2008 canadian copd guidelines definition of copd: “chronic obstructive pulmonary disease (copd) is...
TRANSCRIPT


2008 Canadian COPD Guidelines
Definition of COPD:
“Chronic obstructive pulmonary disease (COPD) is
a respiratory disorder largely caused by
smoking which is characterized by progressive
partially reversible airway obstruction,
systemic manifestations, and increasing severity
and frequency of exacerbations.”
Old Definitions:
• Chronic bronchitis= chronic cough and sputum production for at least 3 months in 2 consecutive years.
• Note: this is a clinical definition
• Emphysema= Pathological loss of lung tissue distal to the terminal bronchiole.
• Note: this is a pathologic definition

EmphysemaChronic bronchitis
Asthma
COPD- classification of patients:
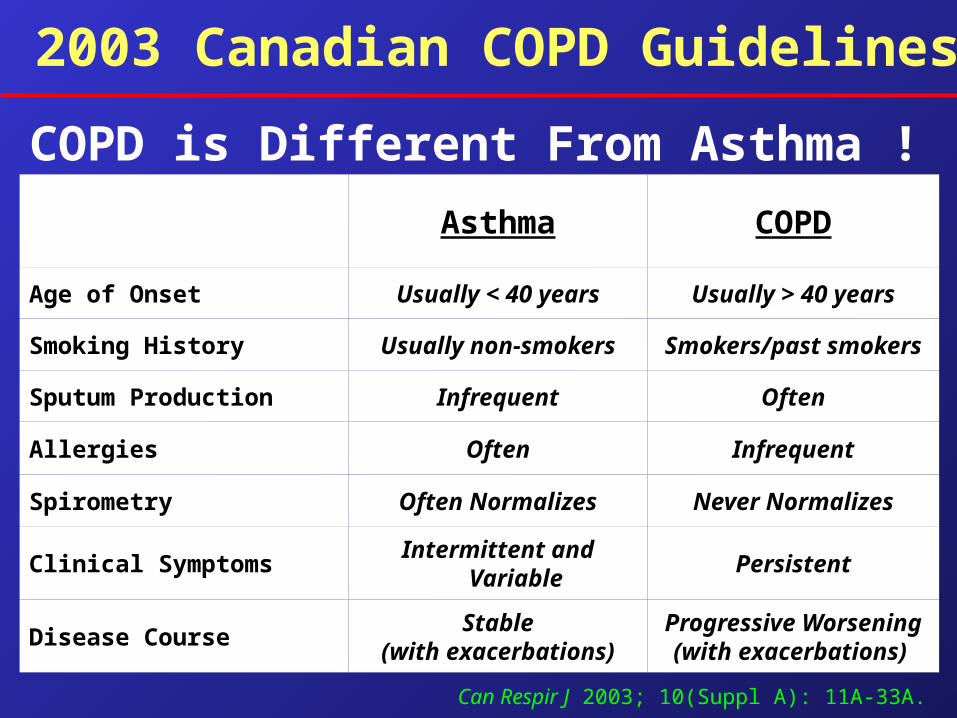
Progressive Worsening(with exacerbations)
Stable(with exacerbations)
Disease Course
PersistentIntermittent and VariableClinical Symptoms
Never NormalizesOften NormalizesSpirometry
InfrequentOftenAllergies
OftenInfrequentSputum Production
Smokers/past smokersUsually non-smokersSmoking History
Usually > 40 yearsUsually < 40 yearsAge of Onset
COPDAsthma
Can Respir J 2003; 10(Suppl A): 11A-33A.
2003 Canadian COPD Guidelines
COPD is Different From Asthma !

Percent Change in Age-Adjusted Death Rates, U.S., 1965-1998Percent Change in Age-Adjusted Death Rates, U.S., 1965-1998
00
0.50.5
1.01.0
1.51.5
2.02.0
2.52.5
3.03.0
Proportion of 1965 Rate Proportion of 1965 Rate
0.0
0.5
1.0
1.5
2.0
2.5
3.0
1965 - 19981965 - 1998 1965 - 19981965 - 1998 1965 - 19981965 - 1998 1965 - 19981965 - 1998 1965 - 19981965 - 1998
–59%–59% –64%–64% –35%–35% +163%+163% –7%–7%
CoronaryHeart
Disease
CoronaryHeart
Disease
StrokeStroke Other CVDOther CVD COPDCOPD All OtherCauses
All OtherCauses
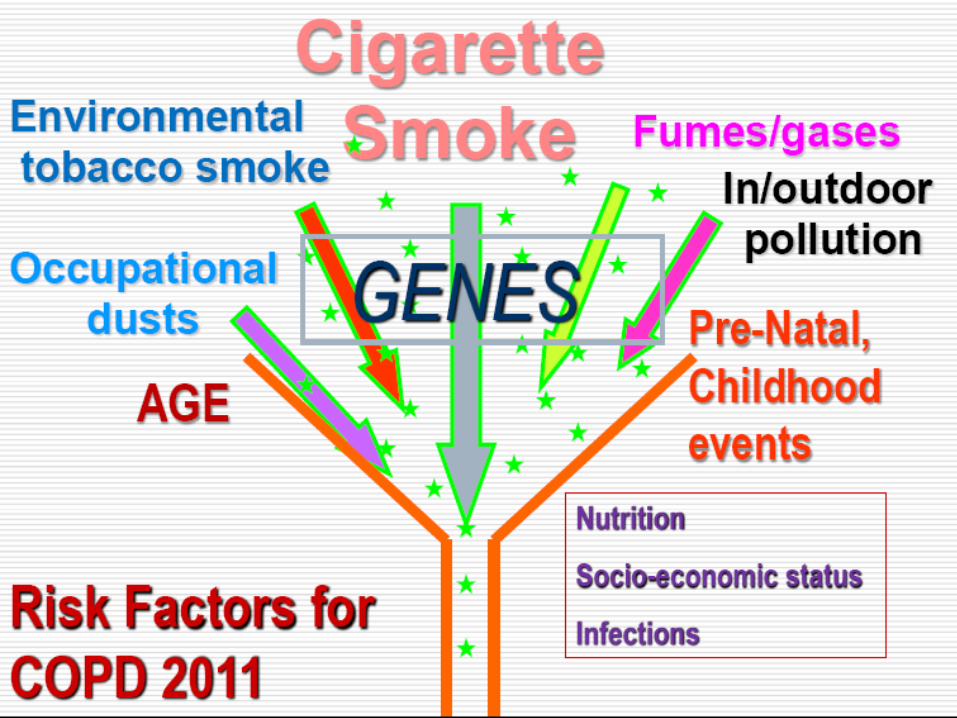
Facts About COPDFacts About COPD Cigarette smoking is the primary cause of
COPD.
In the US 47.2 million people (28% of men and 23% of women) smoke.
The WHO estimates 1.1 billion smokers worldwide, increasing to 1.6 billion by 2025. In low- and middle-income countries, rates are increasing at an alarming rate.
Cigarette smoking is the primary cause of COPD.
In the US 47.2 million people (28% of men and 23% of women) smoke.
The WHO estimates 1.1 billion smokers worldwide, increasing to 1.6 billion by 2025. In low- and middle-income countries, rates are increasing at an alarming rate.


