1. scope of synopsis - oecd.org · scope of synopsis. a. industry ... health insurance mutual...
TRANSCRIPT
INDUSTRY SYNOPSIS:
SIC 6325 – ACCIDENT, HEALTH, AND MEDICAL INSURANCE CARRIERS
1. SCOPE OF SYNOPSIS
A. INDUSTRY DEFINITION: For purposes of this study, SIC 6321 and SIC 6324 have been combined into SIC 6325, Accident, Health, and Medical Insurance Carriers. The 1987 Standard Industrial Classification Manual defines SIC 6321, Accident and Health Insurance, as establishments primarily engaged in underwriting accident and health insurance. Establishments that provide health insurance protection for disability income losses and medical expense coverage on an indemnity basis are also included in SIC 6321. Although there are few exceptions, most of the products included in this industry are considered to be non-comprehensive, indemnity products. Indemnity is defined as a benefit paid by an insurance company for an insured loss. In the case of a traditional indemnity health plan, this includes payment to the health care provider for each service rendered (fee-for-service), a maximum dollar amount of benefits provided (benefit ceiling), and a limited amount of covered services (non-comprehensive). These insurance providers may be owned by stockholders, policyholders, or other insurance carriers. Establishments included in this industry are the following:
Accident and Health Insurance Insurance Carriers, Accident Assessment Associations, Accident and Insurance Carriers, Health Health Insurance Mutual Accident Associations Disability Health Insurance Reciprocal Inter-insurance Exchanges Fraternal Accident and Health Insurance Accident and Health Insurance Organizations Reinsurance Carriers, Accident and Health Insurance, Indemnity Plans: Health except Medical Service Plans Sick Benefit Associations, Mutual
According to the SIC Manual, establishments primarily engaged in providing hospital, medical, and other health services in accordance with prearranged agreements or service plans are classified under SIC 6324, Hospital and Medical Service Plans. Medical Service Plans are defined as service plans that provide benefits to subscribers or members in return for specified subscription charges plus additional charges for services rendered, if applicable. Participating hospitals or physicians provide the covered services to members while charging minimal additional fees, in any. In some cases, the plans may include a partial indemnity and service benefits component. All fee-for-service medical service plans included in this industry are considered to be managed indemnity products. They are not pure indemnity products. In addition, they are all prepaid health plans (medical service plans). Also included in this industry are separate establishments of health
1 6325

maintenance organizations that provide medical insurance. Establishments classified in SIC 6324 include the following:
Dental Insurance (providing services Hospital and Medical Service Plans by contracts with health facilities) Medical Service Plans Group Hospitalization Plans
Basically, the distinction between SIC 6321 and SIC 6324 is the method of reimbursement. The two industries essentially produce the same product, coverage against a loss incurred as a result of accident or illness. The distinction is becoming more blurred as many commercial insurers in SIC 6321 have begun offering HMO or other similar managed care products that typically fall under SIC 6324. Thus, with the implementation of the North American Industrial Classification System (NAICS), the Accident and Health Insurance industry and the Hospital and Medical Service Plan industry will be combined into the Direct Health and Medical Insurance Carriers industry (NAICS 524114). Disability Income Insurance Carriers (NAICS 524113), Other Insurance Funds (NAICS 525190) and Reinsurance Carriers (NAICS 524130) will not be included in NAICS 524114. Therefore, the following types of establishments will most likely be included in this industry:
Accident and Health Insurance Group Hospitalization Plans Assessment Associations, Accident and Hospital and Medical Service Plans Health Insurance Insurance Carriers, Accident Dental Insurance (providing services by Insurance Carriers, Health by contracts with health facilities) Medical Service Plans Fraternal Accident and Health Insurance Mutual Accident Associations Organizations Sick Benefit Associations, Mutual
NAICS 524114, does not include HMO’s that provide services at their own facilities or through physicians employed directly by the HMO. Primary Output The primary output of SIC 6325 is risk protection and financial intermediation. Financial intermediation is the service of managing someone else’s money generally with the goal of increasing its value. In order to assume the risk against a premature death, life insurance companies charge a premium which is insufficient to cover claims payments. Therefore, companies invest their premiums using the interest income generated to offset their lower premium rates in order to pay a death benefit to the beneficiary upon the death of the policyholder. Classification of Establishments Individuals may purchase health insurance from commercial insurers (stock or mutual companies), government agencies, associations such as Blue Cross and Blue Shield, fraternal organizations, assessment associations, high-risk state pools, and some employers who self insure. The most common types of accident and health insurance companies are commercial companies, which include stock companies and mutual companies. A stock company is a corporation, which is owned by stockholders. Most stock companies provide non-participating policies. That is, policyholders are not affected by any profits or losses of the company. A mutual company is a corporation, but it has no stockholders. Instead, it is owned by the policyholders themselves. Tax-free dividends are paid to policyholders essentially as reimbursement for the overpayment of
2

premiums. Commercial insurers are beginning to offer group health insurance only, although individual plans are still available from most. Due to the rise of managed care, many commercial insurers have begun offering HMO and PPO plans in addition to the traditional fee-for-service indemnity type policy. The federal government provides health insurance to many individuals through Medicare, the Civilian Health and Medical Program of the Uniformed Services (CHAMPUS), and the Civilian Health and Medical Program of the Department of Veterans Affairs (CHAMPVA). All of these government sponsored health insurance plans that are not paid through a private insurance company are considered to be out of scope. Except for Medicare Part B, these programs provided by the federal government do not require monthly premium payments for those who qualify. Private fee-for-service plans (PFFS), and Medicare HMO’s and Medicaid HMO’s can replace traditional Medicare Part’s A & B and may sometimes require a small premium to be paid by the member as well. The federal government provides funding in order to assist the state governments in providing health care coverage for the poor. This program is called Medicaid. As with the majority of federal programs, premiums are not required by participants. However, some states allow people to buy into the Medicaid program. One example is the Arizona Medicaid program. The federal government insures approximately 74 million Americans through Medicare and Medicaid. This represents almost one third of the population of the United States. Medicaid and Medicare Parts A & B are considered to be out of scope as well. Blue Cross and Blue Shield, commonly referred to as “The Blue’s”, are currently non-profit community health service corporations that contract with hospitals, physicians, and other health care providers to provide prepaid health care to “subscribers.” Blue Cross and Blue Shield are separate companies that usually share office space and have joint enrollment and billing. Blue Cross began as a hospital insurance provider only. Blue Shield began as a medical service and surgical provider. Today, Blue Cross/Blue Shield offers comprehensive health care policies. There is a national Blue Cross and Blue Shield Association in Chicago that coordinates the sixty local Blue Cross plans and sixty-five Blue Shield plans. The majority of Blue Cross’ and Blue Shield’s subscribers are in group plans, although individual plans are available. Unlike traditional commercial insurers, the Blues traditionally offer service benefits and first dollar coverage. The insured pays monthly premiums and does not have to pay additional charges for most medical services covered by the plan. Today, many of the Blues’ companies offer HMO and PPO plans. Also, some Blues are attempting to become for profit companies and model commercial insurers. Blue Cross and Blue Shield plans collectively insure approximately 68 million people. This represents one fourth of the total population of the United States. Fraternal Organizations are incorporated societies, which are formed solely for the benefit of their members and their beneficiaries. In the past, many fraternal organizations offered health insurance to their members through a self-funded plan. Today, many organizations negotiate special rates for their members through commercial insurers or other health plans. In this case, the fraternal organization would not be considered the health insurance provider. Assessment companies offer insurance to members of a fraternal organization as well as the general public. Like mutual companies, assessment companies offer dividends to their policyholders. However, these companies may also charge an additional premium or assessment. Another source of health coverage is a high-risk state pool. As of 1997, seventeen states had a high-risk pool. These risk pools offer guaranteed availability of health insurance to all individuals
3 6325

regardless of their health. The pools are created for those who were denied health care coverage by commercial insurers due to a preexisting condition, those who have coverage at a high cost, or those who have coverage with severe limitations built into the policy. Although each state may have different rules governing its pool, the design of the pool is similar. In most cases, an association of all entities providing health insurance in the state, excluding large corporations that are self-insured, is created to offer insurance. One member of the association administers the plan under the guidelines for benefits, premiums, deductibles, and other matters as outlined in the state’s law. Residents that meet the eligibility requirements are able to purchase insurance from the plan. The states that currently have high risk pools are California, Colorado, Connecticut, Florida, Georgia, Illinois, Indiana, Iowa, Louisiana, Maine, Minnesota, Missouri, Montana, Nebraska, New Mexico, North Dakota, and Wyoming. Since these high-risk state pools are state subsidized, they are considered to be out of scope. Today, many corporations are providing health insurance benefits directly to their employees through a self-insured fund. Corporations providing insurance to their employees through this mechanism are not bound by the same regulation as commercial insurers and other providers. Self-insured plans are governed by ERISA (Employee Retirement Income Security Act). This type of insurance is out of scope for PPI but will be collected for CPI. However, the fees received by an insurance company for administering claims for these policies are in scope for PPI. Other SIC’s Possibly Confused with SIC’s 6321 and 6324 (NAIC 524114): SIC 6311 – Life Insurance Establishments primarily engaged in underwriting life insurance. Half of these establishments also provide health insurance. SIC 6331 –Fire, Marine, and Casualty Insurance (Property and Casualty Insurance) Establishments primarily engaged in underwriting fire, marine, and casualty insurance. SIC 6371 – Pensions, Health, and Welfare Funds Establishments primarily engaged in managing pension, retirement, health, and welfare funds. SIC 6399 – Insurance Carriers, Not Elsewhere Classified Establishments primarily engaged in underwriting insurance, not elsewhere classified, such as insuring bank deposits and shares in savings and loan associations.
**NOTE** Many health insurance companies provide life insurance and property and casualty insurance. Typically, there are separate departments with separate records for each service. Each department is to be considered a separate PMC.
B. CONTEXTUAL OVERVIEW
In 1992, total revenue of SIC 6321 was much lower than that of SIC 6324. Total revenue for SIC 6321 was $23 billion compared with $124 billion for SIC 6324. Revenues for both of these industries should increase as health care costs continue to rise and the population increases. In addition, the trend in federal legislation has been to require employers to offer policies providing
4

more coverage for longer periods of time, even after an employee is laid off. If legislation and medical inflation cause health insurance premiums to be so high that many more people will no longer be able to afford coverage, future revenue may decrease in this industry. Approximately 72% of households owned health insurance in 1998. Nearly 88% of all Americans had some form of coverage. As long as health care costs do not rise significantly, the number of those who own some form of health insurance coverage should continue to rise. HMO’s have enabled many to afford health insurance coverage by offering more coverage, less options, and containing health care costs in general. In fact, most of the growth in this industry will be fueled by HMO policies. The difference between managed care (HMO’s, PPO’s, etc.) and fee-for-service products will be discussed in Types of Services and Estimated Value of Output.
Currently, 80% of all Medicare recipients own supplemental or Medigap policies. As the population ages, more of these policies will be sold. In addition, more long-term care and disability policies will be sold. The following chart shows 1996 indemnity and managed care enrollment in the private, Medicaid and Medicare markets:
Indemnity & Managed Care Enrollment
55
112.5
34
419 13
020406080
100120
PrivateIndemnity
PrivateM anaged
Care
M edicareIndemnity
M edicareM anaged
Care
M edicaidIndemnity
M edicaidM anaged
Care
Type of Plan
Enro
llmen
t in
Mill
ions
This chart shows the difference between managed care and indemnity plan enrollment in the private and public sectors of the accident and health insurance industry. Sixty-eight percent of people enrolled in a private health plan, are members of a managed care plan. The remaining 32% own an indemnity plan. Conversely, 24% of people enrolled in either Medicare or Medicaid were enrolled in some type of managed care plan. Seventy-six percent of people enrolled in a government subsidized health plan were enrolled in an indemnity plan. The number of people enrolled in managed care plans has been steadily increasing in recent years. This number is expected to increase even more as more Medicare and Medicaid members make the transition from traditional indemnity to managed care plans. The anticipated growth in the managed care market will most likely be at the expense of the indemnity market. The federal government already pays a large portion of the total cost of individual health care in America. It should also be noted that 29%, or 70 million, of all Americans are enrolled in some type of federal government subsidized health insurance program, namely Medicare and Medicaid.
5 6325

As the population ages, this percentage and number is likely to increase. In addition, a severe recession may cause many more people to be eligible for Medicaid.
2. INDUSTRY OVERVIEW A. NUMBER OF ESTABLISHMENTS AND COMPANIES
According to the 1992 Census, there were 1,846 establishments in SIC 6325. The number of establishments has been steadily decreasing as mergers and acquisitions continue to occur in these industries. As competition increases, the need to be large enough to offer substantial cost savings to the consumer becomes more important. Approximately 96% of these companies were stock companies. The remaining establishments were mutual companies or non-profit corporations. In 1992, there were at least two companies domiciled in every state, including the District of Columbia.
B. SIZE AND TYPE OF PRODUCTION BY SIZE
The smaller health insurance companies generally solicit business in a very specific geographic area, near their respective headquarters. Larger companies tend to provide insurance nationwide or in multiple regions. However, the size of the company does not dictate the variety of health insurance products offered.
C. MAJOR SERVICE PROVIDERS AND CONCENTRATION RATIOS
The tables below provide a list of the top ten companies ranked by their assets for accident and health and medical service plan companies. In addition, the tables below give market share data.
ACCIDENT AND HEALTH INSURANCE Company Total Assets Market Share (in billions) 1. Prudential 219.3 9.0% 2. Lincoln National Corporation 119.1 5.0% 3. Cigna Corporation 108.2 5.0% 4. Connecticut General Life 108.0 5.0% 5. Northwestern Mutual Life 54.0 2.5% 6. Mass Mutual Life 53.3 2.5% 7. Principal Mutual 50.0 2.4% 9. Liberty Mutual 50.0 2.4% 10. Aetna 37.0 1.5% Source: The Information Access Company (IAC), 1997.
6

