2121 k street, nw, suite 210 washington, dc 20006 center for integrated behavioral health policy...
TRANSCRIPT

2121 K Street, NW, Suite 210Washington, DC 20006
Center for Integrated Behavioral Health Policy
Department of Health Policy, George Washington University Medical Center

Implementing Alcohol Screening and Brief
Intervention in Your EAP
Chesapeake EAPAJanuary 6, 2011
Eric Goplerud PhDTracy L. McPherson, PhD

Presenters Eric Goplerud, PhD
Research Professor and DirectorCenter for Integrated Behavioral Health PolicyEnsuring Solutions to Alcohol ProblemsDepartment of Health PolicyGeorge Washington University Medical CenterWashington, [email protected]
Tracy L. McPherson, PhDAssistant Research Professor
Center for Integrated Behavioral Health PolicyEnsuring Solutions to Alcohol ProblemsDepartment of Health PolicyGeorge Washington University Medical CenterWashington, [email protected]

Learn about and receive a copy of the World Health Organization’s AUDIT-C/AUDIT – a brief, validated alcohol screening tools that can be integrated into routine EAP practice to identify risky alcohol use.
Learn to relate appropriate levels of brief intervention to level of alcohol use risk.
Today’s Objectives:
Learn to use SBIRT protocols informed by Motivational Interviewing (MI) to assist clients in behavioral change.
Learn about NIAAA’s alcohol education and self-management resources (e.g., “Rethinking Drinking”) for clients.
Today’s Objectives:

Learn about the “BIG” Initiative EAP learning collaborative and how you can benefit
Learn about (and take-away) “BIG” materials and resources to help you integrate alcohol SBIRT in your EAP practice.
Learn about research findings and implementation tips from EAP pilot tests.
Bonus Elements:
Agenda
Background and Rationale Workplace SBIRT Project The BIG Initiative
What is SBIRT?Alcohol Screening ToolsComponents of Brief InterventionMotivational Interviewing StrategiesSBIRT Protocols Using AUDIT (with/without MI)

Bonus Elements
Implementation Tips from PilotsEAP Pilot Test FindingsMore “BIG” ResourcesDemonstrating Impact and Value
Easy-to-Use Outcome Measures
Seed Funding: NHTSA CSAT SAMHSA NETS Alkermes
Corporate Sponsors
Pilot Sites: Aetna OptumHealth ValueOptions
Trainer: Denise Ernst PhD, Training and
Consultation http://www.deniseernst.com
Workplace Alcohol SBI Project Partners: The BIG Initiative

Overall Aim:
Adapt alcohol SBIRT approaches developed in medical settings for work-related settings:
EAP Occupational health & safety Health promotion and wellness Disease management
NHTSA/CSAT Workplace SBI Project (2006-2010)

Conducted extensive literature review, surveys, interviews, convened advisory panel.
Developed a conceptual model (a feasible approach) of workplace SBI.
cont…
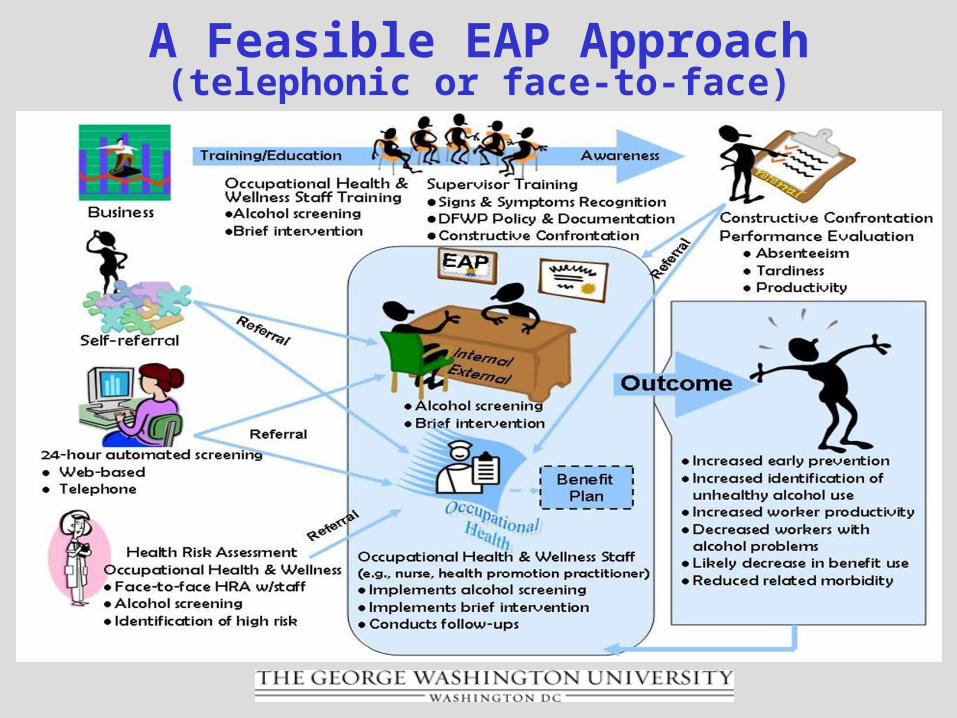
A Feasible EAP Approach(telephonic or face-to-face)
Developed protocols that could be seamlessly integrated into existing EAP practice.
Conducted “proof of concept” studies to pilot test approaches and protocols in EAPs.
Launched “BIG Initiative” to facilitate EAP adoption of alcohol SBIRT through dissemination of materials and pilot test findings, and training.
cont…
EAP industry-wide initiative kicked-off in Dallas at EAPA to adopt alcohol SBIRT as routine practice by 2011.
Learning collaborative facilitated by GW which brings together 80+ organizations in the SBIRT “supply chain”.
What is “BIG”?

EAPs/MBHOs
Employers
Professional Associations
Clinicians
SBIRT/MI Experts
Researchers and Consultants
Pharmaceutical Companies
Federal Agencies
“BIG” Members
National Highway Traffic Safety AdministrationSubstance Abuse and Mental Health Services AdministrationNetwork of Employers for Traffic SafetyAetna Behavioral Health/EAPOptumHealth/UBHValueOptionsOffice of Drug and Alcohol Policy and Compliance, Department
of Labor Office of Demand Reduction, Office of National Drug Control
Policy, Executive Office of the PresidentU.S. Nuclear Regulatory CommissionDepartment of DefenseMaine State Government Federal Occupational Health (FOH)University of Maryland School of Social Work Chestnut Behavioral HealthFirst Sun EAPSELECT, IncCIGNAMagellanAnthem/WellPointMasi ConsultingBurke Consulting
Caterpillar Northrup Grumman Johns Hopkins University and Hospital JP Morgan ChaseHawaii Business Health CouncilNational Business Group on HealthUPSAmtrakContinental Airlines RAND CorporationBaltimore Gas & ElectricHalliburton 3MEAPAEASNACenter for Clinical Social WorkNAADACAssociation of Flight AttendantsAONSt John’s MercyFirst AdvantageThe Rainier GroupReckitt-Benckiser
Brief Intervention Group (“BIG”)

Four Committees
Board of Directors – thought leaders, industry decision-makers provide direction of BIG strategy
Clinical – change EAP provider and network affiliate practice
Systems and Operations – change call center and internal EAP practice
Quality Improvement – identify common metrics (program performance, client outcomes)
What does “BIG” do?

www.EAPBIG.org
FREE SBIRT Training Materials and Resources
Connect with BIG members on LinkedIn
Earn CE/PDHs by participating in BIG events
EAPA chapter meetings; regional and national conference events
EASNA annual meeting
How can you benefit from “BIG”?
Heavy drinking (5+ drinks on one occasion) increases risk of depression, sleep problems, hypertension, and cancer
3 in 10 adults drink at levels that increase risk of physical, mental health, and social problems (NIAAA)
So…Why Should EAP Providers Care About Alcohol SBIRT and
BIG?

