1 practice questions gastro-intestinal. 1 – a 28-year-old male complains of nighttime abdominal...
TRANSCRIPT

1
Practice Questions
Gastro-Intestinal

1 – A 28-year-old male complains of nighttime abdominal pain that is relievedby food. He has no significant past medical history and does not take any medications. Upper gastrointestinal endoscopy reveals a deep mucosal defect in the first portion of the duodenum. Which of the following is most likely to provide long-term relief in this patient?

A. RanitidineB. SucralfateC. MetoclopramideD. MisoprostolE. AntibioticsF. NSAIDs

2 – A 50-year-old male has had increasingly severe epigastric pain that failed to resolve with over-the-counter antacids. Upper 01 endoscopy shows multiple ulcerations in the stomach, duodenum, and jejunum. Fasting serum gastrin levels are elevated. Imaging studies show a pancreatic tumor with diffuse metastasis. Which of the following is the most effective acid suppressive therapy for this patient?

A. Proton pump inhibitorB. High dose H2 receptor blockersC. Combination of antacids and H2
receptor blockersD. Sucralfate and H2 receptor blocker
therapyE. Octreotide

3 – A patient with multiple medical problems is taking theophylline, warfarin, quinidine, and phenytoin. Despite the likelihood of interactions, dosages of each are adjusted carefully so their serum concentrations and effects are acceptable. However, the patient suffers some GI distress and starts taking a drug provided by one of his “well-intentioned” friends. He presents with excessive or toxic effects from all other medications & blood tests reveal that their serum concentrations are high. Which drug was most likely self-prescribed?

A. CimetidineB. EsomeprazoleC. FamotidineD.NizatidineE. RanitidineF. Misoprostol

4 – A new medication ‘Drug A1 has the following effects on HCI output by the stomach mucosa:

Drug A is most similar to which of the following substances?A. AtropineB.CimetidineC.LansoprazoleD.SucralfateE.Bethanechol

aka “ConsumptionConsumption”

TB is an ancient infectious disease caused mainly by Mycobacterium tuberculosis. Known since 3000 – 2000 BC
TB is a disease of respiratory transmission, optimal conditions for transmission include: overcrowding poor personal hygiene poor public hygiene Malnutrition Poverty
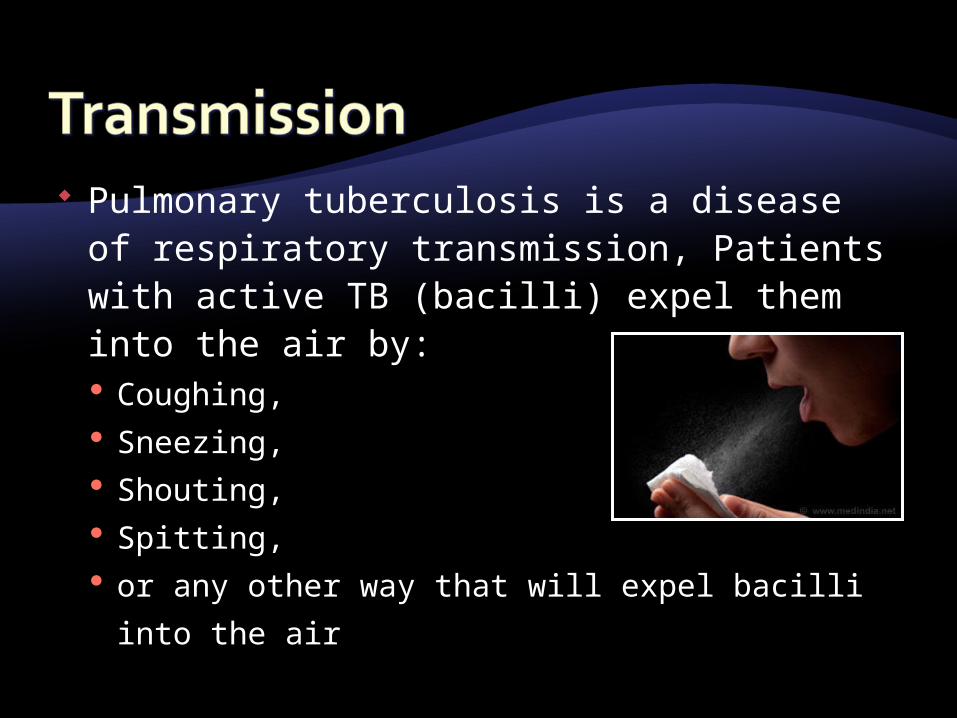
Pulmonary tuberculosis is a disease of respiratory transmission, Patients with active TB (bacilli) expel them into the air by: Coughing, Sneezing, Shouting, Spitting, or any other way that will expel bacilli into the
air


TB Case Rates in U.S.-born vs. Foreign-born Persons, United States, 1993 –
2013*
*Updated as of June 11, 2014.
Case
s per
10
0,0
00

2003 2013
DC
*Updated as of June 11, 2014.
Percentage of TB Cases Among Foreign-born Persons, United States*
DC
>50%25%–49%<25%No cases

TB Case Rates by Race/Ethnicity,* United States, 2003–2013**
*All races are non-Hispanic. **Updated as of June 11, 2014.
Case
s per
10
0,0
00

TB- 2nd to HIV/AIDS as worldwide greatest killer due to a single infectious agent.
In 2013, 9 million people fell ill with TB & 1.5 million died from the disease.
> 95% of TB deaths in low- & middle-income countries & among the top 5 causes of death for women 15 – 44yrs old.
2013, an estimated 550 000 children became ill with TB & 80, 000 HIV-ve children died of TB.
TB is a leading killer of HIV+ patients causing 1/4 of all HIV-related deaths.

