20150112 hip oa
TRANSCRIPT

Division of Geriatrics and Gerontology黃柏誠
Effect of Physical Therapy on Pain and Function in Patients With Hip
OsteoarthritisA Randomized Clinical Trial
JAMA. 2014 May 21;311(19):1987-97.

2
Hip osteoarthritis
• Guideline
– for symptomatic hip osteoarthritis
• conservative non-pharmacological physiotherapy
• irrespective of severity, pain levels, and functional
status
Introduction
OARSI recommendations for the management of hip and knee osteoarthritisOsteoarthritis Cartilage. 2010;18(4):476-499.

3
Importance
• Physical therapy for hip osteoarthritis
– limited evidence of RCT
Introduction

4
ObjectiveIntroduction
Hip osteoarthritis
Pain Function
12-wks multimodal physical therapy

5
Design
• A randomized, participant- and assessor
blinded, parallel-group, placebo-controlled
trial
Methods

6
Setting
• Intervention: 12 wks
• Follow-up: 24 wks
Methods

7
Participants
• 102 volunteers recruited from the community
– May 2010 ~ April 2012
Methods

8
Participants
• Inclusion
– ≧50 y/o
– hip osteoarthritis confirmed by radiograph#
– hip pain for ≧3 months
– average pain intensity in past week ≧40/100mm
(VAS)
– moderate difficulty with daily activities
Methods
# The American College of Rheumatology criteria for the classification and reporting of osteoarthritis of the hip. Arthritis Rheum. 1991;34(5):505-514.

9
Participants
• Exclusion
– Regular structured exercise or walking
– Physical therapy, chiropractic treatment in
past 6 mo
– Hip surgery in past 6 mo or waiting list for hip
surgery
– Hip or knee replacement
– Corticosteroid use
– Inability to walk unaided
Methods

10
FlowchartMethods
1441 patients with hip OA
203 for X-ray
111 for physical screening
102 randomized
1238 Excluded 212 Did not meet inclusion criteria 982 Met exclusion criteria 44 Did not undergo X-ray
92 Excluded 51 Did not meet inclusion criteria 6 No longer interested 35 No longer eligible
9 Could not reproduce hip pain

11
RandomizationMethods
5349
102 randomized
Active Placebo

12
Schedule
• intervention: 10 sessions over 12 weeks
Methods
intervention
60min
30-45min
12
3 4 5 6 7 8 9 10

13
Active treatment (12 wks)
• manual therapy
– hip thrust manipulation
– hip lumbar spine mobilization
– deep tissue massage
– muscle stretches
Methods
12
3 4 5 6 7 8 9 10 intervention

14
Active treatment (12 wks)
• home exercise (4 times/wk)
– strengthening of the hip abductors and quadriceps
– stretching and range of motion
– functional balance and gait drills
Methods
12
3 4 5 6 7 8 9 10 intervention

15
Active treatment (12 wks)
• education and advice
– osteoarthritis
– response to exercise and daily physical activity
– activity-rest cycle versus over-activity cycle
– joint protection advice
Methods
12
3 4 5 6 7 8 9 10 intervention

16
Active treatment (12 wks)
• Prescription of a single walking stick
– only if it will enable the patient to improve their
gait pattern and increase their daily physical
activity
Methods
12
3 4 5 6 7 8 9 10 intervention

17
Placebo (12 wks)
• inactive ultrasound
• inert gel
Methods
12
3 4 5 6 7 8 9 10 intervention

18
Schedule
• intervention: 10 sessions over 12 weeks
Methods
12
3 4 5 6 7 8 9 10 intervention

19
Schedule
• intervention: 10 sessions over 12 weeks
• follow up: 24 weeks
Methods
follow up
12
3 4 5 6 7 8 9 10 intervention

20
Follow up (24 wks)
• active group
– home exercise (3 times/wk)
Methods
follow up

21
Follow up (24 wks)
• placebo group
– self-applied gel (3 times/wk)
Methods
follow up

22
OutcomesMethods
blinded assessor questionnaire
s

23
Primary outcomesResults
PrimaryPain
Function
Pain: VAS (0-100mm) (0: best)
Function: WOMAC (0-68) (0: best)Western Ontario and McMaster Universities Osteoarthritis Index Likert version 3.1

24
OutcomesMethods
SecondaryPrimary
Impairments
Physical performance
Global change
Psychological status
Quality of life
Pain
Function
Pain
Function
Impairments
Physical performance
Global change
Psychological status
Quality of life

25
FlowchartResults
44
50
53
1441 patients with hip OA 1339
Excluded
96 (94%)
83 (81%)
49
46
39
102 randomized
Active Placebo
13 wk
36 wk

26
Characteristics
• similar at baseline
Results

27
Primary outcomesResults
PrimaryPain
Function
Pain: VAS (0-100mm) (0: best)
Function: WOMAC (0-68) (0: best)Western Ontario and McMaster Universities Osteoarthritis Index Likert version 3.1

