1 mechanical ventilation & strategies for oxygenation dawn oddie
TRANSCRIPT

11
Mechanical Ventilation & Strategies for Oxygenation
Dawn Oddie
22
What are we going to talk about?
Physiology Ventilation classifications Types of Ventilation Optimising Oxygenation Complications of Ventilation Weaning from Ventilation
33
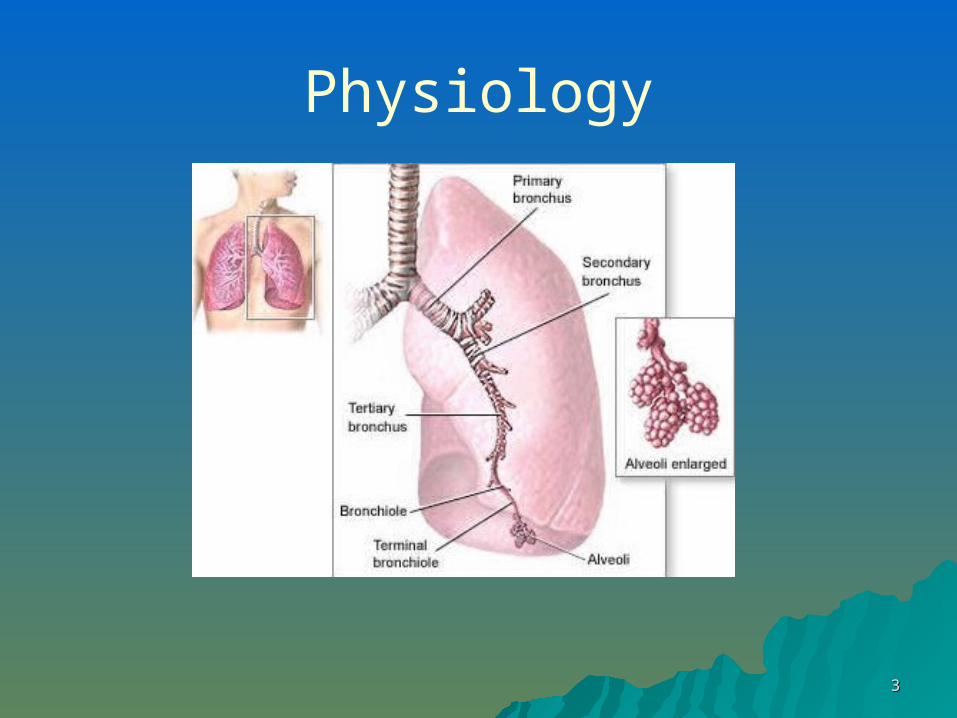
Physiology

44
Where it all happens!
300 millio
n alveoli
55
Physiology of normal breathing
How do we breathe?
Low lung volume (Exhalation) / Functional residual capacity
High lung volume (Inhalation)
Negative pressureI:E ratio times
Tidal volumes
Respiratory rate
Active inspiration Passive expiration

66
How is normal breathing controlled
How do you know, Rate - How fast / slow to breathe? Tidal volume - How big a breathe to
take in? I:E ratio – How long to breath in / out
for? When to cough / sneeze?

77
Nervous Control / Chemical Respiratory centre. Reticular formation – brain stem
– Medullary rhythmicity area– Pneumotaxic area / Apneustic area (transition from I to E)
Inflation (Hering-Breuer) reflex - Stretch receptors Cortical influences – cerebral cortex giving some voluntary
control eg hold breath underwater Central chemosensitive area (pH / H+) – Medulla Peripheral chemoreceptors (CO2 / O2 / H+) – carotid bodies Proprioceptors – joints / muscles
Other influences – Baroreceptors / Temp / Pain / stretching the anal sphincter muscle / Irritation of the air passages

88
Lung Volumes

99
Respiratory Mechanics- Compliance Compliance is ΔV/ΔP (Change in Volume / change in pressure)
– Total lung is made up of thoracic and lung compliance Pulmonary compliance (or lung compliance) is the ability of the lungs
to stretch during a change in volume relative to an applied change in pressure.
Compliance is greatest at moderate lung volumes, and much lower at volumes which are very low or very high. LIP and UIP can be good guides
Pulmonary Surfactant increases compliance by decreasing the surface tension of water. The internal surface of the alveolus is covered with a thin coat of fluid. The water in this fluid has a high surface tension, and provides a force that could collapse the alveolus. The presence of surfactant in this fluid breaks up the surface tension of water, making it less likely that the alveolus can collapse inward. If the alveolus were to collapse, a great force would be required to open it, meaning that compliance would decrease drastically.

