20 the role of surgery for intracranial mass lesions … · intracranial mass lesions after head...
TRANSCRIPT

20 THE ROLE OF SURGERY FORINTRACRANIAL MASS LESIONSAFTER HEAD INJURY
Nigel Jones, Ross Bullock and Peter Reilly
20.1 Introduction
Many uninformed neurosurgeons have regarded sur-gery for post-traumatic intracranial hematomas asunrewarding. This pessimism is based on the belief thatoutcome is determined principally by the magnitude ofthe initial injury and, therefore, frequently remainspoor despite optimal surgery. In fact, management ofpost-traumatic epidural hematoma is one of the most‘cost-effective’ of neurosurgical procedures in terms ofquality of life and years preserved (Pickard et al., 1990).It is particularly in those with moderate head injurythat hematoma management may make the differencebetween survival with permanent disability and a goodoutcome. Intracranial hematoma is by far the mostcommon cause of secondary deterioration after all headinjuries and constitutes over 70% of the causes of deathin patients who ‘talk and die’ (Reilly et al., 1975; Rose,Valtonen and Jennett, 1976). Emergency surgery forpost-traumatic intracranial hematomas may be amongthe most difficult procedures performed by neurosur-geons because of the frequency of complications suchas heavy bleeding and brain swelling yet, because theseoperations frequently occur at night, it is too often theless experienced surgeons who are delegated to dothem. Similarly, decisions regarding removal of hema-tomas, particularly contusions and intracerebral hema-tomas, may be extremely difficult, especially so whensurgery is prophylactic and intended to preventdeterioration. There have been major changes in thepatterns of management of intracranial hematoma inrecent years, and this chapter has in mind neurosur-geons in training and aims to provide some guidelinesfor surgical management.
20.2 Post-traumatic lesions on CT
CT scanning may reveal a number of patterns ofintracranial hematoma often associated with cerebralswelling:
� small, scattered hemorrhages associated with dif-fuse injury;
� isolated, single or multiple deep cerebralhematomas;
� intraventricular hemorrhage;� subdural or extradural ‘extra-axial’ hematomas.
Each of these, particularly intraventricular hemor-rhage, may occur with diffuse axonal injury, ischemiccell damage, contusion or any of the other types ofhemorrhage.
Large hematomas occur most frequently at thefrontal and temporal poles, often associated withextensive contusions and subdural hematoma (‘theexploded pole’). Swelling around these severe par-enchymal injuries may increase in the days followinginjury and ICP may become more difficult tocontrol.
Marshall has proposed a reproducible and quantifi-able ‘CT classification’ for head injury, which is nowwidely accepted as a method of stratifying head injuryin addition to the Glasgow Coma Scale (Marshall et al.,1991; Table 20.1).
Although brain swelling may occur in relation tohematomas, the degree is quite variable and need notrelate to the size of the hematoma. Indeed, swelling ofa hemisphere or of the whole brain may also occurwithout CT evidence of bleeding.
Temporal lobe hematomas are prone to causingbrain-stem compression at low ICP and with littlemidline shift.
20.3 Indications for evacuation ofintracranial hematomas
Craniotomy is not required in all patients with masslesions due to severe closed head injury. In theTraumatic Coma Data Bank series only 37% ofcomatose patients underwent surgery for removal ofintracranial hematomas (Eisenberg et al., 1991).
Head Injury. Edited by Peter Reilly and Ross Bullock. Published in 1997 by Chapman & Hall, London. ISBN 0 412 58540 5

410 THE ROLE OF SURGERY FOR INTRACRANIAL MASS LESIONS
CT is being used earlier and more often in patientswho sustain head injuries, even in those with mildinjuries, partly because of the medicolegal implicationsof failure to detect an intracranial hematoma. Inconsequence, patients with minimal or no neurologicalsigns or symptoms are often found to have intracranialmass lesions. Neurosurgeons must then weigh up therisks and benefits of conservative treatment, knowingthat the majority of such lesions will resolve sponta-neously, yet a relatively small number will developraised ICP and secondary brain damage which couldhave been prevented by prophylactic surgery
At least 25% of patients with intracranial masslesions will show clinical or radiological worsening inthe first 2–3 days after the injury. This is particularlylikely in patients with cerebral contusions, whereswelling is the norm rather than the exception.
Recently, several studies have provided guidelinesfor the management of extradural and subduralhematomas in asymptomatic patients (Bullock, Smithand Van Dellen, 1985; Knuckey, Gelbard and Epstein,1989; Hamilton and Wallace, 1992; Pozzati and Tog-netti, 1986; Mathew et al., 1993). Management decisionsin individual patients must take into account a numberof factors, such as extracranial injuries, the age of thepatient and the presence of associated intracerebralcontusions or hemisphere swelling. Unfortunately,such management decisions are even more difficult inpatients with intraparenchymal lesions such as contu-sions and intracerebral hematomas.
20.3.1 GUIDELINES FOR INITIAL CONSERVATIVETHERAPY
Non-operative therapy should only be considered:
� in patients who are fully conscious;� when the extra-axial mass lesion is the single
dominant lesion, i.e. there should not be multiplecontusions or potentially significant contralateralmass lesions (which may be preventing midlineshift);
� when there are no features of mass effect such asmidline shift greater than 3 mm, or basal cisterneffacement (Bullock and Teasdale, 1991).
In the conscious patient with an acute subduralhematoma where points 1–3 above are fulfilled andthe lesion is less than 10 mm at its thickest point,conservative therapy has been shown to be successfulin most cases (Mathew et al., 1993). The subduralhematoma will usually resorb within 1 month,although there are occasional instances of chronicsubdural hematoma formation.
Similarly, deep-seated interhemispheric or tentorialsubdural hematomas and small extradural hemato-mas in a stable, conscious patient may not needsurgical evacuation.
Indications for surgical removal are:
� presence of a mass lesion >40 ml;� in the conscious, communicating, non-ventilated
patient:– decline in conscious state;– development of focal signs;– severe and especially worsening headache, nau-
sea or vomiting;� in the unconscious, non-communicating, ventilated
patient:– decline in neurological state; (this may only be
indicated by the development of brain-stemsigns);
– increase in ICP, e.g. >25 mmHg;
Either of these developments should lead to anurgent CT scan.
� increase in hematoma size on CT scan (Galbraithand Teasdale, 1981).