Alcohol Problems Nearly as Prevalent as Diabetes
Alcohol Abuse & Dependence
Diabetes
17.6 million1
18.2 million2
A
References:
1. Grant BF, et al. Alcohol Res. and Health. 2006; 29:77.
2. National Center for Chronic Disease and Prevention and Health Promotion. National Diabetes Fact Sheet. http://www.cdc.gov/diabetes/pubs/estimates.htm. Accessed June 25, 2008.

How Many Get identified?
~ 8% of U.S. adults has a diagnosable alcohol use disorder (NSDUH, 2005)
92%
8%

How Many Get Identified?
Health plans identify <1% of members (NCQA, 2007)

Office of Applied Studies. (2004). Results from the 2003 National Survey on Drug Use and Health: National findings. Rockville, MD: Substance Abuse and Mental Health Services Administration.

Alcohol problems have a profound impact on the workplace, its employees and their families:
80% of problem drinkers are employed
60% of alcohol-related absenteeism, tardiness, and poor work quality are caused by at-risk drinkers
20% of employees have covered for a coworker, required to work harder, or injured due to coworkers drinking
more reasons…
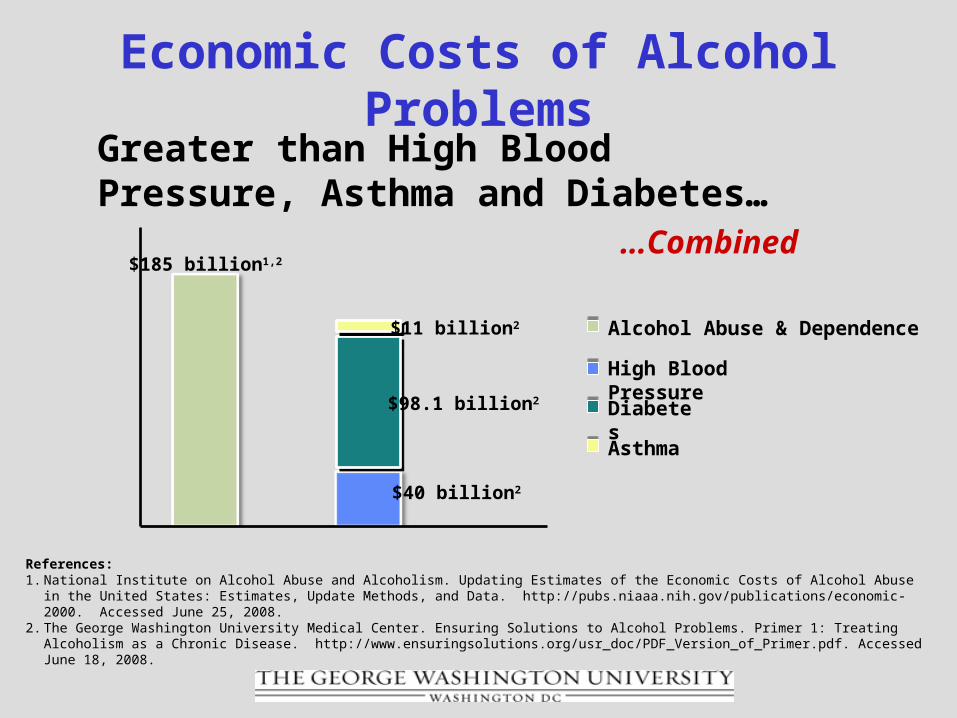
Economic Costs of Alcohol Problems
Greater than High Blood Pressure, Asthma and Diabetes…
…Combined$185 billion1,2
$40 billion2
$11 billion2
$98.1 billion2
Alcohol Abuse & Dependence
High Blood Pressure
Asthma
Diabetes
References:1. National Institute on Alcohol Abuse and Alcoholism. Updating Estimates of the Economic Costs of Alcohol Abuse in the United
States: Estimates, Update Methods, and Data. http://pubs.niaaa.nih.gov/publications/economic-2000. Accessed June 25, 2008.2. The George Washington University Medical Center. Ensuring Solutions to Alcohol Problems. Primer 1: Treating Alcoholism as a
Chronic Disease. http://www.ensuringsolutions.org/usr_doc/PDF_Version_of_Primer.pdf. Accessed June 18, 2008.
EAPs play a vital role to employers and workers
Millions of workers rely on EAP for confidential help for mental health, substance use, work stress and family issues.
Employers see EAP as a crucial resource.
EAPs are uniquely positioned to “case find” (alcohol misuse is not a common presenting problem).
more reasons…
Brief, evidence-based approaches exist for EAP providers to enhance existing practice and increase value of services.
“BIG” provides EAP providers with materials and resources to do SBIRT.
Making the right thing to do, the easy thing to do.
More reasons…

