2010 fluoroscopy safety recertification tutorial
TRANSCRIPT
Radiation protection review for credentialed fluoroscopy operators @ BWH
Dept. of Health Physics and RadiopharmacologyBrigham and Women’s Hospital
Radiation protection review for credentialed fluoroscopy operators @
BWH
Purpose:
Review safe practices of fluoroscopy, including radiation protection strategies for patients and staff
Review occupational dosimetry program Comply with Massachusetts regulations Stimulate dialogue amongst fluoroscopy users and
radiation oversight committees
Radiation protection review for credentialed fluoroscopy operators @
BWH
Who is responsible for fluoroscopy oversight?
Government: U.S. FDA, Massachusetts DPH* Accreditation organizations: JCAHO, ACR BWH Radiation Safety Committee Medical Directors of Radiology, Cardiology, etc.
* inspects and enforces regulations

Radiation protection regulations
105CMR120 Massachusetts Regulations for the Control of Radiation120.400: X‑RAYS IN THE HEALING ARTS120.405: Fluoroscopy
Describes: Shielding requirements Tube output, beam filtration and limitation Exposure and dose rate limits Recording of fluoroscopy time and dose Protection from scattered x-rays Operator qualifications………
Radiation protection regulations
120.405: X‑RAYS IN THE HEALING ARTS Operator Qualifications.
(1) A facility shall ensure that only a l icensed physician or a radiologic technologist who is trained in the safe use of fluoroscopic x-ray systems licensed in accordance with 105 CMR 125.000 shall be allowed to operate these systems. All persons using fluoroscopic x-ray systems shall have, at a minimum, documented training in the topics specified 105 CMR 120.405(K)(2).
Radiation protection regulations120.405: X‑RAYS IN THE HEALING ARTS
Describes: Operator training:
(2) Training to meet requirements of 105 CMR 120.405(K)(1) shall include, but not be limited to the following:
(a) Principles and operation of the fluoroscopic x-ray system; (b) Biological effects of x-ray; (c) Principles of radiation protection; (d) Fluoroscopic outputs; (e) High level control options; (f) Dose reduction techniques for fluoroscopic x-ray systems;
and (g) Application requirements of 105 CMR 120.000.
Radiation protection regulations
120.405: X‑RAYS IN THE HEALING ARTS
Describes: Operator training:
(3) The facility shall maintain all records relating to compliance with the training requirements for five years.
(4) The facility shall establish policies and procedures for restricting the use of fluoroscopic systems to only those physicians who have been granted privileges for the use of fluoroscopy based on a determination of adequate training and knowledge of the curriculum of 105 CMR 120.405(K)(2).