20.3.2 INTRACEREBRAL HEMATOMAS AND FOCALDEFICIT
There has been debate about the benefit of removingan intracerebral hematoma causing a focal deficit but
Table 20.1 Diagnostic categories of types of abnormality visualized on CT scanning (Source: from Marshall et al., 1991)
Category Definition
Diffuse injury I (no visible pathology) No visible intracranial pathology seen on CT scan
Diffuse injury II Cisterns are present with midline shift 0–5 mm and/orLesion densities presentNo high- or mixed-density lesion > 25 cm3
May include bone fragments and foreign bodies
Diffuse injury III (swelling) Cisterns compressed or absent with midline shift 0–5 mm; no high- ormixed-density lesion > 25 cm3
Evacuated mass lesion Any lesion surgically evacuated
Non-evacuated mass lesion High- or mixed-density lesion > 25 cm3 not surgically evacuated

TECHNIQUES FOR CRANIOTOMY 411
without clinical effects of raised pressure or significantmidline shift. Experimental intracerebral hemorrhageproduces ischemia in the surrounding brain, appar-ently due to blood constituents as well as compression(Jenkins et al., 1990). However, clot removal does notrelieve the ischemic neuronal damage, since this hasalready occurred as a result of the clot. Removalshould therefore be based on evidence of harmfulmass effect. When mass effect is present, removal hasbeen reported to lead to a more rapid resolution ofneurological deficits (Levinthal and Stern, 1977).
20.4 Techniques for craniotomy
20.4.1 PREOPERATIVE PREPARATION
In general, cranial surgery should not be performeduntil a stable blood pressure and adequate lungfunction, confirmed by blood gas analysis, have beenachieved (Chapter 17).
However, in a patient who is comatose, particularlyif there has been a documented deterioration inconscious level or development of focal signs, removalof the hematoma is a matter of great urgency. Thepatient should be intubated and hyperventilated, ifthis has not already been done, and mannitol 1 g/kgshould be given immediately as the patient is taken tothe operating theater.
Prior to, or during the preparation for craniotomy,the following ‘checklist’ should be completed:
1. blood to laboratory for:(a) cross matching (2 units of whole blood);(b) coagulation studies
(i) prothrombin index(ii) partial thromboplastin time(iii) platelet count;
(c) blood gas analysis;(d) routine full blood count and electrolytes;
2. X-rays of chest and cervical spine (or keep cervicalspine in collar);
3. consent for surgery;4. Foley catheter in bladder;5. two large bore peripheral i.v. lines, or one periph-
eral and one central line (maintainingCVP > 5 cmH2O);
6. arterial catheter;7. protection of both eyes from fluids and pressure;8. adequately secured cuffed endotracheal tube.
The head should be placed on a horseshoe ordoughnut headrest, turned to place the operative sideuppermost and slightly elevated above the level of theheart. A sandbag placed beneath the ipsilateral shoul-der makes turning the head easier. Pressure pointsshould be carefully padded. Unless deterioration israpid, the scalp should be shaved and prepared with
povidone-iodine as for any other intracranial proce-dure. The drapes can be stapled into place to preventthem becoming dislodged if the head has to be turnedor moved during the procedure. Antibiotics, anti-convulsants and mannitol are used as required. Strictattention to anesthetic techniques is vital to avoidhypercarbia and further elevation of intracranialpressure.
20.4.2 EXPLORATORY BURRHOLES
With the wider availability of CT, the necessity forexploratory burrholes is declining. They will berequired only very rarely in hospitals with a CTscanner; however, they may be life-saving in rurallocations where transfer to a CT-equipped facility mayinvolve long delays.
The use of exploratory burrholes implies thatconfirmation of the position or even the presence of ahematoma is lacking. It is therefore important to haveaccess to the whole head and to explore all likely sitesbilaterally before discarding the diagnosis of intra-cranial hematoma. The extent of this exploration willbe determined at least in part by the experience andskills of the operator, given that this will frequently bea non-neurosurgeon working in less than ideal cir-cumstances. It should always be possible to obtainneurosurgical advice by telephone and this should beencouraged. Specific guidelines for the managementof head injury in remote locations in Australia havebeen established by the Neurosurgical Society ofAustralasia.
(a) Technique
The patient is placed supine on a horseshoe ordoughnut headrest. The whole head is shaved, pre-pared and draped to allow access to both frontal,parietal and temporal areas. The site for the initialburrhole is determined according to the most likelysite of the suspected hematoma. If a dilated pupil ispresent, it will usually be ipsilateral to the hematoma.The next most valuable localizing feature is a hemipar-esis, which will usually be contralateral to a hema-toma. If a fracture is present it is most likely to overliean extradural hematoma. It must be stressed that noneof these signs is absolute and if no hematoma is foundon the suspected side, the other side should beexplored in all cases.
Unless a fracture is present in a different location,the first burrhole should be temporal, as this is the siteof most extradural hematomas. It is frequently writtenthat a burrhole placed as little as 2 mm away from theedge of an extradural hematoma will fail to identify it,and this tends to discourage the inexperienced doctorin a difficult situation. The temporal burrhole is not

412 THE ROLE OF SURGERY FOR INTRACRANIAL MASS LESIONS
intended to be placed in any position to that degree ofaccuracy. It should ideally be just above the zygomaand approximately one finger breadth in front of thetragus. The head is turned away from the side ofexploration if the cervical spine is normal or thepatient is placed in the lateral position in a suitablecollar if there may be a cervical spine fracture.
A vertical scalp incision is made as shown in Figure20.1. The scalpel is used to cut directly through thetemporalis muscle down to the skull. To preventinjury to the facial nerve the inferior limit of theincision is the zygomatic arch. Bleeding will beencountered from the superficial temporal artery butthis can be easily controlled with diathermy or ligationafter a retractor is placed. The periosteum andtemporalis muscle are scraped off the temporal bonewith a sharp periosteal elevator and a self-retainingretractor is inserted to hold back the muscle. Aburrhole is drilled, using the perforator until anirregular wobbling is felt and there is a perforationthrough the central part of the hole that can bepalpated with forceps (Figure 20.2). Through thissmall hole, the surgeon may see either dura orextradural blood, but for a confident diagnosis thehole needs to then be enlarged with the burr tocomplete the hole, but only if the perforator hasbreached the inner table. The temporal bone is usuallyquite thin (2–3 mm), whereas the bone in the frontaland parietal areas may be more than 10 mm thick. If anextradural hematoma is present, the hole will need tobe enlarged to allow removal of the clot. For anexperienced operator in a well-equipped site this willusually involve a craniotomy; for an inexperiencedoperator or when facilities are limited a craniectomy is
often more appropriate. If no abnormality is found atthe temporal burrhole, further burrholes are per-formed in the ipsilateral frontal and posterior parietalareas. The technique is the same but the bone will bethicker. The scalp incisions should be made in such away that they can easily be converted into a ‘question-mark’-type flap (Figure 20.3).
