2013 health care for the homeless network community needs
TRANSCRIPT

2013
Health Care for the Homeless Network
Community Needs Assessment

(This page intentionally left blank)

Public Health – Seattle and King County 2013 Community Needs Assessment
Table of Contents
Acknowledgements ....................................................................................................... 4
Executive Summary ...................................................................................................... 5
Project Motivation ......................................................................................................... 6
Chronic Disease Focus ................................................................................................. 7
2013 HCHN Community Needs Assessment Design .................................................. 8
Target Population ......................................................................................................... 8
Sampling Method ......................................................................................................... 9
Service Site Selection .................................................................................................. 9
Survey Construction ................................................................................................... 11
2013 Preliminary Data Discussion ............................................................................. 15
Conclusions and Next Steps ...................................................................................... 23
Appendices .................................................................................................................. 25
Appendix A: HCHN 2013 CNA Instrument ................................................................. 25
Appendix B: American Diabetes Association Risk Self-Assessment Tool.................. 29
Appendix C: American Heart Association Risk Self-Assessment Tool ....................... 30

Acknowledgments
Health Care for the Homeless Network of Seattle & King County would like to acknowledge the
following individuals and groups for their support of the 2013 Community Needs Assessment:
HCHN Administrative Specialist: John Newcombe
HCHN Data Entry Specialist: Tamara Drain
Seattle & King County Public Health Reserve Corps Program Volunteers
Seattle & King County Public Health Reserve Corps Program Manager: Dave Nichols
Clinical advisors: Maureen Brown, MD; Charissa Fotinos, MD
HCHN 2013 administrative team: Heather Barr, Laurie Becker, Lorri Cox, Tamara Drain,
Karen Eckert, Trudi Fajans, Natalie Lente, John Newcombe, Jason Ortiz, Sarah Sausner,
Winnie Shu, Marcia Stone
Service site partners:
Catholic Community Services – Lazarus Day Center
Chief Seattle Club
Compass Housing Alliance – Adult Service Center
DESC – Connections and Main Shelter
Immanuel Lutheran Hygiene & Day Center
King County Public Health’s Mobile Medical Van Program and Site Partners
Matt Talbot Center
Recovery Café
Union Gospel Mission
YWCA – Angeline’s Bellevue & Seattle
Funders:
City of Seattle Human Services Department
King County Mental Illness and Drug Dependency Sales Tax
King County Veterans and Human Services Levy
United Way of King County
U.S. Department of Health & Human Services, HRSA
Bureau of Primary Health Care
U.S. Department of Housing and Urban Development
5
Executive Summary The 2013 Community Needs Assessment (CNA) is an integral part of the Health Care for the
Homeless Network (HCHN) strategic planning process and orients the program’s goals and
vision for the next Health Resources Services Administration (HRSA) project period. The
information contained in this report will be useful to providers, policy-makers, researchers and
others interested in the chronic disease risk and prevalence of homeless adults, specifically
users of homeless day services in Seattle and King County. The HCHN administrative team
intends to use these data to inform their service delivery model and focus for the next five years
of programming.
Key findings include:
Eighteen percent of HCHN community needs assessment respondents have diabetes.
Sixty percent of HCHN community needs assessment respondents had a diabetes risk that is considered “high risk” by the American Diabetes Association.
Of the roughly 800 respondents who do not have diabetes, 56 percent (449 individuals)
have a risk score of four or higher.
Forty-four percent of respondents have high blood pressure.
Over 80 percent of respondents have three or more risk factors for heart disease.
Sixty percent of respondents are overweight.
Sixty-nine percent of respondents smoke tobacco.
Thirty-seven percent of respondents are uninsured.
Data Source:
One thousand interviews were conducted using a survey instrument developed by the HCHN
CNA design team. The instrument adapted the American Heart Association and the American
Diabetes Association risk self-assessment tools for use with this unique population.
Respondents were selected for the sample based on convenience sampling and received a five
dollar gift card to compensate them for their time in completing the interview. Public Health
Reserve Corps volunteers and Public Health administrative staff conducted one-on-one
interviews on multiple visit days at 15 homeless day service sites throughout Seattle and King
County between May and August, 2013.
Data limitations:
The large sample size provides worthwhile information on a significant number of individuals
within this population; however, it was gathered using convenience, rather than random
sampling thus direct estimates from sample to population are not possible.
For further information please contact:
Sarah M. Sausner
Public Health – Seattle & King County, Health Care for the Homeless Network
401 5th Avenue, 9th Floor
Seattle, WA 98104

6
Project Motivation The stories of Chris, Sandy, and Bennett are composite sketches of homeless or formerly
homeless clients seen by Health Care for the Homeless Network (HCHN) providers.
Chris is a 40 year old Alaska Native man, six feet tall, and weighs one-hundred and
eighty pounds. He does day labor through the Millionair Club, and is a member of the
Chief Seattle Club where he eats breakfast most weekdays. He reports having candy
bars and soda for lunch when he works, and he eats dinner at the mission where he
sleeps. Chris smokes two packs of cigarettes per day and the last few times the nurse at
the day center checked his blood pressure it was very high. His mother had diabetes
and Chris last saw a doctor five years ago when he broke his foot and describes himself
as being “in pretty good shape, except for the smoking”.
Sandy is a 45 year old White woman who has been living in south King County for the
past ten years. She became homeless two years ago and has been sleeping in her car
ever since. She is twenty pounds overweight, has a history of gestational diabetes, and
when she last saw her doctor (before she was homeless), she learned that she was
“borderline diabetic”. She visits the church-based meal programs in south King County
most weeknights for dinner. Last night they served hotdogs and French fries, and a
piece of cake for dessert. Sandy was told to modify her diet and increase her activity to
avoid becoming diabetic-- but she finds it difficult given her current circumstances.
Bennett is a 63 year old African American man who was homeless for twenty years. He
now lives in supportive housing for formerly homeless people and spends most
afternoons at the Lazarus Day Center in Pioneer Square. He is depressed and diabetic,
has painful neuropathy in his feet, and blindness is starting to make it difficult to get
around. He had his great toe amputated a little over a year ago. With help from the case
managers on-site at his building, he sees a doctor every six months, but he is frustrated
and doesn’t see much use in continuing to go when he can’t seem to take the
medications the way he’s supposed to anyway.
Individuals like Chris, Sandy and Bennett motivated the HCHN administrative team to focus on
chronic disease in its 2013 Community Needs Assessment (CNA). Providers in the Health Care
for the Homeless Network (HCHN) see clients who not only struggle with homelessness, mental
illness, and substance abuse—but also untreated diabetes, cardiovascular disease, and other
chronic conditions that have major impacts on their quality of life. Too often, those homeless
individuals who eventually find housing and have their mental health and substance abuse
treatment needs met, too often face serious consequences of chronic diseases that have gone
unmanaged for years. Though many of the determinants of individuals’ health require larger
systems change, HCHN recognizes an opportunity to more directly focus on these important
chronic health issues affecting homeless patients in the upcoming project period.

