1 presented by joanna larson, senior director of health and business services empowering individuals...
TRANSCRIPT

1
Presented byJoanna Larson,
Senior Director of Health and Business Services
Empowering Individuals to Strengthen Communities
Health Homes Care Coordination: A Key to Integrated Care
& Positive Outcomes

2
Part I: What is Health Homes?

HEALTH HOMES The Health Home program resulted from of the
Affordable Care Act and the Medicaid Redesign Team for NY State
The Medicaid Redesign Team was charged with reducing cost while increasing quality and efficiency in NY’s Medicaid program
The chronically ill represents 25% of Medicaid recipients yet, they drive 80% of the cost (6.9B)
It is estimated that at least 975,000 Medicaid individuals meet the criteria for the Health Homes program
Health Homes will improve the health care provided to both Fee-For-Service( FFS) and Managed Care Plan (MCP) members of the Medicaid program 3

TRIPLE AIM – 3 DIMENSIONS OF VALUE
4
Experienceof Care
Per CapitaCost
Population Health

HEALTH HOMES GOALS
Improve the experience of care Improve health outcomes for chronically ill
clients Reduce Medicaid expenditures
Intended outcomes: The Health Homes Program will save money
by reducing preventable hospitalizations, emergency room visits, and unnecessary care via the provision of a higher level of coordination among the patients’ various care providers
5

ELIGIBILITY CRITERIATwo Chronic Conditions, or a Severe
Mental Illness, or HIV/AIDS. Chronic conditions include, but are not limited
to: mental health disorder substance use disorder asthma diabetes heart disease obesity (BMI over 25) HIV/AIDS Hypertension certain types of cancer
7
6

CLIENT ATTRIBUTION TO HEALTH HOMES
The State uses a combination of the following to assign Medicaid enrollees to Health Homes:o clinical risk groups (CRG), o an algorithm that predicts hospitalizations, and o behavioral health indicators
Medicaid enrollees are assigned to a health home, to the extent possible, based on existing relationships with ambulatory, medical and behavioral health care providers or health care system relationships, geography, and/or qualifying condition.
Initial assignments are for members who qualify for Health Home services but are not currently linked with primary care or case management providers.
7

HOW DOES A HEALTH HOME WORK?
Clients are either found in the community and meet eligibility criteria, or are assigned to us directly by the Health Home
The client is outreached, located, engaged and enrolled
Once enrolled, the Care Coordinator identifies areas of need and current providers in the client’s care team, and referrals are given to fill gaps in service
The Care Coordinator and client collaboratively build a care plan that outlines goals, barriers and strengths
The Care Coordinator collaborates with the various treatment providers in the care team to ensure client compliance and continuity of care
If the client is hospitalized or otherwise involved in a critical event the Care Coordinator takes the lead on transitional care planning and stabilization 8
WHAT ARE HEALTH HOME SERVICES?
Health Home services in accordance with federal and State requirements:
Comprehensive Care Management Care Coordination and Health Promotion Comprehensive Transitional Care Patient and Family Support Referral to Community and Social Support Services Use of Health Information Technology (HIT) when
feasible Quality Measure Reporting to NYS
9

EXAMPLES OF SERVICE PROVISION
Client X’s qualifying diagnosis’ are Schizophrenia and Diabetes. The client is linked with a Therapist and Psychiatrist at an outpatient clinic, but does not have a PCP.
Care Coordinator (CC) will refer Client X to a PCP so that their Diabetes can be monitored and treated appropriately.
CC will coordinate with the Client X’s existing providers to create a comprehensive client centered care plan that is collaboratively arrived at with the input of the client and his/her care team.
Client X’s housing is suddenly compromised – CC works with the client’s care team and community providers to ensure housing is reinstated, or client is relocated. 10

11
Part II: Health Homes Results &
Best Practices

NADAP & HEALTH HOME CARE COORDINATION
Since 1971, NADAP has been working with clients diagnosed with Substance Use Disorders (SUD); in the early years our primary focus was on employment support services for recovering addicts
We have been engaged with multiple Health Homes since 2012
We contract with 7 Health Homes in New York City and partner with 30+ community based treatment providers and 2 hospitals to engage clients in Health Homes Care Coordination
We currently serve approximately1,600 clients in outreach and serve 1,000 enrolled members.
Approximately 50% of our enrolled members are diagnosed with a SUD
12

