1 newborn screening
TRANSCRIPT
UWA PATH3305 lecture 02/04/2015
1
Newborn Bloodspot ScreeningAn expanding public health program
Lawrence Greed
Senior Scientist in Charge
Department of Clinical Biochemistry
Biochemical Genetics Unit & WA Newborn Screening Program
PathWest Laboratory Medicine WA
Newborn bloodspot screening
What to take from this presentation
• What newborn bloodspot screening is?
• The process and principles of screening
• The categories of disorders covered
• The impact of screening on health
1
2

UWA PATH3305 lecture 02/04/2015
2
Newborn bloodspot screening
• Population screening program for inherited (genetic) disease
• Targeted and treatable disorders of metabolism
• Bloodspot sample taken at 48 – 72h of age (The Guthrie Card)
• Australasia – All newborns, voluntary, consented, no charge
• North & South America, Europe, UK
• Worldwide program…
https://reproductivehealth.perkinelmer.com/for_parents/newborn_screening
3
4
UWA PATH3305 lecture 02/04/2015
3
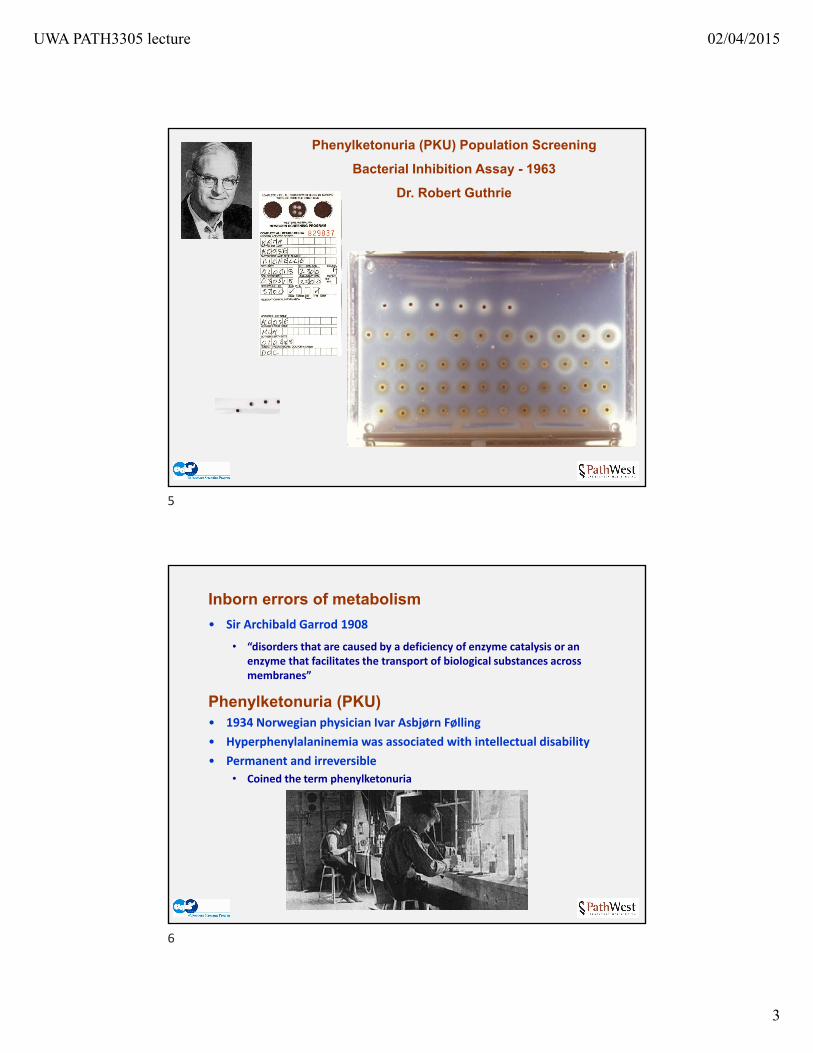
Phenylketonuria (PKU) Population Screening
Bacterial Inhibition Assay - 1963
Dr. Robert Guthrie
Inborn errors of metabolism
• Sir Archibald Garrod 1908
• “disorders that are caused by a deficiency of enzyme catalysis or an enzyme that facilitates the transport of biological substances across membranes”
Phenylketonuria (PKU)• 1934 Norwegian physician Ivar Asbjørn Følling
• Hyperphenylalaninemia was associated with intellectual disability
• Permanent and irreversible
• Coined the term phenylketonuria
5
6
UWA PATH3305 lecture 02/04/2015
4
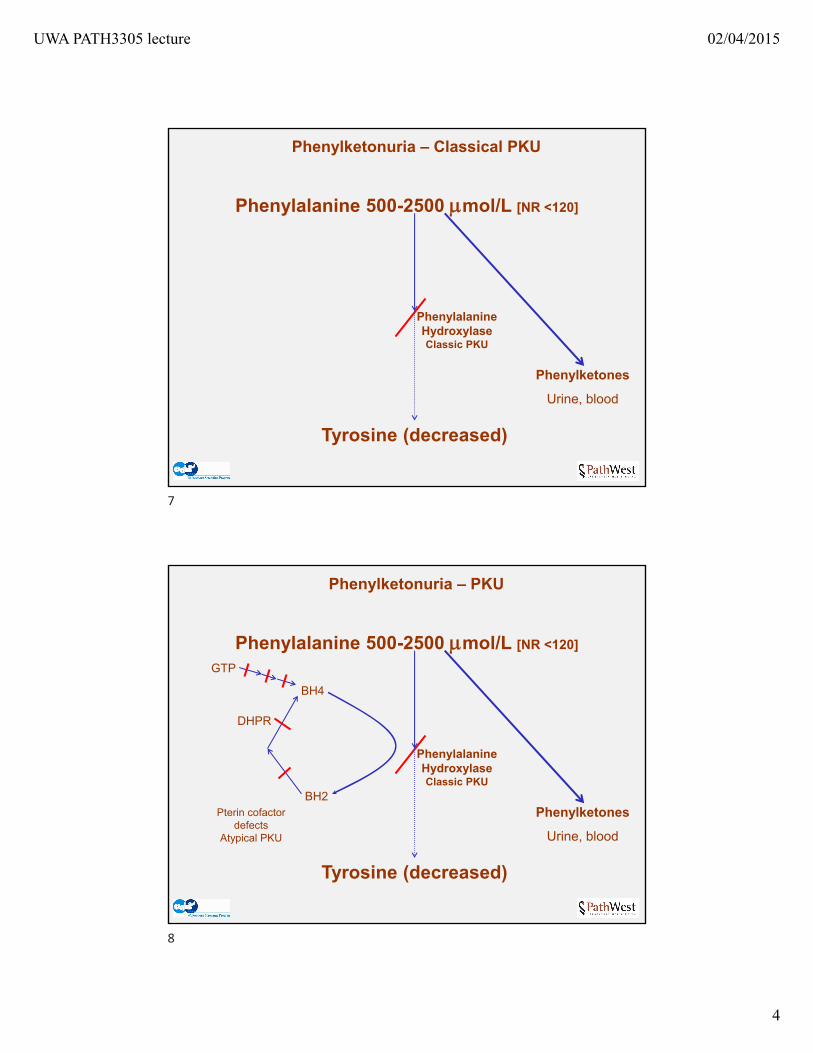
Phenylalanine 500-2500 mol/L [NR <120]
Phenylketonuria – Classical PKU
Phenylketones
Urine, blood
Tyrosine (decreased)
Phenylalanine HydroxylaseClassic PKU
Phenylalanine 500-2500 mol/L [NR <120]
Phenylketonuria – PKU
Phenylketones
Urine, blood
Tyrosine (decreased)
Phenylalanine HydroxylaseClassic PKU
BH4
BH2
DHPR
GTP
Pterin cofactor defects
Atypical PKU
7
8
UWA PATH3305 lecture 02/04/2015