7
Chronic Disease Focus: Heart Disease and Diabetes
Heart disease has persisted as the number one cause of death in the United States since the
1920s. Diabetes is ranked seventh as a cause of death and is a contributing risk factor in
developing heart disease. As a homeless person, managing these two chronic diseases in
particular is challenging. The conditions of homelessness often preclude the behavior
modifications and medical interventions that are effective in reducing the most severe
consequences of the disease. In addition to personal costs, people who have diabetes and
heart disease are costly to the health care system overall. People with diagnosed diabetes have
medical expenditures more than two times higher than what expenditures would be in the
absence of diabetes, and over 60 percent of that cost is shouldered by government insurance
programs (Medicare, Medicaid, and the Veterans Administration). Those with diabetes and
without health insurance have 55 percent more emergency department visits than people who
have insurance (American Diabetes Association, 2013). In proportion to the difficulty of
management, the cost-savings potential of interventions is high if access to appropriate care
and support can be ensured for this population.
Figure 1 is a conceptual map of the path of unmanaged chronic disease as imagined by the
HCHN community needs assessment design team.
Figure 1: Path of Unmanaged Chronic Disease
Without community and individual health interventions, homeless individuals who get started on
this path may proceed through each stage with declining quality of life and costly and
unpleasant medical complications leading to an early death. Research conducted over the past
forty years has demonstrated that a history of homelessness is strongly associated with chronic
illness and an early death rate that is three to four times that of the general population
(Connelly, 2011).The average age of death of homeless persons is between forty-two and fifty
years, and the causes of death are mostly related to chronic medical conditions rather than
overdose, suicide, or homicide as some might expect (O'Connell, 2005). The first step toward
convening a solution that will divert homeless individuals from this path is focusing on chronic
disease risk and prevalence in the adult homeless population in Seattle and King County.
HCHN obtained estimates of the number of adult homeless day center users who are at risk,
diagnosed, and struggling with disease management (those who would be located within the
first three phases of the continuum above). Interventions available to reduce risks of diabetes
and cardiovascular disease such as improved access to healthy food, promotion of physical
activity, campaigns to reduce tobacco use and increased access to stress management support

8
are well within the scope of influence of a Public Health department and the community partners
that carry out the HCHN mission. In the coming project period, HCHN will more intentionally
address these same intervention and prevention strategies in the work it funds within Seattle
and King County.
HCHN Program
Health Care for the Homeless Network (HCHN), a program of Public Health – Seattle & King
County, provides health care and ensures access to adapted health care to more than 20,000
people annually. HCHN’s philosophy of care focuses on strengths-based assessment,
motivational interviewing, harm reduction, and trauma informed care to support homeless clients
in improving their health and well-being. Over 100 providers deliver primary care, nursing
services, case management, mental health care, substance abuse services, referral services,
and assistance for people enrolling in Medicaid and other entitlement programs throughout the
Health Care for the Homeless Network in Seattle and King County. HCHN providers serve
homeless patients in over 40 community settings and 10 public health centers, as well as on the
streets, in parks, homeless encampments, under bridges, and wherever homeless people may
be found. The HCHN sub-contracted service delivery model creates integrated teams of
providers that deliver service to homeless clients ‘where they are at’ rather than requiring clients
to access services within established clinic sites. HCHN is governed by King County Board of
Health and an 18 member community-based Planning Council that advises the program’s
services and budget and ensures that the program is aligned with its mission.
2013 HCHN Community Needs Assessment Design
Target Population
The HCHN administrative team narrowed the focus of its 2013 community needs assessment to
‘adults who use homeless day services in Seattle and King County’. Compared to any other
service type, meal programs and hygiene services (often located within homeless day centers)
are used by individuals who are least engaged in homeless services elsewhere in the
continuum (City of Seattle Office of Housing, 2009).
Homeless service agencies that receive federal or local funding are required to collect data on
the individuals they serve. Day centers, however, remain low-barrier by collecting very little data
as a prerequisite for services, thus comparatively less is known about the population utilizing
day services than other services within the continuum of care.
Safe Harbors, Seattle & King County’s Homeless Management Information System (HMIS) is
generally considered the most comprehensive count of homeless persons in Seattle and King
County. This database may undercount homeless individuals and families who are doubled up
(unstably housed with another family member or friend), those who sleep outside or in other
places not meant for human habitation, and those who stay in shelters simply because the
requirement to enter data into Safe Harbors is attached to certain funding streams, and
individuals in the situations above may not enter into programs attached to those funding
streams. In 2012, Safe Harbors reported data for 18,758 unique individuals served over the
course of the year in emergency shelter, transitional housing, and permanent supportive
housing; however as of late 2012, day centers were not yet entering clients into the HMIS