MEDICAL SERVICE PLANS
Company Total Assets Market Share (in billions) 1. Aetna 96.0 15.0% 2. Hartford Life 79.0 11.0% 3. Kaiser 11.0 3.0% 4. Group Health Coop of Puget Sound 5.8 1.5% 5. Pacificare 5.4 1.5% 6. Standard Insurance Company 4.1 1.3% 7. Foundation Health 4.0 1.3% 8. Wellpoint Health Networks 3.4 1.2% 9. Blue Cross/Blue Shield of MI 3.1 1.2% 10.Blue Cross/Blue Shield, FL 3.0 1.2% Source: Information Access Company, 1997 The following concentration ratios show the percentage of assets for the top 4, 8, 20, and 50 firms in each industry: Accident & Health Medical Service Plans Top 4 Firms 18% Top 4 Firms 15% Top 8 Firms 28% Top 8 Firms 22% Top 20 Firms 46% Top 20 Firms 41% Top 50 Firms 71% Top 50 Firms 65% Source: Information Access Company, 1997
D. STABILITY OF THE INDUSTRY
Health insurance is a growing industry. As long as the population continues to grow and age, there will be an increasing need for health, long-term care, and disability insurance. Health insurance especially, is considered to be a necessity. However, the number of uninsured increased from 1996 to 1997 and is expected to increase even more in the future. Today, 16.1%, or 40 million of all Americans are uninsured. This is equal to one in six Americans. In addition, 15% of American children are uninsured. The decrease in the number of people on Medicaid, medical inflation, and the increase in the percentage of workers working for small companies that do not offer health insurance are partly responsible for this increase. Medical inflation has been contained recently. However, it could cause major problems in the future if it becomes uncontrollable. Even if health care costs continue to rise, causing premiums to rise, the extra revenue collected from those insured will most likely exceed the loss of revenue from those who
7 6325

will no longer be able to afford coverage. Therefore, the outlook for revenue growth is still positive. Most small companies are able to compete with large companies through regional specialization. There are decreased costs associated with operating locally. In addition, many small firms exhibiting regional domination usually merge with or become acquired by a larger firm. Many of the companies formed more than fifty years ago are still in existence today.
E. GEOGRAPHIC DISPERSION
Geographic dispersion in these industries tends to be fairly even. However, the highest concentration of these companies tends to be in the South and Northeast. The geographic breakdown is given in the table below. REGION % OF COMPANIES West 18% South 29% Midwest 23% Northeast 27% Source: AM Best, 1996.
F. SAMPLE INFORMATION
The sample design was developed with an attempt to meet the needs of both PPI and CPI. For PPI we require a nationwide sample of companies sampled systematically with probability proportional to a measure of size. We also require that items be selected from these companies so that all of our product categories are publishable. The requirements from CPI include that all 87 of their primary sample units (PSU) are covered. The PSUs will be covered by sampling in the states in which the PSUs are located.
3. PRODUCTION INFORMATION
A. SERVICE DELIVERY PROCESS
The primary service of the health insurance industries, as in all insurance industries, is the protection from the risk of a potential loss as well as some degree of financial intermediation.. The main risk is the potential expense and/or income loss associated with either an accident or an illness. Policies included in SIC 6321 or SIC 6324 are promises to pay medical expenses and/or an income loss associated with an illness. In addition, a policy may cover an income loss resulting from a serious accident and subsequent disability. In order to provide this service, accident and health insurance companies are involved in rate determination, underwriting, marketing, and financial activities.
8

Rate Determination: Accident and health insurance policies are priced with the intention of covering all of the related costs associated with conducting business in addition to attaining a certain desired level of profit. Administrative and overhead costs are fairly easy to project. Claims costs are the most significant component of the premium rate. The costs associated with claims are directly related to health care costs in general. If hospital costs increase, claims costs will most likely increase. Thus, premiums will have to be increased in order to attain the same previous level of profit, provided everything else is constant. In addition, insurance companies are required to maintain a certain percentage of premiums as claims reserves. These reserves are used to fund claims, which are made at a later date. This cost is essentially a claims cost as well. Underwriting: Through underwriting, an insurer determines whether or not a potential client is a good risk. In addition, the rate a prospective client is ultimately charged is determined through underwriting. Basically, the underwriter uses various demographic statistics in order to determine the degree of risk and the premium rate. Age, gender, race, geographic location, occupation, marital status, and medical history are all examples of demographic statistics underwriters use to determine the degree of risk of a potential client. Less underwriting is needed for group policies than individual policies. The risk associated with an individual is greater than the risk associated with a group. Therefore, medical history is more likely to be a major consideration in the underwriting process for an individual versus a group. In fact, very little underwriting is necessary for large groups. For small groups, the medical histories and ages of potential group members may be more scrutinized during the underwriting process. Distribution: Since all forms of health insurance companies create similar products in the same way, it is important to mention how these products are distributed. Product distribution is a differentiating factor in the accident and health insurance industry. Agency System: Some agents operate independently, while others operated in company owned field offices. This is the main distribution method use by insurance companies to market their products. Long-term care, accident and disability products are most often sold through independent agents, whereas health insurance is most often sold through company employed field agents. Direct Response Distribution: Through this method, companies make their products available to consumers via television, magazine, telemarketing, and radio advertising. This method is not used very often. Financing: Insurance companies are involved in many investment activities. By investing in various types of high yield investments, insurance companies are able to avoid substantial premium costs and still be able to fund future claims costs and other expenses. However, this is less of a factor in the
9 6325

accident and health insurance industry than it is in the life insurance industry. The main reason being that accident and health insurance companies receive claims almost instantaneously whereas life insurance companies usually do not receive claims until many years after the policy is initiated. In addition, claims costs are the most significant portion of the premium rate in the accident and health insurance industry. Thus, accident and health insurance companies have less money to invest and less time in which to invest it.
B. TYPES OF SERVICES AND ESTIMATED VALUE OF OUTPUT
The health insurance industries provide coverage against a loss incurred as a result of an accident or illness. This coverage is provided through health and medical insurance plans. These insurance plans can take on many different forms. The following pages describe the major service lines of this combined industry. The table below shows the value of receipts for each major service line within SIC 6325 and the percentage of total industry revenue that each service line represents. In addition, primary and other services are presented.
Service Value of Shipments Percent (in 1000) Accident, Health, and Medical Insurance 148259000 100.00% Medical Service Plans 124813000 84.19% Group medical service plans 90400000 60.97% Managed care medical service plans 61200000 41.28% Fee-for-service medical service plans 29200000 19.70% Individual medical service plans 10300000 6.95% Dental service plans (stand alone) 9100000 6.14% Supplemental Medicare service plans 7650000 5.16% Other medical service plans 7363000 4.97% Accident and health insurance 19762400 13.33% Disability 9492856 6.40% Long term care 3279350 2.21% Hospital indemnity 3020454 2.04% Specified disease 1553376 1.04% Accidental death & dismemberment 1294480 0.87% Third-party administrative services 3683600 2.48%
MEDICAL SERVICE PLANS The primary types of medical service plans include managed care, fee-for-service dental, and supplemental Medicare policies. Dental and supplemental Medicare policies can be offered as fee-for-service or managed care products as well. Both fee-for-service and managed care medical service plans are comprehensive plans with unlimited benefits. The fee-for-service plans are “managed indemnity” products. These plans are comprehensive, have unlimited benefits and have some form of utilization review in order to contain costs.
10

It should be noted that group business accounts for a much larger percentage of total industry revenue than individual business. Group business represents 85% of total industry revenue. For both health insurance and dental insurance, 90% of all policies sold are group policies. However, only ten percent of supplemental Medicare policies are group policies. The table below lists the various types of managed care medical service plans available to the consumer. In addition, fee-for-service medical service plans and dental medical service plans sold separately are included in the table. This table will be discussed in the next few pages. The main distinction between a managed care and a fee-for-service product is the method of payment by the client. Clients that own a managed care product generally pay a premium to establish benefits and copayments when services are rendered. Clients that own a fee-for-service product pay a premium to establish benefits and deductibles and coinsurance when services are rendered. Providers are reimbursed differently under the two systems as well. Once again, those that own a managed care product typically have less choice with regard to providers than do those that own a fee-for-service product. By giving up a certain degree of choice, clients that own a managed care product typically pay lower premiums and pay less out of pocket expenses for similar services received. In general, the method of payment is similar for each managed care plan and the degree of choice is different. Any differences in the method of payment between the various managed care plans will be discussed in subsequent pages. The chart shows the typical method of payment and the fee-for-service or managed care designation for each health insurance product type. PRODUCT NAME COVERED SERVICES PAYMENT CHOICE ________________________________________________________________________________ FEE-FOR-SERVICE INPATIENT – HOSPITAL PREMIUM UNLIMITED SURGICAL DEDUCTIBLES MATERNITY COINSURANCE MENTAL HEALTH SUBSTANCE ABUSE PHARMACEUTICALS EMERGENCY LIMITED DENTAL AND VISION ________________________________________________________________________________ PPO SAME AS ABOVE PREMIUM HIGH MANAGED CARE DEDUCTIBLES COINSURANCE ________________________________________________________________________________ POS SAME AS ABOVE PREMIUM MEDIUM MANAGED CARE COPAYMENTS ________________________________________________________________________________ EPO SAME AS ABOVE PREMIUM LOW MANAGED CARE COPAYMENTS ________________________________________________________________________________ HMO SAME AS ABOVE PREMIUM LOW MANAGED CARE COPAYMENTS ________________________________________________________________________________ DENTAL PREVENTIVE PREMIUM UNLIMITED FEE-FOR-SERVICE DIAGNOSTIC DEDUCTIBLES PURCHASED RESTORATIVE COINSURANCE SEPARATELY EXTRACTIONS ________________________________________________________________________________ DENTAL (DHMO, DPPO) PREVENTIVE PREMIUM LOW - DHOM PURCHASED DIAGNOSTIC COPAYMENTS HIGH - DPPO SEPARATELY RESTORATIVE EXTRACTIONS
11 6325

**NOTE**
Comprehensive health insurance establishments can be organized as fee-for-service or managed care companies. However, the manner in which a company is organized does not limit the types of products it can provide. Many companies offer both fee-for-service and managed care products. Many of the larger companies offer all product types. It is important to note that PPO’s are generally the only managed care type whereby the insured pays deductibles and coinsurance for services received. There may be exceptions. Most PPO’s are offered by fee-for-service companies. Managed Care Medical Service Plans Unlike fee-for-service medical service plans, where the insured pays a premium, deductibles, and a percentage of the fees for services provided (coinsurance), managed care is generally a prepaid plan. The client pays a monthly or quarterly premium and small copayments when services are received. Managed care plans provide comprehensive health services to their members and offer financial incentives for patients who use plan providers. Office visits, hospital, surgical, emergency, maternity, mental health, substance abuse, dental, vision, and pharmaceutical benefits are all included in a comprehensive medical service plan. There are a variety of managed care plans that provide comprehensive medical coverage. The various managed care plans include health maintenance organizations (HMO’s), preferred provider organizations (PPO’s), point of service organizations (POS’s), and exclusive provider organizations (EPO’s). In both an HMO and an EPO, the client must receive care from plan providers. A plan member selects a primary care physician who coordinates the client’s care, including providing referrals to specialists and hospitals. PPO’s and POS organizations allow for reimbursement if care is provided from a provider outside of the plan network. When using a provider outside of the plan network, the level of reimbursement is lower than if a provider within the network is used. As for all insurance products, the choices available to the consumer with regard to health insurance are really part of a menu of options from which a consumer can choose the services, method of provision, and method of payment that most suits their needs. The health insurance product types differ in three aspects: degree of choice, premium amount, and method of payment as services are rendered. It is evident from the table on the previous page that the HMO product type offers the customer a low degree of choice. However, fees for services received are generally lower for managed care plans versus fee-for-service plans. In addition, the premiums paid for an HMO product are typically the lowest of all health insurance plans. The EPO is the PPO’s answer to the HMO. This product type offers a low degree of choice and a low premium. The POS product type offers slightly more choice for a slightly higher premium. Non-affiliated providers may be used, but the customer is generally reimbursed less for these services than if they use an affiliated provider. The PPO product type offers the most choice of any managed care product type. It is generally the most expensive as well. In general, fee-for-service plans offer the most choice for the highest premium price. In general, fees for surgery and check up’s are more expensive with this plan type than for any of the managed care product types.
12

