2018.09.18. budapest semmelweis university
TRANSCRIPT
Palpation2018.09.18.
Budapest
Semmelweis University

The Posterior Chest
• General approach
Undress to the waist
Sitting position
Inspect – palpate –percuss – auscultate
Compare one side with other
apex and base

The Posterior/Lateral Chest

The Posterior Chest
• Identification of tender areas
intercostal tenderness → inflamed pleura
• Assessment of observed abnormalities
shape of the chest
deformities
asymmetry
masses

The Posterior Chest

The Posterior Chest
• Assessment of respiratory expansion
unilateral diminution
pleural effusion
lobar pneumonia

The Posterior Chest
• Tactile fremitus
Patient says: 99 or 1-1-1 (hungarian 66 =hatvanhat)
palpable vibrations
bronchopulmonary system→chest wall
comparison of symmetrical areas
increased→lobar pneumonia
alveoli filled with fluid,
RBC,WBS→transmission ↑
decreased→ fluid in the pleural cavity = pleural effusion
air, ptx = pneumothorax



The Anterior Chest
• Supine position
• Identification of tender areas
• Assessment of observed abnormalities
respiratory expansion
tactile fremitus
both sides of the chest
Identification of a fractured rib
local pain, tenderness
a-p compression sternum – thoracic spine
increase in local pain


The Arterial Pulse
- radial pulse
- heart rate
- rhythm
- regular
- irregular
atrial fibrillation
premature contraction

The Arterial Pulse
amplitude and contour
carotid artery
decreased pulsation
atherosclerotic occlusion
do not press on both carotids
carotid sinus
amplitude ≈ pulse pressure
small, weak
large, bouding
thrills
vibrations of the carotid artery
arterial narrowing


The Heart
supine position
use your fingerpads
patient→ exhale fully and stop breathing


The Heart
• Apical impulse
undetectable
obesity
muscular chest wall
located behind the rib cage
displaced
left ventricular enlargement
deformities of the thorax
mediasinal shift

The Heart
• Apical impulseincresed amplitude
hyperkinetic states
young persons
hyperthyroidism
severe anemia
AS
prolonged duration
hypertrophy of the left ventricule
Thrills
loud heart murmurs
AS
VSD
MS

The Abdomen• Quadrants, sections
• General approach
relaxed patient
legs flexed et hips and knees
supine position
patient´s right side
arms at the sides of the trunk
warm hands, short fingernails
watch patient´s face for signs of discomfort
• Normal structures palpable
sigmoid colon
normal liver
lower pole of the right kidney
pulsation of the abdominal aorta
distended bladder
tip of the normal spleen