(5) The facility shall ensure that all non-radiologist physician using fluoroscopy equipment obtain annual training in Radiation Safety/Radiation Protection and maintain all records relating to compliance with this training requirement for five years.
Fluoroscopy safety training @ BWH
Since 1990:
All new fellows, residents, and attending physicians undergo a training course with take-home reading
materials, exam, and fluoroscopy competency assessment.
Upon successful completion, are issued a certificate and entered into BICS as holding Fluoroscopy privileges
Ad hoc retraining/radiation safety in-services presented
Fluoroscopy safety training @ BWH
As of 2008 (non-radiologist physicians):
BICS Fluoroscopy privileges will expire annually Recertification takes place by viewing study materials
and retuning quiz to Health Physics Ad hoc retraining/radiation safety in-services
presented
Somatic and genetic damage depends on exposure parameters
the quantity of ionizing radiation to which the subject is exposed
the rate of exposure the ionization ability of the radiation the volume of tissue exposed the types of tissues exposed

Activity Disintegration/sec=1 Becquerel (Bq) 37 billion Bq = 1 curie
Dose (Absorbed) 1 joule/kg=1 Gray(Gy) 1Gray=100 rad =100,000 mrad
Dose (Equivalent) Gray x quality factors= Sievert (Sv) 1 Sievert =100 rem =100,000 mrem
Radiation Units
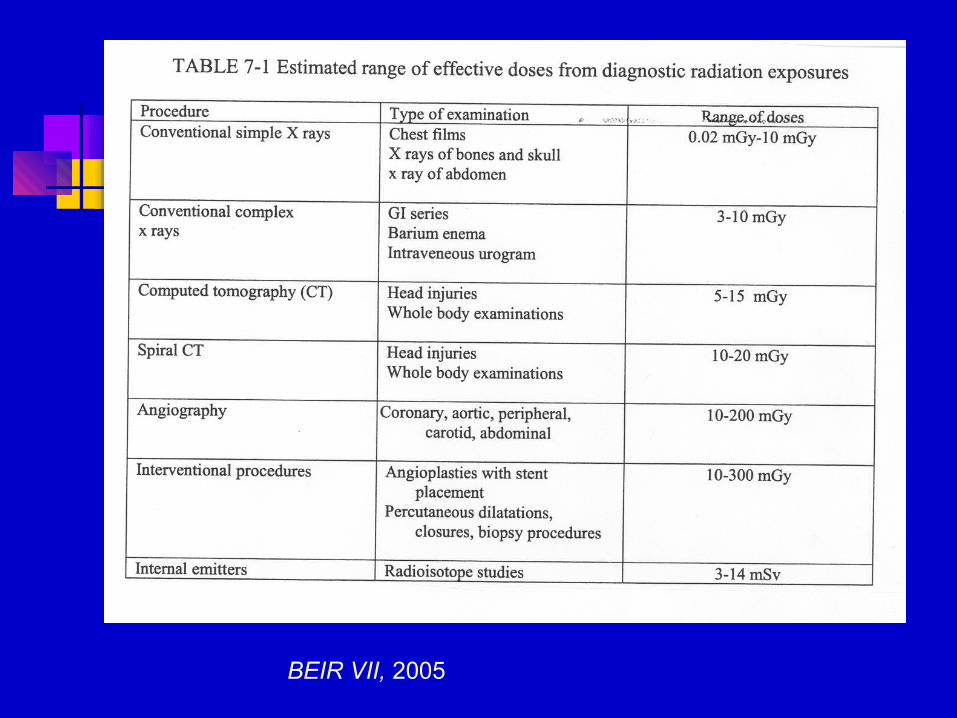
BEIR VII, 2005
Radiation risks
Stochastic effects(= non-threshold, increasing probability with dose)
genetic mutationgenomic instabilitycancer induction
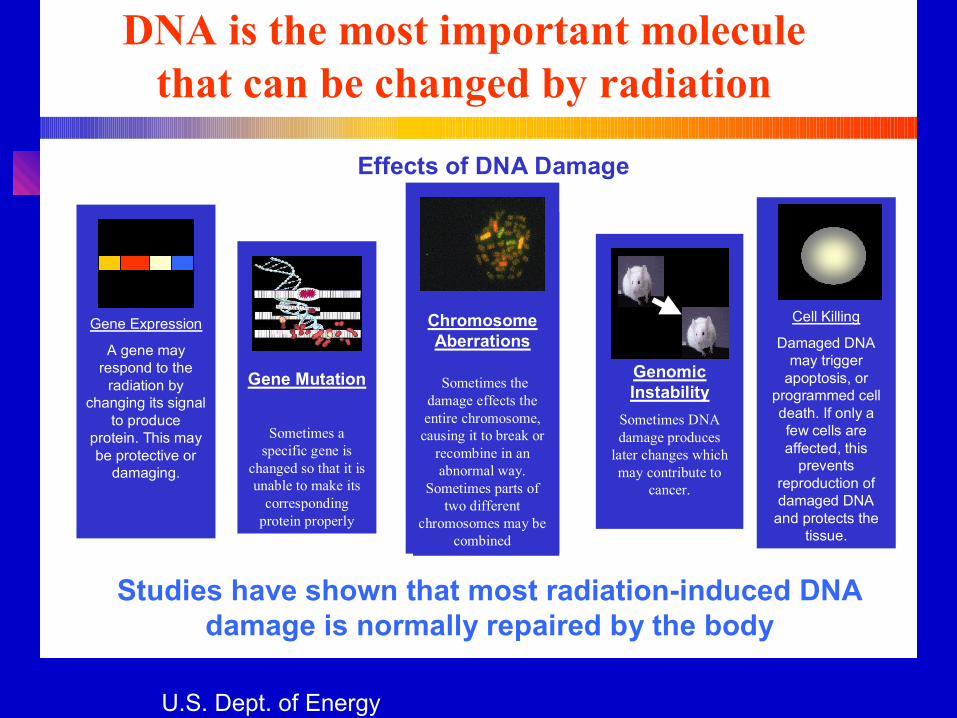
GenomicInstability
Sometimes DNA damage produces
later changes which may contribute to
cancer.
Gene Expression
A gene may respond to the
radiation by changing its signal
to produce protein. This may be protective or
damaging.
Effects of DNA Damage
DNA is the most important moleculethat can be changed by radiation
Studies have shown that most radiation-induced DNA damage is normally repaired by the body
Gene Mutation
Sometimes a specific gene is
changed so that it is unable to make its
corresponding protein properly
Chromosome Aberrations
Sometimes the damage effects the entire chromosome,
causing it to break or recombine in an abnormal way.
Sometimes parts of two different
chromosomes may be combined
Cell Killing
Damaged DNA may trigger
apoptosis, or programmed cell death. If only a few cells are affected, this
prevents reproduction of damaged DNA
and protects the tissue.
