2-malchow-outpatient spinals and epidurals-handout
TRANSCRIPT

DISCLOSURE:
I have no disclosures to report regarding financial incentives or gains from pharmaceutical companies or manufacturers.
INTRODUCTION
Beyond “Marcaine Spinals” vs GAPerioperative physicians/providersPatient’s perceptions and preferences (Shevde, 1991, 800
pts)70% General anesthesia20% Local10% “Spinal”/Epidural
Patient Satisfaction > 90% after CNBSignificant Benefits with Reg Anes
REGIONAL ANALGESIA-IMPROVEMENT IN
OUTCOME Decreased-GA side effects/ complicationsOpiate Side EffectsBlood Loss, DVTLOS, Hosp CostIleus, constipation, N/VStress Response Chronic PainMI, ischemiaPulmonary ComplicationsPOCD, POD?
Improved-OR Efficiency PACU Recovery and rehabPost-op Analgesia Patient SatisfactionSurgeon Satisfaction
High EfficiencyIntraop and Postop
High Success Rates
Low Complication RatesIntraop and Postop
High Patient / Surgeon Satisfaction
GOALS FOR CNB IN AMBULATORY PATIENTS
I. HIGH EFFICIENCY
Intraoperative EfficiencyPostoperative RecoveryLocal Anesthetic and DoseSpinal EpiduralAnesthesia TechniqueGA vs CNB Spinal vs Epidural
Malchow, Randall, MD Outpatient Spinals and Epidurals

ACT (Anesthesia Controlled Time) I: In OR – Turn Over To
Surgeon (TOTS)preoxygenation/ Induction/
Airway Management II: Dressing On – Out of ORemergence/ Extubation/ LMA
Removal
Spinals - quick block time (ave 7min) and
onset time can be comparable to GA (ACT I)
Epidurals - placement of catheter in block room
(initiate low dosing in block room) consider alkalinize solution consider fast onset agent CP: sets up 8min faster than Lido
consider CSE (if in OR and/or uncertain surgical duration) consider dose thru needle technique
(if in OR)
Both techniques eliminate emergence/extubation time (ACTII)
EFFICIENCY INTRAOPSPINAL RECOVERY
DOSE-RESPONSE
Surg Type
Drug Dose
mg
Baricity Motor Blk
Time Disch
Author
Knee Scope
Bupiv 5 Hyper 181* Lui
19967.5 202
10 260
15 471
Knee
Scope
Lido 40 Iso 93 178 Urmey
199560 128 216
80 142 214
DURATION WITH HYPERBARIC BUPIVACAINE
LIU, 1996
Measurement: Duration:
Duration of Surgical Anesthesia
Umbilicus 5 min/mg
Knee 13 min/mg
Ankle 15 min/mg
Achievement of Discharge Criteria 21 min/mg
SPINAL CHLOROPROCAINE-IDEAL AGENT?
History:1951: 1st SAB w/ chloroprocaine; 214 pt series in 19521980: Neurotoxicity case series (8): due to sod bisulfite/low pH1987: Low back pain concerns. Due to EDTA.