1010
Respiratory Mechanics- Compliance
Low compliance indicates a stiff lung and means extra work is required to bring in a normal volume of air. This occurs as the lungs in this case become fibrotic, lose their distensibility and become stiffer.
In a highly compliant lung, as in emphysema, the elastic tissue has been damaged, usually due to their being overstretched by chronic coughing. Patients with emphysema have a very high lung compliance due to the poor elastic recoil, they have no problem inflating the lungs but have extreme difficulty exhaling air. In this condition extra work is required to get air out of the lungs.

1111
Causes of Decreased Intrathoracic Compliance
Decreased Chest Wall Compliance
Decreased Lung Compliance
ObesityAscitesNeuromuscular weaknessFlail ChestKyphoscoliosisParalysisSclerodermaPectus Excavatum
Tension PneumothoraxIntubationPulmonary oedemaARDSConnective tissue diseaseSarcoidosisDynamic HyperinflationLymphangitis Carcinomatosis
1212
Some Important Physiology
V/Q Mismatch Oxygen Cascade Oxyhaemoglobin Dissociation Curve Spirometry Trace

1313
Supply and demand
V/Q mismatch– V = Ventilation– P = Perfusion– Hypoxic Pulmonary Vasoconstriction
Functional alveoli Permeable membranes Circulating volume – with
– Adequate haemoglobin levels– Oxygen saturation of haemoglobin (affinity)– Oxygen dissociation– Perfusion pressure

1414
When room air just isn’t enough…..
Increased metabolic demand
V/Q mismatch – Damaged alveoli /
airways– Blocked alveoli– Inadequate
circulation

1515
Some indications to increase O2
Acute respiratory failure eg pneumonia, asthma, pulmonary oedema, pulmonary embolus
Acute myocardial infarction Cardiac Failure Shock Hypermetabolic states eg major trauma, sepsis, burns Anaemia Carbon monoxide poisoning Cardio respiratory resuscitation During / post anaesthesia Pre-suction Suppressant drug eg narcotics Pyrexia (Oxygen consumption increases by 10% for each
degree rise)

1616
Effect of insufficient oxygen
Reduced oxygen supply leads to cellular shift from aerobic to anaerobic metabolism
Production of lactic acid Increasing metabolic acidosis
– Low pH
– Low HCO3
– Negative base excess Cell death / system wide failure

1717
What is oxygen
What percentage of oxygen is in atmospheric air?
In normal circumstances with a average respiratory rate sufficient to meet
metabolic demandsOxygen delivery (mls O2/min) = Cardiac output
(litres/min) x Hb concentration (g/litre) x 1.31 (mls O2/g Hb) x % saturation
Oxygen Consumption = 200 - 250 mls / min

1818
Haemoglobin

1919
Haemoglobin Intracellular protein contained within erythrocytes
(red blood cells) Made up of 2 pairs of polypeptide chains (2Alpha,
2 Beta), each bound to a haem group that contains iron. Each molecule of haemoglobin can combine with 4 molecules of oxygen
Primary vehicle for oxygen transportation in the blood (small amount in plasma Approx 1.5-3%)
Each haemoglobin molecule has a limited capacity for holding oxygen molecules. How much of that capacity that is filled by oxygen bound to the haemoglobin at any time is the oxygen saturation (SaO2)

2020
Haemoglobin
Average 70Kg Adult = 900g of circulating haemoglobin (Hb 14-18g/dl)
1g Haemoglobin can carry 1.34ml oxygenExample,10g/dl with an average 5l circulating volume =
500g total body haemoglobinIf fully saturated 500 x 1.34 = 670ml of oxygen(Only approx 25% unloads leaving venous sats
(SvO2) 70-75% - useful in times of higher metabolic demand etc

2121
The transfusion debate…
Risks of vs Reduced oxygen transfusion carrying capacity

2222
Factors affecting carriage
Timing of haemoglobin uptake and release of oxygen affected by,– Partial pressure of oxygen (PaO2)
– Temperature– Blood pH– Partial Pressure of Carbon dioxide
(PaCO2)

2323
Partial Pressure - effect of Altitude
At sea level we live under a layer of air that is several miles deep – the atmosphere. The pressure on our bodies is about the same as 10 metres of sea water pressing down on us all the time. At sea level, because air is compressible, the weight of the air around us compresses making it denser. As you go up a mountain, the air becomes less compressed and therefore thinner.

2424
Partial Pressure - effect of Altitude
The important effect of this decrease in pressure is: in agiven volume of air, there are fewer molecules present. The percentage of those molecules that are oxygen is exactly the same: 21%. The problem is that there are fewer molecules of everythingpresent, including oxygen.
So why is this an issue?

