2017 benefits guide - human resources · dearborn - voluntary std, ltd group no ... annual open...
TRANSCRIPT

2017 Benefits Guide

2 | Page
This document is an outline of the coverage proposed by the carrier(s). It does not include all of the terms, coverage, exclusions,
limitations, and conditions of the actual contract language. The policies and contracts themselves must be read for those details. Your
full Summary Plan Document (SPD) is made available through your Human Resources Department.
The intent of this document is to provide you with general information regarding the status of, and/or potential concerns related to your
current employee benefits environment. It does not necessarily fully address all of your specific issues. It should not be construed as,
nor is it intended to provide, legal advice. Questions regarding specific coverage issues can be directed to the Benefit Advocates at
Arthur J. Gallagher & Co., [email protected].

3 | Page
Support Team ················································································································· 2
Carrier Contact Information ························································································· 3
Benefits Guide Information ·························································································· 4
Benefits Overview ··········································································································· 5
Who is Eligible ················································································································· 6
Dependent Eligibility ······································································································· 6
When Coverage Begins ··································································································· 6
Making Changes to Coverage ························································································· 6
Monthly Premiums ····································································································· 7-11
Medical Plans Compared ······························································································· 12
Plan Highlights - UHC Choice Plus PPO ········································································ 13
Plan Highlights - UHC Choice Plus HSA ······································································· 14
Health Savings Account (HSA) Information ···························································· 15-17
UHC Health4Me App ····································································································· 18
Flexible Spending Account (FSA) ············································································· 19-20
FSA Online Claim Submission ························································································· 21 Dental Plan ····················································································································· 22
Voluntary Vision Plan ····································································································· 23
Voluntary Life and AD&D Plan ················································································· 24-25
Disability Coverage ········································································································ 26
COMPASS ······················································································································· 27
Employee Assistance Plan (EAP) ············································································· 28-29
Supplemental AFLAC Plans ··························································································· 30
Supplemental Accident Insurance ············································································ 31-32
Supplemental Cancer Insurance ·············································································· 33-34
Supplemental Critical Illness Insurance ········································································ 35
ID Theft and Legal Shield Coverage ············································································· 36
Newborn & Mothers Health Protection Notice ··························································· 37
Women’s Health and Cancer Rights Act ······································································ 37
Special Enrollment Rules ······························································································ 37
CHIPRA Notice ··············································································································· 38
Medicare D Notice ···································································································· 39-40
**If you (and/or your dependents) have Medicare or will become eligible for
Medicare in the next 12 months, a Federal law gives you more choices about
your prescription drug coverage. Please see pages 39-40 for more details.
Table of Contents

| Page
Hours of Operation Monday thru Friday—8:00 am to 5:00 pm
Claims Dept. Phone 512-499-8005 / 800-492-8005 Claims Dept. Fax 512-233-0102
Claims Dept. Email [email protected]
Gallagher Benefit Services Georgetown Contacts
Benefits Broker/Consultant Jeff Kloc 512-930-8350 [email protected]
Benefits Broker/Consultant Shannon Schooling 512-930-8356 [email protected]
Sr. Account Manager Sandra Quintanilla 512-930-8347 [email protected]
Account Coordinator Tammy Jowers 512-930-8354 [email protected]
City of Georgetown Contacts
HR Director Tadd Phillips 512-930-2504 [email protected]
Assistant Director of HR Laura Maloy 512-930-7233 [email protected]
Benefit/Wellness Program
Administrator
Niki Ross 512-930-3691 [email protected]
Lead HR Generalist Elliott Harper 512-931-7645 [email protected]
HR Generalist Tracey Bousquet 512-930-8494 [email protected]
HR Generalist Carina Reason 512-930-8485 [email protected]
HR Specialist Celina Morales 512-930-3639 [email protected]
Gallagher Benefit Services, Inc. is here to act as a liaison in your dealings with insurance carriers. If you are having problems getting claims paid or have questions regarding your coverage, let us deal with the insurance company for you. Please contact anyone listed below with questions regarding your employee benefits package.
We are here to help!
SUPPORT TEAM
2

3 | Page
CARRIER CONTACT INFORMATION
RESOURCE PHONE/WEB ADDRESS
United Health Care - Medical/Prescription Drugs, Flexible Spend-ing Account (FSA) Choice Plus Network
Group No. 906136 (866) 633-2446 www.myuhc.com
Health4Me App
Ameritas - Dental Group No. 301703 (800) 487-5553 www.ameritas.com
MetLife - Voluntary Vision, Voluntary Life and AD&D Group No. 5996616 (800) 638-5433 www.metlife.com
Dearborn - Voluntary STD, LTD Group No. GAE40395 (800) 348-4512 www.dearbornnational.com
COMPASS - Unlimited Access to healthcare expert and more (800) 513-1667
Email: [email protected]
A+ Federal Credit Union - Health Savings Account (HSA) (512) 302-6800, Option 6- Deborah Self
Alliance Work Partners - Employee Assistance Program (EAP) (800) 343-3822 www.awpnow.com
Aflac - Cancer, Critical Illness, Accident (512) 470-5322 - Stephanie Garland
ID Theft Solutions of America - ID Theft/Legal Shield Coverage (888) 494-8519 www.idtsoa.com
ICMA - Retirement Corporation (457 Plan)
(800) 669-7400 www.lcmarc.org
TMRS - Supplemental Death (512) 476-7577 www.tmrs.com

4 | Page
BENEFITS GUIDE INFORMATION
The City of Georgetown employees have access to benefits approved by the City Council
each year as part of the budget process. The benefits and services offered by the City may
be changed or terminated at any time. These benefits are not a guarantee of your employ
ment with the City. This Guide is designed to help you understand your benefits. Review this
material carefully before making your enrollment decisions. Your rights are governed by
each plan and not by the information in this Guide. If there is a conflict between the plan
documents and this Guide, the terms of the plan document govern. For detailed
information about the plans, refer to each plan document, contact the vendor
or the Employee Benefits Division of the Human Resources Department.
City Benefits Philosophy
The City is concerned for the health and welfare of its employees and is committed to providing cost-effective bene-
fits that assist employees in being physically and mentally healthy. All benefit plans require employees to assume re-
sponsibility for the choices they make and to be informed on how to use their benefits effectively.
Administration
The overall administration of the benefits program is re-evaluated and revised periodically to ensure it is simple, effi-
cient, cost effective and satisfies overall goals.
Communications
In keeping with this philosophy, the City will explore other areas of benefits to the extent they fill a need of a major
portion of the workforce and to the extent they be provided cost effectively and efficiency on a group basis. A variety
of media is used to communicate the benefits program to employees and their dependents. Methods used include
presentations, newsletters, email and the City’s website. In addition, benefits staff is available by phone or in person
to discuss benefits issues with employees and their families. Communication goals of the benefits program include:
Educating employees on how to use their benefits
Educating employees on how to be better consumers of all benefits
Increasing employee understanding of the value of their benefits
Cost
Since rising healthcare costs affect both the City and its employees, the City will continue to study new coverage op-
tions that help control healthcare costs. The program is designed to be cost effective, for both the short-term and
the long-term. The cost of the program is determined on an actuarial basis and does not vary with short-term finan-
cial considerations. Employee contributions are required to finance the cost of parts of the program.

