2004 05-29-ci non miraculum est
TRANSCRIPT

Cochlear Implant –non est miraculum
Dr. Monika LehnhardtCernobbio, May 29, 2004

The first hearing impression

Nucleus® system 3
Nucleus ® 24 Contour Advance™
ESPrit™ 3G

Implant development – the state of the art

Speech Processor development –the state of the art

Failures

Hard failure vs. soft failure
CI24M after strong impact
Hard failure• A device requires explantation due to design weakness,
manufacturing fault, external impact or electrode failure with loss of clinical benefit.
Soft failure• Deviation from the specification with no loss of clinical
benefit. Resolved via programming.

The Cochlear Reporting Standard•“Any explantation which is assessed to be required because of loss of clinical benefit due to the device not meeting its specifications.”
• Outright Device failures e.g. IC• Failure due to external impact• Failure due to fatigue caused by placement error• Failure of array resulting in loss of clinical benefit
Cochlear implant manufacturers are not obliged by any international certification standards to report failures caused by external agents, such as impact to the head. However, Cochlear believes that since the implant is in a part of the body that is vulnerable to impact,especially for children, there is an ethical responsibility to report all failures resulting from impact with an external agent
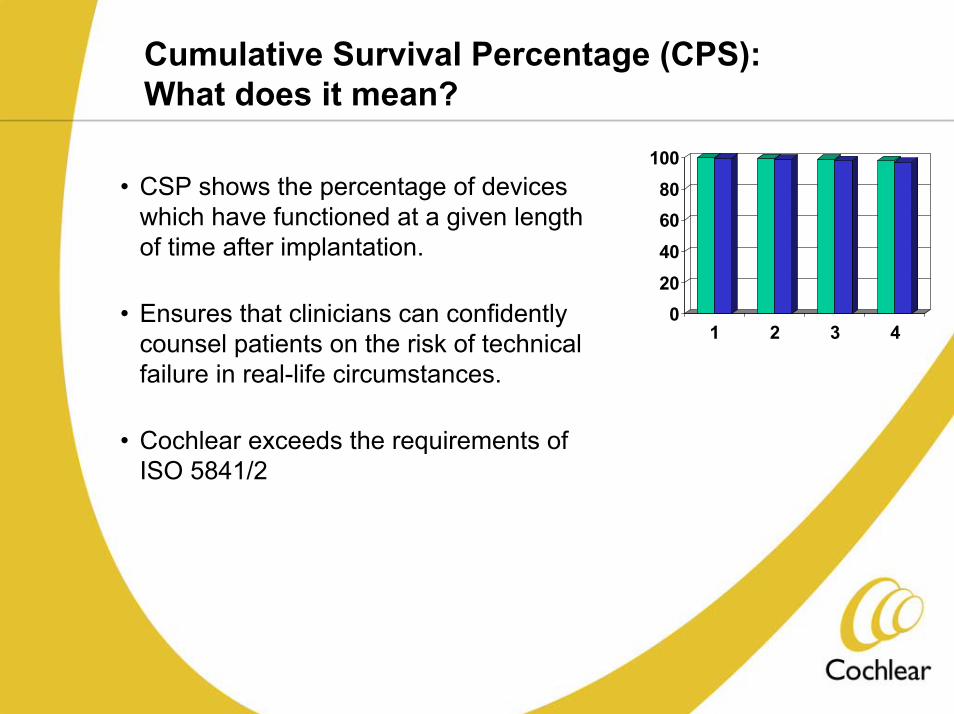
Cumulative Survival Percentage (CPS): What does it mean?
020406080
100
1 2 3 4
• CSP shows the percentage of devices which have functioned at a given length of time after implantation.
• Ensures that clinicians can confidently counsel patients on the risk of technical failure in real-life circumstances.
• Cochlear exceeds the requirements of ISO 5841/2

Cumulative Survival Percentage, CI24R November 2003

Cumulative Survival Percentage, CI24M November 2003

„Human Failures“
•Medical
•Audiological
•Therapeutic
•Psychological
•Sociological

Selection criteria FDA – Broadening IndicationsDevelopment of candidate selection criteria United States (Nucleus Implant Systems)
12 months and older3-6 months hearing aid trialLack of progress in development of auditory skills or <30% score on MLNT or LNT test, depending on age
Limited benefit from hearing aids defined as 60%or less in best aided condition on tape recorded tests of open-set sentences
2000
18 months and older3-6 months hearing aid trial<20% score on MLNT or LNT test
Limited benefit from hearing aids defined as 40%or less in best aided condition on tape recorded tests of open-set sentences
1998
Include pre-and perilinguistically deafened adults Limited benefit from hearing aids defined as 30%or less in best aided condition on tape recorded tests of open-set sentences
1995
FDA approval for implantation of candidates aged2 years and olderprofound bilateral sensorineuronal deafnesslittle or no benefit from hearing aidcandidate and family must be well motivated and possess realistic expectations
1990
FDA approval for implantation of candidates aged18 years and olderpostlingually deafenedprofound bilateral sensorineuronal deafness no benefit from hearing aid
1985
ChildrenAdults

Neonatal hearing screening – OAE and AABR
Otoacoustic Emissions (OAE)
Automated Auditory Brainstem Response (AABR)

Cost effectiveness
Poorvalueformoney
Goodvalue
formoney
CI beforeage 4
0 1 2 3 4 5 6
Cos
t (€)
0
20000
40000
60000
80000
100000
CI betweenages 4 and 6
QALYs gained0 1 2 3 4 5 6
CI afterage 6
0 1 2 3 4 5 6
73 yrs 73 yrs 73 yrs
15 yrs 15 yrs 15 yrs

Soft Surgery

CT and MRI picture of the Cochlea
Image Source: Courtesy of the University of Melbourne

Programming session with a child

Programming session with a child and parent

Auditory-Verbal Philosophy
Auditory-Verbal International, Inc. Position Statement
• The Auditory-Verbal philosophy is a logical and critical set of guiding principles. These principles outline the essential requirements needed to realize the expectation that young children who are deaf or hard of hearing can be educated to use even minimal amounts of amplified residual hearing.
Use of amplified residual hearing in turn permits children who are deaf or hard of hearing to learn to listen, process verbal language, and to speak.
Auditory-Verbal Principles 1 – 5
1. Early detection and diagnosis
2. Aggressive audiological management
3. Appropriate amplification technology to achieve maximum benefits of learning through listening
4. Favourable auditory learning environments for the acquisition of spoken language including individualized therapy
5. Integrating listening into the child’s entire being so listening becomes a way of life

Auditory-Verbal Principles 6 – 10 6. Ongoing assessment, evaluation and prognosis of the
development of audition, speech, language and cognition
7. Integration and mainstreaming of the children who are deaf or hard of hearing into regular education classes to fullest extent possible
8. Active participation of parents in order to improve spoken communication between the child and family members
9. Affirmation of parents as primary models in helping the child learn to listen to his or her own voice, the voice of others and the sounds of the environment
10. Integration of speech, language, audition and cognition in response to the psychological, social and educational needs of the child and family

Parents with Child

Cochlear Implant – a Miracle?