1725077 374
TRANSCRIPT
GENITOURINARY CANCERS (DP PETRYLAK AND JW KIM, SECTION EDITORS)
Improving Systemic Chemotherapy for Bladder Cancer
Tracy L. Rose1 & Matthew I. Milowsky2
# Springer Science+Business Media New York 2016
Abstract Systemic chemotherapy is integral to the manage-ment of muscle-invasive and metastatic bladder cancer (BCa).Neoadjuvant chemotherapy has been increasingly utilized formuscle-invasive BCa over the past several years, and severaloptions for cisplatin-based regimens have emerged. Adjuvantchemotherapy may be considered for select patients who didnot receive neoadjuvant therapy. Systemic chemotherapyadded to radiotherapy is a critical component of a bladder-preserving approach and superior to radiotherapy alone.Cisplatin-based chemotherapy has been the mainstay for met-astatic BCa for more than three decades. Novel targeted agentsare in development fueled by the recent molecular character-ization of BCa. Recent trials of immunotherapy have demon-strated the possibility of a less toxic and potentially moreeffective treatment for metastatic disease. It is an extremelyexciting time for BCa research, and much needed improve-ments in systemic treatment are most certainly on the horizon.
Keywords Bladder cancer . Transitional cell carcinoma .
Urothelial carcinoma . Chemotherapy . Biologic agents .
Targeted agents . Neoadjuvant therapy . Adjuvant therapy .
Trimodality therapy . Immunotherapy .Molecular biology .
Prognostic factors . Personalized therapy
Introduction
Bladder cancer (BCa) is the sixth most common cancer in theUSA with an estimated 74,000 new cases and 16,000 deathsfor 2015 [1]. Although the majority of patients present withnon-invasive disease, 10–20% of these cases eventually prog-ress to muscle-invasive disease. In addition, nearly 30 % ofnew cases have muscle invasion at the time of diagnosis [2].Muscle invasion is associated with a high risk of death fromdistant metastases with level 1 evidence supporting the incor-poration of systemic chemotherapy into treatment.Chemotherapy is also the cornerstone of treatment forunresectable and metastatic disease. This article reviews theuse of perioperative chemotherapy in muscle-invasive dis-ease, the importance of systemic chemotherapy in atrimodality bladder preservation approach, and the use of che-motherapy in advanced and metastatic BCa. This is followedby a discussion of the recent exciting developments in molec-ularly targeted treatments and immunotherapeutic approaches.
Perioperative Chemotherapy for Muscle-InvasiveBladder Cancer
Neoadjuvant Chemotherapy
The standard of care for muscle-invasive bladder cancer(MIBC) is radical cystectomy with pelvic lymphadenectomy.
This article is part of the Topical Collection on Genitourinary Cancers
* Matthew I. [email protected]
Tracy L. [email protected]
1 Division of Hematology/Oncology, Department of Medicine,University of North Carolina Lineberger Comprehensive CancerCenter, 170 Manning Drive, CB #7305, 27599 Chapel Hill, NC,USA
2 Division of Hematology/Oncology, Department of Medicine,University of North Carolina Lineberger Comprehensive CancerCenter, 170 Manning Drive, CB #7295, 27599 Chapel Hill, NC,USA
Curr Oncol Rep (2016) 18:27 DOI 10.1007/s11912-016-0512-2
In the last decade, the addition of neoadjuvant chemotherapy(NAC) has also become standard, based on two randomizedcontrolled trials and a meta-analysis [3–5]. NAC is recom-mended due to the observed improvement in survivalwith its use, and pathologic response rate has emergedas an endpoint for neoadjuvant clinical trials becausepathologic stage at the time of cystectomy correlateswith overall survival (OS) [3, 4].
The Southwest Oncology Group (SWOG) Trial 8710 ran-domized 317 patients with MIBC to neoadjuvant methotrex-ate, vinblastine, doxorubicin, and cisplatin (MVAC) pluscystectomy versus cystectomy alone. Median survival in theNAC arm was 77 months compared to 46 months in thesurgery-alone arm (p=0.06) [3]. The BA06/EORTC 30894trial compared 3 cycles of neoadjuvant cisplatin, methotrex-ate, and vinblastine (CMV) with no chemotherapy prior tocystectomy or full-dose external beam radiotherapy in patientswith MIBC. The NAC group had a 5.5 % benefit in 3-yearsurvival compared to the group that did not receive chemo-therapy (p=0.075), with a 6.5-month improvement in OS [6].Long-term follow-up confirmed a significant improvement insurvival, demonstrating a 16 % reduction in risk of death at10 years in the NAC arm (p=0.04) [7]. A 2005 meta-analysisincluded 11 trials with 3005 total patients and demonstrated a5 % improvement in 5-year survival (p=0.003) [8]. Thesedata have solidified cisplatin-based NAC as standard of carein patients with MIBC.
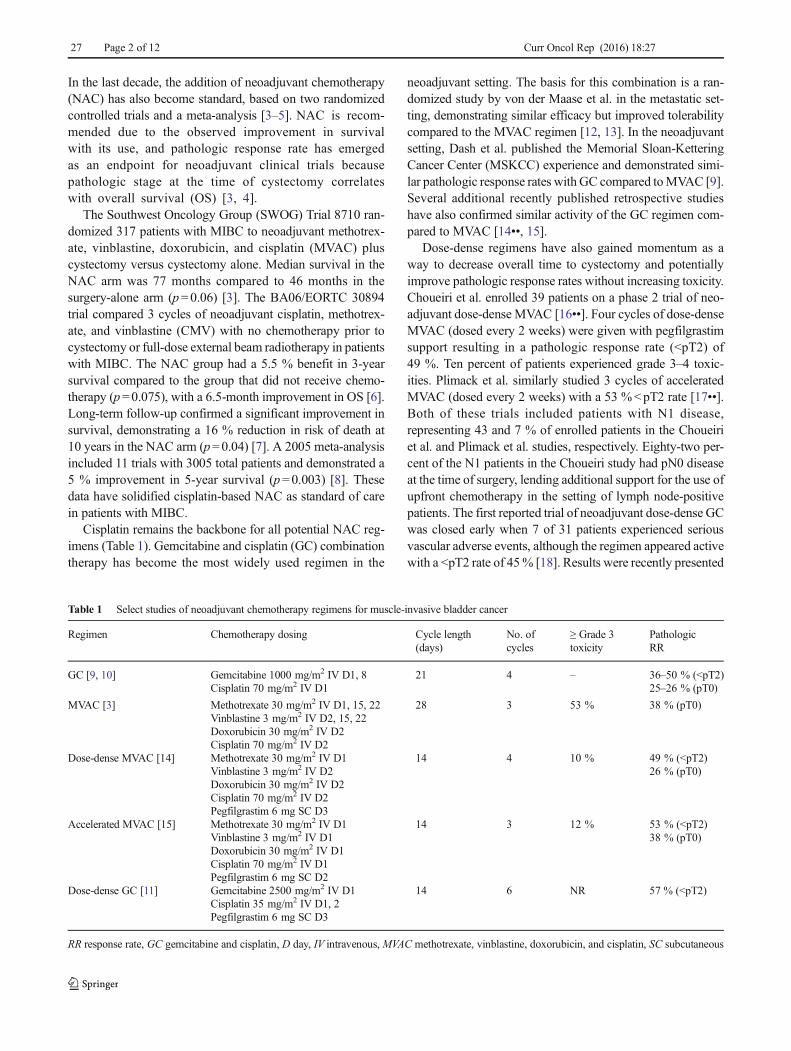
Cisplatin remains the backbone for all potential NAC reg-imens (Table 1). Gemcitabine and cisplatin (GC) combinationtherapy has become the most widely used regimen in the
neoadjuvant setting. The basis for this combination is a ran-domized study by von der Maase et al. in the metastatic set-ting, demonstrating similar efficacy but improved tolerabilitycompared to the MVAC regimen [12, 13]. In the neoadjuvantsetting, Dash et al. published the Memorial Sloan-KetteringCancer Center (MSKCC) experience and demonstrated simi-lar pathologic response rates withGC compared toMVAC [9].Several additional recently published retrospective studieshave also confirmed similar activity of the GC regimen com-pared to MVAC [14••, 15].