The Abdomen• Light palpation
abdominal tenderness
muscular resistance
voluntary
involunntary muscula pasm
superficial organs
masses
• Deep palpation
masses→ location, size, shape, consistency, tenderness, pulsations, mobility
• Assessment of peritoneal irritation
muscular spasm
abdominal pain on coughing and on ligh percussion
tenderness
inflammation of the parietal peritoneum
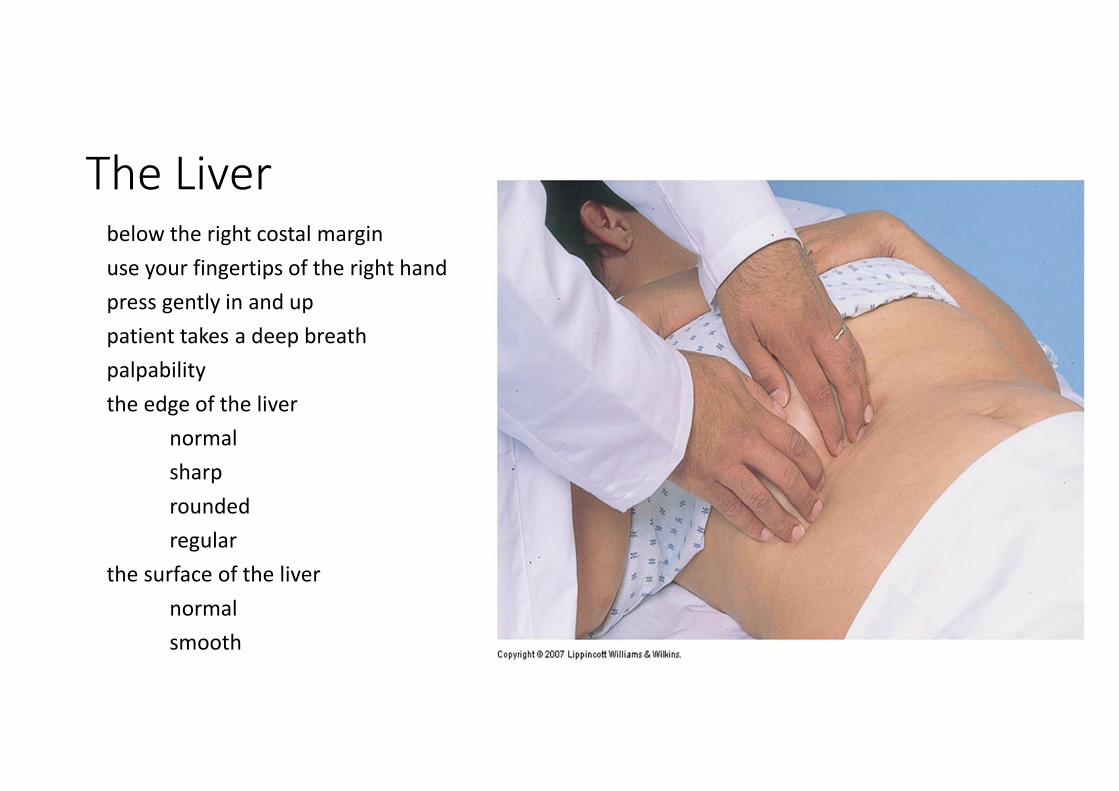
The Liverbelow the right costal margin
use your fingertips of the right hand
press gently in and up
patient takes a deep breath
palpability
the edge of the liver
normal
sharp
rounded
regular
the surface of the liver
normal
smooth

The Liver

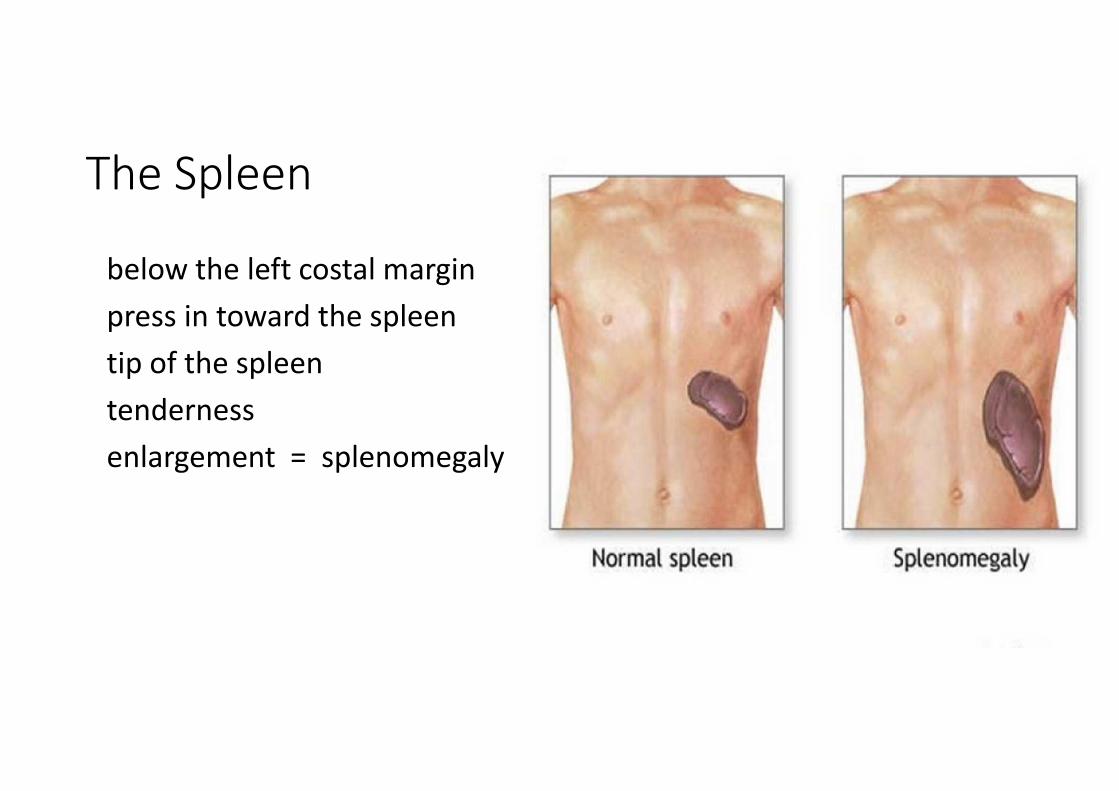
The Spleen
below the left costal margin
press in toward the spleen
tip of the spleen
tenderness
enlargement = splenomegaly