9
system. Therefore, HCHN was unable to obtain an estimate of the population of adult users of
day centers in Seattle and King County from which a sample size target could be generated.
Sampling Method
HCHN used targeted convenience sampling on multiple visit days at 15 homeless day service
sites between May 1 and August 31, 2013 to achieve its sampling goal. Public Health Reserve
Corps volunteers and HCHN administrative staff conducted 1,000 interviews with homeless day
center clients. To put the HCHN sample size into perspective: to represent the homeless
population currently entered into the Safe Harbors HMIS (over 18,000 individuals) a researcher
would need to randomly select 645 individuals for her sample to achieve representativeness
with 99 percent confidence level and a margin of error of three.
HCHN gathered information on average number of clients seen per day from eight homeless
day centers determined to be included in the CNA. A sample size calculator was used to derive
target sample size based on average clients per day at those eight sites and initial assumptions
regarding how much data could be gathered within the data collection time frame. After multiple
visits to the two largest day center locations selected as sampling sites and one or two visits to
smaller sites, it became clear that the ‘churn’ phenomenon of individuals who travel to multiple
day centers within a single day would affect the ability to meet sample size goals at the eight
initially selected sites. HCHN found that after reaching sample size goals at the two largest
sites, it became more difficult— on visits to smaller service sites—to find individuals who had
not already been interviewed. While the magnitude of the churn phenomenon was
unanticipated, the HCHN administrative team used the opportunity to meet its sample size goals
by expanding the list of sampling sites from eight to 15. The expansion of service sites to be
included in the community needs assessment likely improved dramatically the
representativeness of the sample selected.
Service Site Selection
The HCHN administrative team gathered a comprehensive list of homeless day centers
beginning with the 2-1-1 community resource list and augmenting with programs known to be
missing from that listing in order to select the sites to be included in the 2013 community needs
assessment. Agencies that deny services on the basis of color, race, sexual orientation, gender,
religious belief, national origin, or ancestry, as well as organizations whose services are not
available to non-members or that require participation in religious activities or profession of faith
to receive services must be excluded from the 2-1-1 listings. HCHN selected several day
centers that were not listed in the 2-1-1 directory including: Chief Seattle Club, where services
are only available to Native Americans whose membership in a tribe can be demonstrated, two
recovery-based day center programs where some measure of abstinence from drugs/alcohol is
required, and two day programs that exclusively serve women.
Table 1 is a summary of the service sites included in the HCHN 2013 community needs
assessment, their estimated service numbers per day (where available), and the number of
interviews HCHN conducted at each site.

10
Table 1: Service sites included in HCHN 2013 CNA sample
Homeless Day Services
Population Served
Estimated clients/day
Clients interviewed 2013
Angeline's Seattle women 18+ 200 68
Angeline's Bellevue women 18+ 25 10
CCS-Lazarus Center men & women 50+ 225 125
Chief Seattle Club tribal-enrolled 100 85
Compass-ASC adults 300 185
DESC - Main Shelter highly vulnerable
adults 300 161
DESC - Connections
adults whose
homelessness is
primarily related to
economic conditions
150-200 53
Immanuel Lutheran adults 35 12
Matt Talbot Center adults in recovery 25 22
Meal Site - Auburn adults * 51
Meal Site - Burien adults * 26
Meal Site - Kent adults * 30
Meal Site - Renton adults * 33
Recovery Café adults in recovery 150 71
Union Gospel Mission men and women 80 68
Total − − 1000
*Daily use data for this site not available.
Day centers excluded from 2013 HCHN sample
The HCHN administrative team sought to capture the diversity that exists among adult users of
homeless day service centers and addressed as many sources of potential bias as possible by
extending inclusion criteria to sites beyond those listed in 2-1-1. Elizabeth Gregory Home,
Seattle Indian Center, and Bread of Life Mission, appear in the 2-1-1 listings and met the criteria
for inclusion but were excluded from analysis due to constraints on staff time. HCHN ensured
oversampling at other sites believed to draw a similar subset of the homeless day service users
as those who use excluded sites mentioned above: women, Native American/Alaska Natives,
and individuals drawn to religiously-based services respectively. HCHN also excluded two day
centers that have hygiene services but lack the programming that is common among other sites
selected: Urban Rest Stop and Compass Housing Alliance-Waterfront location. Finally, Mary’s
Place is a homeless day center serving single women and families, and excluding this site from
the needs assessment presents bias by excluding adult women who are the primary caregivers
for their children.
HCHN’s methodological approach may have biased the sample in the following ways:
Respondents received a $5 gift card as compensation for their time. This approach may
have drawn individuals into the sample who are most motivated by small economic

11
reimbursements.
Individuals who do not speak or understand English or Spanish are likely
underrepresented in this sample due to limited translation services for data collection.
Respondents with the most severe mental health barriers, brain injury, or cognitive
impairments may have been under-sampled despite outreach attempts because
volunteers were instructed to restrict their outreach to one attempt per person per site
visit.
Survey construction
HCHN identified five areas of interest for the HCHN 2013 community needs assessment data
collection: demographic information; risk and prevalence of selected chronic diseases; chronic
disease management experience; and health care access. In order to efficiently and respectfully
collect data in the five areas of interest, the planning team established two guiding principles in
survey design: (1) the instrument would only include data elements relevant to the area of
interest and (2) each element would be filtered through a trauma-informed lens.
The instrument was constructed to flow conversationally in an interview format with the intention
that interviewers would create a comfortable dialogue with respondents. Questions were read
aloud to respondents and answers were recorded on the instrument by the interviewer.
Respondents were informed that they could refuse to answer any question and that they could
stop the interview at any time.
HCHN attached a unique identifier to each completed survey comprised of the first two letters of
the first and last name of the respondent, as well as their date of birth. This identifier was used
to help identify duplicates during the data analysis phase. The complete survey instrument
along with interviewer instructions may be found in Appendix A.
Demographic information: HCHN limited its demographic data collection to date of birth,
gender, race, ethnicity, and current sleeping location. Gender and race questions were open-
ended to gather rich qualitative data on identity construction within this population. Sleeping
location was asked using open-ended construction as well, and interviewers were trained to
encourage respondents to list all of the sleeping locations they had used recently. Figure 2
provides excerpts from the needs assessment instrument related to demographic information.
Figure 2: Demographic questions, HCHN 2013 CNA instrument
22. Where are you staying now? ______________________________________________________
25. What gender do you identify yourself as? _____________________
26. Which category best describes your race? ____________________
27. Are you of Hispanic, Latino or Spanish origin? NO ☐ YES ☐