Dose-dense regimens have also gained momentum as away to decrease overall time to cystectomy and potentiallyimprove pathologic response rates without increasing toxicity.Choueiri et al. enrolled 39 patients on a phase 2 trial of neo-adjuvant dose-dense MVAC [16••]. Four cycles of dose-denseMVAC (dosed every 2 weeks) were given with pegfilgrastimsupport resulting in a pathologic response rate (<pT2) of49 %. Ten percent of patients experienced grade 3–4 toxic-ities. Plimack et al. similarly studied 3 cycles of acceleratedMVAC (dosed every 2 weeks) with a 53 %<pT2 rate [17••].Both of these trials included patients with N1 disease,representing 43 and 7 % of enrolled patients in the Choueiriet al. and Plimack et al. studies, respectively. Eighty-two per-cent of the N1 patients in the Choueiri study had pN0 diseaseat the time of surgery, lending additional support for the use ofupfront chemotherapy in the setting of lymph node-positivepatients. The first reported trial of neoadjuvant dose-dense GCwas closed early when 7 of 31 patients experienced seriousvascular adverse events, although the regimen appeared activewith a <pT2 rate of 45% [18]. Results were recently presented
Table 1 Select studies of neoadjuvant chemotherapy regimens for muscle-invasive bladder cancer
Regimen Chemotherapy dosing Cycle length(days)
No. ofcycles
≥ Grade 3toxicity
PathologicRR
GC [9, 10] Gemcitabine 1000 mg/m2 IV D1, 8Cisplatin 70 mg/m2 IV D1
21 4 – 36–50 % (<pT2)25–26 % (pT0)
MVAC [3] Methotrexate 30 mg/m2 IV D1, 15, 22Vinblastine 3 mg/m2 IV D2, 15, 22Doxorubicin 30 mg/m2 IV D2Cisplatin 70 mg/m2 IV D2
28 3 53 % 38 % (pT0)
Dose-dense MVAC [14] Methotrexate 30 mg/m2 IV D1Vinblastine 3 mg/m2 IV D2Doxorubicin 30 mg/m2 IV D2Cisplatin 70 mg/m2 IV D2Pegfilgrastim 6 mg SC D3
14 4 10 % 49 % (<pT2)26 % (pT0)
Accelerated MVAC [15] Methotrexate 30 mg/m2 IV D1Vinblastine 3 mg/m2 IV D1Doxorubicin 30 mg/m2 IV D1Cisplatin 70 mg/m2 IV D1Pegfilgrastim 6 mg SC D2
14 3 12 % 53 % (<pT2)38 % (pT0)
Dose-dense GC [11] Gemcitabine 2500 mg/m2 IV D1Cisplatin 35 mg/m2 IV D1, 2Pegfilgrastim 6 mg SC D3
14 6 NR 57 % (<pT2)
RR response rate, GC gemcitabine and cisplatin, D day, IV intravenous, MVAC methotrexate, vinblastine, doxorubicin, and cisplatin, SC subcutaneous
27 Page 2 of 12 Curr Oncol Rep (2016) 18:27

from a second trial of dose-dense GC that demonstrated a 56.5% <pT2 rate [11]. The SWOG is currently enrolling a multi-center trial of neoadjuvant GC versus dose-denseMVAC priorto cystectomy (NCT02177695) in order to evaluate the pre-dictive capacity of a biomarker called the CO-eXpressionExtrapolatioN (COXEN) model, which uses preclinically de-rived gene expression signatures to predict response to differ-ent chemotherapy regimens [19]. Although not designed toassess for efficacy differences between these two NAC regi-mens, it may inform the optimal regimen in subsequentstudies.
Unfortunately, there are no proven chemotherapy optionsfor reducing mortality in patients with MIBC who are noteligible for cisplatin. Ideally, such patients should participatein clinical trials but otherwise should proceed to cystectomywithout NAC.
Adjuvant Chemotherapy
Utilization of NAC in MIBC has historically been low withonly 1–2 % of patients withMIBC receiving NAC in the early2000s [20]. Although rates of NAC use have been steadilyincreasing over the last decade in MIBC, utilization remainslow with an estimated 21 % of patients with MIBC currentlytreated with NAC [21, 22]. Therefore, many patients proceedto cystectomy without preoperative chemotherapy.
No definitive randomized trials provide unequivocal sup-port for the use of adjuvant chemotherapy. However, availableclinical trials and retrospective studies suggest that there maybe a role for chemotherapy after cystectomy in select patientsthat were not treated with NAC. Most of the trials evaluatingadjuvant chemotherapy in MIBC are small, and many havesuffered from poor accrual with initial conflicting results[23–25]. A meta-analysis of available studies published in2005 showed a hazard ratio (HR) for survival of 0.75 foradjuvant chemotherapy (95 % CI 0.60–0.96); however, thismeta-analysis included only 491 patients from six trials andwas thus underpowered [26]. Since then, several larger ran-domized trials have been performed, but results of individualstudies have been conflicting. An updated meta-analysis in2014 found a similar benefit of adjuvant chemotherapy (HR0.77, 95 % CI 0.59–0.99) in pooled data from nine clinicaltrials [27]. The majority of these trials included patients withhigh-risk disease defined as extravesical extension and/or pos-itive lymph nodes.
A Spanish Oncology Genitourinary Group (SOGUG) 99/01 study enrolled high-risk patients with MIBC aftercystectomy and randomized them to 4 cycles of paclitaxel,gemcitabine, and cisplatin (PGC) or observation. This studysuffered from poor recruitment, and 142 patients were en-rolled. However, those that received adjuvant chemotherapyhad a significantly improved 5-year survival compared tothose that did not (60 vs 31 %, p<0.0009) [28]. The largest
adjuvant phase 3 trial to date, EORTC 30994, recruited 284 ofa planned 660 patients, once again limited in power due tounder accrual. Patients with high-risk MIBC (pT3–pT4 ornode positive) were randomized to 4 cycles of adjuvant che-motherapy (GC orMVAC or high-doseMVAC (HD-MVAC))or deferred chemotherapy at relapse. Adjuvant therapy im-proved progression-free survival (PFS) compared to deferredtreatment with a median PFS of 3.11 years (95 % CI 1.84–7.77) in the immediate treatment group compared with0.99 years (0.63–1.49) in the deferred treatment group (HR0.54, 95 % CI 0.4–0.73, p<0.0001) with no statistically sig-nificant improvement in OS (HR 0.78, 95 % 0.56–1.08)[29••]. Interestingly, the patients without pathologic lymphnode involvement appeared to derive the most benefit fromadjuvant therapy, with one interpretation that 4 cycles of che-motherapy may not be adequate in node-positive patients.
Galsky et al. recently presented an abstract of the compar-ative effectiveness of adjuvant chemotherapy using theNational Cancer Data Base (NCDB) [30]. This study com-pared those that received adjuvant chemotherapy with apropensity-score matched control group that receivedcystectomy alone. Adjuvant chemotherapy was associatedwith improved survival with an adjusted HR of 0.72 (95 %CI 0.71–0.86) compared to observation. Unfortunately, a ran-domized trial of adjuvant chemotherapy in MIBC is unlikelyto be completed in the future. At this time, systemic chemo-therapy should be offered to eligible patients with high-riskdisease at cystectomy, including pT3–T4 or lymph node-positive disease, after a discussion of risks and benefits ofadjuvant chemotherapy including a thorough review of therisk of recurrence, toxicities, and acknowledgement of thelimitations of the data in the adjuvant setting.
Chemotherapy in Bladder Preservationfor Muscle-Invasive Bladder Cancer
Bladder preservation with trimodality therapy (TMT) is a po-tential alternative to cystectomy for the treatment of MIBC inappropriately selected patients. This treatment combines ra-diotherapy, chemotherapy, and as complete a transurethral re-section of the bladder tumor (TURBT) as is safely possible.
Initial studies of TMT included cisplatin only or fluoroura-cil (5-FU) in combination with cisplatin as concomitant ther-apy with radiation [31–33]. It appeared from these studies thatsurvival rates were similar to cystectomy, and several subse-quent studies have confirmed a 5-year survival rate of 50–60 % [34–36]. The University of Erlangen experience inGermany demonstrated improvement in overall response rateand 5-year survival with the addition of 5-FU to cisplatin, aswell as higher response rates in cisplatin regimens comparedto carboplatin [37]. Cisplatin has also been combined withpaclitaxel with a 5-year OS of 56 % [38]. An ongoing
Curr Oncol Rep (2016) 18:27 Page 3 of 12 27

randomized phase 2 clinical trial compares concurrentcisplatin with concurrent cisplatin plus gemcitabine(NCT01495676). In the bladder preservation setting, cis-platin should be considered as a standard approachwhen possible. Neoadjuvant and adjuvant chemother-apies have shown no definitive benefit when added toconcurrent chemoradiotherapy [39].
Several chemotherapy options exist as an alternative tocisplatin for concurrent treatment with radiotherapy. TheBC2001 phase 3 randomized clinical trial compared radiother-apy alone to concurrent chemoradiotherapy with 5-FU andmitomycin C [40]. The chemotherapy group had a statisticallysignificant improvement in 2-year locoregional disease-freesurvival (DFS) compared to the control arm (67 vs 54 %,HR 0.68, 95 % CI 0.48–0.96) with a trend toward improve-ment in OS (HR 0.82, 95 % CI 0.63–1.09). Approximately30% of patients underwent NAC prior to enrollment. Oh et al.published the University of Michigan experience with a regi-men of twice weekly gemcitabine in combination with radio-therapy in TMT [41] with a reported 5-year bladder-intactsurvival (BIS) of 62 %, OS 76 %, and disease-specific surviv-al (DSS) of 82%. Results are awaited from the recently closedRadiation Therapy Oncology Group (RTOG) 0712 trial com-paring 5-FU plus cisplatin chemotherapy to gemcitabine incombination with radiation (NCT00777491). Other alterna-tives to cisplatin that have been studied include capecitabine,paclitaxel, and docetaxel [42–44].
Chemotherapy for Metastatic Bladder Cancer
First-Line Therapy
The first-line standard of care in metastatic BCa is combina-tion chemotherapy with GC. A randomized phase 3 trial byvon der Maase et al. showed GC to have similar efficacy toMVAC with improved tolerability, although it was notpowered to show equivalence between the two regimens[12, 13]. After adjusting for prognostic factors, the HR forOS and PFS with GC versus MVAC was 0.99 and 1.01(p>0.05 for both), respectively. Gemcitabine was adminis-tered at 1000 mg/m2 on days 1, 8, and 15 and cisplatin at70 mg/m2 on day 2 for 28 day cycles for a maximum of sixcycles. Despite improved tolerability compared with MVAC,37 % of patients required dose adjustments with the GC reg-imen with most dose adjustments occurring by gemcitabineomission on day 15. Therefore, modifications to the traditionaldosing of GC have been studied to improve tolerability andresponse. Dosing of GC every 3 weeks with omission of theday 15 gemcitabine has become widely used after severalstudies have shown preserved efficacy with a decrease in ratesof significant thrombocytopenia [45, 46]. An option for con-sideration in patients with borderline renal function
(glomerular filtration rate (GFR) 50–60 mL/min) is split dos-ing of cisplatin with administration of 35mg/m2 on days 1 and8 of each cycle [47].