U.S. Dept. of Energy
Review for credentialed fluoroscopy
operators @ BWH
Risks of radiation exposure:
In 2004, ionizing radiation classified as a known carcinogen by the US. National Toxicology Program.The category "known to be a human carcinogen" is reserved forthose substances for which there is sufficient evidence of carcinogenicity from studies in humans that indicates a causal relationship between exposure to the agent, substance, or mixture and human cancer."
Radiogenic cancer = stochastic risk
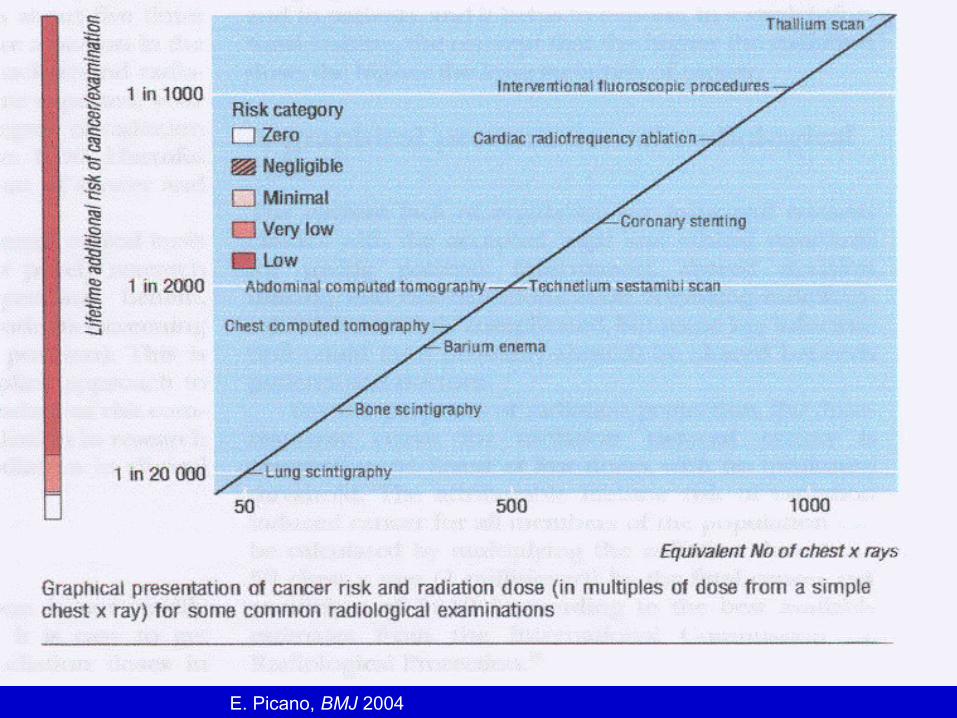
E. Picano, BMJ 2004
Radiation risks(non-stochastic)
Commonly referred to as deterministic effects:
threshold-related symptoms worsen with dose includes:
Skin changes (erythema /hair loss/ulceration) Cataracts Teratogenesis
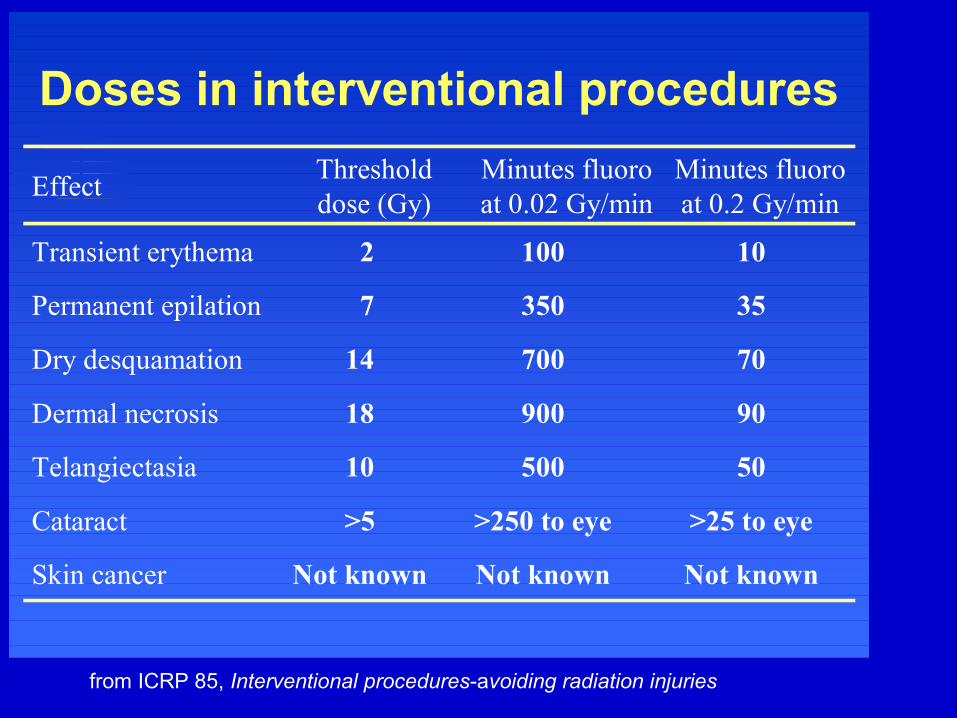
Doses in interventional procedures
Not knownNot knownNot knownSkin cancer
>25 to eye>250 to eye>5Cataract
5050010Telangiectasia
9090018Dermal necrosis
7070014Dry desquamation
353507Permanent epilation
101002Transient erythema
Minutes fluoro at 0.2 Gy/min
Minutes fluoro at 0.02 Gy/min
Threshold dose (Gy)
Effect
from ICRP 85, Interventional procedures-avoiding radiation injuries
Radiation – dose limits, patients?Even with increased utilization of imaging procedures and image-guided interventions, there is no maximum permissible dose or procedure volume for medically indicated procedures.
