1 srnt preconference: progress in the development, monitoring, and implementation of tobacco...
TRANSCRIPT

1
SRNT preconference: Progress in the development,
monitoring, and implementation of tobacco dependence treatment
around the world
Global Bridges Latin America
Gustavo Zabert MD Regional Director

2
Gustavo Zabert Disclosure of COI
19TH ANNUAL INTERNATIONAL MEETING
March 13th 2013, Boston MassOrganization
Type of relationship Content Area
Global Bridges
Regional Director for Latin America
SC promotion and training program
UN Comahue
Associate Professor Pre and post graduate medical ed
Pfizer Principal investigator for MOTIVARE001 research protocol
Investigator initiated research inmotivation to quit
Astra Zeneca
National Coordinator (independent contractor) for PUMA research project
COPD research project in Argentina
GSK Scientific committee member of EPOC Ar
Cross sectional study to explored COPD in Argentina
I never had any relationship with tobacco industries

3
Latin America
• South of Rio Bravo• Area 21,069,500 km²
(7,880,000 sq mi), • 2010 pop 590 million• Languages : Spanish,
Portuguese, Quechua, Maya, Guaraní, Aymara, Nahuatl, and others.
• Combined GDP at 5.16 trillion (US 6.27 trillion)
• 33 countries (CA-Ca-SA)
4
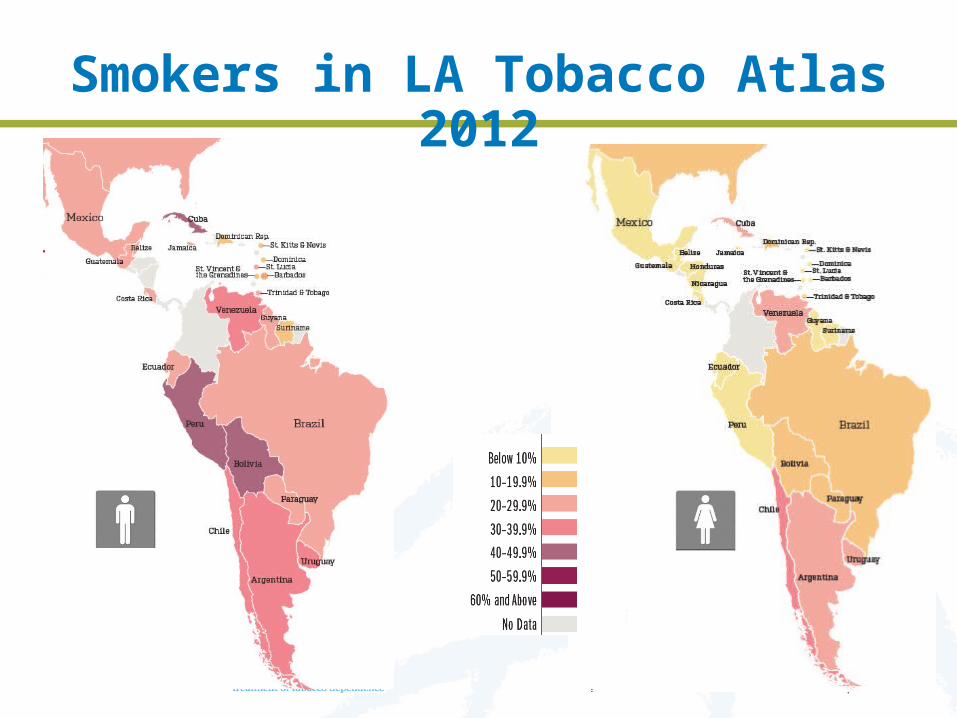
Smokers in LA Tobacco Atlas 2012

