2013-2014 retiree benefits brochure for classified - socccd
TRANSCRIPT
2013-2014 Retiree Benefits Brochure
for Classified Members
DISCLAIMER The information in this brochure is a general outline of the benefits offered under the SOCCCD benefits program. Specific details and limitations are provided in the plan documents which may include a Summary Plan Description (SPD), Evidence of Coverage (EOC) and/or insurance policies. The plan documents contain the relevant plan provisions. If the information in this brochure differs from the plan documents, the plan documents will prevail.
WHAT’S INSIDE
Retiree Benefits Checklist ...................................... 2
Frequently Asked Questions .................................. 3
Medical Plans ........................................................ 6
Dental Plan .......................................................... 11
Vision Plan .......................................................... 11
Rules For Benefit Changes During The Year ......... 12
Required Federal Notices .................................... 13
Health Plan Rates ................................................ 15
Who Should You Call? ......................................... 16
Dear Retiree: South Orange County Community College District takes pride in offering a comprehensive benefit program to all eligible members. It has been our goal to provide you and your families with a "best-in-class" benefits program and we believe we have achieved that goal.
2013/2014 PLAN OFFERINGS: Retirees Under Age 65
Medical: - Blue Shield HMO Plan or
- Blue Shield PPO Plan
Dental: - Delta Dental PPO Plan Vision: - VSP Plan AD&D: - Zurich Insurance (eligible benefit to age 70)
Retirees Age 65+ who are enrolled in Medicare A and B
Medical: - Blue Shield COB PPO Plan (retirees and their spouses/domestic partners age 65+) or - Companion Care Medicare Supplement Plan (retirees and their spouses/domestic partners age 65+) or
- Blue Shield 65+ HMO Medicare Advantage Plan (retirees age 65+)
Dental: - Delta Dental PPO Plan (voluntary/retiree paid) Vision: - VSP Plan (voluntary/retiree paid) AD&D: - Zurich Insurance (eligible benefit to age 70)
2
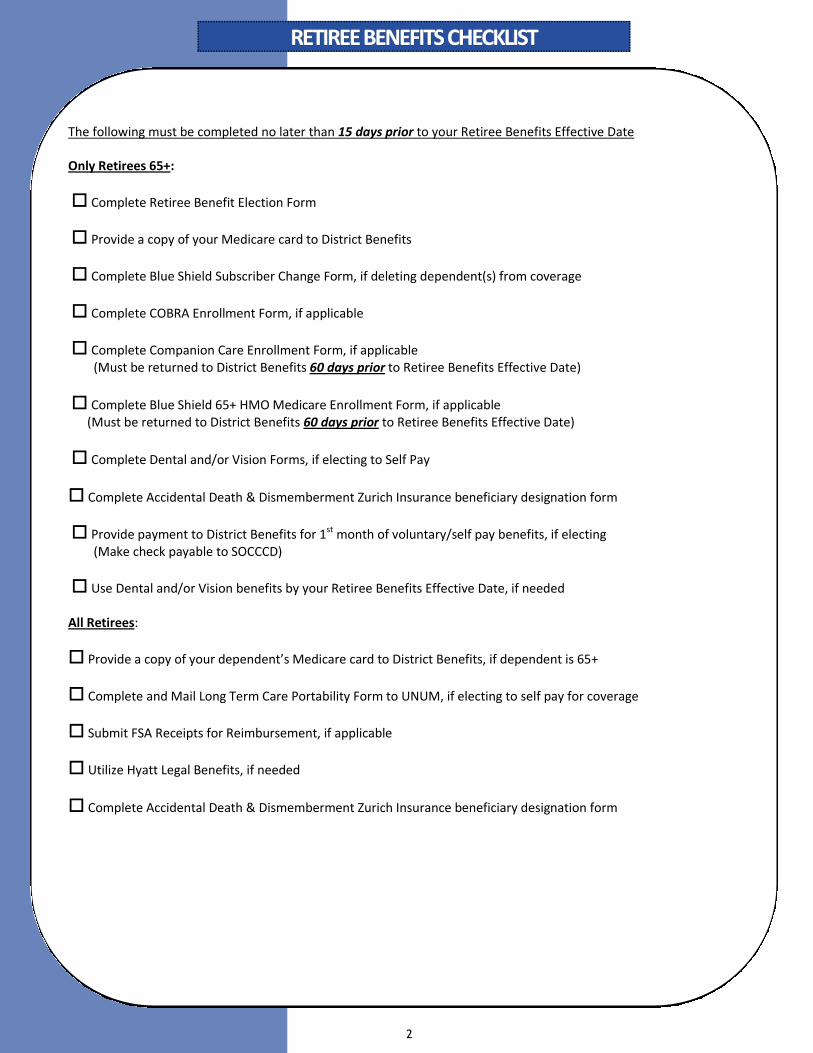
The following must be completed no later than 15 days prior to your Retiree Benefits Effective Date Only Retirees 65+:
Complete Retiree Benefit Election Form
Provide a copy of your Medicare card to District Benefits
Complete Blue Shield Subscriber Change Form, if deleting dependent(s) from coverage
Complete COBRA Enrollment Form, if applicable
Complete Companion Care Enrollment Form, if applicable (Must be returned to District Benefits 60 days prior to Retiree Benefits Effective Date)
Complete Blue Shield 65+ HMO Medicare Enrollment Form, if applicable (Must be returned to District Benefits 60 days prior to Retiree Benefits Effective Date)
Complete Dental and/or Vision Forms, if electing to Self Pay
Complete Accidental Death & Dismemberment Zurich Insurance beneficiary designation form
Provide payment to District Benefits for 1st month of voluntary/self pay benefits, if electing (Make check payable to SOCCCD)
Use Dental and/or Vision benefits by your Retiree Benefits Effective Date, if needed All Retirees:
Provide a copy of your dependent’s Medicare card to District Benefits, if dependent is 65+
Complete and Mail Long Term Care Portability Form to UNUM, if electing to self pay for coverage
Submit FSA Receipts for Reimbursement, if applicable
Utilize Hyatt Legal Benefits, if needed
Complete Accidental Death & Dismemberment Zurich Insurance beneficiary designation form
RETIREE BENEFITS CHECKLISTRETIREE BENEFITS CHECKLISTRETIREE BENEFITS CHECKLIST
3
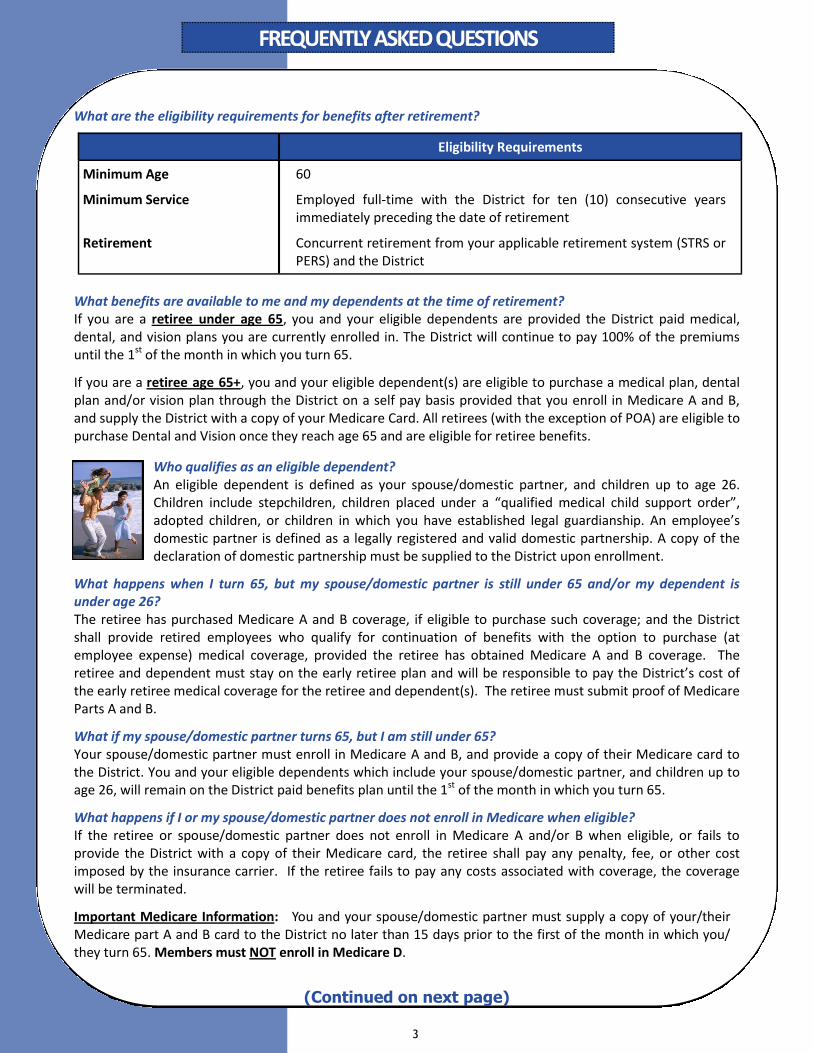
What are the eligibility requirements for benefits after retirement?