•Facts About COPD•Facts About COPD
In India, it is estimated that 400-550 thousand premature deaths can be attributed annually to use of biomass fuels, placing indoor air pollution as a major risk factor in the country.
In India, it is estimated that 400-550 thousand premature deaths can be attributed annually to use of biomass fuels, placing indoor air pollution as a major risk factor in the country.
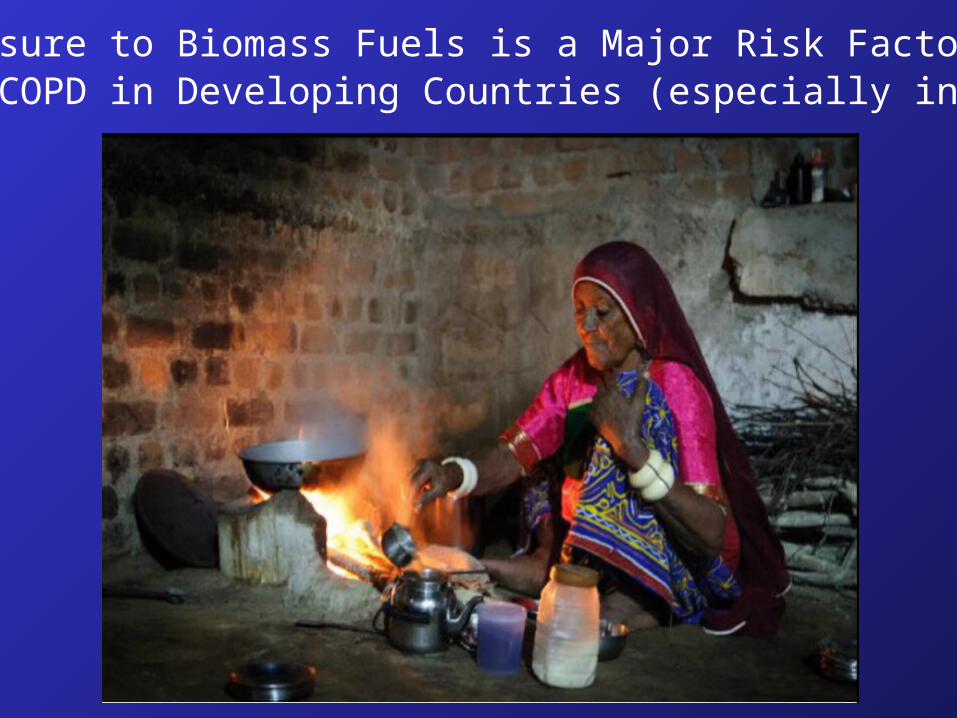
• Exposure to Biomass Fuels is a Major Risk Factor • For COPD in Developing Countries (especially in women).
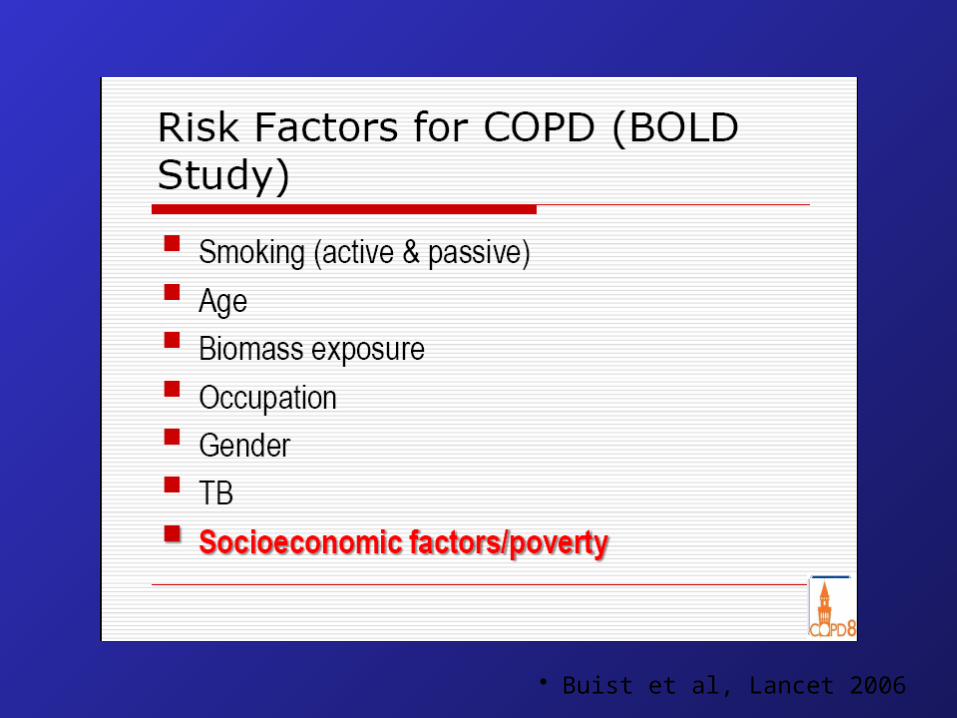
• Buist et al, Lancet 2006
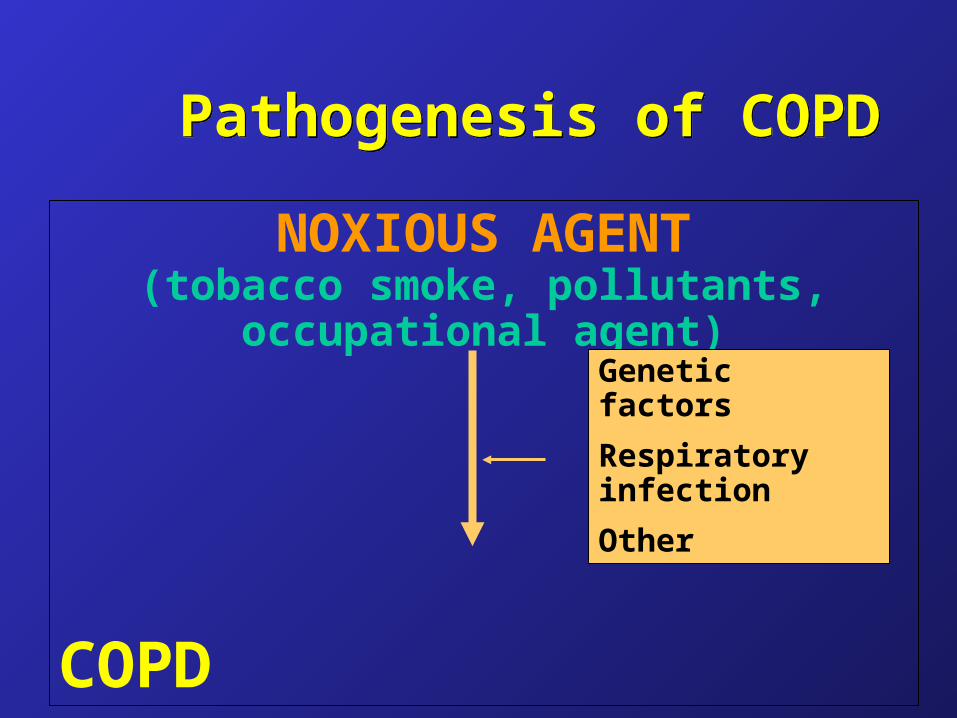
Pathogenesis of COPDPathogenesis of COPD
NOXIOUS AGENT(tobacco smoke, pollutants, occupational
agent)
COPD
Genetic factors
Respiratory infection
Other
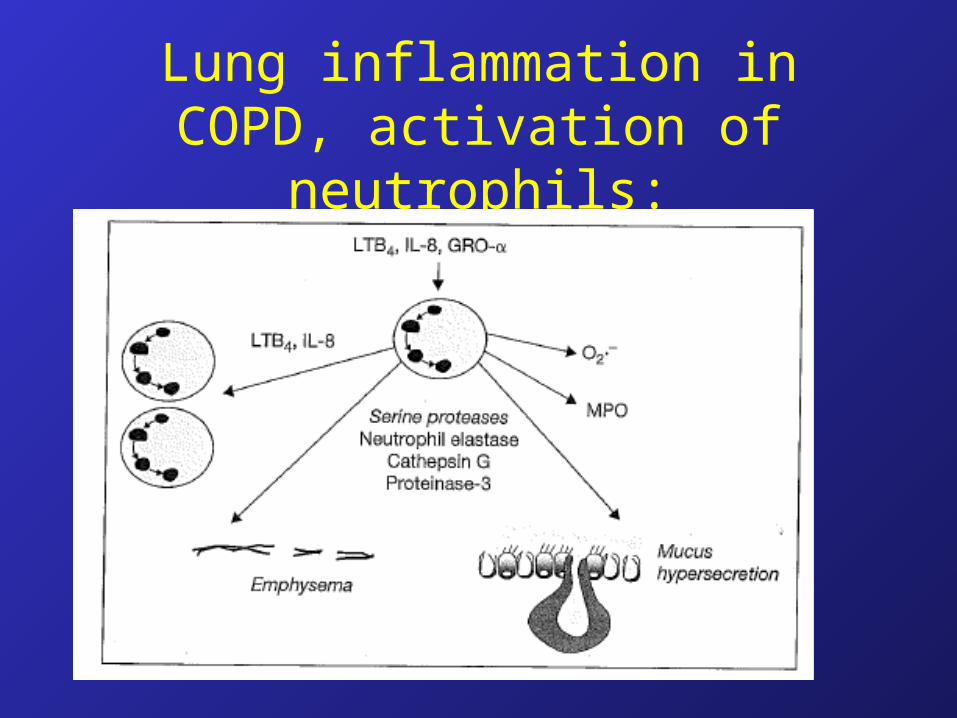
Lung inflammation in COPD, activation of neutrophils:

Noxious particles
and gases
Lung inflammation
Host factors
COPD pathology
ProteinasesOxidative stress
Anti-proteinasesAnti-oxidants
Repair mechanisms

INFLAMMATION
Small airway diseaseAirway inflammationAirway remodeling
Parenchymal destructionLoss of alveolar attachments
Decrease of elastic recoil
AIRFLOW LIMITATION
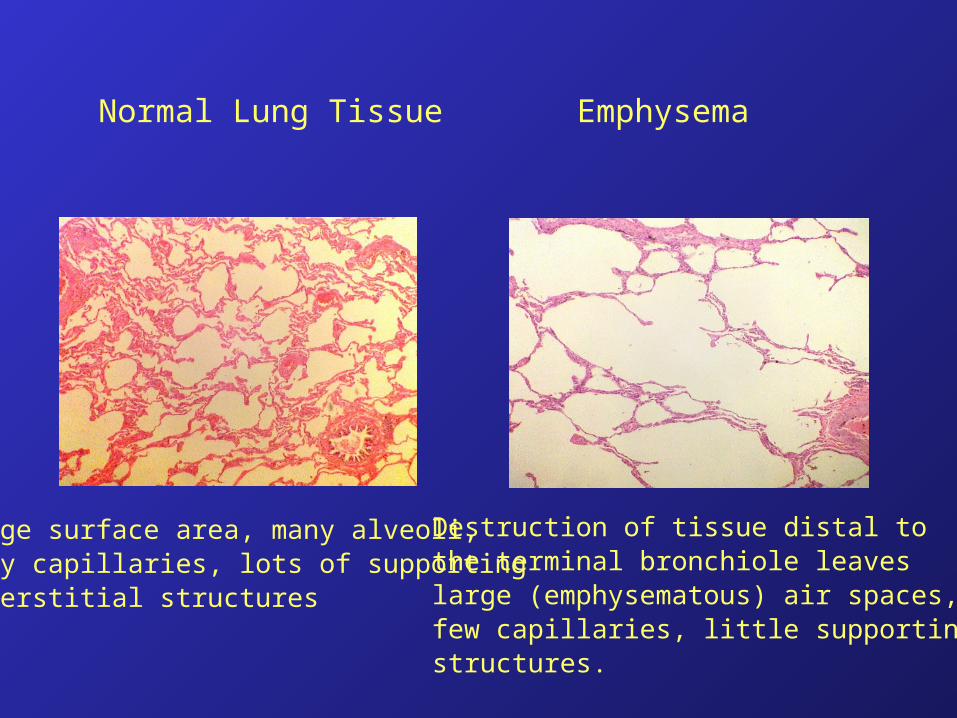
Normal Lung Tissue Emphysema
Large surface area, many alveoli,many capillaries, lots of supportinginterstitial structures
Destruction of tissue distal to the terminal bronchiole leaves large (emphysematous) air spaces,few capillaries, little supporting structures.
Emphysema
• Note that in emphysema there is destruction of the alveoli, the pulmonary capillaries, and the surrounding tissue distal to the terminal bronchiole.
• This means there is loss of the lung interstitium including loss of elastic fibers and other structures that support the alveoli and airways.
• This leads to diminished elastic recoil of the lung, (ie. increased lung compliance).