Weigh risk vs. benefit Advise patient if deterministic effect possible If patient is pregnant, consider limited exam, or alternative (MRI,
sonography) Utilize dose-saving protocols
Fluoroscopy dose-saving protocols
Whenever and wherever possible:
Limit beam-time on (use last image hold) Reduce tube current (mA) Use lower pulse sequence fluoroscopy Limit magnification Maintain adequate x-ray source-skin distance Keep Image intensifier as close as possible to patient Apply positive beam limitation (collimators) Record* and minimize fluoroscopy time
Fluoroscopy dose reporting 105 CMR 120 (as of 6 OCT 2006)
Each facility performing fluoroscopically-guided
interventional procedures shall conduct patient dose
evaluation for any procedure that has a reasonable
probability of resulting in a deterministic injury as
further defined in 105CMR120.405(L)(5). *
* Any cumulative absorbed dose to the skin equal to or greater than 1 Gy (100 rads)
Review for credentialed fluoroscopy
operators @ BWH * Record and minimize fluoroscopy time
Fluoroscopy procedures in which the dose exceeds1,000 mGy are reported to Medical Physics for dose calculations which are then sent to the:
Radiation Safety Officer Radiation Safety Committee In some instances, the patient’s primary care physician
will be notified for deterministic effect surveillance and patient follow-up.
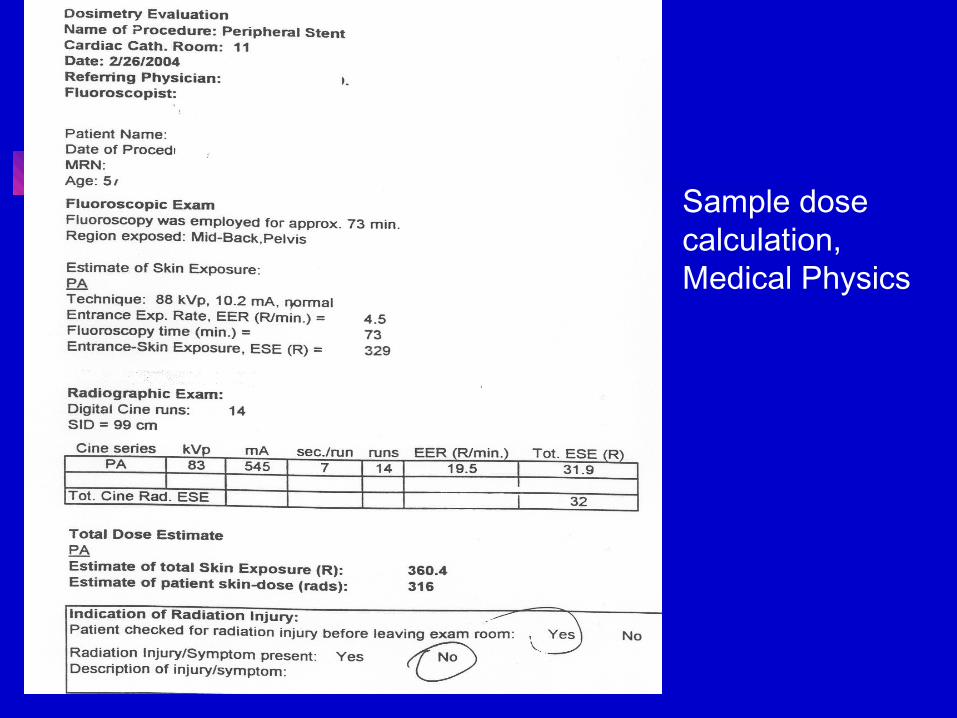
Sample dosecalculation,Medical Physics
Law of Bergonié and Tribondeau = rapidly dividing, less differentiated cells more sensitive to radiation effects…..therefore the conceptus is at higher risk.