Are slender, rod-shaped bacteria with lipid-rich cell wall that stain poorly with Gram stain, but once stained, the walls cannot be easily decolorized. “acid-fast”
Mycobacterial infections are intracellular & result slow-growing granulomatous lesions that cause major tissue destruction eg: granuloma necrosis.
The most common mycobacterial infection: TB
Mycobacteria also cause leprosy



A. Microscopy – B. PPD / Mantoux C. Chest X-ray
A. Microscopy – auramine-rhodamine stain (fluorescent apple-green )
- very sensitive - if positive, followed by acid
fast stain

B. Mantoux Skin Test – ) - Tuberculin (0.1 ml)
injected intra-dermally & read 48 to 72 hrs
- > 5mm in HIV & recent TB contact
- > 10 mm in high risk population
- >15 mm no recent TB contactPPD - if current infection, past exposure, or BCG vaccinated.PPD - if no infection or anergic (steroids, malnutrition, immuno-compromise) & in sarcoidosis.



C. X-Ray – What are we looking for ??
- enlarged lymph nodes ( density)
- regions of excavation - calcifications

Reactivation of M. tuberculosis (e.g., after immune compromise or TNF-α inhibitor use)
has a predilection for the apices of the lung, which have the highest PO2 .
Counselling & Testing for HIV + CD4+ T-cell count in HIV+ (how much ?) AST / ALT testing, AlkP, platelet count,
bilirubin Visual acuity & colour vision testing
(EMB)

Treating tuberculosis as well as other mycobacterial infection poses therapeutic problems.
The organism grows slowly, thus the disease may have to be treated for six moths to two years.

Seen in pts who have had prior therapy Those who fail to comply (e.g. rifampin) Treatment with a single drug MDR – TB:

Multi drug therapy with a minimum of two drugs preferably bactericidal.
Direct observed therapy (DOT) to address the problem of noncompliance

Based on degree of effectiveness and potential side effect.
FIRST-LINE DRUGS: Ethambutol, isoniazid, rifampin, streptomycin and pyrazinamide - (RIPE)
Most effective and less toxic SECOND-LINE DRUGS: Fluoroquinolones,
macrolides, aminosalicylic acid, cycloserine, ethionamide etc.
Second line drugs are less effective and more toxic.


Considered the first drug of choice for the chemotherapy of TB. discovered in 1945 the hydrazide of isonicotonic acid, therefore called INH
Is a synthetic analog of pyridoxine (vit B6)
Only drug that can be used solo with TB

INH is a prodrug that is activated by a mycobacterial catalase-peroxidase (KatG) which inhibits the synthesis of mycolic acid which is part of the bacteria cell wall structure.
is bacteriostatic for resting / slow growing bacilli,
bactericidal for growing/dividing bacilli.


Organism eventually develops resistance. The mechanism of resistance is
related to mutation or deletion of KatG leading to inability to activate the prodrug.

Absorption: INH rapidly absorbed either oral or parenteral route.
Liver metabolized via acetylation resulting in the production of inactive but toxic metabolite called monoacetylhydrazine that is excreted in the urine.
This acetylation is genetically regulated resulting in two types of acetylators: fast and slow acetylators.
Fast-acetylators: have a short half-life(~1 hr) Slow-acetylators: have a long half-life (~3hrs)

Induced Hepatitis (2% of Population) due to the buildup of toxic metabolic products of acetylisoniazid --> acetylhydrazine. Common in fast acetylators.
Hepatic reactions to Isoniazid ↑es with age.
Peripheral neuritis: common adverse effect due to Vit B6 def. & thus can be corrected by supplementation with B6
Others: sideroblastic anemia, SLE(slow acetylators)
INH – Injures Neurons & Hepatocytes

INH interferes with metabolism of phenytoin, therefore increasing the activity of phenytoin and potentiating the adverse effect of phenytoin.
Blocks P450 Prolongs the effect of P450 metabolite
dependent drugs (eg: warfarin ..etc )


Mechanism of Action Rifampin inhibits DNA dependent RNA
polymerase of the bacilli thereby affecting transcription.
Rifampin’s 4 R’s:I. RNA polymerase inhibitorII. Ramps up microsomal cytochrome P-450III.Red/orange body fluids (SE)
IV.Rapid resistance if used aloneV. Rifampin ramps up cytochrome P-450, but
rifabutin does no

Due to alteration of the target enzyme (DNA dependent RNA polymerase) of the drug

Does not cause many side effects in any great frequency.
G.I. upset: Anorexia, Nausea ,Vomiting, Mild abdominal pain,
Hepatitis Red-orange discoloration of body
fluid ( sweat, saliva, stool, urine etc…)


Is an inducer of cytP450, so can decrease the half life of certain drugs that require P450 for their metabolism e.g., warfarin, sulfonyurea, oral contraceptives etc.