The Kidneys
• Right kidney
left hand → costovertebral angle
right hand → right upper quadrant
patient takes a deep breath
maybe palpable the lower pole
enlargement→ tumor, hydronephrosis
(pelvis of the kidney)
left kidney → rarely palpable
kidney tendeness
fist percussion at the costovertebral
angle → kidney infection

The Aorta
deep palpation
upper abdomen
aortic pulsations
abdominal mass with pulsations →
→ aortic aneurysm

The Neck• Lymph nodes
fingerpads
both sides
occipital, preaurical, submandibular,
cervical, supraclavicular
size, shape, discrete or grouped, together, mobility, consistency, tenderness
Normal person → small, mobile, discrete, nontender
Enlarged → lymph nodes elsewhere → regional, generalized

The Thyroid gland
palpate behind the patient
just below the cricoid cartilage
patient swallows
thyroid isthmus rises
feel the isthmus and the lateral lobes
size, shape, consistency, nodules, tenderness
goiter = diffusely enlarged thyroid

The Breasts
Quadrants → upper inner, lower inner, upper outer, lower outer
tenderness
nodules = lumps = masses
location, size in cm, shape, consistency (soft or hard), mobility tothe skin and
underlying chest wall
cancer → hard, irregular, poorly circumscribed nodule, fixed to theskin
discharge of the nipple → milky, bloody



The Axillae
sitting position
normal person → small, nontender nodes
enlarged lymph nodes → hard→ breast cancer or tender � infection

The Anus, Rectum, and Prostate
• Rectal examination
side-lying position
glove, lubricant
perianal area → hemorrhoids, perianal abscess
rectum → carcinoma
anterior surface of the prostate gland
- both lobes
- size, shape, nodules, tenderness
normal → rubbery, nontender, rounded,
2.5 cm in length
- cancer → hard
- BPH (benign prostatic hyperplasia) → 5th decade,
-symmetric enlargement, smooth, obstruction of urinary flow

The Peripheral Vascular Systemsupine position
both legs
swelling
symmetry
size
venous enlargement
ulcers
femoral artery → below the inguinal ligament
popliteal artery → in the tissues behind the knee
dorsalis pedis artery → the dorsum of the foot
posterior tibial artery → behind the medial malleolus of ankle
arterial pulsation
look for edema
ankle, dorsum of the foot
pitting → depression by pressure
severity → light, very marked
swelling → unilateral, bilateral

Percussion

Technique
the pleximeter finger:
hyperextension of the middle finger of the left hand
its DIP joint press firmly
avoid contact by other part of the hand →
→ decrease of vibrations
the plexor finger
right middle finger→ partially flexed
tip of the plexor finger strikes the pleximeter finger

Technique
Technique
transmission of vibrations → through the bones of DIP joint → tothe underlying chest wall
movement of the wrist
thick chest wall → heavier percussion
strike 2x in 1 location
percussion → audible sounds ← motion of the chest wall

Technique
underlying tissues
air-filled
fluid-filled
solid
penetraCon → 5-7cm into the chest
deep-seated lesions → undetected