Emphysema on CT Scan
Resp Med 2000;
Murray & Nadel, Textbook of
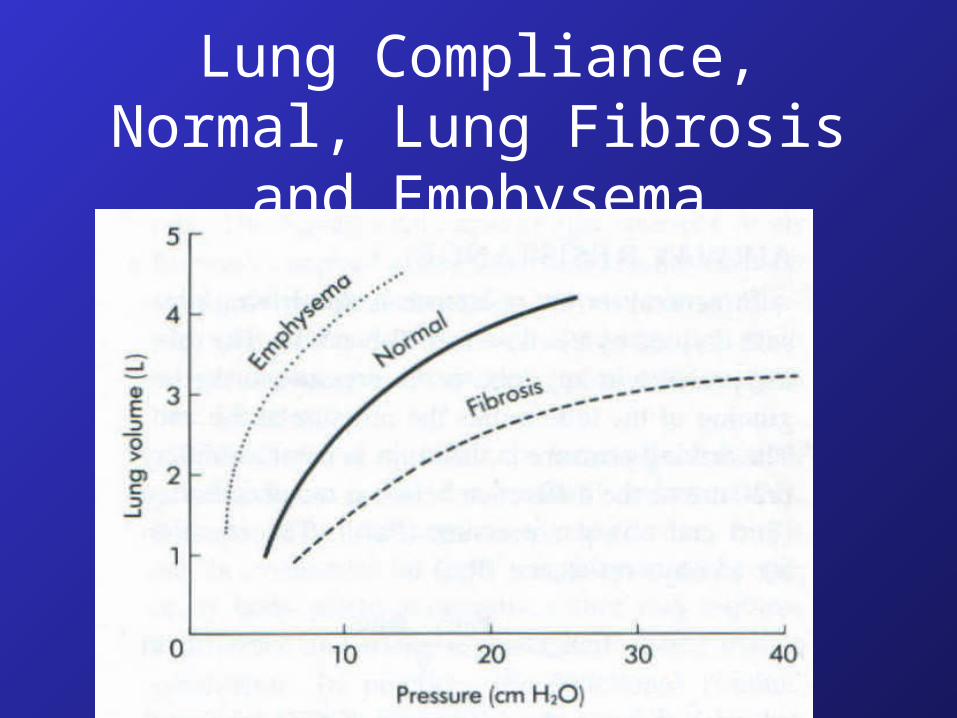
Lung Compliance, Normal, Lung Fibrosis and Emphysema
The typical COPD patient:
1) Is elderly (usually at least 45 years old)
2) Has chronic symptoms of cough, wheeze or breathlessness- SOB is progressive over time.
3) Has airway obstruction documented by spirometry.
4) Is a smoker or has smoked in the past.
“Objective demonstration of airflow obstruction by
spirometry is essential for the diagnosis of
COPD.”
2003 Canadian COPD Guidelines
Definition of Airflow Obstruction
“A post-bronchodilator FEV1 < 100% of the
predicted value associated with an
FEV1/FVC < 0.70 indicates airflow
obstruction, and both are necessary for
the diagnosis of COPD to be established.”
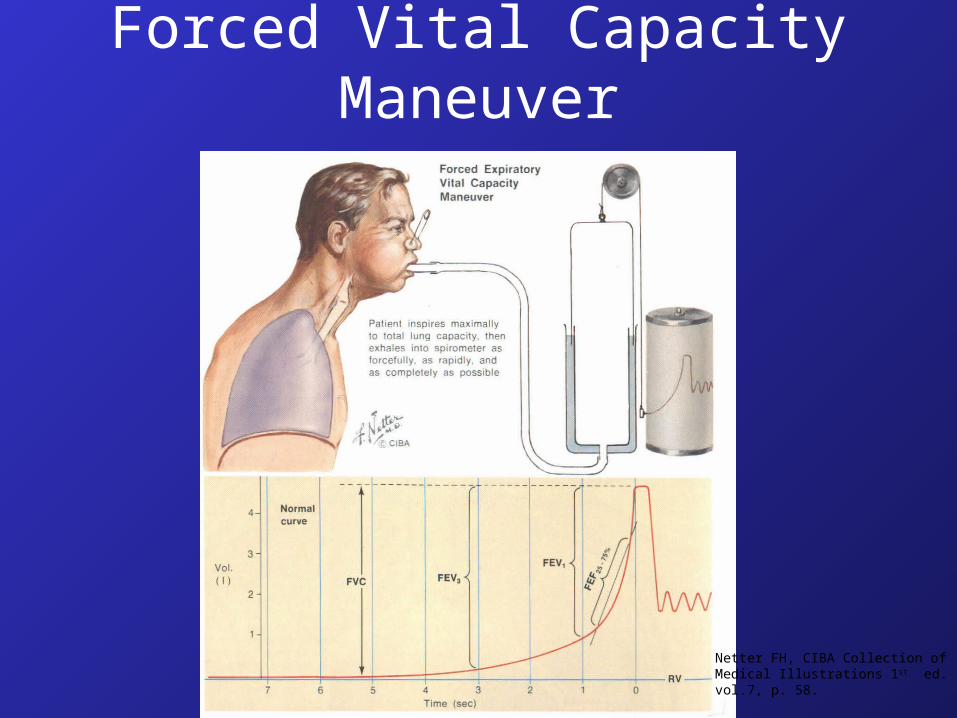
Forced Vital Capacity Maneuver
Netter FH, CIBA Collection ofMedical Illustrations 1st ed. 1979vol.7, p. 58.