12
Risk & Prevalence: HCHN adapted the widely used self-report risk assessment tools from the
American Diabetes Association and the American Heart Association for use in the 2013
community needs assessment. The original tools can be found in Appendices B and C.
Complex sentences were broken into component parts for ease of communication. Questions
numbered 4., 5., 6., 8., 9., 10. in Figure 3, for example, are questions that are part of longer
constructions in the original risk assessment tools.
Questions from the American Diabetes & Heart Associations risk assessment tools related to
gestational diabetes and physical activity were not used due to perceived challenges in
collecting high quality data on these measures given the resources available.
The risk assessment questions regarding prevalence of chronic disease were used without
amendment in the HCHN community needs assessment. Prevalence-related questions are
found in questions numbered 7., 11., 12., also shown in Figure 3.
Figure 3: Risk & Prevalence questions, HCHN 2013 CNA instrument
Chronic Disease Management: Those respondents who indicated that they had been told by a
doctor that they have diabetes, high blood pressure, or high cholesterol, were asked an
additional set of questions related to their management of those conditions. HCHN sought to
capture what respondents understood about disease management and how often it was being
addressed by the provider they last saw. Respondents were also asked if they had been
prescribed medication for their illness (diabetes, high blood pressure, high cholesterol), and if
so, they were asked for more information about medication compliance and management.
All respondents were asked about the things they do each day to manage their stress and about
physical activities they would enjoy participating in if they were offered in the day center location
they visited. Figure 4 includes all questions related to chronic disease management from the
needs assessment instrument.
4. Did your mother have diabetes? DK ☐ NO ☐ YES ☐
5. Did your father have diabetes? DK ☐ NO ☐ YES ☐
6. Did your sister or brother have diabetes? DK ☐ NO ☐ YES ☐
7. Have you ever been told you have diabetes? Borderline ☐ DK ☐ NO ☐ YES ☐
8. Did your mother have: high blood pressure, (heart attack, heart disease, or stroke)? DK ☐ NO ☐ YES ☐
9. Did your father have: high blood pressure, (heart attack, heart disease, or stroke)? DK ☐ NO ☐ YES ☐
10. Did your sibling have: high blood pressure, (heart attack, heart disease, or stroke)? DK ☐ NO ☐ YES ☐
11. Have you ever been told you have high blood pressure? (Or ever had a heart attack or stroke)?
Borderline ☐ DK ☐ NO ☐ YES ☐
12. Have you ever been told your cholesterol is a problem? DK ☐ NO ☐ YES ☐
13. Do you smoke tobacco? NO ☐ YES ☐
14. Do you know how tall you are? __________
15. Do you know your weight? _____________

13
Figure 4: Chronic disease management questions, HCHN 2013 CNA instrument
18. The last time you saw your health care provider, did s/he talk about the things you can do to manage your illness?
(high blood pressure, high cholesterol, diabetes)
a. (if yes)
i. What things did s/he talk about?
b. (if no)
i. Do you know the kinds of things you can do to manage?
19. Has anyone ever told you, you should be taking medication for your illness (diabetes, high blood pressure, high
cholesterol)? NO ☐ YES ☐
a. (If yes)
i. Did you take those medicines today? Some ☐ NO ☐ YES ☐
1. (if Yes) For some people taking medication is kind of hard, how ‘s it going for you?
2. (If No) What has been hard about getting or taking you medications?
23. Is there something you do every day that helps you keep in balance/manage your stress?
24. If you had 3 options for exercise or fun activities you’d be interested in doing – (any kind of movement, activity,
class, equipment, practices…) What would they be?
a. _________________________ b. ___________________________ c.___________________________
Health Care Access: Respondents were asked whether they had a place where they receive
regular medical care, the name of that clinic/provider, the approximate date of last visit, and the
number of visits they had in the past year. Respondents were also queried regarding whether
they obtained medical care anywhere else in the preceding year, and whether they had medical
insurance coverage of any kind. Figure 5 provides excerpts of health care access questions
from the needs assessment instrument.

14
Figure 5: Health care access questions, HCHN 2013 CNA instrument
16. Do you have a place you rely on for regular medical care? NO ☐ YES ☐
a. (If Yes)
i. Where do you go? (clinic/hospital name) ______________________________________________
Ii. When is the last time you went for a visit? (month/year) __________________________________
III. About how often did you go last year (times/year)? _____________________________________
Iv. Did you get medical care anywhere else last year (clinic/hospital name/ER)? _________________
(if No)
i. what places have you gone in the past when you’re sick? ________________________________
17. Do you have health insurance or coverage of any kind? NO ☐ YES ☐
a. (if Yes)
i. what plan? ________________________________________
Preventive Health Screenings: Respondent 50 years or older were asked if they have had a
colonoscopy (men and women), and mammogram (women only). Those questions are seen in
Figure 6.
Figure 6: Preventive health screening questions, HCHN 2013 CNA instrument
AGE
(If client is 50 years old or older, born before 1963, please complete this section)
20. Have you ever been screen for colon cancer? NO ☐ YES ☐
(Prompt: colonoscopy, or checked for blood in stool)
Women Only:
21. Have you ever had a mammogram? NO ☐ YES ☐

15
2013 Preliminary data discussion
HCHN interviewed 1,000 individuals, entered data into EpiData, and then exported to SPSS for
analysis. Cases were discarded from analysis if they were identified as a duplicate or if fewer
than 50 percent of fields contained data. The resulting data set includes 987 valid cases.
Age: Seventy-eight percent of respondents are 40 years of age or older. Chart 1 reflects the
age distribution of HCHN’s 2013 community needs assessment sample.
Chart 1: Age Distribution, HCHN 2013 CNA respondents
Gender: Twenty-nine percent of respondents identified as female, 69 percent identified as male
and two percent identified as transgender, gender-queer, or refused to answer the question. As
mentioned previously, the gender identity question was open-ended and the richness of those
qualitative data was reduced to three categories for the purposes of this preliminary analysis.
Race: The 2013 community needs assessment instrument included an open-ended question
“Which category best describes your race?” which allowed clients to describe their racial identity
in their own words. Data were then coded into the following major race categories: American
Indian / Alaska Native, Asian, Asian Pacific Islander / Native Hawaiian, Black/African American,
and White as seen in Chart 2.
0
50
100
150
200
250
300
350
400
0-17 18 - 29 30 - 39 40 - 49 50 - 59 60 - 69 70 - 79 80 - 89
Age Categories