HD-MVAC has also been compared to standard MVAC inEORTC 30924, demonstrating a 5-year survival of 21.8 % inthe HD-MVAC arm compared to 13.5 % with standardMVAC (HR 0.76, 95 % CI 0.58–0.99), although median OSwas similar in the two arms (15.1 vs 14.9 months, respective-ly) [48]. HD-MVAC was given with granulocyte colony-stimulating factor (G-CSF) support, and therefore, this regi-men was associated with less frequent neutropenic fever (10vs 26%, p<0.001). HD-MVAC or dose-denseMVAC has notbeen compared directly with GC in the metastatic setting.
The EORTC 30987 phase 3 trial of first-line GC with andwithout paclitaxel documented the best median OS in a ran-domized trial to date in metastatic disease with an OS of15.8 months in the paclitaxel plus GC arm compared with12.7 months in the GC alone arm (p=0.075) [49]. The studywas powered to detect a 4-month improvement in OS, andtherefore, the observed 3-month OS benefit did not achievestatistical significance. Hahn et al. demonstrated an impres-sive median OS of 19 months in a phase 2 trial of first-linegemcitabine, cisplatin, and bevacizumab [50]. Seven (41 %)of the first 17 patients enrolled experienced venous thrombo-embolism (VTE) events with initial dosing of gemcitabine at1250 mg/m2. After dose reduction to 1000 mg/m2, subse-quently enrolled patients had an acceptable and lower VTErate of 8 %. This regimen has been evaluated in a phase 3randomized trial that has finished accrual, but results are notyet available (NCT00942331).
Cisplatin-Ineligible Patients
Cisplatin-based combination therapy is consistently associat-ed with higher response rates and improved survival outcomescompared to carboplatin-based combinations, and cisplatinshould be used as the backbone of therapy whenever possible[51–54]. Unfortunately, renal dysfunction in patients withBCa is common and approximately half of all patients withmetastatic disease are not fit to receive cisplatin [55]. Galskyet al. have proposed criteria for determination of candi-dacy for cisplatin including Eastern CooperativeOncology Group (ECOG) performance status <2, creat-inine clearance ≥60 mL/min, grade <2 hearing loss,grade <2 neuropathy, and New York Heart Associationclass II or less heart failure [56].
EORTC 30986 compared gemcitabine plus carboplatinwith the combination of methotrexate, carboplatin, and vin-blastine (MCAVI) in patients ineligible for cisplatin defined asWorld Health Organization (WHO) performance status (PS)of 2 and/or impaired renal function (GFR >30 but not <60mL/min). MCAVI had more toxicity and similar efficacy with anOS of 8.1 months compared to 9.3 months in the gemcitabine
27 Page 4 of 12 Curr Oncol Rep (2016) 18:27
and carboplatin arm (p=0.64) [54]. These results provide lev-el 1 evidence for the use of gemcitabine and carboplatin forthe first-line treatment of patients with advanced/metastaticBCa who are ineligible to receive cisplatin.
Second-Line Therapy
Despite relatively high response rates to cisplatin-based first-line chemotherapy, almost all patients succumb to disease.There are currently no Food and Drug Administration(FDA)-approved chemotherapy agents for metastatic BCa inthe second-line setting, and only vinflunine is approved foruse in Europe based on a 2.6-month survival advantage overbest supportive care [57]. Response rates and survival out-comes to standardly used second-line treatment are poor.Karnofsky PS, presence of visceral metastases, hemoglobin<10 g/dL, and time from prior chemotherapy <3 months areprognostic in this setting and may be used to inform treatmentdecisions [58, 59].
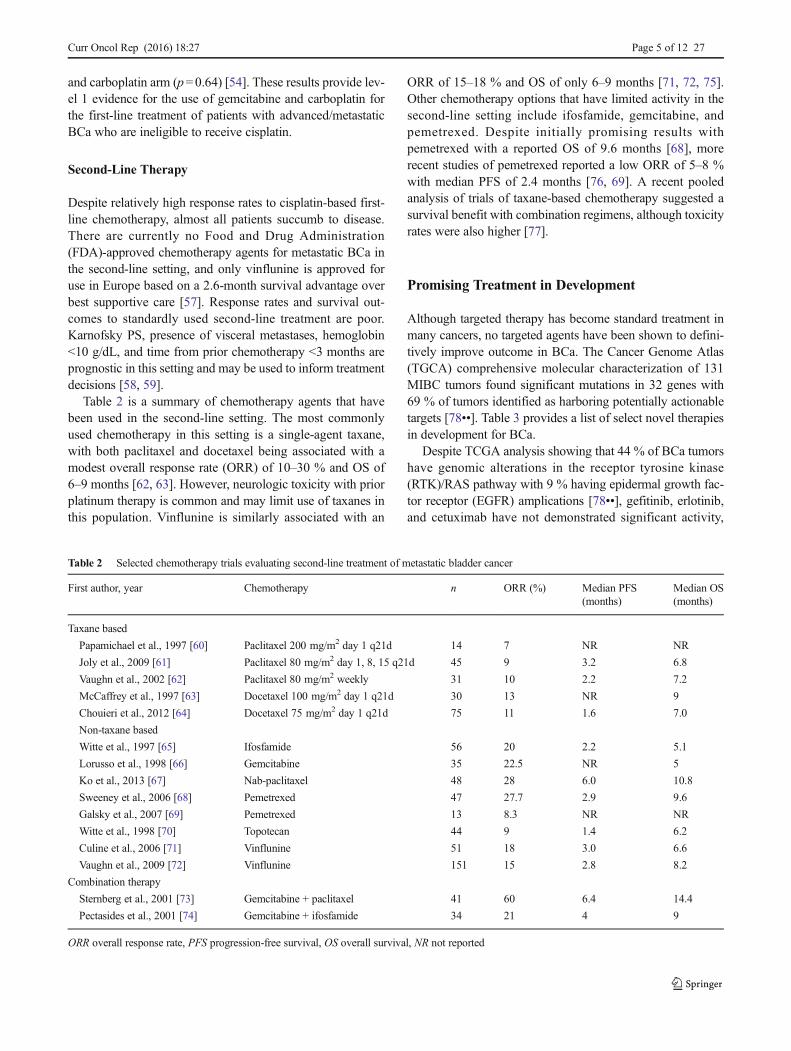
Table 2 is a summary of chemotherapy agents that havebeen used in the second-line setting. The most commonlyused chemotherapy in this setting is a single-agent taxane,with both paclitaxel and docetaxel being associated with amodest overall response rate (ORR) of 10–30 % and OS of6–9 months [62, 63]. However, neurologic toxicity with priorplatinum therapy is common and may limit use of taxanes inthis population. Vinflunine is similarly associated with an
ORR of 15–18 % and OS of only 6–9 months [71, 72, 75].Other chemotherapy options that have limited activity in thesecond-line setting include ifosfamide, gemcitabine, andpemetrexed. Despite initially promising results withpemetrexed with a reported OS of 9.6 months [68], morerecent studies of pemetrexed reported a low ORR of 5–8 %with median PFS of 2.4 months [76, 69]. A recent pooledanalysis of trials of taxane-based chemotherapy suggested asurvival benefit with combination regimens, although toxicityrates were also higher [77].
Promising Treatment in Development
Although targeted therapy has become standard treatment inmany cancers, no targeted agents have been shown to defini-tively improve outcome in BCa. The Cancer Genome Atlas(TGCA) comprehensive molecular characterization of 131MIBC tumors found significant mutations in 32 genes with69 % of tumors identified as harboring potentially actionabletargets [78••]. Table 3 provides a list of select novel therapiesin development for BCa.
Despite TCGA analysis showing that 44 % of BCa tumorshave genomic alterations in the receptor tyrosine kinase(RTK)/RAS pathway with 9 % having epidermal growth fac-tor receptor (EGFR) amplications [78••], gefitinib, erlotinib,and cetuximab have not demonstrated significant activity,
Table 2 Selected chemotherapy trials evaluating second-line treatment of metastatic bladder cancer
First author, year Chemotherapy n ORR (%) Median PFS(months)
Median OS(months)
Taxane based
Papamichael et al., 1997 [60] Paclitaxel 200 mg/m2 day 1 q21d 14 7 NR NR
Joly et al., 2009 [61] Paclitaxel 80 mg/m2 day 1, 8, 15 q21d 45 9 3.2 6.8
Vaughn et al., 2002 [62] Paclitaxel 80 mg/m2 weekly 31 10 2.2 7.2
McCaffrey et al., 1997 [63] Docetaxel 100 mg/m2 day 1 q21d 30 13 NR 9
Chouieri et al., 2012 [64] Docetaxel 75 mg/m2 day 1 q21d 75 11 1.6 7.0
Non-taxane based
Witte et al., 1997 [65] Ifosfamide 56 20 2.2 5.1
Lorusso et al., 1998 [66] Gemcitabine 35 22.5 NR 5
Ko et al., 2013 [67] Nab-paclitaxel 48 28 6.0 10.8
Sweeney et al., 2006 [68] Pemetrexed 47 27.7 2.9 9.6
Galsky et al., 2007 [69] Pemetrexed 13 8.3 NR NR
Witte et al., 1998 [70] Topotecan 44 9 1.4 6.2
Culine et al., 2006 [71] Vinflunine 51 18 3.0 6.6
Vaughn et al., 2009 [72] Vinflunine 151 15 2.8 8.2
Combination therapy
Sternberg et al., 2001 [73] Gemcitabine + paclitaxel 41 60 6.4 14.4
Pectasides et al., 2001 [74] Gemcitabine + ifosfamide 34 21 4 9
ORR overall response rate, PFS progression-free survival, OS overall survival, NR not reported
Curr Oncol Rep (2016) 18:27 Page 5 of 12 27

although study participants were not selected by EGFR status[79–83]. Seven percent of TCGA tumors had ERBB2 copynumber alterations [67], and HER2 signaling was targeted in atrial by Hussain et al. with the combination of trastuzumabwith gemcitabine, carboplatin, and paclitaxel in patients withHER2 overexpressing advanced BCa, as determined byHER2 immunohistochemistry (IHC), gene amplification viafluorescence in situ hybridization (FISH), or elevated serumHer-2/neu. This regimen showed a 70 % ORR with a medianOS of 14.1 months, which is promising but, given the lack ofrandomization in this trial, not definitive for an effect oftrastuzumab. Despite high rates of IHC positivity, a minorityof enrolled patients had positive FISH results, and the optimalmethod to detect HER2 overexpression is not known.