What benefits are available to me and my dependents at the time of retirement? If you are a retiree under age 65, you and your eligible dependents are provided the District paid medical, dental, and vision plans you are currently enrolled in. The District will continue to pay 100% of the premiums until the 1st of the month in which you turn 65.
If you are a retiree age 65+, you and your eligible dependent(s) are eligible to purchase a medical plan, dental plan and/or vision plan through the District on a self pay basis provided that you enroll in Medicare A and B, and supply the District with a copy of your Medicare Card. All retirees (with the exception of POA) are eligible to purchase Dental and Vision once they reach age 65 and are eligible for retiree benefits.
Who qualifies as an eligible dependent? An eligible dependent is defined as your spouse/domestic partner, and children up to age 26. Children include stepchildren, children placed under a “qualified medical child support order”, adopted children, or children in which you have established legal guardianship. An employee’s domestic partner is defined as a legally registered and valid domestic partnership. A copy of the declaration of domestic partnership must be supplied to the District upon enrollment.
What happens when I turn 65, but my spouse/domestic partner is still under 65 and/or my dependent is under age 26? The retiree has purchased Medicare A and B coverage, if eligible to purchase such coverage; and the District shall provide retired employees who qualify for continuation of benefits with the option to purchase (at employee expense) medical coverage, provided the retiree has obtained Medicare A and B coverage. The retiree and dependent must stay on the early retiree plan and will be responsible to pay the District’s cost of the early retiree medical coverage for the retiree and dependent(s). The retiree must submit proof of Medicare Parts A and B.
What if my spouse/domestic partner turns 65, but I am still under 65? Your spouse/domestic partner must enroll in Medicare A and B, and provide a copy of their Medicare card to the District. You and your eligible dependents which include your spouse/domestic partner, and children up to age 26, will remain on the District paid benefits plan until the 1st of the month in which you turn 65.
What happens if I or my spouse/domestic partner does not enroll in Medicare when eligible? If the retiree or spouse/domestic partner does not enroll in Medicare A and/or B when eligible, or fails to provide the District with a copy of their Medicare card, the retiree shall pay any penalty, fee, or other cost imposed by the insurance carrier. If the retiree fails to pay any costs associated with coverage, the coverage will be terminated.
Important Medicare Information: You and your spouse/domestic partner must supply a copy of your/their Medicare part A and B card to the District no later than 15 days prior to the first of the month in which you/they turn 65. Members must NOT enroll in Medicare D.
Eligibility Requirements
Minimum Age 60
Minimum Service Employed full-time with the District for ten (10) consecutive years immediately preceding the date of retirement
Retirement
Concurrent retirement from your applicable retirement system (STRS or PERS) and the District
FREQUENTLY ASKED QUESTIONSFREQUENTLY ASKED QUESTIONSFREQUENTLY ASKED QUESTIONS
(Continued on next page)
4
How much does Medicare cost? Medicare A: Most people receive Part A premium-free because they or their spouse paid Medicare taxes while working. If you do not qualify for premium-free Part A, you could pay up to $441/month (2013 rate). If you pay a late enrollment penalty, this amount is higher. In most cases, if you choose to buy Part A, you must also purchase Part B.
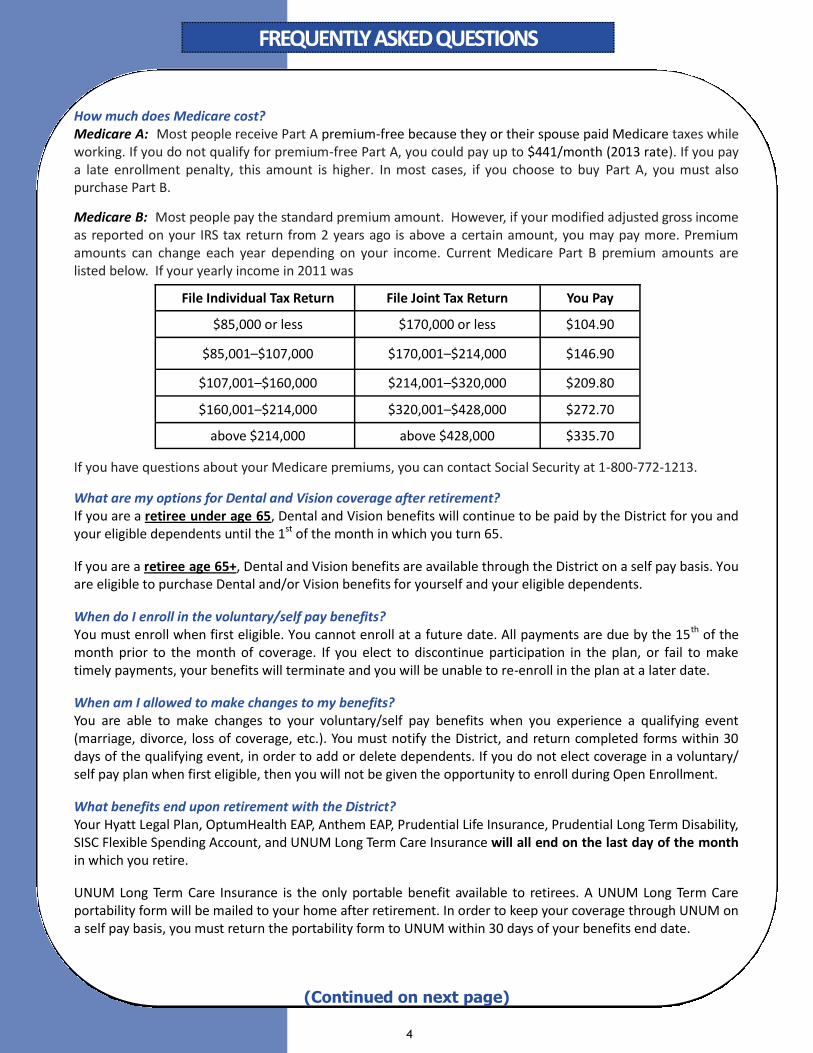
Medicare B: Most people pay the standard premium amount. However, if your modified adjusted gross income as reported on your IRS tax return from 2 years ago is above a certain amount, you may pay more. Premium amounts can change each year depending on your income. Current Medicare Part B premium amounts are listed below. If your yearly income in 2011 was If you have questions about your Medicare premiums, you can contact Social Security at 1-800-772-1213.
What are my options for Dental and Vision coverage after retirement? If you are a retiree under age 65, Dental and Vision benefits will continue to be paid by the District for you and your eligible dependents until the 1st of the month in which you turn 65.
If you are a retiree age 65+, Dental and Vision benefits are available through the District on a self pay basis. You are eligible to purchase Dental and/or Vision benefits for yourself and your eligible dependents.
When do I enroll in the voluntary/self pay benefits? You must enroll when first eligible. You cannot enroll at a future date. All payments are due by the 15th of the month prior to the month of coverage. If you elect to discontinue participation in the plan, or fail to make timely payments, your benefits will terminate and you will be unable to re-enroll in the plan at a later date.
When am I allowed to make changes to my benefits? You are able to make changes to your voluntary/self pay benefits when you experience a qualifying event (marriage, divorce, loss of coverage, etc.). You must notify the District, and return completed forms within 30 days of the qualifying event, in order to add or delete dependents. If you do not elect coverage in a voluntary/self pay plan when first eligible, then you will not be given the opportunity to enroll during Open Enrollment.
What benefits end upon retirement with the District? Your Hyatt Legal Plan, OptumHealth EAP, Anthem EAP, Prudential Life Insurance, Prudential Long Term Disability, SISC Flexible Spending Account, and UNUM Long Term Care Insurance will all end on the last day of the month in which you retire.
UNUM Long Term Care Insurance is the only portable benefit available to retirees. A UNUM Long Term Care portability form will be mailed to your home after retirement. In order to keep your coverage through UNUM on a self pay basis, you must return the portability form to UNUM within 30 days of your benefits end date.
