1195 ssm 1: dr j o’neill - healthy inclusion · 2011-02-11 · 1195 ‐ ssm 1: dr j o’neill ......
TRANSCRIPT

John Paul McLindon 200665371 SSM 1: Addiction Medicine: Alcohol Word Count: 2,828
1195‐ SSM 1: Dr J O’Neill
What are the attitudes & behaviours of the
young population regarding alcohol addiction?
Figure: 1 1
“Responsible Drinking? Now that's an Oxymoron”2
John Paul McLindon
Candidate Number: 1195
1st Year Medical Student University of Liverpool
Word Count: 2,828
1 | P a g e

John Paul McLindon 200665371 SSM 1: Addiction Medicine: Alcohol Word Count: 2,828
Contents
Abstract Page 3
Learning Objectives & Core Learning Activities Page 4
Acknowledgements Page 4
Introduction Pages 5‐6
Definitions Pages 6‐8
Global/National/Local Perspectives of Alcohol Pages 8‐9
Key Statistics of Alcohol in Liverpool Pages 9‐10
Media Portrayal of Alcohol Page 11
Key Health Problems of Alcohol Page 11
Screening Page 12
Treatment Options Page 12
Literature Review
Method Pages 12‐13
Search Results Pages 13‐14
Critical Appraisal Skills Programme Page 14
Chosen Articles Page 15
Strengths & Weaknesses Pages 15‐16
Discussion Pages 16‐18
Conclusion & Recommendations Pages 18‐19
References Pages 20‐22
Reflection Page 23
Appendix Pages 23‐34
2 | P a g e

John Paul McLindon 200665371 SSM 1: Addiction Medicine: Alcohol Word Count: 2,828
Abstract
Figure: 2
Background
Alcohol and its acceptance in society vary from country to country. In the UK alcohol is
widely accepted as a vital ingredient to many social events. Most people drink responsibly
not putting themselves or others at risk, however excessive alcohol consumption can be
harmful. Drinking has a minimum legal limit of eighteen years of age, but in reality the
majority of the population of the UK are introduced to alcohol earlier than this. Young
adults often indulge in binge drinking (BD) a pattern of alcohol consumption seen in many
N. European countries with recent studies suggesting that the UK has the 2nd highest rate
in Europe.5
Aim
The aim is to apply search methods to find articles relevant to the subject matter and
analyse them accordingly.
Method
Using a variety of search tools like Science Direct, NHS Athens and PubMed, a wide
collection of articles were found around alcohol, addiction and the youth. After applying
filters and criteria like year of publication, the number of accepted articles for use was
narrowed.
Results
The results of the Science Direct search produced four usable articles. An article from a
previous health promotion presentation was also used. After applying criteria like a CASP
table three articles were discarded leaving one paper from the Science Direct database
search and the previously owned article.
Conclusion
The Government needs to invest in effective Public Health strategies for harm reduction,
engaging with health providers, service users, voluntary agencies, the legal profession, the
drinks industry and the judicial system to promote safe drinking through a range of
positive actions. Screening tools need to be employed to identify problems at an early
stage and to target specific interventions to those at risk of progressing to harmful
drinking patterns. A cohesive approach between all of these interested parties should
facilitate change and improvement for a more positive approach to drinking in society
3 | P a g e

John Paul McLindon 200665371 SSM 1: Addiction Medicine: Alcohol Word Count: 2,828
Learning Objectives & Core Learning Activities.
Figure: 3
Learning objectives:
1. To understand the attitudes and behaviours of young adults which lead to patterns of
excessive drinking and alcohol dependence, including psychological, social and physical
aspects.
2. Evaluate the clinical and aftercare treatments available for an individual addicted to alcohol
including medication to aid detoxification and strategies to help support mental and
physical dependency on alcohol.
3. To understand the strategies, legal, clinical and social employed to support individuals
addicted to alcohol.
Core Learning Activities:
1. Hospital Placements at Aintree Hospital
2. Case histories from inpatients
3. Journal Club Presentation
Acknowledgements and Thanks.
Figure: 4
I would like to begin by thanking my convenor Dr O’Neil and his administrator Siobhan for
their support. Also I must express my gratitude to Sarah Haywood for all the help and
teaching given to myself and my fellow student Jill Richardson on our placement at Aintree
Hospital. Sarah gave considerable time from her busy working day to allow Jill and myself to
shadow her in her role as the Alcohol Specialist Nurse. In this role Sarah’s aim is to educate,
treat and support those patients in the area who are either addicted to alcohol or binge
drink on a regular basis. It was a great learning curve for me to see the variety of health
problems caused by continuous excessive consumption of alcohol but also to understand
the problems in life that people face which might steer them towards a life dependant upon
alcohol. My final thanks are to those patients who allowed Jill and I to explore their history
related to alcohol. This insight broadened my understanding of their personal experiences.
Examples of these case histories are included in the Appendix 8 & 9.
4 | P a g e

John Paul McLindon 200665371 SSM 1: Addiction Medicine: Alcohol Word Count: 2,828
Introduction
General Medical Council’s (GMC); Duties of a Doctor
Patients must be able to trust doctors with their lives and health. To justify that trust you
must show respect for human life.3 The GMC has published guidelines for doctors to ensure
that they provide the highest standard of healthcare to all service users. These guidelines
cover many areas ranging from clinical skills, knowledge and professionalism to
understanding how to treat patients as individuals. The guidelines are summarised in
appendix 1.
Beauchamp & Childress: four principles of medical ethics.
The “four principles plus scope” approach to ethics developed by Beauchamp and Childress
was reviewed by Gillon in 1994.4 It provides a relatively simple unbiased framework for
ethical issues in clinical practice based on four prima facie moral commitments respect for
autonomy, beneficence, non‐maleficence, and justice with consideration for the scope of
how they are applied. The moral framework couched in basic moral language aids carers to
make decisions in clinical practice.
Figure 5
Respect for Autonomy
Autonomy or “self rule” means to make one’s own decisions following deliberation.
Respect for autonomy is a moral obligation to appreciate autonomy in others. In the
context of health care this includes respect for an individual’s decision following
consultation, full informed consent and with confidentiality.4 Respect for patients'
autonomy requires the carer, not to deceive patients, for example, about their
diagnosed illness unless they clearly wish to be deceived. Respect for autonomy even
requires us to be on time for appointments as an agreed appointment is a kind of
mutual promise and if we do not keep an appointment we break the promise. 4 To
exercise respect for autonomy health care workers must be able to communicate well
with their patients and clients. Effective communication requires, most importantly,
active listening (and not just with the ears) as well as telling (and not just with the lips
or a word processor) and is usually necessary for giving patients adequate information
about any proposed intervention and for finding out whether patients want that
intervention. 4 It is also essential to appreciate when patients do not want to receive
information and to respect their wishes in this context
5 | P a g e