5 | Page
Benefits Overview
The City of Georgetown provides several categories of benefits from which employees may choose to participate.
The plans are in effect January 1, 2017 to December 31, 2017.
*Your cost for Medical, Dental, Vision , Cancer, Accident and Flexible Spending plans in the Benefits Program will
be paid on a before-tax basis through your payroll deductions. This means that your benefit deductions go farther
because you save the federal income tax that would otherwise be required on these contributions.
**If you die while employed by the City, your beneficiary will receive a payment approximately equal to your
current annual salary. This benefit applies to both vested and non-vested members.
***The City pays for COMPASS if you and your dependents are covered under the medical plan.
Benefit Plan Automatic Voluntary Who Pays How You Pay
Medical Plans and Prescription Drugs You and The City Before tax*
Dental Plan You and The City Before tax*
Voluntary Vision Plan You Before tax*
TMRS Supplemental Death Benefit** The City No cost
Voluntary Life and AD&D You After tax
Voluntary Short-Term Disability (STD) You After tax
Long-Term Disability (LTD) The City No cost
Critical Illness You After tax
Cancer, Accident You Before tax*
COMPASS*** The City No cost
Flexible Spending Account (FSA) You Before tax*
Employee Assistance Program (EAP) The City No cost
ID Theft and Legal Shield Protection You After tax
International City Management Association
Retirement Corporation (457 plan) You Before tax*
Retiree Recreation Center Privilege The City No cost

6 | Page
Who is Eligible?
Employees. You are eligible to enroll in the City’s benefit plans if you are a regular, active full-time employee scheduled to work
at least 30 hours per week. As a regular full-time employee you are eligible for benefits on the first day of the month following
your date of hire.
Retirees. The cost to enroll as a retiree on any of the insurance plans is 100% the retirees responsibility. The city makes no con-
tribution towards retiree insurance.
Dependent Eligibility
You may also cover your eligible dependents, including:
Your legal spouse
Your children up to age 26 for medical coverage; your unmarried, eligible children up to age 26 for dental and vision coverage.
Children are defined as your natural children, stepchildren, legally adopted children and children for whom you are the court-
appointed legal guardian.
Dependent Grandchildren. Your unmarried grandchild must meet the requirements listed above and must be listed as a de-
pendent on your last IRS Tax Return or your spouse’s federal income tax return. Proof of claiming the dependent may be re-
quired from time to time.
Physically or mentally disabled children of any age who are incapable of self-support. Proof of disability may be required from
time to time.
When Coverage Begins
Initial Enrollment
When you first join the City you have 31 days to enroll yourself and your dependents for benefits. If you enroll on time, coverage
begins the first of the month following your date of hire. If you do not enroll within 31 days of becoming eligible, you will
automatically be enrolled in company-sponsored benefits, such as Long-Term Disability (LTD) and Dental ,but you will have to
wait until the next annual Open Enrollment to enroll in medical insurance or make changes to coverage. You will be able to
utilize the Employee Assistance Program (EAP) upon hire.
Annual Open Enrollment
Annual Open Enrollment is October 19th through November 9th, 2016. Coverage takes effect on January 1, 2017. Open Enroll-
ment is the only time employees may enroll in coverage without the occurrence of a qualifying event.
Making Changes to Coverage
Once you make your benefit elections, these choices remain in effect until the next annual Open Enrollment. You
may only make changes to your elections during the year if you have one of the following status changes:
Marriage, divorce, legal separation or death of a spouse
Gain or loss of an eligible dependent for reasons such as birth, adoption, court order, disability, death, or
reaching the dependent child age limit
Change in employment status, such as starting or ending employment for you, your spouse or
your children
IRS regulations require that for enrollment due to the qualifying events above, change forms must be submitted to
your benefits office within 30 days of that qualifying event.

7 | Page
Monthly Premiums
United Healthcare Choice PPO Plan
Type of Coverage
Employee Pays Per Month
Employee Only $75.00
Employee & Child(ren) $137.00
Employee & Spouse or Family $549.00
United Healthcare HSA Medical Plan*
Type of Coverage
Employee Pays Per Month
Employee Only $12.00
Employee & Child(ren) $69.00
Employee & Spouse or Family $276.00
If you choose NOT to enroll in one of the United Health Care medical plans, the City will pay you $150 per month.
Restrictions may apply.
Ameritas Dental Plan
Type of Coverage
Employee Pays Per Month
Employee Only $0.00
Employee & Child(ren) $19.32
Employee & Spouse $16.36
Employee & Family $40.55
MetLife Vision Plan
Type of Coverage
Employee Pays Per Month
Employee Only $6.41
Employee & Child(ren) $10.87
Employee & Spouse $12.85
Employee & Family $17.92
*The City of Georgetown contributes to your HSA account. Please see page 16 for details.
Contributions are prorated for employees hired after January 1, 2017

8 | Page
Stand alone AD&D is not available
Voluntary Life and AD&D Premiums
Voluntary Life
Employee/Spouse Monthly Premium
$10,000 $20,000 $30,000 $40,000 $50,000 $60,000 $70,000 $80,000 $90,000 $100,000
0-29 0.40 0.80 1.20 1.60 2.00 2.40 2.80 3.20 3.60 4.00
30-34 0.42 0.84 1.26 1.68 2.10 2.52 2.94 3.36 3.78 4.20
35-39 0.53 1.06 1.59 2.12 2.65 3.18 3.71 4.24 4.77 5.30
40-44 0.80 1.60 2.40 3.20 4.00 4.80 5.60 6.40 7.20 8.00
45-49 1.26 2.52 3.78 5.04 6.30 7.56 8.82 10.08 11.34 12.60
50-54 2.00 4.00 6.00 8.00 10.00 12.00 14.00 16.00 18.00 20.00
55-59 3.11 6.22 9.33 12.44 15.55 18.66 21.77 24.88 27.99 31.10
60-64 4.61 9.22 13.83 18.44 23.05 27.66 32.27 36.88 41.49 46.10
65-69 8.58 17.16 25.74 34.32 42.90 51.48 60.06 68.64 77.22 85.80
70-99 16.21 32.42 48.63 64.84 81.05 97.26 113.47 129.68 145.89 162.10
Voluntary AD&D Monthly Premium
0.35 0.70 1.05 1.40 1.75 2.10 2.45 2.80 3.15 3.50
Employee/Spouse Monthly Premium
$110,000 $120,000 $130,000 $140,000 $150,000 $160,000 $170,000 $180,000 $190,000 $200,000
0-29 4.40 4.80 5.20 5.60 6.00 6.40 6.80 7.20 7.60 8.00
30-34 4.62 5.04 5.46 5.88 6.30 6.72 7.14 7.56 7.98 8.40
35-39 5.83 6.36 6.89 7.42 7.95 8.48 9.01 9.54 10.07 10.60
40-44 8.80 9.60 10.40 11.20 12.00 12.80 13.60 14.40 15.20 16.00
45-49 13.86 15.12 16.38 17.64 18.90 20.16 21.42 22.68 23.94 25.20
50-54 22.00 24.00 26.00 28.00 30.00 32.00 34.00 36.00 38.00 40.00
55-59 34.21 37.32 40.43 43.54 46.65 49.76 52.87 55.98 59.09 62.20
60-64 50.71 55.32 59.93 64.54 69.15 73.76 78.37 82.98 87.59 92.20
65-69 94.38 102.96 111.54 120.12 128.70 137.28 145.86 154.44 163.02 171.60
70-99 178.31 194.52 210.73 226.94 243.15 259.36 275.57 291.78 307.99 324.20
Voluntary AD&D Monthly Premium
3.85 4.20 4.55 4.90 5.25 5.60 5.95 6.30 6.65 7.00
Dependent Child Monthly Premium
$1,000 $2,000 $4,000 $5,000 $10,000
0.24 0.48 0.96 1.20 2.40
Dependent Child AD&D Monthly Premium
0.09 0.17 0.22 0.43 0.04
To request coverage:
1. Choose the amount of employee coverage that you want to buy.
2. Look up the premium cost for your age group for the coverage amount you are electing on the
chart below.
3. Choose the amount of coverage you want to buy for your spouse. Again, find the premium cost on
the chart below. Note: Premiums are based on your age, not your spouse’s.
4. Choose the amount of coverage you want to buy for your dependent children. The premium costs
for each coverage option are shown below.
5. Fill in the enrollment form with the amounts of coverage you are electing. (To request coverage
over the non-medical maximum, please see your Human Resources representative for a medical
questionnaire that you will need to complete.) Remember, you must purchase coverage for your-
self in order to purchase coverage for your spouse or children.