28
Pain: within-group
• both groups
– statistically significant improvements
Primary Outcome
Activemean [ 95% CI ] mm
Placebomean [ 95% CI ] mm
13 week−17.8 [−26.2,
−9.3]−23.6 [−31.4, −15.9]

29
Pain: between-groups
• not significantly different
– mean difference of 6.9 [−3.9, 17.7] in favor of
placebo
Primary Outcome
Activemean(SD) mm
Placebomean(SD) mm
Baseline 58.8 (13.3) 58.0 (11.6)
13 week 40.1 (24.6) 35.2 (21.4)

30
Function: within-group
• both groups
– statistically significant improvements
Primary Outcome
Activemean [ 95% CI ]
Placebomean [ 95% CI ]
13 week−4.5 [−8.5,
−0.4]−5.7 [−9.1,
−2.3]

31
Function: between-groups
• not significantly different
– mean difference of 1.4 [−3.8, 6.5] in favor of
placebo
Primary Outcome
Activemean(SD)
Placebomean(SD)
Baseline 32.3 (9.2) 32.4 (8.4)
13 week 27.5 (12.9) 26.4 (11.3)

32
Secondary outcomes
• no between-group differences
– except balance step test
Results
…
33
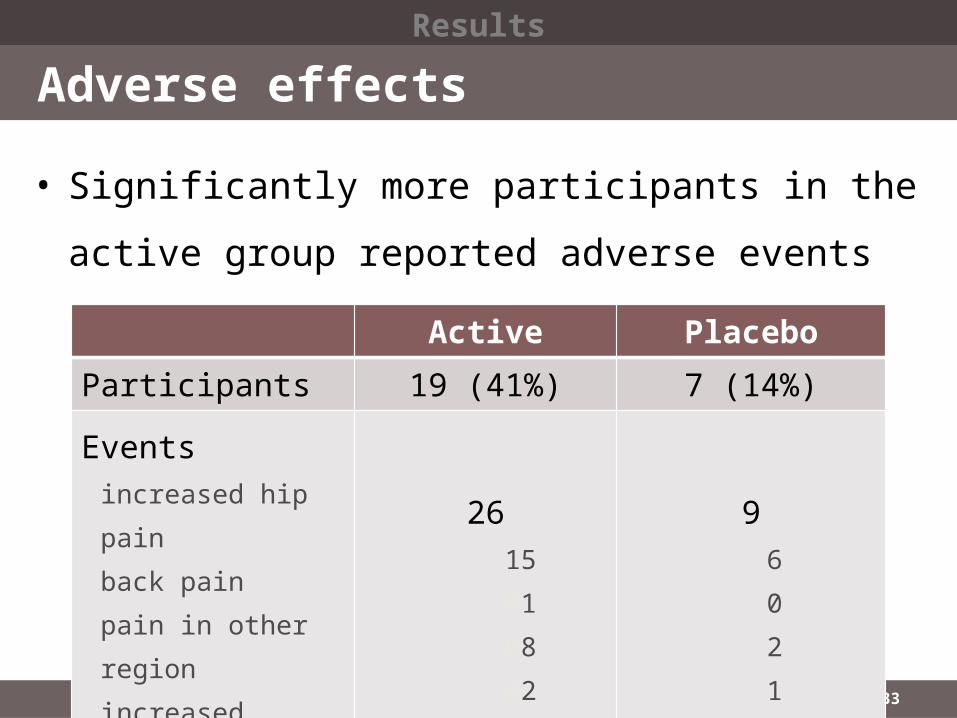
Adverse effects
• Significantly more participants in the active
group reported adverse events (p=0.003)
Results
Active Placebo
Participants 19 (41%) 7 (14%)
Eventsincreased hip painback painpain in other regionincreased stiffness
2615010802
96021

34
No additional benefits
• Both groups showed significant
improvements in pain and function following
treatment.
Discussion

35
Exercise & manual therapy
• Two randomized controlled trials in hip OA
– combining exercise and manual therapy
• does not confer additional benefits
• may have an adverse interaction effect
Discussion
Osteoarthritis Cartilage. 2013;21(4):525-534.Arch Phys Med Rehabil. 2013;94(2):302-314.
36
Strength
• minimized potential for bias
– a credible sham treatment
– concealing treatment allocation
– blinding (participants, assessor, biostatistician)
Discussion

37
Limitation
• lack of therapist blinding
• the absence of more blinding than expected
at the final follow-up assessment
• not all participants adhered fully to treatment
Discussion

38
Limitation
• the results cannot necessarily be generalized
– to different physical therapy programs
– to cohorts of younger patients
– to those with milder symptoms
Discussion

39
ConclusionSummary
Hip osteoarthritis
Pain Function
12-wks multimodal physical therapy
1) no additional benefit2) more adverse effects

40

41

42

43

44

45

46

47

48

49

50