11 november 2014 our approach in community services sara hill, podiatry business manager/clinical...
TRANSCRIPT
11 November 2014
Our Approach in Community Services
Sara Hill, Podiatry Business Manager/Clinical LeadJo Wallis, Senior Community PhysiotherapistJo Hood, Podiatry Service Development Lead
Debbie Beales, Lead Nurse Coronary Heart Disease ServiceJo Reid, Physiotherapy Team Leader
What patients want from talking with their clinicians
Angela Coulter Senior Research Scientist
Nuffield Department of Population Health, University of Oxford
I N F O R M AT I O N , I N VO LV E M E N T , S U P P O RT
What Patients Want
Angela CoulterHealth Coaching conference
Lynford Hall, November 2014
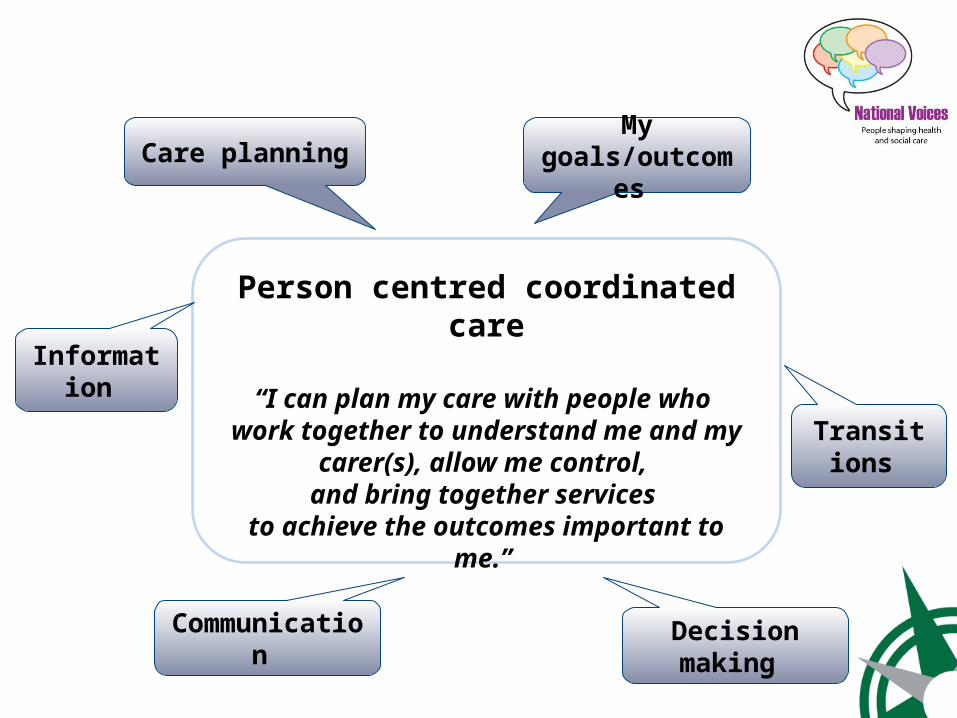
Person centred coordinated care
“I can plan my care with people who work together to understand me and my
carer(s), allow me control, and bring together services
to achieve the outcomes important to me.”