John Paul McLindon 200665371 SSM 1: Addiction Medicine: Alcohol Word Count: 2,828
Definitions
General Phrases Figure: 6
Definition
World Health
Organisation (WHO)
WHO is the directing and coordinating authority for health within the United Nations system. It is responsible for providing leadership on global health matters, shaping the health research agenda, setting norms and standards, articulating evidence‐based policy options, providing technical support to countries and monitoring and assessing health trends. 5
Human Rights Anyone who is in the UK for any reason has fundamental human rights
which government and public authorities are legally obliged to respect.
Beneficence & Non‐maleficence.
Health care workers committed to helping others inevitably risk harming them. In this
context they must consider the principles of beneficence and non‐maleficence.4 in
essence we aim to offer net benefit over harm. Where we can offer no benefit we must
certainly cause no to harm them). i.e. the principles may be considered together but are
in fact separate.
To apply these principles the professional must fully understand the risks and benefits
of a procedure/treatment including proven scientific evidence about the proposed
intervention. Then follows the process of gaining informed consent before applying the
moral and ethical principles of beneficence and non‐maleficence.
Another obligation overlaps with the ethical principal of autonomy as we may not insist
upon treating an individual, even though it may benefit them if their wish is to refuse a
certain treatment/procedure.
Justice.
Justice is often regarded as being synonymous with fairness and can be summarised as
the moral obligation to act on the basis of fair adjudication between competing claims.4
In medical ethics the duties of justice can be subdivided into three categories: fair
distribution of scarce resources (distributive justice), respect for people's rights (rights
based justice) and respect for morally acceptable laws (legal justice).4 In health care the
ethical principle of justice ties closely with the obligation of treating patients equally but
with appropriate adjustment to the individuals needs where applicable.
6 | P a g e
John Paul McLindon 200665371 SSM 1: Addiction Medicine: Alcohol Word Count: 2,828
These became law as part of the Human Rights Act 1998.6 The list of
these Human Rights can be found in Appendix 2.
Inverse Care Law The inverse care law was first described by Julian Tudor Hart in 1971. It
states that "the availability of good medical care tends to vary inversely
with the need for it in the population served." 7
Health Inequalities Health inequality refers to all those barriers in an individual’s life that mean he/she will not receive an equal level of healthcare to another. Some of these inequalities the NHS try to rule out as best as possible but some inequalities they can’t deal with. Health inequalities can be found in many aspects of health; for example, poor people not only live less long than rich, but also have more years of poor health. Access to health is also uneven. The old and disabled receive worse treatment than the young and able bodied. 8
Poverty There is no one true definition for poverty. After researching from
various sources the most widely defined definition is an individual living
on less than 60% of the median income of the population however other
sources have segregated poverty into three areas; social exclusion,
relative poverty and absolute poverty. These are defined further in
Appendix 3.
Vulnerable Groups This has a wide definition that varies from country to country. The key
characteristics of a vulnerable group are age, location, ethnicity and sex
as well as disabilities both physical and mental.
Harm Reduction Harm reduction (or harm minimisation) refers to a range of public health
policies designed to reduce the harmful consequences associated with
recreational drug use and other high risk activities. Harm reduction is
put forward as a useful perspective alongside the more conventional
approaches of demand and supply reduction. 9
Prohibition Prohibition is a method of inhibiting something in law or religion, for
example the advertisement of smoking on the television or alcohol
before a certain time is prohibited.
Polydrug Use Polydrug use refers to the use of two or more psychoactive drugs in combination to achieve a particular effect. In many cases one drug is used as a base‐primary ‐ or preferred drug, with additional drugs to leaven or compensate for the side effects of the primary drug and make the experience more enjoyable with drug synergy effects, or to supplement for primary drug when supply is low. 10
Alcohol Specific
Unit The strength of an alcoholic drink is determined by the percentage of alcohol by volume (ABV). A unit corresponds to approximately 8g (or 10ml) of pure alcohol, regardless of the amount of liquid in which it is diluted. For instance, half a pint of beer has an ABV of 3.5% or a small
7 | P a g e

John Paul McLindon 200665371 SSM 1: Addiction Medicine: Alcohol Word Count: 2,828
glass of wine has an ABV of 12‐14% and is therefore the equivalent to one unit. Guidelines issued by the Department of Health in 1995 recommends a maximum daily alcohol intake of 3‐4 units for men and 2‐3 units for women. This is the equivalent of 2 pints of normal strength (4%) beer for a man or 3 standard 175 ml glasses of wine for a woman.11
Harmful/Hazardous
intake
Hazardous drinking is considered to be drinking between 15 and 35 units a week for women and between 22 and 50 units a week for men. Harmful drinking levels are considered to be drinking more than 35 units a week for women and more than 50 units a week for men. 12
Binge Drinking Binge drinking is the consumption of excessive amounts of alcohol in a limited time period. Although opinions on what constitutes binge drinking vary, the accepted definition is the consumption of twice (or more) maximum daily recommended alcohol intake in the Governments guidelines (3‐4 units for men and 2‐3 units for women). This means that binge drinking is defined as 8 units for men or 6 units for women in either a drinking session or 24 hour period.11
Detoxification Detoxification (detox for short) is the physiological or medicinal removal of toxic substances from a living organism, including, but not limited to, the human body and additionally can refer to the period of withdrawal during which an organism returns to homeostasis after long‐term use of an addictive substance. 13
Abstinence Abstinence is a voluntary restraint from indulging in bodily activities that are widely experienced as giving pleasure. Most frequently, the term refers to Sexual abstinence, or abstention from alcohol or food. The practice can arise from religious prohibitions or practical considerations. 14
Rehabilitation Drug rehabilitation (often drug rehab or just rehab) is a term for the processes of medical and/or psychotherapeutic treatment, for dependency on psychoactive substances such as alcohol, prescription drugs, and so‐called street drugs such as cocaine, heroin or amphetamines. The general intent is to enable the patient to cease substance abuse, in order to avoid the psychological, legal, financial, social, and physical consequences that can be caused, especially by extreme abuse. 15
Global/National & Local Perspectives of Alcohol.
Alcohol and its acceptance in society vary from country to country. In the UK alcohol is widely accepted as a vital ingredient to many social events. Most people drink responsibly not putting themselves or others at risk, however excessive alcohol consumption can be harmful. It may cause accidents and injuries, serious and even fatal illnesses. Drinking too
8 | P a g e

John Paul McLindon 200665371 SSM 1: Addiction Medicine: Alcohol Word Count: 2,828
much may also lead to anti‐social behaviour, alcohol related violence and drink driving all of which have an impact on wider society. Statistics provided by the Home Office for 2008 indicate 9031 deaths directly attributed by alcohol but more than 40,000 alcohol related deaths. There has been a threefold increase in liver cirrhosis deaths between 1970 and 1998 and when broken down into age young groups this reflects an eightfold increase for men and a sevenfold increase for women ages 34 to 44. Of even greater concern is a fourfold increase in cirrhosis deaths in 25 to 34 year olds indicating that drinking is starting at a very young age.16 Drinking has a minimum legal limit of eighteen years of age, but in reality the majority of the population of the UK are introduced to alcohol earlier than this. Young adults often indulge in binge drinking (BD) a pattern of alcohol consumption seen in many N. European countries with recent studies suggesting that the UK has the 2nd highest rate in Europe.11 The peak prevalence of BD is the age group of 16‐24 year olds. The majority of BD problems are visible in urban areas at weekends. Studies on teenage binge drinking conducted by the Academy of Medical Sciences and the Health Development Agency have demonstrated the scale of the problem in the UK.
23% of adult males and 9% of adult females engage in binge drinking, a total of
almost 6 million people in the UK.
Within the last ten years binge drinking in young British women has risen more than
in any other EU country.
Death rates from acute intoxication due to binge drinking have doubled over the
past 20 years in both sexes.
29% of alcohol related deaths are due to the injuries sustained whilst intoxicated and
are more common among 16‐34 year olds. 11
Key Statistics of Alcohol in Liverpool
The Centre for Public Health at Liverpool John Moores University regularly compiles data
related to patterns of alcohol consumption in Merseyside. The following charts detail some
of their findings.12 The chart on alcohol consumption patterns demonstrates that Liverpool
has figures exceeding the N. West and England as a whole for the three main patterns of
excess drinking behaviour. A similar pattern is followed for alcohol specific hospital
admissions where Liverpool again significantly exceeds the figures for the N. West and the
rest of England for both males and females, though in general terms men are admitted
twice as often as women.
9 | P a g e