FREQUENTLY ASKED QUESTIONSFREQUENTLY ASKED QUESTIONSFREQUENTLY ASKED QUESTIONS
(Continued on next page)
File Individual Tax Return File Joint Tax Return You Pay
$85,000 or less $170,000 or less $104.90
$85,001–$107,000 $170,001–$214,000 $146.90
$107,001–$160,000 $214,001–$320,000 $209.80
$160,001–$214,000 $320,001–$428,000 $272.70
above $214,000 above $428,000 $335.70
5
What Benefits are available when I become Medicare eligible? The District shall provide retired employees who qualify for continuation of benefits the option to purchase at employee expense supplemental medical coverage, provided the retiree has obtained Medicare A and B coverage. Qualifying members must submit proof that they have obtained Medicare A and B. This benefit is subject to the approval of the District Insurance carrier. The retiree may select from Options A or B subject to the conditions set forth herein.
Option A: The current District supplemental medical plan is available to retirees. The cost for the plan to the retired employee shall be the actual cost paid by the District which is to be paid monthly by the retiree in advance to the District. Payment must be received by the 15th of the month prior to the month of coverage. If payment is not received by the first day of the month of coverage the employee shall be dropped from the coverage and unable to participate in the future. The District reserves the right to establish a separate medical insurance pool for retirees who qualify under this section. Option B: The Companion Care Medicare Supplemental Plan and the Blue Shield 65+ HMO Medicare Advantage Plan will also be offered to retirees as long as the District is covered by the Self-Insured Schools of California (SISC). This program is directly administered by SISC. If a retired member elects one of these plans they cannot return to the District sponsored Supplement plan.
CSEA Retiree 65+ Voluntary Medical Options
What plans are available? District PPO COB Plan Companion Care Supplement Plan (individual plan that is available only to eligible retirees and their
spouses who have Medicare Parts A and B. Enrollment takes a minimum of 45 days.) Blue Shield 65+ HMO Medicare Advantage Plan (individual plan that is available only to eligible retirees
who have Medicare Parts A and B. Enrollment takes a minimum of 45 days.)
What about Medicare? District PPO COB Plan: Members must supply proof of Medicare part A and B to the District prior to the first of the month in which the member turns age 65. Companion Care and Blue Shield 65+ HMO Medicare Advantage Plans: Members must submit proof of part A and B with application at least a minimum of 45 days prior to coverage effective date. Proof of Medicare must be submitted on all enrolled members who are over age 65 (including spouses in the case of Companion Care). If a member is missing part A or B or both, they will only be allowed to enroll in the COB PPO plan and will pay a higher rate. Members must NOT enroll in Medicare D. This is because prescription drug coverage is included in the COB PPO plan, and Medicare Part D enrollment is automatic with Companion Care and Medicare Advantage plans. Please Note: Retiree members with spouses who are under age 65 will remain on the early retiree PPO plan until that spouse becomes Medicare eligible. The retiree member will be charged the early retiree composite rate and must submit proof of Medicare Parts A and B.
FREQUENTLY ASKED QUESTIONSFREQUENTLY ASKED QUESTIONSFREQUENTLY ASKED QUESTIONS
6
1. Does not accrue toward calendar year copayment maximum.
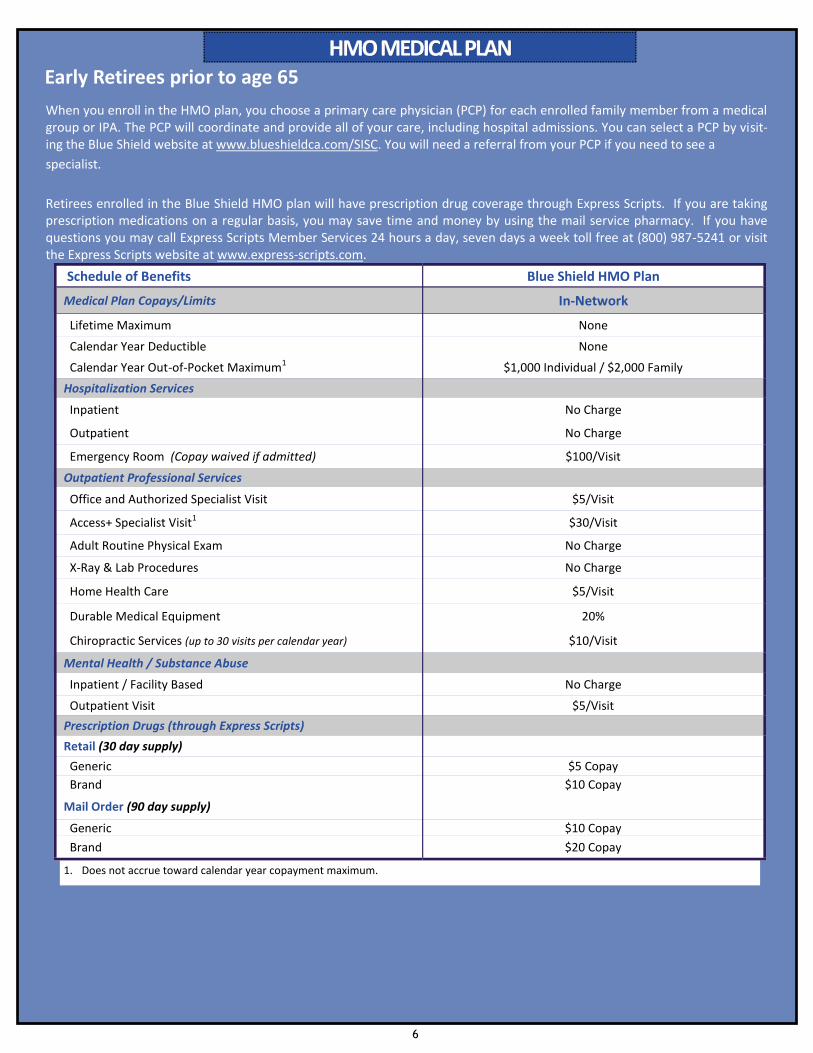
Schedule of Benefits Blue Shield HMO Plan
Medical Plan Copays/Limits In-Network
Lifetime Maximum None
Calendar Year Deductible None
Calendar Year Out-of-Pocket Maximum1 $1,000 Individual / $2,000 Family
Hospitalization Services
Inpatient No Charge
Outpatient No Charge
Emergency Room (Copay waived if admitted) $100/Visit
Outpatient Professional Services
Office and Authorized Specialist Visit $5/Visit
Access+ Specialist Visit1 $30/Visit
Adult Routine Physical Exam No Charge
X-Ray & Lab Procedures No Charge
Home Health Care $5/Visit
Durable Medical Equipment 20%
Chiropractic Services (up to 30 visits per calendar year) $10/Visit
Mental Health / Substance Abuse
Inpatient / Facility Based No Charge
Outpatient Visit $5/Visit
Prescription Drugs (through Express Scripts)
Retail (30 day supply)
Generic $5 Copay
Brand $10 Copay
Mail Order (90 day supply)
Generic $10 Copay
Brand $20 Copay
HMO MEDICAL PLANHMO MEDICAL PLANHMO MEDICAL PLAN
When you enroll in the HMO plan, you choose a primary care physician (PCP) for each enrolled family member from a medical group or IPA. The PCP will coordinate and provide all of your care, including hospital admissions. You can select a PCP by visit-ing the Blue Shield website at www.blueshieldca.com/SISC. You will need a referral from your PCP if you need to see a
specialist.
Retirees enrolled in the Blue Shield HMO plan will have prescription drug coverage through Express Scripts. If you are taking prescription medications on a regular basis, you may save time and money by using the mail service pharmacy. If you have questions you may call Express Scripts Member Services 24 hours a day, seven days a week toll free at (800) 987-5241 or visit the Express Scripts website at www.express-scripts.com.