16
Chart 2: Race, HCHN 2013 CNA respondents
Ten percent of respondents identified with two or more races; the multi-racial identities of those
respondents are found in Table 2.
BLACK 29%
AMERICAN INDIAN / ALASKA
NATIVE 10%
WHITE 39%
ASIAN 2%
ASIAN PACIFIC ISLANDER /
NATIVE HAWAIIAN
1%
TWO OR MORE RACES
11%
UNKNOWN / DECLINED
8%

17
Table 2: Multi-race identification, HCHN 2013 CNA respondents
Two race categories identified Respondents
American Indian / Alaska Native - White 41
American Indian / Alaska Native - Black 17
American Indian / Alaska Native - Asian 5
Asian-White 4
Asian - Asian Pacific Islander / Native Hawaiian 2
Asian Pacific Islander / Native Hawaiian - White 1
Asian Pacific Islander / Native Hawaiian - American Indian / Alaska
Native 1
Black - White 5
"Mixed Race" (Categories unknown, default to two categories) 2
Three race categories identified Respondents
American Indian / Alaska Native - Asian - White 3
Asian - Black - White 2
Asian Pacific Islander / Native Hawaiian- American Indian / Alaska
Native -White 1
Black - American Indian / Alaska Native -White 8
Black - Asian Pacific Islander / Native Hawaiian - White 1
Total number identifying with two or more race categories 93
Thirteen percent of respondents reported Hispanic, Latino, or Spanish origin.
Living Situation: Interviewers were instructed to gather as much detail as possible about
respondents’ living situation histories and to ask follow-up questions to elicit the mix of shelter
types known to be used by many homeless individuals. The majority of respondents, 53
percent, listed an emergency shelter first in their living situation history response. Sixteen
percent of respondents reported that they were housed at the time of interview. Anecdotally, we
know that even after a homeless person finds housing, day centers continue to meet their need
for community, food, services and linkages to care. Fourteen percent of respondents reported
sleeping outdoors and 11 percent reported that they were in a “doubled-up” situation (an
unstable living arrangement with a family member or friend). An additional 10 percent of
respondents reported sleeping outdoors (including cars) as part of their mix of sleeping
locations, but listed their outdoor location either second or third in their list of sleeping locations.
Table 3 reflects the first living situation reported by HCHN 2013 community needs assessment
respondents (secondary and tertiary living situations not reported here).

18
Table 3: First reported living situation, HCHN 2013 CNA respondents
Sleeping Place Category Frequency Percent
Car 29 2.9
Doubled Up 104 10.5
Not Homeless 158 16
Outdoors 139 14.1
Shelter 523 53
Transitional Housing 21 2.1
Unknown 13 1.3
Total 987 100
Diabetes Risk: The diabetes risk self-assessment tool includes seven measures: age, gender,
gestational diabetes diagnosis/history, family history of diabetes, hypertension diagnosis,
physical activity, and weight status. Age and weight status risk are assigned values from zero
through three, with all other measures valued at zero or one, and the total possible risk points
equaling eleven. HCHN omitted gestational diabetes risk and physical activity from the risk
assessment for this survey, making a score of nine the maximum risk score for sample
respondents.
A risk score of four on the American Diabetes Association risk assessment tool indicates high
risk for having type two diabetes (Bang, et al., 2009). Sixty percent of HCHN community needs
assessment respondents had a risk score of four or higher. Considering the HCHN truncated
scoring due to the omission of two risk questions the actual percentage of the population at risk
is likely even higher than 60%.
Chart 3: Diabetes risk distribution in HCHN 2013 CNA sample
0
50
100
150
200
250
.00 1.00 2.00 3.00 4.00 5.00 6.00 7.00 8.00 9.00
Diabetes Risk Score