5
NBS Aim
• Pre‐symptomatic detection & treatment of metabolic genetic disease
• 25 targeted disorders in the screening panel (varies on jurisdiction)
• Early detection & treatment prior to metabolic decompensation
NBS Aim
• Pre‐symptomatic detection & treatment of metabolic genetic disease
• 25 targeted disorders in the screening panel (varies on jurisdiction)
• Early detection & treatment prior to metabolic decompensation
Newborn bloodspot screening process
• Bloodspot samples taken (optimally) at 48 – 72h of life by midwife
• The “Guthrie” test – blood spotted onto “filter paper”
• Sample dried & sent by express post/courier
• Analysis by a central NBS laboratory
• Referral to consultant for infant recall & confirmatory testing
9
10
UWA PATH3305 lecture 02/04/2015
6
NBS Aim
• Pre‐symptomatic detection & treatment of metabolic genetic disease
• 25 targeted disorders in the screening panel (varies on jurisdiction)
• Early detection & treatment prior to metabolic decompensation
Newborn bloodspot screening process
• Bloodspot samples taken (optimally) at 48 – 72h of life by midwife
• The “Guthrie” test – blood spotted onto “filter paper”
• Sample dried & sent by express post/courier
• Analysis by a central NBS laboratory – result within 24 (<72h)
• Referral to consultant for recall & confirmatory biochemical/genetic testing
Metabolites vs genetic analysis
• Time/speed, cost, VUSs
• Direct genetic analysis: SCID, SMA…
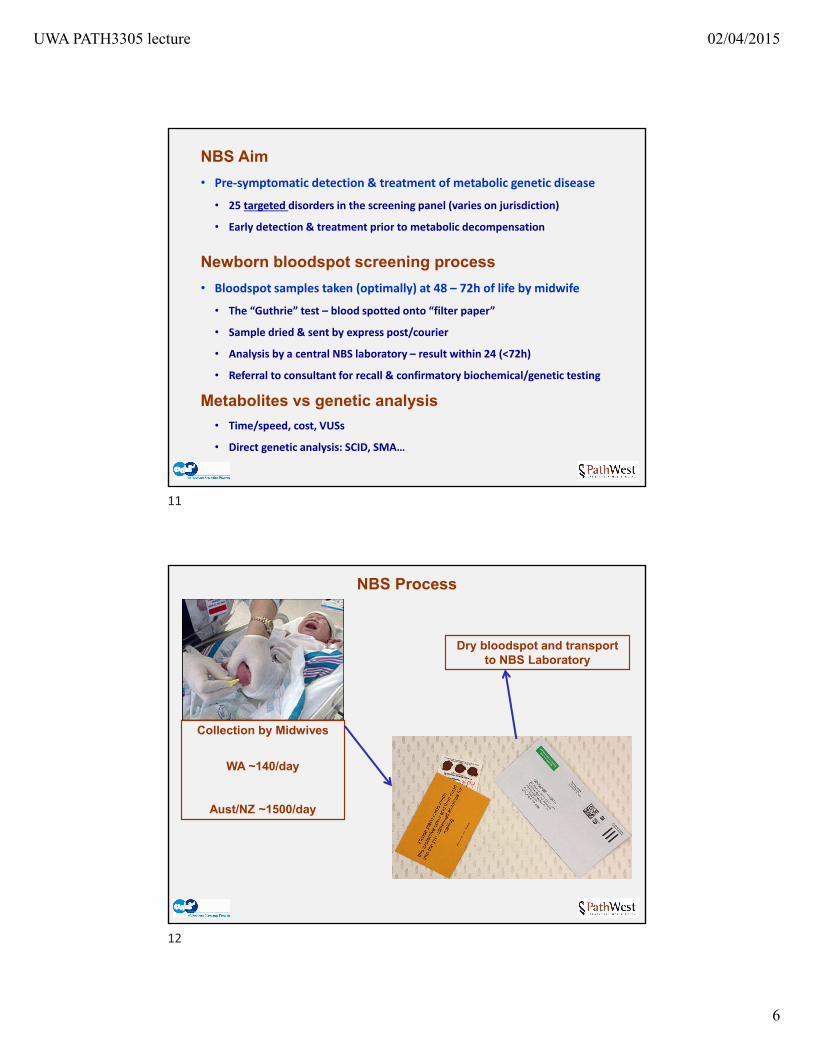
NBS Process
Dry bloodspot and transport to NBS Laboratory
Collection by Midwives
WA ~140/day
Aust/NZ ~1500/day
11
12
UWA PATH3305 lecture 02/04/2015
7
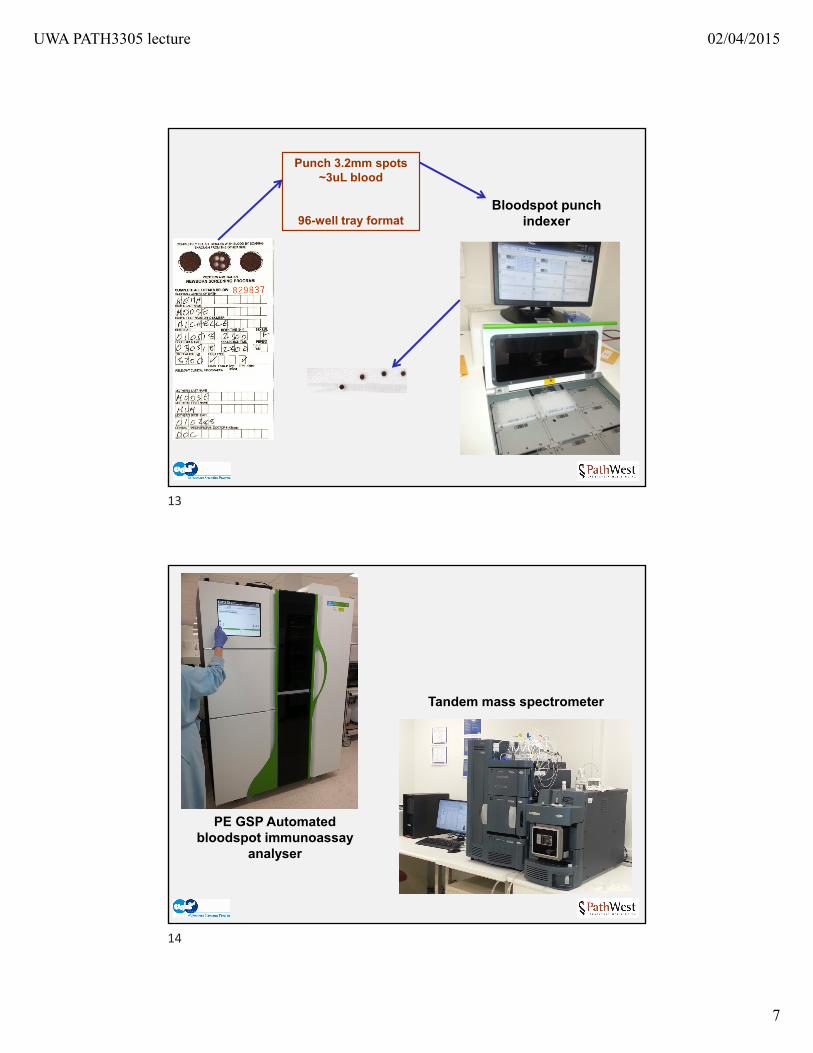
Bloodspot punch indexer
Punch 3.2mm spots~3uL blood
96-well tray format
PE GSP Automated bloodspot immunoassay
analyser
Tandem mass spectrometer
13
14
UWA PATH3305 lecture 02/04/2015
8
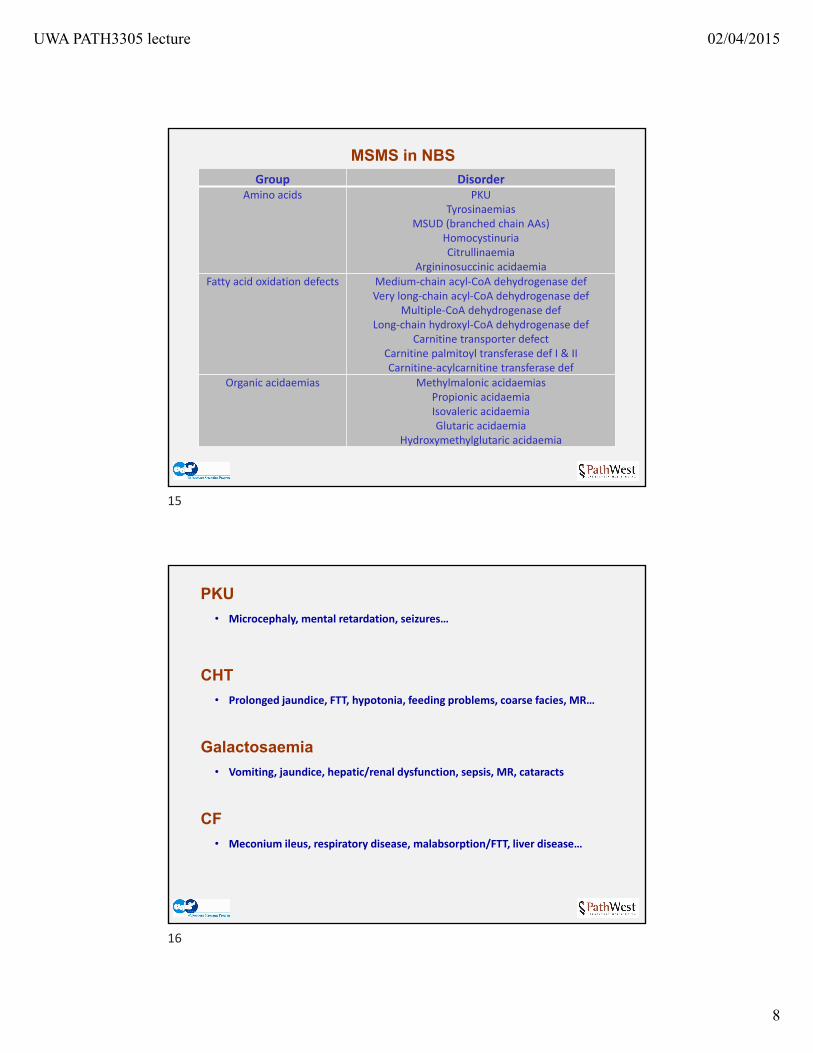
MSMS in NBS
Group DisorderAmino acids PKU
TyrosinaemiasMSUD (branched chain AAs)