Information
My goals/outcomes
Communication Decision making
Care planning
Transitions
Managing Long Term Conditions
Professional care – 5 hours per year
Self-care – 8,755 hours per year

Diabetes Web of Care

Alzheimer’s Web of Care
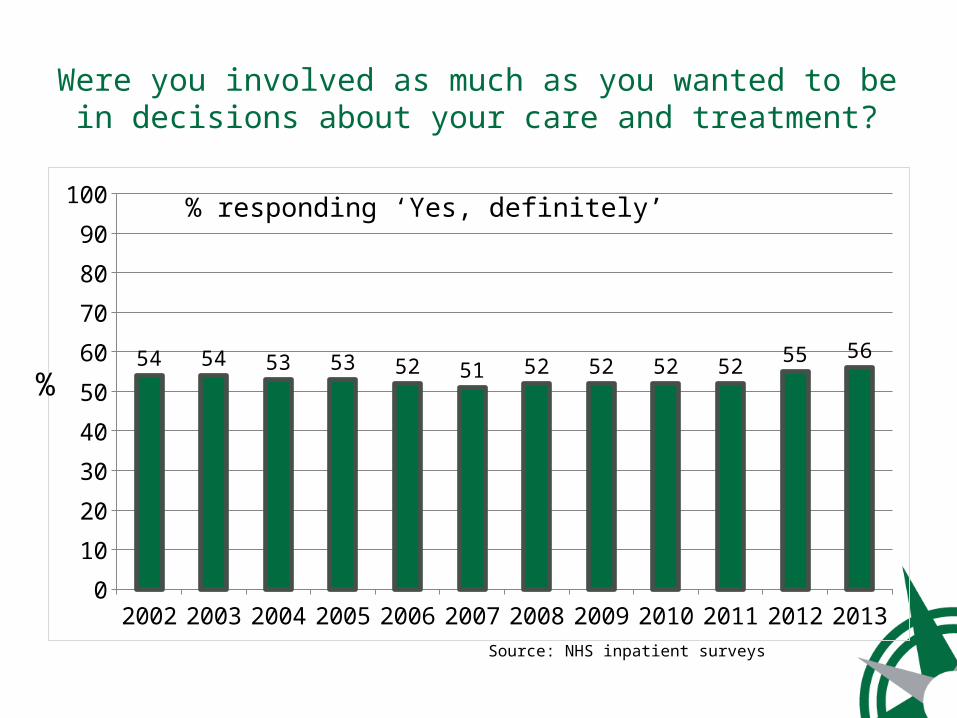
Were you involved as much as you wanted to be in decisions about your care and treatment?
2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 20130
10
20
30
40
50
60
70
80
90
100
54 54 53 53 52 51 52 52 52 52 55 56
%
% responding ‘Yes, definitely’
Source: NHS inpatient surveys

Care and Support Planning
Personalised care planning aims to ensure that individuals’ values and concerns shape the way in which they are supported to live with and self-manage their long-term condition(s)
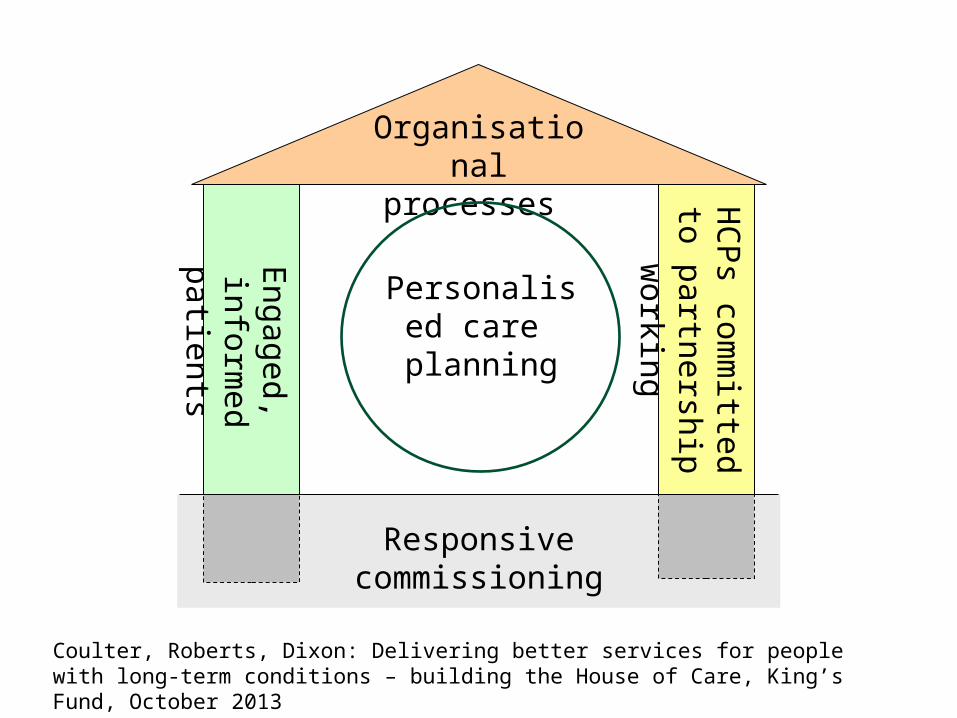
Engaged,
informed patients
HC
Ps com
mitted to
partnership working
Organisationalprocesses
Responsive commissioning
Personalised care
planning
Coulter, Roberts, Dixon: Delivering better services for people with long-term conditions – building the House of Care, King’s Fund, October 2013
What Patients Need to Know
• What are my options?• What are the benefits and
possible harms?• How likely are these benefits
and harms?• What are your goals, do they
match mine?• What can I do to help myself?• What can you do to support
me?