1996: New PF/antioxidant free CP:No known neurotoxicity not FDA approved for SAB use; “off-label”(nor is isobaric bupiv or lidocaine, fentanyl)Use only preparations in “brown vials”:Bedford Labs, generic CPAstra Zeneca, “Nesacaine-MPF”; pH= 2.7-4.0(Avoid Abbott, clear vial, with sodium bisulfate)
SPINAL CHLOROPROCAINE
30-60mg dose range (40mg most common)40-50mg: 45-70min60mg: 60-90min< duration compared to lidocaine
<< duration comp to bupivacaine
Casati, 2007 CP- 50mg Lidocaine-50mg
Motor (min) 60 100
Sensory (min) 95 120
Ambulation (min) 103 152
Lacassee, 2011 CP- 40mg Bupivacaine- 7.5
Motor (min) 76 119
Sensory (min) 146 329
Discharge (min) 76 min faster for CP
SPINALS:CP 40MG
LIDO 40MG BUPIV 7.5MG
(ALL ISOBARIC)
CP
CP
< duration CP vs lidocaine. 104 vs 134min for d/c criteria
<< duration CP vs Bup113 vs 191min for d/c criteria
Kouri, 2004; Yoos, 2005; Casati, 2007
Lido
Bupiv
Malchow, Randall, MD Outpatient Spinals and Epidurals

ADJUNCTS (NON-OPIOID) WITH SPINALS/EPIDURALS
E P I N E P H R I N E :
20-50% > in duration (esplido and tetracaine)Greater effect on Time to
Discharge than blk durationPoor Recovery Profile
(Urmey, 1996)added 81 min to Time to
Ambulationadded 106 min to Time to
DischargeRecommendation: Avoid
C L O N I D I N E :
Dose: 15-30ugEven 15ug > motor/sens
durationHigh Cost in U.S.10ml SD vial (1000ug)Europe has low dose vialsHigh dose (1-2mcg/kg):
hypotension, bradycardia, sedationRecommendation: Avoid
EPIDURAL-RECOVERY2CP VS LIDOCAINE VS MEPIVACAINE
Kopacz, 1990
CP Lido Mepiv
2 CHLOROPROCAINE-EPIDURAL ADVANTAGES
Rapidly Metabolized t1/2 = 25sec“no significant plasma concentration”More “titratable” due to short durationRapid RecoveryReady for discharge one hour earlier compared to lido (Neal)Lidocaine may double discharge time comp to CP< time to void
EFFICIENCY OF EPIDURAL VS GA
48 Knee Arthroscopy (Epidural vs GA vs SAB)
Epidural, 2CPGA/LMA, Prop/N2O/Fent Spinal, Procaine 75/ Fent 20mcg
All IA Bupiv
All IV Toradol
Upshot: CLE and GA:Similar discharge times (92 vs
104min)Spinal? Interpret due to procaine useslowest recovery, 146min> nausea and pruritis
Epidural Washout:10-20ml of N.S. in pacuRecovered 48min sooner (Lido/epi)Malchow, anecdotal: appears
helpful
Mulroy, 2000; DiFazio, 1997.
EFFICIENCY OF SPINAL VS GA
84 Knee ArthroscopySpinal: Lido 50mgGA/LMA:Propofol/N20/Fent
Similar discharge times (120 min) and pt sat
Spinal:< PACU pain> backache (35 vs 13%)
GA:>Sore throat, drowsiness, pain
< Costs w/ RA:2o to < pacu time, nsg
interventions, and unplanned admissionsConsider spinals early in day
Wong, 2001; Williams, 2005
Consider entering OR 5 min sooner if possible for possibly difficult pts
COMBINED SPINAL EPIDURAL
Capitalize advantages from eachFast onset< hemodynamic changes TitratableMinimize disadvantages from eachSlow onset w/ epiduralsAvoid sacral sparing/patchy blk from epiduralSlow recovery from lg spinal dose
Malchow, Randall, MD Outpatient Spinals and Epidurals

EFFICIENCY OF EPIDURAL VSSPINAL
63 Knee Arthroscopy30 Epidural: 2CP-3% x 15ml33 Spinal:Lido 25mgFentanyl 20 mcgDextrose
Similar failure rate (10%)
Similar Discharge Times (152 vs 142 m)
Similar satisfaction scores (>90%)
Nashville Surg Ctr:
Epidural-CP quicker recover than Spinal-L
Pollock, 2003
II. SUCCESS RATES:
EpiduralsAdjuncts
Why do they Fail?