Medical percussion sounds
• NORMAL PERCUSSION SOUNDS
• Resonance: heard over lung tissue
• Tympany: heard over most portions of the abdominal cavity
• Dullness: heard over solid organs (eg, liver) and muscles
• ABNORMAL PERCUSSION SOUNDS
• Lung: dullness, which may be produced by pneumonia,
• tumor, infarction, or fluid collection;
• hyperresonance or even tympany, which may result from confluent air collection, as seen inpneumothorax or emphysema
• Abdomen: dullness, which may be produced by intra-abdominal tumors or masses; shifting dullness may indicate presence of ascites
• Heart: an expanded area of dullness may indicatecardiomegaly or pericardial effusion


The Posterior ChestPercussion → compare one side with other
symmetrical areas
sitting position
undress to the waist
apex → base
omit the scapular areas ← thick musculosceletal structures
normal lung percussion → resonance →
→ intensity: loud, pitch: low, duration: long
emphysema (lungs are hyperinflated) percussion →
→diffuse hyperresonance
→ intensity: very loud, pitch: lower, duration: longer

The Posterior Chest
Abnormal dullness
fluid in the pleural space = pleural effusion
hemothorax (blood), empyema (pus)
solid tissue in the lung → lobar pneumonia
alveoli filled with fluid, RBC, WBC
Unilateral hyperresonance
large air-filled bulla in the lung or large amount of air in thepleural space

The Posterior Chest
• Identification of the level of diaphagmaticdullnes
percussion: apex → base
resonance→ dullness = diaphragm
abnormally high level→ diaphragmaticparalysis
• Diaphragmatic excursion
distance between levels of dullness
on full exspiration
on full inspiration
5-6 cm

Summary• Normal case:
percussion note → resonant
tactile fremitus → normal
• Lobar pneumonia (bacterial infection, alveoli filled)
percussion note → dull over the airless area
tactile fremitus → increased
• Pleural effusion (fluid accumulates and separates the ai-filled lung from the chestwall and blocks the transmission of the sound)
percussion note → dull over the fluid
tactile fremitus → decreased

The Posterior Chest
• Ptx
air in the pleural space → blocks the transmission of the sounds
percussion note → hyperresonant or tympanic over the pleural air
tactile fremitus → decreased or absent over the pleural air


The Anterior Chest
supine position
compare both sides
dullness behind the right breast → right middle lobe pneumonia
identification of the upper border of liver dullness

The Heart
supine position
estimation of cardiac size
percussion: lung resonance → cardiac dullness
percuss for the right, left and upper border
leF border → LV
right border → RA



The Abdomen
relaxed patient
supine position
full exposure
warm hands
stand on patient´s right side

The Abdomen
• Orientation
4 quadrants
tympany predominates → gastric air bubble, gas in the GI tract
dullnes → each side solid structures(liver, spleen)
suprapubic area → distended bladder, enlarged uterus

Traube's spaceTraube's spaceTraube's spaceTraube's space
• Anatomical boundaries are:
1. Right : Lateral margin of left lobe of liver.2. Left : Spleen.3. Superior : Resonance of lung.4. Inferior : Costal margin.
Contents
1. Fundus of stomach (Hence percussion of Traubes area normally gives Tympanitic resonance).2. Costo-phrenic recess of left pleura devoid of lungs.
Causes of obliteration of Traubes space:1. Full stomach.2. Left sided Pleural effusion.3.Splenomegaly.4. Enlargment ofleft lobe of liver due to any etiology.5. Dextrocardia.6. Proloiferative growth in fundus of stomach.


The Liver
liver dullness
vertical span = height
in cm
in the right midclavicular line
lung resonance → upper border of liver dullness
tympany → lower border of liver dullness
increased span → enlarged liver=hepatomegaly
decreased span → small liver
liver dullness disappears → free air present below the diaphragm → signof perforation



The Spleen
posterior to the midaxillary line
splenic dullness → oval area
surroundings
pulmonary resonance
abdominal tympany
enlarged spleen = splenomegaly
→ large dull area


Ascites
protuberant abdomen
ascites fluid → sinks with the gravity
percussion → dullness outward → central tympanic area
shifting dullnes
paCent turns onto one side → dullness shifts
fluid wave
impulse transmitted through the fluid