Spirometry - Flow/Volume Loop
Volume (L)
Flo
w (
L/se
c)
4321
1
2
3
4
0
measured predicted
Predicted
FEV1 = 3.0 L
FVC = 4.0 L
FEV1/FVC = 75%
Measured
FEV1 = 2.0 L
FVC = 3.6 L
FEV1/FVC = 56%
0
2003 Canadian COPD Guidelines
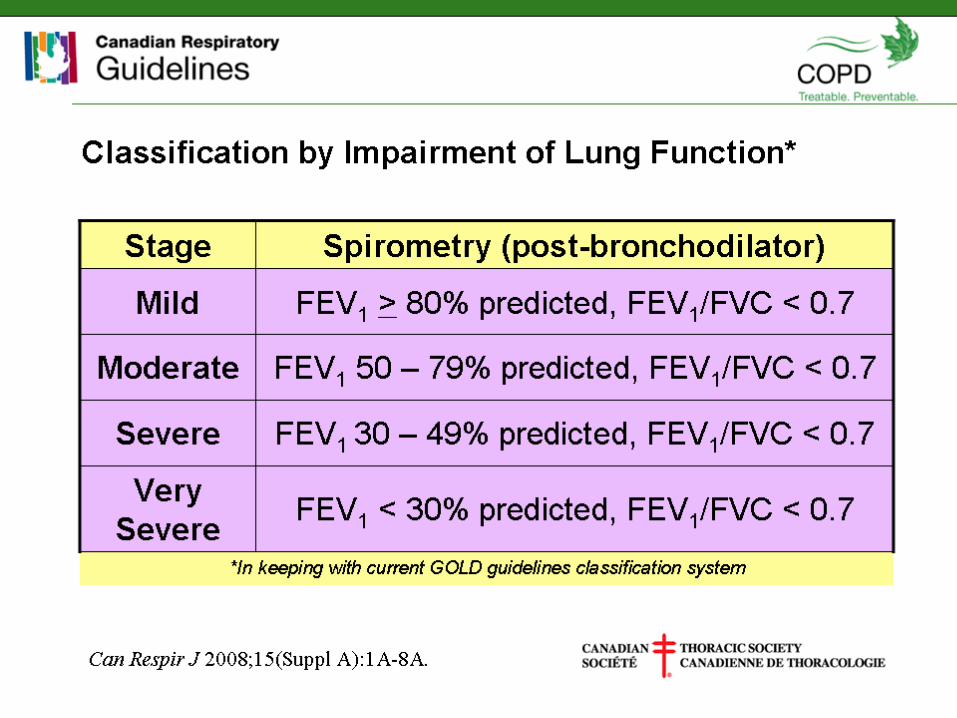
Classification by Impairment of Lung Function
Causes of Airflow Obstruction:
• Irreversible–Loss of elastic recoil due to alveolar
destruction–Destruction of alveolar support that
maintains patency of small airways–Fibrosis and narrowing of the
airways
Causes of Airflow Obstruction:
• Partially Reversible–Accumulation of inflammatory cells,
mucus, and plasma exudate in bronchi
–Smooth muscle contraction in peripheral and central airways

Forced Expiration with Pleural Pressure of 20 cm H2O

Emphysema, loss of small airway supporting structures:
• Small airways lack alveolar structural support.
• With expiration, +vepleural and intrathoracicpressures create smallairway closure.
• This traps air behind theequal pressure point
• Alveoli can’t empty
• Results in air trapping andhyperinflation.
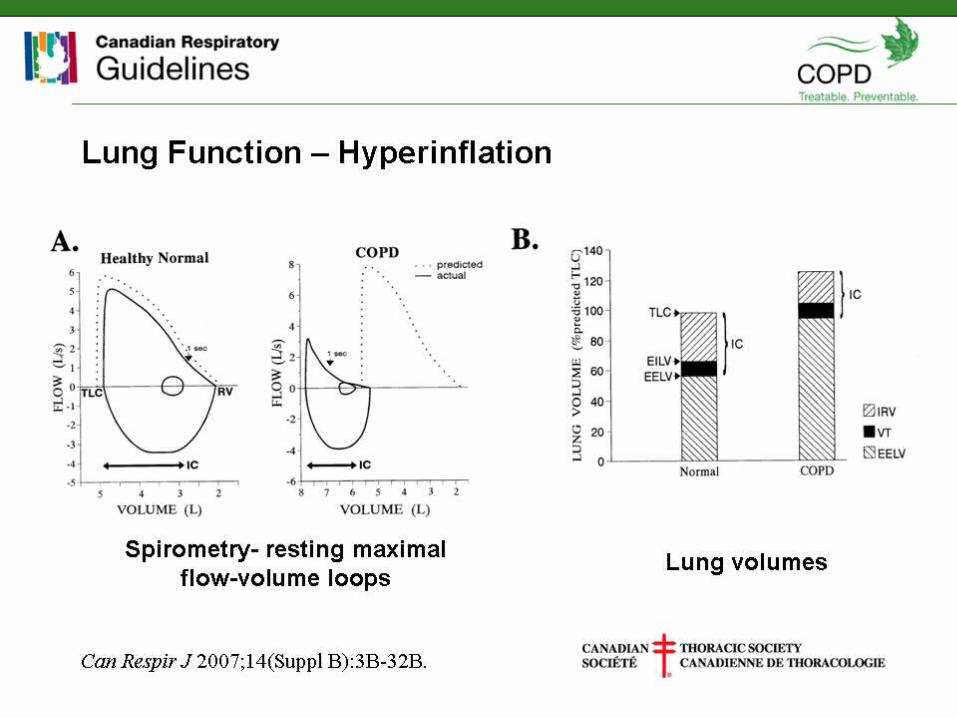
Lung Function - Hyperinflation
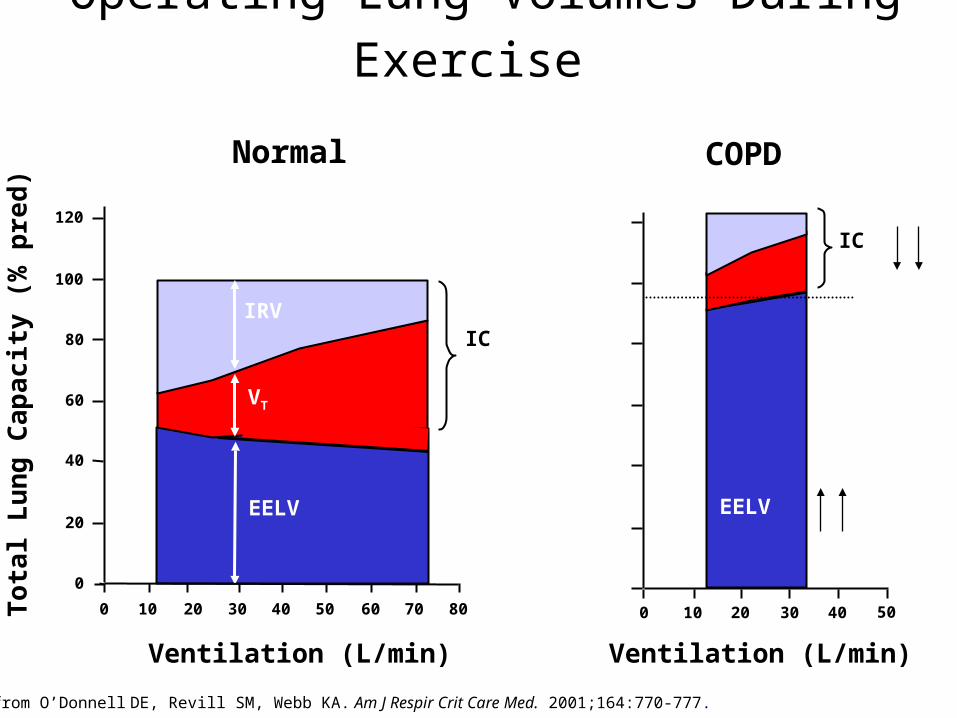
Operating Lung Volumes During Exercise
Adapted from O’Donnell DE, Revill SM, Webb KA. Am J Respir Crit Care Med. 2001;164:770-777.
Ventilation (L/min)
0
20
40
60
80
100
120
Tota
l Lu
ng
Ca
pac
ity
(%
pre
d)
EELV
IRV
VT
Normal
0 10 20 30 40 50 60 70 80
IC
COPD
0 10 20 30 40 50
IC
Ventilation (L/min)
EELV