In general, HMO’s are the least expensive and require the least out of pocket expense for most types of medical care. Of course, the premium amount will depend on the company and the plan selected. HMO’s are able to offer increased benefits at a lower cost by using utilization review to limit customer choice and the performance of unnecessary medical procedures. Patients choose a primary care physician from a list of approved physicians provided by the insurance company. This primary care physician acts as a “gatekeeper”. He or she decides which specialists will be seen, if at all. Physician decisions are then reviewed by the insurance company. In addition, specialists must be part of the HMO system, limiting choice even further. Should a customer use a non-affiliated provider or hospital, he or she must pay the entire cost. If an affiliated provider is used, the client generally pays a small copayment. This copayment generally ranges from $5 to $10 for office visits and pharmaceuticals, and $50 to $100 for surgery and emergency care. There are no deductibles for this type of plan nor coinsurance should affiliated providers be used. Major procedures, such as surgery, must be approved by the insurance company as well as the primary care physician. This extensive review procedure helps to contain costs. In most cases, premiums are less for HMO’s than all other health insurance product types, especially fee for service. Again, the total price of an HMO plan is dependent upon the company, and its ability to contain costs. In addition, premium amounts depend on the profit goals of a particular company. EPO’s are very similar to HMO’s. However, the premiums are generally slightly more expensive. This is because EPO’s are generally offered by PPO’s in order to compete with HMO products. Utilization review is not as extensive for this product type as it is for HMO’s. Should a customer use a non-affiliated provider or hospital, he or she must pay the entire cost. If an affiliated provider is used, the client generally pays a small co-payment. This copayment generally ranges from $5 to $10. EPO’s are the least popular managed care product type. POS plans offer still more choice for a slightly higher premium. Customers may use non-affiliated providers and generally pay slightly more than if they use an affiliated provider. Copayments are made for office visits and other medical procedures should an affiliated provider be used. Should a non-affiliated provider be used, coinsurance rates will apply. However, customers are generally not responsible to pay the full amount, as is the case with an HMO or EPO. The preferred provider organization is similar to an HMO in terms of structure. PPO’s are panels of physicians, hospitals, dentists, and other providers who negotiate with employers, insurance companies, or other organizations in order to provide services at reduced fees to members of a specified group. PPO’s may be group practices, individual providers, or facilities that offer a range of services or a limited set of services. Customers have the most choice and pay higher premiums than any other managed care product type if they are enrolled in a PPO. This type of product is a combination of a fee-for-service and a managed care product. Small deductibles must be met for some services before benefits are received. Once deductibles are met, the insurer pays a certain percentage and the customer pays a percentage (coinsurance). Coinsurance rates are generally less for a PPO than for a fee-for-service product. Customers may use non-affiliated providers at a similar cost, but are generally rewarded if they use affiliated providers.
13 6325
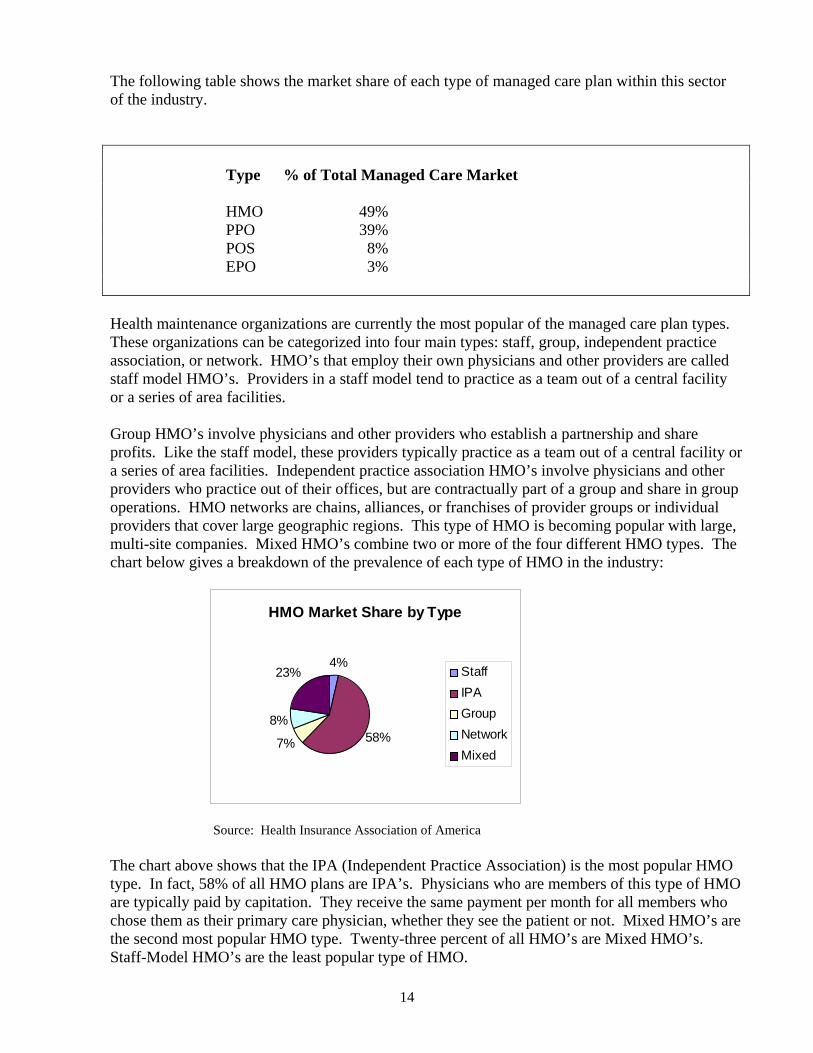
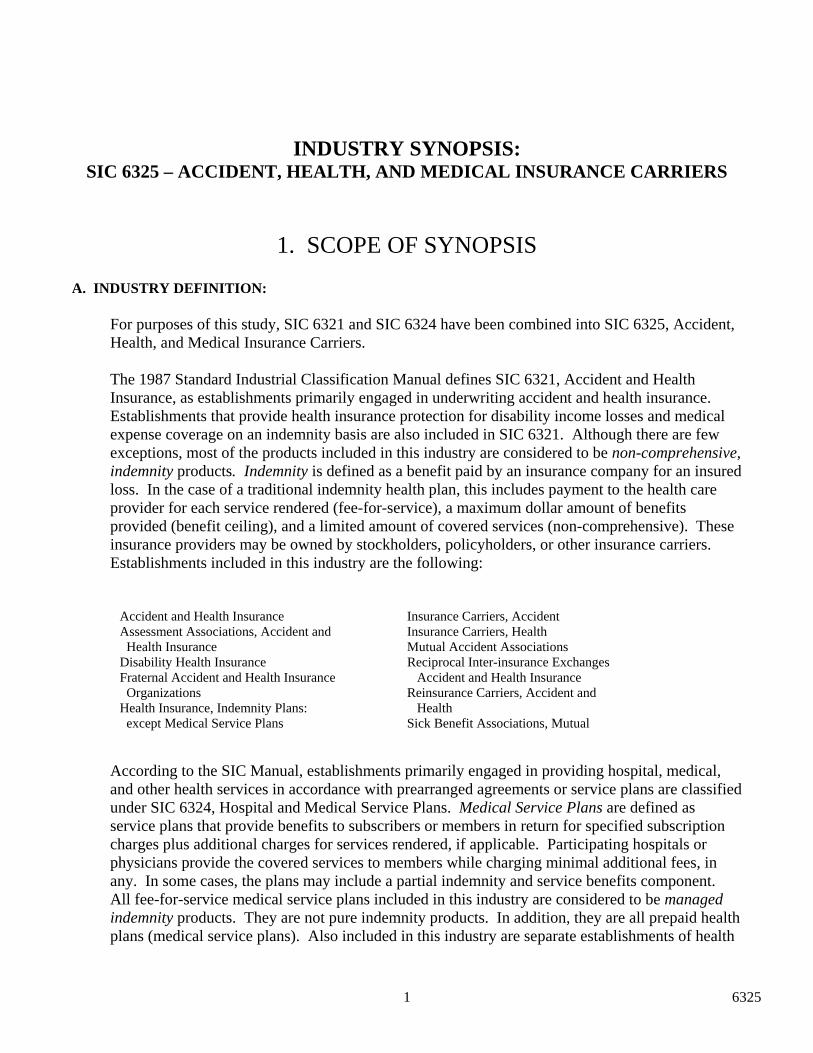
The following table shows the market share of each type of managed care plan within this sector of the industry. Type % of Total Managed Care Market HMO 49% PPO 39% POS 8% EPO 3% Health maintenance organizations are currently the most popular of the managed care plan types. These organizations can be categorized into four main types: staff, group, independent practice association, or network. HMO’s that employ their own physicians and other providers are called staff model HMO’s. Providers in a staff model tend to practice as a team out of a central facility or a series of area facilities. Group HMO’s involve physicians and other providers who establish a partnership and share profits. Like the staff model, these providers typically practice as a team out of a central facility or a series of area facilities. Independent practice association HMO’s involve physicians and other providers who practice out of their offices, but are contractually part of a group and share in group operations. HMO networks are chains, alliances, or franchises of provider groups or individual providers that cover large geographic regions. This type of HMO is becoming popular with large, multi-site companies. Mixed HMO’s combine two or more of the four different HMO types. The chart below gives a breakdown of the prevalence of each type of HMO in the industry:
HMO Market Share by Type
4%
58%7%
8%
23% StaffIPAGroupNetworkMixed
Source: Health Insurance Association of America
are t of all HMO’s are Mixed HMO’s.
taff-Model HMO’s are the least popular type of HMO.
The chart above shows that the IPA (Independent Practice Association) is the most popular HMO type. In fact, 58% of all HMO plans are IPA’s. Physicians who are members of this type of HMOare typically paid by capitation. They receive the same payment per month for all members who chose them as their primary care physician, whether they see the patient or not. Mixed HMO’sthe second most popular HMO type. Twenty-three percenS
14

HMO policies can be purchased through companies, unions, commercial insurers, Blue Cross anBlue Shield, associations, hospitals, medical centers, and other health organizations. Some are non-profit and others are for-profit. Like commercial insurers, most regulation is handled bystates, although applicable federal HMO laws and regulations exist. An example of federal legislation is the Health Maintenance Organ
d
the
ization Act of 1973. This act provides the minimum tandards for “federally qualified” HMO’s.
ee-for-Service Medical Service Plans
d coinsurance and some sort of utilization review takes place in order to ttempt to contain costs.
he
g r procedures which are not deemed medically necessary by the provider and the company.
ce
f
rse s”
review and the insurance company is not involved in the provision of health care
ervices.
ental Service Plans
ely
s F Fee-for-service plans offer unlimited choice, but higher deductibles and coinsurance than a PPO product. In addition, premiums for fee-for-service plans are generally the highest of any health insurance product type. Fee-for-service medical service plans can also be considered “managed indemnity plans”. Providers are reimbursed on a discounted fee-for-service basis, the insured pays a premium, deductibles ana A fee-for-service plan pays a medical provider a discounted fee for each service rendered. This serves to reduce the costs of the insurer. Insurers are able to pass some of these savings on to tconsumer based on contractual agreements between the insurance company and a provider or group of providers. Providers receive a guaranteed volume of business. Insurance companies receive lower costs and the ability to employ utilization review in order to determine whether a procedure is “medically necessary” or not. Fee-for-service insurers generally reimburse nothinfo Fee-for-service medical service plan products are also comprehensive health insurance plans. Under this type of plan, the client selects any medical service provider and the medical serviprovider submits a claim to the insurance company. In general, this type of policy does not reimburse one hundred percent of the claim. The level of reimbursement depends on the terms othe policy with regard to deductibles and coinsurance. Typically, the higher the deductible, the lower the premiums will be. These policies also have an annual, out-of -pocket maximum and a lifetime ceiling on benefits provided. Even though fee-for-service plans have a “lifetime” ceiling on benefits provided, they are not traditional indemnity plans. Indemnity plans do not reimbuthe service provider on a discounted fee-for-service base. They are “compensation for lospolicies meaning they pay the exact cost for services provided. These plans assign a low maximum dollar amount to benefits provided, are usually not comprehensive, do not employutilizations D Dental insurance can be purchased as part of a managed care or fee-for-service product, separatas a dental managed care product, or as a dental fee-for-service product. There are two dental managed care product types, the DHMO and the DPPO. The DHMO is very similar to an HMO and the DPPO is very similar to a PPO with regard to structure, method of payment, and provider reimbursement. Most of the revenue for dental insurance products sold separately is from the two managed care product types, approximately 90%. In addition, most dental insurance sold separately is group business, approximately 90%. Thus, experience rating is used based on groups
15 6325

of similar size, in a similar industry and a similar geographic region of the country. Only 10% ofdental insurance sold separately is purchased by individuals. Rating criteria for dental insurance sold separately is less detailed and stringent than rating criteria for health insurance plabenefits include check-up’s and x-ray’s (diagnostic), cleanings (preventative), fillings (restorative), extractions and anesthesia (oral surgery), gum treatment (periodontics), braces (orthodontics), crowns, dentures and bridges (prothodontics), and root canals (endodontics). The same dental benefits are usually offered when dental insurance is included with a fee-for-servior manag
ns. Typical
ce ed care, medical service plan product. However, the degree of benefits will vary of
ourse.
upplemental Medicare Medical Service Plans
.
private duty st
s
made ls the gaps”
ifferently. Medigap plans can be fee-for- service or managed care plans.
roduct.
entucky, Minnesota, Missouri, North Dakota, Ohio, Texas, Washington and Wisconsin.
**NOTE**
ed
government purchases coverage from a private surance company, this service is in scope.
benefits through enrollment in ne of an array of private health plans that contract with HCFA.
e
c S This type of policy is private insurance. Medicare was never designed to be an all-inclusive health care plan. Currently, Medicare has very high deductibles and does not cover many itemsMedicare does not cover skilled nursing facilities beyond one hundred days per benefit period, skilled nursing facilities not approved by Medicare, out of hospital prescription drugs,nursing, care received outside the United States, routine check-ups, dental care, moimmunizations, cosmetic surgery, routine foot care, eyeglasses, and hearing aids. Medigap. Since Medicare is so limited, 80% of seniors currently own Medigap policies. The Medicare Part B premium must be paid in order to purchase a Medigap policy. Medigap policiemust cover certain gaps in Medicare. In addition, Medigap insurance may cover certain things, which Medicare does not cover at all. There are 10 standard plans available, designated by the letters A through J. All ten plans may not be available in every state, but Plan A must beavailable to all Medicare recipients. Each plan covers different things or “fild Medicare Select. This is a Medigap insurance product that may be available in designated states through either HMOs or insurance companies. It is essentially a managed care, Medigap pThe states where these policies are currently authorized to be sold are Alabama, Arizona, California, Florida, Indiana, K
Medigap policies, including Medicare Select, are the only Medicare policies that are considerto be in-scope for this industry. All other types of Medicare policies are either completely orpartially subsidized by the federal government. Insurance coverage provided by the federal government is out-of-scope. However, if the in Medicare Plus Choice. This is a HCFA (Health Care Financing Administration) program through which eligible individuals may elect to receive Medicareo Traditional Medicare includes Medicare Parts A & B. In addition, seniors may purchase privatfee-for-service insurance, managed care coverage, or a Medicare medical savings account. In order for the Medicare beneficiary to be eligible to choose one of these alternative plan types, heor she must first be enrolled in Medicare Part’s A & B and pay the Medicare Part B premium..
16