5
Teens smoking in LA Tobacco Atlas 2012
6
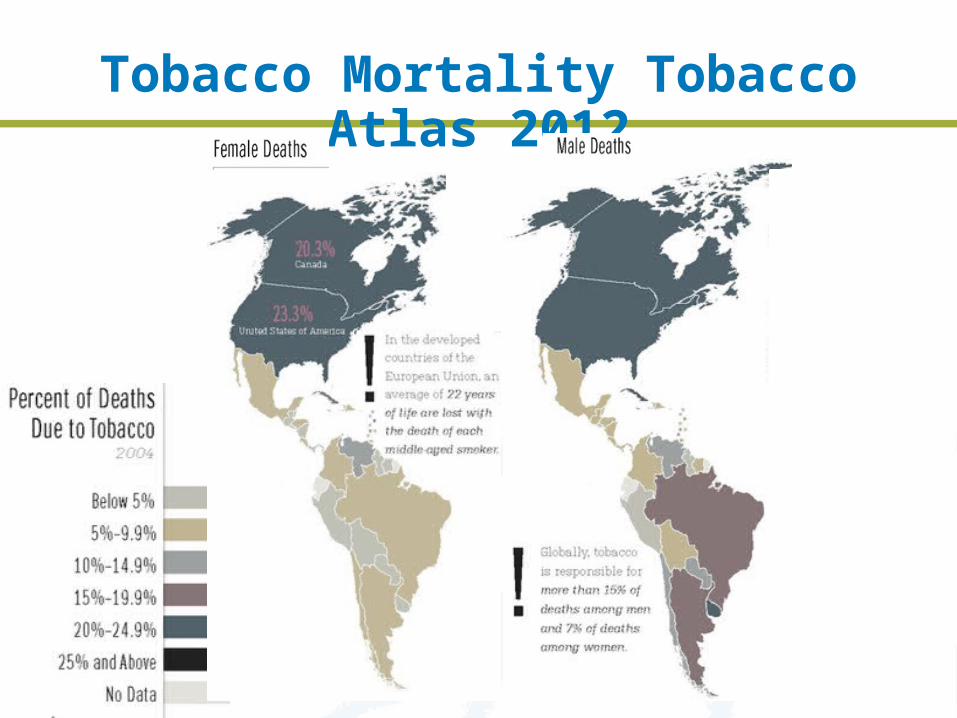
Tobacco Mortality Tobacco Atlas 2012

7
Tobacco Atributable Mortality in LA
Deaths per year
México 60.000
Argentina 40.000
Uruguay 4.700
Paraguay 4.000
Less 30% LA pop
108.700

8
Smoking in Latin America
• 1/3 of population smoke (higher among men)
• Highest prevalence • Males: Cuba and Chile • Females: Argentina and Chile • Teens: Argentina and Chile• Physicians: Cuba, Argentina and
Chile• 2000 tobacco related mortality 265.000 death per year (underestimated)

9
López, Collishaw, 1994
Tobacco epidemic in LA
0 10 20 30 40 50 60 70 80 90 100
Años
Stage I Stage II Stage III StageIV
Tobacc
o d
eath
s
40%
30%
20%
10%males
70%
60%
50%
40%
30%
20%
10%
0%Fe
mal
es Male deaths
Sm
oke
rs
Female
deaths

10
CountryPrevalence among Doctors
Year Females Males
Argentina 2005 25- 31%
Brasil 2006 14.4 % 19.7%
Colombia 22 %‡ 21%‡
Costa Rica 1999 19 %
Cuba 36,4%
Chile 2004 30,5%
Ecuador SD
México 2006 29.3% 37.9%
Perú 2006 22.1% 41.8%
Uruguay 27%
Venezuela 2007 10,8%
Smoking Prevalence among Doctors

11
1992 2001 2007 2011
Año
Smoker physicians: Uruguay
353025201510
50
% fumadores
Boado M, Bianco E. Rev Urug Cardiol 2011;26:214-24
11,1% mujeres 8,2% hombres,
Scenario may be changed!