Multiple novel agents are being studied targeting the fibro-blast growth factor receptor (FGFR) pathway, which is alteredin nearly 70 % of non-invasive BCa and 15 % of MIBCtumors [78••, 84]. The complementary vascular endothelialgrowth factor (VEGF) pathway has also been investigatedextensively. Sunitinib did not show an improvement in re-sponse or survival in patients with advanced, previously treat-ed BCa compared to historical controls with PFS of approxi-mately 2 months and median OS of 6–7 months [85]. First-line treatment with sunitinib in cisplatin-ineligible metastaticBCa showed a PFS and OS of only 4.8 and 8.1 months, re-spectively [86]. Results with sorafenib were similarlyunderwhelming [87, 88]. In one study by Necchi et al.,pazopanib was associated with a modest ORR of 17 % in
Table 3 Select trials of novel agents for advanced bladder cancer
Agent Mechanism of action Phase Trial description
Cytotoxic therapy
Eribulin Microtubule inhibitor 2 Single-agent trial in previously treated patients(NCT00365157)
Nab-paclitaxel Microtubule inhibitor 2 Randomized trial of nab-paclitaxel vs paclitaxelin previously treated patients (NCT020339933)
Targeted therapy
ACP-196 Bruton tyrosine kinase inhibitor 2 ACP196 + pembrolizumab in previously treatedpatients (NCT02351739)
Alisertib Aurora A kinase inhibitor 2 Single-agent trial in previously treated patients(NCT02109328)
B-701 Anti-FGFR3 antibody 2 B-701 + docetaxel vs docetaxel alone in previouslytreated patients (NCT02401542)
Cabozantinib MET, VEGF2, and RET inhibitor 2 Single-agent trial in previously treated patients(NCT01688999)
JNJ-42756492 Pan-FGFR tyrosine kinase inhibitor 2 Single-agent dose-finding trial in previously treatedpatients (NCT02365597)
Mocetinostat Histone deacetylase inhibitor 2 Single-agent trial in previously treated patients(NCT02236195)
Palbociclib CDK4/6 inhibitor 2 Single-agent trial in previously treated patients(NCT02334527)
Pazopanib VEGF tyrosine kinase inhibitor 2 Pazopanib + paclitaxel trial in previously treatedpatients (NCT01108055)
Regorafenib Multikinase inhibitor 2 Single-agent trial in previously treated patients(NCT02459119)
Tipifarnib Farnesyl transferase inhibitor 2 Single-agent trial in HRAS-mutated previouslytreated patients (NCT02535650)
Immune therapy
ALT-801 IL-2 fused to T cell receptor directed against p53 2 ALT-801 + gemcitabine + cisplatin or ALT-801 +gemcitabine alone (NCT01326871)
Atezolizumab PD-L1 antibody 3 Atezolizumab vs standard chemotherapy inpreviously treated patients (NCT02302807)
Pembrolizumab PD-1 antibody 3 Pembrolizumab vs standard chemotherapy inpreviously treated patients(NCT02256436, completed accrual)
From clinicaltrials.gov, accessed October 20, 2015
FGFR fibroblast growth factor receptor, VEGF vascular endothelial growth factor, CDK cyclin-dependent kinase, PD-1 programmed death-1, PD-L1programmed death ligand 1
27 Page 6 of 12 Curr Oncol Rep (2016) 18:27

previously treated BCa patients, but 5 % of patients developedfistulas during the study [89]. As discussed earlier,bevacizumab has been evaluated in a randomized, phase 3trial in the first-line metastatic setting after promising resultsin a phase 2 trial of gemcitabine, cisplatin, and bevacizumab[50]. A randomized phase 2 trial of docetaxel with or withoutramucirumab, a monoclonal antibody directed against VEGF-receptor 2, showed that the combination had a promising im-provement in median PFS compared with docetaxel alone (5.4vs 2.8 months, p<0.001) with non-significant improvementsin ORR and median OS (24 vs 9 %, p=0.088 and 10.4 vs9.2 months, p=0.20, respectively) [90].
The mammalian target of rapamycin (mTOR) inhibi-tor everolimus was evaluated in several trials with over-all disappointing results [91, 92], in spite of 42 % oftumors with mTOR pathway alterations in TCGA [67].However, there are several reports of exceptional re-sponses to everolimus, one in a patient with two acti-vating mutations in mTOR, and one in a patient withalterations in TSC1 and NF2, known negative regulatorsof the mTOR pathway where inactivation leads to en-hanced mTOR signaling and potential sensitivity toeverolimus [92, 93]. Such exceptional responder reportssupport a potential role for tumor sequencing to guidetherapy.
Other promising drugs are also in development. Given thehigh frequency of retinoblastoma (RB) and cyclin-dependentkinase pathway alterations in BCa, a phase 2 trial of theCDK4/6 inhibitor palbociclib is underway in molecularly se-lected patients with metastatic BCa (NCT02334527). Novelcytotoxic chemotherapy regimens are also being studied. Aphase 2 trial of eribulin presented at the 2015 ASCO AnnualMeeting showed a response rate (RR) of 35 % and median OSof 9.5 months in metastatic BCa, a slight improvement com-pared to historical rates [94]. Further studies of eribulin areongoing (NCT02178241, NCT00365157).
Immunotherapy in Bladder Cancer
Immunotherapy has emerged as the most promising class ofagents in development for the treatment of metastatic BCaafter progression on first-line chemotherapy. Many tumorcells express receptors such as programmed death ligand-1(PD-L1) and cytotoxic T cell lymphocyte antigen (CTLA-4),which inhibit T cell-mediated tumor cell killing via interactionwith T cell receptors.
Anti-programmed death-1 (PD-1) and anti-PD-L1 agentscalled immune checkpoint inhibitors have demonstrated ex-citing activity in many human cancers [95]. Initial data showactivity of PD-1 and PD-L1 inhibition in metastatic BCa aswell [96••]. An updated analysis of a phase 1 trial in platinum-refractory metastatic BCa presented at the 2015 ASCO
Annual Meeting by Petrylak et al. showed that atezolizumab(MPDL3280A, Genentech) had an ORR of 50 % in PD-L1-positive patients and 17 % in PD-L1-negative patients, with55 % of all patients showing a reduction in tumor burden witha number of ongoing, durable responses [97]. Atezolizumabwas granted Breakthrough Therapy Designation by the FDA.The phase 2 IMvigor 210 (NCT02108652) results were pre-sented at the 2015 European Cancer Congress, andatezolizumab had an ORR of 18 % based on modifiedRECIST criteria with higher response rates in PD-L1-positive patients. A phase 3 trial of this agent is underway(IMvigor 211, NCT02302807), as well as trials in the adjuvant(IMgivor 010, NCT02450331) and neoadjuvant settings(NCT02451423).
Similarly, initial data from KEYNOTE-012, a phase1b study of the PD-1 antibody pembrolizumab (MK-3475, Merck), showed promising results in PD-L1-positive metastatic BCa with an ORR of 28 % with64 % of patients experiencing a reduction in tumor bur-den. Median OS was 12.7 months [98]. A phase 3second-line randomized clinical trial of pembrolizumabagainst standard cytotoxic chemotherapy has recentlycompleted accrual (KEYNOTE-045, NCT02256436).This agent is also being tested in the first-line metastaticsetting for cisplatin-ineligible patients (KEYNOTE-052,NCT02335424) and in the neoadjuvant set t ing(NCT02365766). The Bristol-Myers Squibb anti-PD1antibody nivolumab is also being investigated in severalcancers including BCa (NCT02387996).
The CTLA-4 inhibitor ipilimumab underwent evaluation ina first-line trial of gemcitabine, cisplatin, and ipilimumab formetastatic BCa [99]. This regimen demonstrated an ORR of64 %, median PFS of 8 months, and median OS of 14.6months with similar efficacy but more toxicity than historicalcontrols of GC alone. I pilimumab is associated with moresevere immune-related side effects than the newer immunecheckpoint inhibitors. Vaccines and other biological com-pounds are also in development, including ALT-801, a biolog-ic compound of interleukin-2 (IL-2) fused to a humanizedsoluble T cell receptor directed against the p53-derived pep-tides expressed on tumor cells (NCT01326871). This com-pound has shown promising early results [100].