The managed care company is paid a set monthly amount per member should the managed careoption be chosen. Seniors can choose between HMO, PPO, or POS coverage. In addition, the Medicare member may pay a premium to the managed care company. A Medicare memberchoose private fee-for-service insurance instead of the traditional Medicare Part A (fee-for-service) option. Under this arrangement, Medicare will pay the plan premium for Medicare covered services. The insurance company may charge the Medicare member a premium as wMedicare medical savings accounts (MSA’s) are functionally similar to traditional MSA’s. Medicare will pay the premium of a high-deductible, medical expense plan and deposit some money into a savings account. The Medicare beneficiary can use the money deposited into thiaccount to pay for routine medical expenses or deductibles. The medical expense policy will cover catastrophic illnesses or accidents. The tabl
may
ell.
s
e below clarifies which Medicare policies are ublic, private, fee-for-service, or managed care.
PUB C PRIVAT FEE-FOR RVICE MANAGED CARE PREMIUM
p
LI E -SEMEDICARE PART A X X N/A MEDICARE PART B $4 ) X X 5.50 (1999MEDICARECHOICE
PLUS X X X X VARIES
MEDIGAP X X X VARIES
Other Medical Service Plans
are,
may
n the
ally the only o characteristics needed in order for an insurer to provide a price for these policies.
.
ctually the insurer. If the employer is acting as the insurer, these services are out of scope.
. Prescription Drug Plan: Most health insurance plans, either fee-for-service or managed cprovide benefits for prescription drugs. Some stand-alone dental plans offer coverage for prescription drugs as well. However, the benefits these plans provide for prescription drugs be limited. Stand alone prescription drug plans are supplemental plans that usually provide benefits after a deductible is met. Once the deductible is met, a small copayment is required for each prescription. The copayment for brand name prescriptions is usually slightly higher thacopayment for generics. In addition, there is usually a maximum amount of yearly benefits provided. The age of the insured and number of people included in the policy are usutw Vision Expense Insurance: This type of policy provides reimbursement for routine eye examinations, eyeglass lenses, contact lenses, and the purchase and fitting of frames. Vision carepolicies are usually integrated into a major medical plan or are part of an employer, self-insured plan. Vision services included with a fee-for-service or managed care health insurance plan areusually very minimal. One eye exam and lenses may be covered. Frames are rarely coveredEmployers typically offer this as a benefit to their employees. In this case, the employer is a
17 6325

ACCIDENT AND HEALTH INSURANCE
Accident and health insurance policies include disability, long-term care, hospital indemnity, specified disease, and acciden
tal death and dismemberment. With the exception of disability surance and credit health, all accident and health products are indemnity products. In addition,
e and they have a lifetime ceiling on the dollar mount of benefits provided.
or those
ability insurance generally provides come replacement should an accident or illness cause the insured to be unable to work for a
ribes g n these two service
inthese insurance products are not comprehensiva Disability and Long-Term Care Insurance Disability and long-term care insurance products are similar in that they provide benefits in the case of an accident or illness, which leaves the insured disabled either temporarily or permanently. However, long-term care insurance provides nursing home or home health care coverage fwho are disabled and generally over age 65. Long-term care insurance generally provides benefits for supportive functions that provide assistance with daily activities in order to minimize, rehabilitate, or compensate for loss of functioning due to disability. In addition, disabled individuals do not always require long-term care services. Disinprolonged period of time. The table below desc eneral services included ilines, services they are likely to cover, and payment methods. PRODUCT SERVICES PROVIDED METHOD OF PAYMENT ____________________________________________________________________________ SHORT-TERM INCOME REPLACEMENT PREMIUM DISABILITY SIX MONTHS TO TWO YEARS __________________________________________ _ ____________________ ______ _______ LONG-TERM INCOME REPLACEMENT PREMIUM D FIVE YEARS UP TO IND N ISABILITY EFI ITELY___________________ _________ ______ ________________________ _ ________________LONG-TERM CARE NURSING HOME CARE PREMIUM RESIDENTIAL COMMUNITY CARE DEDUCTIBLES HOME HEALTH CARE COINSURANCE
s, until age 65, or
indefinitely. Benefits typically expire at age 65. Maternity insurance is not sold separately, but
rt-
t
Disability Insurance: This type of insurance provides partial income replacement in case the insured is unable to work as a result of an accident or illness. The insured receives benefits aslong as the accident or illness is not covered by workers’ compensation. Short-term disability insurance generally pays benefits up to twenty-six weeks, but can provide benefits as long as twoyears. Long-term disability insurance pays benefits for five years, ten year
may be included with the benefits of a long-term disability insurance product. The benefits are usually short-term unless complications arise as a result of the pregnancy.
There are five different types of disability income insurance that can be purchased as either shoterm or long-term coverage. These include general DI (disability income), DI-loss of earnings, DI-overhead expense, DI-buyout, and DI-key person. The first two have to do with the coverage for individuals. The last three have to do with coverage for businesses. DI-overhead expense provides benefits for all overhead expenses, including salaries of and benefits to all employees thaare not owners, should the principal owner of the business become disabled. DI-buyout provides
18

a lump-sum benefit should the insured become disabled. The insurance company agrees to buy the insured’s share of the business for a predetermined amount. DI-key person provides benefits
the owner of a company should a key person of the firm become disabled. Benefits are paid to
lude
benefit. Typically businesses can only purchase the additional purchase benefit. However, they may ometimes purchase a future increase benefit. The options available to businesses depend on the
cribes t
tothe business until a replacement in found. If a replacement is found during the benefit period, a replacement benefit will be paid to the owner of the company. Several riders or additional services can be purchased as part of a disability policy. These incadditional purchase benefit, waiver of premium benefit, rehabilitation benefit, deferred disability benefit, future increase benefit, indexed income benefit, and a social security substitute
scompany. The table below des he additional benefits available to individuals.
Additional Purchase Benefit . Additional coverage can be purchased as income increases Waiver of Premium Benefit If the disability lasts longer than a certain period of time,
the premium may be waived until the disability no longer exists.
Rehabilitation Benefit Rehabilitative therapy is included. Deferred Disability Benefit Provides retirement benefits. Future Increase Benefit The maximum benefit amount is increased to account for
inflation. Benefits are usually indexed to the CPI. Indexed Income Benefit After twelve months of disability, the benefit is indexed to
account for inflation. Social Security Substitute Increases the benefit at age 65 if benefits are not available from Social Security or a state plan. Long-Term Care: This type of insurance covers medical care, nursing care, and other assistanceon a fee-for-service basis in the event that the person insured is unable to care for themselvesan extended period of time. Services covered under this type of policy are not typically covered under other health insurance policies. Usually, these policies pay a fixed dollar amount for each day care is received. Many of these policies have an inflation adjustment feature in order to
for
rovide adequate coverage in the future. Thirty- percent of long-term care policies are owned by dividuals who belong to a group plan. Seventy-percent of long-term care policies are owned by dividuals. The table below describes possible services covered by long-term care policies.
pinin
19 6325

Nursing Home Daily maximum between $50 and $200 B Reserves a bed in a nursing home in the caseed Reservation of a temporary
hospitalization. Benefits up to the daily maximum amount are usually paid. In addition, benefits
are paid up to a maximum number of days. Alternate Facility Includes care given in an assisted living facility or Alzheimer’s care facility. Usually pays a percentage of the daily nursing home maximum. Home Health Care Includes care given at home or at Adult Day Care Centers. A percentage
of the daily nursing home maximum is usually paid. Respite care is also included. This gives the informal care-giver a break from providing care. Benefits are provided on a twenty four hour basis for a maximum number of days.
t
payment is made directly to the client who can use the money any ay they choose. The client must be hospitalized for a certain number of days before the policy
up .
it of a basic medical policy is low. This is a fee-for-service product. These policies ay include a maximum lifetime benefit of a high dollar amount. Supplemental medical expense
ccidental Death and Dismemberment Insurance: This form of health and accident insurance of
ccident Insurance: This is a type of insurance insures against a loss caused by accidental purchased in order to compensate the beneficiary
r a loss incurred as a result of work related travel.
e installment loan. This type of insurance can be purchased to cover a credit card loan, car loan,
Hospital Indemnity: This type of insurance policy provides a per diem cash benefit to the clienfor each day he/she is hospitalized. There is usually a maximum number of days for which benefits are provided. The cashwwill be paid. Hospital/surgical policies include surgery benefits, should surgery be performed during a hospital stay, as well. Major Medical Expense: Insurance that provides benefits for most types of medical expenses to a high maximum benefit. Such contracts are normally subject to deductibles and coinsuranceThis type of policy provides hospital and medical expenses above a certain deductible. This type of policy is selected as a safeguard to cover the costs of a catastrophic illness when the lifetime benefit limmpolicies may be purchased to supplement a hospital indemnity or MSA (medical savings account) product. Aprovides payment to an insured’s beneficiary in the event of death or the insured in the event specific bodily losses resulting from an accident. Abodily injury. This type of insurance is usually fo Other Accident and Health Insurance Plans Credit Health: This type of insurance will pay a particular installment loan for an individual should the individual be too sick or injured to work. The premium is paid monthly and added to th
20

or an installment home equity loan. Coverage only applies to the loan for which credit health insurance is owned. A separate policy for each loan must be owned in order for coverage to apply Medical Savings Account (MSA): This instrument was created by Congress in the summer of 1996. An MSA is an individual savings account, which is used to cover office visits and generalhealth care expenses. These accounts provide tax-free savings, tax-free payment of medical bills,and tax-free use of savings for any reason after the age of 65. Currently, this type of plan iavailable to the self-employed and small businesses with less than 50 employees. Congress has limited the number of MSA’s that can be sold through the year 2000 to 750,0
.
s only
00. In conjunction ith an MSA, one must also have a high deductible, fee-for-service, catastrophic medical surance product. The catastrophic medical policy will cover medical expenses above a certain
deductible. The savings port ible.
tain price per member in order to receive this service. Since this type of lan is really a contract to administer the claims process for a company or organization, it is
s a
, known as the remium equivalent, paid to the employer providing the policy influences the price for these
sold rance and medical service plans.
er ts
ith an insurance company to pay claims if claims in a given period should exceed 100% of the
a
m
e for should they exceed 90% of the expected claims. This
service is very similar to a Stop/Loss contract and is typically sold in conjunction with an ASO or many different types of accident and health
insurance and medical service plans.
win
ion of an MSA is used to cover the deduct
3RD PARTY ADMINISTRATIVE SERVICES Administrative Services Only Contracts (ASO): This is a contract whereby the insurance company agrees to administer the claims process for a self insured, employer health plan. The client agrees to pay a cerpneither a fee-for-service, nor a managed care product. ASO contracts account for $4.5 billion of total industry revenue. Insurers typically determine the price based on the total number of members in the group or apercentage of total average or anticipated claims. The insurer may also look at the average number of claims per member in order to provide a price. In addition, the premiumpcontracts. The price is usually quoted as a price per member per month. ASO contracts arefor virtually all types of accident and health insu Special procedures for collecting this type of service are presented in Types of Prices and Industry Specific Questions and Procedures. Stop/Loss Contracts: This type of insurance policy is for self-insured employers, (an employthat both administers and pays claims against large fluctuations in claims). An employer contracwexpected claims. Stop/Loss contracts are sold for many different types of accident and health insurance and medical service plans and are very often sold in conjunction with ASO contracts. Minimum Premium Plan (MPP): An arrangement under which an insurance carrier will, forfee, handle the administration of claims and insure against large claims for a self- insured group. Under this type of plan, the insurance company will receive a certain percentage of the premiuand pay claims should they reach a certain level, less than 100% of the expected claims. For example, an insurance company may agree to receive ten percent of the premium in exchangthe guarantee that they will pay claims
contract. Minimum premium plans are sold f
21 6325