12
Asociación Argentina de Medicina Respiratoria(AAMR) 1997 ⃰ 2006 2011**
Pulmonologists surveyed 386 418 234
Smoking prevalence 25% 10% 5%
Is Smoking an addictive behaviour? 88% 93% 98%
Do you agree with smoke free hospitals? 96% 97% 99,5%
Do you recall 5 A strategy? 8% 54% 70%
Is NRT effective for SC? 17% 51% 91%
Have you been formally trained in SC? 33% 30% 24%
• *Minervini MC et al .RAMR 2006(3):100-105• ** Schotlender J et al Report AAMR 2012
Scenario may be changed!

13
Population of Latin America
Accessibility of care
30%Smokers
70% consulta
Basic levelbrief
intervention(5 A ABC)
should receive
Acknowledge to receive(50%)
Intermediate level(Drugs + Intensive
Intervention)should prescribe
Reported prescription (15-20%)
Higher levelintensive intervention
specialized teams
population survey
health careproviders´ surveys
Reports Nicotine Dependence Centers

14
Equity in smoking cessation
For every smoker
For every smoker dependent
For smokers highly dependent and co-morbidities
How is?How should it be?
Higher level
Intermediate level
Basic level
Población de Latinoamérica30%fumante
70% consulta
Health Serviceshousing
Workpoverty
UBN
Health coverageInsurance and/or mutualism
socioeconomic level
Higher education and incomes

15
Faculty Puebla 2011

16
Global Bridges Latin America: 2012 Team
LA Regional Director Gustavo Zabert [email protected] LA Regional secretary Vicki Baldi [email protected] LA Host Organization Inter American Heart Foundation (IAHF)
Beatriz Champagne [email protected] Valenzuela [email protected]
Faculty teamCarlos Jimenez Ruiz (Spain) Raul Sansores Martinez (Mexico)
Alvaro Huarte (Uruguay)Erika Urdapilleta (Mexico) Eduardo Bianco (Uruguay)
Veronica Torres (UruguayDaniel Buljubacich (Argentina) Rogelio Pendino (Argentina) Nicolas Flandorffer (Argentina)Edgardo Sandoya (Uruguay) Victor San Martin (Paraguay) Maribel Fernandez Cristobal (Spain)Roberto Castro Cordoba (Costa Rica) Fernando Müller (Argentina) Carlos Araujo (Brasil)Justino Regalado Pineda (Mexico) Andres Mainini (Argentina) Miriam Di Loretto (Argentina)Javier Saimovici (Argentina) Ernesto Ruiz (Argentina)
Eduardo Valeff (Argentina)Elma Correa (Mexico) Mark Cohen Todd (Guatemala)
Elba Esteves (Uruguay)Roberto Castro (Costa Rica) Fernando Muller (Argentina)
Jose Miguel Chatkin (Brasil)Marcelino de Vega (Argentina) Luis D Larrateguy (Argentina)
Carlos Viegas (Brasil)