HomocystinuriaCitrullinaemia
Argininosuccinic acidaemiaFatty acid oxidation defects Medium‐chain acyl‐CoA dehydrogenase def
Very long‐chain acyl‐CoA dehydrogenase defMultiple‐CoA dehydrogenase def
Long‐chain hydroxyl‐CoA dehydrogenase defCarnitine transporter defect
Carnitine palmitoyl transferase def I & IICarnitine‐acylcarnitine transferase def
Organic acidaemias Methylmalonic acidaemiasPropionic acidaemiaIsovaleric acidaemiaGlutaric acidaemia
Hydroxymethylglutaric acidaemia
PKU
• Microcephaly, mental retardation, seizures…
CHT
• Prolonged jaundice, FTT, hypotonia, feeding problems, coarse facies, MR…
Galactosaemia
• Vomiting, jaundice, hepatic/renal dysfunction, sepsis, MR, cataracts
CF
• Meconium ileus, respiratory disease, malabsorption/FTT, liver disease…
15
16
UWA PATH3305 lecture 02/04/2015
9
Tandem Mass Spectrometry (MSMS)in newborn bloodspot screening
MSMS flow injection analysis (no LC)• Australia 1998 (NSW), 2002 (Vic), and 2004 (WA Qld NZ)
• ACT, NT, Tas covered by other states
• Enabled screening for a large number of disorders, difficult to detect• Measures metabolic markers in an extract of a single bloodspot
• Amino acids, Acylcarnitines• Sequential analysis of a panel of disorders from a bloodspot extract• ~90s sample cycle
LCMSMS in NBS – second tier/reflex selected analysis• Specific analysis on selected screening samples• E.g Specific metabolite analysis (homocysteine, steroid profiling…)
Mass spectrometry panel (MSMS expanded screening)
• Amino acid disorders
• PKU, tyrosinaemias, MSUD, homocystinuria, citrullinaemia, ASAuria
• MR, DD, neurological sequelae (brain, Seizures, MR..)
• Liver dysfunction/failure, renal dysfunction, cardiomyopathy, eye, vascular
• Metabolic acidosis, ketolactic acidosis, hyperammonaemia
• Death
• Fatty acid oxidation – energy supply (oxidation and transport)
• Medium & very long chain FA oxidation, carnitine, ETF cofactor
• Hypoketotic hypoglycaemia, acute encephalopathy
• Neurological sequelae (brain, seizures, MR..)