John Paul McLindon 200665371 SSM 1: Addiction Medicine: Alcohol Word Count: 2,828
27
23
8
23 22
6
1820
5
0
5
10
15
20
25
30
Binge Hazardous Harmful
percentage of population(synthetic estimate)
Alcohol Consumption Patterns
Liverpool
N.West
England
Figure: 7
915
536
340422
270164
0
100
200
300
400
500
600
700
800
900
1000
Liverpool N.West
rate per 100,000
pop
Alcohol specific hospital admissions for Liverpool 2005/06
England
Males
Females
Figure: 8
10 | P a g e

John Paul McLindon 200665371 SSM 1: Addiction Medicine: Alcohol Word Count: 2,828
Media Portrayal of Alcoholics
There would appear to be a great conflict in the portrayal of alcohol and alcoholics in a
variety of media settings. Newspapers in particular will often highlight the negative impact
of alcohol often related to criminal activities and anti‐social behaviours such as drink driving.
In T.V and film alcoholism is often portrayed, particularly amongst older individuals as
secretive and likely to cause problems in relationships, at work and also with health.
Contrast this with the generally more positive attributes of alcohol promoted to the younger
generation through celebrity magazines and in music videos. This is particularly relevant
over recent years for younger females influenced by the “ladette” culture of celebrities and
radio DJ’s. Alcohol is often promoted for its effects in increasing confidence in social settings
and sexual success. Media coverage typically focuses on the effects of alcoholism rather
than the root causes. The potential effect of this is to stigmatise and stereotype the alcohol
making it increasingly difficult for the individual to obtain help and support.
Key Health Problems Associated with Alcohol
Physical effects of alcohol on our bodies are largely dose‐dependent. This means that the
more we drink the more pronounced the effects will be. The effects of alcohol intoxication
are also related to the time scale in which alcohol is consumed. Drinking alcohol quickly
leads to a rapid increase in the blood alcohol concentration (BAC) and this is a characteristic
of binge drinking. A rapid increase in BAC leads to intoxication and impaired neurological
functions. Further physical risks include hypothermia, hypoglycaemia (extremely low blood
sugar levels), coma, heart irregularities and strokes. Vomiting is a common effect of
intoxication and if the conscious level is impaired then there is an increased risk of
aspiration of vomit into the lungs leading to pneumonia and even death due to airway
obstruction. 11
Binge drinking is closely related to mental health problems. In up to 25% of suicides and
65% of suicide attempts binge drinking has been a contributing factor. The figure is up to
75% of other cases of deliberate self harm. The number of teenagers being admitted to
hospital for psychiatric problems attributed to the effects of binge drinking has increased in
the last 10 years. Alcohol has direct effects upon the brain affecting mood, motivation,
memory, attention span and lowering overall performance at school. 11
Alcohol consumption and in particular binge drinking affects not only physical and mental
health but also social health. Binge drinking promotes violent and aggressive behaviour
particularly in men. In women binge drinking increases their risk of being a victim of assault
and in particular serious sexual assaults. It also increases the chance of having unsafe and
unprotected intercourse with resultant effects being sexually transmitted infections and
unplanned pregnancies. Antisocial behaviour and criminal offences linked to binge drinking
contribute to a considerable burden for the countries healthcare systems, police, courts and
prisons. 11
11 | P a g e
John Paul McLindon 200665371 SSM 1: Addiction Medicine: Alcohol Word Count: 2,828
Screening
Screening tools can be used to determine if a patient has alcohol dependency problems and
may also help guide management and treatment. Various screening tests are available, they
all should be easy to administer, consistent to interpret and relevant in a clinical setting.
Examples including; Alcohol Use Disorders Identification Test (AUDIT), Alcohol Assessment
Tool (AED) and Severity of Alcohol Dependence Questionnaire (SADQ‐C) are shown in
Appendix 4, 5 & 6.
Treatment Options
Treatment options for alcohol dependency are limited both in terms of range and success.
Where screening tools identify problem drinking structured brief interventions may help
reduce drinking back to normal levels. Patients admitted to hospital with acute
detoxification may benefit from sedative treatments such as chlordiazepoxide or lorazepam,
together with vitamin supplements such as pabrinex or thiamine for nutritional support. For
longer term management of alcohol dependency various drugs such as disulfiram,
acamprosate and naltrexone have been used. From my discussions with Sarah Haywood it
would appear that few of these treatment options offer significant long term benefit.
Literature Review
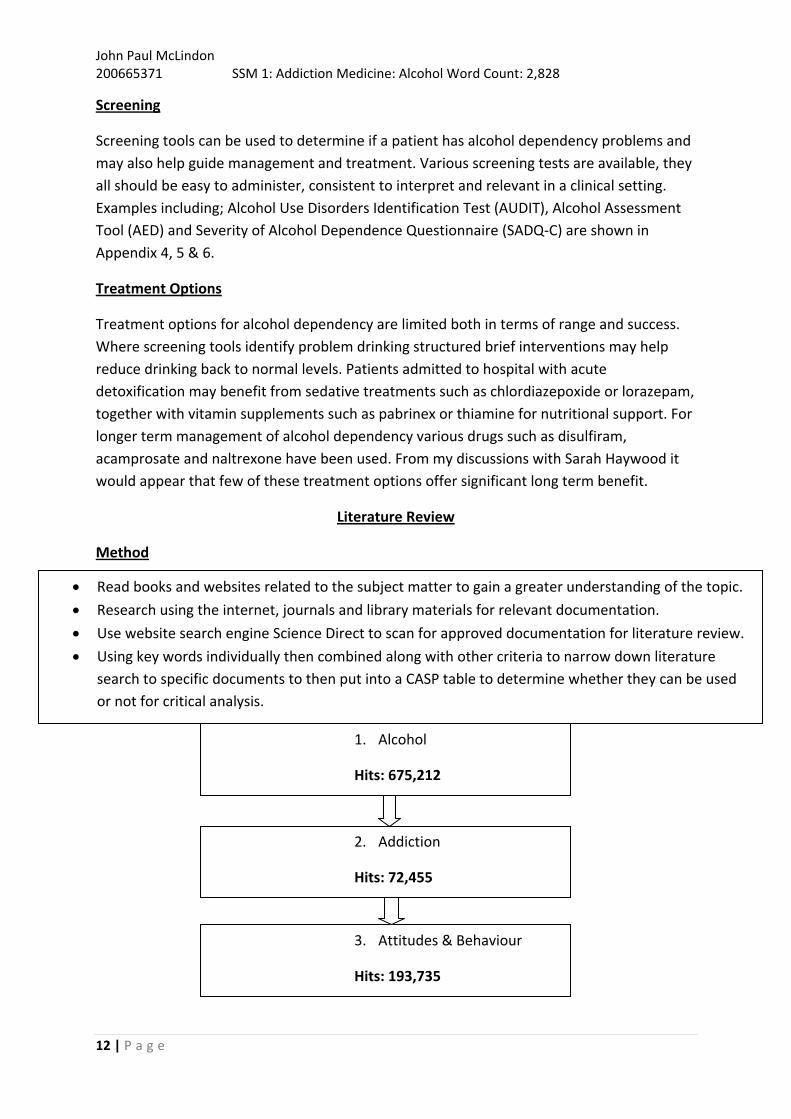
Method
3. Attitudes & Behaviour
Hits: 193,735
2. Addiction
Hits: 72,455
1. Alcohol
Hits: 675,212
Read books and websites related to the subject matter to gain a greater understanding of the topic.
Research using the internet, journals and library materials for relevant documentation.
Use website search engine Science Direct to scan for approved documentation for literature review.
Using key words individually then combined along with other criteria to narrow down literature
search to specific documents to then put into a CASP table to determine whether they can be used
or not for critical analysis.
12 | P a g e