Alcohol identification rates by EAP providers remain abysmal!
~ 160,000 EAP alcohol cases each year (Amaral 2009)
Baseline identification <1 to 5% (GW pilot studies)
Historically EAP providers have focused on workers with alcohol addiction.
EAP providers have not focused on early intervention to identify at-risk drinkers but don’t meet diagnostic criteria.
“BIG” Challenges
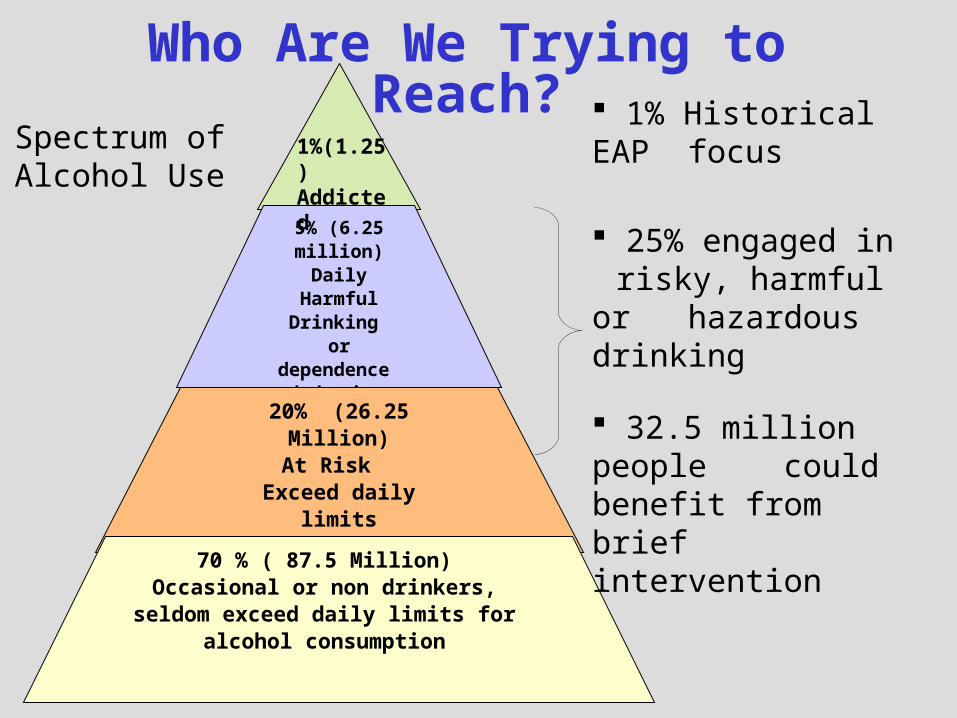
Who Are We Trying to Reach?
5% (6.25 million)
Daily HarmfulDrinking or dependence
behavior
20% (26.25 Million)At Risk
Exceed daily limits
70 % ( 87.5 Million)Occasional or non drinkers, seldom
exceed daily limits for alcohol consumption
1% Historical EAP focus
25% engaged in risky, harmful or hazardous drinking
32.5 million people could benefit from brief intervention
1%(1.25)Addicted
Spectrum ofAlcohol Use
How do we identify workers at risk?
“Case Finding” through SBIRT
What is SBIRT?
S: Screening using a validated tool
BI: Brief Intervention using an evidence-based framework
RT: Referral to Treatment
SBIRT: Screening, Brief Intervention and Referral to Treatment
Follow-up: administrative, clinical, outcomes
MI: Motivational Interviewing
Approach developed in the medical setting (trauma, ED), backed by scientific evidence of effectiveness.
Recent efforts to adapt for EAP and other behavioral settings (e.g., community health centers).
What is SBIRT?

Increase early identification of clients at risk for alcohol problems.
Build awareness and educate clients on U.S. guidelines and risks associated with alcohol use.
Motivate at-risk clients to reduce unhealthy, risky alcohol use; adopt health promoting practices.
Motivate clients to seek help for alcohol use.
Aim of SBIRT

http://pubs.niaaa.nih.gov/publications/arh28-1/toc28-
1.htm
http://pubs.niaaa.nih.gov/publications/arh28-2/toc28-
2.htm
Evidence behind SBIRT

Identification Rates at 5 months approached U.S. population estimates
18.5% using AUDIT screening tool
6% based on “presenting problem”
At baseline: < 1% (prior vendor data)
Aetna Pilot Findings
McPherson, T.L., Goplerud, E., Derr, D., Mickenberg, J., Courtemanche, S. (in press, 2010). Telephonic Screening and Brief Intervention for Alcohol Misuse Among Workers Contacting the Employee Assistance Program: A Feasibility Study. Drug and Alcohol Review.
78% agreement to follow-up by EAP clinician
72% set an appointment for face-to-face counseling
Findings at 5 Months
McPherson, T.L., Goplerud, E., Derr, D., Mickenberg, J., Courtemanche, S. (in press, 2010). Telephonic Screening and Brief Intervention for Alcohol Misuse Among Workers Contacting the Employee Assistance Program: A Feasibility Study. Drug and Alcohol Review.

Pre-SBI
Time Period(n=68
1)
Post-SBI Time
Period(n=383
)
p-value
EAP Alcohol Identification
Hazardous alcohol use
7.5% (51)
20.1% (77)
<0.0001
Alcohol abuse/dependence
7.1% (48)
10.4% (40)
0.0536
OptumHealth EAPReplicated Findings
Greenwood, G., Goplerud, E., McPherson, T.L., Azocar, F., Baker, E., & Dybdahl, S. (in press, 2010). Alcohol Screening & Brief Intervention (SBI) in Telephonic EAP. Journal of Workplace Behavioral Health.
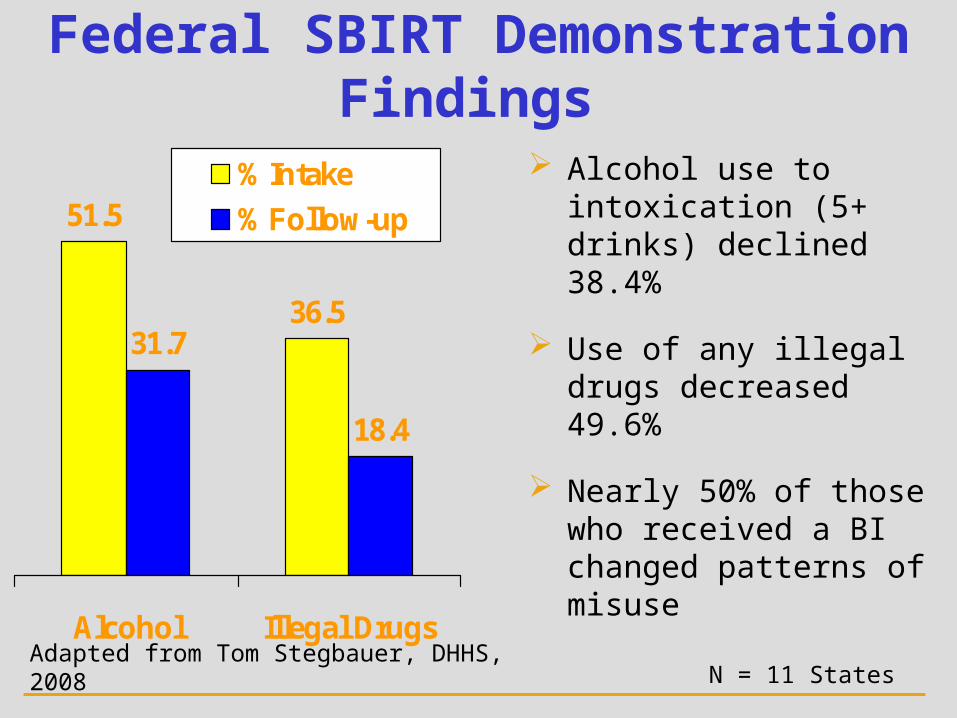
51.5
36.531.7
18.4
Alcohol Illegal Drugs
% Intake
% Follow-up
Alcohol use to intoxication (5+ drinks) declined 38.4%
Use of any illegal drugs decreased 49.6%
Nearly 50% of those who received a BI changed patterns of misuse
N = 11 States
Federal SBIRT DemonstrationFindings
Adapted from Tom Stegbauer, DHHS, 2008

QUESTIONS?
Components ofSBIRT

SBIRT Core Components
ScreeningIdentification of
behavioral problems/risk
(alcohol, tobacco,drugs,
depression)
Brief InterventionRaises awareness
of risks and reinforces staying
at low risk
Referral to TX Referral of those with
more serious or complicated mental or substance use
conditions
Brief Intervention/ Brief Treatment
Cognitive behavioral, medications with
clients who acknowledge risks
and are seeking help
High
Moderate
Low
Adapted from Tom Stegbauer, DHHS, 2008

