusion
• Focus on promotion and rehab care has great potential with aging population
• Not focus solely on specific disease
• Content must be based on clinical expertise AND lived experience
• HIV care can be ideal for learning about chronic illness or episodic disability
21
Contact Info and References• O’Brien K, Bone G, Sinclair L, Solomon P. Rehabilitation in the Context of
HIV: An Interprofessional Multi-Stakeholder Process for Curriculum Development. Fall 2010. Journal of Allied Health.39(3 part 1): 131-137.
• O’Brien K, Bone G, Zack E, Solomon P. HIV and Rehabilitation: Development of a Conceptual Framework for Curriculum Planning. International Journal of Rehabilitation Research. September 2008; 31(3):189-197.
• Solomon P, O’Brien K, Hard J, Worthington C, Zack E. An HIV mentorship program for rehabilitation professionals: Lessons learned from a pilot initiative. Submitted to: International Journal of Therapy and Rehabilitation. Accepted: (October 2010). In Press.
For further details please contact: Le-Ann Dolan, Program Director
www.hivandrehab.ca
22