John Paul McLindon 200665371 SSM 1: Addiction Medicine: Alcohol Word Count: 2,828
9. Criteria same as 8, but years 2009‐2011
Hits: 215
Chosen Papers (4 from website search, 1 from previous research)
Of the 215 results those related to drugs were excluded. I then reviewed the abstracts of the remaining
documents and identified four that appeared suitable for my literature appraisal. From my foundation
course health promotion presentation I already had the article by Lightowlers C et al. Database articles
found were;
1. Cranford J A, Zucker R A, Jester J M, Puttler L I, Fitzgerald H E. Parental alcohol involvement &
adolescent alcohol expectancies predict alcohol in male adolescents. Psychology of Addictive
Behaviours. 21/09/2009. Volume 24. Issue 3. Pages 386‐396. 06/02/2011 17
2. Chartier K G, Hesselbrock M N, Hesselbrock V M. Alcohol problems in young adults transitioning from
adolescence to adulthood: The association with race & gender. Addictive Behaviours. March 2011.
Volume 36. Issue 3. Pages 167‐174. 06/02/2011 18
3. Corbin W R, Iwamoto D K, Fromme K. Broad social motives, alcohol use, and related problems:
mechanisms of risk from high school through college. Addictive Behaviours. March 2011. Volume 36.
Issue 3. Pages 222‐230. 06/02/2011 19
Figure: 9
8. Clicked; addictive behaviour, drug & alcohol
dependence & psychology of addictive behaviours
Hits : 288
7. Clicked Years 2008‐2011
Hits: 1,264
6. Clicked Journals Only
Hits: 4,309
5. Combine 1,2,3 & 4
Hits: 4,666
4. Adolescents
Hits: 227,883
13 | P a g e

John Paul McLindon 200665371 SSM 1: Addiction Medicine: Alcohol Word Count: 2,828
4. Clark H K, Ringwalt C L, Shamblen S R. Predicting adolescent substance use: The effects
of depressed mood and positive expectancies. Addictive Behaviours. Available on
database from 11/01/2011. 06/02/2011 20
Previously owned article was;
5. Lightowlers C, Morleo M, Harkins C. Understanding young people’s alcohol‐related
social norms in Sefton‐Interim Report. Centre for Public Health. April 2099. Accessed
December 2009. 21
Critical Appraisal Skills Programme
To help me determine whether the chosen articles are suffice to use in my literature review
I created a small CASP table to compare and review the contents of each article.
Article/Journal Number CASP Question
1 2 3 4 5
Are the aims of the research clearly stated? Yes Yes Yes Yes Yes
Is the qualitative method appropriate for design?
Yes
Yes Yes Yes Yes
Have ethical issues been considered? Yes No Yes Yes Yes
Is there a clear statement of the findings? Yes No Yes Yes Yes
Were the results processed appropriately? Yes No Yes Yes Yes
14 | P a g e
There are 4 criteria an article must match for it to be suitable;
1. Is it Relevant?
2. Is it Readable?
3. Is it Reliable?
4. Is It Recent?
Article 1; this was a well structured article with relevant subject material and also recent, however
only male participants were used and therefore the young population isn’t portrayed accurately.
This article is discarded.
Article 2; this article was recent and quite relevant, however it focussed on two variables; race
and gender and how these affected alcohol behaviours. As many other variables were excluded I
have discarded this article.
Figure: 10

John Paul McLindon 200665371 SSM 1: Addiction Medicine: Alcohol Word Count: 2,828
Article 4; this document focused only on depression as a factor contributing to drinking. In
addition I struggled to find a published date for this article therefore discarded
This left me with both article 3 & 5 left as possibilities to analyse.
Article 3; this is a current article assessing relevant criteria across a broad range of factors
and multiple behavioural aspects contributing to excessive drinking in individuals over a
period of time. As the study is performed in a population based in the U.S it will allow a
comparison with the experience of alcohol and youth in the U.K.
Article 5; article 5 is dated 2009, not as recent as the other three articles, it is focussed on
the attitudes and behaviours towards alcohol of young people in a borough of Merseyside. I
therefore feel its findings are relevant as it evaluates the local population near the Primary
Care Trust in which I had my SSM placement.
I also searched the NHS Athens database but found no additional relevant material which would
have broadened my understanding of alcohol problems in youth.
Strengths & Weaknesses
Article 3
Strengths;
Published in a renowned American journal
Looks professional
Copyrighted
Clear outline in the introduction as to why the research is required
Participant number high (2245)
Initial survey reported, follow up awaited
Females well represented
Wide range of race/ethnic groups surveyed
Survey measures frequency and quantity of alcohol use
Use of standardised survey tool (Rutgers Alcohol Problem Index‐ Appendix 7)
Broad social motives researched addressing why an individual feels the need to drink
e.g. drinking to feel popular.
Personal drinking values assessed e.g. “it’s okay if I get drunk frequently if that is
what I want to do” 17
Investigated participants perception of “normal” drinking patterns for their peers
Investigated participant’s expectations of alcohol consumption, e.g. will it heighten
their sexual experiences?
15 | P a g e

John Paul McLindon 200665371 SSM 1: Addiction Medicine: Alcohol Word Count: 2,828
Relevant age range (17‐19)
Results analysed by recognised statistical means and tabulated for data comparison.
In depth discussion drawing appropriate conclusions.
Numerous references.
weaknesses;
Non‐random selection for participation.
Voluntary participation may have biased against those with alcohol dependency or
those not willing to admit to drink problems
Tables and results sections difficult to interpret
Conclusions difficult to interpret due to use of jargon
Article 5
Strengths;
Published by a known agency of local PCT
Local population studied
Clear introduction explaining reasons for research
Clear and understandable methodology
Ethically approved
Participants chose at random
Relevant age range (15‐16)
Looks professional
Broad range of social factors investigated
Personal drinking values assessed
Investigated participants perception of “normal” drinking patterns for their peers
Easy to read results from the study in graphs, most of which include the questions
asked
Explanation of statistics displayed in the graphs
Recommendations page is helpful with understanding what can be done to help as a
conclusion
Numerous references
Weaknesses;
Participant number low (149)
Only 2 of 6 schools participated, may generate bias in results
Discussion
Both articles identify that the factors underlying problem drinking in young adults in both
the U.K and the U.S are multifactorial. As both studies were conducted across a diverse
16 | P a g e