Heterogeneity of Alcohol Use
Never exceedsdaily limits
•Exceedsdaily limits
•No distressor harm
•Exceedsdaily limits
•Harmful
•Daily or neardaily heavydrinking
•Impairedcontrol
•3-5 criteria
•Daily or neardaily heavydrinking
•Chronic orrelapsing
•6-7 criteria•Functionalimpairment
None Mild(“At-risk”)
Moderate(Harmful use)
Severe(Dependence)
Chronicdependence
70% ~21% ~5% ~3% ~1%
DSM-IV Abuse/Dependence
EAP and Workplace BH Programs

NIDA Single-Item Drug Use
"How many times in the past year have you used an illegal drug or used a
prescription medication for non-medical reasons?”
Identifies overall drug usePositive screen = 1 or moreProvide BI /RT
Barclay, Laurie (2010). Single Screening Question May Identify Drug Use in Primary
Care. Arch Intern Med. 2010;170:1155-1160
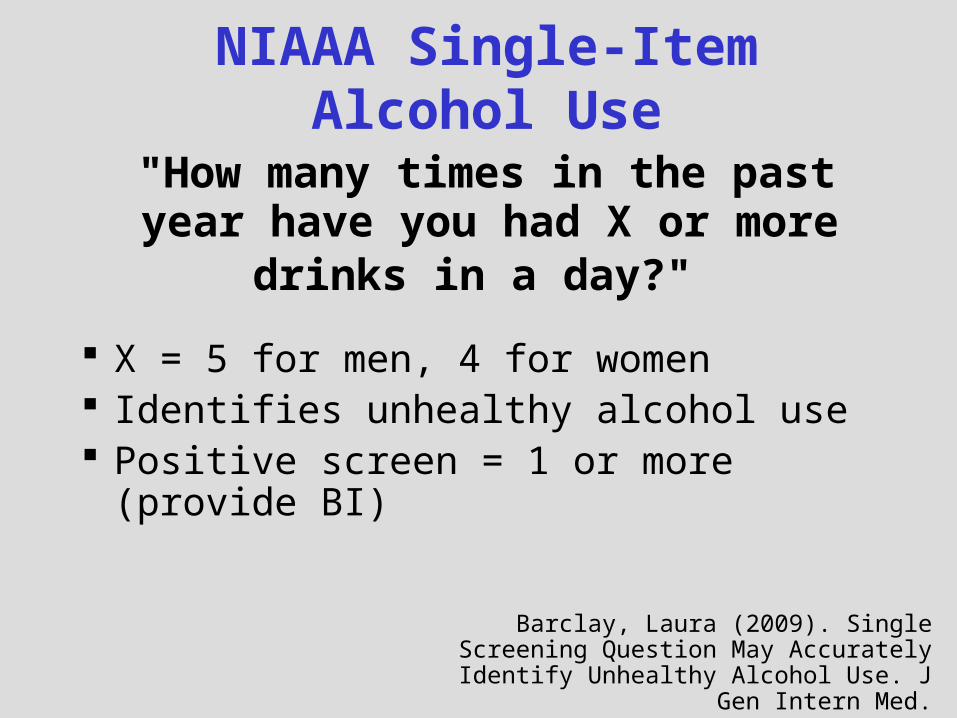
NIAAA Single-Item Alcohol Use
"How many times in the past year have you had X or more
drinks in a day?"
X = 5 for men, 4 for women Identifies unhealthy alcohol use Positive screen = 1 or more (provide
BI)
Barclay, Laura (2009). Single Screening Question May Accurately Identify
Unhealthy Alcohol Use. J Gen Intern Med.

Alcohol Screening(handout)
AUDIT-C
AUDIT


4747
AUDITAlcohol Use Disorder Alcohol Use Disorder
Identification TestIdentification Test
Developed by WHODeveloped by WHOEnglish:http://whqlibdoc.who.int/
hq/2001/WHO_MSD_MSB_01.6a.pdf
Spanish:http://www.who.int/substance_abuse/activities/en/
AUDITmanualSpanish.pdf
Detects Alcohol Detects Alcohol Problems in the Last Problems in the Last
YearYear
AUDIT-C <2 minAUDIT-C <2 minAUDIT <5 minAUDIT <5 min

AUDIT Domains

AUDIT-C Hazardous Use (AUDIT Items
1-3)
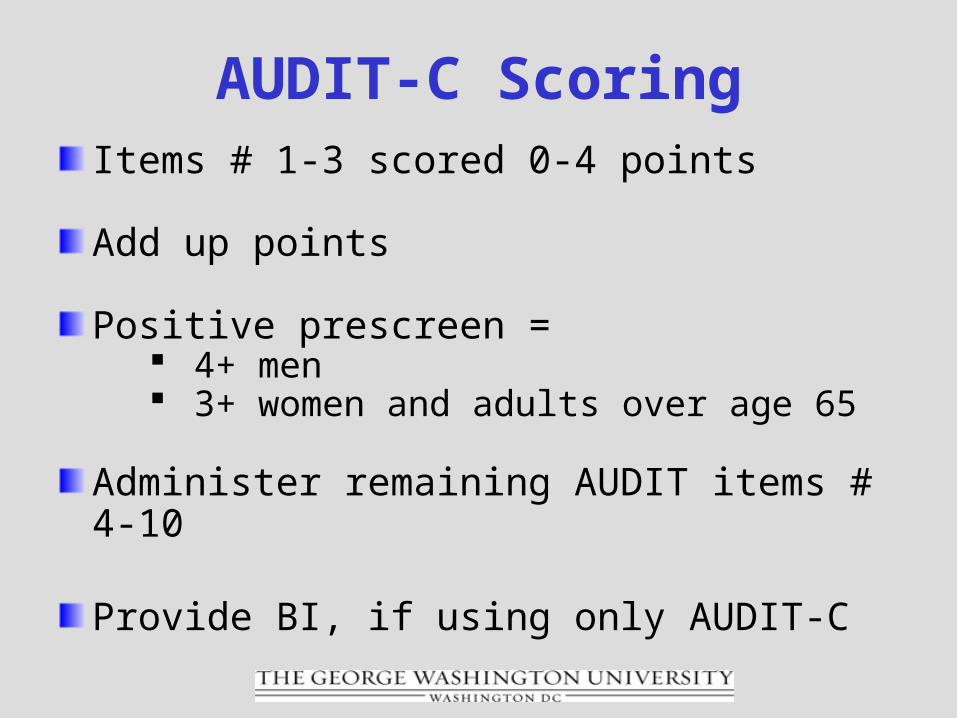
AUDIT-C ScoringItems # 1-3 scored 0-4 points
Add up points
Positive prescreen = 4+ men 3+ women and adults over age 65
Administer remaining AUDIT items # 4-10
Provide BI, if using only AUDIT-C

Dependence Symptoms (Items 4-6)

Harmful Use (Items 7-10)
AUDIT Scoring
Add up points Items # 1-8 scored 0-4 points Items 9-10 scored 0, 2 or 4 points
8+ indicates at-risk, harmful or hazardous drinking

World Health Organization (WHO) Recommended
Levels of Brief Intervention (4 Zones)
Adaptations of WHO for EAP
3 Risk Level Intervention
AUDIT InterpretationLevels of Brief Intervention

WHO

“BIG” Adapted – 3 levels

AUDIT Online

http://rethinkingdrinking.niaaa.nih.gov/

http://rethinkingdrinking.niaaa.nih.gov/
QUESTIONS?