9 | Page
Short-Term Disability (STD) Premiums

10 | Page
Aflac Premiums
AFLAC CANCER CARE PLAN CLASSIC - Series A78300
Premium IDR* (5 units) DCR* SDR* Total
18-75 INDIVIDUAL $15.86 $2.93 $0.00 $0.46 19.25
18-75 INSURED/SPOUSE $26.98 $6.50 $0.00 $0.85 34.33
18-75 ONE-PARENT FAMILY $15.86 $2.93 $0.46 $0.46 19.71
18-75 TWO-PARENT FAMILY $26.98 $6.50 $0.46 $0.85 34.79
IDR* = Optional Initial Diagnosis Rider (Series A-78050) premium 1-5 units
DCR*= Optional Dependent Child Rider (Series A-78051) premium
SDR*= Optional Specified Disease Rider (Series A-78052) premium
The rates shown below are for illustration purposes only; they do not imply coverage.
Rates are based on a semi –monthly payroll deduction.
ACCIDENT ADVANTAGE - 24 HOUR ACCIDENT OPTION 2 - Series A36000
Premium Total
18-75 $8.65 $8.65
18-75 $12.29 $12.29
18-75 $14.63 $14.63
18-75
INDIVIDUAL
NAMED INSURED/SPOUSE
ONE-PARENT FAMILY
TWO-PARENT FAMILY $19.11 $19.11

11 | Page
Aflac Premiums
The rates shown below are for illustration purposes only; they do not imply coverage.
LUMP SUM CRITICAL ILLNESS POLICY - Series A73100 - NON TOBACCO RATES
AGE COVERAGE $10,000 $20,000 $30,000
Total Total Total
18-24 INDIVIDUAL OR
ONE-PARENT FAMILY
$2.21 $2.99 $3.77
25-29 $2.47 $3.64 $4.81
30-34 $3.25 $4.81 $6.37
35-39 $4.42 $6.63 $8.84
40-44 $5.72 $8.71 $11.70
45-49 $6.96 $10.73 $14.50
50-54 $8.13 $12.55 $16.97
55-59 $9.23 $14.30 $19.37
60-64 $10.86 $16.84 $22.82
65-70 $10.86 $16.84 $22.82
18-24 HUSBAND WIFE OR
TWO-PARENT FAMILY
$3.58 $5.01 $6.44
25-29 $4.03 $5.98 $7.93
30-34 $5.27 $7.87 $10.47
35-39 $6.96 $10.60 $14.24
40-44 $8.71 $13.26 $17.81
45-49 $10.60 $16.32 $22.04
50-54 $12.74 $19.63 $26.52
55-59 $14.95 $23.01 $31.07
60-64 $18.40 $28.54 $38.68
65-70 $18.40 $28.54 $38.68
LUMP SUM CRITICAL ILLNESS POLICY - Series A73100 - TOBACCO RATES
AGE COVERAGE $10,000 $20,000 $30,000
Total Total Total
18-24 INDIVIDUAL OR
ONE-PARENT FAMILY
$2.86 $4.29 $5.72
25-29 $3.58 $5.53 $7.48
30-34 $4.94 $7.80 $10.66
35-39 $6.76 $10.66 $14.56
40-44 $8.78 $14.11 $19.44
45-49 $10.73 $17.23 $23.73
50-54 $12.55 $20.35 $28.15
55-59 $14.17 $23.01 $31.85
60-64 $16.58 $26.98 $37.38
65-70 $16.58 $26.98 $37.38
18-24 HUSBAND WIFE OR
TWO-PARENT FAMILY
$4.94 $7.54 $10.14
25-29 $5.98 $9.36 $12.74
30-34 $8.06 $12.74 $17.42
35-39 $10.73 $17.10 $23.47
40-44 $13.52 $21.58 $29.64
45-49 $16.51 $26.39 $36.27
50-54 $19.89 $31.85 $43.81
55-59 $23.21 $37.38 $51.55
60-64 $28.34 $46.02 $63.70
65-70 $28.34 $46.02 $63.70

12 | Page
Medical Plan Comparison Chart
Benefit Description UHC Choice Plus PPO Plan UHC Choice Plus HSA Plan
Calendar Year Deductible
· Individual
· Family
$3,000 $6,000
$3,000 $6,000
Maximum Out of Pocket (per calendar year)
· Individual
· Family
Includes Ded & Copays $4,000 $8,000
Includes Ded & Copays $4,000 $8,000
Maximum Lifetime Benefits Unlimited Unlimited
Physician/Specialist Office Visit
· Primary Physician
· Specialist Physician
$30 co-pay$50 co-pay
90% after deductible 90% after deductible
Emergency Room Services 100% after $250 co-pay* 90% after deductible
Urgent Care Provider 100% after $75 co-pay 90% after deductible
Hospital Care
· Inpatient Coverage
· Outpatient Surgery
100% after deductible 100% after deductible
90% after deductible 90% after deductible
Preventive Care 100% 100%
Labs and X-Rays
· Diagnostic-Outpatient
· Major Diagnostic (CT/PET Scans, MRIs)
100% after $50 co-pay 100% after deductible
90% after deductible 90% after deductible
Maternity (Includes delivery & postpartum care)
· Physician
· Facility
$50 co-pay* 100% after deductible
90% after deductible 90% after deductible
Home Health Care (60 visits/year) 100% after deductible 90% after deductible
Hospice Care 100% after deductible 90% after deductible
Outpatient Rehabilitation Therapy (limited visits/see plan summary)
100% after $50 co-pay 90% after deductible
Chemical Dependency
· Inpatient
· Outpatient
100% after deductible $50 co-pay
90% after deductible 90% after deductible
Mental Health Services
· Inpatient
· Outpatient
100% after deductible $50 co-pay
90% after deductible 90% after deductible
Prescription Drugs · Generic· Preferred Brand Name· Non-Preferred Brand Name· Mail Order (90 Day Supply)
$10 co-pay $40 co-pay $70 co-pay
3 times retail
Deductible must be met before copays apply $10 co-pay2 $40 co-pay2 $70 co-pay2
3 times retail
*Waived if admitted
The following comparison chart reflects In-Network coverage only. For Out-of-Network descriptions, please refer
to the following Summary of Benefits for each plan.

13 | Page
Choice Plus PPO Plan (1)
Benefit Description In-Network Coverage Out-of-Network Coverage
Calendar Year Deductible
· Individual
· Family
$3,000 $6,000
$5,000 $10,000
Maximum Out of Pocket (per calendar year)
· Individual
· Family
Includes Ded & Copays $4,000 $8,000
Includes Ded & Copays $15,000 $30,000
Maximum Lifetime Benefits Unlimited Unlimited
Physician/Specialist Office Visit
· Primary Physician
· Specialist Physician
$30 co-pay $50 co-pay
50% after deductible 50% after deductible
Emergency Room Services 100% after $250 co-pay1 100% after $250 co-pay1
Urgent Care Provider 100% after $75 co-pay 50% after deductible
Hospital Care
· Inpatient Coverage
· Outpatient Surgery
100% after deductible 100% after deductible
50% after deductible 50% after deductible
Preventive Care 100% Not Covered
Labs and X-Rays
· Diagnostic-Outpatient
· Major Diagnostic (CT/PET Scans, MRIs)
100% after $50 co-pay 100% after deductible
50% after deductible 50% after deductible
Maternity (Includes delivery & postpartum care)
· Physician
· Facility
$50 co-pay1
100% after deductible
50% after deductible 50% after deductible
Home Health Care (60 visits/year) 100% after deductible 50% after deductible
Hospice Care 100% after deductible 50% after deductible
Outpatient Rehabilitation Therapy (limited visits/see plan summary)
100% after $50 co-pay 50% after deductible
Chemical Dependency
· Inpatient
100% after deductible
$50 co-pay
50% after deductible 50% after deductible
Mental Health Services
· Inpatient
· Outpatient
100% after deductible
$50 co-pay
50% after deductible 50% after deductible
Prescription Drugs · Generic · Preferred Brand Name · Non-Preferred Brand Name · Mail Order
$10 co-pay $40 co-pay $70 co-pay
3 times retail
70% after co-pay 70% after co-pay 70% after co-pay
N/A
*Waived if admitted