John Paul McLindon 200665371 SSM 1: Addiction Medicine: Alcohol Word Count: 2,828
range of students and found that the results were largely consistent across the group it is
reasonable to suppose that the findings will translate to the young population as a whole.
The broad analysis of social norms and mediators which might trigger alcohol consumption
and problem drinking might be useful in planning strategies for prevention and support.
Both articles explore the theme of perceived normal drinking patterns in youth together
with an evaluation of potentially harmful drinking patterns. Furthermore both articles also
explore the reasons why the participants feel they have to drink. In both studies
participation was voluntary, though whether this is possible to achieve given that they were
administered within places of education, is difficult to assess. The age range in both studies
is similar though it is not possible to determine whether cultural and contextual differences
between the two countries will have an impact upon behaviours, even in the same age
groups, therefore skewing the results and making comparisons difficult. The U.S article
(article 3) has larger participant number which should in theory make the results more
reliable and representative than in the smaller cohort UK study. In addition, the US study
utilises a validated and standardised tool for their questionnaire. This should make data
comparison between other studies using the same tool easier. Statistical analysis of the
results in the US study also uses validated tools which again would facilitate comparison
with subsequent data collection or with other studies using the same tools. However, I
found navigation and interpretation in the results section to be difficult. The UK paper uses
a researcher designed online questionnaire which might well be fit for purpose in this study
but would make comparison with other studies more difficult. The results are presented as a
series of percentage bar histograms without further evaluation. However, they are very easy
to interpret and understand, clearly conveying the answers to each question.
Both articles cover a range of psychological and motivational factors which contribute to
drinking. They raise the importance of drinking to be liked, to fit in, engage socially with
friends and to be sociable. Peer pressure is acknowledged in both papers as an important
factor leading to drinking. Both papers also comment on the role of drinking in obtaining a
high, getting a buzz or to enhance confidence in social settings. Perhaps of greater concern
is the role of alcohol to help forget, cheer people up from depression or to help the drinker
from feeling left out. These might be considered the mindsets most likely to favour problem
drinking.
The UK paper offers worrying findings about complicity of adults with adolescent drinking.
Whilst it might be acceptable to drink safely at home with parents a significant number
reported that adults outside shops purchases alcohol for them. Considering that many then
consume the alcohol on the streets, in friends houses or other sites where there may be no
responsible adults this increases their risk from drinking. Other safety measures such as
whether the participant is accompanied and if they have other security measures like a
mobile telephone present whilst drinking are evaluated in the UK paper but are not covered
by Corbin R et al.
17 | P a g e

John Paul McLindon 200665371 SSM 1: Addiction Medicine: Alcohol Word Count: 2,828
One area that is questioned in article 5 that isn’t explored in article 3 is the influence of the
media and celebrities on the alcohol consumption of the young population. The participants
might see alcohol promoted in advertisements or as content in films and videos. When
asked whether they feel the media and celebrities portrayal of alcohol influences their own
consumption the majority responded that they “neither agreed nor disagreed”19 with the
comment. However a greater number of respondents felt that media and celebrities
influence increased their consumption than those who stated it had no effect on their
consumption.
The layout and language used in article 3 appears more academic than article 5. This is
consistent with the complicated way the results have been comprised into formatted tables
and analysed as mentioned above. Although the tables are comprehensive they aren’t easy
to interpret as the numbers in the table aren’t explained easily making it hard to draw a
conclusion. Also the explanation of the results contains considerable jargon and multiple
layers of statistical analysis make it difficult to understand. On the other the language
utilised in article 5 is typically simple, jargon free and therefore easy to understand.
Additionally, the results are laid out in a simple, consistent manner, well formatted and
straightforward to interpret.
Conclusion & Recommendations
Both articles have contributed to furthering my understanding of alcohol problems in a
youthful population. They both identify and I agree that further research needs to be
completed on the drinking behaviours and attitudes of the youth within the UK and the US.
This research might help to identify strategies for reducing levels of harmful drinking. Public
education programmes need to be considered that not only educate the youths themselves
but also those providing alcohol for the youths, parents, unknown adults and shop keepers.
Legislation may be of benefit, minimum pricing strategies and reduced drinking sales hours
or availability may help to reduce drinking patterns. Understanding the pressures that
motivate youths to drink might provide them with alternate strategies to employ in order to
avoid those pressures and situations which lead them to drinking. The positive effects of
such programmes will not only be upon health but many other social and criminal type
behaviours. This will have a net effect in cost saving for the country as a whole.
Whilst not an integral part of this systematic review, through my reading it is also clear to
me how limited the strategies are for interventions once harmful drinking patterns are
established. Prevention is clearly better than cure but for established drinkers we need a
greater range of more effective interventions and treatments to allow self determination of
normal drinking patterns or abstinence.
The Government needs to invest in effective Public Health strategies for harm reduction,
engaging with health providers, service users, voluntary agencies, the legal profession, the
drinks industry and the judicial system to promote safe drinking through a range of positive
18 | P a g e

John Paul McLindon 200665371 SSM 1: Addiction Medicine: Alcohol Word Count: 2,828
actions. Screening tools need to be employed to identify problems at an early stage and to
target specific interventions to those at risk of progressing to harmful drinking patterns. A
cohesive approach between all of these interested parties should facilitate change and
improvement for a more positive approach to drinking in society.
The three main conclusions are;
1. The need for more UK based research into the attitudes and behaviours of the young
population in regards to alcohol consumption
2. The need to explore in detail what influences the consumption of alcohol youth
3. To provide greater education to society about alcohol & it’s effects
19 | P a g e

John Paul McLindon 200665371 SSM 1: Addiction Medicine: Alcohol Word Count: 2,828
References.
1. http://www.google.co.uk/imgres?imgurl=http://assets.nydailynews.com/img/2009/0
7/12/alg_teen_alcohol.jpg&imgrefurl=http://www.nydailynews.com/lifestyle/health/
2009/07/11/2009‐07‐
11_teen_drinking_linked_to_depression_anxiety_particularly_among_girls_study.htm
l&usg=__aQLcBgr60SVhTDhwuEt_D98LV‐
M=&h=291&w=450&sz=78&hl=en&start=0&zoom=1&tbnid=8BzA0FNaxyilvM:&tbnh=1
28&tbnw=186&ei=Z51GTcPpEYuYhQeUssSxAQ&prev=/images%3Fq%3Dteenage%2Ba
ddiction%2Bto%2Balcohol%26hl%3Den%26biw%3D1362%26bih%3D553%26gbv%3D2
%26tbs%3Disch:1&itbs=1&iact=hc&vpx=891&vpy=79&dur=140&hovh=180&hovw=279
&tx=166&ty=80&oei=Z51GTcPpEYuYhQeUssSxAQ&esq=1&page=1&ndsp=23&ved=1t:4
29,r:5,s:0 , date accessed [31/01/2011]
2. Howard. A. http://www.finestquotes.com/select_quote‐category‐Drinking‐page‐
0.htm. Accessed [31/01/2011]
3. General Medical Council: Duties of a Doctor. http://www.gmc‐
uk.org/guidance/good_medical_practice/duties_of_a_doctor.asp. Accessed
[31/01/2011]
4. Gillon R. Medical Ethics: four principles plus attention to scope. British Medical Journal.
16th July 1994; 309 : 184. Available from
http://www.bmj.com/content/309/6948/184.full?ijkey=a3ed9f8cb3df8f310bec00940e1
d889524f6ba98&keytype2=tf_ipsecsha. Accessed 01/02/2011
5. World Health Organisation website. http://www.who.int/about/en/. Accessed
30/02/2011
6. Direct Government Website. Human Rights. Human Rights Act 1998. Available from
http://www.direct.gov.uk/en/Governmentcitizensandrights/Yourrightsandresponsibilitie
s/DG_4002951. date accessed 08/02/2011
7. Patient UK website. Document ID: 2339. Document Version: 21. Document Reference:
bgp2412. Last Updated: 16 Jun 2009. Planned Review: 16 Jun 2011.
http://www.patient.co.uk/doctor/Inverse‐Care‐Law‐and‐Distributive‐Justice.htm.
Accessed 03/02/2011
8. House of Commons Health Committee. Health Inequalities, Third Report of Session
2008‐09. Volume 1. Printed 26th February 2009. Published 15th March 2009. Page 11.
Accessed 03/02/2011. Available from
http://www.publications.parliament.uk/pa/cm200809/cmselect/cmhealth/286/286.pdf
9. The Free Online Dictionary; definition of harm reduction. Accessed 06/02/2011.
Available http://encyclopedia.thefreedictionary.com/Harm+Reduction
10. The Free Online Dictionary; definition of poly drug use. Accessed 06/02/2011. Available
http://encyclopedia.thefreedictionary.com/polydrug+use
20 | P a g e