What is Brief Intervention?

….IT’S NOT THIS!

BI: Definition & Implications
Short, non-confrontational health counseling technique.
A practice to identify a real or potential alcohol use problem, and
to motivate an individual to do something about it.
Effective with other conditions (e.g., tobacco and drug use, depression, diabetes).

BI: Definition & Implications
Not a quick fix treatment.
Persons with addiction or a mental health disorder require specialist care or other treatment modalities beyond BI.
May help identify persons with a disorder and facilitate referral.
Elements of BI Screening score feedback Education (risks, guidelines) Normative feedback Simple advice Enhance motivation Assist with action plan Give encouragement Provide resources Close on good terms Ask for permission Provide Referral
Screening Score Feedback
Low risk
“From your responses, your drinking is in a healthy range which puts you at lower risk for many health and emotional concerns than those who drink at higher ranges.”
Screening Score Feedback
Moderate and High Risk
"From your responses, your drinking puts you at higher risk for many health and emotional concerns than those who drink at lower ranges. These questions have been given to thousands of people, so you can compare your drinking to others. Your score was [#]…on a scale of 0-40 which places you in the category of [moderate or high] risk.

Education
Discuss health risks of alcohol and other substances
“Unhealthy alcohol use can put you at risk for injury, accidents, and health problems such as depression, diabetes, cancer, insomnia, high blood pressure, stroke, heart and gastrointestinal problems, and other conditions.”
Education
Review drinking guidelines
“The recommended guidelines for healthy adults are no more than 1 drink per day (or 7 drinks per week) for women and adults over age 65, and no more than 2 drinks per day (or 14 drinks per week) for men.”

Normative Feedback
Provide feedback on how client’s use compares to others (i.e., men, women, adolescents, general population)
“Your alcohol consumption is similar to [different from/higher than] most people (about 72% of adults) in the U.S. who never exceed the recommended guidelines.”
“Reducing your consumption to safer drinking levels can decrease your risk.”
“Cutting back on the number of drinks you typically have each day can decrease your risk of health problems.”
“I advise you to Cut Back your alcohol consumption.”
Simple Advice
“Cut Back”/Moderation
Recommend drinking or using at “moderate levels” which are safe/within guidelines.
Not a request to Abstain/STOP.Alcohol: (m) 2-14-5, (w) 1-7-4
(Adapted from NIAAA, 10th Report to Congress 2000)
“Based on my assessment, you are at-risk for future health problems…I advise you to cut back/quit.”
Non-judgmental feedback and appraisal of risks by a practitioner….
10-30% patients will significantly reduce (alcohol/tobacco/diabetic) risky
behavior.(WHO, 1996; CSAT TIP 24, 1997)
Non-Judgmental Tone
Exploring Motivation using MI Strategies
Explore Ambivalence Pros and Cons of Alcohol Use
Explore Readiness Importance and Confidence Rulers
Explore Goals quit, cut down, make no change?
Elicit Change Talk – Use your OARS “I really want to cut-back on drinking with
the guys after work.”
Using Your OARS
O = Open Questions
A = Affirmations
R = Reflections
S = Summary
Source: Mary Velasquez, HOT EAPA Motivational Interviewing Training, September 1, 2010
What are the good things about your ____?
What are some of the less good things?
What concerns do you have about your ____?
If you were to change, what would it be like?
Where does this leave you now?
Source: Mary Velasquez, HOT EAPA Motivational Interviewing Training, September 1, 2010
Exploring Pros/Cons

0 10
Importance Ruler
“How important is it to you to ____ ( e.g., quit using, begin treatment)?
If 0 was “not important,” and 10 was “very important,” what number would
you give yourself ?”
Source: Mary Velasquez, HOT EAPA Motivational Interviewing Training, September 1, 2010
Exploring Importance
Why are you at x and not y? (always start with the higher number)
What would have to happen for it to become much more important for you to change?
Source: Mary Velasquez, HOT EAPA Motivational Interviewing Training, September 1, 2010

Confidence Ruler
“If you decided right now to ___ (e.g., stop drinking, using drugs, enter treatment), how confident do you feel about succeeding with this?
If 0 was ‘not confident’ and 10 was
‘very confident’, what number would you give yourself?”
0
10Source: Mary Velasquez, HOT EAPA Motivational Interviewing Training, September 1, 2010

Building Confidence
What would make you more confident about making these changes?
Why have you given yourself such a high score on confidence?
How could you move up higher, so that your score goes from x to y?
How can I help you succeed?
Source: Mary Velasquez, HOT EAPA Motivational Interviewing Training, September 1, 2010
Assist with Action Plan
If you were to decide to change, what might your options be?
What is your next step?
How will you do that?
Are there any ways you know about that have worked for other people?
Is there anything you found helpful in any previous attempts to change?
Source: Mary Velasquez, HOT EAPA Motivational Interviewing Training, September 1, 2010
Assist with Action Plan
Who will you ask to help you?
What might get in the way?
What have you learned from the things that went wrong last time you tried?
How will you deal with those challenges?
Source: Mary Velasquez, HOT EAPA Motivational Interviewing Training, September 1, 2010
Give Encouragement
“I believe you can take that next step to…”
“I believe you’ll be able to implement that plan when you have those challenges.”

Provide Resources
Rethinking Drinking (booklet, online)
http://rethinkingdrinking.niaaa.nih.gov/
Tips for Cutting Down on Your Drinking
Mixing Alcohol and Medication

http://rethinkingdrinking.niaaa.nih.gov/
http://pubs.niaaa.nih.gov/publications/tips/tips.pdf

http://pubs.niaaa.nih.gov/publications/Medicine/Harmful_Interactions.pdf

Close on Good Terms
Say “Thank You”
“Thank you for taking a few minutes to talk with me about your alcohol use. I appreciate your openness and sharing your experiences/thoughts with me today.”

Ask for Permission
“I would like to see how things are going for you over the next few months. Would you mind if I followed up with you?”

Provide ReferralHigh Risk Cases: Referral to Specialist/Treatmente.g.,
addiction specialist behavioral health provider alcohol disease management chemical dependency program community resource (e.g., mutual help)
other referral sources
Moderate Risk Cases (as appropriate)
Provide Referral
“Based on the information you provided, I would encourage you to consider getting additional help for dealing with issues related to alcohol.”
“I would like to refer you/put you in touch with a provider on your health plan.”
“What do you think about this?”