• Fatty liver (Reye syndrome) & liver dysfunction, cardiomyopathy
• Death
17
18
UWA PATH3305 lecture 02/04/2015
10
Mass spectrometry panel (MSMS expanded screening)
• Organic acidaemias – amino acid degradation (Val, Leu, Ile + others)
• Methylmalonic, propionic, isovaleric, glutaric acidaemias….
• Hyperammonaemia & metabolic acidosis (ketolactic and organic acids)
• Acute encephalopathy
• Neurological sequelae (brain, seizures, MR..)
• Cardiac, liver renal dysfunction
Mass spectrometry panel (MSMS expanded screening)
• Organic acidaemias – amino acid degradation (Val, Leu, Ile + others)
• Methylmalonic, propionic, isovaleric, glutaric acidaemias….
• Hyperammonaemia & metabolic acidosis (ketolactic and organic acids)
• Acute encephalopathy
• Neurological sequelae (brain, seizures, MR..)
• Cardiac, liver renal dysfunction
Not screened by MSMS (in WA/Aus)
• Urea cycle – OTC deficiency, CPS deficiency
• Mitochondrial lactic acidaemias, peroxisomal disorders
• Storage disorders: glycogen, lysosomal
• CAH (Immunoassay + LCMSMS)
19
20
UWA PATH3305 lecture 02/04/2015
11
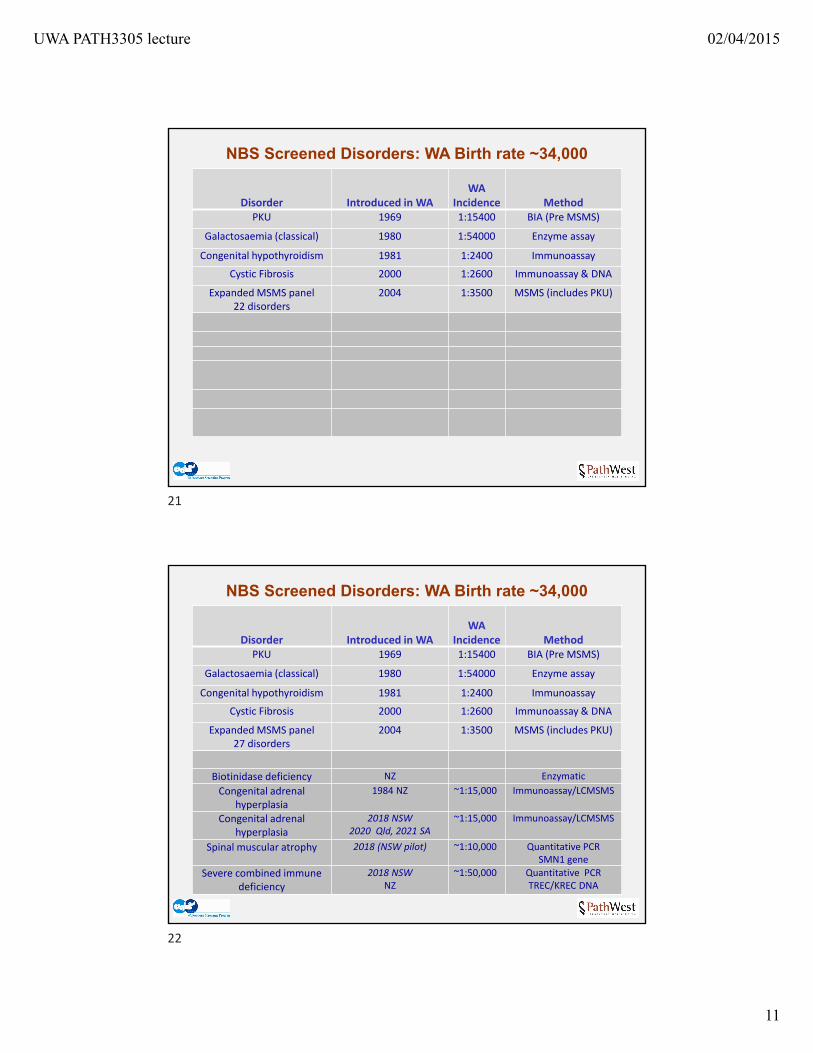
NBS Screened Disorders: WA Birth rate ~34,000
Disorder Introduced in WAWA
Incidence MethodPKU 1969 1:15400 BIA (Pre MSMS)
Galactosaemia (classical) 1980 1:54000 Enzyme assay
Congenital hypothyroidism 1981 1:2400 Immunoassay
Cystic Fibrosis 2000 1:2600 Immunoassay & DNA
Expanded MSMS panel22 disorders
2004 1:3500 MSMS (includes PKU)
NBS Screened Disorders: WA Birth rate ~34,000
Disorder Introduced in WAWA
Incidence MethodPKU 1969 1:15400 BIA (Pre MSMS)
Galactosaemia (classical) 1980 1:54000 Enzyme assay
Congenital hypothyroidism 1981 1:2400 Immunoassay
Cystic Fibrosis 2000 1:2600 Immunoassay & DNA
Expanded MSMS panel27 disorders
2004 1:3500 MSMS (includes PKU)
Biotinidase deficiency NZ Enzymatic
Congenital adrenal hyperplasia
1984 NZ ~1:15,000 Immunoassay/LCMSMS
Congenital adrenal hyperplasia
2018 NSW2020 Qld, 2021 SA
~1:15,000 Immunoassay/LCMSMS
Spinal muscular atrophy 2018 (NSW pilot) ~1:10,000 Quantitative PCRSMN1 gene