If all three burrholes on one side are negative, theprocess should be repeated on the opposite side.Opinions regarding opening of the dura vary. It is verydifficult to determine whether a significant intraduralhematoma exists without first opening the dura. Thepresence of blue, bulging dura seen through a burr-hole is a very poor diagnostic feature. Following
Figure 20.1 The inital burr hole is made through a verticalincision just above the zygoma and one fingerbreadth infront of the tragus.
Figure 20.2 The preforator makes a small hole in the innertable of the skull through which extradural blood may beseen.
Figure 20.3 The scalp incision for exploratory burr holesshould be made in a direction suitable for later conversion toa flap (as shown by the dotted line).

TECHNIQUES FOR CRANIOTOMY 413
trauma, the brain is often swollen and frequently thereis a thin rim of acute subdural blood which is of littlesignificance. Inexperienced operators performingexploratory burrholes for the first time will oftenmistake this for a significant acute subdural hema-toma and may be dissuaded from looking elsewhere,thereby missing a more important hematoma. Webelieve it is better to complete the standard sixburrholes to exclude an extradural hematoma beforeopening the dura in search of an acute subduralhematoma. The dura is opened by gently incising theouter layers with a number 15 blade, picking these upwith a sharp hook to lift the dura off the brain beforecompleting the incision. The dural edges can then bepicked up with forceps and a cruciate incision can becompleted. The dural edges are diathermied, takingcare to avoid any underlying cerebral vessels. A thinlayer (2–3 mm) of blood is common and should not bemistaken for a significant acute subdural hematoma. Ifa thicker layer of blood is encountered, it should beexposed by performing a craniotomy or craniectomy,depending on the circumstances.
20.4.3 EXTRADURAL HEMATOMA
(a) Craniectomy
Although craniotomy is preferable when skills andconditions permit, craniectomy is often used as ameans of extending the exposure after exploratoryburrholes. Initial evacuation should be performedrapidly through the craniectomy in order to relievebrain-stem pressure, then either a formal craniotomyor a more extensive craniectomy may be performed,the hematoma evacuated and the bleeding pointsecured.
The technique is simple. A rongeur is used to nibblebone away and expose the entire hematoma. When thebone is very thick, it is sometimes easier to makeseveral burrholes and nibble the bone away betweenthem. The dura will have already been separated fromthe inner table of the skull by the hematoma and is notprone to injury. At the margins of the hematoma thedura will be adherent to the bone and should not bestripped any further. If there is a bleeding point on thedura it should be coagulated with bipolar diathermyor, if this is not available, unipolar diathermy may beused on a low setting. Bleeding from the edges of thewound may be troublesome and difficult to stop withdiathermy. It is best to pack a little Surgicell or Avitene(postage-stamp size) under the bone edge and then‘hitch up’ the dura to surrounding pericranium withfine sutures (Figure 20.4). It is however, important notto traumatize the underlying brain with these sutures,and this may be achieved by first lifting the dura offthe brain with forceps, or opening the dura to allow
air or saline to lift the dura from the brain. The bonefragments should be left out, and the wound closed inlayers with a suction drain in the subgaleal (extra-dural) space for 12 hours. One should not be deterredby the amount of bone that is removed since anelective cranioplasty is easily performed when thepatient has recovered.
(b) Craniotomy
When the site of the hematoma has been determinedpreoperatively by CT scan, the operation of choice willusually be a craniotomy. It is helpful to transpose theposition of the hematoma on to the CT scout film, asunusual gantry angles may be confusing (Figure 20.5).Most extradural hematomas are temporal and can beadequately removed through the standard ‘questionmark’ trauma scalp flap (Figure 20.3). More posteriorhematomas may be approached through an invertedhorseshoe flap (Figure 20.6). Frontal and subfrontalhematomas should be exposed through a bicoronalflap (Figure 20.7) to avoid an unsightly midlineforehead scar.
The patient is positioned with the head in ahorseshoe headrest and turned to bring the operativesite uppermost. (A three-pin headrest may be used ifthe location of the hematoma is established.) The scalpis shaved and prepared with povidone-iodine.Depending on the urgency of the situation, the wholescalp flap can be turned down initially, or a smallincision can be made and a burrhole craniectomyperformed to allow rapid decompression, beforecompleting the craniotomy. In most cases it is moreefficient to quickly turn down a myocutaneous scalpflap followed by a free bone flap. The use of a high-
Figure 20.4 ‘Hitching’ the dura to the pericranium is aneffective means of controlling venous bleeding from beneaththe bone edges.

414 THE ROLE OF SURGERY FOR INTRACRANIAL MASS LESIONS
speed drill system permits this to be done just asquickly in skilled hands as hand-drilling a singleburrhole. A small hole is drilled in the thin temporalbone or elsewhere depending on the location of thehematoma. A craniotome cutting attachment is thenused to complete the craniotomy. The risk of duraldamage is small, especially in the presence of anextradural hematoma. The medial edge of the bone
flap is taken no closer than 2 cm from the midline toavoid injury to the superior sagittal sinus and itsdraining veins. Unless the CT dictates otherwise, theinferior edge of the bone flap is taken well down intothe temporal region to allow clear access to the middlefossa.After removing the bone flap, the hematoma is suckedand irrigated away. Bleeding dural arteries and veins
(a)
(b)
Figure 20.5 The extradural hematoma seen in the axialscans in (a) has been measured and transposed on to thecorresponding scout film (b). This may be of considerableassitance in planning the site for craniotomy.

TECHNIQUES FOR CRANIOTOMY 415
are then coagulated with bipolar diathermy. Bleedingbone edges are controlled with bone wax. Hemostaticagents such as Surgicell or Avitene can be used aroundthe margins of the craniotomy to control venousbleeding, which often seeps out from just beneath thebone edge. The addition of dural ‘hitching’ sutures
also helps to control this bleeding and preventrecurrent hematoma formation.
The bone flap is replaced and fixed with mini-platesor stainless-steel wire if the brain is not swollen, andsuction drains are used in the extradural and sub-galeal spaces for 12 hours. The muscle and galea areclosed with Vicryl and the skin with staples. Inpatients who have sustained a significant primaryinjury (that is all who were in coma), an ICP monitoris inserted at the end of the procedure. When brainswelling occurs the dura becomes tense and it shouldalways be opened to exclude an underlying subduralhematoma.