SpinalsDose responseBaricityAdjuncts
REASONS FORCNB FAILURE
Poor patient selectionNeedle/orifice not in spaceSlow onsetInadequate / low doseTourniquet painMaldistribution of local
anesthetics (caudal aperture of pencil-ptneedles)
Unilateral blocks
Lengthy surgeryInexperienced surgeonsSubdural injectionsAbnormal anatomyCyst formation in
interspinous ligamentsOther
LIDOCAINE SPINALSDOSE-SUCCESS
(40MG LOWEST SUCCESSFUL DOSE W/O ADJUNCTS)
Surg Type
Bari-city
Dose Adjunct Failure Rate
Com-ments
Author
Knee Scope
Iso 80 3%
Urmey
199540 10
30 100
Knee Scope
Hyper 25 Fent 20 9% IA Bupiv
Pollock2003
20 Fent 20 0 Ben-David
2001
BUPIVACAINE SPINALDOSE-SUCCESS
(7.5MG DOSE LOWEST SUCCESSFUL DOSE W/O ADJUNCTS)
Surg Type
Bari-
city
Dose Adjunct Failure Rate
Com-ments
Author
Knee
Scope
Hyper 7.5 0% Ben-
David5 Fent 10 0
4-5 24
Knee Hyper 4-6 2-6% SSA Valanne
Hernia Hyper 6 Clon 15 0% SSA Dobryd-njon33
Hernia Hyper 6 Fent 25 5% Gupta
Alternative to CP or Lido spinals (knee scope, IHR)
with “low dose, low volume, low flow”
Local Anesthetic: usually hyperbaric bupivacaine (4-6mg)
Ipsilateral side down
Pencil point needle, aperture towards ipsilat side, slow injection (1-2min)
Maintenance of posn 10-15min (block room)
Results in < motor and sensory duration on contralateral side (Fig)
Quicker Recovery
home readiness 15min < than GA
> pt sat than GA
< Urinary retention
CONSIDER SELECTIVE SPINAL ANESTHESIA?
Enk, 1998 Valanne, 2001 DobrydnjovKorhonen, 2004Capelleri, 2005 Mulroy, 2005
Malchow, Randall, MD Outpatient Spinals and Epidurals

BARICITY CHOICE
Hyperbaric: sacral roots or extensive spread importantIsobaric: > duration; LE/groin/GU surgeryHypobaric: jack-knife posn (lido 20-40)Spread: also depend on dose and direction of orifice
Urmey, ‘03
PERI-RECTAL CASES- “SADDLE” BLOCKS
For Jack-Knife Cases: - Use Reverse T-burg for needle placement, then use T-burg for hypobaric LA (Lido 20-40mg)(or sitting pos’n for placement with hyperbaric, then wait 10 min)
For Lithotomy- Perirectal cases:- Consider Saddle block hyperbaric, low dose LA (Lido 20-30mg or Bupiv 3-
5mg)
MEPIVACAINE SPINAL FOR OUTPTKNEE SURGERY
(60) ACL ptsIsobaric mepiv 1.5%60 vs 80mgPros, RCT, DBEpidural
Supplementation: 12% in 60mg grp 3% in 80mg grp
L1 Regression: 146 min vs 159 min
Knee Scopes:M-30mg + F10 vs M-40mg
Other Estimates: Other: 40-50mg = 90-120min
surgical anesthesia 45mg = 220min for discharge
readiness
Pawlowski, 2000; YaDeau, 2005; O’Donnell, 2010
M30 + F10 M40