C. PRICE DETERMINING CHARACTERISTICS
is typically set for policies purchased by companies located in several regions or ationwide. The guidelines for receiving a national rate can vary amongst insurance companies.
ies purchased by companies with fewer locations. This rate will be ased on the region, state, or city in which the policyholder is located.
f y
ilar groups in similar dustries. Basically, an average claims cost per individual is determined for similar groups and
tal number of individuals in the group. All other costs and desired profit argins are then added in order to determine the final rate for the group.
nderwriting small group olicies. Thus, the underwriter may use the claims experience of similar groups in the same
nce again, large group policies generally require minimal underwriting. The list below presents
mount of Coverage (Richness of Benefits): The number of covered services, the dollar amount of
ensus class: Prices for the same service within the same group will differ according to the rate or
he
whereby e employer pays 100% of the premium. The percentage contribution of the employer or the
All policies Rates for insurance policies are set on either national or regional (region, state, or city) basis. A national ratenThis rate is generally the same for all employees within the same rate (or census) class regardless of location. A regional rate is set for policb Large Group Policies: Large groups usually require minimal underwriting. Groups are typically considered to be large ithey have more than 300 members. However, the distinction between small and large will vary bcompany. In general, experience rating is used in order to determine a rate for these groups. These groups are rated based on the company’s claims experience with siminthen multiplied by the tom Small Group Policies: A combination of experience rating and individual rating is used in upindustry and consider the demographic and health characteristics of every individual in the group. These are the most difficult policies for which to determine a price. Oall possible price-determining characteristics used by underwriters when determining a price for either a large or small group policy: Type of Coverage: Underwriters will require different information in order to provide prices for medical service plans, disability, long-term care and other services. Acoverage for each service, and the maximum dollar amount of coverage will all influence the policy price. Ccensus class. Generally, families will pay a higher premium than an individual within the same group plan. Voluntary vs. Non-Voluntary (Contributory vs. Non-Contributory) For our purposes, voluntary(contributory) group policies will be defined as policies for which the employee pays 100% of tpremium. Non-voluntary (non-contributory) group policies will be defined as policies th
22

employee can vary anywhere between 0.0 and 100.0%. The total will always sum to 100.Utilization tends to increase as the percentage contribution of the employee increases.
0%.
roup composition: The combination of gender and age ranges is an important factor in
and children.
ccupation: People employed in dangerous occupations will generally pay more than those in
The zip code sually the first three digits) is used for underwriting purposes. For large groups, or small groups
arnings: As incomes rise, utilization rates tend to increase. Thus, premiums tend to increase as ice for disability
surance. Maximum benefits paid are usually based on income.
tus: Smokers generally pay higher premiums than non-smokers.
ype of Company: Premiums of mutual companies are generally less than those of stock
ividual policies is usually the most stringent. This may include health screening, in addition to analyzing the individual price determining characteristics listed above for
. Again, individual policies (non-group) represent approximately 10% of total industry revenue.
D. CU
payment is the primary
rm of customization in this industry. Clients can be given different payment options including ayment of the entire annual premium in advance as well as quarterly or monthly payments. An centive may be offered for payment of the annual premium in advance.
Gdetermining the premium. Therefore, companies require the age and gender of each person covered by the policy, including spouses Medical History: Previously healthy people will generally pay lower premiums than those who have a record of health care utilization. Osedentary, low risk occupations. The SIC code of the industry is usually used for underwritingpurposes. Geographic Location: People who live in areas in which natural disasters often occur and/or pollution is a problem will generally pay higher premiums than those who do not. (uwhich are geographically dispersed, several zip codes/geographic regions may apply. However, a national rate may be used if a group is very well dispersed throughout the nation. Eincome increases as well. Earnings will be most important in determining a prin Smoking Sta Tcompanies. Individual Policies: The number of rating structures and the complexity with which individuals are rated vary from company to company within the industry. Since the risk of underwriting one individual is so great, rating for ind
small group policies
STOM SERVICES
Among individual policies, products are generally standard industry wide. However, many grouppolicies can be tailored in order to satisfy customer needs. The method of fopin
23 6325

E. SEASONALITY
Health and medical insurance services are not seasonal. F. SE
The only foreseen need to substitute would be to replace an actual policy that is no longer in force or to replace
4. MARKET AND TRANSACTION INFORMATION A. IN
stry for either SIC 6324 or SIC 6321 is unknown. However, the
ercentage is likely quite small. Reinsurance will not be included with one of these two industries aptured in the collection of the SIC 6311 – Life Insurance or SIC 6331 –
Property and Casualty Insurance.
B. PR
crease in
lation, eneral inflation, an increase in AIDS related diseases, and the performance of unnecessary edical procedures have all contributed to the rapid rise in health care costs. Today, national
lth care expenditures represent nearly 14% of the nation’s Gross Domestic Product.
RVICE SUBSTITUTION
a policy that is no longer sold by the company.
TERPLANT AND INTRAINDUSTRY SALES
Reinsurance is the only known form of intraindustry sale in the accident and health insurance industry. Reinsurance is the practice whereby the original underwriter, known as the direct-writing or ceding company transfers either part or all of the liability of a policy to another underwriter(s). The company that assumes a portion of the risk is known as the reinsuring or assuming company. It is a contract made between insurers. The original insured has no right to make a claim against the ceding company in the case of a loss. The percentage of total indurevenue that reinsurance comprisespjust as it was not c
ICE BEHAVIOR
Prices in the industry increased substantially during the 1980’s. The rise of managed care companies during the late 1980’s and early 1990’s have contributed to the more stable inhealth care costs recently. Today, 110 million people belong to some form of managed care program. Currently, premium prices are increasing only slightly more than the general inflation rate. The table below shows the amount of per capita health care expenditures and their percentage change from the previous year. Technological improvements, an aging popugmhea YEAR PER CAPITA HEALTH % CHANGE CARE EXPENDITURES 1994 $ 3,510 5.3% 1993 $ 3,331 6.0% 1992 $ 3,144 8.3% 1991 $ 2,902 8.0% 1990 $ 2,688 11.0% Source: Health Insurance Association of America
24

PES OF PRICES C. TY
For all services, the item being priced is a medical service plan or accident and health insurance
tput. Since the premium for risk protection is considered to be set below market rates, the return earned for investing those premiums should be included in the price. Without the investment earnings, companies would not be able to cover
primary component of this price is the premium. his premium should be reported on a per person (or per family) basis for the selected policy.
he other price component is the earned rate on investments. The rate to be collected is the nt and health insurance
ervices.
lude any pass-through expenses, such as broker fees, paid by the elf-insured company purchasing the administrative services contract. These expenses are often
ong to the appropriate entity as part of the dministrative service provided.
ote: There is no earned rate component for this type of price. Self-insured companies are of their employees. Thus, the insurance company providing
e administrative services do not bear any risk.
remium equivalent. For third party administrative services plans, duplicate quotes will be aid to an employer who self-
insures its employees. While self-insurance is out of scope for PPI, it is in scope for CPI.
policy. As explained under Industry Specific Questions and Procedures, the policy will either be hypothetical or live.
For all services except the third party administrative services, the type of price is a combination of the premium and investment income. Investment income is included to represent the financial intermediation component of the industry ou
claims unless premiums were much higher.
TYPE OF PRICE FOR ALL SERVICES EXCEPT THIRD PARTY ADMINISTRATIVE SERVICES Premium plus earned rate on investments. TheT Enter the annual premium as the ITEM PRICE. Tannual rate that the sample unit earns on its investments related to accides Enter the earned rate on investments as an ADJUSTMENT TO PRICE. TYPE OF PRICE FOR THIRD PARTY ADMINISTRATIVE SERVICES (PPI only) Flat fee. Self-insured companies pay the insurance company a flat fee on either a monthly or annual basis. This fee should excsincluded in the contract fees, but are then passed ala Enter this fee as the ITEM PRICE for PPI quotes. Nresponsible for covering the claimsth TYPE OF PRICE FOR CPI QUOTES Pcreated for CPI. The premium equivalent represents the premium p
25 6325

Enter the premium equivalent as the ITEM PRICE for CPI quotes.
D. TY
be protected against the ossibility of a loss due to an accident or an illness. These policies can be purchased separately or
company or government sponsored employee group plan.
E. DI
lti-
s may be provided to the insured if the performance of the company
favorable. Dividends should be recorded in the adjustments to price section of the transaction ND.
F. AD
ade. It is only known that riders exist for isability, long-term care, accident, and accidental death and dismemberment insurance. These
ined in a previous section.
G. SIZ
e with high maximum dollar amounts for various covered ervices and low deductibles or copayments, will be more expensive than the same type of service
ims is limited. For groups of 100-150, the insurance company is paid a fixed amount er month. If claims experience is favorable, then dividends or rate credits are given at the end of
H. CO
ontract between the insurance company and the insured. The insurance ompany promises to pay a certain amount of expenses and/or income replacement in the advent
red,
must accompany the application in order for the policy to become effective on the
PES OF BUYERS Any individual, group, or corporation can purchase policies in order to pas part of a
SCOUNTS
The only known discounts for accident and health insurance and medical service plans are muproduct discounts. These discounts are given to clients that purchase more than one product from the company. Not all companies provide multi-product discounts. Dividends should also be excluded from the price of insurance. Since the policyholders of mutual companies actually ownpart of the company, dividendischecklist under DIVIDE
DITIONAL CHARGES
Additional charges may be applied should riders be purchased or if non-standard financial arrangements for the payment of premiums are mdriders have been def
E OF PURCHASE
As mentioned previously, the premium will increase as the richness of benefits increases. For example, the premium for a servicswith benefits that are less “rich”. For group insurance, pricing varies with the size of the group. For large groups (over 150), thereis a flexible funding arrangement. The employer pays claims, expenses, and profits. The amount paid in clapthe year.
NTRACTS
An insurance policy is a ccof an accident or illness. Creation of this contract begins with the filing of an application. In turn, the company issues a policy, the terms of which are determined by the application. The contract identifies the insuthe beneficiary, the type of policy, the amount of coverage, premiums, etc. The first premiumpayment
26

desired date. Also, delivery of the policy establishes the precise moment at which coverage
ong-term contracts are sometimes signed. However, most insurance companies renew contracts en increasing so much lately.
I. OT
The main priority of the federal overnment is to maintain the competitiveness of the industry. There is a long list of disclosure
ims reserve requirements. As a result, insurers ccumulate more reserves than they would if there were no minimum level. The amount of assets
the reserve requirements.
es are orted.
ifficulty. States also regulate the operation of an insurer by requiring the fair treatment of cludes regulation of policy forms, rates, conduct and settlement practices.
rities laws. Many of these ws revolve around acquisitions and mergers. At this time, there is legislation pending that could
78. This amendment requires employers to treat regnancy the same as any illness. This includes the payment of disability income and medical
g in all areas of employment, including mployee benefits, against individuals 40 or older. The law provides for a reduction in disability
oyment, transportation, public facilities, and lecommunications. This has been interpreted to include health insurance and other benefits that
begins. Leach year since medical expenses have be
HER VARIABLES AFFECTING PRICE
Federal and state governments regulate insurance premiums. gregulations that work to enhance industry competitiveness. The industry is regulated indirectly through claausually determines State Regulation: State regulations focus on the financial stability of the insurer. These regulations include reserve requirements, nature of permitted investments, and capital and surplus requirements. Reservrequired for unearned premiums, future payments on claims received, and claims not yet repStates oversee the licensing of insurance companies and agents, examination of companies, approval of policy forms, and liquidation of insurance companies in the advent of financial dpolicyholders. This in Federal Regulation: Health insurance companies are subject to federal antitrust and seculacreate direct regulation for the solvency of insurance companies. Title 7 of the Civil Rights Act of 1964 makes it unlawful for an employer to discriminate on the basis of race, color, religion, sex, or national origin. Thus, employees involved in an employer-sponsored health insurance program are guaranteed equal health care coverage under this act. Title 7 of the Civil Rights Act was amended in 19pexpense benefits under fringe benefits programs. The Age Discrimination in Employment Act (ADEA), which was enacted in 1967, prohibits employers with 20 or more employees from discriminatinebenefits, as long as the reduction is actuarially justified. The Americans with Disabilities Act (ADA), enacted in 1990, bans discrimination against disabled people in the areas of empltemay be provided by an employer.
27 6325