20.4.4 ACUTE SUBDURAL HEMATOMA
The treatment of acute subdural hematoma followsthe same principles as extradural hematoma, althoughthe prognosis is much worse (60% die or survive witha bad outcome – Chapter 18). The affected area isexposed by craniectomy or preferably craniotomy asdescribed for extradural hematoma, taking care to useall means available to reduce ICP first (see Chapter18). The dura is opened using a sharp hook andscalpel, revealing dark, clotted blood under pressure.For the inexperienced, it is preferable to make severalslits in the dura without joining them together (Figure20.8) as this will minimize herniation of the brain,which can be dramatic and may even prevent closureof the scalp. If a dural flap is used, it should be basedmedially to avoid damage to the superior sagittalsinus and the draining veins running into it (Figure20.9). The hematoma is removed by suction andirrigation, taking care not to use suction beyond thelimits of the craniotomy in areas that are not directlyvisible and accessible. Often there will be no obviousbleeding point. Bleeding from a contused cortical
Figure 20.6 An ‘inverted horseshoe’ flap may be moreappropriate than a ‘question mark’ flap for hematomas thatare positioned more posteriorly.
Figure 20.7 A bicoronal or ‘aneurysm’ flap for a frontalhematoma avoids a visible forehead scar.
Figure 20.8 To minimize brain herniation an acute sub-dural hematoma may be evacuated through several smalldural incisions rather than one large dural flap.

416 THE ROLE OF SURGERY FOR INTRACRANIAL MASS LESIONS
surface can be controlled with bipolar diathermy orGelfoam. This may not be easy, especially if the brainis swelling rapidly.
An attempt should always be made to identify aparasagittal venous bleeder, if no cortical source ofbleeding is found. The medial cortex should be verygently depressed, while irrigating parasagittally. Rais-ing the venous pressure may reveal the bleeder. This isbest done by asking the anesthetist to increaseinflation pressure for three or four breaths to40 cmH2O. If a bleeding parasagittal vein is found, itshould be coagulated with bipolar diathermy, If thevein is avulsed from the sagittal sinus, bleeding maybe very difficult to arrest, requiring application of‘ligaclips’ or a muscle patch for tamponade. Failure toseek a parasagittal bleeding source (present in 40–50%of subdural hematomas) may account for the highincidence of recurrent hematomas in some series(Richards and Hoff, 1974).
Contused and necrotic brain is best removed withsuction and gentle irrigation, with consideration ofpartial frontal or temporal lobectomy when the dam-age is severe. This should not be undertaken by non-neurosurgeons, who should only remove damagedbrain.
After removal of the hematoma the dura is closed.This may require a duroplasty, using an insert oftemporalis fascia, pericranium or other dural sub-stitute such as lyophilized bovine dura or wovencollagen. Commercial forms of human lyophilizeddura are no longer available in many countriesbecause of the known cases of transmitted Creutz-feldt–Jakob disease (Will and Matthews, 1982; Simp-son et al., 1996).
It is generally preferable to replace the bone flap, asthe advantages of decompression in this situation are
outweighed by the disadvantages of cerebral hernia-tion through the wound with consequent venous andeven arterial compromise. The bone may be securedwith mini-plates or stainless-steel wire unless brainswelling is present, in which case the bone is best left‘free’ and secured only by a few pericranial sutures toallow expansion. A suction drain is placed in thesubgaleal space with or without another in theextradural space (if the dura has been closed). Thescalp is closed in two layers and an ICP monitor isused routinely.
20.4.5 POSTERIOR FOSSA HEMATOMAS
Suspicion of a posterior fossa hematoma shouldmandate rapid transfer to a neurosurgical facility, ora neurosurgical retrieval team (Chapter 15). Themajor concerns are rapid onset of CSF obstructionand brain-stem compression, and air embolism dur-ing surgery due to venous sinus injury. The patientis positioned prone with the head fixed in a three-pinheadrest. The head should be slightly elevated toreduce venous bleeding but not so much as topromote air embolism. A midline incision and stand-ard suboccipital craniectomy are performed. It isimportant to continue the decompression throughthe rim of the foramen magnum, as postoperativeswelling in the posterior fossa may cause death bybrain-stem compression. If the trauma has alreadyinvolved a sinus, bleeding should be controlled bytamponade with muscle, Gelfoam, Surgicel or similarsubstances while carefully elevating the head. Anesophageal stethoscope and end-tidal CO2 measure-ments should be used to detect any air embolism.Many extradural hematomas extend both above andbelow the level of the tentorium, overlying thetransverse sinus. In these cases, a bridge of boneshould be left over the sinus to allow the dura to betented up and tamponade bleeding sites.
20.5 Specific surgical problems
20.5.1 INTRAVENTRICULAR HEMORRHAGE
Intraventricular hemorrhage usually occurs in thesetting of a severe diffuse injury with other CTevidence of parenchymal injury. In about 40% of casesthere is no evidence of an intraparenchymal source ofthe bleeding, although there will often be an injury tothe corpus callosum or septum pellucidum (Sato et al.,1987). Hydrocephalus is uncommon (Christie, Marksand Liddington, 1988; Jayakumar et al., 1990) butwhen it is present, raised ICP should be treated byventricular drainage. Mortality is high in most seriesbut tends to reflect the GCS on admission and hencethe severity of the primary injury (Chapter 10).
Figure 20.9 Basing a dural flap medially reduces the risk ofdamage to the superior sagittal sinus and the draining veinsrunning into it.

SPECIFIC SURGICAL PROBLEMS 417
20.5.2 INTRACEREBRAL HEMATOMAS
Some 88% of patients with intracranial hematomasafter trauma were found to have raised ICP post-operatively (Miller et al., 1981). When control of ICP byall available medical means fails then removal ofcontusions may be a highly effective form of ICPcontrol, especially when accompanied by a largecraniotomy and duroplasty. A swollen and contusedtemporal pole may cause early tentorial herniationand brain-stem compression, even at surprisingly lowICP in the sedated, ventilated patient.
