2015 legislative update regina godette-crawford, chief north carolina office of emergency medical...
TRANSCRIPT
2015 Legislative Update
Regina Godette-Crawford, ChiefNorth Carolina Office of Emergency Medical Services
2015 Session Legislation
• S99 Definition of Firefighter• H142/S144 Require Safety
Helmets / Under 21• S154-Clarifying the Good
Samaritan Law• H327-Allow Use of Pepper Spray
by EMS Workers• S377-Appropriate Funds for
Drug Overdose Meds.
• H429-Amend Med. Mal. Health Care Provider Definition
• H472/H487/S381-Community Paramedicine Pilot Project/Funds
• H512- Amend/Clarify Back-Up PSAP Requirements
• S531-Study Need for Pulse Oximeters in Schools

2015 Session Legislation Con’t
• H560-Assault Emergency Workers/Hospital Personnel
• H562-Amend Firearm Laws• S571-Expand Uses of 911 Fee• H611-Enact Death With Dignity
Act• H647-Epi Pens in All Child-
Serving Businesses• H652-Right to Try Act for
Terminally Ill Patients
• S707-Assignment of Benefits• H712-Pilot Project/Used Needle
Disposal• H715-Payments for Ambulance
Services• H730-County Provide 911
Dispatch Services• H847-Amend Laws Re: Medical
Treatment for Minors

FY 2016 Budget Resolution
What to expect?• A joint Senate - House continuing resolution• Consideration for Medicaid Expansion????• August 15th deadline for current continuing resolution….Budget• Possible tax reductions• Election & Restricting Law changes• Monument issues• Imposing a session length/limit???• The $4 billion House Infrastructure Plan -Bonds

Budget Woes
• Thirty-nine days past the July 1 start of the 2015-16 fiscal year – the due date for the new budget.
• House approach- examining the legislation bit-by-bit to figure out what the Senate wants to do. Seeking public input.
• Senate approach-At 508 pages, the Senate’s budget is nearly 200 pages longer than the House edition. Including changes that state senators want to make to state law.
• Medicaid reform- The Senate put its preference into the budget bill. The House wants Medicaid handled separately. After much debate…

Budget Woes Con’t
• To negotiate differences between the House & Senate budgets, the House appointed a team of 82 members of the NC House of Representatives to serve as conferees. (19 of which were democrats)
• The Senate appointed 32 Senators to serve as conferees to negotiate with the 82 House members. The only Senators not appointed to the conference committee were Sen. Phil Berger, the leader of the Senate and Sen. Bob Rucho who did not vote for the Senate budget. (0 of which were democrats)
• Budget negotiations are front stage and full focus. Any bill that did not come out of Senate committee by on July 24th, will likely not be heard until after all budget issues are fully resolved. The House has followed suit in shutting down its committees as well. There will be little legislation movement in the next few weeks except working behind closed doors on the state budget.
Budget Woes Con’t
• After 30 plus days of debate with the House and Senate President Pro Tem Phil Berger announced Wednesday that the Medicaid, sales tax and corporate incentives items would come off the table in the budget negotiations.
• Other disagreements:• Teacher & Teacher Assistants Layoffs• Taxes• State employee pay and benefits• Historic property tax credits
• One of the longest sessions in recent history was in 1998- budget work completed by October 31st.
• The last time the state budget was enacted before the start of the fiscal year was 2011.

Budget Key PlayersAppropriations & Health Committee
Senate: Ralph House, Louis Pate, Tommy Tucker ( Appr. & Health Chairs) House: Brian Brown, Justin Burr, Bert
Jones, Donny Lambeth (Health Chairs) Josh Dobson & Marilyn Avila (Appr. Chairs)

DHHS News
•WOS Resigns as DHHS Secretary•Medicaid Out of Budget Plan “stand-alone”•MCO vs. Doctors/Hospitals/AOC/CCNC model•New Secretary-Rick Brajer – LipoScience & ProNerve Bio-Tech Engineer “Business vs. Medical background”

New Medicaid Plan Senate, the House and Gov. Pat McCrory’s administration about how best to run the state’s $20 billion Medicaid program
• North Carolina would create a new department to run its health insurance program for the poor and disabled under a bill the Senate Health Care Committee
• The new plan would control the state’s spending by placing more of the risk for rising health care costs on private-sector companies. (Maintain the $130 million cash surplus)
• Move away from the current fee-for-service model in which doctors are paid for each procedure they perform and toward a system known as “capitation.”
• Under capitation, a health care provider is paid a flat fee for each patient it manages. Companies make money by keeping patients healthy and controlling costs of care when a patient gets sick.