COPD Classification by Symptoms and Disability
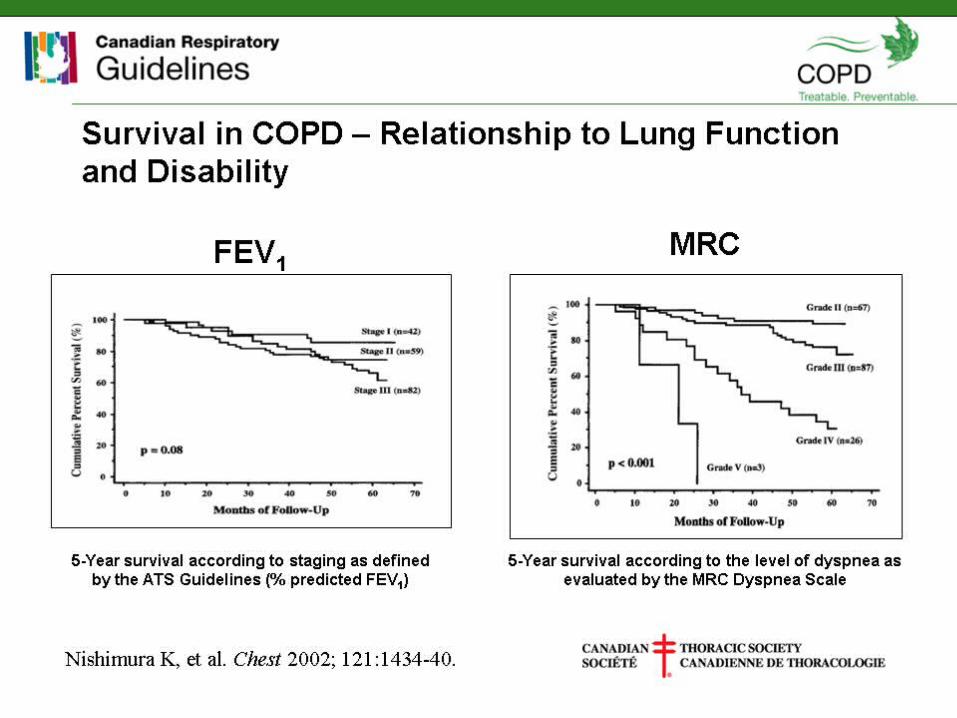
Survival in COPD – Relationship to Lung Function and Disability
Goals of COPD Management• Prevent disease progression• Relieve symptoms• Improve exercise tolerance • Improve health status• Prevent and treat complications• Prevent and treat exacerbations• Reduce mortality• Prevent or minimize side effects from treatment
• GOLD Workshop Report 2003

What Decreases Mortality?Non-Pharmacologic
• Smoking cessation• Flu shot• Pneumonia vaccine• Pulmonary Rehab
Pharmacologic• Oxygen• Systemic Steroids• Antibiotics• SABA (Ventolin)• Anti-cholinergics • Theophylline• Inhaled Steroids• LABAs• Combo ICS/LABA• Roflumilast
• • X
• X
• X
• • X
• X
• X
• X
• X
• X
• X
• X
• X