20.5.3 SURGICAL DECOMPRESSION FOR BRAINSWELLING
Decompression by large craniotomy has been advo-cated in several older studies when other methods ofcontrolling ICP have failed (Kjellberg and Prieto, 1971;Ransohoff et al., 1971, Britt and Hamilton, 1978).Although all these older clinical (Cooper, Rovit andRansohoff, 1976; Venes and Collins, 1975), and experi-mental studies (Cooper et al., 1979) suggested nobenefit, and indeed worsening of brain edema follow-ing craniectomy, there are many more recent anecdotalexperiences in many neurosurgical centers wheredecompressive craniectomy has been successful. Gaabet al. (1990) proposed indications for large unilateral orbilateral fronto-temporo-parietal decompression inselected trauma patients. This was considered whenmedical treatment had failed in patients under 40years, with initial GCS of 7 or more and evidence ofclinical deterioration, but without the signs of brain-stem failure. In their report, 30 of their 37 carefullyselected patients made good recoveries or had onlymoderate disability. Alexander, Ball and Laster repor-ted on the application of the more limited surgicalapproach used by Cushing. In patients who did notrespond to medical treatment, they performed asubtemporal decompression, leaving dura open andresecting the anterior temporal lobe if it was damaged.(Alexander, Ball and Laster, 1987).
One of the well known hazards of craniotomy forbrain swelling is herniation through the craniotomy.Hence, large craniotomies have generally been advo-cated. Bifrontal craniotomies should be made so thatthe inferior margin is cut low across the supraorbitalmargin, and they should extend well posterior sothat the brain can expand forward and not herniateagainst the bony margin. For effective decompressionthe dural envelope must be enlarged. The durashould be opened widely, hinged medially and thefalx and sagittal sinus divided as low as possibletaking care to preserve draining veins wheneverpossible. An augmentation duroplasty is used tocover the brain.
At the Medical College of Virginia, a wide decom-pressive craniotomy with duraplasty and bone-flapremoval is performed for ICP control under thefollowing circumstances:
� ICP control not achieved with maximal therapyusing mannitol, ventricular drainage, pressors,moderate hyperventilation (PaCO2 = 32 ± 2 mmHg)and moderate hypothermia (32 ± 2°C);
� pupils not fixed and dilated;� preserved brain-stem responses and central conduc-
tion time on evoked potential testing.
Decompression is used before barbiturate therapy, inview of the propensity for barbiturate therapy tolower CPP and worsen outcome (Figure 20.10).
20.5.4 LOBECTOMY FOR BRAIN SWELLING
Surgery for removal of swollen and contused brain ismore controversial. It frequently does not control ICPand more than 80% of such patients may still haveraised ICP postoperatively (Miller et al., 1981). It istherefore better to control ICP by medical meansinitially, removing contusions only when this treat-ment has failed (Miller, 1992). However, as notedearlier, a swollen and contused temporal pole maycause tentorial herniation and brain-stem compressionat quite low ICP and, in the sedated, ventilatedpatient, the only (late) sign of this may be pupillarydilatation.
Removal of contused and swollen brain to controlintracranial pressure may be beneficial when othermeans of control have failed. Litofsky et al. (1994) foundthis to be so in patients under 40 years with higherinitial GCS scores. In this small retrospective report55% of patients had a ‘good’ or ‘moderately disabled’outcome and there was no increase in vegetativesurvivors. Lobectomy aimed to remove damaged brainand to avoid eloquent areas (Figure 20.11).
20.5.5 INTRAOPERATIVE BRAIN SWELLING
As noted above, removal of acute hematomas may befollowed by severe brain herniation. The brain her-niating through the craniotomy may occlude surfaceveins and even rupture against the bony–duralmargins. This is most commonly seen with acutesubdural hematomas and may be anticipated whenthe preoperative CT scan shows brain swelling inaddition to the hematoma (Bullock and Teasdale,1991). There are several potentially remediable causesthat must be considered urgently before concludingthat the swelling is simply a reflection of a non-survivable injury. The surgeon should quickly estab-lish with the anesthetist that ventilation has notbecome impaired (e.g. by pneumothorax, endotra-
418 THE ROLE OF SURGERY FOR INTRACRANIAL MASS LESIONS
cheal tube dislodgment or occlusion) and that thepatient is hyperventilated. Secondly, a hidden hema-toma, either intracerebral or beyond the craniotomymargin, may have developed. An intracerebral hema-toma is possible if there is a cerebral contusion or‘exploded pole’. Acute hydrocephalus is uncommonbut should be excluded by attempting to cannulate theipsilateral frontal horn. Intraoperative ultrasound isvaluable in seeking and excluding these events.Contralateral hematomas occasionally develop orenlarge after removal of the major hematoma. Thispossibility should be considered particularly if there isa contralateral fracture or small hematoma on thepreoperative CT, but indeed has been reported ifneither of these features is present.
20.5.6 MANAGEMENT OF DIFFUSE INTRAOPERATIVEBLEEDING
(a) Prevention