Pregnant females should not be irradiated unless absolute medical necessity
Pregnant radiation workers restricted to much lower doses.
Why limit exposure to pregnant patients (and staff)?
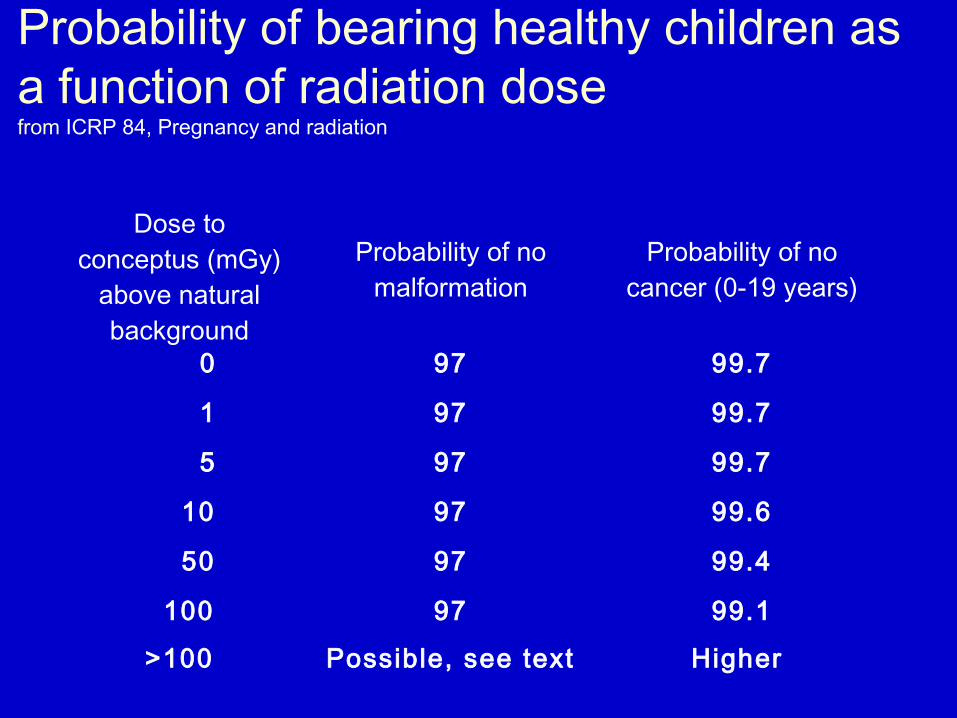
Probability of bearing healthy children as a function of radiation dose from ICRP 84, Pregnancy and radiation
Dose to conceptus (mGy)
above natural background
Probability of no malformation
Probability of no cancer (0-19 years)
0 97 99.7
1 97 99.7
5 97 99.7
10 97 99.6
50 97 99.4
100 97 99.1
>100 Possible, see text Higher
Conceptus dose, interventional procedures(mGy)
For BWH-specific protocols, please see:
http://brighamrad.harvard.edu/education/fetaldose/
Part III-Occupational exposures and radiation protection program
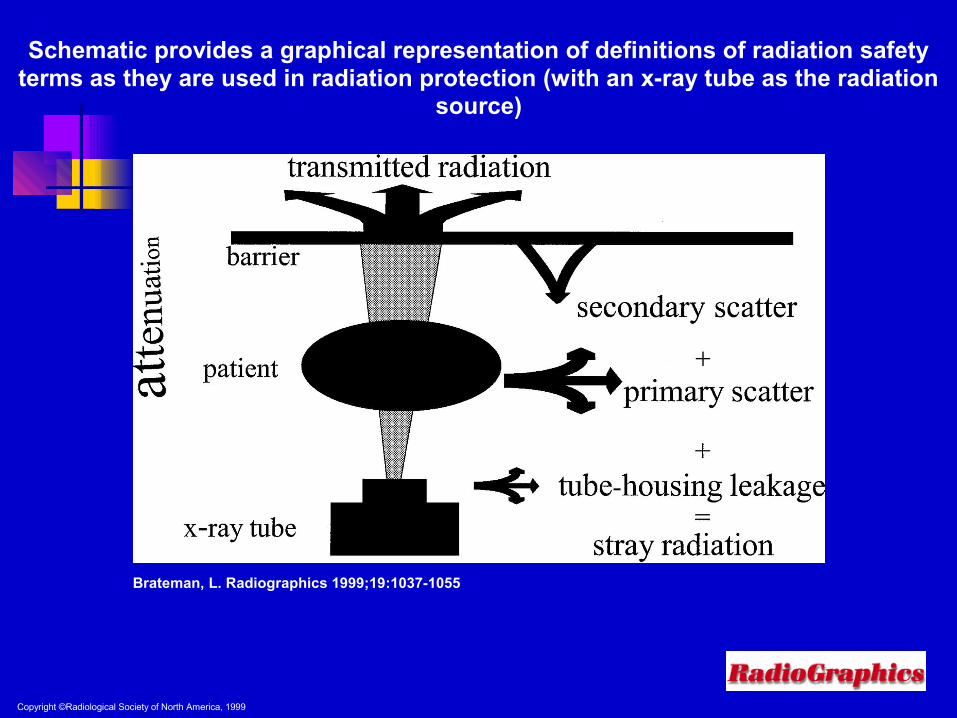
Copyright ©Radiological Society of North America, 1999
Brateman, L. Radiographics 1999;19:1037-1055
Schematic provides a graphical representation of definitions of radiation safety terms as they are used in radiation protection (with an x-ray tube as the radiation
source)
Scattered radiation fields
Various studies have shown scattered radiation in a fluoroscopy procedure
room will range from 0.03 to 0.5 R per hour of actual x-ray beam time.