Early Retirees prior to age 65
7
PPO MEDICAL PLANPPO MEDICAL PLANPPO MEDICAL PLAN Early Retirees prior to age 65
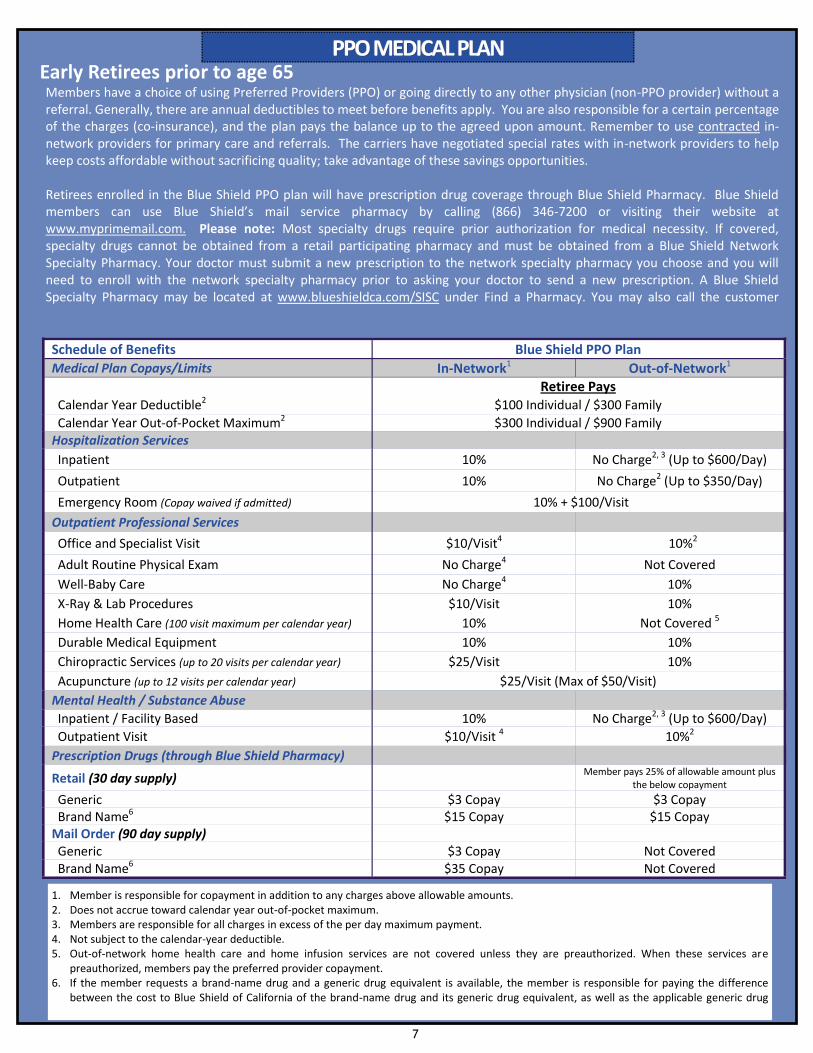
Schedule of Benefits Blue Shield PPO Plan
Medical Plan Copays/Limits In-Network1 Out-of-Network1 Retiree Pays Calendar Year Deductible2 $100 Individual / $300 Family
Calendar Year Out-of-Pocket Maximum2 $300 Individual / $900 Family Hospitalization Services
Inpatient 10% No Charge2, 3 (Up to $600/Day)
Outpatient 10% No Charge2 (Up to $350/Day)
Emergency Room (Copay waived if admitted) 10% + $100/Visit
Outpatient Professional Services
Office and Specialist Visit $10/Visit4 10%2
Adult Routine Physical Exam No Charge4 Not Covered
Well-Baby Care No Charge4 10%
X-Ray & Lab Procedures $10/Visit 10%
Home Health Care (100 visit maximum per calendar year) 10% Not Covered 5
Durable Medical Equipment 10% 10%
Chiropractic Services (up to 20 visits per calendar year) $25/Visit 10%
Acupuncture (up to 12 visits per calendar year) $25/Visit (Max of $50/Visit)
Mental Health / Substance Abuse
Inpatient / Facility Based 10% No Charge2, 3 (Up to $600/Day)
Outpatient Visit $10/Visit 4 10%2
Prescription Drugs (through Blue Shield Pharmacy)
Retail (30 day supply) Member pays 25% of allowable amount plus
the below copayment
Generic $3 Copay $3 Copay Brand Name6 $15 Copay $15 Copay
Mail Order (90 day supply) Generic $3 Copay Not Covered Brand Name6 $35 Copay Not Covered
1. Member is responsible for copayment in addition to any charges above allowable amounts. 2. Does not accrue toward calendar year out-of-pocket maximum. 3. Members are responsible for all charges in excess of the per day maximum payment. 4. Not subject to the calendar-year deductible. 5. Out-of-network home health care and home infusion services are not covered unless they are preauthorized. When these services are
preauthorized, members pay the preferred provider copayment. 6. If the member requests a brand-name drug and a generic drug equivalent is available, the member is responsible for paying the difference
between the cost to Blue Shield of California of the brand-name drug and its generic drug equivalent, as well as the applicable generic drug
Members have a choice of using Preferred Providers (PPO) or going directly to any other physician (non-PPO provider) without a referral. Generally, there are annual deductibles to meet before benefits apply. You are also responsible for a certain percentage of the charges (co-insurance), and the plan pays the balance up to the agreed upon amount. Remember to use contracted in-network providers for primary care and referrals. The carriers have negotiated special rates with in-network providers to help keep costs affordable without sacrificing quality; take advantage of these savings opportunities. Retirees enrolled in the Blue Shield PPO plan will have prescription drug coverage through Blue Shield Pharmacy. Blue Shield members can use Blue Shield’s mail service pharmacy by calling (866) 346-7200 or visiting their website at www.myprimemail.com. Please note: Most specialty drugs require prior authorization for medical necessity. If covered, specialty drugs cannot be obtained from a retail participating pharmacy and must be obtained from a Blue Shield Network Specialty Pharmacy. Your doctor must submit a new prescription to the network specialty pharmacy you choose and you will need to enroll with the network specialty pharmacy prior to asking your doctor to send a new prescription. A Blue Shield Specialty Pharmacy may be located at www.blueshieldca.com/SISC under Find a Pharmacy. You may also call the customer
8
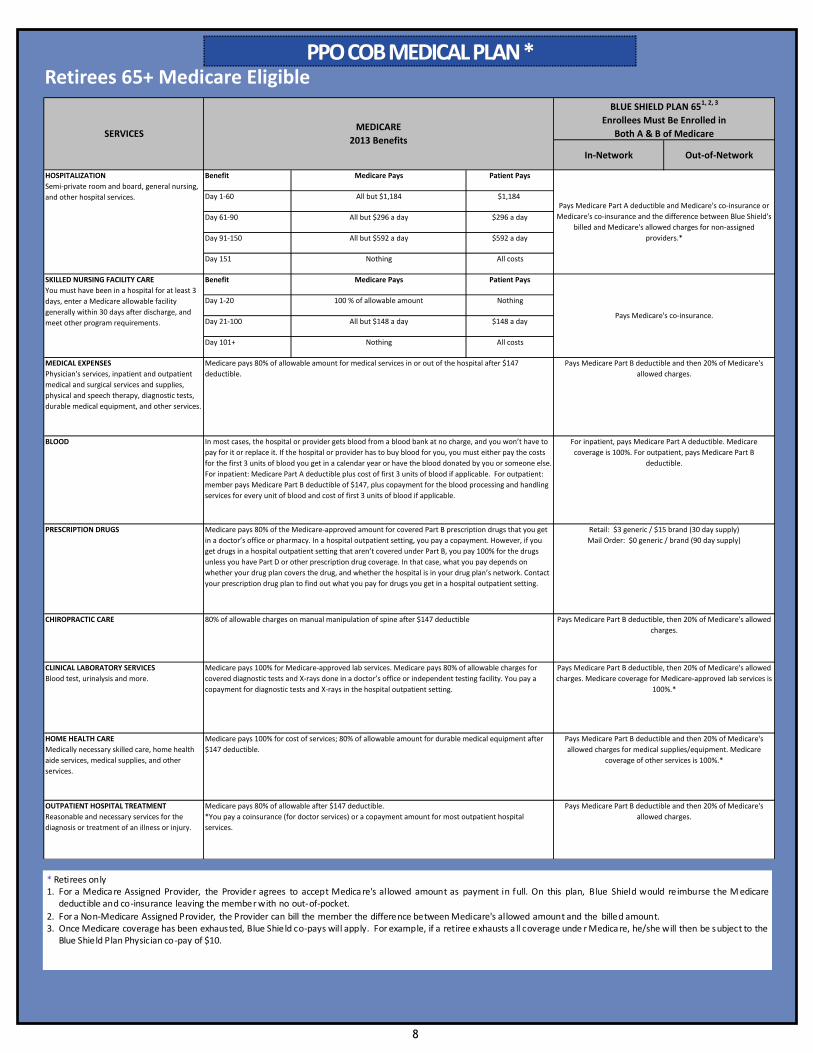
PPO COB MEDICAL PLAN *PPO COB MEDICAL PLAN *PPO COB MEDICAL PLAN * Retirees 65+ Medicare Eligible
In-Network Out-of-Network
Benefit Patient Pays
Day 1-60 $1,184
Day 61-90 $296 a day
Day 91-150 $592 a day
Day 151 All costs
Benefit Patient Pays
Day 1-20 Nothing
Day 21-100 $148 a day
Day 101+ All costs
Medicare PaysSKILLED NURSING FACILITY CARE
You must have been in a hospital for at least 3
days, enter a Medicare allowable facility
generally within 30 days after discharge, and
meet other program requirements.