2525
Partial Pressure of gases In a mixture of ideal gases, each gas has a
partial pressure which is the pressure which the gas would have if it alone occupied the volume. The total pressure of a gas mixture is the sum of the partial pressures of each individual gas in the mixture.
Dalton's law (also called Dalton's law of partial pressures) states that the total pressure exerted
by a gaseous mixture is equal to the sum of the partial pressures of each individual component in
a gas mixture.
2626
Partial Pressure Partial pressure (PP) is a way of describing how much of a
gas is present. All gases exert pressure on the walls of their container as gas molecules bounce constantly of the walls
PP is also used to describe dissolved gases. In this case, the PP of a gas dissolved in blood is the PP that the gas would have, if the blood were allowed to equilibrate with a volume of gas. When blood is exposed to fresh air in the lungs, it equilibrates almost completely so that the PP of oxygen in the air spaces in the lungs is equal to the partial pressure of oxygen in the blood.
PP of arterial blood is slightly less than PP of oxygen in lungs – due to physiological shunt (some blood passing through lungs without encountering an air space)

2727
Partial Pressure of gases The partial pressure of a gas dissolved in a liquid
is the partial pressure of that gas which would be generated in a gas phase in equilibrium with the liquid at the same temperature. The partial pressure of a gas is a measure of thermodynamic activity of the gas's molecules. Gases will always flow from a region of higher partial pressure to one of lower pressure; the larger this difference, the faster the flow.
Gases dissolve, diffuse, and react according to their partial pressures, and not necessarily according to their concentrations in a gas mixture.

2828
Oxygen dissociation curve
Dissociation curve relates oxygen saturation of Haemoglobin (Y axis) and partial pressure of arterial oxygen (X axis) in the blood

2929
Dissociation curve explained Extent of oxygen binding to haemoglobin
depends on PaO2 of blood, but relationship not precisely linear
Slope steeply progressive between 1.5 – 7kPa (area of most rapid uptake and delivery of oxygen to and from haemoglobin), then plateaus out between 9 – 13.5kPa
Haemoglobin almost completely saturated at 9kPa – further increases in partial pressure of oxygen will result in only slight rises in oxygen binding

3030
Oxygen dissociation curve The partial pressure of
oxygen in the blood at which haemoglobin is 50% saturated (26.6mmHg) is known as the P50
P50 is conventional measure of haemoglobin affinity for oxygen
Increased P50 indicates a right shift of the standard curve – meaning larger partial pressure necessary to maintain a 50% oxygen saturation

3131
Oxygen dissociation curve
Reduced AffinityIncreased affinity

3232
Factors influencing the position of oxygen dissociation curve
To the right, Hyperthermia Acidosis (pH) Increased pCO2
Endocrine disorders
Curve shifts to left, Hypothermia Alkalosis Decreased pCO2
Carbon monoxide
Generally a shift to the,Right will favour unloading of oxygen to the tissuesLeft will favour reduced tissue oxygenation

3333
Factors influencing the position of oxygen dissociation curve - explained
To the right As pH declines
(acidosis) the affinity of haemoglobin for oxygen reduces. Result – less oxygen is bound while more oxygen is unloaded
Bohr effect
To the left Temperature – as
body temp falls the affinity of haemoglobin for oxygen increases. Result – more oxygen is bound while less oxygen is unloaded

3434
mmHg vs. kPa Both measures commonly in use
The kiloPascal: A pressure of one thousand pascals (1 kPa) is about 10.2 cm H2O or about 7.75 mmHg.
Atmospheric pressure is about 1034 cmH2O or 101.9 kPa. The useful approximations are 1000 cm H2O or 100 kPa.
mmHg to kPa: To convert pressure in mmHg to kPa, divide the value in mmHg by 7.5.
Eg.– 60mmHg = 8.0kPa– 30mmHg = 4.0kPa
3535
The oxygen cascade Transport has three stages (steps),
– By gas exchange in the lungs Partial pressure gradient of oxygen (PaO2) in alveoli
13.7kPa Partial pressure gradient of oxygen (PaO2) in pulmonary
capillaries 5.3kPa
– Transport of gases in the blood Partial pressure gradient of oxygen (PaO2) in arterial
blood 13.3kPa
– Movement from blood into the tissues Partial pressure gradient of oxygen (PaO2) in tissues
2.7kPa Mitochondrial pressure 0.13-1.3kPa
3636
Oxygen delivery to tissues…. The amount of oxygen bound to the haemoglobin
at any time is related to the partial pressure of oxygen to which the haemoglobin is exposed.
Eg in lungs at the alveolar-capillary interface, partial pressure of oxygen is high so oxygen readily binds. As the blood circulates to other body tissue in which the partial pressure of oxygen is less the haemoglobin releases the oxygen into the tissues.
Haemoglobin cannot maintain its full bound capacity in the presence of lower oxygen partial pressures.