D. Allard, CHP; Health Physics Society
Radiation – dose limits for staff
Maximum permissible dose, annual limits:
Occupational workers:
Whole body = 5,000 mrem/yr (= 50 mSv) Eyes = 15,000 mrem/yr (= 150 mSv) Skin = 50,000 mrem/yr (= 500 mSv)
Radiation – occup.dose limits
If declared pregnancy= 500 mrem/gestational period (5.0 mSv)
= not to exceed 50 mrem/month (0.5 mSv)
Radiation safety strategies
Decrease time around source
Increase distance from source
Use appropriate shielding
Contamination control (PPE)
Monitor badge reports - ALARA
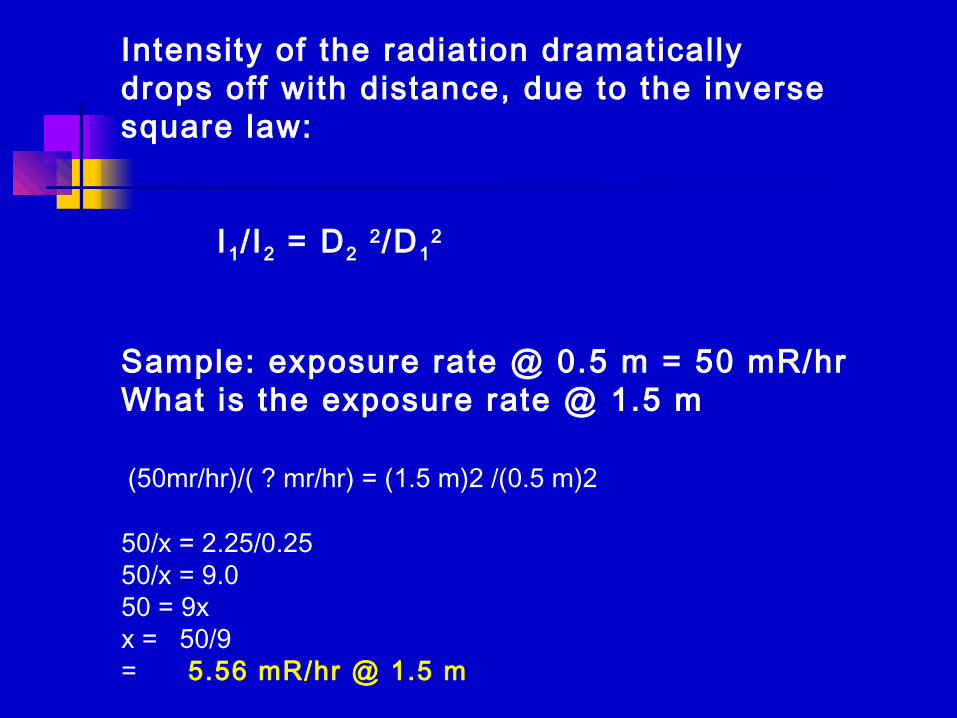
Intensity of the radiat ion dramaticallydrops off with distance, due to the inverse square law:
I1/ I2 = D2 2/D12
Sample: exposure rate @ 0.5 m = 50 mR/hr What is the exposure rate @ 1.5 m (50mr/hr)/( ? mr/hr) = (1.5 m)2 /(0.5 m)2
50/x = 2.25/0.2550/x = 9.050 = 9xx = 50/9= 5.56 mR/hr @ 1.5 m
Staff and trainees working with ionizing radiation are issued monthly radiation
dosimeters. You may be issued:
- a single collar badge, with red icon (WORN ABOVE Pb APRON)
- a single whole body badge, with black icon (WORN BELOW Pb APRON)
- both badges, if you regularly operate the fluoroscope during interventional studies.