It’s SBIRT using MI strategies(It’s not MI)
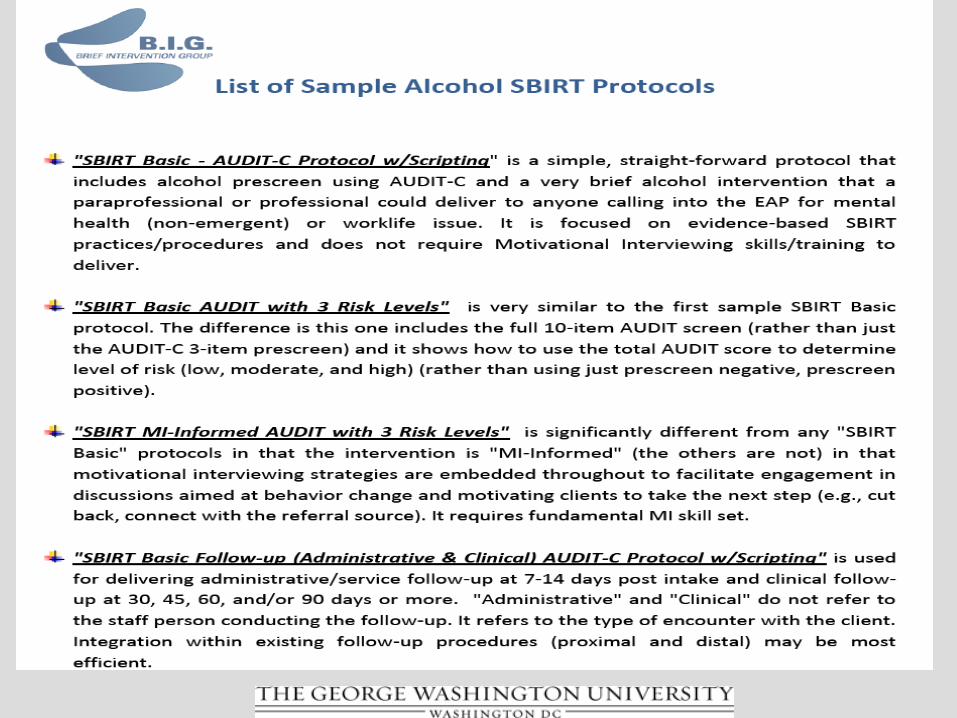
Sample Protocols “SBIRT Basic” (no MI) “SBIRT MI-Informed”
How does it all fit together?
Sample Protocols(handouts)



QUESTIONS?

BONUSELEMENTS

Bonus Element:
Implementation Tips
Tips
Normalize screening (and outcomes measurement) procedures
“We ask all clients who contact the EAP these questions.”
Give a reason for asking“We are trying to understand the impact
of EAP counseling in the workplace.”
Stress the need to follow-up“It’s important that I follow-up with you
to see how you’re doing, what is the best way to reach you?”
Adapted from: CGP’s Workplace Outcomes Suite: Overview, Rationale, and Implementation. Rik Lennox, Chestnut Global Partners

More Tips
Ask permission to follow-up “May I follow-up with you in X
(days/months)?”
Get good “locater” information “What is the best way to reach you?”
Stress confidentiality“Answering these questions is
completely voluntary and confidential, we will not share it with your employer.”
Adapted from: CGP’s Workplace Outcomes Suite: Overview, Rationale, and Implementation. Rik Lennox, Chestnut Global Partners

Integrate Screening and Outcome Measures at Intake
before EAP consultation, counseling
embed in existing intake assessment
often called “baseline” or “pre-test”
Adapted from: CGP’s Workplace Outcomes Suite: Overview, Rationale, and Implementation. Rik Lennox, Chestnut Global Partners
Recommendations

Integrate Screening and Outcome Measures at Follow-up
After EAP consultation, counseling embed in existing follow-up procedure often referred to as “post-test” time period varies
(30, 45, 60, 90 days; 6, 12, 24 months) consider instrument recommendations
when selecting time period (e.g., 90 days for “Workplace Outcomes Suite”)
Adapted from: CGP’s Workplace Outcomes Suite: Overview, Rationale, and Implementation. Rik Lennox, Chestnut Global Partners
Recommendations
Bonus Element:
EAP Pilot Tests
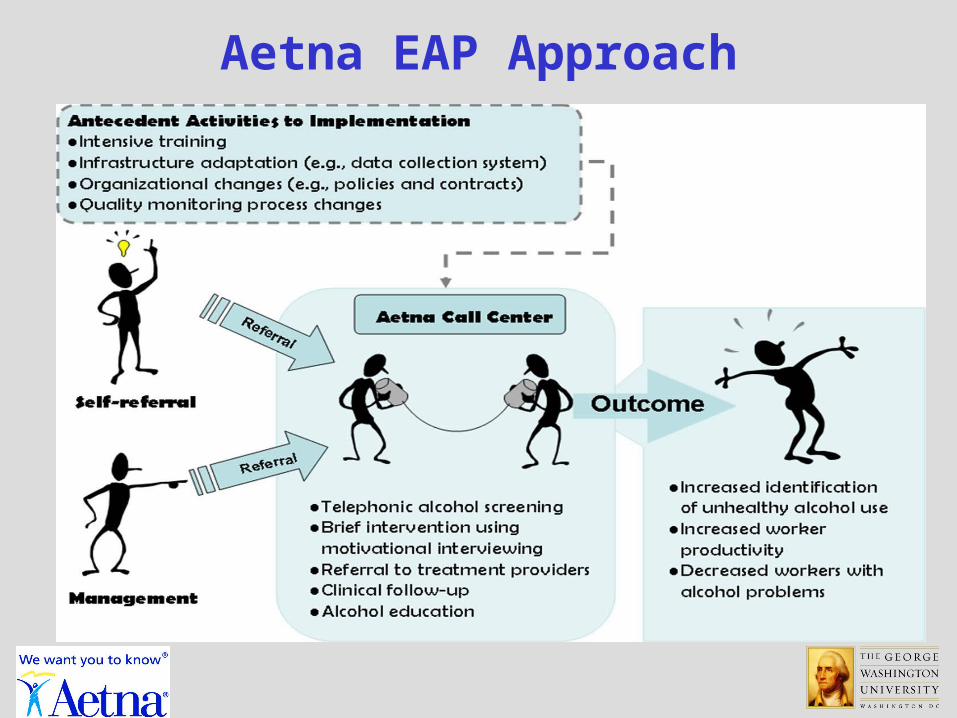
Aetna EAP Approach
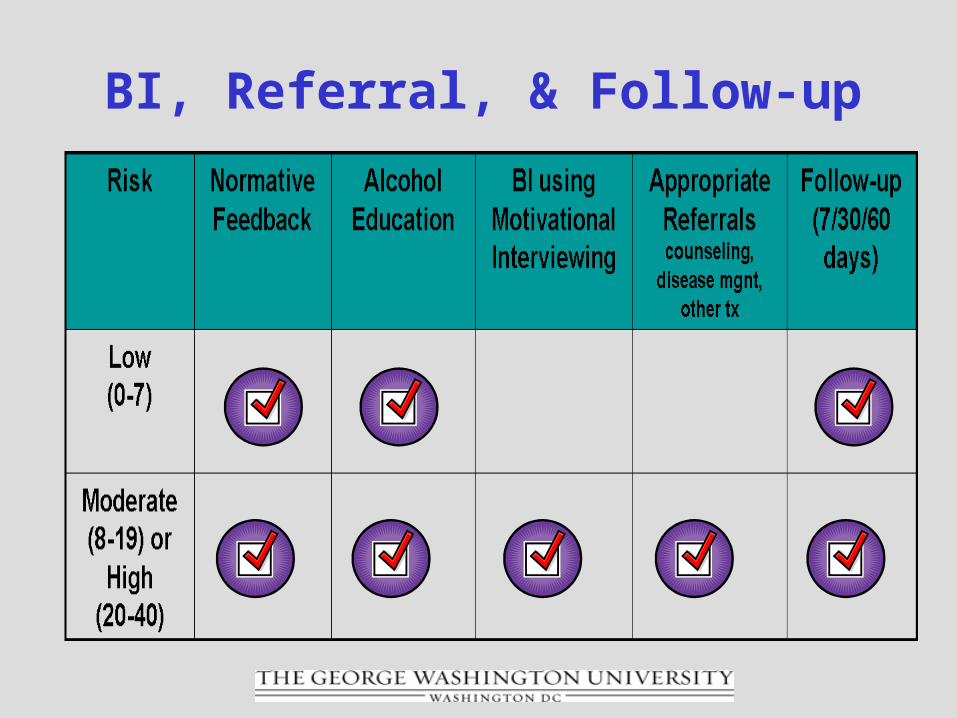
BI, Referral, & Follow-up