19
To better understand the overlap between respondents who have high risk scores and those
who reported being told by their doctor that they have diabetes, it is helpful to look at a cross
tabulation of these two variables. In Table 4, total diabetes risk scores are displayed in rows and
respondent diabetes diagnosis (Yes/No) is displayed in columns. Of the roughly 800
respondents who report they have not been told they have diabetes, 56 percent (449
individuals) have a risk score of four or higher. Considering the barriers to care that homeless
individuals experience and the high risk scores of people who report that they have not been
told they have diabetes, we expect the actual prevalence of diabetes within the population to be
higher than the 18% found in the sample.
Table 4: Total diabetes risk and respondent diabetes diagnosis, cross tabulation
Diabetes Diagnosis
Diabetes Risk Score No Yes Total
.00 17 1 18
1.00 59 5 64
2.00 121 10 131
3.00 161 24 185
4.00 164 29 193
5.00 145 40 185
6.00 97 27 124
7.00 32 29 61
8.00 7 10 17
9.00 4 5 9
Total 807 180 987
Heart Disease Risk: The American Heart Association risk assessment tool includes the
following nine measures: age, family history of heart disease or diabetes, race/ethnicity,
diabetes diagnosis, tobacco use, hypertension, hyperlipidemia, obesity, and inactivity. Each risk
measure is valued at zero or one and the total possible risk score is nine. HCHN omitted
‘inactivity’ from its risk assessment due to perceived difficulty in collecting high-quality data for
this measure, thus the HCHN community needs assessment maximum risk score for heart
disease is eight.
In the American Heart Association risk assessment, presence of one risk factor indicates a risk
for heart disease that is two times the risk of a person who has no risk factors. However, due to
the multiplier effect, presence of three risk factors indicates that an individual’s risk for heart
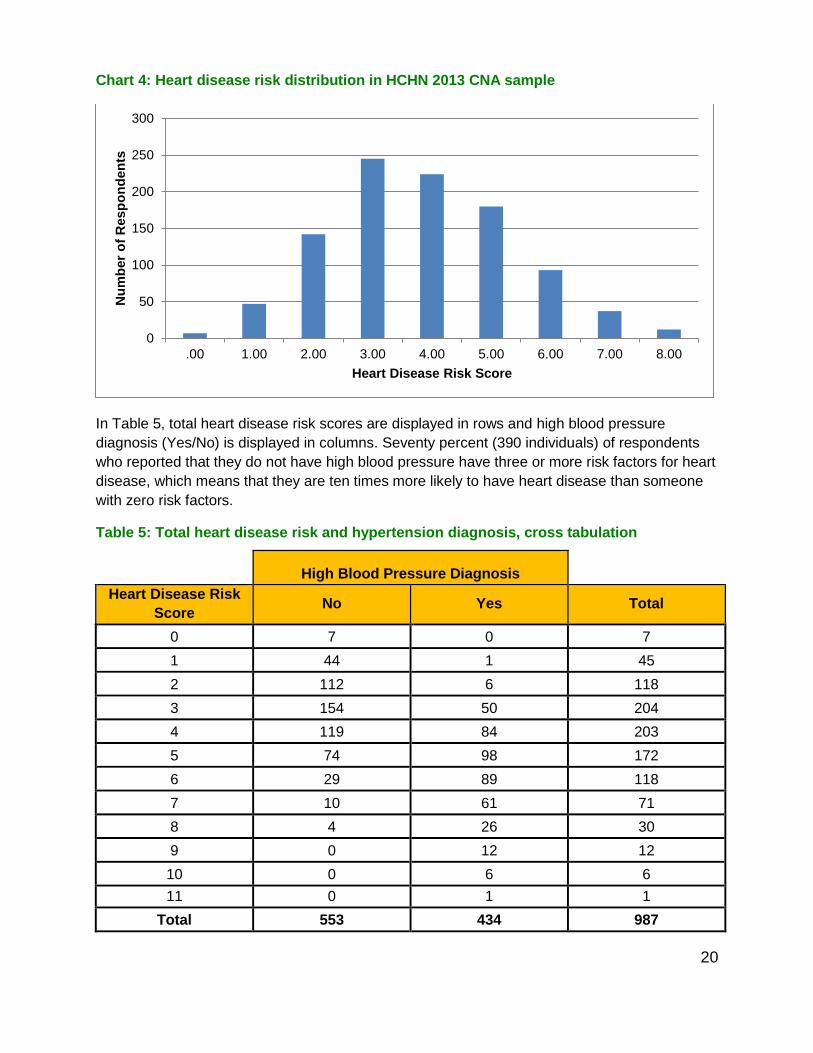
disease is ten times higher than a person who has no risk factors for the disease. Chart 4
displays the heart disease risk factor distribution in the HCHN 2013 community needs
assessment sample. Over 80 percent of respondents have three or more risk factors for heart
disease.
20
Chart 4: Heart disease risk distribution in HCHN 2013 CNA sample
In Table 5, total heart disease risk scores are displayed in rows and high blood pressure
diagnosis (Yes/No) is displayed in columns. Seventy percent (390 individuals) of respondents
who reported that they do not have high blood pressure have three or more risk factors for heart
disease, which means that they are ten times more likely to have heart disease than someone
with zero risk factors.
Table 5: Total heart disease risk and hypertension diagnosis, cross tabulation
High Blood Pressure Diagnosis
Heart Disease Risk
Score No Yes Total
0 7 0 7
1 44 1 45
2 112 6 118
3 154 50 204
4 119 84 203
5 74 98 172
6 29 89 118
7 10 61 71
8 4 26 30
9 0 12 12
10 0 6 6
11 0 1 1
Total 553 434 987
0
50
100
150
200
250
300
.00 1.00 2.00 3.00 4.00 5.00 6.00 7.00 8.00
Nu
mb
er
of
Resp
on
den
ts
Heart Disease Risk Score
21
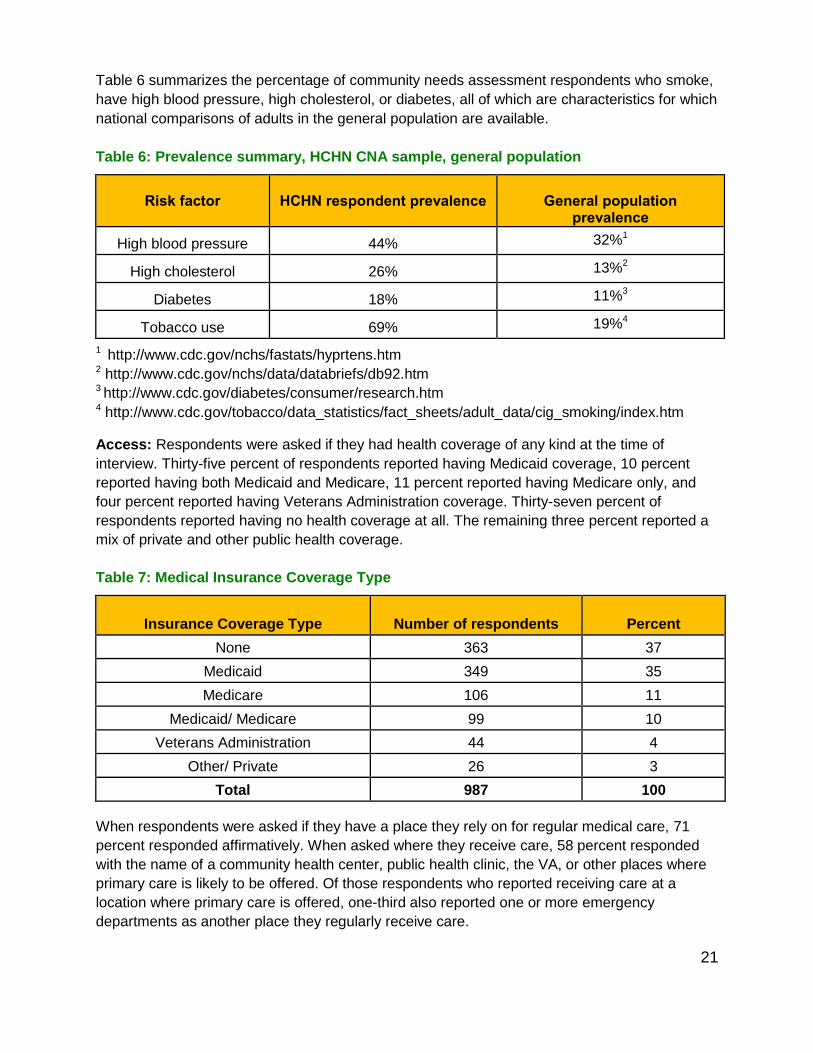
Table 6 summarizes the percentage of community needs assessment respondents who smoke,
have high blood pressure, high cholesterol, or diabetes, all of which are characteristics for which
national comparisons of adults in the general population are available.
Table 6: Prevalence summary, HCHN CNA sample, general population
Risk factor
HCHN respondent prevalence
General population
prevalence
High blood pressure 44% 32%1
High cholesterol 26% 13%2
Diabetes 18% 11%3
Tobacco use 69% 19%4
1 http://www.cdc.gov/nchs/fastats/hyprtens.htm 2 http://www.cdc.gov/nchs/data/databriefs/db92.htm 3 http://www.cdc.gov/diabetes/consumer/research.htm 4 http://www.cdc.gov/tobacco/data_statistics/fact_sheets/adult_data/cig_smoking/index.htm
Access: Respondents were asked if they had health coverage of any kind at the time of
interview. Thirty-five percent of respondents reported having Medicaid coverage, 10 percent
reported having both Medicaid and Medicare, 11 percent reported having Medicare only, and
four percent reported having Veterans Administration coverage. Thirty-seven percent of
respondents reported having no health coverage at all. The remaining three percent reported a
mix of private and other public health coverage.
Table 7: Medical Insurance Coverage Type
Insurance Coverage Type
Number of respondents Percent
None 363 37
Medicaid 349 35
Medicare 106 11
Medicaid/ Medicare 99 10
Veterans Administration 44 4
Other/ Private 26 3
Total 987 100
When respondents were asked if they have a place they rely on for regular medical care, 71
percent responded affirmatively. When asked where they receive care, 58 percent responded
with the name of a community health center, public health clinic, the VA, or other places where
primary care is likely to be offered. Of those respondents who reported receiving care at a
location where primary care is offered, one-third also reported one or more emergency
departments as another place they regularly receive care.