Pays Medicare Part B deductible and then 20% of Medicare's
allowed charges.
Pays Medicare Part B deductible and then 20% of Medicare's
allowed charges for medical supplies/equipment. Medicare
coverage of other services is 100%.*
Pays Medicare Part B deductible, then 20% of Medicare's allowed
charges. Medicare coverage for Medicare-approved lab services is
100%.*
Pays Medicare Part B deductible, then 20% of Medicare's allowed
charges.
BLUE SHIELD PLAN 651, 2, 3
Enrollees Must Be Enrolled in
Both A & B of MedicareSERVICESMEDICARE
2013 Benefits
HOSPITALIZATION
Semi-private room and board, general nursing,
and other hospital services.
CLINICAL LABORATORY SERVICES
Blood test, urinalysis and more.
Medicare pays 100% for Medicare-approved lab services. Medicare pays 80% of allowable charges for
covered diagnostic tests and X-rays done in a doctor’s office or independent testing facility. You pay a
copayment for diagnostic tests and X-rays in the hospital outpatient setting.
Medicare Pays
MEDICAL EXPENSES
Physician's services, inpatient and outpatient
medical and surgical services and supplies,
physical and speech therapy, diagnostic tests,
durable medical equipment, and other services.
Pays Medicare Part A deductible and Medicare's co-insurance or
Medicare's co-insurance and the difference between Blue Shield's
billed and Medicare's allowed charges for non-assigned
providers.*
For inpatient, pays Medicare Part A deductible. Medicare
coverage is 100%. For outpatient, pays Medicare Part B
deductible.
Pays Medicare Part B deductible and then 20% of Medicare's
allowed charges.
OUTPATIENT HOSPITAL TREATMENT
Reasonable and necessary services for the
diagnosis or treatment of an illness or injury.
PRESCRIPTION DRUGS
BLOOD In most cases, the hospital or provider gets blood from a blood bank at no charge, and you won’t have to
pay for it or replace it. If the hospital or provider has to buy blood for you, you must either pay the costs
for the first 3 units of blood you get in a calendar year or have the blood donated by you or someone else.
For inpatient: Medicare Part A deductible plus cost of first 3 units of blood if applicable. For outpatient:
member pays Medicare Part B deductible of $147, plus copayment for the blood processing and handling
services for every unit of blood and cost of first 3 units of blood if applicable.
Medicare pays 80% of allowable amount for medical services in or out of the hospital after $147
deductible.
Medicare pays 80% of the Medicare-approved amount for covered Part B prescription drugs that you get
in a doctor’s office or pharmacy. In a hospital outpatient setting, you pay a copayment. However, if you
get drugs in a hospital outpatient setting that aren’t covered under Part B, you pay 100% for the drugs
unless you have Part D or other prescription drug coverage. In that case, what you pay depends on
whether your drug plan covers the drug, and whether the hospital is in your drug plan’s network. Contact
your prescription drug plan to find out what you pay for drugs you get in a hospital outpatient setting.
Nothing
All but $1,184
All but $148 a day
All but $296 a day
All but $592 a day
Pays Medicare's co-insurance.
CHIROPRACTIC CARE 80% of allowable charges on manual manipulation of spine after $147 deductible
Nothing
100 % of allowable amount
Medicare pays 80% of allowable after $147 deductible.
*You pay a coinsurance (for doctor services) or a copayment amount for most outpatient hospital
services.
Retail: $3 generic / $15 brand (30 day supply)
Mail Order: $0 generic / brand (90 day supply)
HOME HEALTH CARE
Medically necessary skilled care, home health
aide services, medical supplies, and other
services.
Medicare pays 100% for cost of services; 80% of allowable amount for durable medical equipment after
$147 deductible.
* Retirees only 1. For a Medica re Assigned Provider, the Provider agrees to accept Medica re's allowed amount as payment in full. On this plan, Blue Shield would reimburse the M edicare
deductible and co-insurance leaving the member with no out-of-pocket.
2. For a Non-Medicare Assigned Provider, the Provider can bill the member the difference between Medicare's allowed amount and the billed amount. 3. Once Medicare coverage has been exhausted, Blue Shield co-pays will apply. For example, if a retiree exhausts a ll coverage unde r Medica re, he/she will then be subject to the
Blue Shield Plan Physician co-pay of $10.
9
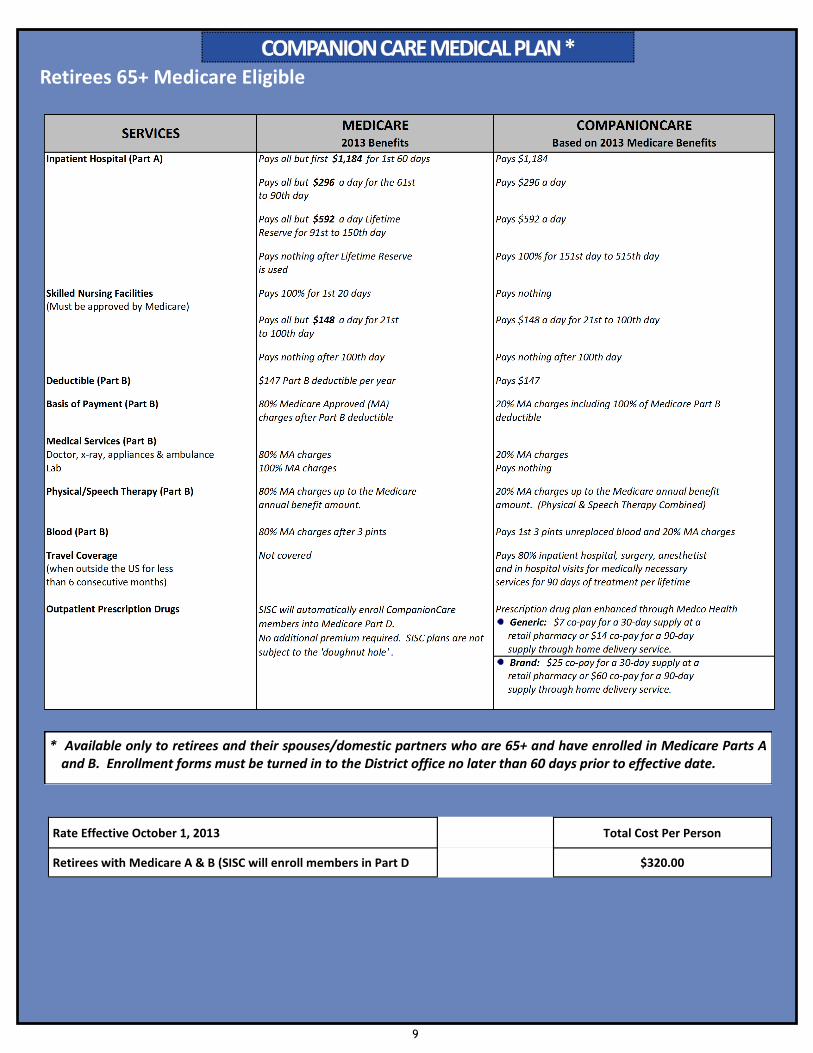
COMPANION CARE MEDICAL PLAN *COMPANION CARE MEDICAL PLAN *COMPANION CARE MEDICAL PLAN * Retirees 65+ Medicare Eligible
* Available only to retirees and their spouses/domestic partners who are 65+ and have enrolled in Medicare Parts A and B. Enrollment forms must be turned in to the District office no later than 60 days prior to effective date.