14 | Page
Choice Plus HSA Plan (2)*
*The City of Georgetown contributes to your HSA account. Please see page 16 for details.
Contribution is prorated for employees hired after January 1, 2017
Benefit Description In-Network Out-of-Network
Calendar Year Deductible
· Individual
· Family
$3,000 $6,000
$6,000 $12,000
Maximum Out of Pocket (per calendar year)
· Individual
· Family
Includes Ded & Copays $4,000 $8,000
Includes Ded & Copays $6,000 $12,000
Maximum Lifetime Benefits Unlimited Unlimited
Physician/Specialist Office Visit
· Primary Physician
· Specialist Physician
90% after deductible 90% after deductible
50% after deductible 50% after deductible
Emergency Room Services 90% after deductible 90% after deductible
Urgent Care Provider 90% after deductible 50% after deductible
Hospital Care
· Inpatient Coverage
· Outpatient Surgery
90% after deductible 90% after deductible
50% after deductible 50% after deductible
Preventive Care 100% Not Covered
Labs and X-Rays
· Diagnostic-Outpatient
· Major Diagnostic (CT/PET Scans, MRIs)
90% after deductible 90% after deductible
50% after deductible 50% after deductible
Maternity (Includes delivery & postpartum care)
· Physician
· Facility
90% after deductible 90% after deductible
50% after deductible 50% after deductible
Home Health Care (60 visits/year) 90% after deductible 50% after deductible
Hospice Care 90% after deductible 50% after deductible
Outpatient Rehabilitation Therapy (limited visits/see plan summary)
90% after deductible 50% after deductible
Chemical Dependency
· Inpatient
· Outpatient
90% after deductible 90% after deductible
50% after deductible 50% after deductible
Mental Health Services
· Inpatient
· Outpatient
90% after deductible 90% after deductible
50% after deductible 50% after deductible
Pharmacy Drugs. The full cost of the drug is applied to the deductible before benefits are considered for payment under the pharmacy plan.
· Generic· Preferred Brand Name· Non-Preferred Brand Name
· Mail Order
$10 co-pay $40 co-pay $70 co-pay
3 times retail
70% after co-pay 70% after co-pay 70% after co-pay
N/A

15 | Page
Health Savings Accounts (HSA)
What is an HSA?
A Health Savings account (HSA) is a tax-advantaged personal
savings account that works in conjunction with a high deducti-
ble health plan (HDHP). Participants can pay for qualified
medical expenses with tax-free dollars from their HSA.
There is no ‘use-it-or-lose-it’ requirement, the account is porta-
ble and the balance plus earnings (from interest and/or
investments) carries over year after year, all tax-free. If HSA
monies are used for non-qualified medical expenses prior
to age 65, a 20% penalty plus ordinary income tax must be
paid to the IRS.
Eligibility Requirements:
In order to open a Health Savings Account, you MUST meet
the following requirements:
Covered by the City of Georgetown’s HDHP Plan
NOT covered by another health insurance plan that is
not a qualified HDHP including:
A spouse’s medical plan
Medicare
Tricare
Note: Does not apply to specific injury, accident,
disability, dental care, vision care and/or long term
care insurance plans.
NOT participating in an employer-sponsored Flexible
Spending Account (unless limited use)
NOT claimed as a dependent on someone else’s tax
return
Your spouse must also NOT participate in a Healthcare
Flexible Spending Account. The Dependent Care FSA will
not disqualify you from opening an HSA.
HSAs allow:
Tax-free contributions by employer, employee or others
Tax-free growth of interest or investment earnings
Tax-free distributions of principal and interest to pay
for qualified medical expenses
Accumulation of unused funds and portability between
employers. No “Use it or Lose it” rules. Portable from em-
ployer to employer and across state lines.
Flexible use – You choose whether or when to use the
account for health expenses, now or after employment.
In addition to paying for current expenses,
funds can be used to pay for:
COBRA premiums
Long-term Care premiums
Out-of-Pocket expenses for Medicare
Medical insurance during unemployment
Services not covered under a future health plan
Medicare premiums
If you are covered under the qualified High Deductible
Health Plan and meet the eligibility requirements you
may open a Health Savings Account (HSA). HSA plans
are intended to be used to pay for healthcare for the
individual and his or her covered dependents.
Distributions from an HSA to pay for qualified medical
expenses are not taxable.
Qualified health care expenses are expenses which are:
Incurred for the individual, his/her spouse or a tax
dependent;
Eligible as defined in Internal Revenue Code Section
213(d) – generally defined as expenses for the
diagnosis, cure, mitigation, treatment or prevention of
disease;
Not reimbursed by insurance or another health plan;
and
Not deducted on the individual’s tax return.
Medical expenses that may be reimbursed through a
Health Savings Account under IRS Code Section 213
include (but are not limited to) the following:
Deductible payments;
Coinsurance payments;
Dental care not provided through another health
insurance plan;
Prescription drugs;
Emergency ambulance service;
Chiropractic services;
Eyeglasses and/or contact lenses;
Hearing devices;
Psychiatric care;
Psychologists’ fees;
Acupuncture
Over the Counter Drugs can be reimbursed from the
HSA as long as they meet the criteria set out in
Internal Revenue Code Section 213(d) and you have
a prescription on file for the medication.