22
Twenty-four percent of respondents did not have a place where they receive medical care,
fourteen percent listed an emergency department as their primary source of medical care, and
four percent listed a shelter, meal site, or other place that likely does not offer primary care as
the place they receive care. Table 8 summarizes the places respondents reported receiving
care.
Table 8: Place respondent receives medical care
Where do you go for medical care? Number of respondents Valid Percent
Place where primary care is likely offered 573 58
Emergency department 138 14
Other 42 4
No place reported 234 24
Total 987 100
Risk, Prevalence, and Access: Of the 234 individuals (24 percent of respondents) who
reported that they had not received medical care at all in the past year, 170 (71%) have a heart
disease risk score of three or higher, which is 10 times the risk of a person who has no risk
factors; 42 percent have a diabetes risk score of four or higher which puts them at high risk for
undiagnosed diabetes.
Cancer screenings: High quality self-report data of both the timing and type of colon cancer
screenings was deemed unlikely given the resources available for this needs assessment and
the population of interest. The 2013 CNA required interviewers to ask respondents age 50 and
older if they had ever had a screening for colon cancer by colonoscopy or fecal occult blood
test. Forty-four percent of male respondents and 56 percent of female respondents in this age
category had received colon cancer screening at the time of interview. The Center for Disease
Control reports that the National Health Interview Survey, 2010, found the overall screening
rates for the U.S. population overall is around 59 percent (Centers for Disease Control and
Prevention, 2012), however, the national data collect much more detailed information regarding
timing and type of screening, thus direct comparison must be done with caution.
In 2010, 73 percent of women in the U.S. ages 50 to 74 had had a mammogram within the past
two years (Centers for Disease Control and Prevention, 2012). Of the 142 female respondents
age 50 or older, 77 percent reported ever having had at least one mammogram. HCHN
community needs assessment respondents were not asked about the date of their last
mammogram so direct comparison with national breast cancer screening rates are not
appropriate. However, HCHN finds it noteworthy that the breast and colon cancer screening
rates are as high as they are given the barriers to health care access within this population.

23
Conclusions and next steps Health care providers, planners, and policymakers know that promoting health in the homeless
population presents a formidable challenge at the individual and population level. The stress of
poverty, co-occurring conditions such as mental illness and chemical dependency, and trauma,
compounded with homelessness, speeds the onset and exacerbates the symptoms of many
chronic diseases. Locally, there is still minimal understanding of the population-level health
status of homeless individuals, and even less is known about users of homeless day center
services as a sub-group that may be the least engaged in health services. The results of the
preliminary analysis of the HCHN 2013 community needs assessment indicate that of the 987
individuals for whom complete data could be analyzed, almost 700 smoke tobacco, over 600
are not maintaining a healthy weight, more than 400 have high blood pressure, and almost 200
are diagnosed diabetics. These results indicate a clear demand for intervention and prevention.
Tobacco use, weight, diet and exercise are risk factors that can be addressed by collaborations
between Public Health, homeless service providers, and funders whose respective interests
could align to benefit homeless individuals already on the path of unmanaged chronic disease.
Further analysis of these data must be done to examine the chronic disease management
issues of those who have been diagnosed with high blood pressure, high cholesterol, or
diabetes, and to learn more about the kind of support homeless people may need. Additionally,
analysis of the stress management practices and activity interests of respondents could provide
planners and service providers with ideas for interventions that would be welcomed by this
population.
As health systems in Washington state begin to shift in 2014 with the implementation of the
Affordable Care Act and expansion of Medicaid, Public Health - Seattle & King County’s Health
Care for the Homeless Network (HCHN) hopes this needs assessment will both inform
community stakeholders within the homeless services industry of the shockingly high risk and
prevalence of chronic disease currently afflicting the adult homeless day center population and
motivate action toward better integration of health promotion in all facets of homeless service
delivery.