Severe combined immune deficiency
2018 NSW NZ
~1:50,000 Quantitative PCR TREC/KREC DNA
21
22
UWA PATH3305 lecture 02/04/2015
12
Criteria for selecting disorders screened
Policy statement on newborn screening: Joint subcommittee of the HGSA and the Division of Paediatrics of the RACP
• There is benefit to the baby from early diagnosis
• The benefit is reasonably balanced against any harms and costs
• There is a reliable test suitable for newborn bloodspot screening
• There is a satisfactory system in place to deal with diagnostic testing and follow-up care of babies with abnormal screening results
These are based on the original screening principles of Wilson & Jungner 1968(Wilson JMG, Jungner G. Principles and practice of screening for disease. Geneva: WHO; 1968. Available from: http://www.who.int/bulletin/volumes/86/4/07‐050112BP.pdf )
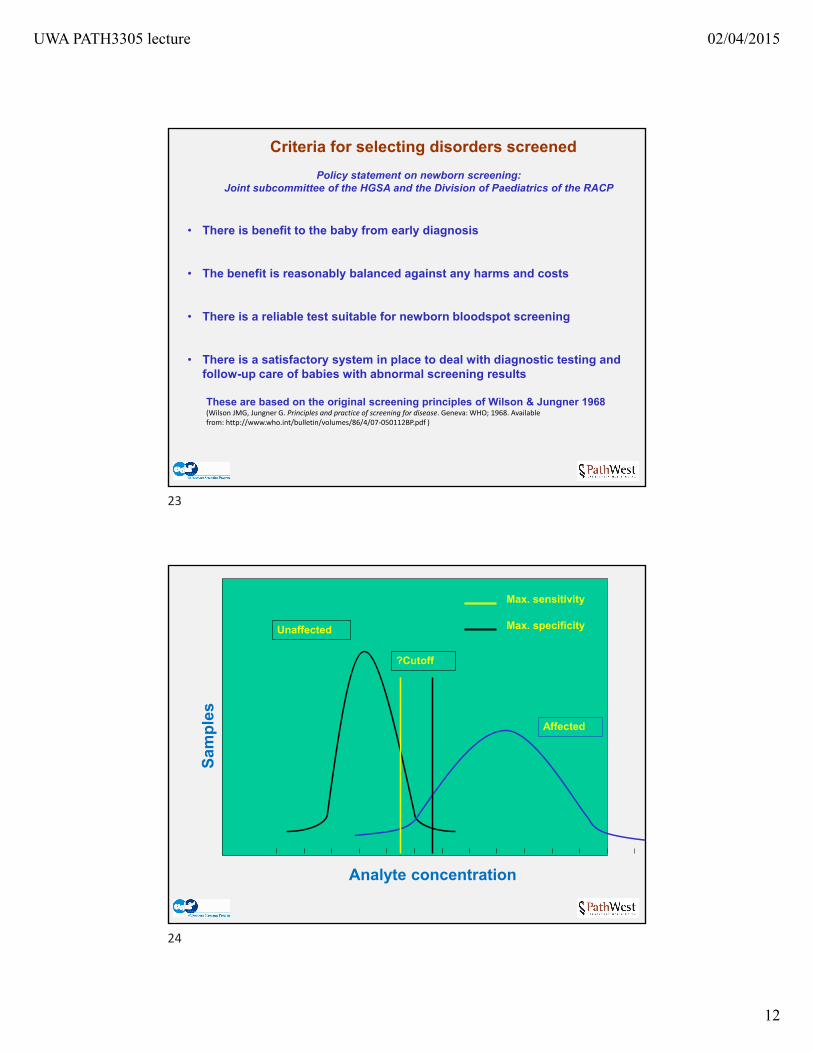
Unaffected
Affected
Analyte concentration
Max. sensitivity
Max. specificity
?Cutoff
Sam
ple
s
23
24
UWA PATH3305 lecture 02/04/2015
13
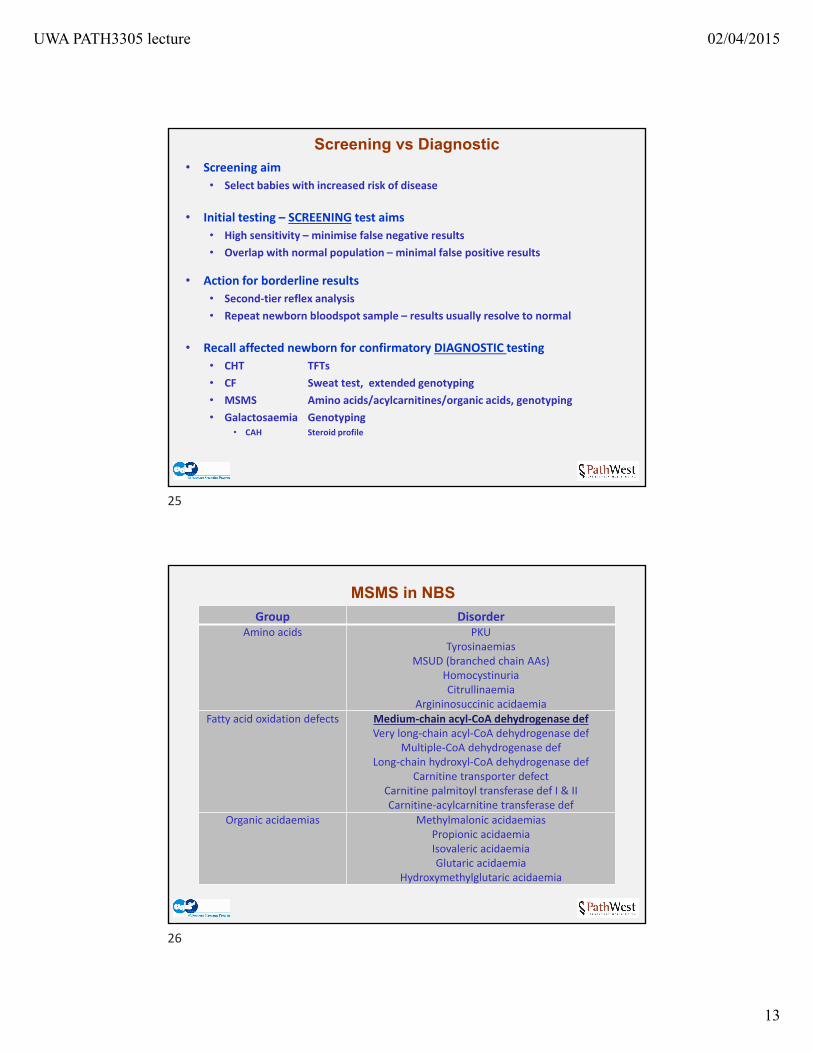
Screening vs Diagnostic• Screening aim
• Select babies with increased risk of disease
• Initial testing – SCREENING test aims
• High sensitivity – minimise false negative results
• Overlap with normal population – minimal false positive results
• Action for borderline results
• Second‐tier reflex analysis
• Repeat newborn bloodspot sample – results usually resolve to normal
• Recall affected newborn for confirmatory DIAGNOSTIC testing
• CHT TFTs
• CF Sweat test, extended genotyping
• MSMS Amino acids/acylcarnitines/organic acids, genotyping
• Galactosaemia Genotyping• CAH Steroid profile
MSMS in NBS
Group DisorderAmino acids PKU
TyrosinaemiasMSUD (branched chain AAs)
HomocystinuriaCitrullinaemia
Argininosuccinic acidaemiaFatty acid oxidation defects Medium‐chain acyl‐CoA dehydrogenase def
Very long‐chain acyl‐CoA dehydrogenase defMultiple‐CoA dehydrogenase def
Long‐chain hydroxyl‐CoA dehydrogenase defCarnitine transporter defect
Carnitine palmitoyl transferase def I & IICarnitine‐acylcarnitine transferase def