John Paul McLindon 200665371 SSM 1: Addiction Medicine: Alcohol Word Count: 2,828
11. Parliamentary office of science and technology. Binge Drinking and Public Health.
Published July 2005. Number 244.
http://www.parliament.uk/documents/post/postpn244.pdf
12. Lightowlers C, Morleo M, Cook P A. The impact of alcohol quarterly report. Centre for
Public Health: Liverpool John Moore University. February 2008. Pages 4‐9. Available
from http://www.cph.org.uk/showPublication.aspx?pubid=362. Accessed 30/02/2011
13. The Free Online Dictionary; definition of detoxification. Accessed 06/02/2011. Available
http://encyclopedia.thefreedictionary.com/detoxification
14. The Free Online Dictionary; definition of abstinence. Accessed 06/02/2011. Available
http://encyclopedia.thefreedictionary.com/abstinence
15. The Free Online Dictionary; definition of rehabilitation. Accessed 06/02/2011. Available
http://encyclopedia.thefreedictionary.com/Drug+rehabilitation
16. Moriarty K J, Cassidy P, Dalton D, Farrell M, Owens L, Gilmore I, et al. Meeting the
challenge of improved quality care and better use of resources. British Society of
Gastroenterology. Accessed 04/02/2011
17. Cranford J A, Zucker R A, Jester J M, Puttler L I, Fitzgerald H E. Parental alcohol
involvement & adolescent alcohol expectancies predict alcohol in male adolescents.
Psychology of Addictive Behaviours. 21/09/2009. Volume 24. Issue 3. Pages 386‐396.
06/02/2011
18. Chartier K G, Hesselbrock M N, Hesselbrock V M. Alcohol problems in young adults
transitioning from adolescence to adulthood: The association with race & gender.
Addictive Behaviours. March 2011. Volume 36. Issue 3. Pages 167‐174. 06/02/2011
19. Corbin W R, Iwamoto D K, Fromme K. Broad social motives, alcohol use, and related
problems: mechanisms of risk from high school through college. Addictive Behaviours.
March 2011. Volume 36. Issue 3. Pages 222‐230. 06/02/2011
20. Clark H K, Ringwalt C L, Shamblen S R. Predicting adolescent substance use: The effects
of depressed mood and positive expectancies. Addictive Behaviours. 11/01/2011.
06/02/2011
21. Lightowlers C, Morleo M, Harkins C. Understanding young people’s alcohol‐related social
norms in Sefton‐Interim Report. Centre for Public Health. April 2099. Accessed
December 2009.
22. Department for Children, Schools & Families, The Home Office, The Department of
Health. Youth Alcohol Action Plan. June 2008. Accessed December 2009.
Best References
The three best/most useful references were;
1. The Free Online Dictionary. http://encyclopedia.thefreedictionary.com. This was
useful as it described all my definitions in detail allowing me to fully understand them
and it was also very easy to use.
21 | P a g e

John Paul McLindon 200665371 SSM 1: Addiction Medicine: Alcohol Word Count: 2,828
2. Lightowlers C, Morleo M, Harkins C. Understanding young people’s alcohol‐related
social norms in Sefton‐Interim Report. Centre for Public Health. April 2099.
06/02/2011. This was very useful reference as it was one of the articles I used to
analyse
3. Corbin W R, Iwamoto D K, Fromme K. Broad social motives, alcohol use, and related
problems: mechanisms of risk from high school through college. Addictive
Behaviours. March 2011. Volume 36. Issue 3. Pages 222‐230. 06/02/2011. This was
the other paper used and therefore also extremely helpful.
22 | P a g e

John Paul McLindon 200665371 SSM 1: Addiction Medicine: Alcohol Word Count: 2,828
Reflection
23 | P a g e
The past three weeks whilst being on SSM timetabled period has been a great learning curve for
me. I have learnt how to search for scientific research that will explain and display statistics on a
subject area of interest. In addition to this I learnt how to critically appraise the materials that I
found to decide whether or not they were reliable enough to use and how to extract the key pieces
of information.
The research also gave me a great insight into the scale of the alcohol problem not just within the
UK but globally too. These was extremely interesting to me as I am only twenty years old and
therefore have just left the age bracket at which the documentation I researched was aimed at.
This allowed me to relate too many of the psychological stresses that have forced the participants
to drink alcohol, not only in such a high frequency and quantity but also at such a delicate age. The
mean age of one of the articles for the first ever drinking experience was 11.68 years old a whole
six years below the legal drinking limit which was staggering.
Even more shocking to me was the fact the participants parents not only knew they were drinking
under age but were also supplying them with alcohol. This would of never happened in my past
and so it was interesting to discover how the upbringings of different children vary with what is
acceptable and not.
The most exciting experience I gained during this three week period was the opportunity to have
clinical placement for a week at Aintree Hospital with the Alcohol Specialist Nurse; Sarah Haywood.
Sarah was a very well informed, exemplary health care professional that was thought of highly by
all her colleagues and patients alike. She treated her patients with a great deal of respect and
displayed no prejudice opinions towards her patients, which was reflected well in her patient’s
recovery process. Sarah spent the bulk of her time teaching me and my fellow student Jill
Richardson. She informed us not only about her role in the health care system but also about all
the science and psychosocial information about alcohol and the people who suffer from alcohol
addiction.
She arranged many things for us to see while we were on placement ranging from sitting in on her
alcohol detoxification clinic in which patients who are suffering with addiction to alcohol attend as
an outpatient to gain help and advice into how to break the habits which are causing adverse
health problems to them, to watching nurse practitioners perform a colonoscopy scope lists. I also
witnessed a consultant urologist perform a cystectomy. We also visited patients that had been
admitted onto a gastroenterology ward where I had the opportunity to talk to and take histories
from several patients. This experience was further in the A&E department and Medical Assessment
Unit where the more acute cases of alcohol had been admitted.
All these opportunities have emphasised to me the work and care that consummate health care
professionals provide on a daily basis and I would like to take this opportunity to display my sincere
gratitude to all of those who made my placement not only educational but enjoyable too.