First step in COPD management:
• Patient education, education, education!
• Smoking Cessation!• Exercise!
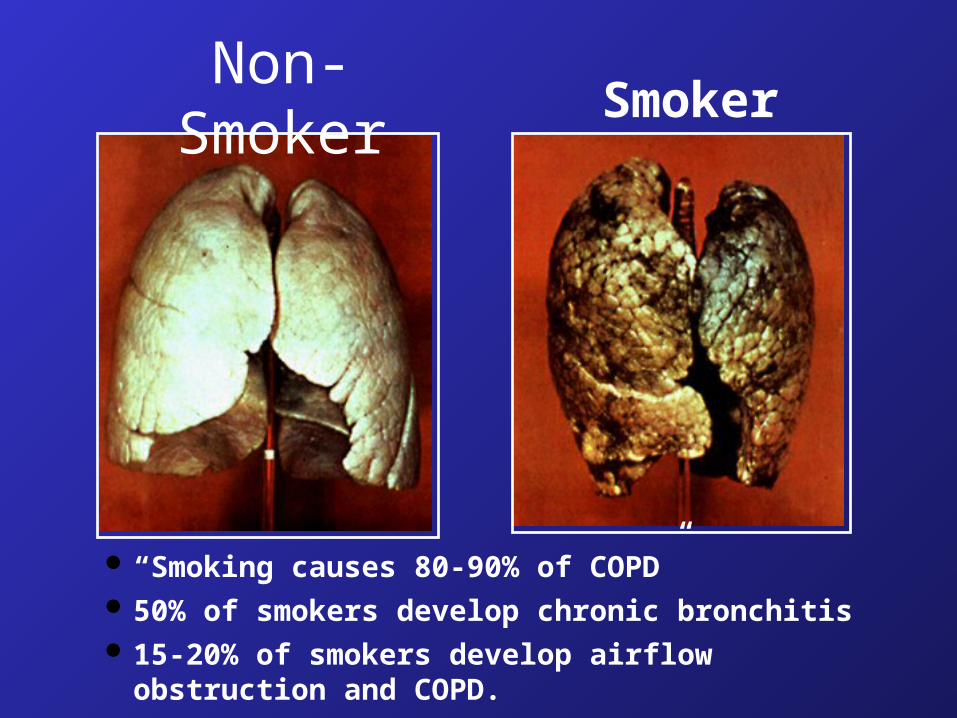
“Smoking causes 80-90% of COPD” 50% of smokers develop chronic bronchitis 15-20% of smokers develop airflow obstruction and
COPD.
Non-Smoker Smoker
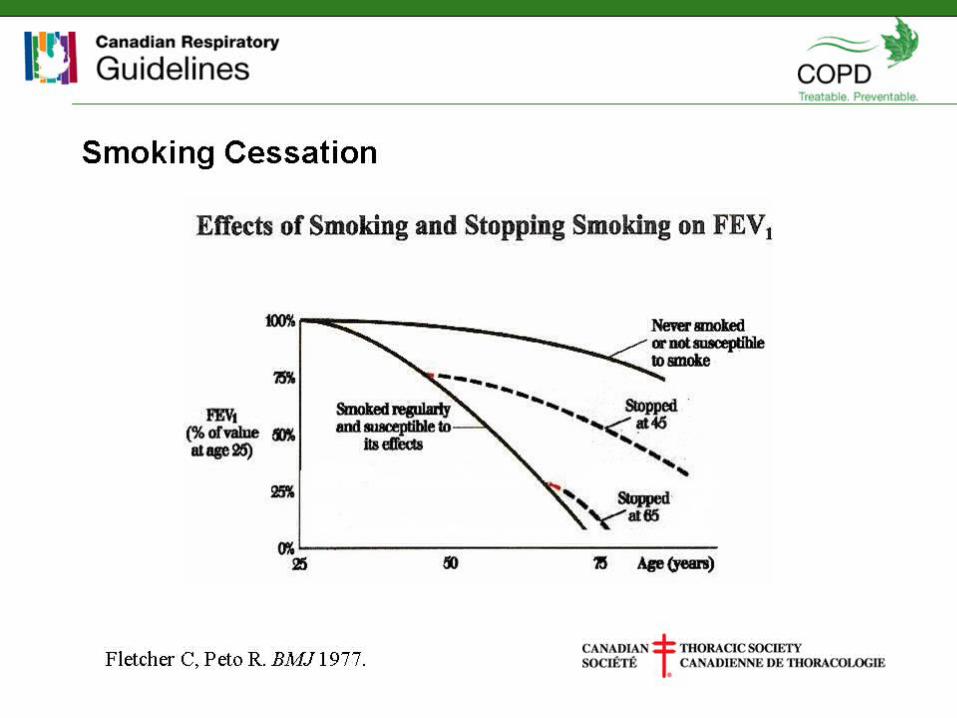
Smoking Cessation

Decline of Lung Function in Susceptible Smokers:
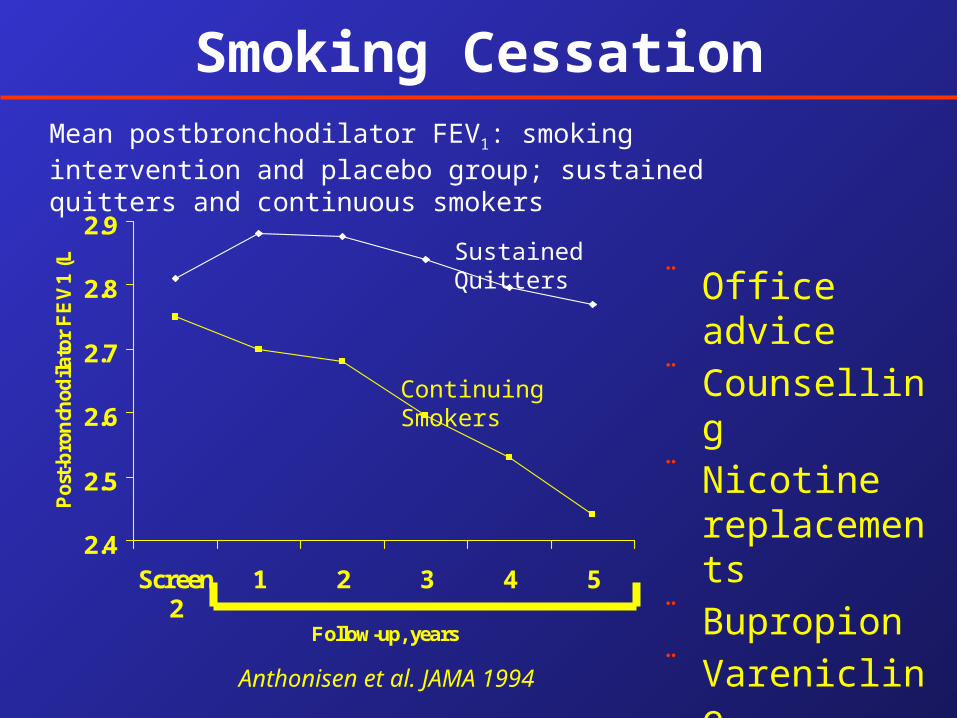
Smoking CessationMean postbronchodilator FEV1: smoking intervention and placebo group; sustained quitters and continuous smokers
¨ Office advice¨ Counselling¨ Nicotine
replacements¨ Bupropion¨ Varenicline2.4
2.5
2.6
2.7
2.8
2.9
Screen2
1 2 3 4 5
Follow-up, years
Pos
t-b
ron
chod
ilato
r F
EV
1 (L
)
Anthonisen et al. JAMA 1994
Continuing Smokers
Sustained Quitters