- a ring badge, if you handle > 1.0 mCi of radionuclides
- a fetal dose monitor, if pregnancy declared
- an Area monitor badge will be placed in your workspace if little to no exposure is anticipated
Dosimeter exposure estimates calculated several ways
EDE 1 – 2 dosimeters; one worn at waist (under Pb apron), the other at collar level (outside of Pb apron)
Assigned deep dose =[1.5 (waist) + 0.04 (collar)]
most commonly done with routine fluoroscopy
Dosimeter exposure estimates
EDE 2 – one whole body dosimeter worn at collar level (outside of Pb apron)
Assigned deep dose = 0.3 x (whole body badge)
most commonly used for occasional fluoroscopy users
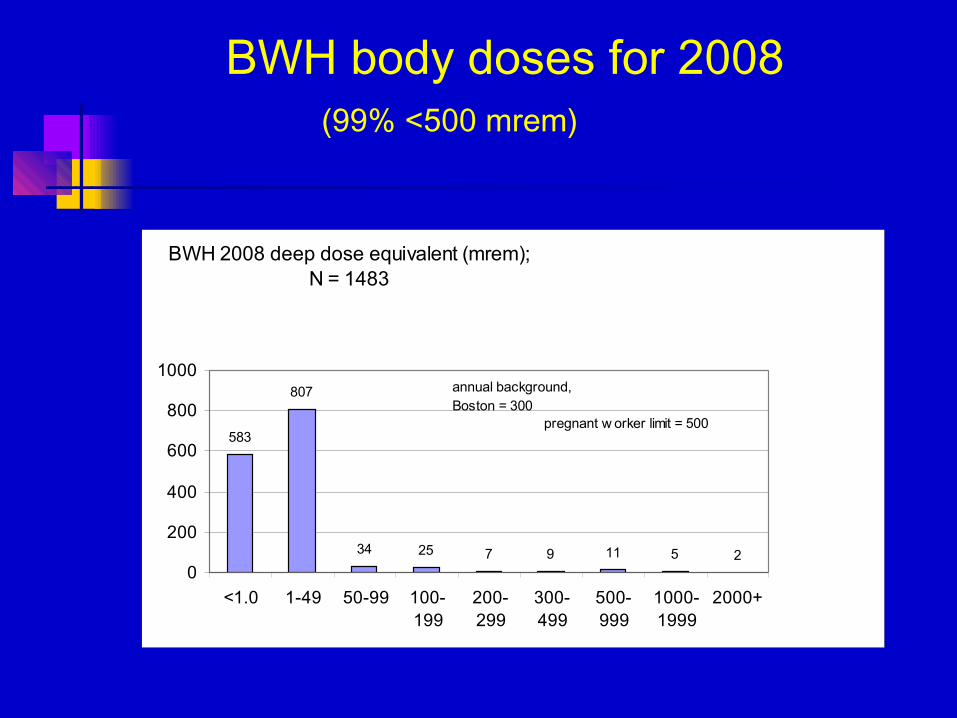
BWH body doses for 2008(99% <500 mrem)
BWH 2008 deep dose equivalent (mrem);N = 1483
583
807
34 25 7 9 11 5 20
200
400
600
800
1000
<1.0 1-49 50-99 100-199
200-299
300-499
500-999
1000-1999
2000+
pregnant w orker limit = 500
annual background,Boston = 300
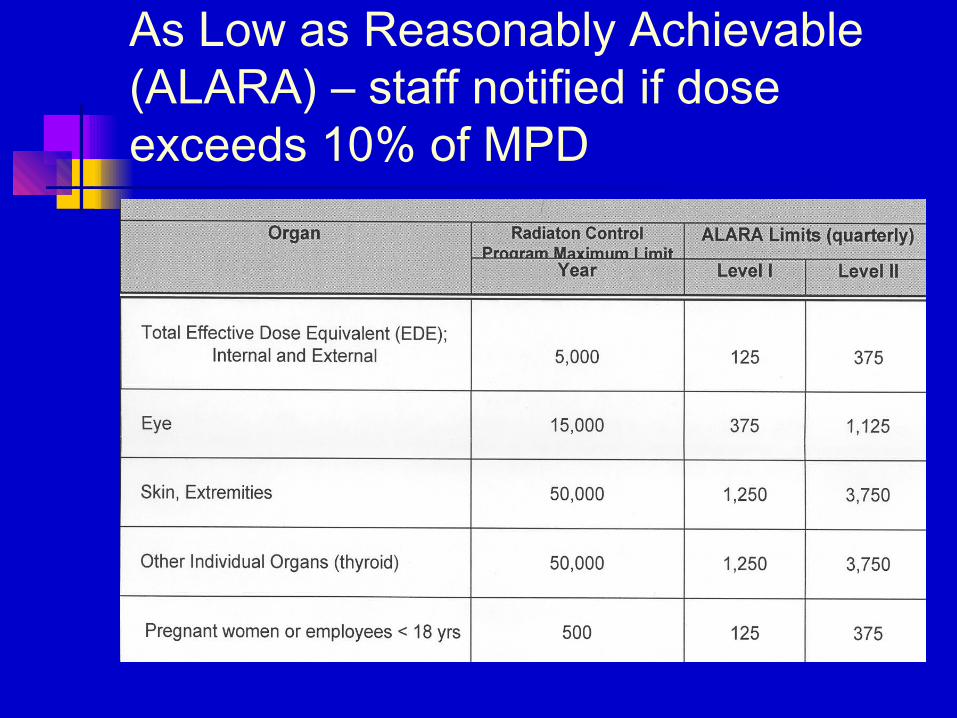
As Low as Reasonably Achievable (ALARA) – staff notified if dose exceeds 10% of MPD
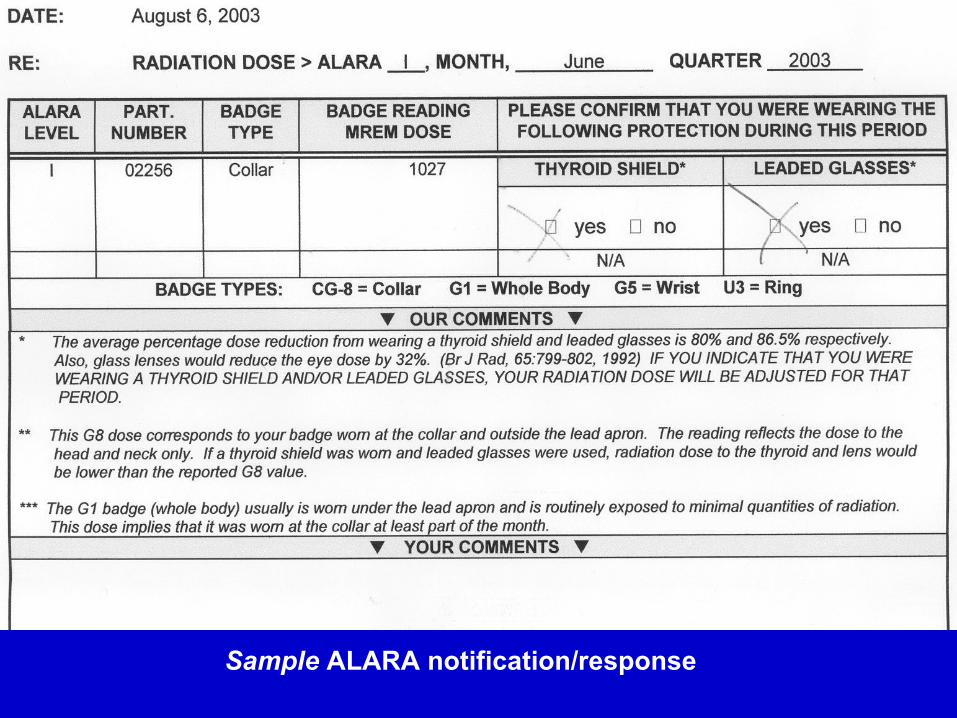
Sample ALARA notification/response