No matter how urgent the need to evacuate ahematoma, it is imperative that a fixed surgicalroutine be followed in order to avoid excessivebleeding. After marking out the large craniotomy flaprequired to evacuate an acute subdural hematoma orintracerebral contusions, a burr hole should be madeand the hematoma should be decompressed acutely.This allows the surgeon to open the remainder of thecraniotomy in a controlled fashion, securing thebleeding points in the scalp with diathermy, scalpclips or hemostats. Bleeding points in the temporalis
(a) (b)
(c)
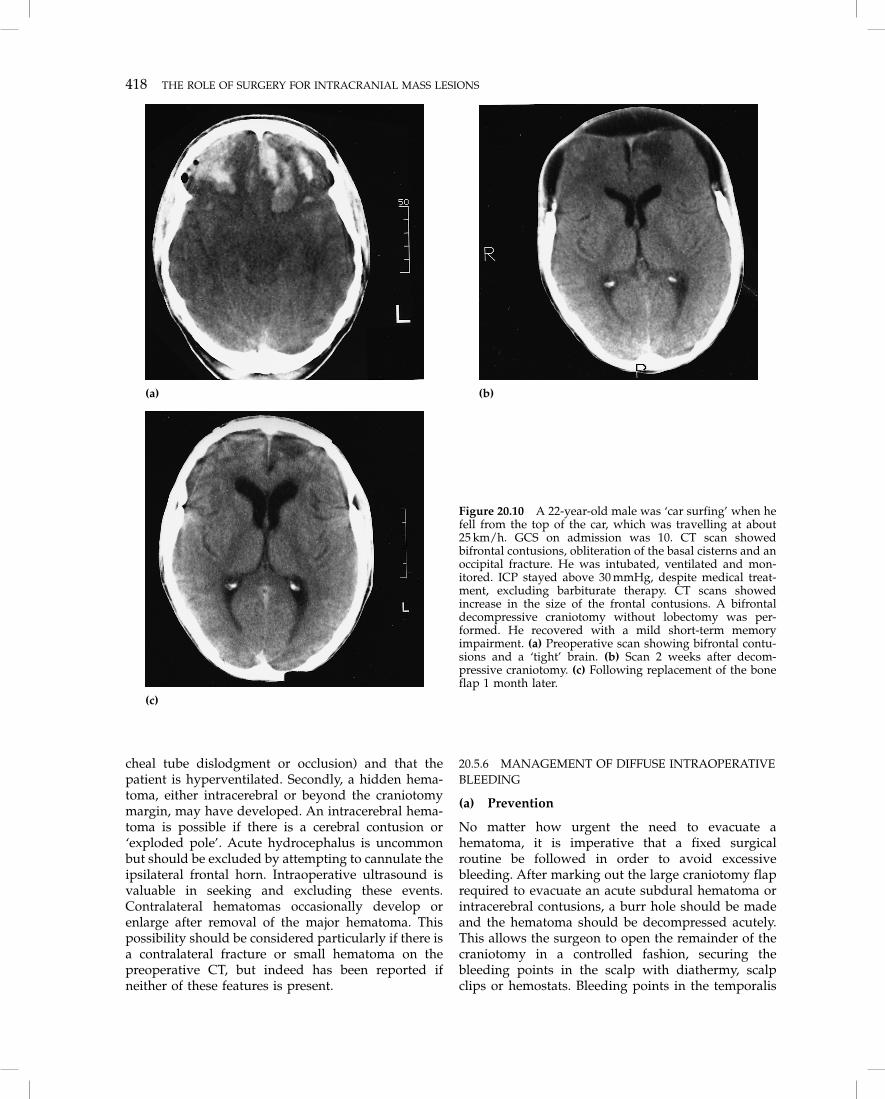
Figure 20.10 A 22-year-old male was ‘car surfing’ when hefell from the top of the car, which was travelling at about25 km/h. GCS on admission was 10. CT scan showedbifrontal contusions, obliteration of the basal cisterns and anoccipital fracture. He was intubated, ventilated and mon-itored. ICP stayed above 30 mmHg, despite medical treat-ment, excluding barbiturate therapy. CT scans showedincrease in the size of the frontal contusions. A bifrontaldecompressive craniotomy without lobectomy was per-formed. He recovered with a mild short-term memoryimpairment. (a) Preoperative scan showing bifrontal contu-sions and a ‘tight’ brain. (b) Scan 2 weeks after decom-pressive craniotomy. (c) Following replacement of the boneflap 1 month later.

SPECIFIC SURGICAL PROBLEMS 419
muscle are coagulated. Several units of blood may belost from badly secured scalp edges.
(b) Management
Profuse and diffuse bleeding from brain and menin-geal surfaces almost always indicates a significantcoagulopathy. Blood should be sent intraoperativelyfor coagulation studies, and a transfusion of freshfrozen plasma and/or whole blood should be givenwhile awaiting the results of these studies. Diffusehemorrhage may be accompanied by massive brainswelling and herniation through the craniotomy. Thesurgeon is then faced with the prospect of worseningthe bleeding by performing a temporal or frontallobectomy in order to control the brain swelling. Amanagement checklist should be followed beforeproceeding with lobectomy.
1. Check the coagulation studies.2. Transfuse blood and fresh frozen plasma as appro-
priate, usually 6–10 units.3. Consider intraoperative ultrasound to detect the
development of an intraoperative hematoma, eitherintracerebral, epidural or subdural on the same oropposite side.
4. Optimize cerebral perfusion pressure. Sometimesincreasing CPP intraoperatively to a mean of 80 or90 mmHg will help to control brain swelling bypromoting vasoconstriction if the patient has intact
autoregulation. Clearly, however, it is equally pos-sible that this maneuver will worsen the brainswelling if the patient does not autoregulate. (Thesepatients almost always die.)
5. Give thiopental 250 mg–1 g in incremental doses, tosuppress any cerebral electrical activity (Chapter19). CPP must be maintained at about 70 mmHg,using vasopressor agents if necessary.
6. Give more mannitol to a dose of 1 g/kg and lowerthe PaCO2 to approximately 28 mmHg by increasingventilation.
7. Occasionally, massive brain swelling may becaused by an intraoperative pneumothorax, whichraises inflation and ventilatory pressures and henceintracranial venous pressure. The chest should,therefore be auscultated and, if necessary, X-rayed,during the surgery.
It is usually advisable to wait 15 minutes to assess theeffect of these measures before proceeding. If there is noimprovement, or if bleeding is ongoing, it is usuallynecessary to perform a lobectomy. It is important toemphasize that, for any chance of success in thisdesperate situation, the surgeon and a highly skilledanesthesiologist must work closely together through-out and necessary assistants should be called in.
The best course of action is to perform a swift andgenerous lobectomy where the damage is greatest,avoiding where possible the speech areas in the
(a) (b)
Figure 20.11 A 19-year-old pedestrian was struck by a car travelling at high speed. GCS on admission was 3. CT scanshowed a basal ganglionic hematoma with 1 cm midline shift. ICP was 26 mmHg. The clot was partially removed bycraniotomy but ICP rose to 30–40 mmHg over the next 24 h, despite medical therapy, excluding barbiturates. A frontallobectomy was performed and ICP and CPP were well controlled thereafter. (a) CT on admission showing a deepintracerebral hematoma with 1 cm midline shift. (b) Following partial frontal lobectomy.

420 THE ROLE OF SURGERY FOR INTRACRANIAL MASS LESIONS
dominant hemisphere. It may be necessary to removebone very rapidly by extending the craniotomy with acraniotome or rongeur in order to obtain sufficientaccess for this. Hemostatic adjuncts may includethrombin-soaked gel foam, Surgicel, and peroxide-soaked cotton wool patties.
20.5.7 CRANIOBASAL SKULL FRACTURE
Penetrating open wounds of the skull are not withinthe provenance of this book, but craniobasal skullfractures may be internally compound and will bebriefly considered. The presence of a dural fistula isindicated by intracranial air, cerebrospinal fluid rhi-norrhea or otorrhea or later by meningitis. An intra-cranial aerocele may expand if the dural tear acts as aone-way valve (North, 1971). Cerebrospinal fluidleakage may occur early, or after some days. It maycease spontaneously, but this may not in itself indicatesatisfactory dural healing and the risk of late meningi-tis may still exist.
Recommendations for treatment have ranged fromdural repair in all cases, irrespective of whether therhinorrhea ceases (Lewin, 1954), to a more selectiverepair when there is continued CSF leakage, anosmiaor wide fractures (Loew et al., 1984).