Aetna EAP Pilot
Site Characteristics: large U.S. employer (financial services) 147,000 employees non-emergent, self-referral cases dedicated EAP team
Evaluation Design: compared baseline to post-SBIRT
implementation at 5-months

Participation
93% completed the AUDIT-C 87% completed the AUDIT
AUDIT-C prescreen
40% positive, asked remaining 7 items 60% negative, stopped at item #3
Findings at 5 Months

AUDIT screen
Identification approached U.S. population estimates
18.5% using AUDIT screening tool
6% based on “presenting problem”
At baseline: < 1% (prior vendor data)
Findings at 5 Months

78% agreement to follow-up by EAP clinician
72% set an appointment for face-to-face counseling
Findings at 5 Months
McPherson, T.L., Goplerud, E., Derr, D., Mickenberg, J., Courtemanche, S. (in press, 2010). Telephonic Screening and Brief Intervention for Alcohol Misuse Among Workers Contacting the Employee Assistance Program: A Feasibility Study. Drug and Alcohol Review.

Pre-SBI
Time Period(n=68
1)
Post-SBI Time
Period(n=383
)
p-value
EAP Alcohol Identification
Hazardous alcohol use
7.5% (51)
20.1% (77)
<0.0001
Alcohol abuse/dependence
7.1% (48)
10.4% (40)
0.0536
OptumHealth EAPReplicated Findings
Greenwood, G., Goplerud, E., McPherson, T.L., Azocar, F., Baker, E., & Dybdahl, S. (in press, 2010). Alcohol Screening & Brief Intervention (SBI) in Telephonic EAP. Journal of Workplace Behavioral Health.

Bonus Element:
More “BIG” Resources(handout)

World Health Organization (WHO)
SBIRT ManualsEnglish: AUDIT http://whqlibdoc.who.int/hq/2001/WHO_MSD_MSB_01.6a.pdf
BI Manual http://whqlibdoc.who.int/hq/2001/WHO_MSD_MSB_01.6b.pdf
Spanish: AUDIT http://www.who.int/substance_abuse/activities/en/AUDITmanualSpanish.pdf
BI Manualhttp://www.who.int/substance_abuse/activities/en/
BImanualSpanish.pdf
AUDIT Online

117117
NIAAA 2005 Guidelines
http://pubs.niaaa.nih.gov/publications/Practitioner/CliniciansGuide2005/clinicians_guide.htm

• Free Online Training
• Video Cases: Helping Patients Who Drink Too Much
• Free CME/CE credit for physicians or nurses
http://www.niaaa.nih.gov/Publications/EducationTrainingMaterials/CME_CE.htm

119
AMA Approved Billing Codes
Providers can be reimbursed for SBI
http://www.ensuringsolutions.org/resources/resources_show.htm?doc_id=385233&cat_id=2005
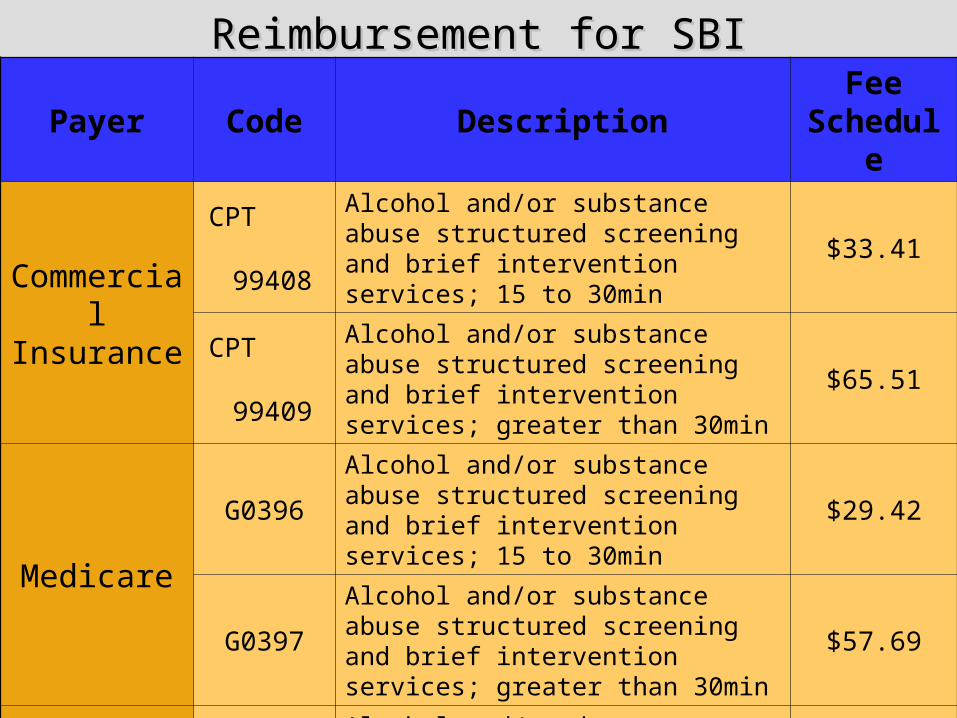
Reimbursement for SBIReimbursement for SBI
Payer Code DescriptionFee
Schedule
Commercial
Insurance
CPT
99408
Alcohol and/or substance abuse structured screening and brief intervention services; 15 to 30min
$33.41
CPT
99409
Alcohol and/or substance abuse structured screening and brief intervention services; greater than 30min
$65.51
Medicare
G0396Alcohol and/or substance abuse structured screening and brief intervention services; 15 to 30min
$29.42
G0397
Alcohol and/or substance abuse structured screening and brief intervention services; greater than 30min
$57.69
MedicaidH0049 Alcohol and/or drug screening $24.00
H0050Alcohol and/or drug service, brief intervention, per 15 min $48.00
Bonus Element:
Measuring Performance and Client Outcomes –
Demonstrating Impact and Value