Dyspnea: Its importance in COPD
• Most common symptom
• Intensifies as the disease progresses
• Reason most patients seek medical attention
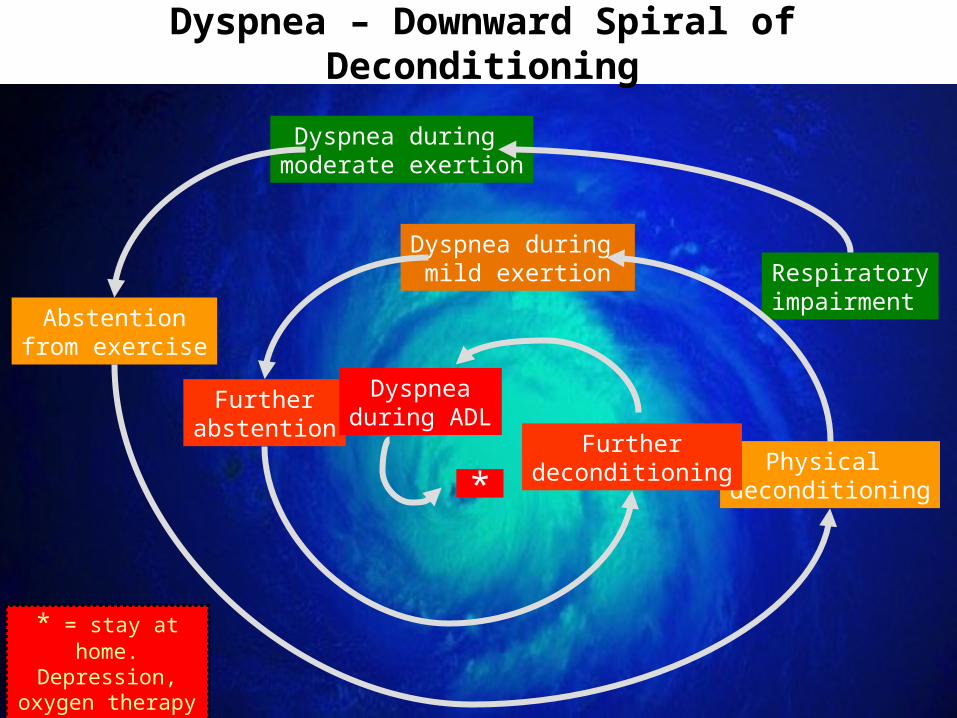
Dyspnea – Downward Spiral of Deconditioning
Respiratoryimpairment
Dyspnea during moderate exertion
Abstentionfrom exercise
Physical deconditioning
Dyspnea during mild exertion
Furtherabstention
Furtherdeconditioning
Dyspneaduring ADL
*
* = stay at home. Depression, oxygen
therapy etc.

Pulmonary Rehabilitation
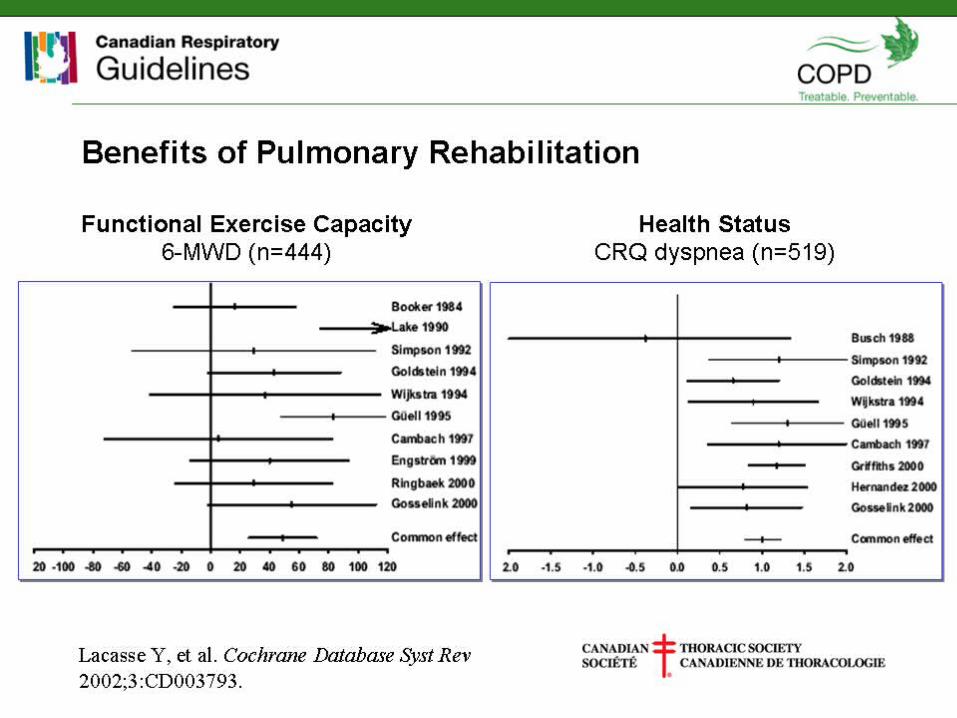
Benefits of Pulmonary Rehabilitation
Summary: Epidemiology of COPD
• COPD is highly prevalent, it affects at least 8% of Canadians > 65 years old.
• After smoking, age is the second biggest independent risk factor for COPD.
• In the developing world exposure to pollution and biomass fuels is also an important risk factor.
• COPD is now an ‘equal-opportunity disease’ when it comes to gender.
• COPD is a poor person’s disease- more prevalent in patients of lower SES.
Summary: Treatment for COPD
• FEV1 relentlessly declines; only smoking cessation will halt progression.
• Education/pulmonary rehabilitation/smoking cessation are unsexy therapies but they work best!
• Long-acting BD’s are indicated for most patients to improve symptoms, exercise and QOL.
• For patients with severe COPD and hypoxemia at rest- home oxygen will prevent cor pulmonale and improve survival.