The Family and Medical Leave Act (FMLA), enacted in 1993, allows eligible employees to take up to 12 work weeks of unpaid leave in a twelve month period for several reasons. Acceptable reasons include birth, adoption, a serious health condition that prohibits the employee from doing
e essential functions of his or her job, and caring for a child, spouse, or parent with a serious
HMO movement in an ttempt to improve the health care delivery system in the United States. Amendments were made
he Profit margin is the esired return a company would like to realize as a reward for assuming risk. A contingency argin is a buffer in case of unexpected, adverse claims experience.
STRY INFORMATION AND RELATIONS
A. IND
th Plans (AAHP) et, NW, Suite 600
Washington, DC 20036-3421
inistration (HCFA) alth and Human Services
Baltimore, MD 21207-0519 atistics
ance Association of America (HIAA) st
(202)824-1600 ch
ssociation of Insurance Commissioners st
(202)624-7790 Contact: Marcia A. Marshall, Health Analyst
thhealth condition. The FMLA applies to companies with more than 50 employees. The Health Maintenance Organization Act of 1973 gave formal recognition to the HMO concept. It encouraged and exerted some control over the development of theato the HMO Act in 1988 in response to the changing marketplace. As always, desired profit levels will effect premium prices as well. Tdm
5. INDU
USTRY RELATIONS
American Association of Heal1129 20th Stre
202.778.3200 Health Care Financing Adm Department of He Attention: HCFA-1906-P P.O. Box 26676 Contacts: Maria Diacoganis and Helen Lazenby, st Health Insur 555 13th Street, Northwe Suite 600E Washington, DC 20004
Contacts: Tom Musco and William Wellar, Resear National A444 N. Capitol Street, NorthweSuite 701 Washington, DC 20001-1512
28
B. CU
However, this information is not very etailed. Both surveys have data for 1998 with regard to the average premium by plan type. This
hese companies do not produce an index or weighted time series data. In addition, the data
It is not known under which company name the survey will be produced in the future.
C. LI PROBLEMS
There is no known litigation at this time.
D. SE
olicy from
dard throughout the industry (i.e. a policy that is a group medical service plan HMO at one company would be
the same name at another company). E. CH
anaged care and fee-for-service medical service lans, represent comprehensive medical service plan products. These plans provide coverage for
s are sold separately and are not included as part of a omprehensive medical service plan. For code 004, indicate the type of supplemental Medicare
, which are pically sold separately. Tandem plans are not limited to the combination of dental and vision
odes 009-017 represent the primary types of accident and health insurance policies. For olicy.
RRENTLY AVAILABLE PRICE DATA
KPMG and Mercer, both consulting firms, currently provide premium price information for medical service plans and accident and health insurance. dinformation is further divided into geographic regions. Tcollected is not based on a constant service specification.
TIGATION AND OTHER COOPERATIVE
RVICE IDENTIFICATION
The distinctions between the different medical service plans and accident and health insurance products seem to be clear enough as to not cause any identification problems. Each type of phas some characteristic (purpose, method of payment, set of benefits, etc.) that sets it apart the others. Also, policy terminology and certain characteristics are stan
considered the same policy with
ECKLIST CLARIFICATIONS Type of service (group 01) – Codes 001 – 002, mpmany services. Codes 003 – 006, dental, supplemental Medicare, vision, and prescription drug plans, represent “stand-alone” policies. These plancplan selected (i.e. Medigap, etc.). Code 007, tandem plans, refers to plans that include multiple types of insurance included in a single plan. For example, many tandem plans include benefits for dental and visiontyinsurance. Enter the types of coverage provided by the tandem plan for code 007. Cspecified disease policies, indicate the disease covered by the selected p Codes 018-021 represent the third party administrative services plans.
29 6325

Service identification (group 02) – For code 001, enter the number and name of the selected policy. Many companies will name the policies to distinguish the different variations of policies offered by the company. If the company uses enrollment codes, enter the code for the selected
or anniversary date (code 003), enter the date on which the policy is renewed each year. This
If the selected policy is provided by a company that is a member of a cluster, identify that
d only
ty. These policyholders are charged a regional rate based on the cations of its various facilities. Code these policies as “regional” policies, code 002. See
omments. For sample units in strata MO that earn revenue in multiple states, this will be the
5, codes 001-005) – Insurance companies generally have up to four rating ers (i.e. single, family, etc.) for the policies they sell. Indicate the appropriate number of tiers for
ry for rate determination, disaggregate to a specific census class to represent the entire policy. Please
ge at issue (group 07, code 003) - For the chosen policy, enter the policyholder’s age at the time
4-007) – This refers to the general level of health of the dividual insured. If the sample unit uses terminology for health rating other than that provided,
icyholder does not currently smoke, but as in the past,this is to be captured for “other” (code 010). For example, if the policyholder has
roup size (group 09, code 001) – Enter the total number of person covered by the selected
policy for code 002.
Fwill determine the repricing schedule for the given quote.
company in code 004.
Policy scope (group 03) - Should a policy be written for a group that has facilities in several regions, or throughout the nation, a national rate may apply to the policy. The guidelines for receiving a national rate will vary between companies. Some companies may offer a national rate should the client (group) have facilities in three or more regions. These policies should be codeas “national” policies, code 001. Other policyholders may have facilities in fewer regions orin a single city, state, or localiloindustry specific procedures. In addition, the state in which the policy is sampled should be entered in the space provided for code selected. For sample units in strata B and AH, this will be the state provided in SUcstate selected through disaggregation (see Industry Specific Questions and Procedures. Rating tiers (group 0tithe selected policy. Census class (group 06, codes 001-006) – Although a description of the entire group is necessa
note that “census class” is an insurance industry term used to describe various rate categories.
Athe policy was issued. Health rating (group 07, codes 00inenter the this rating for code 007. Smoking status (group 07, codes 008-010)) - If the polhnot smoked for 10 years, enter “10 years no tobacco.” Salary (group 08, code 003) – Enter the salary of the individual insured. Gpolicy. This would include employees, spouses, and children.
30

SIC code (groups 09, code 003) – Enter the SIC code of the company insured by the selected
ip code/location (group 09, code 004) – Enter the zip code or area in which the insured group is
rganizational structure (group 09, code 005) – Indicate whether the company covered by the
xperience rating (group 09, codes 006-007) – Enter the dollar value of claims and number of
articipation rate (group 09, 008) – Indicate the percentage of employees who are covered by the
aximum benefit (group 13, codes 001-002) – Enter the maximum dollar amount of benefits
ut-of-pocket maximum (group 13, code 003) – Enter the annual out-of-pocket maximum dollar
enefit period (group 13, code 004) – Enter the maximum length of time that benefits will be
first ce companies and
ployee pays 100% of the total premium, the policy is 100% voluntary. Should a percentage f the total premium be paid by both the employer and employees, enter the percentages for code
oup 19) – The monthly benefit for disability and accident policies can be xpressed as either a percentage of the policyholder’s monthly salary (code 001) or as a flat dollar
ty to
ccupation* (group 21) – For disability and accident insurance, the price may vary by
(group 22) - For disability and accident insurance, the price may vary by salary. Should is be the case, disaggregation will need to be performed to this level. Enter the selected salary
policy.
Zlocated. If the policy is nationwide, enter as such. Oselected policy is a corporation, partnership, or has some other type of organizational structure. Egroup members for the previous year. Pselected policy. Mprovided. Please obtain the annual, lifetime, and out-of-pocket maximum. Oamount for the individual or the group. Bprovided. Policy duration (group 13, code 005) - This refers to the nth year of the insurance policy (i.e., year, fifth year, etc.). Policy duration is sometimes called “policy year.” Insuraninsured groups do not want to lock in to a price if conditions may change drastically in future years allowing for flexible premiums. Thus, the duration is to remain constant.. Contribution (group 13, codes 006-008) – This refers to the percentage of the total premium paidby the employers versus the percentage paid by the employee. These percentages will always sum to 100%. If the employer pays 100% of the total premium, the policy is 100% non-voluntary. If the emo008. Monthly benefit (greamount (code 002). Typically, the policyholder must wait a certain period of time after the onset of a disabilireceive benefits. Enter this waiting period for code 003. Ooccupation. Should this be the case, disaggregation will need to be performed to this level. Salary*thlevel.
31 6325

*Note that groups 21 and 22 should only be completed if a group disability or accident policy is selected and occupation and/or salary are price determining.
Contract description (group 28) – All entries made for this group should refer to the self-inspolicy for which the selected contract is written. F
ured
or code 001, enter the number of persons overed by the policy. For code 002, enter the number of enrollment codes offered. For code
or premium equivalent (code 005), enter the total employer and employee premium contribution ice for
is contract. In addition, this is the item price to be reported for the duplicate CPI quotes.
or codes 006-011, enter the type of coverage provided by the self-insured policy.
inancial payment arrangements (group 29) - If any non-standard payment arrangement
uld correspond to the breakdowns used by the ample unit. Companies typically use a 5-year age range. If the sample unit does not categorize
class is to be riced, it is necessary to describe the entire group.
of the box.
c003, indicate the number of sites at which the self–insured company operates. The expected number of claims should be entered for code 004. Ffor the self-insured policy. The sample unit will need this value in order to determine the prth F For code 012, indicate the company for which the contract is written. Fapplies, enter the name of the payment option and describe the terms of the special arrangement in the space provided. Group composition (group 31) – Enter the number of group members for each sex and age range under each applicable rating tier. The age range shosgroup members by age range, use the fallback of 5 years. Although only one censusp Enter the effective date of the census in the line provided at the bottom Age Rang Tier 1: Sel Tier Self +e f 2: Spouse Ma Fem e Mal Female al e le 15-20 2 3 0 0 21-25 3 2 2 0 26-30 4 4 4 2 31-35 10 6 8 6 36-40 4 7 2 4 41-45 8 9 4 2 46-50 6 5 2 4 Policy benefits (group 32) – Enter all deductibles, copayments, and coinsurance that apply feach category of service that may be covered by the selected policy. If the se
or lected policy is
ental only, vision only, or pharmacy only, complete only those sections which are applicable to dthe coverage offered. To enter the copayment or coinsurance amounts, indicate both the in-network and out-of-network amounts. For example: 20%/30% or $20/$40.
32

It is possible for companies to have different benefit schedules depending on census class. If this oinsurance amounts for the selected
nsus class.
F. IND
the following components:
dends paid ? __________________
nts to be used in r the sample unit. Further instructions for calculating the VOS are provided
. a. What is the value of all premium equivalents for this sample unit?
ever, the value of the fees paid for third party administrative services plans cally included in the premium equivalent is needed for VOS calculations.
pany’s premium revenue is derived from national policies versus gional policies?
Regional policies: ____%
rance other than health surance. All other lines of insurance are out of scope. These other insurance lines were given a
hance of selection in their appropriate industry. Only the health insurance portion of the sampled companies is to be collected. Unless otherw the synopsis, normal DCM sample unit
entification procedures apply to initiating sample units in this industry.
**NOTE**
being shared with the CPI program. Therefore, coverage of all states is quired.
is the case, only provide the deductible, copayment and cce
USTRY SPECIFIC QUESTIONS AND PROCEDURES
INDUSTRY SPECIFIC QUESTIONS
1. For this sample unit, what is the value of receipts for Insurance premiums? __________________ Investment income? __________________ Divi The purpose of this question is to help you obtain the necessary componecalculating the VOS fobelow. 2 _____________ b. Of this total, what percentage is the actual fees paid to this sample unit? _____________ The value of premium equivalents will be excluded from VOS, but it is necessary to provide this value to CPI. Howtypi 3. What percentage of your comre
National policies: ____%
PROCEDURES FOR ALL SERVICES Be aware that the sampled insurance companies may also carry lines of insuinc
ise noted in id
Data for this industry isre
33 6325

Facesheet procedures 1) The measure of size indicated on the facesheet is premiums rather than employment. For
collection system.
sary to
m) ill be used by CPI. Follow the normal DCM procedures for coding the status of the PPI quote
ed quotes items for disaggregation purposes.
al DCM procedures for updating the number of items collected.
ercent field should be left blank for all items in all cases.
chief actuary. The chief actuary should be miliar with the pricing for all services offered by the company. Actuaries are responsible for
setting insurance premiums and thus, will be the most familiar with pricing. The contact provided may or may not be the chief actuary.
equivalents” for SO contracts, stop/loss contracts, and minimum premium plans should also be excluded. Please
oss, included in the VOS.
stratum B, a dummy value of 999 will appear. Leave “RU premiums” blank on the SU information screen in the 2) There are no counties provided on the facesheet or cluster form. Therefore, it is unnecesobtain this information. 3) No VOS per employee edit range is provided for this industry. Therefore, the VOS per employee calculation is not required. 4) If the sample unit no longer carries health insurance, code it as out of business – 34. If the sample unit never provided health insurance services, code it as out of scope - 43. 5) For ASO contracts, stop/loss contracts, and minimum premium plans, create a duplicate item for each policy selected. The original item will be used by PPI while the duplicate quote (itew(item). Code the CPI item as “other” (4). Please note that the CPI items for any of these servicesare not to be included in the number of assign Update the number of items to reflect the additional CPI item. Follow norm
6) The relative p
Contact person The most appropriate contact for obtaining data is the fa
on the facesheet
Entering VOS 1) The VOS is to be calculated as the sum of direct premiums written for health insurance and investment income less dividends paid plus revenue derived from other receipts. Insurance premiums should not include life insurance or reinsurance premiums. “PremiumAnote that these premium equivalents include the fees paid to the sample unit for ASO, stop/land minimum premium contracts. These fees are to be Commissions should not be excluded from the VOS as they are considered a cost of doing business and are typically embedded in the premium.
34