Organic acidaemias Methylmalonic acidaemiasPropionic acidaemiaIsovaleric acidaemiaGlutaric acidaemia
Hydroxymethylglutaric acidaemia
25
26
UWA PATH3305 lecture 02/04/2015
14
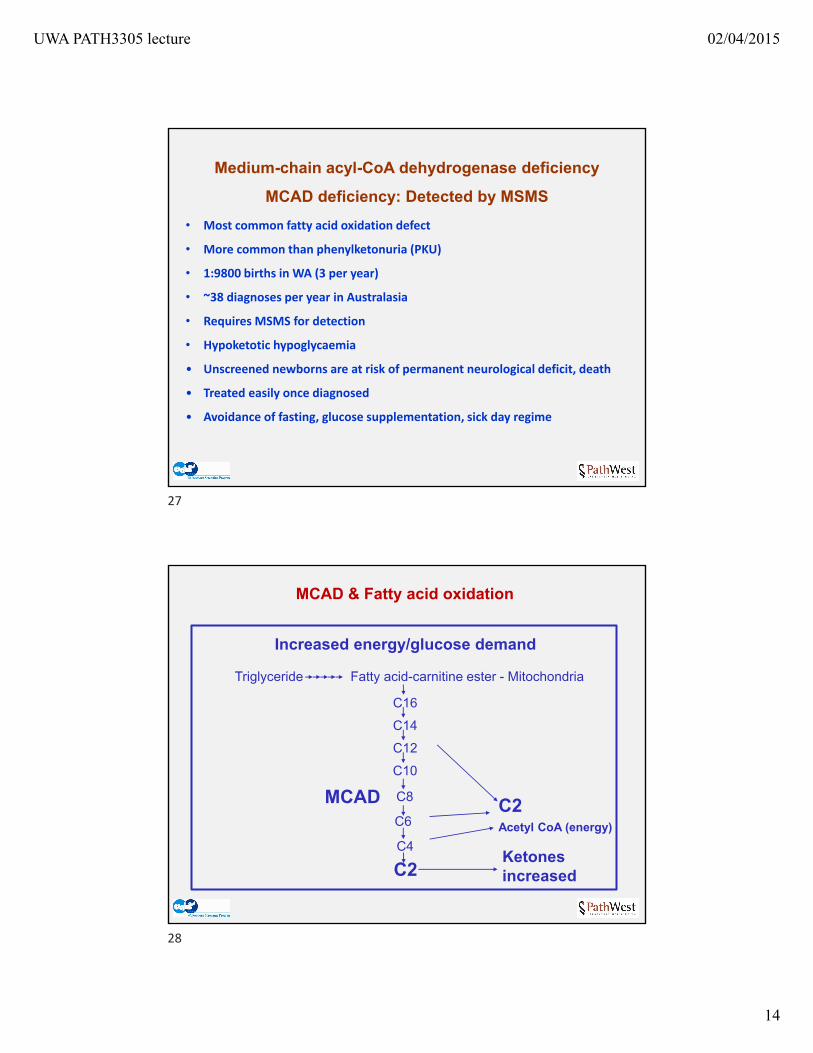
Medium-chain acyl-CoA dehydrogenase deficiency
MCAD deficiency: Detected by MSMS
• Most common fatty acid oxidation defect
• More common than phenylketonuria (PKU)
• 1:9800 births in WA (3 per year)
• ~38 diagnoses per year in Australasia
• Requires MSMS for detection
• Hypoketotic hypoglycaemia
• Unscreened newborns are at risk of permanent neurological deficit, death
• Treated easily once diagnosed
• Avoidance of fasting, glucose supplementation, sick day regime
MCAD & Fatty acid oxidation
MCADC6
C8
C2Ketones increased
Triglyceride
C2Acetyl CoA (energy)
Increased energy/glucose demand
C16
C14
C12
C4
C10
Fatty acid-carnitine ester - Mitochondria
27
28
UWA PATH3305 lecture 02/04/2015
15
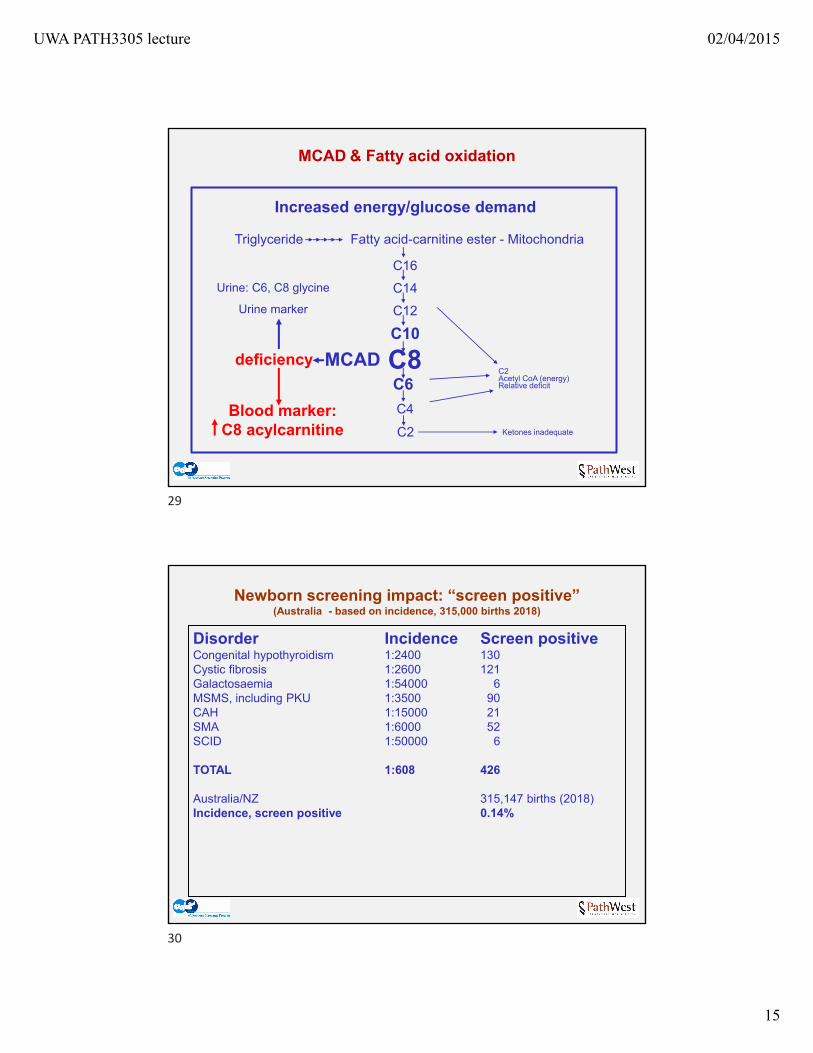
MCAD & Fatty acid oxidation
MCADC6C8
C2 Ketones inadequate
Triglyceride
C2Acetyl CoA (energy)Relative deficit
Increased energy/glucose demand
C16
C14
C12
C4
C10
Fatty acid-carnitine ester - Mitochondria
Blood marker:C8 acylcarnitine
Urine: C6, C8 glycine
Urine marker
deficiency
Newborn screening impact: “screen positive”(Australia - based on incidence, 315,000 births 2018)
Disorder Incidence Screen positiveCongenital hypothyroidism 1:2400 130Cystic fibrosis 1:2600 121Galactosaemia 1:54000 6MSMS, including PKU 1:3500 90CAH 1:15000 21SMA 1:6000 52SCID 1:50000 6
TOTAL 1:608 426
Australia/NZ 315,147 births (2018)Incidence, screen positive 0.14%
4190 screen positive treatable newborns
29
30
UWA PATH3305 lecture 02/04/2015
16
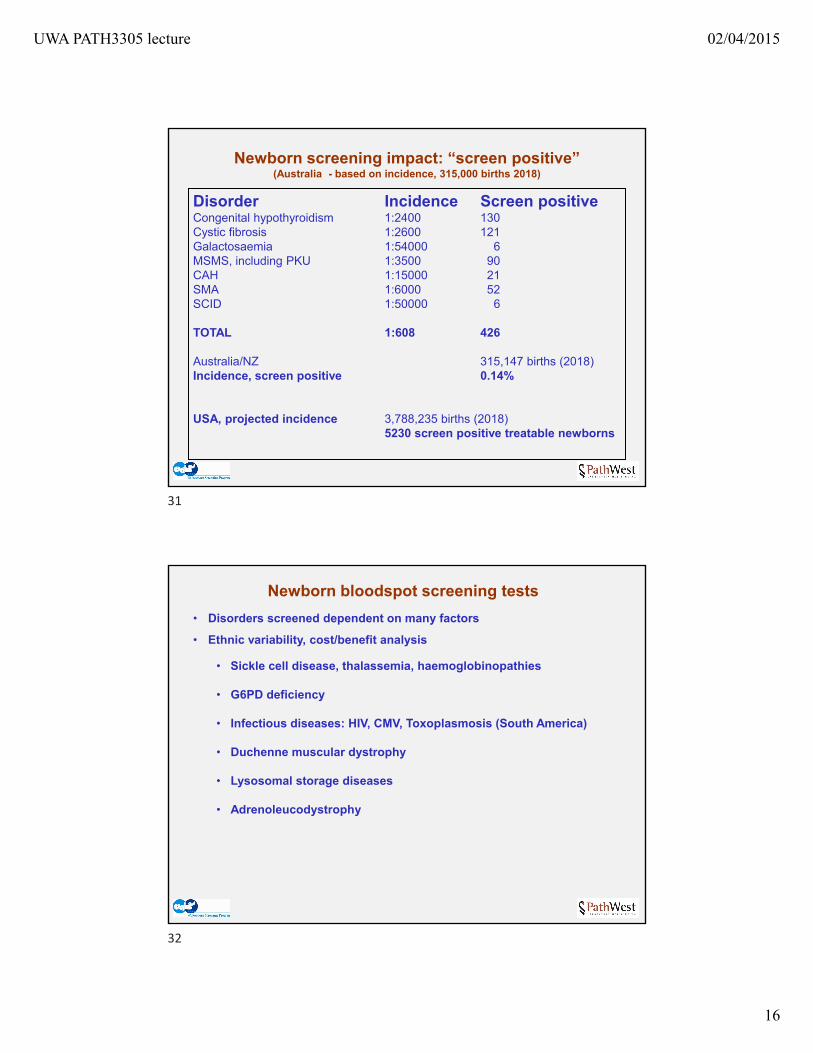
Newborn screening impact: “screen positive”(Australia - based on incidence, 315,000 births 2018)
Disorder Incidence Screen positiveCongenital hypothyroidism 1:2400 130Cystic fibrosis 1:2600 121Galactosaemia 1:54000 6MSMS, including PKU 1:3500 90CAH 1:15000 21SMA 1:6000 52SCID 1:50000 6
TOTAL 1:608 426