Sensory (min): 118 170
Ambulation (min): 176 206
Ropivacaine 50% spinal potency
compared to bupiv or levobupiv same recovery profile as
bupivacaine (> 3hr dischtimes) (1 study of volunteers
demonstrated 14min/mg for Time of Discharge)No advantage over bupiv
Levobupivacaine similar potency to bupiv same recovery profile as
bupivacaine (> 3 hr dischtimes) (1 study w/ hypobaric LB-4
or 5mg w/ Fent 10ug = 90 and 132min Time of Discharge for knee scopes)No advantage over bupiv
OTHER SPINAL LOCAL ANESTHETICSMcDonald, 1999, Capelleri, 2005, O’Donnell, 2008; DeSantiago, 2009; DeSantiago, 2011
ProcaineOlder drug, short actinghigh failure rate (17%)10% solution; 60-
100mgprolonged discharge increased n/v, pruritisRecommendation:
Avoid
Prilocaine avail in Europe (not U.S.) high failure rate w/o fentanyl high rate of POUR (up to
25%)Recommendation: Avoid Articaine older drug, used in dentistry dosing: 60, 72. 84 mg similar duration of lido some concern with
neurotoxicityRecommendation: Avoid
OTHER SPINAL AGENTSArticaine: Forster, 2011; Kallio, 2006; O’Donnell, 2010; Bachmann, 2012
Prilocaine: Forster, 2011; Hendricks, 2009; Campanovo, 2010; Black 2011
SPINAL/EPIDURAL OPIOIDS
Synergistic effect with local anesthetics
Increased intensity/quality of block
Critical with low dose spinals
Pruritis: 30-100% Dose dependent
Recovery: No effect on motor block, nausea No effect on time to void,
discharge
Spinal DosesFentanyl 10-25mcgSufentanil 2.5-5.0mcg
Epidural DosesFentanyl 3-5mcg/ml0.5-1 mcg/kg/hr (inpts)Sufentanil 0.5mcg/ml
NSC: we avoid opiates
Malchow, Randall, MD Outpatient Spinals and Epidurals
SUCCESS - SPINALS
90-95% averageNSC: 92.%
Higher failure rate with pencil point needles
Select drug, dose, adjunct, baricity for each procedure, surgeon
Higher success than epidural s/p lumbar fusion
Ensures sacral coverage more reliably
Consider 22gu quincke for patients > 50 yo
Opioid critical at low doses
IMPROVING SUCCESS- EPIDURALS
85-90% averageNSC: 91.5%
Block Room important
Place Epidural at Epicenter of incision
Confirmation of Epidural Space30% false positive rate with LOR10% false positive rate with ease of cath advancement p LOR
Avoid catheter advancement beyond 5cm
Consider use of CP, quicker onset (NSC CP 94%)
Consider opiate adjunct for synergy/ > quality
III. MINIMIZING CNB COMPLICATIONS
(INTRAOPERATIVE)
Hypotension
Bradycardia
Cardiac Arrest
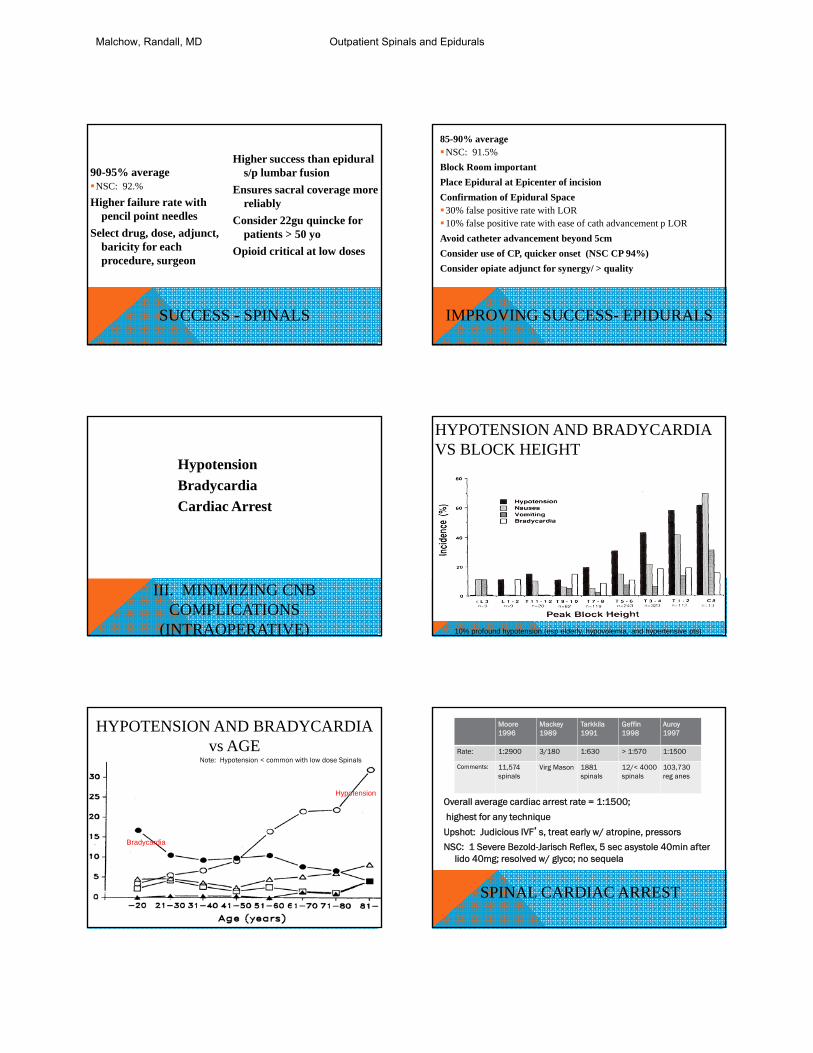
HYPOTENSION AND BRADYCARDIAVS BLOCK HEIGHT