17

18
GLOBAL BRIDGES LA: training sessions Fecha Lugar Entrenados Horas
April 28, 2011 Puebla (Mexico) 70 8
May 7, 2011 Neuquén (Argentina) 15 8
March 31, 2011 Neuquén (Argentina) 42 12
July 1, 2011 Asuncion (Paraguay) 86 8
August 4, 2011 Cordoba (Argentina) 62 4
August 8, 2011 Parana (Argentina) 39 8
September 7, 2011 San José (Costa Rica) 43 8
October 15, 2011 Lima (Peru) 17 4
October 25, 2011 Quito (Ecuador) 36 12
March 12, 2012 La Plata (Argentina) 45 8
April 10, 2012 Cancun (Mexico) 41 8
May 22, 2012 Rio Grande (Argentina) 28 8
May 28, 2012 Salta (Argentina) 43 8
May 30, 2012 Kingston (Jamaica) 28 8
July 3, 2012 Montevideo (Uruguay) 23 8
July 12, 2012 Bahia Blanca (Argentina) 32 8
August 26, 2012 Mendoza (Argentina) 29 8
August 10, 2012 Buenos Aires (Argentina) 24 6
September 20, 2012 Asuncion (Paraguay) 60 6
October 29, 2012 Madrid (Spain) 26 6
Total 789
19
What would be the impact if each HCP trained offers ONE (1) brief advice (BA)
every working day in the year after training?
789 HCP trained X 240 working days =
189.360 smokers would had received BA
189.360 smokers X 2,5% (abstience rate) =
4.734 quitters
Training in smoking cessation: Real world impact estimation
December 3rd, 2012
20
What would be the impact if 20% of remaining smokers receive NRT plus
intensive intervention (IT) in the following year work?
189.360 smokers – 4.734 quitters = 184.626 smokers
184.626 smokers X 20%= 34.210 smokers IT + NRT
36.925 smokers IT + NRT X 12% (abstience rate)=
4431 quitters
Training in smoking cessation: Real world impact estimation
December 3rd, 2012
21
4734 quitters w/brief advice
+
4.431 quitters w/IT +NRT
9.165 quitters in 2013
Training in smoking cessation: Real world impact estimation
December 3rd, 2012

22
Was GB LA training program effective?
Facts: Behaviour change interventions are
typically complex with multiple, potentially interacting, components
Two categories of intervention components What´s intervention program How is provided
Behaviour change techniques (BCT) involve competencies (knowledge and skills)
Knowledges are easier to assess
GLOBAL BRIDGES Latin America Training 2011/2012
Competence-based training for a national stop smoking service: an English case study
World Conference on Tobacco or HealthSingapore, Wednesday 21st March 2012
Dr Andy McEwenNCSCT Executive Director

2424
Overall score
Smoking in population
Smoking and health
Why hard to stop
Process of stopping
Effective help
Plan and deliver
0 10 20 30 40 50 60 70 80 90 100
63.2
56.9
60.8
65.8
57.9
66.9
68.6
76.6
74.3
78.1
78.4
68.6
76.7
79.4
Change in knowledge scores
Post-training Baseline
Percent correct
All changes p<0.001
• 5,510 unique trainees registered• 2,289 UK stop smoking practitioners• 1,540 completed both assessments

25
GLOBAL BRIDGES Latin America Evaluation 2011/2012
Percentage of questions scored correctly among 500 trained

Behaviour change techniques (BCTs) 1. Describe treatment programme2. Build rapport3. Describe what behavioural support involves4. Facilitate and advise on use of social support5. Describe stop smoking medications6. Assist smoker to set a quit date7. Enhance motivation and self-efficacy8. Emphasise the importance of the not-a-puff rule9. Secure commitment to the not-a-puff rule10. Help smoker cope with barriers, cues and triggers11. Review experience of medication usage12. Advise on adjustment of medication use13. Use CO measurement14. Deal with discrepancies between self-report and CO measures15. Deal with lapses16. Assess commitment, readiness and ability to quit

27
1. Describing treatment programme
2. Building rapport
3. Describing behavioural support
4. Facilitating and advising on social support
5. Describing stop smoking medications
6. Assisting clients to set a quit date
7. Enhancing motivation and self-efficacy
8. Emphasising importance of not a puff rule
9. Securing commitment to not a puff rule
10. Helping to cope with barriers, cues, triggers
11. Assessing experience of medication
12. Advising on adjusting medication usage
13. Using CO measurement
14. Dealing with discrepancies self-report and CO
15. Dealing with lapses
16. Assessing commitment, readiness, ability to quit
1.0 1.5 2.0 2.5 3.0 3.5 4.0 4.5 5.0
3-month follow-up After course Before course
Mean confidence
Competences
Highly con-fident
Not confident
719 trainees in 28 courses 21 courses with follow-up data (N=569)

28
GLOBAL BRIDGES Latin America Evaluation 16 competences 2012
Not confident Highly confident
Mean confident224 trainees in 6 courses
83 with follow-up data

29
Conclusions