Australia/NZ 315,147 births (2018)Incidence, screen positive 0.14%
USA, projected incidence 3,788,235 births (2018)5230 screen positive treatable newborns
4190 screen positive treatable newborns
Newborn bloodspot screening tests
• Disorders screened dependent on many factors
• Ethnic variability, cost/benefit analysis
• Sickle cell disease, thalassemia, haemoglobinopathies
• G6PD deficiency
• Infectious diseases: HIV, CMV, Toxoplasmosis (South America)
• Duchenne muscular dystrophy
• Lysosomal storage diseases
• Adrenoleucodystrophy
31
32
UWA PATH3305 lecture 02/04/2015
17
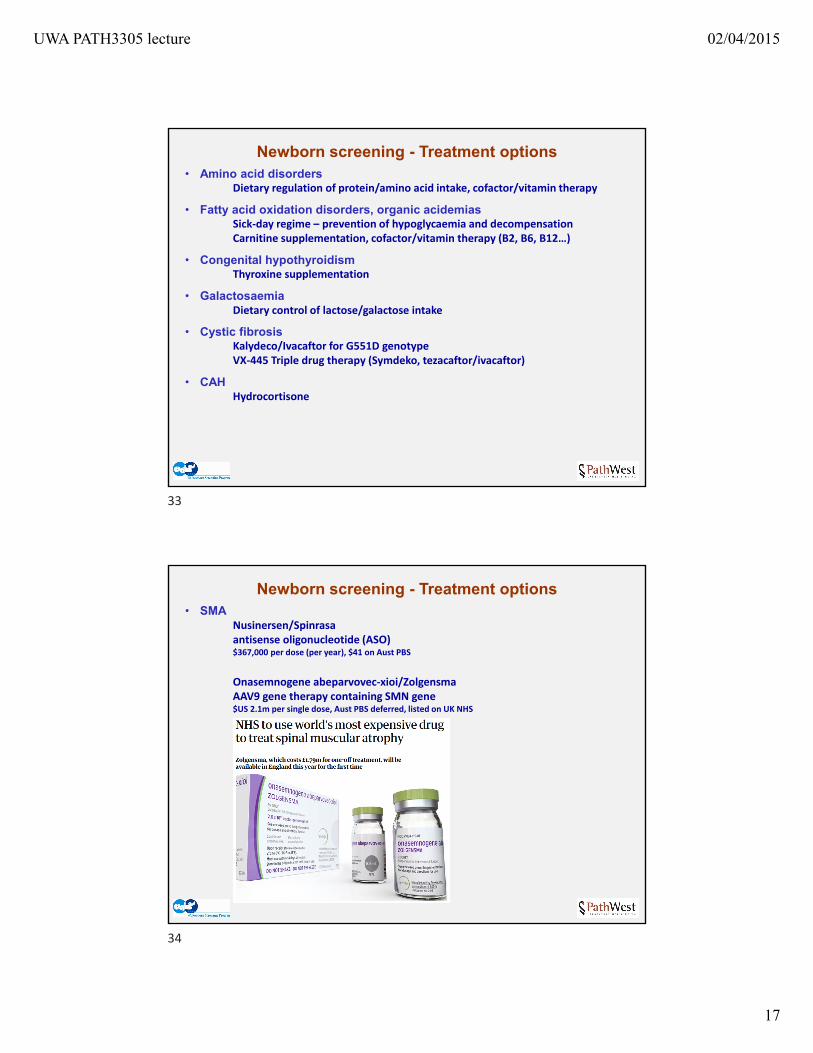
Newborn screening - Treatment options• Amino acid disorders
Dietary regulation of protein/amino acid intake, cofactor/vitamin therapy
• Fatty acid oxidation disorders, organic acidemiasSick‐day regime – prevention of hypoglycaemia and decompensationCarnitine supplementation, cofactor/vitamin therapy (B2, B6, B12…)
• Congenital hypothyroidismThyroxine supplementation
• GalactosaemiaDietary control of lactose/galactose intake
• Cystic fibrosisKalydeco/Ivacaftor for G551D genotypeVX‐445 Triple drug therapy (Symdeko, tezacaftor/ivacaftor)
• CAHHydrocortisone
Newborn screening - Treatment options• SMA
Nusinersen/Spinrasaantisense oligonucleotide (ASO)$367,000 per dose (per year), $41 on Aust PBS
Onasemnogene abeparvovec‐xioi/ZolgensmaAAV9 gene therapy containing SMN gene$US 2.1m per single dose, Aust PBS deferred, listed on UK NHS
33
34
UWA PATH3305 lecture 02/04/2015
18
Newborn screening - Treatment options• SCID
Bone marrow transplant
• Lysosomal storage diseasesEnzyme replacement therapy, BMT
• Duchenne muscular dystrophyExon skipping & stop codon read‐through
• PEG-ylated enzymese.g. Phenylalanine ammonia lyase for PKU
• CRISPR/CAS Gene editingClinical trials active: Beta thalassemia
• Gene therapyVectors, viral vectors, retroviruses, AAV
• Prenatal genetic diagnosis & pre-implantation genetic diagnosis
NBS & cost savings
Economic evaluation of neonatal screening for phenylketonuria and congenital hypothyroidism..