Biomarker Development
Improved technologies for molecular profiling such ashigh-throughput sequencing have launched an integratedapproach to drug development with the concurrent dis-covery of predictive and prognostic biomarkers. This isparticularly important in the development of immuno-therapy since responses can be complete and durable,but at present, only a minority of patients respond to
Curr Oncol Rep (2016) 18:27 Page 7 of 12 27

treatment. Identifying patients most likely to respond istherefore critical. Immunohistochemical PD-L1 positivityis associated with higher response to immune check-point inhibition, but PD-L1 status does not reliably dif-ferentiate responders from non-responders [97].
Tumor somatic mutations can give rise to neoantigens,which are peptides presented on the surface of the cell thatare unique to the cancer and may be able to elicit an im-mune response. A study in melanoma demonstrated that ahigh tumor mutational load correlates with benefit fromimmunotherapy with CTLA-4 blockade [101]. BCa hasone of the highest mutational burdens compared to otherhuman cancers [102], and this may contribute to the prom-ising activity of immune checkpoint inhibition in BCa.Molecular subtypes of BCa have also recently been iden-tified and resemble the subtypes of breast cancer includingBbasal^ and Bluminal^ subtypes [103••, 104••]. These sub-types have distinct RNA expression profiles and appear tobe prognostic of clinical outcome. The basal subtype isenriched for biomarkers reflective of immune infiltration,potentially suggesting a predictive role for immunothera-py [104••].
Conclusions
Progress in the treatment of advanced BCa is no longer stag-nant. Utilization rates of NAC are rising in response to theunequivocal survival benefit in muscle-invasive BCa.Adjuvant chemotherapy may be considered for select patientswho did not receive NAC. The addition of systemic therapy toradiation in bladder preservation approaches improves out-comes compared to radiation alone.
Development of targeted agents has been fueled by themolecular characterization of BCa. Immunotherapy withcheckpoint inhibitors has promising clinical trial results, andrandomized trials are underway. Predictive biomarker devel-opment must parallel drug development to best select patientsfor novel targeted agents and immunotherapies. It is an ex-tremely exciting time in BCa research, and much needed im-provements in systemic treatment are most certainly on thehorizon.
Compliance with Ethical Standards
Conflict of Interest Tracy L. Rose declares that she has no conflict ofinterest.
Matthew I. Milowsky has received has received research fundingfrom BIND Therapeutics, Dendreon, Exelixis, J&J, Astellas, MiratiTherapetics, Pfizer, Cerulean Pharma, Merck, and Seattle Genetics.
Human and Animal Rights and Informed Consent This article doesnot contain any studies with human or animal subjects performed by anyof the authors.
References
Papers of particular interest, published recently, have beenhighlighted as:•• Of importanc
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2015. CACancer J Clin. 2015;65(1):5–29. doi:10.3322/caac.21254.
2. Kaufman DS, Shipley WU, Feldman AS. Bladder cancer. Lancet.2009;374(9685):239–49. doi:10.1016/s0140-6736(09)60491-8.
3. Grossman HB, Natale RB, Tangen CM, Speights VO, VogelzangNJ, Trump DL, et al. Neoadjuvant chemotherapy plus cystectomycompared with cystectomy alone for locally advanced bladdercancer. N Engl J Med. 2003;349(9):859–66. doi:10.1056/NEJMoa022148.
4. Sonpavde G, Goldman BH, Speights VO, Lerner SP, Wood DP,Vogelzang NJ, et al. Quality of pathologic response and surgerycorrelate with survival for patients with completely resected blad-der cancer after neoadjuvant chemotherapy. Cancer.2009;115(18):4104–9. doi:10.1002/cncr.24466.
5. Rosenblatt R, Sherif A, Rintala E, Wahlqvist R, Ullen A, NilssonS, et al. Pathologic downstaging is a surrogate marker for efficacyand increased survival following neoadjuvant chemotherapy andradical cystectomy for muscle-invasive urothelial bladder cancer.Eur Urol. 2012;61(6):1229–38. doi:10.1016/j.eururo.2011.12.010.
6. Neoadjuvant cisplatin, methotrexate, and vinblastine chemothera-py for muscle-invasive bladder cancer: a randomised controlledtrial. International collaboration of trialists. Lancet.1999;354(9178):533-40.
7. Griffiths G, Hall R, Sylvester R, Raghavan D, Parmar MK.International phase III trial assessing neoadjuvant cisplatin, meth-otrexate, and vinblastine chemotherapy for muscle-invasive blad-der cancer: long-term results of the BA06 30894 trial. J ClinOncol. 2011;29(16):2171–7. doi:10.1200/jco.2010.32.3139.
8. Neoadjuvant chemotherapy in invasive bladder cancer: update ofa systematic review and meta-analysis of individual patient dataadvanced bladder cancer (ABC) meta-analysis collaboration.European urology. 2005;48(2):202-5; discussion 5-6. doi:10.1016/j.eururo.2005.04.006.
9. Dash A, Pettus JA, Herr HW, Bochner BH, Dalbagni G, DonatSM, et al. A role for neoadjuvant gemcitabine plus cisplatin inmuscle-invasive urothelial carcinoma of the bladder: a retrospec-tive experience. Cancer. 2008;113(9):2471–7. doi:10.1002/cncr.23848.
10. Yeshchina O, Badalato GM, Wosnitzer MS, Hruby G,RoyChoudhury A, BensonMC, et al. Relative efficacy of periop-erative gemcitabine and cisplatin versus methotrexate, vinblas-tine, adriamycin, and cisplatin in the management of locally ad-vanced urothelial carcinoma of the bladder. Urology. 2012;79(2):384–90. doi:10.1016/j.urology.2011.10.050.
11. Balar AV, Iyer G, Milowsky MI, Huang WC, Woods M, DonatSM, et al. Multicenter prospective phase II trial of neoadjuvant(neo) dose dense gemcitabine and cisplatin (DD-GC) in patients(pts) with muscle-invasive bladder cancer (MIBC). ASCOMeeting Abstracts. 2016;34:436.
12. von der Maase H, Sengelov L, Roberts JT, Ricci S, Dogliotti L,Oliver T, et al. Long-term survival results of a randomized trialcomparing gemcitabine plus cisplatin, with methotrexate, vinblas-tine, doxorubicin, plus cisplatin in patients with bladder cancer. JClin Oncol. 2005;23(21):4602–8. doi:10.1200/jco.2005.07.757.
27 Page 8 of 12 Curr Oncol Rep (2016) 18:27
13. von der Maase H, Hansen SW, Roberts JT, Dogliotti L, Oliver T,Moore MJ, et al. Gemcitabine and cisplatin versus methotrexate,vinblastine, doxorubicin, and cisplatin in advanced or metastaticbladder cancer: results of a large, randomized, multinational, mul-ticenter, phase III study. J Clin Oncol. 2000;18(17):3068–77.
14.•• Galsky MD, Pal SK, Chowdhury S, Harshman LC, Crabb SJ,Wong YN et al. Comparative effectiveness of gemcitabine pluscisplatin versus methotrexate, vinblastine, doxorubicin, plus cis-platin as neoadjuvant therapy for muscle-invasive bladder cancer.Cancer. 2015. doi:10.1002/cncr.29387. There is no difference inpathologic complete response between neoadjuvant GC andMVAC chemotherapy.
15. Zargar H, Espiritu PN, Fairey AS, Mertens LS, Dinney CP, MirMC, et al. Multicenter assessment of neoadjuvant chemotherapyfor muscle-invasive bladder cancer. Eur Urol. 2015;67(2):241–9.doi:10.1016/j.eururo.2014.09.007.
16.•• Choueiri TK, Jacobus S, Bellmunt J, Qu A, Appleman LJ, TretterC, et al. Neoadjuvant dose-dense methotrexate, vinblastine, doxo-rubicin, and cisplatin with pegfilgrastim support in muscle-invasive urothelial cancer: pathologic, radiologic, and biomarkercorrelates. J Clin Oncol. 2014;32(18):1889–94. doi:10.1200/jco.2013.52.4785. Neoadjuvant dose-dense MVAC is well-tolerated and results in significant pathologic downstagingwith 49% of patients achieving <pT2.
17.•• Plimack ER, Hoffman-Censits JH, Viterbo R, Trabulsi EJ, RossEA, Greenberg RE, et al. Accelerated methotrexate, vinblastine,doxorubicin, and cisplatin is safe, effective, and efficient neoadju-vant treatment for muscle-invasive bladder cancer: results of amulticenter phase II study with molecular correlates of responseand toxicity. J Clin Oncol. 2014;32(18):1895–901. doi:10.1200/jco.2013.53.2465. Neoadjuvant accelerated MVAC is well-tolerated and results in significant pathologic downstagingwith 38% of patients achieving pT0.
18. Plimack ER, Hoffman-Censits JH, Kutikov A, Greenberg RE,Bilusic M, Chen DYT, et al. Neoadjuvant dose-dense gemcitabineand cisplatin (DDGC) in patients (pts) with muscle-invasive blad-der cancer (MIBC): final results of a multicenter phase II study.ASCO Meeting Abstracts. 2014;32(15_suppl):4513.
19. Smith SC, Baras AS, Lee JK, Theodorescu D. The COXEN prin-ciple: translating signatures of in vitro chemosensitivity into toolsfor clinical outcome prediction and drug discovery in cancer.Cancer Res. 2010;70(5):1753–8. doi:10.1158/0008-5472.can-09-3562.