16 | Page
Health Savings Accounts (HSA)
Contributing to your HSA
When you participate in an HSA, you set aside money to
pay for eligible out-of-pocket expenses. Money can be
contributed to your HSA by you or anyone else. The IRS
2017 calendar year maximums for these savings
accounts are:
Maximum 2017 (calendar year) Contribution:
$3,400 for Employee Only
$6,750 for Employee + Spouse, Employee +
Child(ren), Employee + Family
$1,000 Catch Up Contribution for Employees
age 55 and up
A Calendar Year is the 12-month period of January
1st - December 31st.
If you are age 55 or older, you can make an additional
contribution amount of $1,000. The HSA cannot receive
contributions after the individual has enrolled in
Medicare. For the most current HSA contribution
information, please go to the U.S. Dept. of Treasury web
site at http://www.ustreas.gov/offices/public-affairs/hsa.
Note for Newly Eligible and Partial Year Participants:
If you become newly eligible to contribute to an HSA
during the year, you may contribute the maximum
contribution for the year (without incurring taxes or a
penalty on the amount of the contribution) provided you
continue to remain eligible for a 13 month period
beginning December 1st of the year in which you
become eligible and ending on December 31st of the
following year.
If you do not remain eligible for a 13 month period shown
above, your excess contributions will be subject to
federal income tax and may be subject to the 6% excise
tax. Please contact your tax advisor for assistance
determining if your partial year contributions will be
subject to taxes and penalties.
Using your HSA
With an HSA, your contributions, earnings and eligible
withdrawals are all tax-free. As long as your withdrawals
are used to pay for qualified health care expenses, you
won’t pay taxes. Contributions that the City of Georgetown
makes to your HSA are yours. There are no vesting re-
quirements or forfeiture provisions. Unlike flexible spend-
ing accounts, HSAs do not have a “use it or lose it” re-
quirement. Your account balance rolls over from year to
year and will earn interest tax-free.
Tax Filing
You will receive a 1099SA and a 5498SA and be required
to file Form 8889 with your annual tax return. Please see
your tax advisor if you have any questions.
Employer Contributions
The City of Georgetown contributes annually to employee
accounts. This amount does count towards your maximum
contribution (calendar year). This amount is prorated for
employees hired after January 1, 2017.
You are responsible for the eligibility of all
items and keeping receipts for tax purposes.
Not all expenses that are
qualified health care
expenses under the HSA
count towards the
satisfaction of the calen-
dar year deductible.
The City of Georgetown HSA Contributions*:
*One-time contribution increase for Calendar Year 2017
Tier Annual Contribution
Employee Only $1100
Employee + Spouse $1200
Employee + Child(ren) $1200
Employee + Family $1400
17 | Page
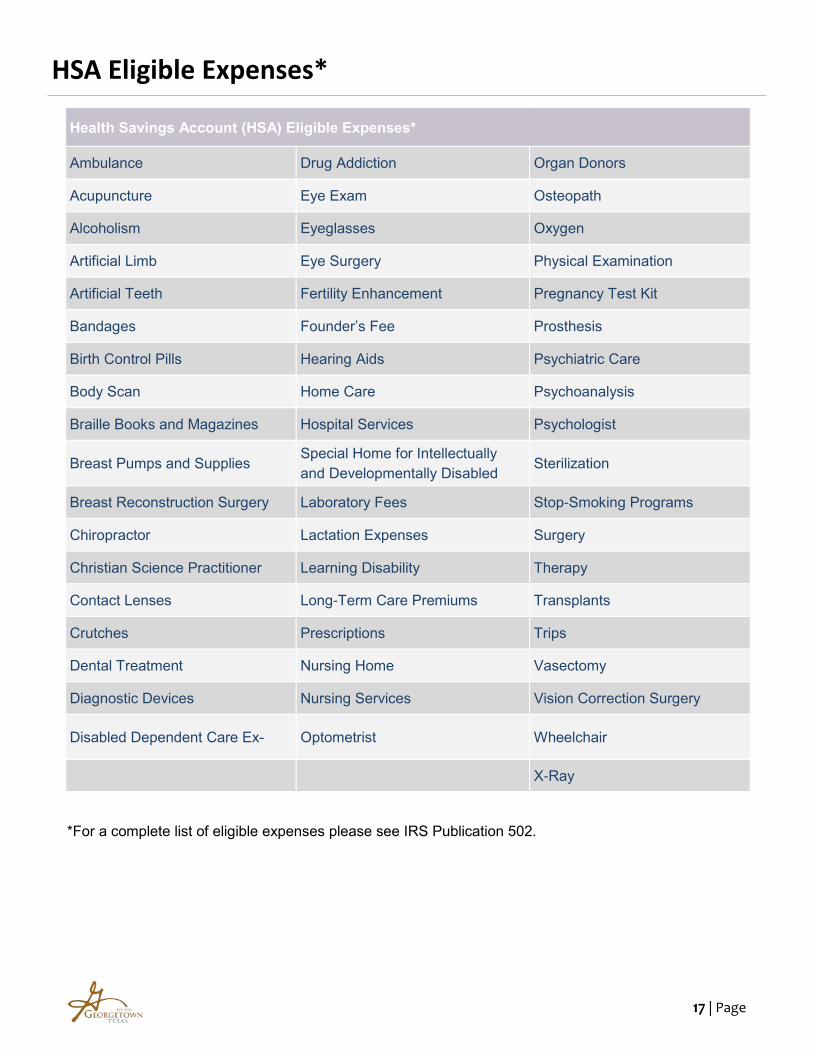
HSA Eligible Expenses*
*For a complete list of eligible expenses please see IRS Publication 502.
Health Savings Account (HSA) Eligible Expenses*
Ambulance Drug Addiction Organ Donors
Acupuncture Eye Exam Osteopath
Alcoholism Eyeglasses Oxygen
Artificial Limb Eye Surgery Physical Examination
Artificial Teeth Fertility Enhancement Pregnancy Test Kit
Bandages Founder’s Fee Prosthesis
Birth Control Pills Hearing Aids Psychiatric Care
Body Scan Home Care Psychoanalysis
Braille Books and Magazines Hospital Services Psychologist
Breast Pumps and Supplies Special Home for Intellectually
and Developmentally Disabled Sterilization
Breast Reconstruction Surgery Laboratory Fees Stop-Smoking Programs
Chiropractor Lactation Expenses Surgery
Christian Science Practitioner Learning Disability Therapy
Contact Lenses Long-Term Care Premiums Transplants
Crutches Prescriptions Trips
Dental Treatment Nursing Home Vasectomy
Diagnostic Devices Nursing Services Vision Correction Surgery
Disabled Dependent Care Ex- Optometrist Wheelchair
X-Ray