New Medicaid Plan Con’t
• Creates a new department but allows the governor to appoint the director.
• The General Assembly would have broad authority to sign contracts, adjust salaries and control costs beyond the typical cabinet secretary.
• Allow large, national managed care companies to oversee patient care or to create North Carolina-based “provider-led entities” to manage patient costs.
• New companies, known as Provider-led entities (PLEs), would be run by doctors, hospitals and other providers.

New Medicaid Plan Con’t
• Carves out three slots for managed care organizations, which would be able to enroll patients across the state, and up to 12 slots for PLEs serving patients in different regions.
• The state would be carved up into either five, six, seven or eight regions by the new Medicaid department.
• Plan passed by the Senate Health Committee on August 6th
• Local mental health agencies, known as LME-MCOs, that were forged from old county mental health departments would continue to function for at least five years under the bill. However, this plan ends the state’s contract with Community Care of North Carolina, a nonprofit that provides case management services to Medicaid patients.

Ambulance Transports to Crisis CentersSession Law 2014-100, Section 12H.32Legislative Report DHHS-DMA March 1, 2015
• The NC DHHS examined the Wake County EMS Advanced Practice Paramedic Pilot and believed it to be good public policy and a basis to further explore the behavioral health system.
• The report included information on the Wake County pilot, other Advanced Practice Paramedic programs an overview of funding considerations, recommendations and remaining issues to be resolved.
• DMH/DD/SAS partnered with OEMS to pilot and assess “Community Paramedicine Behavioral Health Crisis Response”Block grants.
• To date, eight Crisis Solutions Initiative mini-grants have been allocated across the state.

Ambulance Transports to Crisis CentersSession Law 2014-100, Section 12H.32Legislative Report DHHS-DMA March 1, 2015
• Within 30 days of the end of the fiscal year, the LMO/MCO and EMS agency in each of the pilots will prepare a report on use of the funds and readiness for future implementation.
• At the conclusion of the pilot, LME/MCO and DMH and the participating EMS agency have agreed to standardize and refine data elements.
Ambulance Transports to Crisis CentersSession Law 2014-100, Section 12H.32Legislative Report DHHS-DMA March 1, 2015
• North Carolina Policy Options1. Attempt to have Medicaid Reimburse for alternative
health care locations.2. Examine the expansion of Advanced Practice Paramedic
pilot programs3. Examine allowing EMS agencies to utilize existing “treat,
no transport” billing codes for mental health assessments.
EMS & the New Medicaid Plan
What are ACO’s?
• Mandated by the ACA• The ACA included provisions for providers to be able to voluntarily
form an ACO, and for CMS to start this program.
• Definition of an ACO• CMS defines an ACO as a group of providers and suppliers of
services that will work together to coordinate care for the patients they serve under Original Medicare