3737
Supplementing Oxygen Nasal cannula Fixed performance mask Variable performance mask Non rebreathe reservoir Tracheostomy mask Tents / head boxes Bag valve mask CPAP – nasal / facial or hood
BiPAP – IPAP / EPAP Intubation and mechanical ventilation

3838
Indicators for initiating mechanical ventilation?

3939
Types of positive pressure ventilation
Non invasive
Invasive

4040
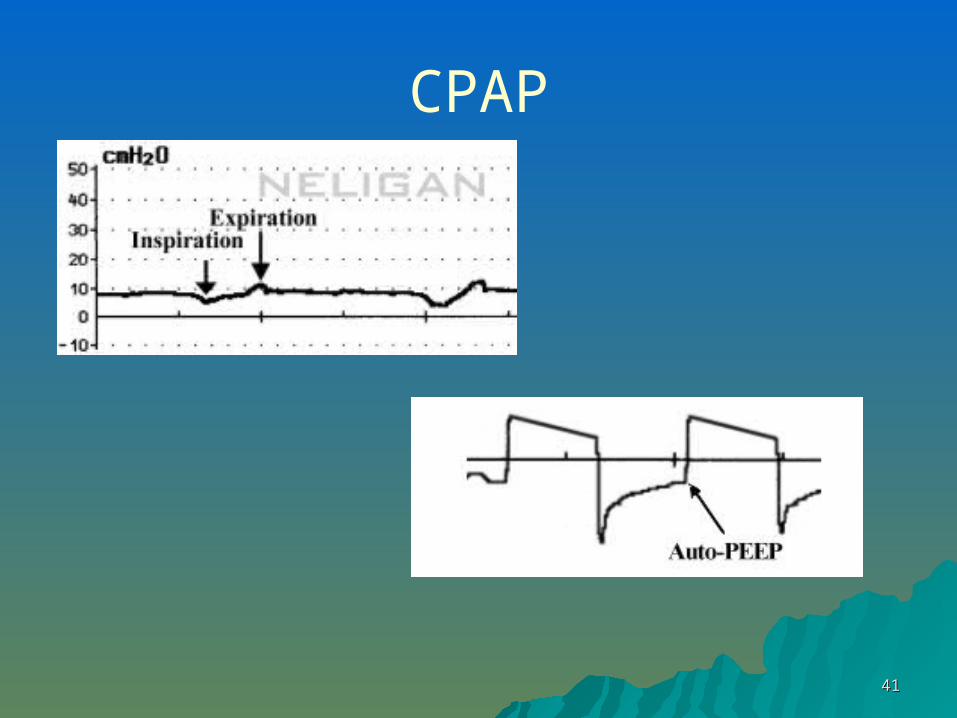
CPAP / PEEP / EPAP Pressure applied at end of expiration to maintain
alveolar recruitment Airway pressure kept positive
Beware of gas trapping (autoPEEP) in non compliant lungs
4141
CPAP

4242
NIV - BiPAP
IPAP / PS / ASB– Inspiratory assistance with each
spontaneous breath
EPAP– Expiratory resistance

4343
The science of mechanical ventilation is to optimise pulmonary gas
exchange; the art is to achieve this without damaging the lungs

4444
What is a Mechanical Ventilator?
Generates a controlled flow of gas in and out of a patient
Inhalation replenishes alveolar gas
Balance needed between O2 replenishment and CO2 removal

4545
Ventilators – What do they need to do…
Mechanical ventilators are flow generators
Must be able to,– Control– Cycling– Triggering– Breaths– Flow pattern– Mode or breath pattern

4646
Ventilator strategy
Aim to achieve adequate minute volume with the lowest possible airway pressure

4747
Ventilator Classification
Control– How the ventilator knows how much
flow to deliver Can be,
– Volume controlled (volume limited, volume targeted) & pressure variable
– Pressure controlled (pressure limited, pressure targeted) & volume variable
– Dual controlled (volume targeted (guaranteed) pressure limited

4848
Ventilator Classification
Cycling How the ventilator switches from
inspiration to expiration (the flow has been delivered – how long does it stay there?)
– Time cycled e.g. pressure controlled ventilation
– Flow cycled e.g. pressure support
– Volume cycled. The ventilator cycles to expiration once a set tidal volume has been delivered.

4949
Ventilator Classification
Triggering What causes the ventilator to cycle to
inspiration. Ventilators may be……– Time triggered
Cycles at set frequency as determined by the rate
– Pressure triggered Ventilator senses the patients inspiratory effort by
sensing a decrease in baseline pressure
– Flow triggered Constant flow through circuit – flow-by. Ventilator
detects a deflection or change in this flow. Requires less work from the patient than pressure triggered