18 | Page
UHC Health4Me App

19 | Page
Flexible Spending Account (FSA)
What is the purpose of the plan?
The City of Georgetown has established this plan to help employees save tax dollars and increase their net pay.
What Is a Flexible Spending Account?
A Flexible Spending Account is designed exclusively for employees, and is established by your employer under Section
125, 129, 132f or 105 of the Internal Revenue Code. This plan allows a participating employee to take certain expenses
from their paycheck on a pre-tax basis. This means that all amounts deducted from your paycheck and contributed
toward your plan will not be subject to Federal Income tax, nor will it be subject to Social Security tax.
What are eligible expenses under the plan?
Premium Payments
Allows you to use pre-tax rather than after-tax dollars to pay for your share of employer sponsored insurance
premiums (medical, dental and vision). Premium payment is a simple payroll adjustment which is handled internally
by your employer’s payroll department. Do not add premium contributions to your medical expense account
contributions.
Medical Expenses (Paid By the Employee)
An employee’s out-of-pocket health care expenses can be paid with before-tax dollars when an employee elects to
deposit some of those dollars into their Medical Expense Reimbursement Account. The amount the employee elects
to set aside in this account will be held until he or she submits receipts for eligible expenses to be reimbursed. The
maximum amount an employee can elect is $2,550 for the 2017 plan year. Eligible expenses can include (not limited
to*:
Above Usual & Customary Charges Chiropractor
Co-insurance Deductibles
Dental Expenses Eyeglasses & Contact Lenses
Hearing Aids Physical Exams
Pre-Existing Conditions Prescribed Birth Control
Psychologist Special Medical Equipment
Special Tests (allergy, etc.)
*For a complete list of eligible expenses please see IRS Publication 508.
Your FSA Plan includes an Debit Card
You will be provided with a Health Care Spending Card Debit MasterCard® that may be used to pay for certain Eligible
Expenses directly from your HCSA and/or DCSA. The Health Care Spending Card Debit MasterCard® allows for direct
payment to qualified locations and providers and can be used at any approved location that accepts MasterCard®. Use
of the Health Care Spending Card Debit MasterCard® is voluntary.
The Health Care Spending Card Debit MasterCard® may be used at any approved provider or merchant with a Point-of-
Service (POS) bankcard terminal that accepts MasterCard® or your Health Care Spending Card Debit MasterCard®
number can be entered online or on an order form, similar to using a credit card number. You can even use your Health
Care Spending Card Debit MasterCard® to pay for a bill you receive in the mail if the merchant or provider accepts
MasterCard®. Examples of qualified locations and providers include hospitals, physician and dental offices, vision care
providers, retail pharmacy counters, and child and adult day care facilities.
20 | Page
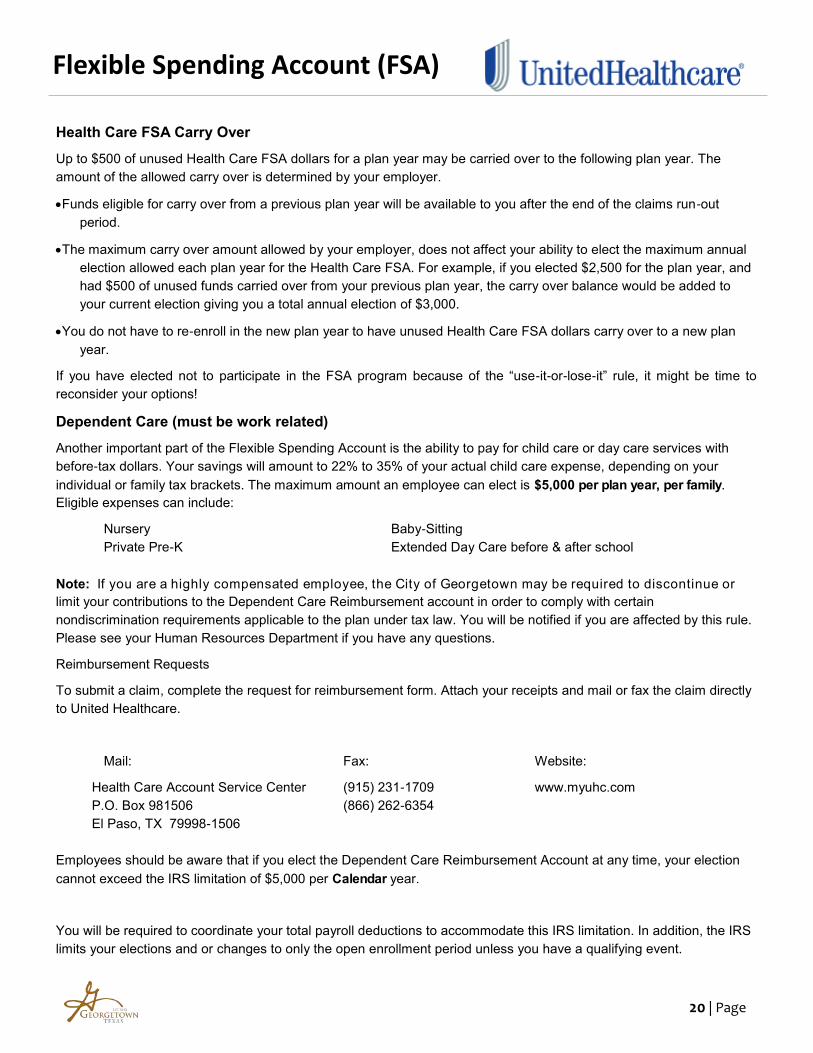
Health Care FSA Carry Over
Up to $500 of unused Health Care FSA dollars for a plan year may be carried over to the following plan year. The
amount of the allowed carry over is determined by your employer.
Funds eligible for carry over from a previous plan year will be available to you after the end of the claims run-out
period.
The maximum carry over amount allowed by your employer, does not affect your ability to elect the maximum annual
election allowed each plan year for the Health Care FSA. For example, if you elected $2,500 for the plan year, and
had $500 of unused funds carried over from your previous plan year, the carry over balance would be added to
your current election giving you a total annual election of $3,000.
You do not have to re-enroll in the new plan year to have unused Health Care FSA dollars carry over to a new plan
year.
If you have elected not to participate in the FSA program because of the “use-it-or-lose-it” rule, it might be time to
reconsider your options!
Dependent Care (must be work related)
Another important part of the Flexible Spending Account is the ability to pay for child care or day care services with
before-tax dollars. Your savings will amount to 22% to 35% of your actual child care expense, depending on your
individual or family tax brackets. The maximum amount an employee can elect is $5,000 per plan year, per family.
Eligible expenses can include:
Nursery Baby-Sitting
Private Pre-K Extended Day Care before & after school
Note: If you are a highly compensated employee, the City of Georgetown may be required to discontinue or
limit your contributions to the Dependent Care Reimbursement account in order to comply with certain
nondiscrimination requirements applicable to the plan under tax law. You will be notified if you are affected by this rule.
Please see your Human Resources Department if you have any questions.
Reimbursement Requests
To submit a claim, complete the request for reimbursement form. Attach your receipts and mail or fax the claim directly
to United Healthcare.
Mail: Fax: Website:
Health Care Account Service Center (915) 231-1709 www.myuhc.com
P.O. Box 981506 (866) 262-6354
El Paso, TX 79998-1506
Employees should be aware that if you elect the Dependent Care Reimbursement Account at any time, your election
cannot exceed the IRS limitation of $5,000 per Calendar year.
You will be required to coordinate your total payroll deductions to accommodate this IRS limitation. In addition, the IRS
limits your elections and or changes to only the open enrollment period unless you have a qualifying event.
Flexible Spending Account (FSA)

21 | Page

22 | Page
Dental Plan
City of Georgetown’s dental plan is administered through Ameritas Group and provides you and your family with
coverage for typical dental expenses such as cleanings, x-rays, fillings and orthodontia for children. You get bene-
fits for a wide range of services. While there is a network of providers you can utilize, benefit percentages are the
same regardless of whether you visit an in-network or out-of-network provider. Utilizing an in-network provider will
result in a lower patient responsibility overall. Out-of-Network benefits are subject to Reasonable and Customary
charges and you may be balance billed if your dentist charges above this amount.
You can take advantage of online self-service capabilities with Ameritas online services at www.ameritas.com.
Check the status of your claims Estimate dental cost
Find a provider View your Explanation of Benefits online
Coverage Type In-Network Out-of-Network
Deductible
Individual
Family
Annual Maximum Benefit (per Individual)
$50 $150
$2,000
$50 $150
$2,000
Preventive Care (No deductible)
Cleanings 4 in 12 months
Examinations 1 in 6 months
Fluoride Treatments 2 in 12 months*
Full-Mouth X-rays 1 in 60 months
Bitewing X-rays 1 in 12 months
Space Maintainers
Sealants*
100%
100%
Basic Restorative Endodontics Root Canal
Periodontal Surgery
Periodontal Maintenance
General Anesthesia
Oral Surgery
80% 80%
Major Restorative Implants
Bridges 1 in 5 years
Dentures 1 in 5 years
Crowns / Inlays /Onlays 1 per tooth in 5 years
Repairs
Consultations
50% 50%
Orthodontia Children only up to age 19
Lifetime maximum $1,500
60% 60%
*Children 13 and under

23 | Page
Vision Plan
The City’s basic Vision Plan promotes preventive care through regular eye exams and provides coverage for correc-
tive materials, such as glasses and contact lenses. The Vision Plan is administered through MetLife. The vision plan
includes a routine/basic vision examination yearly and provides coverage for lenses or contacts every year.
In-Network Providers
With your vision benefits, choose a provider from the participating provider list. Present your ID card for services
at the time of service. Except for any applicable copayment, do NOT pay your participating provider for services or
eyewear covered by your MetLife benefit.
Non-Network Providers
If you choose a non-participating provider, you will be expected to pay the doctor for services received. You will
then need to send the original receipt from your non-participating doctor to MetLife for reimbursement. MetLife
will review your eligibility and send the appropriate reimbursement to you.
Plan Feature In-Network Provider Out-of-Network Provider
Vision Examination $10 co-pay $45 Allowance
Frames
$25 co-pay & up to $150
Allowance
$85 Costco Allowance
$25 Co-pay & up to $70
retail value
Lenses (Clear, Standard, Glass or Plastic)
Single Vision (per pair)
Bifocal (per pair)
Trifocal (per pair)
Lenticular (per pair)
$25 co-pay $25 co-pay $25 co-pay $25 co-pay
$30 Allowance $50 Allowance $65 Allowance
Up to $100 Reimbursement
Contact Lenses*
Elective
Medically required
$25 co-pay & up to $150 Allowance
$25 co-pay
$105 Allowance $210 Allowance
Frequency
Vision Examination
Frames
Lenses
Contact Lenses
Once each 12 months Once each 12 months Once each 12 months Once every 12 months
*Contact lenses and related professional services (fitting, evaluation and follow-up) are covered in lieu of eyeglasses. Coverage includes all
contact lens types (i.e., standard daily wear, extended wear, disposable, toric, gas permeable, and bifocal).

