17:15 serra - bvs in cto pci
TRANSCRIPT

The role of BVS in CTO PCI : Mid-term Clinical Outcomes with
Multi-imaging Techniques.Antonio Serra M.D.

Is one of the most challenging scenarios to test, due to long fibrocalcified lesions with high plaque burden 1, 2
In this setting is where “vessel reparation” might be most needed.
Avoid a “full metal jacked”, precluding future CABG
Rationale: BVS in CTOs
1.- Rubartelli A , et al. Eur Heart J 20102.- Galassi AR, et al. EuroIntervention 2011

Objectives CTO-ABSORB pilot study is a prospective,
observational, single-center registry designed to :
Assess the safety and performance of the Absorb everolimus-eluting scaffold BVS, in unselected consecutive patients undergoing PCI for CTO, under guidance of imaging techniques
To provide preliminary observations and generate hypotheses for future studies with large proportion of patients.

ObjectivesAll comers registry with few exclusion criteria :
- Patient or refering physician refusal- Extremely calcified lesions + tortuosity- True Bifurcated lesions with SB > 2.5 mm- Reference vessel diameter < 2.5 mm or < 4.5 mm (out of the Absorb measures)- Complications treated with metallic stents

MethodsWire Crossing
1st dilatation small balloon 1.5- 2.0mm
NTG 400 mcgr
IVUS analysis
Further dil. with NC /Cutting/ Rota + cutting
IVUS analysis
BVS implantation
OCT analysis
Further dil with NC if needed
Renal function & CK, US Troponin- Pre & 6, 12 & 24 hours post-PCI

Follow-up
Clinical FU by Phone Call: 1 month
Angio FU & OCT: 12 months
Clinical Visit & MSCT: 18 months
Clinical Visit & MSCT/MRI: 6-8 month
Clinical FU by Phone Call: 24 months, 3, 4 and 5 years

67 succeed CTOs (2013-2014)
49 clinical eligible CTOs
38 Absorb CTO cases
35 Absorb CTO cases
7 patients excluded:Patient or referent physician refuse
6 patients excluded:Live CTO courses with other DES
5 patients excluded:Old patients with comorbilities
Clinical criteria (n=18)
5 patients excluded:Angio Calcium + tortuosity
4 patients excluded:True bifurcated lesions + SB ≥ 2.5mm
2 patients excluded:Reference vessel diameter < 2.5 (n=1)
or ≥ 4mm (n=1)
Angiographic criteria (n=11)
Bail-out stent (DES) used (n=3)
(1) Coronary perforation after balloon: stent graft
(1) Aorto-ostial disection after rotational atheretomy: 4mm DES(1) Distal coronary disection after
BVS: 2.25mm DES
28.5% of clinical eligible CTOs were excluded due to predefined-angio criteria or PCI related complications
Study Profile

Pre-procedure
RCA CTO. J- CTO Score Complexity 2
1
14
4 3
3
2
2
IVUS pre- BVS implantation
Side branch
Cutting balloon pre-
dilatation
After wiring & pre-dilatation
21mm

3.0 x 28mm3.5 x 28mm3.5 x 28mm
2.25 x20 mm
Drug-
coated Balloon
3 overlapped BVS Absorb 3.0 x 28; 3.5 x 28 & 3.5 x 28 mm (84 mm length)+ drug-eluting balloon 2.25 x 20 mm in LPD
Post-BVS implantation

Final OCT1.
1.2*.
2*.
3.
3.4*.
4*.5.
5.
OCT post-BVS implantation
After NC balloon post-dilatation

LAO 30º/ CRAN 12º
6-months MSCT FU 12-months Angio FU
* **
*
1.
1.
2.2.
3*.
3*.4*.
4*.
5.
5.
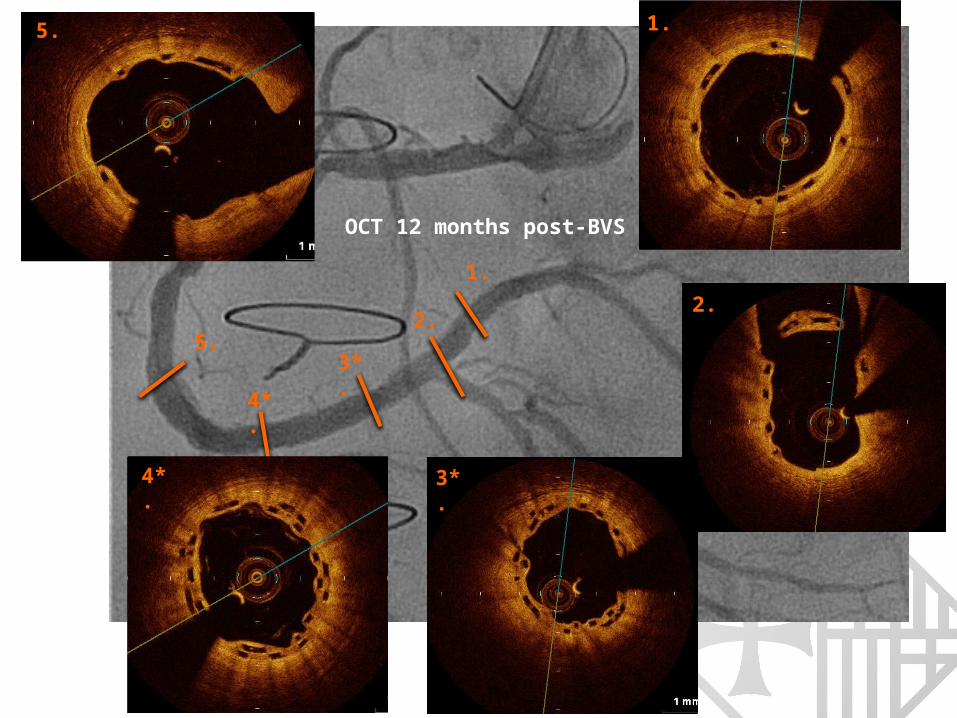
OCT 12 months post-BVS