…..A net saving of dollar A2.9 million is attributable to the programme annually. The
economic benefits derive from the prevention of intellectual disability which otherwise incurs costs throughout the life of the affected individual….. (Geelhoed et al J Paediatr Child Health. 2005 Nov;41(11):575-9)
Healthcare Use and Costs of Medium‐chain Acyl‐CoA Dehydrogenase Deficiency in Australia: Screening Versus No Screening
….. screening children cost an average of $A1676 (US$1297) per year for inpatient, emergency department, and outpatient visits, compared with $A1796 for children in whom a clinical
diagnosis was made. Forty‐two percent of the children who underwent screening were admitted
to the hospital, compared with 71% of children who did not undergo screening. Children who did not undergo screening used significantly more inpatient services and
cost significantly more in emergency services. (Haas et al, J Pediatr 2007;151:121‐6)
Economic Evaluation of Tandem Mass Spectrometry Screening in California…..The total estimated, annualized, incremental costs of MS/MS screening of 540,000 births in
California were nearly $5.7 million; 83 affected newborns would be identified…..…..MS/MS screening produced a benefit/cost ratio of $9.32…..….. We found that the benefits
of MS/MS screening outweighed the costs and that the net benefits were significant and robust in various scenarios with various conservative underlying assumptions.…..
(Feuchtbaum Pediatrics 2006;117;S280‐S286)
35
36
UWA PATH3305 lecture 02/04/2015
19
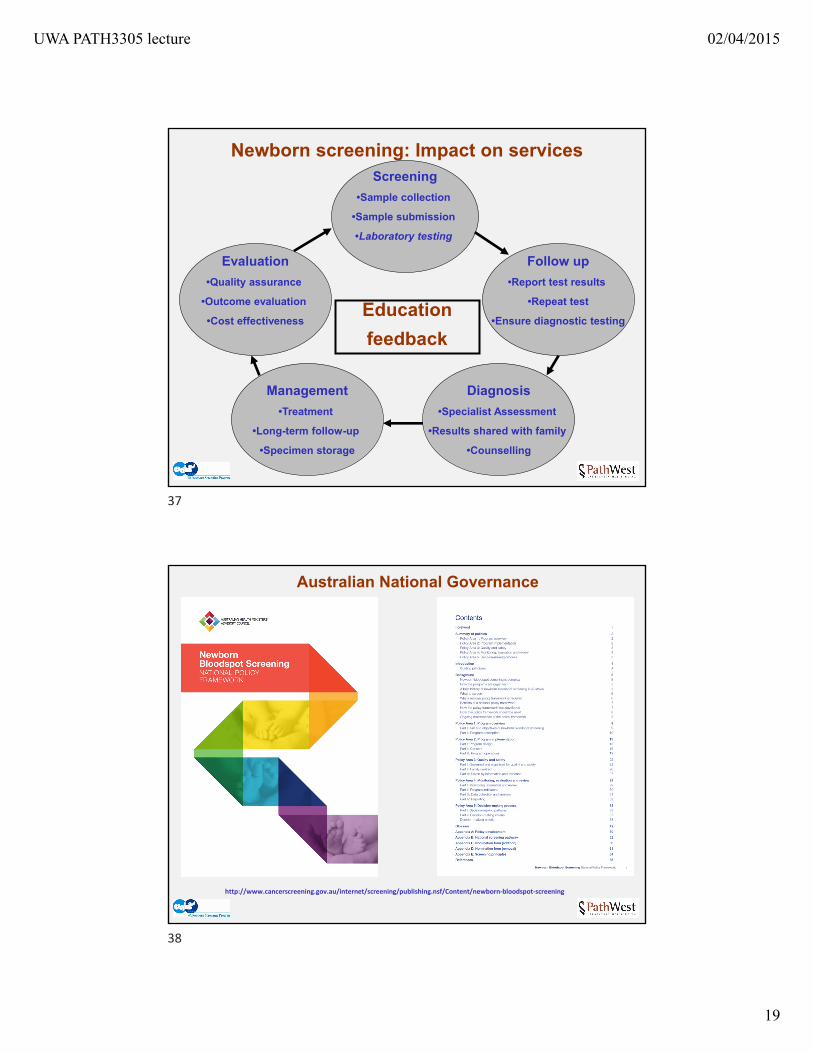
Newborn screening: Impact on servicesScreening
•Sample collection
•Sample submission
•Laboratory testing
Education
feedback
Diagnosis
•Specialist Assessment
•Results shared with family
•Counselling
Management
•Treatment
•Long-term follow-up
•Specimen storage
Evaluation
•Quality assurance
•Outcome evaluation
•Cost effectiveness
Follow up
•Report test results
•Repeat test
•Ensure diagnostic testing
Australian National Governance
http://www.cancerscreening.gov.au/internet/screening/publishing.nsf/Content/newborn‐bloodspot‐screening
37
38
UWA PATH3305 lecture 02/04/2015
20
50 years of NBS
Bacterial Inhibition Agar ‐ 1963
Immunoassay ‐ DELFIA MSMS
50 years of NBS
Bacterial Inhibition Agar ‐ 1963
39
40
UWA PATH3305 lecture 02/04/2015
21
Immunoassay ‐ DELFIA MSMS
DNA Quantification
50 years of NBS
Bacterial Inhibition Agar ‐ 1963
Thank you for listening!
41
42