24 | Page
Voluntary Life and AD&D
Life and AD&D Amount Must Match!
Please note, that the Non Medical Maximum applies to NEW HIRES ONLY. Any new enrollments that were previ-
ously waived or increases in coverage for Employees, Spouse and Children will require the completion of an Evi-
dence of Insurability form from each individual for approval. Please see HR for details.

25 | Page

26 | Page
Disability Plans
Plan Features Benefits
Eligibility You are eligible to participate if you are an active full-time employee working 30 or more hours per week.
Weekly Benefit Amount You may select units of $50 with a minimum election of $100 and a maximum election of $1,000, not to exceed 60% of your weekly covered basic pay.
Maximum Duration 13 weeks
Benefits Begin 8th day for accident 8th day for sickness or pregnancy
According to City policy, all of your existing sick and vacation time must be exhausted be-fore STD kicks in.
Voluntary Short-Term Disability (STD)
The City offers you the option of obtaining Short-Term Disability (STD) insurance administered by Dearborn Nation-al. Short-Term disability is intended to protect your income for a short duration in case you become ill or injured.
If you are currently enrolled in the Short-Term Disability insurance, you may increase your benefit amount without proof of good health; however, the amount of your increase will be subject to a new pre-existing conditions limita-tion period. If you are a new hire and are applying within 31 days of becoming eligible, the employee Guarantee issue amount is $1,000. This means you will be able to purchase up to $1,000 of Voluntary Short-Term Disability in-surance coverage without having to fill out a health questionnaire.
Plan Feature Benefits
Eligibility All full-time active employees working 30 or more hours per week.
Monthly Benefit 60% of your covered monthly pre-disability pay to a maximum of $8,000 per month.
Benefits Begin After 90 days of disability
Maximum Benefit Duration Social Security Normal Retirement Age (SSNRA)
Long-Term Disability (LTD)
The City provides you with Long-Term Disability insurance through Dearborn National. Long-term disability is intended to help continue your income if you become unable to work due to illness or injury. This plan is 100% Employer-paid.
27 | Page
COMPASS

28 | Page
Employee Assistance Program (EAP)

29 | Page

30 | Page
Aflac Plans
31 | Page
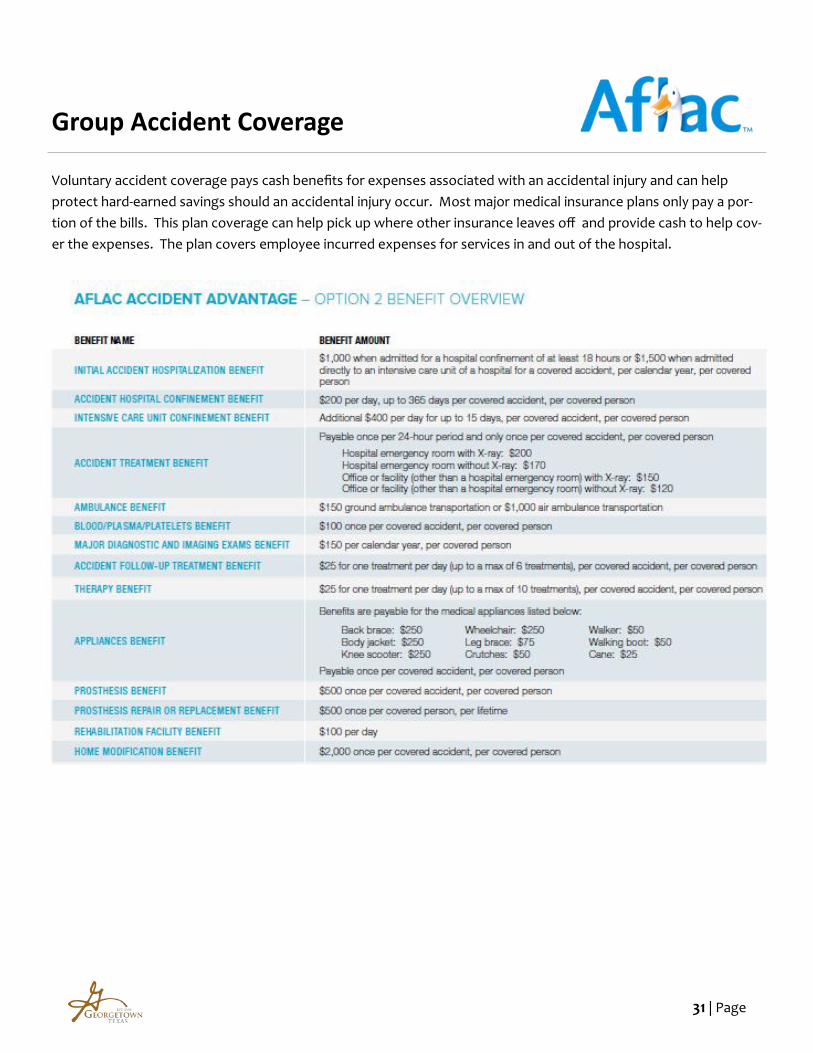
Group Accident Coverage
Voluntary accident coverage pays cash benefits for expenses associated with an accidental injury and can help
protect hard-earned savings should an accidental injury occur. Most major medical insurance plans only pay a por-
tion of the bills. This plan coverage can help pick up where other insurance leaves off and provide cash to help cov-
er the expenses. The plan covers employee incurred expenses for services in and out of the hospital.

32 | Page

33 | Page
Group cancer coverage provides cash benefits for cancer and other specified diseases, and can help cover the costs
of specific cancer and specified disease treatments and expenses as they happen. This plan can help provide added
financial security when it is needed most.
Group Cancer Coverage

34 | Page

35 | Page
Voluntary critical illness coverage provides a lump sum cash benefit to help you cover the out-of-pocket expenses
associated with a critical illness. Critical illness coverage can help offer peace of mind when a critical illness
diagnosis occurs.
Group Critical Illness Coverage
Critical illness events covered by the Lump Sum Critical Illness policy include:
Lump Sum Benefit options of $10,000, $20,000 or $30,000 for primary insured.
• Coma
• End-Stage Renal Failure
• Heart Attack
• Major Human Organ Transplant
• Paralysis
• Stroke