5050
Ventilator Classification
Breaths– Mandatory
(controlled) – determined by the respiratory rate
– AssistedE.g. synchronised intermittent mandatory
ventilation (SIMV)
– SpontaneousNo additional assistance during inspiration
e.g. CPAP
5151
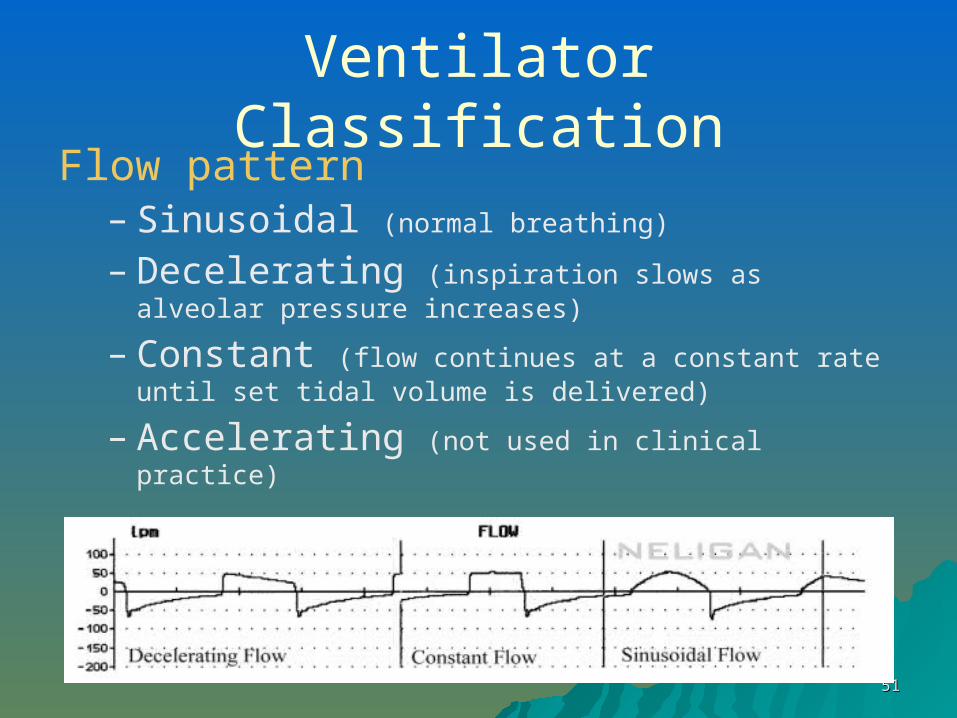
Ventilator ClassificationFlow pattern
– Sinusoidal (normal breathing)
– Decelerating (inspiration slows as alveolar pressure increases)
– Constant (flow continues at a constant rate until set tidal volume is delivered)
– Accelerating (not used in clinical practice)
5252
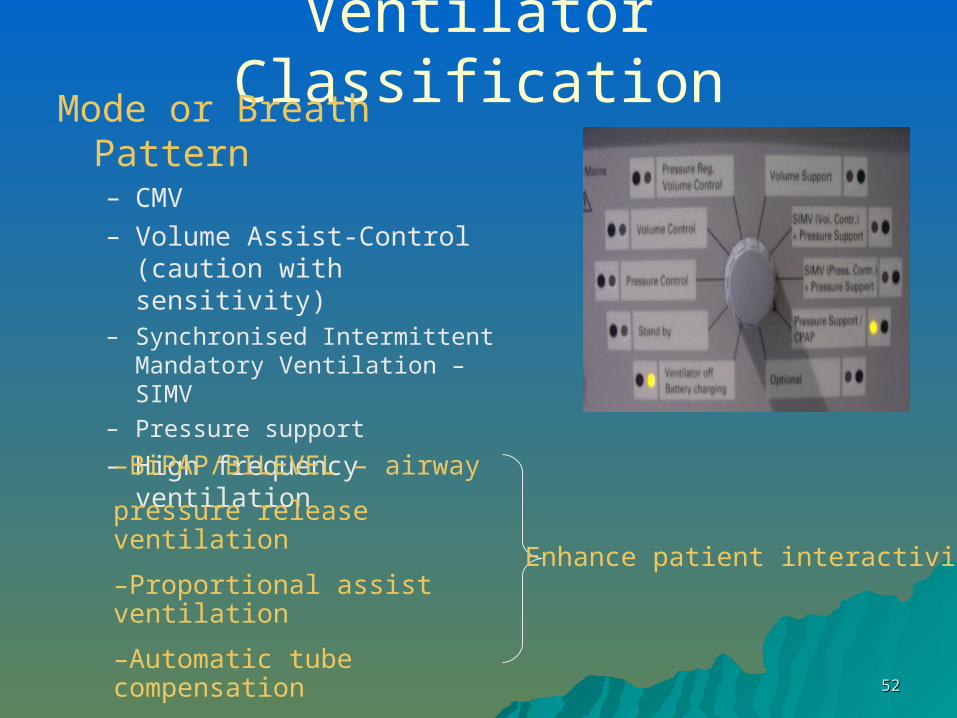
Ventilator ClassificationMode or Breath Pattern
– CMV– Volume Assist-Control
(caution with sensitivity)– Synchronised Intermittent
Mandatory Ventilation – SIMV – Pressure support
– High frequency ventilation
–BiPAP/BILEVEL – airway
pressure release ventilation
–Proportional assist ventilation
–Automatic tube compensation
Enhance patient interactivity