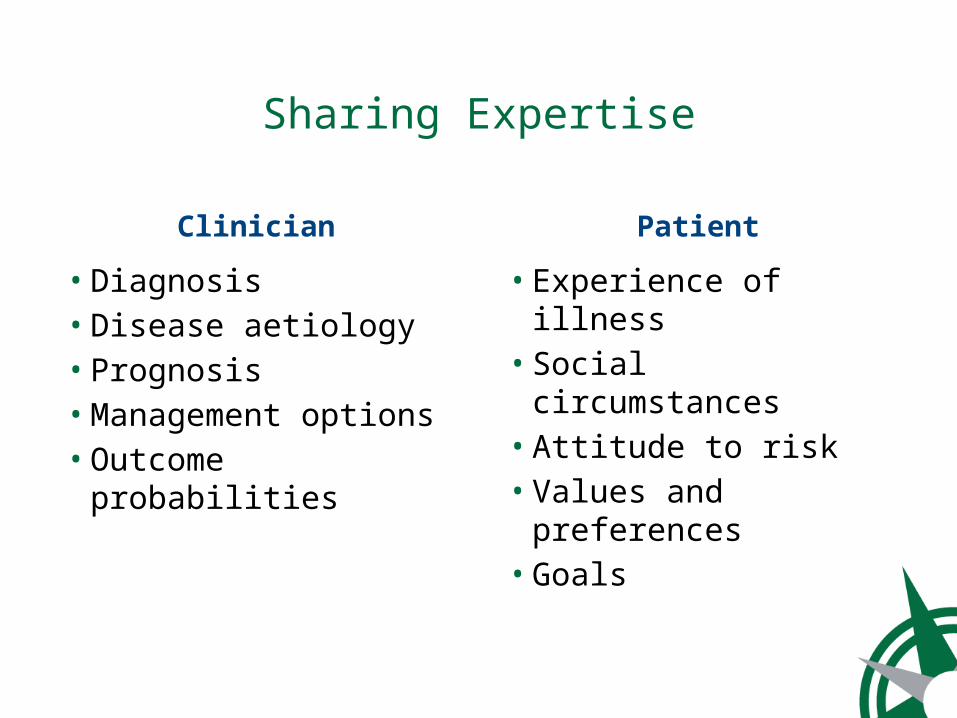
Sharing Expertise
Clinician
• Diagnosis• Disease aetiology• Prognosis• Management options• Outcome probabilities
Patient
• Experience of illness• Social circumstances• Attitude to risk• Values and
preferences• Goals

One-time Decisions for Tests or Treatments
Chronic Care Management Decisions
Personal Care Planning
Shared Decision Making
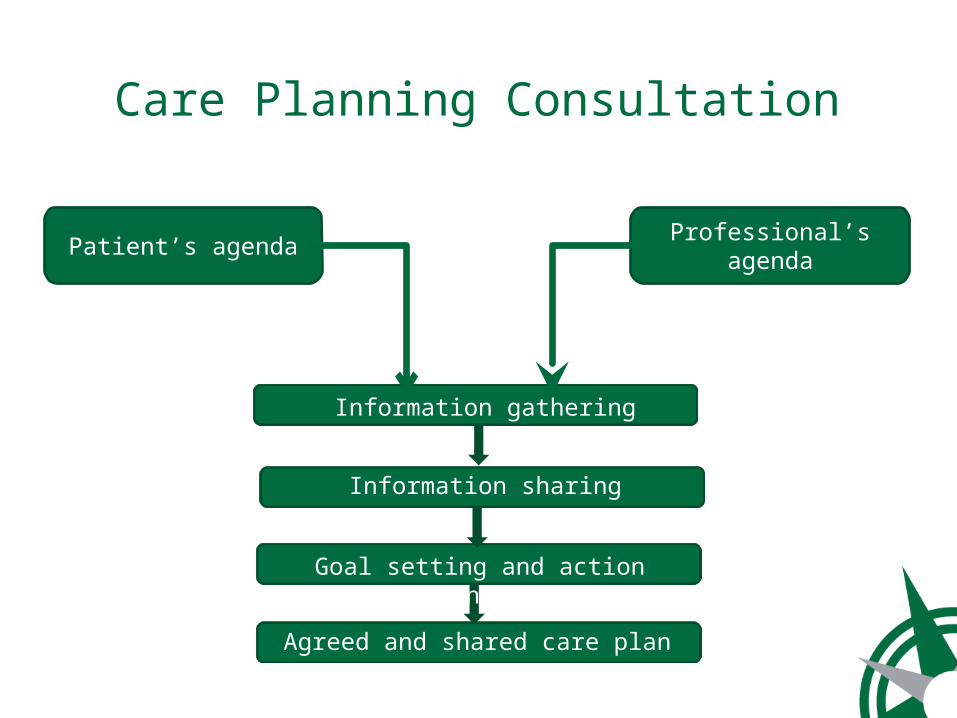
Care Planning Consultation
Patient’s agenda Professional’s agenda
Goal setting and action planning
Information sharing
Agreed and shared care plan
Information gathering
Information sharing

14
1. Preparation
2. Goal setting
3. Action planning
4. Documentin
g
5. Coordinating
6. Suppor
ting
7. Review
ing
Care planning
cycle
TEAMcare, USA
Aim: • To improve outcomes for patients with major depression and poorly controlled diabetes, coronary heart disease or both by developing a patient-centred, primary care-based, care management intervention for multiple conditions
TEAMcare Tools
• Collaborative goal-setting and action planning
• Evidence-based pharmacotherapy• Structured consultations and monitoring every 2-3 weeks with physician or nurse
• Proactive nurse follow-ups to support self-care using motivational interviewing, problem-solving techniques and maintenance plans
• Staff training and weekly supervision
TEAMcare – Results
Improvements in:• HbA1c• Cholesterol• Blood pressure• Depression• Quality of life• Confidence to self-manage• Cost-effectivenessKaton 2010, von Korff 2011, Lin 2012, Katon 2012, Ludman 2013
Systematic Review of Personalised Care Planning
• 10,000 abstracts scanned• 43 articles included describing 19 unique studies (RCTs)
• USA (13 trials), Australia (1), China (1), Denmark (1), Netherlands (1), Taiwan (1), UK (1)
Participants and Settings