20. David KA, MilowskyMI, Ritchey J, Carroll PR, Nanus DM. Lowincidence of perioperative chemotherapy for stage III bladder can-cer 1998 to 2003: a report from the National Cancer Data Base. JUrol. 2007;178(2):451–4. doi:10.1016/j.juro.2007.03.101.
21. Zaid HB, Patel SG, Stimson CJ, Resnick MJ, Cookson MS,Barocas DA, et al. Trends in the utilization of neoadjuvant che-motherapy in muscle-invasive bladder cancer: results from theNational Cancer Database. Urology. 2014;83(1):75–80. doi:10.1016/j.urology.2013.07.072.
22. Reardon ZD, Patel SG, Zaid HB, Stimson CJ, Resnick MJ,Keegan KA, et al. Trends in the use of perioperative chemother-apy for localized and locally advanced muscle-invasive bladdercancer: a sign of changing tides. Eur Urol. 2014. doi:10.1016/j.eururo.2014.01.009.
23. Cognetti F, Ruggeri EM, Felici A, Gallucci M, Muto G, PolleraCF, et al. Adjuvant chemotherapy with cisplatin and gemcitabineversus chemotherapy at relapse in patients with muscle-invasivebladder cancer submitted to radical cystectomy: an Italian, multi-center, randomized phase III trial. Ann Oncol. 2012;23(3):695–700. doi:10.1093/annonc/mdr354.
24. Stockle M, Meyenburg W, Wellek S, Voges G, Gertenbach U,Thuroff JW, et al. Advanced bladder cancer (stages pT3b, pT4a,pN1 and pN2): improved survival after radical cystectomy and 3
adjuvant cycles of chemotherapy. Results of a controlled prospec-tive study. J Urol. 1992;148(2 Pt 1):302–6. discussion 6-7.
25. Skinner DG, Daniels JR, Russell CA, Lieskovsky G, Boyd SD,Nichols P, et al. The role of adjuvant chemotherapy followingcystectomy for invasive bladder cancer: a prospective comparativetrial. J Urol. 1991;145(3):459–64. discussion 64-7.
26. Adjuvant chemotherapy in invasive bladder cancer: a systematicreview and meta-analysis of individual patient data AdvancedBladder Cancer (ABC) Meta-analysis Collaboration. EuropeanUrology. 2005;48(2):189-99; discussion 99-201. doi:10.1016/j.eururo.2005.04.005.
27. Leow JJ, Martin-Doyle W, Rajagopal PS, Patel CG, AndersonEM,RothmanAT, et al. Adjuvant chemotherapy for invasive blad-der cancer: a 2013 updated systematic review andmeta-analysis ofrandomized trials. Eur Urol. 2014;66(1):42–54. doi:10.1016/j.eururo.2013.08.033.
28. Paz-Ares LG, Solsona E, Esteban E, Saez A, Gonzalez-Larriba J,Anton A, et al. Randomized phase III trial comparing adjuvantpaclitaxel/gemcitabine/cisplatin (PGC) to observation in patientswith resected invasive bladder cancer: results of the SpanishOncology Genitourinary Group (SOGUG) 99/01 study. ASCOMeeting Abstracts. 2010;28(18_suppl):LBA4518.
29.•• Sternberg CN, Skoneczna I, Kerst JM, Albers P, Fossa SD,Agerbaek M, et al. Immediate versus deferred chemotherapy afterradical cystectomy in patients with pT3-pT4 or N+ M0 urothelialcarcinoma of the bladder (EORTC 30994): an intergroup, open-label, randomised phase 3 trial. Lancet Oncol. 2015;16(1):76–86.doi:10.1016/s1470-2045(14)71160-x. There was no survivalbenefit of immediate over deferred chemotherapy forpatients with high-risk MIBC after radical cystectomy. Thisstudy was underpowered and did not meet goal of accrual.
30. Galsky MD, Stensland K, Moshier EL, Sfakianos J, McBride RB,Tsao C-K, et al. Effectiveness of adjuvant chemotherapy (AC)versus observation in patients with >= pT3 and/or pN+ bladdercancer (BCa). ASCO Meeting Abstracts. 2015;33(15_suppl):4517.
31. Shipley WU, Prout Jr GR, Einstein AB, Coombs LJ, Wajsman Z,Soloway MS, et al. Treatment of invasive bladder cancer by cis-platin and radiation in patients unsuited for surgery. Jama.1987;258(7):931–5.
32. Housset M, Maulard C, Chretien Y, Dufour B, Delanian S, HuartJ, et al. Combined radiation and chemotherapy for invasivetransitional-cell carcinoma of the bladder: a prospective study. JClin Oncol. 1993;11(11):2150–7.
33. Sauer R, Dunst J, Altendorf-Hofmann A, Fischer H, Bornhof C,Schrott KM. Radiotherapy with and without cisplatin in bladdercancer. Int J Radiat Oncol Biol Phys. 1990;19(3):687–91.
34. ShipleyWU, Kaufman DS, Zehr E, Heney NM, Lane SC, ThakralHK, et al. Selective bladder preservation by combined modalityprotocol treatment: long-term outcomes of 190 patients with inva-sive bladder cancer. Urology. 2002;60(1):62–7. discussion 7-8.
35. Weiss C, Engehausen DG, Krause FS, Papadopoulos T, Dunst J,Sauer R, et al. Radiochemotherapy with cisplatin and 5-fluorouracil after transurethral surgery in patients with bladdercancer. Int J Radiat Oncol Biol Phys. 2007;68(4):1072–80. doi:10.1016/j.ijrobp.2007.01.054.
36. Chung PW, Bristow RG, Milosevic MF, Yi QL, Jewett MA,Warde PR, et al. Long-term outcome of radiation-based conserva-tion therapy for invasive bladder cancer. Urol Oncol. 2007;25(4):303–9. doi:10.1016/j.urolonc.2006.09.015.
37. Rodel C, Grabenbauer GG, Kuhn R, Papadopoulos T, Dunst J,Meyer M, et al. Combined-modality treatment and selective organpreservation in invasive bladder cancer: long-term results. J ClinOncol. 2002;20(14):3061–71.
38. Kaufman DS, Winter KA, Shipley WU, Heney NM, Wallace 3rdHJ, Toonkel LM, et al. Phase I-II RTOG study (99-06) of patients
Curr Oncol Rep (2016) 18:27 Page 9 of 12 27
with muscle-invasive bladder cancer undergoing transurethral sur-gery, paclitaxel, cisplatin, and twice-daily radiotherapy followedby selective bladder preservation or radical cystectomy and adju-vant chemotherapy. Urology. 2009;73(4):833–7. doi:10.1016/j.urology.2008.09.036.
39. Rodel C, Weiss C, Sauer R. Trimodality treatment and selectiveorgan preservation for bladder cancer. J Clin Oncol. 2006;24(35):5536–44. doi:10.1200/jco.2006.07.6729.
40. James ND, Hussain SA, Hall E, Jenkins P, Tremlett J, Rawlings C,et al. Radiotherapy with or without chemotherapy in muscle-invasive bladder cancer. N Engl J Med. 2012;366(16):1477–88.doi:10.1056/NEJMoa1106106.
41. Oh KS, Soto DE, Smith DC, Montie JE, Lee CT, Sandler HM.Combined-modality therapy with gemcitabine and radiation ther-apy as a bladder preservation strategy: long-term results of a phaseI trial. Int J Radiat Oncol Biol Phys. 2009;74(2):511–7. doi:10.1016/j.ijrobp.2008.08.021.
42. Patel B, Forman J, Fontana J, Frazier A, Pontes E, VaishampayanU. A single institution experience with concurrent capecitabineand radiation therapy in weak and/or elderly patients withurothelial cancer. Int J Radiat Oncol Biol Phys. 2005;62(5):1332–8. doi:10.1016/j.ijrobp.2005.01.004.
43. Dunst J, Weigel C, Heynemann H, Becker A. Preliminary resultsof simultaneous radiochemotherapy with paclitaxel for urinarybladder cancer. Strahlentherapie und Onkologie : Organ derDeutschen Rontgengesellschaft [et al]. 1999;175 Suppl 3:7–10.
44. Nichols Jr RC, Sweetser MG, Mahmood SK, Malamud FC, DunnNP, Adams JP, et al. Radiation therapy and concomitant paclitaxel/carboplatin chemotherapy for muscle invasive transitional cell carci-noma of the bladder: a well-tolerated combination. International jour-nal of cancer Journal international du cancer. 2000;90(5):281–6.
45. Adamo V, Magno C, Spitaleri G, Garipoli C, Maisano C, AlafaciE, et al. Phase II study of gemcitabine and cisplatin in patients withadvanced ormetastatic bladder cancer: long-term follow-up of a 3-week regimen. Oncology. 2005;69(5):391–8. doi:10.1159/000089993.
46. Soto Parra H, Cavina R, Latteri F, Sala A, DambrosioM, AntonelliG, et al. Three-week versus four-week schedule of cisplatin andgemcitabine: results of a randomized phase II study. Ann Oncol.2002;13(7):1080–6.
47. Hussain SA, Palmer DH, Lloyd B, Collins SI, Barton D, Ansari J,et al. A study of split-dose cisplatin-based neo-adjuvant chemo-therapy in muscle-invasive bladder cancer. Oncology letters.2012;3(4):855–9. doi:10.3892/ol.2012.563.
48. Sternberg CN, de Mulder P, Schornagel JH, Theodore C, FossaSD, van Oosterom AT, et al. Seven year update of an EORTCphase III trial of high-dose intensity M-VAC chemotherapy andG-CSF versus classic M-VAC in advanced urothelial tract tu-mours. European journal of cancer (Oxford, England : 1990).2006;42(1):50–4.