John Paul McLindon 200665371 SSM 1: Addiction Medicine: Alcohol Word Count: 2,828
Appendix
1.
Appendix 1
3
Make the care of your patient your first concern
Protect and promote the health of patients and the public
Provide a good standard of practice and care
o Keep your professional knowledge and skills up to date
o Recognise and work within the limits of your competence
o Work with colleagues in the ways that best serve patients'
interests
Treat patients as individuals and respect their dignity
o Treat patients politely and considerately
o Respect patients' right to confidentiality
Work in partnership with patients
o Listen to patients and respond to their concerns and preferences
o Give patients the information they want or need in a way they
can understand
o Respect patients' right to reach decisions with you about their
treatment and care
o Support patients in caring for themselves to improve and
maintain their health
Be honest and open and act with integrity
o Act without delay if you have good reason to believe that you or
a colleague may be putting patients at risk
o Never discriminate unfairly against patients or colleagues
o Never abuse your patients' trust in you or the public's trust in
the profession.
You are personally accountable for your professional practice and must always
be prepared to justify your decisions and actions.
24 | P a g e

John Paul McLindon 200665371 SSM 1: Addiction Medicine: Alcohol Word Count: 2,828
2. Human Rights Act 1998 found on the Direct Government website,
http://www.direct.gov.uk/en/Governmentcitizensandrights/Yourrightsandresponsibi
lities/DG_4002951 , date accessed; 03/02/2011;
a. the right to life
b. freedom from torture and degrading treatment
c. freedom from slavery and forced labour
d. the right to liberty
e. the right to a fair trial
f. the right not to be punished for something that wasn't a crime when you did it
g. the right to respect for private and family life
h. freedom of thought, conscience and religion, and freedom to express your beliefs
i. freedom of expression
j. freedom of assembly and association
k. the right to marry and to start a family
l. the right not to be discriminated against in respect of these rights and freedoms
m. the right to peaceful enjoyment of your property
n. the right to an education
o. the right to participate in free elections
p. the right not to be subjected to the death penalty
3. The Poverty Site, http://www.poverty.org.uk/summary/social%20exclusion.shtml,
date accessed 03/02/2011
Absolute poverty refers to a set standard which is the same in all countries and which does not change over time. An income‐related example would be living on less than $X per day.
Relative poverty refers to a standard which is defined in terms of the society in which an individual lives and which therefore differs between countries and over time. An income‐related example would be living on less than X% of average UK income.
Absolute poverty and relative poverty are both valid concepts. The concept of absolute poverty is that there are minimum standards below which no one anywhere in the world should ever fall. The concept of relative poverty is that, in a rich country such as the UK, there are higher minimum standards below which no one should fall, and that these standards should rise if and as the country becomes richer.
One of the advantages of the term 'social exclusion' is that it is reasonably self‐explanatory, clearly relating to the alienation or disenfranchisement of certain people within society
25 | P a g e

John Paul McLindon 200665371 SSM 1: Addiction Medicine: Alcohol Word Count: 2,828
4.
26 | P a g e

John Paul McLindon 200665371 SSM 1: Addiction Medicine: Alcohol Word Count: 2,828
5.
27 | P a g e
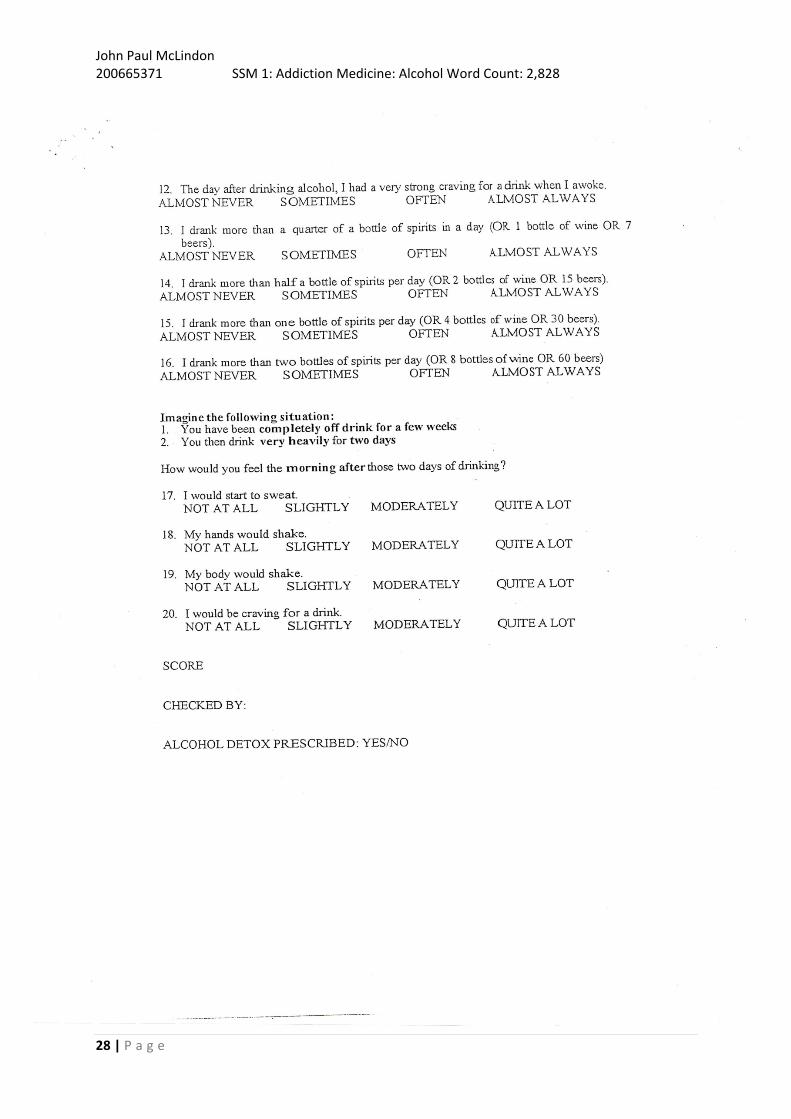
John Paul McLindon 200665371 SSM 1: Addiction Medicine: Alcohol Word Count: 2,828
28 | P a g e

John Paul McLindon 200665371 SSM 1: Addiction Medicine: Alcohol Word Count: 2,828
29 | P a g e

John Paul McLindon 200665371 SSM 1: Addiction Medicine: Alcohol Word Count: 2,828
6.
30 | P a g e