A tool which may be useful in obtaining the VOS components is the insurance company’s annual statement. All life insurance companies are required by law to prepare these statements. “Analysis
f Operations by Lines of Business” found on page 6 of this statement includes all of the VOS
n line 28. An example of this exhibit is attached as an appendix.
S component are
siderations,” page 8. (b) Investment income: “Exhibit 2 - Net Investment Income,” page 10. (c) Dividends paid: “Exhibit 7 - Dividends and Coupons to Policyholders,” page 12.
stratum AH, the VOS should only include the revenue for the state indicated on the cesheet. For example, if Tennessee appears on the facesheet as Premiums State, the VOS
tates.
or the other strata, the VOS should not be limited to the state in which the sample unit is located.
) Once the ISDWS has been completed, disaggregate between national and regional policies for
gregate by the states in hich the sampled establishment earns revenue. All services provided at the sampled location are
e eet to determine the sample unit.
by
3) Once the type of service and scope of policy (national vs. regional) have been selected , ld
) Next, after pulling the policy, select the census class which will represent the entire policy
rice vary for different occupations or salary levels within the same census class. Should this be
ocomponents. Health insurance premiums are given on line 1, net investment income on line 4, anddividends paid o Other exhibits which provide more detailed information for each individual VOlisted below: (a) Health insurance premiums: “Exhibit 1, Part 1- Premiums and Annuity Con
2) For fashould only include revenue generated in Tennessee even if the company earns revenue in other s F Disaggregation procedures 1each ISDWS category selected. For each product line, list these percentages in the comments section of the ISDWS. This information is required by CPI to weight all items. 2) For sample units in strata B and MO, the next step should be to disagweligible for selection. Again, if more than one company is located at the sampled address, use thAMB number provided on the facesh List these percentages in the comments section of the ISDWS. This information is required CPI to weight items in stratum MO.
disaggregate between group and individual policies. At this point, the policy to be priced shoube pulled.
4(group and individual policies). It is the per member premium for the selected census class which will be repriced. 5) Group disability and accident insurance policies may require further disaggregation should thep
35 6325

the case, disaggregate to an occupation in group 21 or salary level in group 22. It is the per ium for this salary or occupation for the selected census class that will be repriced.
) It is possible for companies to offer multiple option policies. Group members can choose d
r only to the
lan options. For example, if the group members are able to purchase dental and
ed.
, two items will be ollected for each selected contract or plan. The PPI will use the original item for collecting the
er-
e fees for the employer-ponsored plan. At repricing, the actuary will need the total number of group members, the type of
m.
culate the administrative fees.
n
I.
a medical savings account be selected, the price to be collected is the net interest come earned on the selected account. This is calculated as the difference between the interest
t credited to the account holder. It will be necessary to btain the value of the account, current interest rate earned on investments and current rate
credited.
Price = [account value ($)] [earned rate(%)-credited rate(%)]
member prem Collection procedures
All Services 1between managed care and fee-for-service plans. Each option is priced independently and shoulbe treated as separate policies for collection purposes. Group descriptions should refegroup covered by the selected option. 2) If the type of service selected is a tandem policy, be sure to describe all relevant pvision under a single plan, it is necessary to complete the box for dental as well as other applicable checklist sections for both types of insurance. These policies are to be coded as “tandem policies” for type of service (code 007). Indicate the types of coverage in space provid 3) For ASO contracts, stop/loss contracts, and minimum premium planscfees for servicing the actual contract and the CPI will use the additional item for the employsponsored plan that applies to the contract collected. Therefore, only one set of data needs to be collected for the selected contract. For PPI, the item price is the fees. For CPI, the item price is the total premium equivalent including thsplan, and the company name in order to compute the new premium equivalent for the CPI iteBy law, the premium contribution has to be the same for every employee. The premium equivalent is usually required to cal
To record the information for the CPI item, use the copy & paste functions of the collectiosystem to copy all data from the ASO, stop/loss, or minimum premium contract items to the premium equivalent item for CP
When numbering items, the duplicate CPI items should receive the highest numbers. For example, if 8 items are assigned and 2 of these items are ASO contracts, the duplicate items should be numbered 9 and 10. 4) Should inearned by the sample unit and the intereso
The price should calculated as follows:
36

Please show the calculation in comments. Keep in mind that these accounts are not widely
omplete Group Composition (group 31) for this purpose. For each rating tier used for the should
ears. Although only one census class is to be priced, it is necessary to describe the entire group.
e collected. Collect a printout of the census that orresponds to the most recent anniversary date of the policy. This will essentially be a frozen
or these plans, it may be necessary to identify the characteristics of the underlying policy for is purchased. If this is the case, describe the underlying policy using the
appropriate checklist groupings. For example, if a contract is purchased for administering the on to
ompanies’ divisions for these services were given their proper chance of selection in the
m be collected. Therefore, convert any monthly premiums to an annual premium.
e price for le that
, record it as ero.
vestments specifically related to services included in this industry. Many companies will
o record the rate, enter the annualized rate for EARNED RATE ON INVESTMENTS. For
offered.
Group Policies Although it is a census class that will be repriced, it is necessary to describe the entire group. Cselected policy, enter the number of males and females for each age range. The age rangecorrespond to the breakdowns used by the sample unit. Companies typically use a 5-year age range. If the sample unit does not categorize group members by age range, use the fallback of 5 y Ideally, a printout of the census should bc“snapshot” of the group on which repricing can be based. Third Party Administrative Services Fwhich the contract
claims of self-insured dental plan, it may be necessary to complete groups 11 and 12 in additiany other checklist groups necessary to describe the underlying dental policy. Other procedures
1) For “other receipts,” exclude all other types of insurance provided (i.e. life, property andcasualty, etc.) as well as all real estate services and other financial services. The insurancecappropriate industry. 2) For all services except third party administrative services, it is preferred that an annual premiu 3) It is imperative that the earned rate on investments be collected as a component of thboth accident and health insurance policies and medical service plans. However, it is possibthe rate of return for a particular line of insurance could be zero. If that is the casez The rate to be collected is that which the insurance company is currently earning on its incalculate an annualized rate each quarter. Collect the most recent rate available. Tterms, enter the type of rate (i.e., average portfolio, etc.). Order applied should be 01.
37 6325

If the earned rate is negative, enter it as a discount in the collection system even though the checklist provides surcharge as the only option. NOTE: Fees earned from ASO, stop/loss, and minimum premium plans should be excluded from
are paid to the policyholder, enter the dividend amount for DIVIDEND. If the dividend is a percentage, order applied should be 01. If it is a dollar amount, order applied should
collection will be handled on a case by case asis. Please notify the Washington Office (through PPIQUES) if any mergers or acquisitions are
repricing period.
. The respondents would have to provide a per member cost change whenever there a considerable change in group size, benefit levels, etc.
) Respondents will be asked to reprice each item only once a year. The repricing month should
wing the respondent to have a steadier flow
r repricing.
ce industry. Once data is collected by
I, CPI will receive the following data components:
) Premiums for medical service plans and accident and health policies
Sending documentation to Washington Office The docum the checklist is the summary of policy benefits (for all policies) an composition (for group policies only, if available). Enter the SU ID and these documents. Please forward to:
the calculation of the earned rate. 4) If dividends
be 02.
5) Any mergers or acquisitions that occur duringbencountered.
Repricing procedures
1) Respondents have two options for repricing: (a) The first option is to select an actual policy or a hypothetical that is representative and keep all policy and policyholder characteristics constant over time. The respondent will be asked to provide the premium for the same hypothetical policy each
(b) The second option is to reprice a live policy. The respondent will be asked to provide the current premium charged for the selected policy upon renegotiation of the contract. However, this method of repricing is only desirable if, and only if, the respondent can provide quality adjustment data as neededis
2coincide with the anniversary date of the policy. Therefore, at initiation, attempt to select policieswith varying anniversary dates throughout the year allofo CPI Data Sharing
CPI will also be calculating an index for the health insuranPP ab) Premium equivalents for duplicate items collected for third party administrative services
The CPI will not use prices collected for “other receipts”.
entation required in addition tod a printout of the groupitem numbers on each of
38
Industry Analyst for SIC 6325 Bureau of Labor Statistics
PSB Bldg Room 3840 Washington DC 20212
FAX: (202) 691-7019
se your standard regional office procedures for mailing.
G. Q
It is anticipated that quality adjustment will be less frequent when pricing hypothetical policies. or this particular pricing method, quality adjustment will not be required for changes in the total umber of group members or the demographic characteristics of new/deleted members because the haracteristics of the original group will be held constant. Listed below are the anticipated hanges that will be considered a quality change. Cost changes associated with each of these risk hanges can be provided by insurance companies.
Quality Change ) Plan/benefit changes Changes in covered benefits due to regulation or a
Example: Company may not offer a particular benefit any longer or they may require that all future policies include a
cipated chang
) Plan /benefit changes Changes in benefit maximums, deductibles, copayments or coinsurance as determined by insuring company . These are adjusted periodically for inflation (self-escalating).
2 Massachusetts Avenue NE
U
UALITY ADJUSTMENT
Option 1: Pricing Hypothetical Policies
Fnccc
Type of change
1particular health insurance company’s policy
particular benefit not covered previously 2) Utilization Changes Extreme, long-term, changes such as epidemics (AIDS) or
medical advance in treatments
Listed below are the anti es that will be considered a price change. 1
2) Utilization changes Short-term changes such as a severe flu season
39 6325

Option 2: Pricing Live Policies
is anticipated that quality adjustment will only be necessary when contracts are renegotiated at time that
nticipated changes that will be considered a quality change. Cost changes associated with each of these risk changes can be provided by
uality Change Type of Change
) Number of members Major increase or decrease from the prior year
Example: Membership changes from1000 to 5000
2) Demographic changes Example: Avg. age changes from 40 to 60
b) Change in geographic location of insured company
hicago relocates to Omaha
nt
3) Plan/benefit changes
c) Deductibles, copayments or coinsurance as negotiated
) Utilization changes Extreme, long-term, changes such as epidemics (AIDS) or
5) Industry classification Change to different NAICS code for insured company –
any changes from SIC 6211 to NAIC 523120
Itonce a year. It is only at th premiums will change for a policy. Listed below are the a
insurance companies. Q 1
a) Major change in average age
Example: Insured company in C
c) Major changes in census distribution
Example: Percentage of single members increases from 30 to 70 perce
a) Changes in covered services (regulatory, company mandated, or choice of insured group)
b) Benefit maximums as negotiated between insurance company and insured group
between insurance company and insured group
4medical advances in treatments
split or combined
Example: Insured comp
40

Listed below are the anticipated chang
1) Number of members
2) Demographic changes
Example: One of GM’s plants is relocated to another state
3) Plan /benefit changes Changes in benefit maximums, deductibles, copayments or coinsurance as determined by insuring company . These are adjusted periodically for inflation (self-escalating).
4) Utilization rates Short-term changes such as a severe flu season
es that will be considered a price change. Price change Type of Change
Minor increases or decreases from prior year
Example: Membership changes from 140 to 150
Change in geographic location for insured company
41 6325

DEFINITIONS Accident Insurance: A type of insurance that insures against loss by accidental bodily injury.
y in the event of death or the insured in the event of specific odily losses resulting from an accident.
o process only for a self insured, employer health plan. ASO contracts can be
urchased for many different types of insurance.
who are of poorer-than-average health to apply for health surance coverage.
: A method of selling insurance that uses persons under contract to an insurance ompany to act as agents for that company.
llocated Benefits: Benefits for which the maximum amount payable for specific services is itemized
ssurance: A term synonymous to insurance.
designated by a policyholder to receive insurance policy proceeds. sed in life, accident, and disability insurance.
by the insurer to a claimant, asignee, or beneficiary when the insured ffers a loss covered by the policy.
ding protection against the costs of hospital care a limited geographic area.
rporation providing protection against the costs of surgery and ther items of medical care in a limited georaphic area.
er
osts of a atastrophic illness when the lifetime benefit limit of either a basic or major medical policy is low.
t may include serves for future claims fluctuations. Some reserves may be required by state law.
Accidental Death and Dismemberment Insurance: A form of health and accident insurance that provides payment to an insured’s beneficiarb Actuary: An accredited insurance mathematician who calculates premium rates, dividends, reserves, and prepares statistical studies and reports. Administrative Services Only Contracts (ASO): A contract whereby an insurance company agrees tadminister the claimsp Adverse Selection: The tendency for those in Agency Systemc Ain the contract. A Beneficiary: The person or persons U Benefit: The amount payablesu Blue Cross: A nonprofit membership corporation proviin Blue Shield: A nonprofit membership coo Capitation: A reimbursement method by which doctors receive the same amount per member pmonth regardless if care is given or not. Catastrophic Medical Policy: (6321) This type of policy provides hospital and medical expenses above a certain deductible. This type of policy is selected as a safeguard to cover the cc Claim Reserves: Funds retained by an insurer to settle incurred but unpaid claims thare
42