49. Bellmunt J, von der Maase H, Mead GM, Skoneczna I, De SantisM, Daugaard G, et al. Randomized phase III study comparingpaclitaxel/cisplatin/gemcitabine and gemcitabine/cisplatin in pa-tients with locally advanced ormetastatic urothelial cancer withoutprior systemic therapy: EORTC Intergroup Study 30987. J ClinOncol. 2012;30(10):1107–13. doi:10.1200/jco.2011.38.6979.
50. Hahn NM, Stadler WM, Zon RT, Waterhouse D, Picus J, NattamS, et al. Phase II trial of cisplatin, gemcitabine, and bevacizumabas first-line therapy for metastatic urothelial carcinoma: HoosierOncology Group GU 04-75. J Clin Oncol. 2011;29(12):1525–30.doi:10.1200/jco.2010.31.6067.
51. Dreicer R,Manola J, Roth BJ, SeeWA, Kuross S, EdelmanMJ, etal. Phase III trial of methotrexate, vinblastine, doxorubicin, andcisplatin versus carboplatin and paclitaxel in patients with ad-vanced carcinoma of the urothelium. Cancer. 2004;100(8):1639–45. doi:10.1002/cncr.20123.
52. Dogliotti L, Carteni G, Siena S, Bertetto O,Martoni A, Bono A, etal. Gemcitabine plus cisplatin versus gemcitabine plus carboplatinas first-line chemotherapy in advanced transitional cell carcinomaof the urothelium: results of a randomized phase 2 trial. Eur Urol.2007;52(1):134–41. doi:10.1016/j.eururo.2006.12.029.
53. GalskyMD, Chen GJ, OhWK, Bellmunt J, Roth BJ, Petrioli R, etal. Comparative effectiveness of cisplatin-based and carboplatin-based chemotherapy for treatment of advanced urothelial carcino-ma. Ann Oncol. 2012;23(2):406–10. doi:10.1093/annonc/mdr156.
54. De Santis M, Bellmunt J, Mead G, Kerst JM, LeahyM, Maroto P,et al. Randomized phase II/III trial assessing gemcitabine/carboplatin and methotrexate/carboplatin/vinblastine in patientswith advanced urothelial cancer who are unfit for cisplatin-basedchemotherapy: EORTC study 30986. J Clin Oncol. 2012;30(2):191–9. doi:10.1200/jco.2011.37.3571.
55. Dash A, Galsky MD, Vickers AJ, Serio AM, Koppie TM,Dalbagni G, et al. Impact of renal impairment on eligibility foradjuvant cisplatin-based chemotherapy in patients with urothelialcarcinoma of the bladder. Cancer. 2006;107(3):506–13. doi:10.1002/cncr.22031.
56. Galsky MD, Hahn NM, Rosenberg J, Sonpavde G, Hutson T, OhWK, et al. Treatment of patients with metastatic urothelial cancerBunfit^ for cisplatin-based chemotherapy. J Clin Oncol.2011;29(17):2432–8. doi:10.1200/jco.2011.34.8433.
57. Bellmunt J, Theodore C, Demkov T, Komyakov B, Sengelov L,Daugaard G, et al. Phase III trial of vinflunine plus best supportivecare compared with best supportive care alone after a platinum-containing regimen in patients with advanced transitional cell car-cinoma of the urothelial tract. J Clin Oncol. 2009;27(27):4454–61.doi:10.1200/jco.2008.20.5534.
58. Bajorin DF, Dodd PM, Mazumdar M, Fazzari M, McCaffrey JA,Scher HI, et al. Long-term survival in metastatic transitional-cellcarcinoma and prognostic factors predicting outcome of therapy. JClin Oncol. 1999;17(10):3173–81.
59. Sonpavde G, Pond GR, Rosenberg JE, Bajorin DF, Choueiri TK,NecchiA,et al. Improved5-factor prognostic classificationofpatientsreceivingsalvagesystemic therapyforadvancedurothelialcarcinoma.J Urol. 2015. doi:10.1016/j.juro.2015.07.111.
60. Papamichael D, Gallagher CJ, Oliver RT, Johnson PW,Waxman J.Phase II study of paclitaxel in pretreated patients with locallyadvanced/metastatic cancer of the bladder and ureter. Br JCancer. 1997;75(4):606–7.
61. JolyF,HouedeN,NoalS,ChevreauC,PriouF,Chinet-CharrotP, etal.Do patients with advanced urothelial carcinoma benefit fromweeklypaclitaxel chemotherapy? AGETUG phase II study. Clin GenitourinCancer. 2009;7(2):E28–33. doi:10.3816/CGC.2009.n.018.
62. Vaughn DJ, Broome CM, HussainM, Gutheil JC, Markowitz AB.Phase II trial of weekly paclitaxel in patients with previously treat-ed advanced urothelial cancer. J Clin Oncol. 2002;20(4):937–40.
63. McCaffrey JA, Hilton S,MazumdarM, Sadan S, KellyWK, ScherHI, et al. Phase II trial of docetaxel in patients with advanced ormetastatic transitional-cell carcinoma. J Clin Oncol. 1997;15(5):1853–7.
64. Choueiri TK, Ross RW, Jacobus S, Vaishampayan U, Yu EY,Quinn DI, et al. Double-blind, randomized trial of docetaxel plusvandetanib versus docetaxel plus placebo in platinum-pretreatedmetastatic urothelial cancer. J Clin Oncol. 2012;30(5):507–12.doi:10.1200/jco.2011.37.7002.
65. Witte RS, Elson P, Bono B, Knop R, Richardson RR, Dreicer R, etal. Eastern Cooperative Oncology Group phase II trial ofifosfamide in the treatment of previously treated advancedurothelial carcinoma. J Clin Oncol. 1997;15(2):589–93.
66. Lorusso V, Pollera CF, Antimi M, Luporini G, Gridelli C,Frassineti GL, et al. A phase II study of gemcitabine in patientswith transitional cell carcinoma of the urinary tract previously
27 Page 10 of 12 Curr Oncol Rep (2016) 18:27

treated with platinum. Italian Co-operative Group on BladderCancer. European journal of cancer (Oxford, England : 1990).1998;34(8):1208–12.
67. KoYJ, Canil CM,Mukherjee SD,Winquist E, Elser C, EisenA, etal. Nanoparticle albumin-bound paclitaxel for second-line treat-ment of metastatic urothelial carcinoma: a single group,multicentre, phase 2 study. Lancet Oncol. 2013;14(8):769–76.doi:10.1016/s1470-2045(13)70162-1.
68. Sweeney CJ, Roth BJ, Kabbinavar FF, Vaughn DJ, Arning M,Curiel RE, et al. Phase II study of pemetrexed for second-linetreatment of transitional cell cancer of the urothelium. J ClinOncol. 2006;24(21):3451–7. doi:10.1200/jco.2005.03.6699.
69. Galsky MD, Mironov S, Iasonos A, Scattergood J, Boyle MG,Bajorin DF. Phase II trial of pemetrexed as second-line therapyin patients with metastatic urothelial carcinoma. Invest NewDrugs. 2007;25(3):265–70. doi:10.1007/s10637-006-9020-9.
70. Witte RS, Manola J, Burch PA, Kuzel T, Weinshel EL, Loehrer SrPJ. Topotecan in previously treated advanced urothelial carcino-ma: an ECOGphase II trial. Invest NewDrugs. 1998;16(2):191–5.
71. Culine S, Theodore C, De Santis M, Bui B, Demkow T, Lorenz J,et al. A phase II study of vinflunine in bladder cancer patientsprogressing after first-line platinum-containing regimen. Br JCancer. 2006;94(10):1395–401. doi:10.1038/sj.bjc.6603118.
72. Vaughn DJ, Srinivas S, Stadler WM, Pili R, Petrylak D, SternbergCN, et al. Vinflunine in platinum-pretreated patients with locallyadvanced or metastatic urothelial carcinoma: results of a largephase 2 study. Cancer. 2009;115(18):4110–7. doi:10.1002/cncr.24460.
73. Sternberg CN, Calabro F, Pizzocaro G, Marini L, Schnetzer S,Sella A. Chemotherapy with an every-2-week regimen ofgemcitabine and paclitaxel in patients with transitional cell carci-noma who have received prior cisplatin-based therapy. Cancer.2001;92:2993–8.
74. Pectasides D, Aravantinos G, Kalofonos H, Kiamouris C,Bafaloukos D, Xiros N, et al. Combination chemotherapy withgemcitabine and ifosfamide as second-line treatment in metastaticurothelial cancer. A phase II trial conducted by the HellenicCooperative Oncology Group. Annals of oncology: official jour-nal of the European Society for Medic al Oncology/ESMO.2001;12:1417–22.
75. Sonpavde G, Sternberg CN, Rosenberg JE, Hahn NM, GalskyMD, Vogelzang NJ. Second-line systemic therapy and emergingdrugs for metastatic transitional-cell carcinoma of the urothelium.Lancet Oncol. 2010;11(9):861–70. doi:10.1016/s1470-2045(10)70086-3.
76. Bambury RM, Benjamin DJ, Chaim JL, Zabor EC, Sullivan J,Garcia-Grossman IR, et al. The safety and efficacy of single-agent pemetrexed in platinum-resistant advanced urothelial carci-noma: a large single-institution experience. Oncologist.2015;20(5):508–15. doi:10.1634/theoncologist.2014-0354.