24
(This page intentionally left blank)

Appendix A: HCHN 2013 Community Needs Assessment Instrument
25
Health Care for the Homeless Community Needs Assessment 2013 Hi. My name is ____________________ and I’m a volunteer with the Health Department. We want to know more about chronic health conditions that people here might have. If you are interested in talking with me for a little while about your health, family history of heart disease and diabetes, and a little bit about your access to medical care, we are able to offer you a $5 gift card to Bartell’s to thank you for your time. This should take about 20 minutes or so. Would you like to start now?
YES NO, Stop Interview

26
We will record just the first two letters of your first name, and the first two letters of your last name—and your Date of Birth.
First Last Birth Month Birth Day Birth Year
1. What is your first name? (Enter first two letters in boxes above) a. What do you like to be called?
2. What are the first 2 letters of your last name? (Enter first two letters in boxes above)
3. What is your date of birth? (Enter MM/DD/YY in boxes above) (Born before 1963?) NO YES Complete AGE section
Next I’ll ask about your history and your family history with diabetes and heart disease. If you don’t know an answer it’s okay to say “Don’t Know”.
4. Did your mother have diabetes? DK NO YES
5. Did your father have diabetes? DK NO YES
6. Did your sister or brother have diabetes? DK NO YES
7. Have you ever been told you have diabetes? Borderline DK NO YES Complete DX section
8. Did your mother have: high blood pressure, (heart attack, heart disease, or stroke)? DK NO YES
9. Did your father have: high blood pressure, (heart attack, heart disease, or stroke)? DK NO YES
10. Did your sibling have: high blood pressure, (heart attack, heart disease, or stroke)? DK NO YES
11. Have you ever been told you have high blood pressure? (OR ever had a heart attack or stroke)?
Borderline DK NO YES
12. Have you ever been told your cholesterol is a problem? DK NO YES
Complete DX section
13. Do you smoke tobacco? NO YES
14. Do you know how tall you are? ____________
15. Do you know your weight? ____________
In this next section I want to ask some questions about where you go when you’re sick.
16. Do you have a place you rely on for regular medical care? NO YES
a. (If Yes) i. Where do you go? (clinic/hospital name)_________________________________________________
ii. When is the last time you went for a visit? (month/year)___________________________________
iii. About how often did you go last year (times/year)? _______________________________________
iv. Did you get medical care anywhere else last year (clinic/hospital name/ER)? ____________________
b. (If no) i. What places have you gone in the past when you’re sick? ___________________________________
_____________________________________________________________________
17. Do you have health insurance or coverage of any kind? NO YES
a. (If Yes)

27
i. What plan? _________________________________
DX
18. The last time you saw your health care provider, did s/he talk about the things you can do to manage your illness? (high blood pressure, high cholesterol, diabetes)
a. (If yes) i. What things did s/he talk about?
(prompts: insulin salt stress mgmt. oral meds monitoring with strips feet exercise lose weight diet )
b. (If no) i. Do you know the kinds of things you can do to manage?
19. Has anyone ever told you you should be taking medication for your illness (diabetes, high blood pressure, high
cholesterol)? NO YES
a. (If Yes)
i. Did you take those medicines today? Some NO YES 1. (If Yes)
a. For some people taking medication is kind of hard, how’s it going for you?
2. (If No) a. What has been hard about getting or taking your medications?
b. (If NO) No one has told respondent they should be taking medication, skip to next section)
AGE (If client is 50 years old or older, born before 1963, please complete this section)
It has been recommended that people over 50 be screened for colon cancer and breast cancer.
20. Have you ever been screened for colon cancer? NO YES
(Prompt: colonoscopy, or checked for blood in your stool)
Women Only:
21. Have you ever had a mammogram? NO YES

28
Next I want to ask about your living situation and the things you do to manage your stress.
22. Where are you staying now? (record as much detail as provided, building name, shelter name, colloquial name, street location, all OK, multiple
locations expected—please capture as much detail as possible)
23. Is there something you do every day that helps you keep in balance/manage your stress?
24. If you had 3 options for exercise or fun activities you’d be interested in doing—(any kind of movement, activity,
class, equipment, practices… )What would they be?
a. _________________________ b. __________________________ c. ___________________________
I just have 3 more questions that I have to ask. We ask about gender because we don’t like to make any assumptions. We ask about race and ethnicity because some races and ethnic groups have a higher chance of having diabetes or hypertension.
25. What gender do you identify yourself as? ____________________
26. Which category best describes your race? ____________________
27. Are you of Hispanic, Latino, or Spanish origin? NO YES
28. Is there anything you’d like me to know about your health or about services that would help you manage your health better? (Offer FYI Card if response is longer than space allows)

29
Appendix B: American Diabetes Association Risk Self-Assessment Tool

30
Appendix C: American Heart Association Risk Self-Assessment Tool
Risk factors that you cannot control:
Yes No______________________________________________________________
□ □ Increasing age For men: are you over age 45?
For women: are you post-menopausal or over age 55?
□ □ Heredity (Including race)
Does anyone in you immediate family have a history of heart
disease or diabetes?
□ □ Are you black American or Latino American?
Risk factors that you can control1,2:
Yes No______________________________________________________________
□ □ Do you have diabetes?
□ □ Do you smoke?
□ □ High blood pressure
Is your blood pressure140/90 mmHg or higher? (normal is below
120/80 mmHg)
□ □ High cholesterol
Is your total cholesterol over 200?
□ □ Obesity
Are you 30 pounds or more over your recommended weight?
For men: is your waist measurement greater than 40 inches?
For women: is your waist measurement greater than 35 inches?
Inactivity
□ □ Do you exercise less than three times per week?
1.American Heart Association, Heart Disease and Stroke Statistics 2009 Update. Available at www.americanheart.org
2.U.S. Department of Human Services, National Institute for Health & National Heart Lung & Blood Institute. “Your Guide to
aHealthy Heart”NIH Publication No: 06-5269, November 2005. Available at www.nhibi.nih.gov
3.National Heart, Lung and Blood Institute “The Heart Truth for Women-A Speaker’s Guide.”NIH Publication No.06-5208.
Available at www.nhibi.nih.gov/health/hearttruth
4.National Heart, Lung and Blood Institute. Infographs, “Heart Disease Risk Factor ‘Multiplier Effect’ in Midlife Women.”
Available at www.nhibi.nih.gov/health/hearttruth. Accessed on September 10, 2007.