Rate Effective October 1, 2013 Total Cost Per Person
Retirees with Medicare A & B (SISC will enroll members in Part D $320.00
10
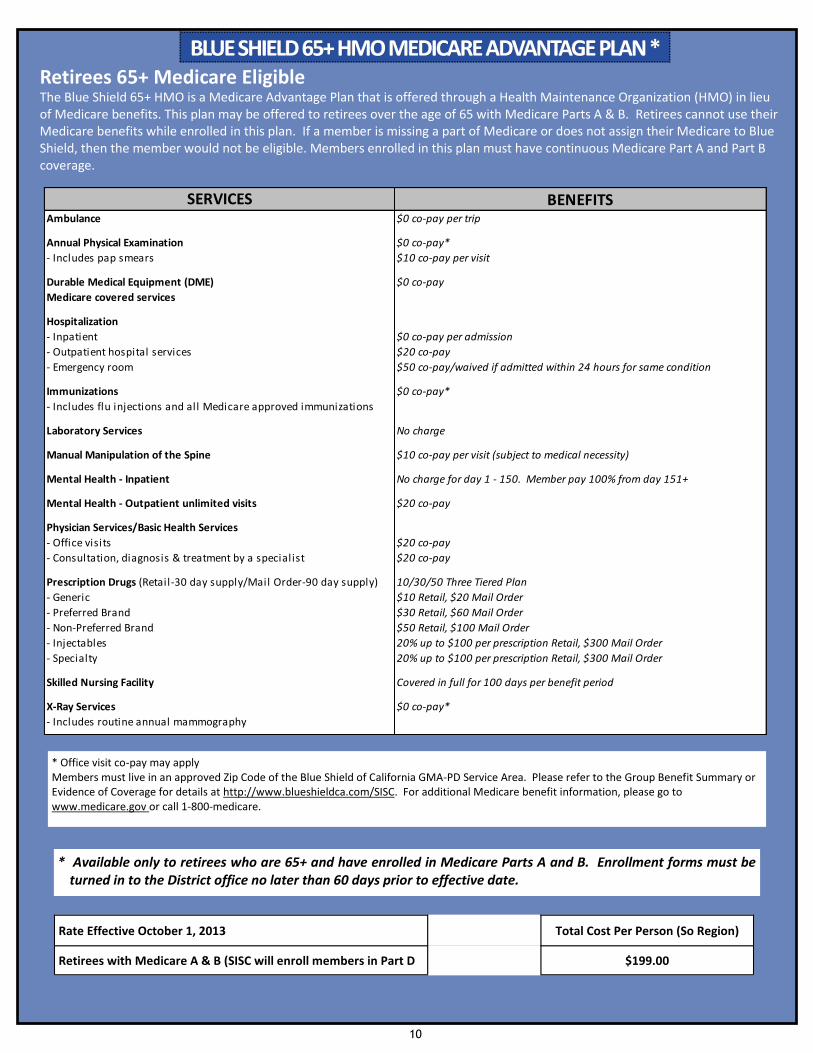
BLUE SHIELD 65+ HMO MEDICARE ADVANTAGE PLAN *BLUE SHIELD 65+ HMO MEDICARE ADVANTAGE PLAN *BLUE SHIELD 65+ HMO MEDICARE ADVANTAGE PLAN * Retirees 65+ Medicare Eligible
* Available only to retirees who are 65+ and have enrolled in Medicare Parts A and B. Enrollment forms must be turned in to the District office no later than 60 days prior to effective date.
Rate Effective October 1, 2013 Total Cost Per Person (So Region)
Retirees with Medicare A & B (SISC will enroll members in Part D $199.00
* Office visit co-pay may apply Members must live in an approved Zip Code of the Blue Shield of California GMA-PD Service Area. Please refer to the Group Benefit Summary or Evidence of Coverage for details at http://www.blueshieldca.com/SISC. For additional Medicare benefit information, please go to www.medicare.gov or call 1-800-medicare.
The Blue Shield 65+ HMO is a Medicare Advantage Plan that is offered through a Health Maintenance Organization (HMO) in lieu of Medicare benefits. This plan may be offered to retirees over the age of 65 with Medicare Parts A & B. Retirees cannot use their Medicare benefits while enrolled in this plan. If a member is missing a part of Medicare or does not assign their Medicare to Blue Shield, then the member would not be eligible. Members enrolled in this plan must have continuous Medicare Part A and Part B coverage.
10/30/50 Three Tiered Plan
$10 Retail, $20 Mail Order
$30 Retail, $60 Mail Order
$50 Retail, $100 Mail Order
20% up to $100 per prescription Retail, $300 Mail Order
20% up to $100 per prescription Retail, $300 Mail Order
Mental Health - Inpatient No charge for day 1 - 150. Member pay 100% from day 151+
Skilled Nursing Facility Covered in full for 100 days per benefit period
X-Ray Services
- Consultation, diagnosis & treatment by a specialist
Prescription Drugs (Retail-30 day supply/Mail Order-90 day supply)
$10 co-pay per visit (subject to medical necessity)
$20 co-pay
$20 co-pay
$20 co-pay
No charge
SERVICES
Medicare covered services
- Inpatient
Annual Physical Examination
- Includes pap smears
BENEFITS
Immunizations
- Specialty
- Generic
- Injectables
Physician Services/Basic Health Services
Manual Manipulation of the Spine
Mental Health - Outpatient unlimited visits
Laboratory Services
- Office visits
- Includes flu injections and all Medicare approved immunizations
$0 co-pay*
$20 co-pay
$50 co-pay/waived if admitted within 24 hours for same condition
$0 co-pay*
- Non-Preferred Brand
- Preferred Brand
- Outpatient hospital services
- Emergency room
- Includes routine annual mammography
$0 co-pay per trip
$0 co-pay per admission
$10 co-pay per visit
Hospitalization
Durable Medical Equipment (DME) $0 co-pay
$0 co-pay*
Ambulance
11
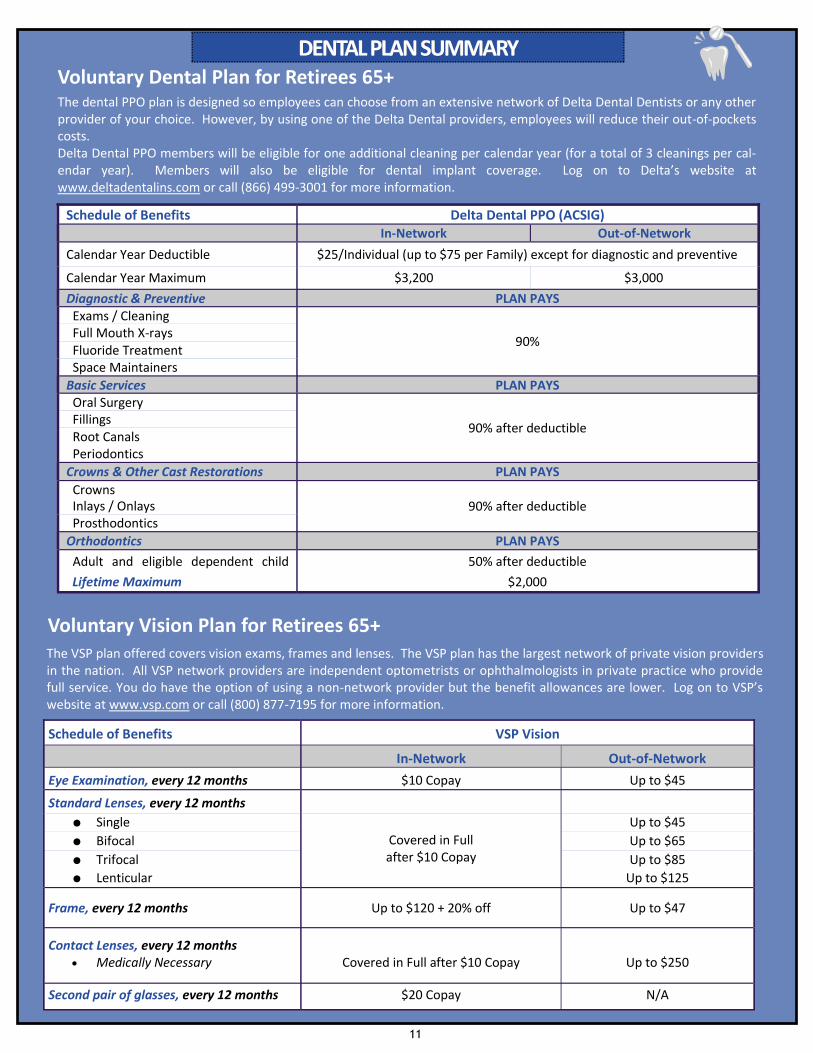
DENTAL PLAN SUMMARYDENTAL PLAN SUMMARYDENTAL PLAN SUMMARY
The dental PPO plan is designed so employees can choose from an extensive network of Delta Dental Dentists or any other provider of your choice. However, by using one of the Delta Dental providers, employees will reduce their out-of-pockets costs. Delta Dental PPO members will be eligible for one additional cleaning per calendar year (for a total of 3 cleanings per cal-endar year). Members will also be eligible for dental implant coverage. Log on to Delta’s website at www.deltadentalins.com or call (866) 499-3001 for more information.