John Paul McLindon 200665371 SSM 1: Addiction Medicine: Alcohol Word Count: 2,828
7. RUTGERS ALCOHOL PROBLEM INDEX
RAPI (23‐item version) Different things happen to people while they are drinking ALCOHOL or because of their ALCOHOL drinking. Several of these things are listed below. Indicate how many times each of these things happened to you WITHIN THE LAST YEAR. Use the following code: 0 = None 1 = 1‐2 times 2 = 3‐5 times 3 = More than 5 times HOW MANY TIMES HAS THIS HAPPENED TO YOU WHILE YOU WERE DRINKING OR BECAUSE OF YOUR DRINKING DURING THE LAST YEAR?
0 1 2 3
Not able to do your homework or study for a test
Got into fights with other people (friends, relatives, strangers)
Missed out on other things because you spent too much money on alcohol
Went to work or school high or drunk
Caused shame or embarrassment to someone
Neglected your responsibilities
Relatives avoided you
Felt that you needed more alcohol than you used to in order to get the same effect
Tried to control your drinking (tried to drink only at certain times of the day or in certain places, that is, tried to change your pattern of drinking)
Had withdrawal symptoms, that is, felt sick because you stopped or cut down on drinking
Noticed a change in your personality
Felt that you had a problem with alcohol
Missed a day (or part of a day) of school or work
Wanted to stop drinking but couldn't
Suddenly found yourself in a place that you could not remember getting to
Passed out or fainted suddenly
Had a fight, argument or bad feeling with a friend
Had a fight, argument or bad feeling with a family member
Kept drinking when you promised yourself not to
Felt you were going crazy
Had a bad time
Felt physically or psychologically dependent on alcohol
Was told by a friend, neighbour or relative to stop or cut down drinking
31 | P a g e

John Paul McLindon 200665371 SSM 1: Addiction Medicine: Alcohol Word Count: 2,828
8.
Case Histories
Patient A (25/01/2011);
Patient A was an inpatient on the gastroenterology ward at Aintree Hospital. He was towards the end
of his inpatient detoxification plan and soon to be discharged with a scheduled outpatient
appointment to follow in a few days time. On general inspection Patient A was slightly jaundice, had
black dried blood covering his lips and he was slightly confused and a little dazed.
The reason Patient A was admitted to hospital was for his persistent vomiting of black blood for
roughly four days but more importantly whilst out shopping he was found collapsed in the street by
police officers. The reason for his persistent haematemisis could be to do with the fact he drank 2 litres
of vodka everyday and has done for approximately ten years. However he stated that since is previous
admission he had cut is intake down to 1 litre of vodka a day.
He has been in and out of hospital and other rehab clinics on numerous occasions including visits to
the Windsor Clinic. On one of the previous admissions, four years ago, he was diagnosed with Diabetes
after losing 4stone of weight. He says he is normally fit and healthy and swims on a regular basis
however has a poor appetite; however had an MRI scan back in November 2010.
From the tests done on his current and previous admissions Patient A had been diagnosed with a
cirrhotic liver which was a main concern for him.
Patient B (25/01/2011);
Sarah Haywood was asked to visit a gentleman that was in the A&E department at Aintree Hospital. He
had been brought in by ambulance at roughly 9 o’clock that morning. The emergency services were
called when Patient B, a polish man in his late twenties, had collapsed at work and began to seize. It
was apparent that Patient B couldn’t remember any of the accident happening. In addition to this the
case history taken from Patient B was a great challenge as he didn’t speak any English; however his
brother who was with him spoke a little.
Asking Patient B to tell us some of his medical and social history it was discovered that his last drink
was on the 24/01/2011 on which he had drunk a bottle of red wine and a 2 litre bottle of vodka. He
said this was a change from normal as his preferred drinks are beer and vodka. He is a long term
diabetic and takes insulin regularly. He also didn’t appear jaundice or confused, other than not
remembering the accident, but he had quite a severe tremor. Patient B has previously had an
operation on his stomach although what type and the reasons for this operation weren’t discovered.
He used to be a heavy smoker but has never taken recreational drugs.
Sarah Haywood advised Patient B to carry on his drinking decreasing the intake amount as a sudden
stop in alcohol intake can cause seizures which could be fatal. Sarah designed a drinking table for
Patient B where his intake decreased everyday over two weeks until inside recommended limits.
32 | P a g e

John Paul McLindon 200665371 SSM 1: Addiction Medicine: Alcohol Word Count: 2,828
Contact List
1. Sarah Haywood, Alcohol Specialist Nurse, Aintree Hospital
2. Addaction Croxteth Project, 83‐93 Stonebridge Lane, Croxteth, Liverpool, L11 4SJ, 0151 5461411
3. Addaction (Central Office), 67‐69 Cowcross Street, London, EC1M 6PU, Tel. 020 7251 5860, Fax. 020 7251 5890, Email: [email protected]
4. Kieran Lamb, Librarian, Fade Library, Regatta Place, Summers Road, Brunswick
Business Park, Liverpool, L3 4BL, 0151 2854493
5. Alcoholics Anonymous, PO Box 1, 10 Toft Green, York YO1 7ND, Tel. 01904 644026, [email protected]
6. SMASH Team (North Sefton), Southport Community Drugs Team, 8 Church Street, Southport, PR9 0QT, 01704 534759
7. SMASH Team (South Sefton), Sefton Careers Centre 2nd Floor, 27‐37 South Road, Waterloo, L22 5RF, 0151 949 4470
8. Windsor Clinic, 0151 473 0303 ‐ for all general inquiries (Switchboard including Trust Offices and Ashworth Hospital), 0151 250 3000 ‐ Rathbone Hospital Switchboard (including Mossley Hill Hospital and Liverpool Services), 01704 383600 ‐ Hesketh Centre, Southport (including North Sefton Services)
9. British Liver Trust, 0800 6527330, www.britishlivertruts.org.uk 10. Alcoholics Anonymous, www.al‐anonuk.org.uk
Timetable
Monday Tuesday Wednesday Thursday Friday
Week 1 Placement Placement Placement Placement Research
Week 2 Research Placement Research SSM Journal Club
Week 3 SSM SSM SSM SSM
33 | P a g e

John Paul McLindon 200665371 SSM 1: Addiction Medicine: Alcohol Word Count: 2,828
34 | P a g e
Background
• 90% of 15yr olds admit they drink!
• UK has 2nd highest BD rate in Europe.
• ¼ of men & 10% of women BD regularly.
• BD in young women doubled in last 10yrs.
• Death from intoxication doubled in 20yrs.
• >¼ of all alcohol related deaths occur when
intoxicated.
• Peak prevalence of BD is in 16‐24 yr olds.
Understanding young people’salcohol‐related social norms in
Sefton – Interim Report
Lightowlers C, Morleo M, Harkins C; Centre for Public Health. April 2009
John Paul McLindon
1stYear Medical Student at the University of Liverpool
30/20/2011
Why This Article?
• Explores the statistics of alcohol binge drinking in local area
• It focus’ on reasons as to why teenagers drink and who with not just what/how much they drink
• Study looks at; drink behaviour, sources of alcohol, safety precautions, drinking motives, frequency & consequences
Discussion
• Most drinking was done in places surrounded by peers/family
• Majority of alcohol was given/bought by
adults for teenagers, mainly by family
• Main reasons for drinking are to celebrate at parties
• Low % of pupils results show parents drinking daily, high % showed mates drinking weekly
Criticisms
• Sample size is only 149 participants
• Only initial set of results, follow up results are to be published at a later date so no comparison of intervention
• Answers on questionnaires aren’t greatly specific so specificity of results decreases
Take Home Messages
• Mean age of first alcohol consumption was 11.68 years
• Peer pressure not main reason for drinking, but pleasure and to make an event more enjoyable, 1/3 drank to forget worries
• Alcohol availability made easy by family & strangers buying for the underage teenagers
THE END
Journal Club Presentation