10% profound hypotension (esp elderly, hypovolemia, and hypertensive pts)
HYPOTENSION AND BRADYCARDIAvs AGE
Bradycardia
Hypotension
Note: Hypotension < common with low dose Spinals
SPINAL CARDIAC ARREST
Overall average cardiac arrest rate = 1:1500;
highest for any technique
Upshot: Judicious IVF’s, treat early w/ atropine, pressors
NSC: 1 Severe Bezold-Jarisch Reflex, 5 sec asystole 40min after lido 40mg; resolved w/ glyco; no sequela
Moore1996
Mackey1989
Tarkkila1991
Geffin1998
Auroy1997
Rate: 1:2900 3/180 1:630 > 1:570 1:1500
Comments: 11,574 spinals
Virg Mason 1881 spinals
12/< 4000 spinals
103,730 reg anes
Malchow, Randall, MD Outpatient Spinals and Epidurals

III. MINIMIZING COMPLICATIONS(POST-OPERATIVE)
EarlyN/VUrinary Retention (POUR)
LatePDPHBackache Transient Radicular Irritation
NAUSEA AND VOMITING
PNB: < 5 %Epidural: 3-9%NSC: Nausea 11%, Vomiting 0%Spinal: 12-18%NSC: Nausea 10%, Vomiting 3%GA: 13-32%Mechanism: unopposed vagal activityEpinephrine associated with incr. N/VLipophylic opioids do not significantly incr. N/VAvoid opiates if possible (use of multimodal, pnb if appropriate)Antiemetics prn
POUR: SPINALS AND EPIDURALS
S P I N A L S :3-35% Incidence overall Depends on dose, adjuncts 3-4% for CP, lidocaine NSC: No POUR
Urge to void disappears immediately
Causes: overdistension of bladder/bladder
neck edema (ie > 600ml) urinary sphincter spasm
(pain/anxiety) bed confinement epinephrine: incr. time to void by
81min
E P I D U R A L S :
Low incidence 1% Similar to GA for CP, Lidocaine NSC: No POUR
Time to void (Kopacz, 1990): CP: 211 min Lido: 235 minMepiv: 308 min
URINARY TRACT NEUROANATOMY
*
Spinal anes blocks both afferent and efferent innervation to bladder fxn
URINARY RETENTION-SPINALKAMPHUIS, 1998
Hyperbaric 100mg
Hyperbaric 10mg
1=motor resolution2=detrusor resolution
Lasts until regression to S3
Consider epidural (esp CP) for higher risk pts (IHR)
Avoid excess IVFs< 1000 ml if possibleEarly use of ephedrine prn
Consider SSA
Local Anesthetics: Short acting LA-spinalsLow dose bupiv
Adjuncts:Avoid epinephrine, clonidineLipophylic opiates, esp w/ low
dose bupiv acceptableLimit opiate dose
Low threshold for catheterization (see algorithm)
Encourage sitting/walking asap
URINARY RETENTIONPREVENTION
Malchow, Randall, MD Outpatient Spinals and Epidurals

POUR ALGORITHM:
High Risk Group: 5% POUR w/ GA
Hernia, Pelvic, Perirectal > 70 yo H/o POUR, BPH
Low Risk Group: No epinephrine or
clonidine, bupiv < 7.5 or short acting agents (CP, Lido) If not high risk group