Coinsurance: The arrangement by which the insurer and the insured share a percentage of covered losses after the deductible. This translates into out-of-pocket expenses to the insured. Comprehensive Medical (Major Medical): This type of plan covers an array of medical, surgical, ahospital expenses. Some plans also pr
nd ovide coverage for prescriptions, dental, and vision care.
omprehensive medical plans are available through the traditional fee-for-service, indemnity insurance
ontributory Plan: An insurance plan in which the employee shares the cost of insurance with the
redibility: The weight assigned to a group’s past claim experience in order to determine future
n do
isability Insurance: This type of insurance provides partial income replacement in case the insured
on. Short-term disability insurance generally ays benefits up to twenty-six weeks, but can provide benefits as long as two years. Long-term
ligibility: The provisions of a group policy that state the requirements that members of the group
xclusive Provider Organization (EPO): Form of managed care in which participants are reimbursed
ts.
ed premiums.
sit or
irst Dollar Coverage: A hospital or surgical policy with no deductibles.
raternal Insurance: A cooperative type of insurance provided by social organizations for their e
illness of one of its members.
Gross Premium: The contracted premium before applying any discounts.
C(maximum level of benefits) or through a managed care program. Cemployer (the employee contributes). Cexpected claims premiums for the group. Deductible: The amount of covered expenses that must be incurred and paid by the insured before benefits become payable to the insured. Dental Expense Insurance: This type of policy provides reimbursement for expenses related to dental services and supplies. Dental policies place greater emphasis on preventive care and education thamost major medical policies. These policies can either be free standing (not supplemented with other forms of coverage) or integrated into major medical coverage. Dis unable to work as a result of an accident or illness. The insured receives benefits as long as the accident or illness is not covered by workers’ compensatipdisability insurance pays benefits for five years, ten years, until age 65, or indefinitely. Eand/or their dependants must satisfy to become insured. Efor care received only from affiliated providers. The PPO version of an HMO. Expense Loading: That portion of a group insurance premium required to cover acquisition and administrative cos Expense Ratio: A percentage showing the relationship of expenses to earn Fee-For-Service: A method of charging whereby a physician or other practitioner bills for each viservice rendered. F Fmembers. The social group may pay premiums into a fund and withdraw monies to pay claims upon thdeath or
43 6325
Group Insurance: An arrangement for insuring a number of people under a single, master insurance policy. Health Maintenance Organization (HMO): An organization that provides for a wide range of comprehensive health care services for a specified group at a fixed periodic prepayment. When sare rendered, small copayments are usually required. Hospital Indemnity: (6321) This type of insurance policy provides a per diem c
ervices
ash benefit to the client r each day he/she is hospitalized. There is a maximum number of days for which benefits are
hoose. client
ed for a certain number of days before the policy will be paid.
ically not involved in the service elivery process.
e of insurance is sometimes called personal insurance.
fee-for-service basis. It is one model of an MO.
Force: The total volume of insurance on the lives of covered employees at any given time (measured
surer: The party, usually a company, that promises to pay benefits should a claim be made.
: The number of insured who discontinue payment divided by the total number of policies force.
throughout the life of e policy.
covered under other health insurance policies.
sually, these policies pay a fixed dollar amount for each day care is received. Many of these policies he future. Thirty- percent
f long-term care policies are owned by individuals who belong to a group plan. Seventy-percent of
foprovided. The cash payment is made directly to the client who can use the money any way they cSome policies may have a pre-existing condition clause and/or contain an elimination period. Themust be hospitaliz Indemnity: A benefit paid by an insurance company for an insured loss. Indemnity plans pay a maximum amount for services rendered. Also, the insurer is typd Individual Insurance: Policies that provide protection to the policyholder and/or his or her family. This typ Individual Practice Association (IPA): An association of individual physicians that provide services on a negotiated per capita rate, flat retainer fee, or negotiatedH Inin terms of cases, lives, amount of insurance, or premium). Insured: The person or persons who are covered and may receive benefits form an insurance policy. In Lapse Ratein Level Premium: A rating structure in which the premium level remains the same th Loading Factor: The amount added to the net premium rate determined for a group insurance plan in order to cover the possibility that losses will be greater than statistically expected. Long-Term Care: This type of insurance covers medical care, nursing care, and other assistance in the event that the person insured is unable to care for themselves for an extended period of time. Servicescovered under this type of policy are not typically Uhave an inflation adjustment feature in order to provide adequate coverage in tolong-term care policies are owned by individuals.
44

Loss Ratio: The ratio of claims to premiums (claims divided by premiums).
to describe the coordination of financing and provision of health care to rovide high-quality health care on a cost-effective basis.
les.
.
ree savings, tax-free payment of medical bills, and tax-free use of savings for any reason fter the age of 65. Currently, this type of plan is only available to the self-employed and small
igh deductible ealth plan.
medical care, nd catastrophic coverages to persons aged 65 and older, and to some disabled people.
An employer contracts with n insurance company to pay claims if claims in a given period should reach some specified level.
azard: Risk from any nonphysical, personal characteristic or habit of an applicant or insured at may either increase the possibility or intensify the serverity of a loss.
orbidity: The frequency and severity of sickness and accidents in a well-defined class or classes of
ortality: The death rate in a group of people as determined from prior experience.
NAIC): A national organization of state officials ho are charged with the regulation of insurance. It was formed to promote national uniformity in the
et Premium: The premium adjusted for discounts.
up insurance policy in which the employer does not require the mployees to share the cost.
Managed Care: The term usedp Manual Premium (Manual Rating): The premium developed for a group’s coverage from the insurer’s standard rate tab Medicaid: Government insurance program for persons of all ages whose income and resources are insufficient to pay for health care. Medicaid is state-administered and financed by both the states and the federal government. Medical Savings Account (MSA): This instrument was created by Congress in the summer of 1996An MSA is an individual savings account, which is used to cover health care expenses. These accountsprovide tax-fabusinesses with less than 50 employees. Congress has limited the number of MSA’s that can be sold through the year 2000 to 750,000. In conjunction with an MSA, one must also have a hh Medicare: A federally sponsored program that provides hospital benefits, supplementarya Medicare Supplement: This type of private insurance includes Medigap and Medicare Select. These policies cover many services that traditional Medicare (Medicare Parts A & B) does not. Minimum Premium Plan: This type of insurance policy is for self-insuring employers, (an employer that both administers and pays claims against large fluctuations in claims).a Moral Hth Mpersons. M Mutual Insurance Company: An insurer in which the ownership and control is vested in the policyholders. National Association of Insurance Commissioners (wregulation of insurance. It has no official power but has tremendous influence. N Noncontributory Plan: A groe
45 6325

Occupational Hazard: Dangers inherent in the insured’s profession that expose him or her to greater
an average physical danger.
pen Enrollment: The period during which an insured may purchase an insurance policy or switch
verinsurance: Coverage exceeding the probable loss to which it applies.
n: The number of insureds covered under the group plan in relation to the total number ligible to be covered, usually expressed as a percentage.
ider Organization (PPO): A managed care arrangement consisting of a group of ospitals, physicians, and other providers who have contracts with an insurer, employer, third-party
re services to covered persons. PPO’s offer ore choice than HMO’s. Specialists may be seen without approval from a primary care physician (a
remium Rate: The price of a unit of coverage or benefit.
the net premium come collected in a particular jurisdiction by an insurer.
HMO, the PCP acts as a “gatekeeper”. He or she decides what rvices will be provided and whether or not an insured needs to see a specialist.
einsurance: Acceptance by one insurer (the reinsurer) of all or part of the risk of a loss underwritten
se or ses named in the policy are contracted. Examples of this type of policy would include
ancer or AIDS. Specified or dread disease policies are not available in every state.
fulfillment of the insurance contract. Also, the company employee who decides hether or not the company should assume a certain risk.
th Ocompanies. O Participatioe Persistency: The degree to which policies stay in force through the continued payment of renewal premiums. Point of Service Plan (POS): Health care delivery method offered as an option of an employer’s indemnity program. Under such a program, employees coordinate their health care needs through a primary care physician. Preferred Provhadministrator, or other sponsoring group to provide health cam“Gatekeeper”). P Premium Tax: An assessment levied by a federal or state government usually onin Primary Care Physician (PCP): In anse Rby another insurer (the ceding insurer). Rider: A document that modifies or amends the insurance contract. Specified or Dread Disease: This type of health policy provides benefits only if the specific diseagroup of diseaC Stock Insurance Company: An insurer in which the legal ownership and control is vested in the stockholders. Underwriter: The term generally applies to a company that receives the premiums and accepts responsibility for thew
46

Uniform Premium: A rating structure in which one premium applies to all insureds, regardless of agsex, or oc
e, cupation.
nt for routine eye examinations, yeglass lenses, contact lenses, and the purchase and fitting of frames. Vision care policies can be
orkers’ Compensation: Liability insurance requiring certain employers to pay benefits and furnish edical care to employees for on-the-job injuries. Workers’ compensation also pays benefits to
ependents of an employee killed on-the-job.
Producer Price Index Revision
Utilization Rate: The number of insureds who use services divided by the total number of members insured. Vision Expense Insurance: This type of policy provides reimbursemeeintegrated into a major medical plan or purchased separately. Employers typically offer this as a benefitto their employees. In this case, the employer is actually the insurer. Wmd
47 6325

48
edical insurance carriers
ual medical service plans
ice plans
lans
lth insurance
25M Miscellaneous receipts
25MM Miscellaneous rece ts
6325S Secondary services 6325SS Secondary services
Publication Title Listing ( ordered by higher map code )
SIC/Cycle/Version – 6325A1
PPIR Code PPIR Title _________ __________ 6325 Accident, health, and m 6325P Primary services 63251 Medical service plans 6325101 Group comprehensive medical service plans 632510101 Group managed care medical service plans 632510102 Group fee-for-service medical service plans 6325102 Other group and individ 632510201 Individual comprehensive medical serv 632510202 Dental service plans 632510203 Supplemental Medicare service p 632510204 Other medical service plans 63252 Accident and hea 63253 Third party administrative services 6235SM Other receipts 63 63 ip

Form 1 ANNUAL STATEMENT FOR THE YEAR 1995 OF THE
ANALYSIS OF OPERATIONS BY LINES OF BUSINESS (Gain and Loss Exhibit) (Excluding Capital Gains and Losses)
Ordinary Group Accident and Health
1 2 3 4
5
6 7 8 9 10 11 12
Individual Supplementary Credit Life Credit Aggregate of Total Industrial Life Life Insurance Annuities Contracts (Group and Life Insurance Annuities Group (Group and Other Other Lines of Individual) (a) Individual) Business
1. Premiums and annuity considerations . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . XXX . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . XXX . . . 1A. Deposit-type funds . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . XXX . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2. Considerations for supplementary contracts with life contingencies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . XXX . . . . . XXX . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . XXX . . . . . . XXX . . . . . . XXX . . . . . . . . . . . . . 3. Considerations for supplementary contracts without life contingencies and dividend accumulations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3A. Coupons left to accumulate at interest . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4. Net investment income . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4A. Amortization of interest maintenance reserve (IMR) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5. Commissions and expense allowances an reinsurance ceded . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5A. Reserve adjustments on reinsurance ceded . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6. Aggregate mile ins for miscellaneous . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7. Totals (Items 1 to 6) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . XXX . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . XXX . . . . . XXX . . . . . . XXX . . . . . . . . . . . . . . . . . . . . . . . 8. Death benefits . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9. Matured endowments (excluding guaranteed annual pure endowments) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . XXX . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10. Annuity benefits . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . XXX . . . . . . . . . . . . . . . . . . . . . . . . . XXX . . . . . . XXX . . . . . . . . . . . . . . . XXX . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11. Disability benefits and benefits under accident and health policies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11A. Coupons. guaranteed annual pure endowments and similar benefits . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12. Surrender benefits and other fund withdrawals . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . XXX . . . . . . XXX . . . . . . XXX . . . . . . . . . . . . . 13. Group conversions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . XXX . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . XXX . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13A. Transfers on account of group package and contracts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . XXX . . . . . . XXX . . . . . . XXX . . . . . XXX . . . . . XXX . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . XXX . . . . . . . . . . . . . 14. Interest on policy or contract funds . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15. Payments on supplementary contracts with life contingencies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . XXX . . . . . XXX . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . XXX . . . . . . XXX . . . . . . XXX . . . . . . . . . . . . . 16. Payments on supplementary contracts without life contingencies and of dividend accumulations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16A. Accumulated coupon payments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17. Increase in aggregate reserves for life and accident and health policies and contracts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17A. Increase in liability for premium and other deposit funds . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18. Increase in reserve for supplementary contracts without life contingencies and for dividend and coupon accumulations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19. Totals (Items 8 to 18) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20. Commissions on premiums and annuity considerations (direct business only) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21. Commissions and expenses allowances on reinsurance assumed . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22. General insurance expenses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23. Insurance taxes, licenses and fees, excluding federal income taxes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24. Increase in loading on and cost of collection in excess of loading an deferred and uncollected premiums . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24A. Net transfers to or (from Separate Accounts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25. Aggregate write-ins for deductions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26. Totals (Items 19 to 25) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .27. Net gain from operations before dividends to policyholders and federal income taxes (Item 7 minus item 26) . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
28. Dividends to policyholders . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29. Net gain from operations; after dividends to policyholders and before federal income taxes Item 27 minus item 28) . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
30. Federal income taxes incurred (excluding tax an capital gains) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31. Net gain from operations after dividends to policyholders and federal income taxes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . and before realized capital gains or (losses) (Item 29 minus Item 30) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
6
DETAILS OF WRITE-INS 0601 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 0602 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 0603 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 0698. Summary of remaining write-ins for Item 5 from overflow page . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 0699. Totals Items 0601 thru 0603 plus 0698 1 (item 6 above) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2501 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2502 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2503 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2598. Summary of remaining write-ins for item 25 from overflow page . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2599. Totals Items 2501 thru 2503 plus 25981 (Item 25 above) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . (a) Includes the following amounts for FEGLI/SGLI: Item I ................................... Item 8 ................................ Item 13 ................................... Item 22 ................................... Item 23 ...........................
49 6325