We recommend operative repair when:
� CSF leakage persists for 7–10 days;� CSF leakage ceases, but recurs after 7–10 days;� there is clinical evidence of a large dural defect
indicated by a large aerocele, or by escape of braintissue through the nostrils;
� meningitis or brain abscess develop after trauma atany time;
� there is radiological evidence suggesting that natu-ral dural repair is unlikely, e.g. a basal skull fractureinvolving the paranasal sinuses, wide separation ofbone edges, a spike of bone or a possible cerebralhernia into the nasal cavity (Reilly and Simpson,1995).
The incidence of meningitis after cerebrospinal fluidrhinorrhea associated with the Le Fort III fracturesappears to be lower than that associated with a vaultfracture (O’Brien and Reade, 1984). Indeed, CSFleakage often ceases once the midface fracture isreduced, but the indications for dural repair remain asoutlined above. Whether prophylactic antibiotics areprotective against meningitis continues to be debated(Brown, 1993; Working Party Report, 1994). Althoughthere is no strong evidence favoring prophylacticantibiotics it is our policy to use intravenous metroni-dazole, co-trimoxazole and ampicillin if there isevidence of a fistula. These are continued until CSFleakage ceases or for several days after surgical repairis undertaken.
(a) Timing of transcranial repair
The transcranial repair of a dural fistula is usuallyundertaken electively and therefore does not affect theearly acute management of the patient with severehead injury. Acute transcranial repair is often verydifficult, because the brain is ‘tight’ and resistsretraction and the repair may therefore be inadequateor impossible. If there are facial fractures, a one-stagecombined transcranial repair and internal fixation ofthe facial fractures may be undertaken with the plasticsurgery team, usually 5–10 days after injury. Recently,well-localized fractures involving the sphenoid and/or ethmoid sinuses have been approached subcra-nially via an ethmoidectomy or transnasally aided byendoscopy. This has the merit of not requiring brainretraction and may be performed within days ofinjury. It is also less likely to cause anosmia whenolfaction is still present (Raveh, Redli and Mark-walder, 1984).
20.5.8 COAGULOPATHY IN PATIENTS WITH HEADINJURY
Coagulopathy develops in one quarter to one third ofpatients who undergo surgery for removal of anintracranial hematoma (Bullock et al., 1990; Stein et al.,1992). In many, this may be mild and self-limiting, butin others it may be sufficiently severe to cause deathon the operating table. It is consequently mandatory todetermine the coagulation status in every patient whois considered for surgical evacuation of a traumaticintracranial hematoma. Frequently, this will need to beperformed as an emergency. Full evaluation shouldinclude a prothrombin index, partial thromboplastintime and a platelet count. A template bleeding time, ifavailable, can be used to assess bleeding time. Theincreasing frequency of coagulation disorders inpatients with intracranial hematoma has many causes,but the most important are:
� prior medication with warfarin, heparin oraspirin;
� chronic alcoholism: excess bleeding in alcoholicsmay be related to reduced levels of coagulationfactors; an ethanol-induced decrease in plateletfunction and nutritional factors may contribute;
� disseminated intravascular coagulation (DIC) dueto thromboplastin activator substances derivedfrom brain or from sites of multiple trauma (Simp-son, Speed and Blumbergs, 1991);
� coagulopathy associated with massive blood trans-fusion to replace blood loss from abdominal or limbinjuries;
� a pre-existing coagulation problem, e.g. von Wille-brand’s disease, thrombocytopenia or hemophilia.

REFERENCES 421
These patients may be predisposed to develop largeintracranial hematomas with relatively minor cranialinjuries. It is imperative, therefore, to obtain a historyfrom relatives as early as possible, so that relevant pre-existing diseases are known prior to surgery.
A marked hyperemic response is frequentlyencountered in the injured brain, scalp and meninges,and relatively minor abnormalities of coagulation,which might be acceptable for abdominal or ortho-pedic surgery, can make emergency neurosurgeryextremely hazardous. The management goal in suchpatients should be complete normalization of thehematological parameters by replacing the appro-priate factors (see below). Hematological and bloodtransfusion services should be aware that platelets orfresh frozen plasma may be needed in patients withpersistent severe intracranial bleeding, even whencoagulation parameters are only mildly abnormal – orindeed normal, in patients with qualitative plateletfunction disorders.
(a) Qualitative platelet disorders
Chronic aspirin therapy, which is increasingly preva-lent in the general population, and chronic alcoholismare the two most common causes of coagulopathyafter neurotrauma. When the platelet count is margin-ally depressed, as in chronic alcoholism, and plateletfunction is also significantly compromised, the coagu-lation problem can be particularly severe. Unfortu-nately, qualitative platelet disorders may be undetect-able by standard tests such as bleeding time. Morecomplex measures such as glass bead platelet adhe-sion tests may be needed and these are not routinelyavailable in the emergency situation that often con-fronts neurotrauma patients.
20.6 ReferencesAlexander, E. Jr, Ball, M. and Laster, D. W. (1987) Subtemporal decompression:
radiological observations and recurrent surgical experience. British Journalof Neurosurgery, 1, 427–433.
Britt, R. H. and Hamilton, R. D. (1978) Large decompressive craniotomy in thetreatment of acute subdural hematoma. Neurosurgery, 2, 195–200.
Brown, E. M. (1993) Antimicrobial prophylaxis in neurosurgery. Journal ofAntimicrobial Chemotherapy, 31(Suppl. B), 49–63
Bullock, R., Smith, R. M. and Van Dellen, J. R. (1985) Nonoperative treatmentof extradural haematoma. Neurosurgery, 16, 602–606.
Bullock, R. and Teasdale, G. (1990) Head injuries – surgical management oftraumatic intracerebral haematomas, in Handbook of Clinical Neurology, vol.57 – Head Injury, (ed. R. Braakman), Elsevier, Amsterdam, ch. 10, pp.249–298.
Bullock R., Hanneman, C. O., Murray, L. and Teasdale, G. M. (1990) Recurrenthaematomas following craniotomy for traumatic intracranial mass. Journalof Neurosurgery, 72, 9–14.
Christie, M., Marks, P. and Liddington, M. (1988) Post-traumatic intra-ventricular haemorrhage: a reappraisal. British Journal of Neurosurgery, 2,343–349.
Cooper, P. R., Rovit, R. L. and Ransohoff, J. (1976) Hemicraniectomy in thetreatment of acute subdural hematoma: a re-appraisal. Surgical Neurology, 5,25–28.