Outcome Measures
WOS
WLQ
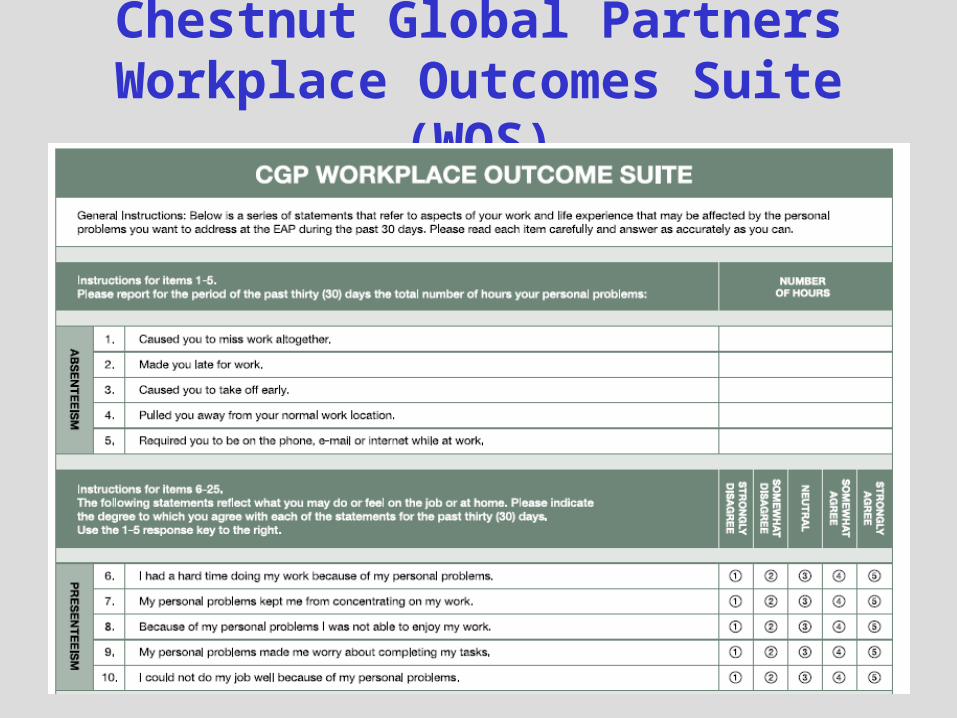
Chestnut Global PartnersWorkplace Outcomes Suite
(WOS)

WOS Developed by Rik Lennox, Dave Sharar et
al., Chestnut Global Partners
Free, with licensing agreement
20 items, 5 scales (5 items each)
Scales used stand-alone or together
Workplace focus (not clinical outcomes)
Short, sensitive to change
Administered at EAP Intake and at 90 days

WOS ScalesAbsenteeism
# hours away from work in past 30 days, can be monetized
Presenteeism proxy for productivity, extent to which
problems inhibit work
Work Engagement measure of "over" involvement with the
job
Life Satisfaction gauges importance of job to "life“
Workplace Distress looks at "distress at work" across all
problems

WOSRead more: Sharar and Lennox (2009). A New
Measure of EAP Success. Society of Human Resource Management.http://www.chestnutglobalpartners.org/LinkClick.aspx?fileticket=oE7rAAU5GMM%3D&tabid=364
Lennox, R.D., Sharar, D., Schmitz, E. , Goehner, D.B. (2010). Development and Validation of the Chestnut Global Partners Workplace Outcome Suite. JWBH, 25, 107-131. http://www.informaworld.com/smpp/content~content=a922042152~db=all~jumptype=rss
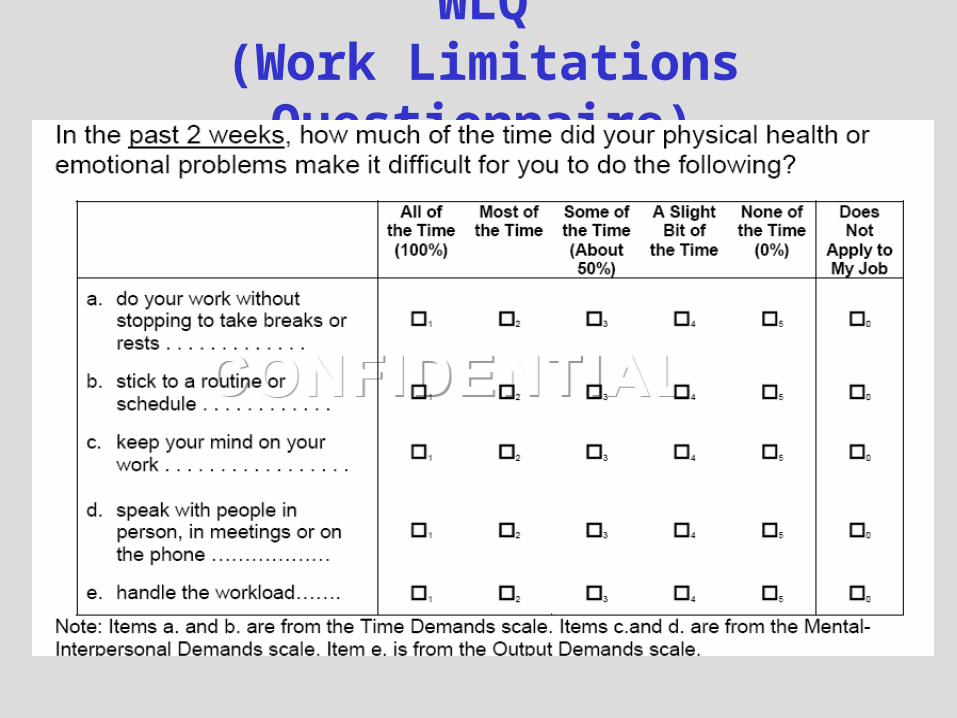
WLQ(Work Limitations
Questionnaire)

WLQDeveloped by Debra Lerner, Tufts Medical Centerhttp://160.109.101.132/icrhps/resprog/thi/wlq.asp
Available with licensing agreement
8 item (WLQ-Short Form) “presenteeism” or “on-the-job disability” measure
Four scales, used together
Designed for assessing groups of individuals currently employed
Indicates the degree health problems interfere with the ability to perform job roles, and productivity impact of these work limitations.

WLQ ScalesTime Management Scale
Difficulty performing a job easily at the beginning of the workday and starting the job soon after arriving at work.
Physical Demands Scale Ability to perform job tasks that involve
sitting and standing in one position and repeating the same motion repeatedly.
Mental-Interpersonal Demands Scale Difficulty concentrating on work and ability
to interact with people on-the-job.
Output Demands Scale Ability to complete work.

WLQ Productivity Loss Score
Estimates percent difference in an employee’s at-work
productivity compared to employees who do not have health-related work limitations (a healthy benchmark group).
Read more: Lerner, D., Amick, B.C., Rogers,
W.H., Malspeis, S., Bungay, K., Cynn, D. (2001). The work limitations questionnaire. Medical Care. 39, 72-85. http://www.ncbi.nlm.nih.gov/pubmed/11176545
WLQ website: http://160.109.101.132/icrhps/resprog/thi/wlq.asp

THANKYOU

Tracy L. McPherson, PhD
Assistant Research [email protected]
202-994-4307
Center for Integrated Behavioral Health Policy
Department of Health Policy, George Washington University Medical Center
Eric Goplerud, PhDResearch [email protected]
202-994-4307