Ben-David, 2001; Pavlin, 1999; Mulroy, 2002; Mulroy 2012
Condition: Action:
High Risk:
Not Voided w/i 60 min
Check BUS
BUS > 600ml In/out cath, thenDischarge or further obs
BUS < 600ml Wait add’l 60min and repeat
Low Risk: Discharge w/ low risk pts or BUS < 400ml; Instruct to return to ER w/i 8 hrs if no void
ESTIMATING BLADDER VOLUME:
Curvilinear ProbeProlate Ellipsoid EquationVol = lgth x width x hgt x 0.52 = (9.77 x 11.6 x 15.2) x 0.52= 895 ml
11.66 cm
9.77 cm
15.2 cm
Transverse View
SagittalView
LATE COMPLICATIONS:POST-DURAL PUNCTURE HEADACHE
FactorsAge, needle, guage, bevel orientation
Pencil-point important for younger patients
27gu/30gu offer little advantage
Equivalent risk: SAB vs CLE vs CSE 1-2% ave incidence w/ pencil pt needlesNSC: SAB: 2.1%; Epid: 2.1%CLE and wet-tap (4%): bevel parallel 30% incidence vs bevel
perpendicular 75%
LATE COMPLICATIONS: BACK PAIN
Chloroprocaine Still some assoc
with high volume (>25ml)
Consider Rare Complications
Epid hematoma in healthy 35yo knee scope w/ excruciating LBP 2hrs post-disch(Gilbert, 2001)
Duration of Surgery: (hr) Incidence of LBP: (%)
0-1 18
2-3 24
3-4 34
4-5 50
Technique: Incidence of LBP: (%)
Spinal 21
Epidural 30
General Anesthesia 19
Brown 1961; Finucaine, 1999; Gilbert, 2001
NSC: 4.2% LBP after Epidural
TRANSIENT NEUROLOGICAL SYNDROMETRANSIENT RADICULAR IRRITATION
POST-SPINAL MUSCULOSKELETAL SYNDROME
Description:Dysesthesias to buttocks, LE’s, 1-
4 days, w/ nml PE
Incidence: lido 70-100mg 16-80%<60mg 1-3%NSC: 0.5%mepiv 16-30% bupiv 3-13%CP rare
Epinephrine:animal studies: > sens deficits
comp to plain little reason to add to lidocaine
Increased Incidence:Obesity, lith posn, outpts
No significant role:GlucoseConcentration of LABaricityDoseAge
REASONS TO CONSIDER CONTINUED LIDOCAINE USE
Flawed studies- lack of random, sml studies
Phillips, 1969: 10,440 ptsw/ 5% lidocaine
40-100mg dose, mainly obstetrics 0.3% “TRI” type symptoms
Wong, 1999: 0% incidence in C/S pts
Malchow, NSC series:No reports of TNS
If present, “transient” w/o deficits
neg emg, ncv, ssep studies>40 years before 1st case
reportBack pain: common
regardless of anesthesiaPosition probably more impt
issue (Lith)If concerned, discuss w/ pt
and use lido < 60mg
Malchow, Randall, MD Outpatient Spinals and Epidurals

IV. HIGH PATIENT/SURGEON SATISFACTION
Dependent on:EfficiencyHigh Success RateLow Complication
Rate
If these 3 conditions met, Goal IV will be achieved as well.