Cooper, P. R., Hagler, H., Clark, W. K. and Barnett, P. (1979) Enhancement ofexperimental cerebral edema after decompressive craniectomy: implica-tions for the management of severe head injuries. Neurosurgery, 4,296–300.
Eisenberg, H. M., Jane J. A., Marmarou, A. et al. (1991) The Traumatic ComaData Bank: design methods and baseline characteristics. Journal of Neu-rosurgery, 75, S8–S13.
Gaab, M. R., Rittierodt, M., Lorenz, M. and Heissler, H. E. (1990) Traumaticbrain swelling and operative decompression: a prospective investigation.Acta Neurochirurgica (Supplement) (Vienna), 51, 326–328.
Galbraith, S. and Teasdale, G. (1981) Predicting the need for operation in thepatient with an occult traumatic intracranial hematoma. Journal of Neu-rosurgery, 55, 75–81.
Hamilton, M. and Wallace, C. (1992) Nonoperative management of acuteepidural haematoma diagnosed by CT: the neuroradiologist’s role. Amer-ican Journal of Neuroradiology, 13, 853–859.
Jayakumar, P. N., Kolluri, V. R., Basavakumar, D. G. et al. (1990) Prognosis intraumatic intraventricular haemorrhage. Acta Neurochirurgica (Vienna), 106,48–51.
Jenkins, A., Mendelow, A. D., Graham, D. I. et al. (1990) Experimentalintracerebral haematoma: the role of blood constituents in early ischaemia.British Journal of Neurosurgery, 4, 45–52.
Kjellberg, R. N. and Prieto, A. J. (1971) Bifrontal decompressive craniotomyfor massive cerebral edema. Journal of Neurosurgery, 34, 488–493.
Knuckey, N. W., Gelbard, S. and Epstein, M. H. (1989) The management of‘asymptomatic’ epidural hematomas. A prospective study. Journal ofNeurosurgery, 70, 392–396.
Levinthal, R. and Stern, W. E. (1977) Traumatic intracerebral hematoma withstable neurological deficit. Surgical Neurology, 7, 269–273.
Lewin, W. (1954) Cerebrospinal rhinorrhoea in closed head injuries. BritishJournal Surgery, 42, 1–18.
Litofsky, N. S., Chin, L. S., Tang, G. et al. (1994) The use of lobectomy in themanagement of severe closed head trauma. Neurosurgery, 34, 628–633.
Loew, F., Pertuiset, B., Chaumier, E. E. and Jaksche, H. (1984) Traumatic,spontaneous and postoperative CSF rhinorrhoea. Advances and TechnicalStandards in Neurosurgery, 11, 169–207.
Marshall, L. F., Bowers-Marshall, S., Klauber, M. R. et al. (1991) A newclassification of head injury based on computerised tomography. Journal ofNeurosurgery, 75, S14–S20.
Mathew, P., Oluoch-Olunya, D. L., Condon, B. R. and Bullock, R. (1993) Acutesubdural haematoma in the conscious patient: outcome with initial non-operative management. Acta Neurochirurgica (Vienna), 121, 100–108.
Miller, J. D. (1992) Head injury in adults. Neurosurgery Quarterly, 2, 28–43.Miller, J. D., Butterworth, J. F., Gudeman, S. K. et al. (1981) Further experience
in the management of severe head injury. Journal of Neurosurgery, 54,289–299.
North, J. B. (1971) On the importance of intracranial air. British Journal ofSurgery, 58, 826–829.
O’Brien, M. D. and Reade, P. C. (1984) The management of dural tear resultingfrom mid-facial fracture. Head and Neck Surgery, 6, 810–818.
Pickard. J. D., Bailey, S., Sanderson, H. et al. (1990). Steps towards cost- benefitanalysis of regional neurosurgical care. British Medical Journal, 301,629–635.
Pozzatti, E. and Tognetti, F. (1986) Spontaneous healing of acute extraduralhaematoma: study of 22 cases. Neurosurgery, 18, 696–700.
Ransohoff, J., Benjamin, M. V., Gage, E. L. Jr and Epstein, F. (1971)Hemicraniectomy in the management of acute subdural hematoma. Journalof Neurosurgery, 34, 70–76.
Raveh, J., Redli, M. and Markwalder, T. M. (1984) Operative management of 194cases of combined maxillofacial frontobasal fractures: principles and surgicalmodifications. Journal of Oral and Maxillofacial Surgery, 42, 555–564.
Reilly, P. L. and Simpson, D. A. (1995) Craniocerebral injuries, in Craniomax-illofacial Trauma, (ed. D. J. David and D. A. Simpson), Churchill Livingstone,Edinburgh, pp. 367–396.
Reilly, P. L., Graham, D. I., Adams, J. H. and Jennett, B. (1975) Patients withhead injury who talk and die. Lancet, i, 375–377.
Richards, T. and Hoff, J. (1974) Factors affecting survival from subduralhematoma. Surgery, 75, 253–258.
Rose, J., Valtonen, S. and Jennett, B. (1977) Avoidable factors contributing todeath after head injury. British Medical Journal, 2, 615–618.
Sato, M., Tanaka, S., Kohama, A. and Fujii, C. (1987) Traumatic intra-ventricular haemorrhage. Acta Neurochirurgica (Vienna), 88, 95–103.
Simpson, D. A., Speed, I. E. and Blumbergs, P. C. (1991) Embolism of cerebraltissue: a cause of coagulopathy and cerebral infarction? Report of a case.Surgical Neurology, 35, 159–162.
Simpson, D. A., Masters, C. L., Ohlrich, G. et al. (1996) Iatrogenic Creutzfeldt–Jacob disease and its neurosurgical implications. Journal of the ClinicalNeurosciences, 3: 118–123.
Stein, S. C., Young, G. S., Talucci, R. C. et al. (1992) Delayed brain injury afterhead trauma: significance of coagulopathy. Neurosurgery, 30, 160–165.
Venes, J. L. and Collins, W. F. (1975) Bifrontal decompressive craniectomy inthe management of head trauma. Journal of Neurosurgery, 42, 429–433.
Will, R. G. and Matthews, W. B. (1982) Evidence for case-to-case transmissionof Creutzfeldt-Jacob disease. Journal of Neurology, Neurosurgery and Psy-chiatry, 45, 235–238.
Working Party Report (1994) Antimicrobial prophylaxis in neurosurgery andafter head injury. Infection in Neurosurgery Working Party of the BritishSociety for Antimicrobial Chemotherapy. Lancet, 344, 1547–1551.