Treatment of leprosy Prophylaxis for individuals exposed to
meningitis caused by meningococci or H. influenza


Capreomycin Viomycin Kanamycin STREPTOMYCIN

The first drug used clinically to treat TB 1947-1952; was the only drug available at that time.
is an aminoglycoside antibiotic acts by protein synthesis inhibitor and
decreases the fidelity mRNA & garbles the message, leading to nonsense proteins.
Streptomycin only binds to the 30s subunit

These drugs are: Nephrotoxic - will cause Proteinuria, Hematuria, Nitrogen metabolism, and Electrolyte disturbances
Ototoxic: involving both hearing and balance.
Hearing is irreversible but balance is reversible once drug is stopped.

Bactericidal antitubercular drug. mechanism of action is not understood. Used
in combination with isoniazid and rifampin. Must be enzymatically hydrolyzed to
pyrazinoic acid(active form) by pyrazinamidase
Active against tubercle bacilli in lysosomes and in macrophages.
Adverse effect: gout (DOC ??)


MOA: Inhibition of arabinogalactan, a component of the bacteria cell wall
Adverse effect: inhibits urate excretion – GOUT
OPTIC NEURITIS - vision changes (e.g., blurring, inability to distinguish between red-green color blindness)

. Aminosalicylic acid Capreomycin Cycloserine Ethionamide Fluoroquinolones macrolides

a structural analog of PABA (p-aminobenzoic acid) is bacteriostatic inhibits de novo folate synthesis

GI irritation due to the amount of drug
given (high doses) nausea, vomiting,
bleeding, occurs in 30-40% of the patients. Hypersensitivity reactions Rash, Fever hepatotoxicity All will disappear when the drug is
stopped

Structural analog of isoniazid but not believed to act by the same mechanism
Oral administration Widely distributed throughout the body Adverse effects- hepatotoxicity,
optic neuritis, Peripheral neuropathy.

Also called Hansen disease Caused by Mycobacterium
leprae, (acid-fast bacillus); likes cool temperatures (infects skin & superficial nerves —“glove & stocking” loss of sensation)
Not grown in culture Treated with a triple drug
regimen of dapsone, clofazimine and rifampin for 6 to 24 months to decrease prevalence

Structurally related to sulfonamides It is bacteriostatic MOA: acts as a PABA antagonist to
inhibit folate synthesis Undergoes hepatic acetylation Excreted through urine Adverse effects: hemolysis in pts with
G6PD def, metHb, peripheral neuropathy and erythema nodosum leprosum

X-linked recessive disorder; most common human enzyme
deficiency; more prevalent among African descent
↓↓ NADPH in RBCs leads to hemolytic anemia due to poor RBC defense against oxidizing agents
Microscopy – Heinz Bodies & Bite Cells

A serious and severe skin complication of leprosy which is due to inflammation of fat cells in the face, arms and shins of pts treated with dapsone
Treatment: corticosteroid or thalidomide



MOA: Binds to DNA and prevents it from serving as a template for future DNA replication.
Also has redox properties → production of oxygen free radicals.
Is bactericidal Adverse effect: red-brown discoloration
of the skin, eosinophilic enteritis No erythema nodosum leprosum.


Caused by Adverse Reaction Signs and SymptomsAny drug Allergy Skin rash
Ethambutol Eye damage Blurred or changed visionChanged color vision
Isoniazid,Pyrazinamide,orRifampin
Hepatitis Abdominal painAbnormal liver function test resultsFatigueLack of appetiteNauseaVomitingYellowish skin or eyesDark urine
Common Adverse Reactions to Drug Treatment (1)

Common Adverse Reactions to Drug Treatment (2)
Caused by Adverse Reaction Signs and SymptomsIsoniazid Peripheral
neuropathyTingling sensation in hands and feet
Pyrazinamide Gastrointestinalintolerance
Arthralgia
Arthritis
Upset stomach, vomiting, lack of appetite
Joint aches
Gout (rare)Streptomycin Ear damage
Kidney damage
Balance problems
Hearing loss
Ringing in the ears
Abnormal kidney function test results

Common Adverse Reactions to Drug Treatment (3)
Caused by Adverse Reaction Signs and SymptomsRifamycins
• Rifabutin
• Rifapentine
• Rifampin
Thrombocytopenia
Gastrointestinal intolerance
Drug interactions
Easy bruising
Slow blood clotting
Upset stomach
Interferes with certain medications, such as birth control pills, birth control implants, and methadone treatment