Jankowski, LPB vs spinal vsGA for knee scope. AA, 2003
Techniques:GA- Prop/Fent/LMASAB- B6, F15LPB- M1.5% w/ epiGA had lowest pt satisfaction
scores and higher postop painSAB and LPB similar
NSC Pat Satisfaction for both Epidural/Spinals: V.G.-Excellent: 97%, Good: 3%; Poor/Fair: 0%
Anesthesia for Knee Scope
GA-LMASAB/
Epidural
Leg Block (LPB-
LE/Sci-CP)
Pro:
Con:
“Asleep”Easier
PONV (30%)Delirium/ opiatesSore throatPainAspiration risk
PDPH 2%< BP, HRFear of “spinal”Possible prolonged recoveryBack pain (30%)
Able to observeSuccess (95%)PONV 10-20%
Good recoveryUnilateral blockHemodyn stabilityMin PONV (5%)
Procedure pain> Failure (10-20%)Epidural spread 5%LAST 1:1000 LPB
- Young, anxious, desires to be asleep
- Would like to avoid GA and CNB- Wants to watch?
- h/o PONV?- ? >40 yo?
SUMMARY OF OUTPATIENT SPINALS AND EPIDURALS
High Efficiency Possible: Intraop and Postop Esp w/ use of block room (epid) Short-acting agents (CP, Lido) Consider SSA, low dose
bupiv/opiate
Adjuncts: Avoid epinephrine, clonidine Lipophyllic opiates acceptable
High Success Rates PossibleConsider CNB/ PNB when
appropriate (ACL)
Minimize Complications Bradycardia, Cardiac Arrest PONV Urinary Retention – algorithm PDPH Backache TNS
High Patient / Surgeon Satisfaction
SELECT REFERENCES:
Campanovo et al. A Prospective Double Blinded RCT Comparing the Efficacy of 40mg and 60mg Hyperbaric and Isobaric 2% Prilocaine for Intrathecal Anesthesia in the Ambulatory Surg. A&A. 2010; 111: 568-72.
Choi et al. Neuraxial anesthesia and Bladder Dysfunction in the Perioperative Period: A Systematic Review. CJA. 2012; 59;681-703.
Casati et al. Spinal Anesthesia with Lidocaine or Prev Free 2-Chloroprocaine for Outpatient Knee Arthroscopy. A&A. 2007; 104:959-64.
Forster. Revival of Old Local Anesthetics for Spinal Anesthesia in Ambulatory Surgery. Curr Opn Anes. 2011; 24:633-7.
Forster. Short-acting Spinal Anesthesia in the Ambulatory Setting. Curr Opn Anes; 2014; 27:597-604.
Goldblum et al. The use of 2-Chloroprocaine for Spinal Anesthesia: A Review. Acta Anaesth Scand. 2013; 57: 545-552.
Korkonen et al. A Comparison of Selective Spinal Anesthesia with Hyperbaric Bupivacaine and General Anesthesia with Desflurane for Outpatient Knee Arthroscopy. A&A. 2004; 99: 1668-73.
Lacasse M. Comparison of Bupivacaine and 2-Chloroprocaine for Spinal Anesthesia for Outpatient Surgery. C Jnl Anesth. 2011; 58:384-391.
Mulroy et al. Managemetn of Bladder Volumes When Using Neuraxial Anesthesia. Intl Anes Clin. 2012; 50: 101-110.
O’Donnell et al. Reg Anes Techniques for Ambulatory Orthopedic Surg. Curr Opn Anes. 2008; 21: 723-8.
Santiago et al. Low Dose Low Concentration Levobupivacaine Plus Fentanyl Selective Spinal Anesthesia for Knee Arthroscopy: A Dose Finding Study. A&A 2011; 112: 477-80.
Williams et al. Reg Anes Procedures for Ambulatory Knee Surgery: Effects on In-Hosp Outcomes. Intl Anes Clin. 2005.
Malchow, Randall, MD Outpatient Spinals and Epidurals