Results

• Age (years) (mean±SD) 60.7 + 9.7• Male gender 80.0 (28)Risk Factors Diabetes 20.0 (7) Hypertension 60.0 (21) Dyslipidemia 74.3 (26) Current Smoker 20.0 (7)
Clinical Presentation Silent ischemia/Stable angina 85.7 (5/25)
• Baseline cMRI 48.6 (17)• Baseline MSCT 88.0 (31)• LVEF (≤ 50%) 22.9 (8)• 3 vessel disease 25.0 (5)
Unless specified otherwise, values are % and (n) of patients
Clinical Characteristics (n=35)
History of Myocardial Infarction 28.6 (10) PCI 37.1 (13)

Unless specified otherwise, values are % and (n) of patients
Target Vessel:- RCA 45.7% (16)- LAD 40.0% (14)- LCx/Marginal Branch 11.4% (4)
CTO location:- Ostial/proximal 28.6% (10)- Mid 65.7% (23)
CTO involving bifurcated lesion 20.0% (7)
In-stent restenosis (Class IV) 5.7% (2)
Lesion Characteristics (n=35)

CTO angiographic characteristics• Blunt stump type* 40.0 (14)• Severe Tortuosity (Bending)* 11.4 (4)• Significant Calcification* 34.3 (12)• Previously Failed Lesion* 8.6 (3)• Occlusion length ≥ 20mm* 31.4 (11)
CTO complexity (J-CTO Score)
• Easy (score of 0) 25.6 (9)• Intermediate (score of 1) 48.6 (17)• Difficult (score of 2) 8.6 (3)• Very difficult (score of ≥3) 17.2 (6)
• Occlusion length (mm) 18.6 + 12.5• Target Lesion length (mm) 35.9 + 15.8
Unless specified otherwise, values are % and (n) of patients
CTO complexity (n=35)

• Radial or bi-radial approach 60.0 (21)
• 6- Sheath Size 51.4 (18)
• Antegrade Strategy 85.7 (30)
• Number of GW used per lesion 1.8 + 1.1
• Number of pre-dilatation balloons used per lesion 2.6 + 0.97
• Plaque modification: Cutting balloon pre-dilatation 71.4 (25)
Rotational Aterecthomy 8.6 (3)
• Number of scaffolds used per lesion 2.2 + 0.89
• Total scaffold lenght implanted per lesion, mm 52.5 + 22.9
• Post-dilatation (0.5mm bigger NC balloon / scaffold) 62.9 (22)
Unless specified otherwise, values are % and (n) of patients
Procedural Characteristics (n=35)

Immediate Results (n=35)
• Total number of visible analyzed SBs covered by BVS(n) 109 Mean number/lesion 3.2 1.4 SB < 0.5mm 41.3 (45) SB ≥ 0.5mm 58.7 (64)
• Post-BVS SBO 6.4 (7) SB < 0.5mm 3.7 (4) SB ≥ 0.5mm 2.7 (3)
• All scaffolds were successfully delivery and deployed• Side Branch Occlusion (SBO)6: as a reduction in TIMI flow to grade 0 or 1.
Accordingly, side branches with pre-BVS implantation TIMI flow grade 0 or 1, were excluded
6.- Muramatsu T, et al. JACC Cardiovasc Interv. 2013
• Dissection before BVS was observed in (4/7) 57% of all SBO cases (100% of SBO with bigger SB ≥ 0.5mm)

• Contrast-induced nephropathy 0 (0)
• Peri-PCI Myocardial damage (only markers) 8.6 (3/30)
• Peri-PCI Myocardial infarction 0 (0)
• Vascular access site complication 2.8 (1)
7.- Kristian Thygesen K, et al. Eur Heart J 2012
In-Hospital Results (n=35)Peri-PCI myocardial damage: CPK ≥3 times the upper limit of normal (ULN) & US troponin ≥5 times ULN. In case of symptoms and/or electrocardiogram changes suggesting MI, was defined as Myocardial infarction7
A procedure-related contrast-induced nephropathy (CIN) was defined as an increase of 25% or 0.5 mg/dl in serum creatinine at 24-48 hours after PCI comparing baseline values8
8.- Mehran R, et al. J Am Coll Cardiol 2004
Blood test was performed pre and 6, 12, 24h post-PCI

1-month FU (n=35) 6-months FU (n=35)
Overall Death 0 0
Cardiac 0 0
MI 0 0
TLR 0 0
MACE 0 0
BVS Thrombosis* 0 0
In-scaffold re-occlusion** (2) 5.7%
ARC definition*
Results (n=35)
MSCT** (100% FU completed)

Pre-PCI Post-PCI
6 mo MSCT6 mo MSCT

1.1.2.
2.
3.
4.
4.3.
12 months OCT

Conclusions
We reported excellent mid-term patency and safety by 6-8 months clinical and MSCT follow-up
The ABSORB-CTO pilot study demonstrated the safety and feasibility of PCI of CTO lesions with the fully bioresorbable Absorb® BVS, under imaging guidance techniques.
Further clinical and imaging follow-up at future time points is required to extend the significance of the current findings.