ACO vs. MCO Model
• Accountable Care Organizations (ACOs) is a healthcare organization characterized by a payment and care delivery model that seeks to tie provider reimbursements to quality metrics and reductions in the total cost of care for an assigned population of patients. Groups of doctors, hospitals, and other health care providers, come together voluntarily to give coordinated high quality care to their Medicare patients.
• Managed Care Organizations (MCOs)- A health care delivery system consisting of affiliated and/or owned hospitals, physicians and others which provide a wide range of coordinated health services; an umbrella term for health plans that provide health care in return for a predetermined monthly fee and coordinate care through a defined network of physicians and hospitals Examples HMO, POS
ACOs Becoming Managed Care Organizations?
• Capitation• Many ACOs are approaching their third year where they may begin
to receive partially capitated payments from CMS.
• Closed Networks• ACOs already aggressively narrowing their networks in many
markets• MedPAC has espoused the notion of creating beneficiary
incentives (e.g., lower cost-sharing) for staying “in network” within an ACO
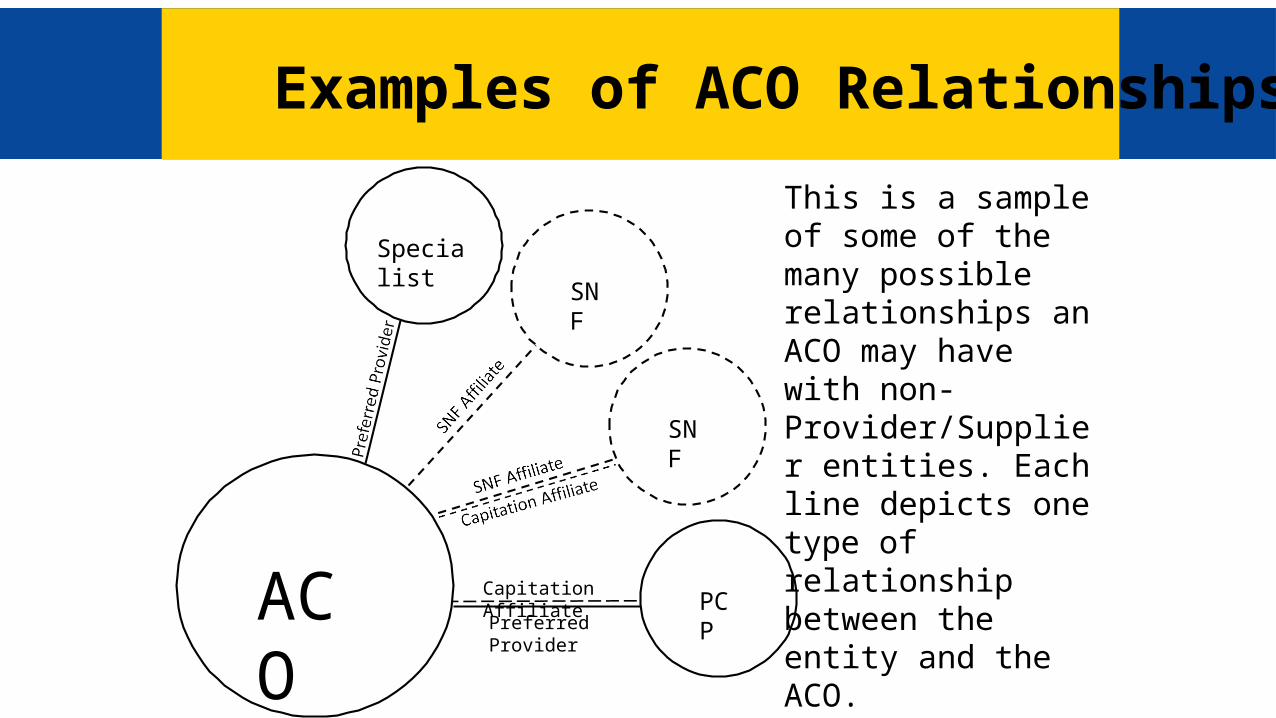
Examples of ACO Relationships
Preferred Provider
Capitation AffiliateACO
SNF
SNF
PCP
Specialist
This is a sample of some of the many possible relationships an ACO may have with non- Provider/Supplier entities. Each line depicts one type of relationship between the entity and the ACO.

ACO Readiness Collaborative Members
RI CT NJ
DE
MD
DC
WA
IL
WI
LA
AR
MM
OO
IA
MN
KS
NE
SD
NDMT
WY
CO
NM
ID
UT
AZ
NV
CA
OR
MA
SC
NC
VAW V
PA
VTNH
ME
FL
GAALMS
TN
KY
MI
OHIN
NY
TX
OK
As of 10/15/10
Confidential information of Premier, Inc. Not to be reproduced, copied or distributed without prior written consent of Premier, Inc.

Preparing for the Transition
• Establishing relationships with key partners/stakeholders to reach consensus on the gaps in technical knowledge and resources needed to determine how to pay for health care services based on quality rather than quantity.
• Regional Health Partnerships• Regional Health Plans• Infrastructure development (Pay for performance)• Program innovation and redesign (APP & Community Paramedicine, LME pilot
projects)• Quality Improvement (30 day readmissions/ED visits)• Policy Changes to Encourage Integration

Leadership Considerations and Questions
• When to make call for your agency/organization to start to shift to this new business model?
• How to initiate discussions with County Elected Officials/Board of Directors and other key parties such as hospitals?
• What is the process for negotiation and execution? • Is administrative infrastructure needed?• Should new talent be recruited to aid with transformation? • What factors should be considered when planning for change?• How do I engage and prepare my workforce?

General Assembly Considerations/Options• Legislators may introduce legislation designed to enable and promote
formation of health care collaboratives.• Other state initiatives may include a transition for the delivery and
payment of health care in NC from a fragmented, volume-driven fee-for-service system to one that is integrated, coordinated, efficient, quality-based and accountable for improving health outcomes, benefiting providers, consumers and all involved.
• Re-write or modify §G.S.153A-250. Ambulance services.

Next Steps
• Moving forward we will have to analyze pre- and post-ACA data, seek and acquire new data assets to support health reform evaluation, continue to forge and strengthen partnerships across sectors and agencies, and advocate for a unified approach to health reform in North Carolina.
• We will continue to assess the pressing issues of access to care and health system capacity. Our focus must shift to utilization, quality, patient experience, and cost of care.
Questions and Discussion