Voluntary Dental Plan for Retirees 65+
The VSP plan offered covers vision exams, frames and lenses. The VSP plan has the largest network of private vision providers in the nation. All VSP network providers are independent optometrists or ophthalmologists in private practice who provide full service. You do have the option of using a non-network provider but the benefit allowances are lower. Log on to VSP’s website at www.vsp.com or call (800) 877-7195 for more information.
Voluntary Vision Plan for Retirees 65+
Schedule of Benefits VSP Vision
In-Network Out-of-Network
Eye Examination, every 12 months $10 Copay Up to $45
Standard Lenses, every 12 months
● Single
Covered in Full after $10 Copay
Up to $45
● Bifocal Up to $65
● Trifocal Up to $85
● Lenticular Up to $125
Frame, every 12 months Up to $120 + 20% off Up to $47
Contact Lenses, every 12 months
Medically Necessary
Covered in Full after $10 Copay
Up to $250
Second pair of glasses, every 12 months $20 Copay N/A
Schedule of Benefits Delta Dental PPO (ACSIG) In-Network Out-of-Network
Calendar Year Deductible $25/Individual (up to $75 per Family) except for diagnostic and preventive
Calendar Year Maximum $3,200 $3,000
Diagnostic & Preventive PLAN PAYS Exams / Cleaning
90% Full Mouth X-rays Fluoride Treatment Space Maintainers
Basic Services PLAN PAYS Oral Surgery
90% after deductible Fillings Root Canals Periodontics
Crowns & Other Cast Restorations PLAN PAYS
Crowns 90% after deductible Inlays / Onlays
Prosthodontics
Orthodontics PLAN PAYS
Adult and eligible dependent child 50% after deductible
Lifetime Maximum $2,000
12
Other than during annual open enrollment, you may only make changes to your benefit elections if you experience a qualified status change or qualify for a “special enrollment”. If you qualify for a mid-year benefit change, you may be required to submit proof of the change or evidence of prior coverage. Qualified Status Changes include:
Change in legal marital status, including marriage, divorce, legal separation, annulment, and death of a
spouse.
Change in number of dependents, including birth, adoption, placement for adoption, or death of a dependent
child.
Change in employment status that affects benefit eligibility, including the start or termination of
employment by you, your spouse, or your dependent child.
Change in work schedule, including an increase or decrease in hours of employment by you, your spouse, or
your dependent child, including a switch between part-time and full-time employment that affects eligibility
for benefits.
Change in a child's dependent status, either newly satisfying the requirements for dependent child status or
ceasing to satisfy them.
Change in place of residence or worksite, including a change that affects the accessibility of network
providers.
Change in your health coverage or your spouse's coverage attributable to your spouse's employment.
Change in an individual's eligibility for Medicare or Medicaid.
A court order resulting from a divorce, legal separation, annulment, or change in legal custody (including a
Qualified Medical Child Support Order) requiring coverage for your child.
An event that is a “special enrollment” under the Health Insurance Portability and Accountability Act
(HIPAA) including acquisition of a new dependent by marriage, birth or adoption, or loss of coverage under
another health insurance plan.
An event that is allowed under the Children's Health Insurance Program (CHIP) Reauthorization Act. Under
provisions of the Act, employees have 60 days after the following events to request enrollment if:
Employee or dependent loses eligibility for Medicaid (known as Medi-Cal in CA) or CHIP (known as Healthy Families in CA).
Employee or dependent becomes eligible to participate in a premium assistance program under Medicaid or CHIP.
Two rules apply to making changes to your benefits during the year:
Any change you make must be consistent with the change in status, AND
You must make the change within 30 days of the date the event occurs (unless otherwise noted above).
RULES FOR BENEFIT CHANGES DURING THE YEARRULES FOR BENEFIT CHANGES DURING THE YEARRULES FOR BENEFIT CHANGES DURING THE YEAR
13
REQUIRED FEDERAL NOTICESREQUIRED FEDERAL NOTICESREQUIRED FEDERAL NOTICES
HEALTH INSURANCE PORTABILITY AND ACCOUNTABILITY ACT (HIPAA)
Your medical benefit plan may impose a preexisting condition exclusion upon enrollees age 19 and older. That means that if you are age 19 or older and have a medical condition before coming to our Plan, you might have to wait a certain period of time before the Plan will provide coverage for that condition. This exclusion applies only to conditions for which medical advice, diagnosis, care, or treatment was recommended or received within the 6 month period. Generally, this 6 month period ends the day before your coverage becomes effective. However, if you were in a waiting period for coverage, the 6 month period ends on the day before the waiting period begins. The preexisting condition exclusion does not apply to pregnancy. This exclusion may last up to 12 months from your first day of coverage or, if you were in a waiting period, from the first day of your waiting period. However, you can reduce the length of this exclusion period by the number of days of your prior “creditable coverage.” Most prior health coverage is creditable coverage and can be used to reduce the preexisting condition exclusion if you have not experienced a break in coverage of at least 63 days. To reduce the exclusion period by your creditable coverage, you should provide the new carrier with a copy of any certificates of creditable coverage (HIPAA Certificates) you have. If you do not have a Certificate, but you do have prior health coverage, you can obtain one from your prior plan or issuer.
THE WOMEN’S HEALTH AND CANCER RIGHTS ACT
The Women’s Health and Cancer Rights Act (WHCRA) requires employer groups to notify participants and beneficiaries of the group health plan, of their rights to mastectomy benefits under the plan. Participants and beneficiaries have rights to coverage to be provided in a manner determined in consultation with the attending Physician for: All stages of reconstruction of the breast on which the mastectomy was performed; Surgery and reconstruction of the other breast to produce a symmetrical appearance; Prostheses; and Treatment of physical complications of the mastectomy, including lymphedema. These benefits are subject to the same deductible and co-payments applicable to other medical and surgical benefits provided under this plan. You can contact your health plan’s Member Services for more information.
Notice of Availability of HIPAA Privacy Notice The Federal Health Insurance Portability and Accountability Act of 1996 (“HIPAA”) requires that we periodically remind you of your right to receive a copy of the HIPAA Privacy Notice. You can request a copy of the Privacy Notice by contacting District Benefits.
14
REQUIRED FEDERAL NOTICESREQUIRED FEDERAL NOTICESREQUIRED FEDERAL NOTICES
Premium Assistance Under Medicaid and the Children’s Health Insurance Program (CHIP)
If you or your children are eligible for Medicaid or CHIP and you are eligible for health coverage from your employer, your State may have a premium assistance program that can help pay for coverage. These States use funds from their Medicaid or CHIP programs to help people who are eligible for these programs, but also have access to health insurance through their employer. If you or your children are not eligible for Medicaid or CHIP, you will not be eligible for these premium assistance programs.
If you or your dependents are already enrolled in Medicaid or CHIP and you live in a State listed below, you can contact your State Medicaid or CHIP office to find out if premium assistance is available.
If you or your dependents are NOT currently enrolled in Medicaid or CHIP, and you think you or any of your dependents might be eligible for either of these programs, you can contact your State Medicaid or CHIP office or dial 1-877-KIDS NOW or www.insurekidsnow.gov to find out how to apply. If you qualify, you can ask the State if it has a program that might help you pay the premiums for an employer-sponsored plan.