5353
Methods of Ventilation
Synchronised Intermittent Mandatory Ventilation – SIMV
Pressure Control Volume control Pressure regulated volume control Pressure support Continuous positive airway pressure
(CPAP)

5454
Waveforms

5555
So the problem is this
If the patient is hypoxic then they need O2
If still hypoxic then they need +ve pressure If still hypoxic then you need to increase
the Ti time (at the expense of the Te time) Adjustment of the I:E ratio (did) mean
increased sedation as it was impossible to breath with the flipped ratio.
New modes have now been developed to allow spontaneous ventilation on adjusted I:E ratios e.g. BIPAP and APRV

5656
Biphasic Positive Airway Pressure

5757
BIPAP / APRV (Airway pressure release ventilation)
5858
Why is mechanical ventilation bad for you?

5959
Problems with Mechanical Ventilation
Mechanical Ventilation
IntubationProlonged Ventilation
Ventilator Induced Lung Injury

6060
Problems with Intubation

6161
Problems with Intubation
Bypass natural protective mechanisms – moisten, filter, warm
Plastic tubing – airway trauma, vocal cord damage
Pressure sores – oral or from cuff Mouth care! Need sedation

6262
Sedation and Ventilation
Good Points– Reduced pain– Reduced stress– Easier to nurse– Better for relatives– Less chance of lines
falling out
Bad Points– Increased
pneumonia risk– Venous thrombosis– Pressure area
problems– Hypotension– Prolonged ICU stay– Better for relatives– Increased
barotrauma

6363
Problems with Prolonged Ventilation
Barotrauma Volutrauma Oxygen Toxicity Pneumonia (VAP) Sheer Stress – flow delivery

6464
Barotrauma – pressure Air leak from alveoli
situated near respiratory bronchioles
10 – 20% of ventilated patients
Predisposing factors– Frequent +ve pressure
breaths– Infection– ARDS– Hypovolaemia
6565
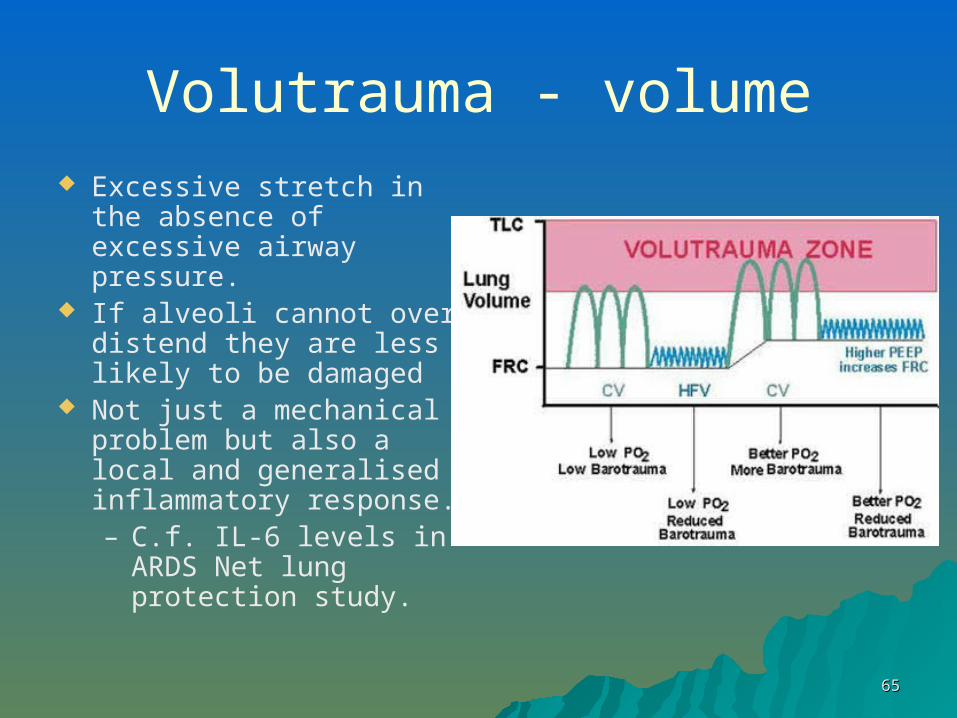
Volutrauma - volume Excessive stretch in the
absence of excessive airway pressure.
If alveoli cannot over distend they are less likely to be damaged
Not just a mechanical problem but also a local and generalised inflammatory response.– C.f. IL-6 levels in
ARDS Net lung protection study.