77. SonpavdeG,PondGR,ChoueiriTK,MullaneS,NiegischG,AlbersP,et al. Single-agent taxane versus taxane-containing combination che-motherapy as salvage therapy for advanced urothelial carcinoma. EurUrol. 2015. doi:10.1016/j.eururo.2015.07.042.
78.•• Comprehensive molecular characterization of urothelial bladdercarcinoma. Nature. 2014;507(7492):315-22. doi:10.1038/nature12965. Integrated analysis of 131 urothelial carcinomatumors demonstrating that 69% of tumors have potentiallyactionable molecular alterations
79. Petrylak DP, Tangen CM, Van Veldhuizen Jr PJ, Goodwin JW,Twardowski PW, Atkins JN, et al. Results of the SouthwestOncology Group phase II evaluation (study S0031) of ZD1839 foradvanced transitional cell carcinoma of the urothelium. BJU Int.2010;105(3):317–21. doi:10.1111/j.1464-410X.2009.08799.x.
80. Pruthi RS, Nielsen M, Heathcote S, Wallen EM, Rathmell WK,Godley P, et al. A phase II trial of neoadjuvant erlotinib in patients
with muscle-invasive bladder cancer undergoing radicalcystectomy: clinical and pathological results. BJU Int.2010;106(3):349–54. doi:10.1111/j.1464-410X.2009.09101.x.
81. Wulfing C, Machiels JP, Richel DJ, Grimm MO, Treiber U, DeGroot MR, et al. A single-arm, multicenter, open-label phase 2study of lapatinib as the second-line treatment of patients withlocally advanced or metastatic transitional cell carcinoma.Cancer. 2009;115(13):2881–90. doi:10.1002/cncr.24337.
82. WongYN, Litwin S, VaughnD, Cohen S, Plimack ER, Lee J, et al.Phase II trial of cetuximab with or without paclitaxel in patientswith advanced urothelial tract carcinoma. J Clin Oncol.2012;30(28):3545–51. doi:10.1200/jco.2012.41.9572.
83. Hussain M, Daignault S, Agarwal N, Grivas PD, Siefker-RadtkeAO, Puzanov I, et al. A randomized phase 2 trial of gemcitabine/cisplatin with or without cetuximab in patients with advancedurothelial carcinoma. Cancer. 2014;120(17):2684–93. doi:10.1002/cncr.28767.
84. Junker K, van Oers JM, Zwarthoff EC, Kania I, Schubert J,Hartmann A. Fibroblast growth factor receptor 3 mutations inbladder tumors correlate with low frequency of chromosome al-terations. Neoplasia. 2008;10(1):1–7.
85. Gallagher DJ, MilowskyMI, Gerst SR, Ishill N, Riches J, RegazziA, et al. Phase II study of sunitinib in patients with metastaticurothelial cancer. J Clin Oncol. 2010;28(8):1373–9. doi:10.1200/jco.2009.25.3922.
86. Bellmunt J, Gonzalez-Larriba JL, Prior C, Maroto P, Carles J,Castellano D, et al. Phase II study of sunitinib as first-line treat-ment of urothelial cancer patients ineligible to receive cisplatin-based chemotherapy: baseline interleukin-8 and tumor contrastenhancement as potential predictive factors of activity. AnnOncol. 2011;22(12):2646–53. doi:10.1093/annonc/mdr023.
87. Sridhar SS,Winquist E, Eisen A, Hotte SJ, McWhirter E, TannockIF, et al. A phase II trial of sorafenib in first-line metastaticurothelial cancer: a study of the PMH Phase II Consortium.Invest New Drugs. 2011;29(5):1045–9. doi:10.1007/s10637-010-9408-4.
88. Dreicer R, Li H, SteinM, DiPaola R, EleffM, Roth BJ, et al. Phase2 trial of sorafenib in patients with advanced urothelial cancer: atrial of the Eastern Cooperative Oncology Group. Cancer.2009;115(18):4090–5. doi:10.1002/cncr.24467.
89. Necchi A, Mariani L, Zaffaroni N, Schwartz LH, Giannatempo P,Crippa F, et al. Pazopanib in advanced and platinum-resistanturothelial cancer: an open-label, single group, phase 2 trial. LancetOncol. 2012;13(8):810–6. doi:10.1016/s1470-2045(12)70294-2.
90. Petrylak D, Tagawa ST, KohlM, Eisen A, Canil CM, Sridhar SS etal. Three-arm phase II randomized trial of docetaxel monotherapyor combined with ramucirumab or icrucumab in second-line lo-cally advanced or metastatic urothelial carcinoma. Abstract 2508(Presented at European Cancer Congress 2015).
91. Seront E, Rottey S, Sautois B, Kerger J, D’Hondt LA, VerschaeveV, et al. Phase II study of everolimus in patients with locallyadvanced or metastatic transitional cell carcinoma of the urothelialtract: clinical activity, molecular response, and biomarkers. AnnOncol. 2012;23(10):2663–70. doi:10.1093/annonc/mds057.
92. Milowsky MI, Iyer G, Regazzi AM, Al-Ahmadie H, Gerst SR,Ostrovnaya I, et al. Phase II study of everolimus in metastaticurothelial cancer. BJU Int. 2013;112(4):462–70. doi:10.1111/j.1464-410X.2012.11720.x.
93. WagleN,GrabinerBC,VanAllenEM,HodisE,JacobusS,SupkoJG,et al. Activating mTOR mutations in a patient with an extraordinaryresponse on a phase I trial of everolimus and pazopanib. Cancer dis-covery. 2014;4(5):546–53. doi:10.1158/2159-8290.cd-13-0353.
94. Quinn DI, Ruel N, Twardowski P, Groshen SG, Dorff TB, Pal SK,et al. Eribulin in advanced urothelial cancer (AUC) patients (pts): aCalifornia Cancer Consortium trial—NCI/CTEP 7435. ASCOMeeting Abstracts. 2015;33(15_suppl):4504.
Curr Oncol Rep (2016) 18:27 Page 11 of 12 27

95. Herbst RS, Gordon MS, Fine GD, Sosman JA, Soria J-C, HamidO et al. A study of MPDL3280A, an engineered PD-L1 antibodyin patients with locally advanced or metastatic tumors. ASCOMeeting Abstracts. 2013;31(15_suppl):3000.
96.•• Powles T, Eder JP, Fine GD, Braiteh FS, Loriot Y, Cruz C, et al.MPDL3280A (anti-PD-L1) treatment leads to clinical activity inmetastatic bladder cancer. Nature. 2014;515(7528):558–62. doi:10.1038/nature13904. Anti-PD-L1 MPDL3280 has activity inmetastatic bladder cancer with several durable responses ina phase I study.
97. Petrylak DP, Powles T, Bellmunt J, Braiteh FS, Loriot Y, CruzZambrano C, et al. A phase Ia study of MPDL3280A (anti-PDL1): updated response and survival data in urothelial bladdercancer (UBC). ASCO Meeting Abstracts. 2015;33(15_suppl):4501.
98. PlimackER,Bellmunt J,Gupta S,BergerR,MontgomeryRB,HeathK, et al. Pembrolizumab (MK-3475) for advanced urothelial cancer:updated results andbiomarker analysis fromKEYNOTE-012.ASCOMeetingAbstracts. 2015;33(15_suppl):4502.
99. Galsky MD, Hahn NM, Albany C, Fleming MT, Starodub A,Twardowski P, et al. Phase II trial of gemcitabine + cisplatin +ipilimumab in patients with metastatic urothelial cancer. ASCOMeeting Abstracts. 2016;34:357.
100. Hajdenberg J, Landau D, Vaena DA, Fishman MN, Rosser CJ,Milhem MM, et al. Early outcome results of a phase I/II studyfor an IL-2/T-cell receptor fusion protein in combination withgemcitabine and cisplatin (GC) in patients with locally advanced
or metastatic urothelial cancer. ASCO Meeting Abstracts.2012;30(15_suppl):e15010.
101. Snyder A, Makarov V, Merghoub T, Yuan J, Zaretsky JM,Desrichard A, et al. Genetic basis for clinical response toCTLA-4 blockade in melanoma. N Engl J Med. 2014;371(23):2189–99. doi:10.1056/NEJMoa1406498.
102. Alexandrov LB, Nik-Zainal S, Wedge DC, Aparicio SA, BehjatiS, Biankin AV, et al. Signatures of mutational processes in humancancer. Nature. 2013;500(7463):415–21. doi:10.1038/nature12477.
103.•• Damrauer JS, Hoadley KA, Chism DD, Fan C, Tiganelli CJ,Wobker SE, et al. Intrinsic subtypes of high-grade bladder cancerreflect the hallmarks of breast cancer biology. Proc Natl Acad Sci US A. 2014;111(8):3110–5. doi:10.1073/pnas.1318376111. Thereare molecular subtypes of bladder cancer that resemble thesubtypes of breast cancer including Bbasal^ and Bluminal^subtypes. These subtypes have distinct RNA expressionprofiles and appear to be prognostic of clinical outcome.
104.•• ChoiW, Porten S, Kim S, Willis D, Plimack ER, Hoffman-CensitsJ, et al. Identification of distinct basal and luminal subtypes ofmuscle-invasive bladder cancer with different sensitivities to front-line chemotherapy. Cancer Cell. 2014;25(2):152–65. doi:10.1016/j.ccr.2014.01.009. There are molecular subtypes of bladdercancer with distinct RNA expression profiles that appear tobe prognostic of clinical outcome. The basal subtype isenriched for biomarkers reflective of immune infiltration,potentially suggesting a predictive role for immunotherapy.
27 Page 12 of 12 Curr Oncol Rep (2016) 18:27