Health Home Members with Substance Use Disorders
13

ASSESSMENT SCORES The total Average for this sample is 71.55 from a range of 0 – 112
Physical well-being:17Social well-being:10.36Emotional well-being:10.53Functional well-being: 12.71Health Home Functional Questionnaire: 20.95
Clients in Staten Island have lower overall average social well-being scores, followed closely by clients in the Bronx
This sample shows low social/emotional/functional well-being scores on average
Clients who are homeless or who have unstable housing have lower overall emotional well-being assessment scores.
Clients who are linked with SUD services have higher overall assessment scores. 14
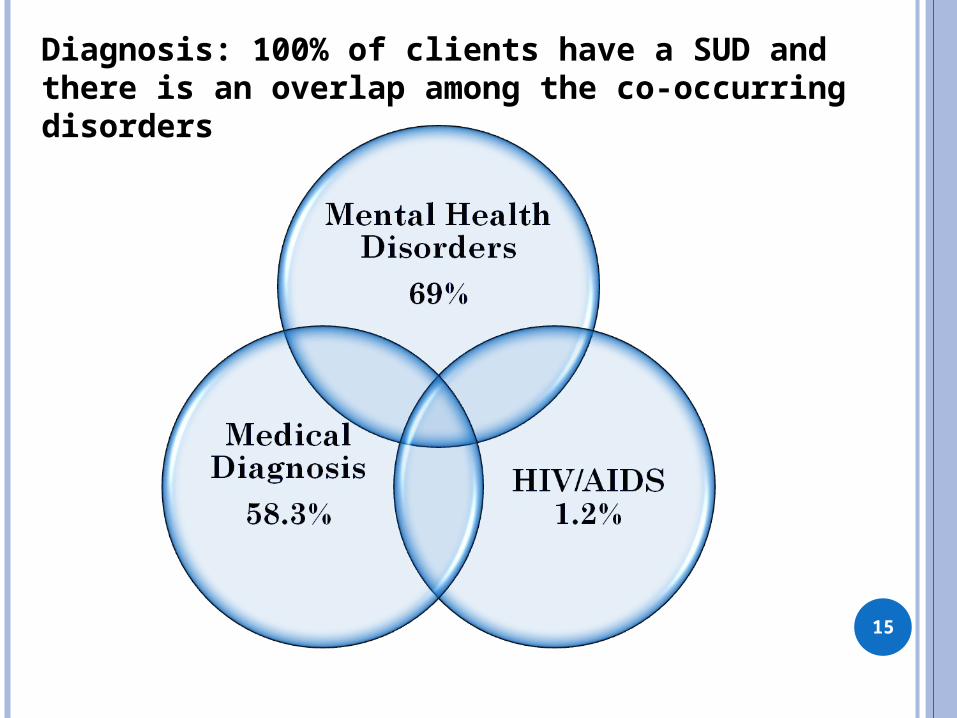
Diagnosis: 100% of clients have a SUD and there is an overlap among the co-occurring disorders
15

WHAT WAS IT LIKE PRIOR TO HEALTH HOMES?
In the years from 2000 through 2012, Medicaid enrollment grew by more than 80 percent statewide to cover about 5 million New Yorkers
With high rates of chronic illness and homelessness the inpatient hospital and ED expenditures skyrocketed
$54 billion in Medicaid expenditures in 2012 in NY alone, which is double or triple the majority of other states in the US
16

OUTCOMES
17

CASE EXAMPLE – CLIENT X Age – 55 Gender – Male Race/Ethnicity – African American Location – Brooklyn, NY Diagnosis – Major Depressive Disorder with Psychotic
Features, Drug Induced Mood Disorder, Diabetes Barrier to achieving wellness – chronic illnesses,
history of non-adherence to treatment, history of chronic homelessness, history of frequent hospitalization
Strengths – Openness to a new service model, engaged with his Care Coordinator, close relationship with his Brother
Average number of monthly contacts/attempts to serve this client – 12 per month; sometimes as many as 20 18

CASE EXAMPLE CONT’D Length of enrollment – 2.5 years Number of months without hospitalization
since enrollment – 29, no hospitalization since enrollment, for the past 2.5 years
Linkages achieved – PCP, Therapist, Psychiatrist, SUD clinic counselor and outpatient program, completed 2010E housing application and was placed in permanent housing
Next Steps – Care Coordinator has recently linked this client with a GED prep program so that he can pursue a degree and employment
19

RESULTS OVERALL
Clients with SUD’s have higher rates of hospitalization than other client populations; even when linked with SUD services
Hospitalization rates are highest among the homeless or clients with unstable housing
Clients who are linked with mental heath services have lower rates of hospitalization
The most common discharge reasons for the SUD HH population: “Inability to Contact/Locate” and “Enrolled HH Patient Lost to Services”
The average number of attempted contacts/interventions required per client per month in the sample is 5, but in some cases as many as 20 in one month are required
20

SUMMARY
What does this tell us about the role that linkage to
Substance Use and Mental Health services
play in the success of the triple aim?
Outcomes are more successful Detox and ED admissions are less frequent Long-term recovery is being supported Care Coordination efforts are more successful Interdisciplinary team approaches are fostered Continuity of care increases
21

LOOKING TO THE FUTURE
Client satisfaction scores –
22
Inquiry Average Answers (1—5)
I have an understanding of what Health Homes are.
4.2
My urgent needs are being met. 4.5
I have been linked to community based treatment for my Substance Use Disorder.
3.9
I feel that my addiction issues have improved since my enrollment in Care Coordination.
3.9
I would recommend Health Homes services to a friend or family member in need.
4.5

NEXT STEPS Build and sustain more co-location projects with
Health Homes staff imbedded in emergency departments, outpatient psych units, detoxes, and rehabs
Ensure that clients are linked with SUD and MH services in the community in order to promote better outcomes
Accurately identify acuity levels amongst clients from a care coordination perspective through use of a risk stratification tool
Inform key stakeholders that more resources are needed to appropriately compensate staff for the intensive work that is required to achieve successful outcomes
Effectively partner with the MCO’s to bridge the gap between health plans and service providers
Increase awareness about Health Homes throughout the larger health care community
23

24
Empowering Individuals to Strengthen Communities
Joanna LarsonSenior Director of
Health and Business Services NADAP
[email protected](212)986-1170 ext. 111

RESOURCES
http://www.health.ny.gov/health_care/medicaid/program/medicaid_health_homes/
http://kff.org/medicaid/state-indicator/total-medicaid-spending/
http://www.ibo.nyc.ny.us/iboreports/2013medicaid.html
https://www.health.ny.gov/health_care/docs/2010-11_medicaid_admin_report.pdf
25