6666
Volutrauma

6767
Ventilators
Aim to achieve adequate minute volume with the lowest possible airway pressure– High PEEP levels 10 – 20 (open lung)– Permissive hypercapnia– Patient specific tidal volume 6 – 7ml/Kg– Improved inverse ratio capabilities

6868
Oxygen – the risks Highly flammable Compressed Dry gas – Think humidification!
Blindness in neonates (overgrowth of blood vessels)
Drying of mucus membranes / secretions COPD – respiratory drive Toxic – inflammation / scarring after 40hrs with
100% Dry eyes

6969
Oxygen toxicity
Central nervous system– Visual changes, ringing in ears, nausea,
twitching, irritability, dizziness, convulsions
Pulmonary– Lungs show inflammation / scarring
(ARDS) and pulmonary oedema Retinopathic
– Retinal damage

7070
Other Complications
Decreased cardiac output
Pneumonia (VAP) Psychological problems Endotracheal tube
complications– Laryngeal injury– Tracheal stenosis– Tracheomalacia– Endobronchial intubation– Sinusitis

7171
Suctioning and Mechanical Ventilation
Causes Lung de-recruitment due to– Disconnection from the ventilator
Loss of PEEPWorse V/Q mismatch
– Suctioning procedure itselfHigh negative pressure decreases lung
volumeWorse if the suction is open
Suction only when clinically indicated / Pre oxygenate / Minimal suction pressure / limit suction time

7272
Prone Positioning
What a nightmare! Can dramatically
alter oxygenation Also
– Induces a uniform V/Q distribution
– Promotes alveolar recruitment
– Promotes secretion drainage
7373
Prone Positioning
Debate about outcome in the most hypoxic
Complications,– Manual Handling– Accidental Extubation– Pressure sores– Facial Oedema– Line disconnection

7474
Gattinoni et al (2001) NEJM 345 (8): 568
Oxygenation Survival
Improved oxygenation, but not overall survival rate
7575
High-Frequency Oscillatory Ventilation in Adults
Seems a nice idea 3 – 10 Hz oscillation ‘Tidal volume’ less
than normal Less opening and
closing of lungs Well established in
neonatal and paediatric population
Issues, Patients need heavy
sedation / NMJ blockade
Drop in preload Transport not possible Clinical Ex difficult Little research until
now

7676
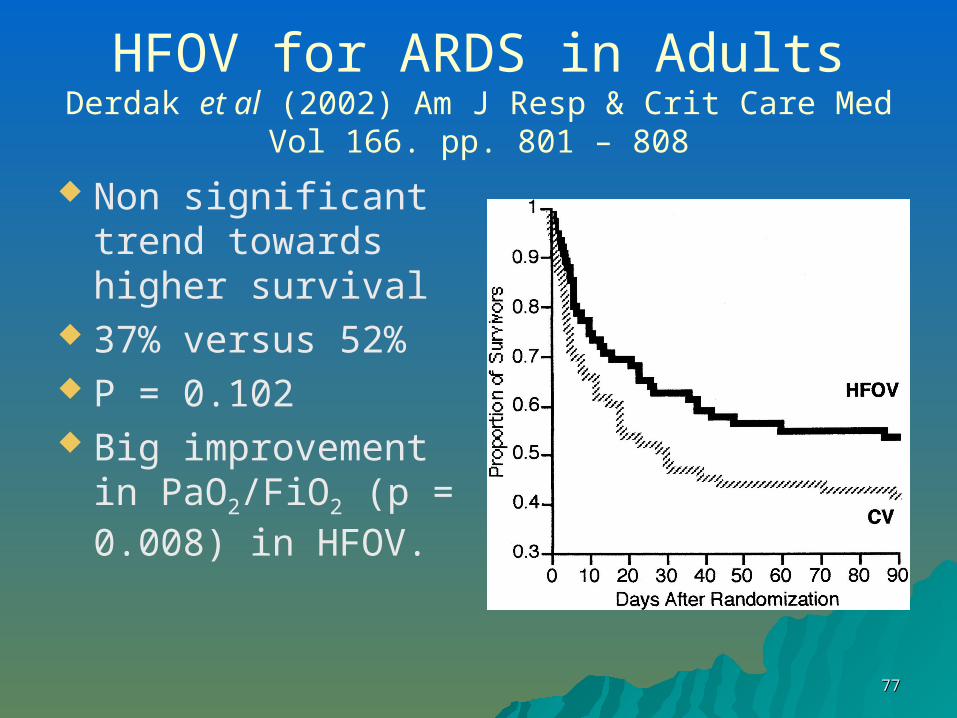
HFOV for ARDS in AdultsDerdak et al (2002) Am J Resp & Crit Care Med Vol 166.
pp. 801 – 808
Multi-centre randomised control trial 148 patients HFOV n = 75 Conventional Ventilation n = 73 Outcome measure was survival
without mechanical ventilation at 30 days
7777
HFOV for ARDS in AdultsDerdak et al (2002) Am J Resp & Crit Care Med Vol 166.
pp. 801 – 808
Non significant trend towards higher survival
37% versus 52% P = 0.102 Big improvement in
PaO2/FiO2 (p = 0.008) in HFOV.