Once it is determined that you or your dependents are eligible for premium assistance under Medicaid or CHIP, as well as eligible under your employer plan, your employer must permit you to enroll in your employer plan if you are not already enrolled. This is called a “special enrollment” opportunity, and you must request coverage within 60 days of being determined eligible for premium assistance. If you have questions about enrolling in your employer plan, you can contact the Department of Labor electronically at www.askebsa.dol.gov or by calling toll-free 1-866-444-EBSA
(3272). This information is current as of January 31, 2013. For more information, you can contact either: U.S. Department of Labor U.S. Department of Health and Human Services Employee Benefits Security Administration Centers for Medicare & Medicaid Services www.dol.gov/ebsa www.cms.hhs.gov 1-866-444-EBSA (3272) 1-877-267-2323, Ext. 61565
15
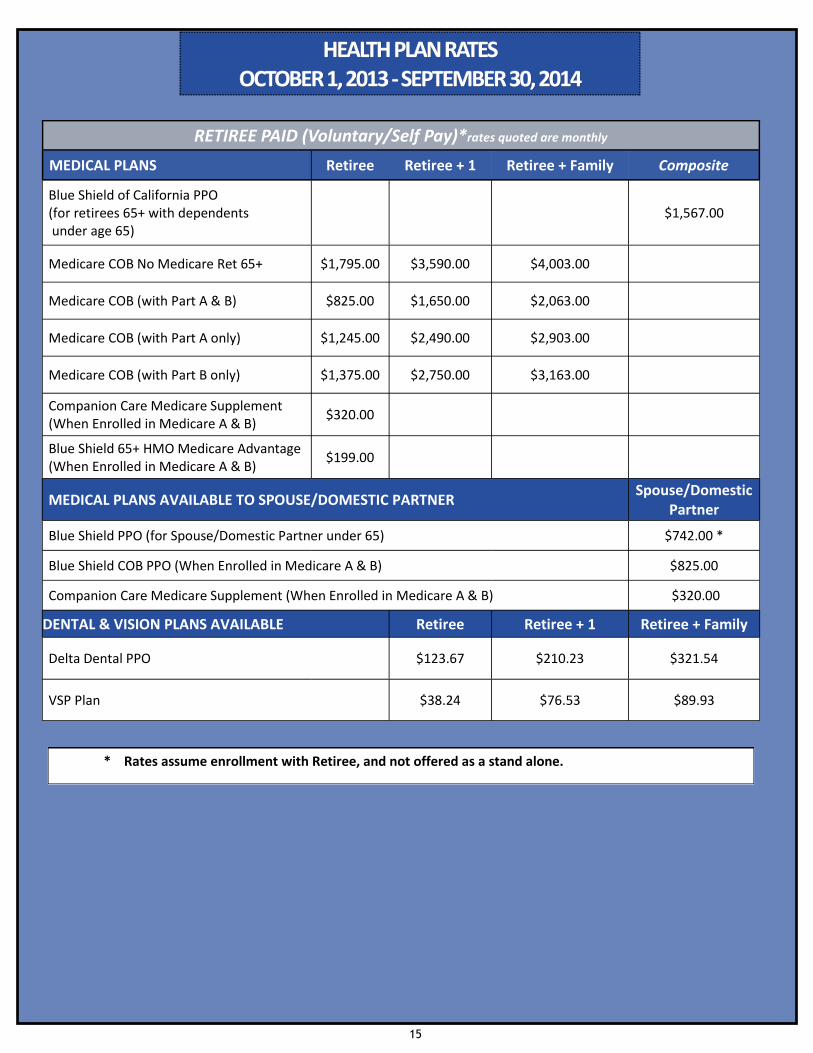
HEALTH PLAN RATESHEALTH PLAN RATESHEALTH PLAN RATES OCTOBER 1, 2013 OCTOBER 1, 2013 OCTOBER 1, 2013 --- SEPTEMBER 30, 2014 SEPTEMBER 30, 2014 SEPTEMBER 30, 2014
RETIREE PAID (Voluntary/Self Pay)*rates quoted are monthly
MEDICAL PLANS Retiree Retiree + 1 Retiree + Family Composite
Blue Shield of California PPO (for retirees 65+ with dependents under age 65)
$1,567.00
Medicare COB No Medicare Ret 65+ $1,795.00 $3,590.00 $4,003.00
Medicare COB (with Part A & B) $825.00 $1,650.00 $2,063.00
Medicare COB (with Part A only) $1,245.00 $2,490.00 $2,903.00
Medicare COB (with Part B only) $1,375.00 $2,750.00 $3,163.00
Companion Care Medicare Supplement (When Enrolled in Medicare A & B)
$320.00
Blue Shield 65+ HMO Medicare Advantage (When Enrolled in Medicare A & B)
$199.00
MEDICAL PLANS AVAILABLE TO SPOUSE/DOMESTIC PARTNER Spouse/Domestic
Partner
Blue Shield PPO (for Spouse/Domestic Partner under 65) $742.00 *
Blue Shield COB PPO (When Enrolled in Medicare A & B) $825.00
Companion Care Medicare Supplement (When Enrolled in Medicare A & B) $320.00
DENTAL & VISION PLANS AVAILABLE Retiree Retiree + 1 Retiree + Family
Delta Dental PPO $123.67 $210.23 $321.54
VSP Plan $38.24 $76.53 $89.93
* Rates assume enrollment with Retiree, and not offered as a stand alone.
16
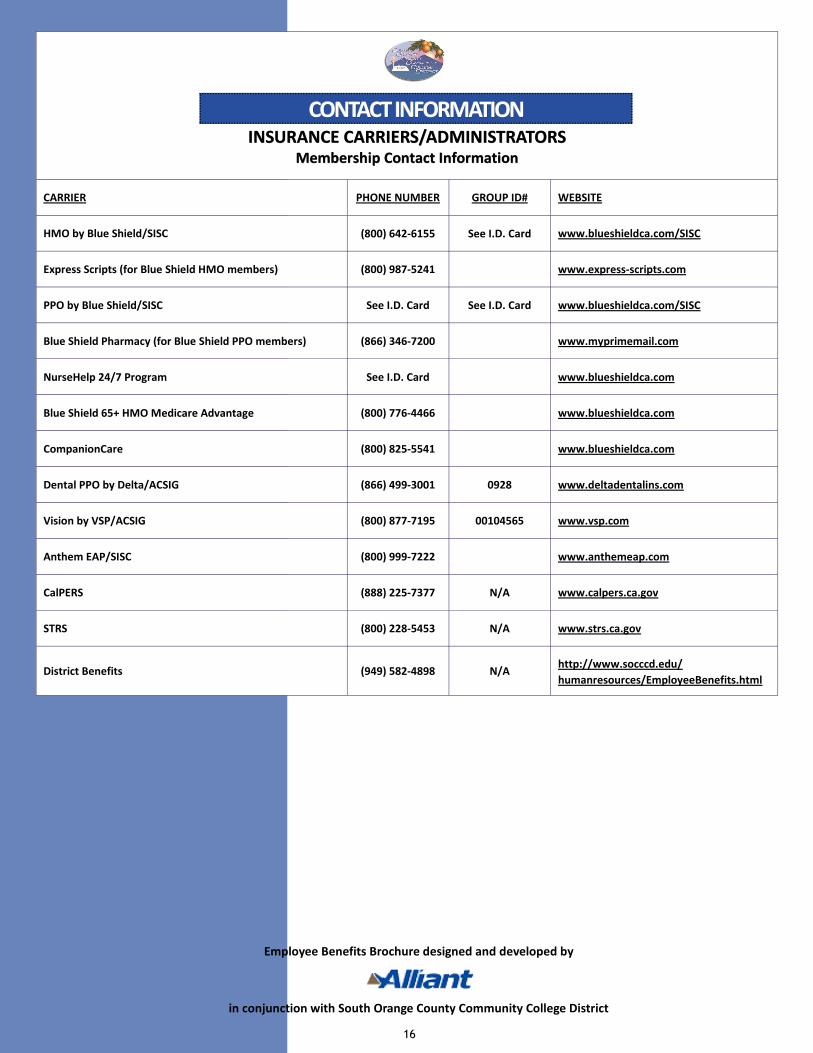
INSURANCE CARRIERS/ADMINISTRATORSINSURANCE CARRIERS/ADMINISTRATORSINSURANCE CARRIERS/ADMINISTRATORS
Membership Contact InformationMembership Contact InformationMembership Contact Information
CARRIER PHONE NUMBER GROUP ID# WEBSITE
HMO by Blue Shield/SISC (800) 642-6155 See I.D. Card www.blueshieldca.com/SISC
Express Scripts (for Blue Shield HMO members) (800) 987-5241 www.express-scripts.com
PPO by Blue Shield/SISC See I.D. Card See I.D. Card www.blueshieldca.com/SISC
Blue Shield Pharmacy (for Blue Shield PPO members) (866) 346-7200 www.myprimemail.com
NurseHelp 24/7 Program See I.D. Card www.blueshieldca.com
Blue Shield 65+ HMO Medicare Advantage (800) 776-4466 www.blueshieldca.com
CompanionCare (800) 825-5541 www.blueshieldca.com
Dental PPO by Delta/ACSIG (866) 499-3001 0928 www.deltadentalins.com
Vision by VSP/ACSIG (800) 877-7195 00104565 www.vsp.com
Anthem EAP/SISC (800) 999-7222 www.anthemeap.com
CalPERS (888) 225-7377 N/A www.calpers.ca.gov
STRS (800) 228-5453 N/A www.strs.ca.gov
District Benefits (949) 582-4898 N/A http://www.socccd.edu/
humanresources/EmployeeBenefits.html
CONTACT INFORMATIONCONTACT INFORMATIONCONTACT INFORMATION
Employee Benefits Brochure designed and developed by
in conjunction with South Orange County Community College District