BWH Radiation Safety Contacts
Health Physics @ RadiopharmacologyMain # = 617 732 605624 hr emergency pager = 33330
Christopher Martel, MS, DABHPDirector & Radiation Safety Officer= 617 732 6057
A. Robert Schleipman, RT, CNMT, MScEducation, Occupational Dosimetry= 617 732 5963
Medical Physics, RadiologyRichard Nawfel, MSPatient dose calculations= 617 732 7201
Radiation Safety Liaisons have been established for each area to assist you with badges, Pb PPE, etc.
CDIC = Kelley Grassi, RTEP Lab = Jim McConville, RT, CNMTEndoscopy = Sandra Cialfi, RNPain Management = Diane Palombi, RNInterventional Radiology = Carol Upson, RTDiagnostic (L1) Radiology = Charles David Healy, RTEmergency Dept. = Angela McLaughlin, RTNuclear Medicine = Victor Gerbaudo, PhDO.R. Nursing = Mike Bickerstaff, RNO.R. Radiology equipment = Steve Kenary, RT
Radiation protection review for credentialed fluoroscopy operators @
BWH
Process:
BICS fluoroscopy credential expires annually Participant reviews slide show Participant contacts RSO with any questions Participant completes and returns quiz BICS Fluoroscopy credentials renewed for 12 months