36 | Page
Legal Shield & Identity Theft Coverage

37 | Page
Important Notices
This book highlights some of the main features of
your benefit programs, but does not include all plan
rules, features, limitations or exclusions. The terms of
your benefit plans are governed by legal documents,
including insurance contracts. Should there be any
inconsistencies between this book and the legal plan
documents, the plan documents are the final authori-
ty. The City of Georgetown reserves the right to
change or discontinue its benefit plans at any time.
HIPAA Privacy Notice
HIPAA requires the City of Georgetown to notify you that
a privacy notice is available upon request. Please contact
Human Resources if you have any questions.
Special Enrollment Notice
If you are declining coverage for yourself or your depend-
ents (including your spouse) because of other health in-
surance or group health plan coverage, you may be able
to enroll yourself or your dependents in this plan if your
dependents lose eligibility for that other coverage (or if the
employer stops contributing towards your or your depend-
ents ‘ other coverage). However, you must request and
complete enrollment within 31 days after yours or your
dependents’ coverage ends (or after the employer stops
contributing towards the other coverage). In addition, if
you have a new dependent as a result of marriage, birth,
adoption, or placement for adoption, you may be able to
enroll yourself and your dependents. However, you must
request and complete enrollment within 31 days after the
marriage, birth, adoption, or placement for adoption.
Special enrollment rights also may exist in the following
circumstances:
If you or your dependents experience a loss of eligibil-
ity for Medicaid or a state Children’s Health Insurance
Program (CHIP) coverage and you request enroll-
ment within 60 days after that coverage ends; or
If you or your dependents become eligible for a state
premium assistance subsidy through Medicaid or a
state CHIP with respect to coverage under this plan
and you request enrollment within 60 days after the
determination of eligibility for such assistance.
Note: The 60 day period for requesting enrollment ap-
plies only in these last two listed circumstances relating to
Medicaid and State CHIP. As described above, a 31 day
period applies to most special enrollments. To request
special enrollment or obtain more information, contact
Human Resources at the City of Georgetown.
The Women’s Health and Cancer Rights Act
The Women’s Health and Cancer Rights Act of 1998
requires group health plans that provide coverage for a
mastectomy to provide coverage for certain reconstructive
services. This law also requires that written notice of the
availability of the coverage be delivered to all plan
participants upon enrollment and annually thereafter.
This language serves to fulfill that requirement for this
year. These services include:
Reconstruction of the breast upon which the mastec-
tomy has been performed;
Surgery / reconstruction of the other breast to pro-
duce a symmetrical appearance;
Prostheses; and
Treatment for physical complications during all stages
of mastectomy, including lymphedemas.
In addition, the plan may not:
Interfere with a participant’s rights under the plan to
avoid these requirements; or
Offer inducements to the healthcare provider, or
assess penalties against the provider, in an attempt to
interfere with the requirements of the law.
However, the plan may apply deductibles, coinsurance,
and co-payments consistent with other coverage provided
by the plan.
Newborns Act Disclosure
Group health plans and health insurance issuers general-
ly may not, under Federal law, restrict benefits for any
hospital length of stay in connection with childbirth for the
mother or newborn child to less than 48 hours following a
vaginal delivery, or less than 96 hours following a cesare-
an section.
However, Federal law generally does not prohibit the
mother’s or newborn’s attending provider, after consulting
with the mother, from discharging the mother or her new-
born earlier than 48 hours or 96 hours as applicable). In
any case, plans and issuers may not, under Federal law,
require that a provider obtain authorization from the plan
or the insurance issuer for prescribing a length of stay not
in excess of 48 hours or 96 hours).

38 | Page
CHIPRA Notice
39 | Page
Medicare D Notice
Important Notice from the City of Georgetown
About Your Prescription Drug Coverage and Medicare
Please read this notice carefully and keep it where you can find it. This notice has information about your current prescription drug coverage with the City of Georgetown and about your options under Medicare’s prescription drug coverage. This information can help you decide whether or not you want to join a Medicare drug plan. If you are considering joining, you should compare your current coverage, including which drugs are covered at what cost, with the coverage and costs of the plans offering Medicare prescription drug coverage in your area. Information about where you can get help to make decisions about your prescription drug coverage is at the end of this notice.
There are two important things you need to know about your current coverage and Medicare’s prescription drug
coverage:
1. Medicare prescription drug coverage became available in 2006 to everyone with Medicare. You can get this
coverage if you join a Medicare Prescription Drug Plan or join a Medicare Advantage Plan (like an HMO or
PPO) that offers prescription drug coverage. All Medicare drug plans provide at least a standard level of
coverage set by Medicare. Some plans may also offer more coverage for a higher monthly premium.
2. The City of Georgetown has determined that the prescription drug coverage offered by the company’s
Medical Plans are, on average for all plan participants, expected to pay out as much as standard Medicare
prescription drug coverage pays and is therefore considered Creditable Coverage. Because your existing
coverage is Creditable Coverage, you can keep this coverage and not pay a higher premium (a penalty) if
you later decide to join a Medicare drug plan.
When Can You Join A Medicare Drug Plan?
You can join a Medicare drug plan when you first become eligible for Medicare and each year from October 15th to
December 7th.
However, if you lose your current creditable prescription drug coverage, through no fault of your own, you will also be
eligible for a two (2) month Special Enrollment Period (SEP) to join a Medicare drug plan.
What Happens To Your Current Coverage If You Decide to Join A Medicare Drug Plan?
If you decide to join a Medicare drug plan, your current the City of Georgetown coverage will not be affected. Your
current coverage pays for other health expenses in addition to prescription drug.
If you enroll in a Medicare prescription drug plan, you and your eligible dependents will be eligible to receive all of your
current health and prescription drug benefits and your coverage will coordinate with Medicare.
If you do decide to join a Medicare drug plan and drop your current City of Georgetown coverage, be aware that you and
your dependents may not be able to get this coverage back.
CMS Form 10182-CC Updated April 1, 2011
According to the Paperwork Reduction Act of 1995, no persons are required to respond to a collection of information unless it displays a valid OMB control
number. The valid OMB control number for this information collection is 0938-0990. The time required to complete this information collection is estimated to
average 8 hours per response initially, including the time to review instructions, search existing data resources, gather the data needed, and complete and
review the information collection. If you have comments concerning the accuracy of the time estimates or suggestions for improving this form, please write
to: CMS, 7500 Security Boulevard, Attn: PRA Reports Clearance Officer, Mail Stop C4-26-05, Baltimore, Maryland 21244-1850.

40 | Page
Medicare D Notice
When Will You Pay A Higher Premium (Penalty) To Join A Medicare Drug Plan?
You should also know that if you drop or lose your current coverage with City of Georgetown and don’t join a Medicare
drug plan within 63 continuous days after your current coverage ends, you may pay a higher premium (a penalty) to join
a Medicare drug plan later.
If you go 63 continuous days or longer without creditable prescription drug coverage, your monthly premium may go up
by at least 1% of the Medicare base beneficiary premium per month for every month that you did not have that coverage.
For example, if you go nineteen months without creditable coverage, your premium may consistently be at least 19%
higher than the Medicare base beneficiary premium. You may have to pay this higher premium (a penalty) as long as you
have Medicare prescription drug coverage. In addition, you may have to wait until the following October to join.
For More Information About This Notice Or Your Current Prescription Drug Coverage
Contact the Human Resources department for further information. NOTE: You’ll get this notice each year. You will also
get it before the next period you can join a Medicare drug plan, and if this coverage through City of Georgetown changes.
You also may request a copy of this notice at any time.
For More Information About Your Options Under Medicare Prescription Drug Coverage
More detailed information about Medicare plans that offer prescription drug coverage is in the “Medicare & You”
handbook. You’ll get a copy of the handbook in the mail every year from Medicare. You may also be contacted directly by
Medicare drug plans.
For more information about Medicare prescription drug coverage:
Visit www.medicare.gov
Call your State Health Insurance Assistance Program (see the inside back cover of your copy of the “Medicare & You” handbook for their telephone number) for personalized help
Call 1-800-MEDICARE (1-800-633-4227). TTY users should call 1-877-486-2048.
If you have limited income and resources, extra help paying for Medicare prescription drug coverage is available. For
information about this extra help, visit Social Security on the web at www.socialsecurity.gov, or call them at 1-800-772-
1213 (TTY 1-800-325-0778).
CMS Form 10182-CC Updated April 1, 2011
According to the Paperwork Reduction Act of 1995, no persons are required to respond to a collection of information unless it displays a valid OMB control
number. The valid OMB control number for this information collection is 0938-0990. The time required to complete this information collection is estimated
to average 8 hours per response initially, including the time to review instructions, search existing data resources, gather the data needed, and complete and
review the information collection. If you have comments concerning the accuracy of the time estimates or suggestions for improving this form, please write
to: CMS, 7500 Security Boulevard, Attn: PRA Reports Clearance Officer, Mail Stop C4-26-05, Baltimore, Maryland 21244-1850.
Remember: Keep this Creditable Coverage notice. If you decide to join one of the Medicare
drug plans, you may be required to provide a copy of this notice when you join to show
whether or not you have maintained creditable coverage and, therefore, whether or not you
are required to pay a higher premium (a penalty).
Date January 1, 2017 - December 31, 2017
Name of Entity/Sender City of Georgetown
Contact Office Human Resources Department
Address 113 E. 8th Street, Georgetown, Texas 78626
Phone Number (512) 930-3691


41 | Page
4411 South IH-35, Suite 105 Georgetown, Texas 78626
(512) 930-7700 Phone (512) 930-7701 Fax www.ajg.com