• 10,856 participants• Diabetes (12 trials), mental health (3), heart failure (1), end-stage renal disease (1), asthma (1), various conditions (1)
• Primary/community clinics (17)• Hospital clinics (3)
Interventions
• Aims – behaviour change among patients (19)• Behaviour change among patients AND clinicians (4)
• Goal setting, action planning, follow-up (19)• Tools – information packages, structured consultations (coaching), peer support, group visits
• Clinicians – nurses/therapists (14), doctors (6), peer coaches (2), mental health providers (2)
Outcomes
• Physical health• Psychological health• Subjective health status• Self-management capabilities• Health-related behaviours• Resource use• Adverse effects
Outcomes
• Physical health: blood glucose control
• Psychological health: depression• Subjective health status: mixed• Self-management capabilities: self-efficacy
• Health-related behaviours: mixed• Resource use: mixed• Adverse effects: none

Care Planning Works Best When it is ………
• Comprehensive (all 7 stages of care planning cycle)
• Higher intensity (longer duration (> 3 months), more contacts)
• Integrated with usual care• Well supported (training, supervision and support for clinicians as well as patients)
What We Have Learnt
Traditional practice styles…….
• Create dependency• Discourage self-care• Ignore preferences• Undermine confidence• Do not encourage
healthy behaviours• Lead to fragmented
care
Informed, Empowered Patients Have the knowledge, skills and
confidence to manage their own health and healthcare,
And they……• Make healthy lifestyle choices• Make informed and personally
relevant decisions about their treatment and care
• Adhere to treatment regimes • Experience fewer adverse events• Use less costly healthcare
Health Affairs Feb 2013
The Greatest Untapped Resource