7878
HFOV for ARDS in AdultsDerdak et al (2002) Am J Resp & Crit Care Med Vol 166.
pp. 801 – 808
Unanswered Questions– Ideal timing of the intervention– Prone position– Nitric Oxide– When do you discontinue– Long term effects on lung function– Use of volume recruitment methods

7979
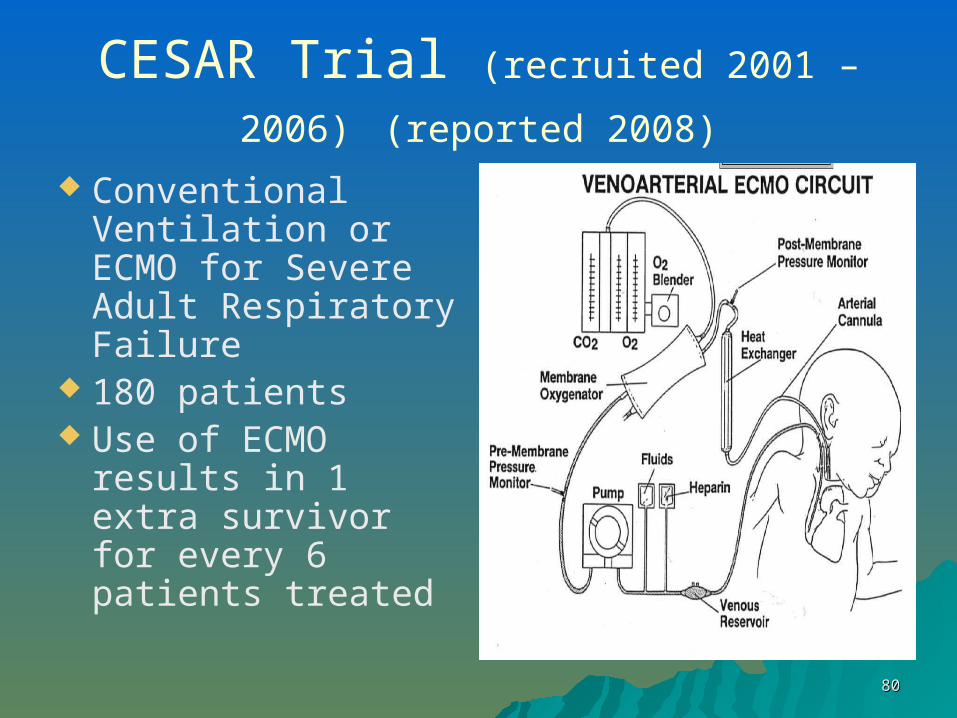
ECMO It involves connecting the
internal circulation to an external blood pump and artificial lung.
A catheter placed in the right side of the heart carries blood to a pump, then to a membrane oxygenator, where gas exchange of O2 and CO2 takes place.
The blood then passes through tubing back into the patient's veins or arteries.
Patients are anticoagulated
8080
CESAR Trial (recruited 2001 – 2006) (reported 2008)
Conventional Ventilation or ECMO for Severe Adult Respiratory Failure
180 patients Use of ECMO
results in 1 extra survivor for every 6 patients treated

8181
Your Patient is Hypoxic So What Do You Do
Remember– “Air goes in and out and blood goes
round and round”– That just getting air into the lungs may
not be enough

8282
Your Patient is Hypoxic So What Do You Do
Decide– How much time to you have?– What resources are available– Is escalation appropriate

8383
Your Patient is Hypoxic - What Do You Do?
– Increase the supply of Oxygen– Drive it into the lungs– Get the lungs in the best shape possible– Make sure blood is getting to the lungs– Reduce the metabolic demand for
oxygen

8484
Scenarios

8585
Case
44 year old lady 11/7 post intubation for pneumonia.
Trachy. FiO2 .3, PO2
11 Sudden SOB FiO2 1.0, Sats 80%
– Increase the supply of Oxygen
– Drive it into the lungs
– Get the lungs in the best shape possible
– Make sure blood is getting to the lungs
– Reduce the demand for oxygen

8686
Case
70 year old gentleman
Sudden SOB HR 150 bpm RR 50 FiO2 0.21
– Increase the supply of Oxygen
– Drive it into the lungs
– Get the lungs in the best shape possible
– Make sure blood is getting to the lungs
– Reduce the demand for oxygen

8787
Case
55 year old Rescued from
smoke filled room PaO2 7 on FiO2
85%
– Increase the supply of Oxygen
– Drive it into the lungs
– Get the lungs in the best shape possible
– Make sure blood is getting to the lungs
– Reduce the demand for oxygen
8888
THE ENDTHE END