3-hours continuing education sasi course: ems003...3-hours continuing education sasi course: ems003...
TRANSCRIPT

The Somatic Arts and Sciences Institute www.sasionline.com
3-Hours Continuing Education
SASI Course: EMS003
The Somatic Arts and Sciences Institute P.O. Box 3181 Merced, CA 95344 (209) 777-6305 www.sasionline.com
NCBTMB Approved
Provider #450872-08

2
Table of Contents Instructions…………………………………………………………………………………………………..……… 3 Educational Objectives……………………………………………………………………….………………….… 3 Chapter 1: The Hot Stone Massage…………...…………...………………………………………..…………….4 Chapter 2: The Science Behind Hot and Cold Stone Therapy……………………………………...…………24 Chapter 3: Unhealthy temperatures and injury treatment………………………………………………...……42 Summary of Hot Stone Massage…………………………………………………………………………………61 Course Completion: Certificate of Completion and Transcript……………………………………………...…63 Course Evaluation and Errata.………………………………………………………………….……….……..…64 Help and Technical Support Line……………………………………………………………………….…...……64 Bibliography (Sources)………………………………………………………………………………………..…...65 APPENDIX I Thermotherapy Study………………………………………………………………………………68 APPENDIX II Ice Massage versus Conventional Icing: a comparison on the effectiveness of each in the inflammation phase of healing……………………………………………………………………………….……84 APPENDIX III Human thermoregulation and the cardiovascular system………………………………….…92

3
Fundamentals of Hot Stone Massage
Instructions Thanks for downloading this Somatic Arts and Sciences continuing education course. You are looking at the plain text version of the course, which can be printed out if you like. Target Audience This continuing education course has been designed to meet the educational needs of massage therapists. Degree of Difficulty Beginner/Entry Level Course Description The course shows the student how hot stone techniques can be incorporated into holistic therapeutic practice, which will be of great value to practitioners of body working therapies. Safety measures, contraindications and proper care and cleaning of the stones is also covered. Educational Objectives Upon completion of this home study continuing education course, the massage practitioner should be able to: � Describe the physiological benefits of hot stone therapy
(thermotherapy) � List the appropriate range of temperature for safe use of stones. � Describe the motions used when incorporating hot stones in a
massage. � Identify the contraindications for hot stone therapy.
Introduction This course is presented for educational purposes only. It was developed and marketed specifically for massage therapists that are required to obtain

4
continuing education hours for licensing purposes. The author is not giving medical, legal or other professional advice. This course is classified as “Cognitive” learning, meaning that there is no hands on portion. The Somatic Arts and Sciences Institute strives to provide the most up to date and accurate material possible, however research and new discoveries continue daily and we assume no responsibility for errors or omissions due to the rapid advancement of science. Chapter 1 The Hot Stone Massage A hot stone massage is a variation of the typical massage, which uses smooth, water-heated stones on points around the body. Hot stone massages aredeeply soothing and relaxing and act to release tight muscles. Hot Stone massages are easy to perform, very therapeutic, and highly lucrative, making them an excellent addition to the massage practice. History of the Massage This is not a new treatment; people have been using hot stones for therapy for literally, thousands of years. The Japanese use stones to warm their abdomens to aid digestion and the Chinese have been rubbing themselves with hot stones to relieve muscular pain for about 2,000 years. It was also used as an ancient healing tradition in India when river stones were warmed in hot coals or hot water. Both the Ancient Romans and the Native Americans used heated stones to generate steam for saunas. This shouldn’t surprise anyone, after all, stones were among the first tools used by humans, and anthropologists have found decorative stones ranging from ornate to semi-precious quality among the buried remains of countless primitive cultures. As a species we seem to like rocks. The modern hot stone massage became popular after Mary Nelson, a massage therapist, introduced a massage technique in 1993 called La Stone Therapy using hot stones.

5
It has since become widespread across the United States. Hot Stone Massage is so popular now that you would have difficulty finding a Day Spa that does not include some form of Hot Rock Massage. Many massage schools are now including hot stone massage in their core curriculum-but some don’t, which is why we offer this basic course. The Stones The stones that are most often used in hot stone massages are smooth basalt rock from volcanoes. The basalt stones are usually fine-grained as a result of rapid cooling of lava on the Earth’s surface. As a result, these basalt stones retain heat very well. Stones that are artificially smoothed in a tumbler may also be used. River stones, smoothed by many years of submersion are commonly used by massage therapists for their ease in gliding across the skin. Mexican Pebble is a variety of stone that can be purchased very inexpensively at a landscape supply store, or at a stone quarry and it makes an excellent stone for massage use. Do not be fooled by it’s crude appearance. When you see it at the landscape supply store it looks like this: I know it doesn’t look like the fancy black polished stones you see in the spa brochures. Don’t worry, it will once you wash it, heat it up and put your oil on it.
Mexican Pebble at the landscape supply company The same stones at the Day Spa

6
Various sizes, shapes and weights of the stones are used during the hot stone massage depending on whether you are using it as a stationary stone or as a tool for bodywork. The larger stones are generally used as stationary stones, placed on the sacrum and other areas, whereas the smaller hand sized stones are used as tools to perform petrissage. Some therapists like to use very small stones to place on the face or even between the toes of the client. The number of stones needed during a hot stone massage can vary. For a typical full body massage, you’ll want to use approximately 40 to 50 stones, most of which should be the size of the palm of your hand. It is possible to use fewer stones, but you will need to constantly keep them reheated. If you do not want to constantly reheat stones, make sure you consider this factor when you are stocking your massage stones. Most stones in the Hot Stone massage should be used in the hand and worked over the body, in effleurage and petrissage strokes Some will be stationary stones, placed on strategic places on the body and left there for as long as it is convenient. Good places for stationary stones include the palms of the hands, the feet, the sacrum, along the spine and on the Charka Points. Precautions must be taken with stationary stones. Stationary stones should be cooler than the ones moving along the body, or they should be wrapped in linen before being placed on the body. Stationary stones are more likely to burn your client than a moving stone, so take the necessary precautions. I will be going over a simple routine for using hot stones in a massage later in this module, but for now let’s just get the science out of the way. The Therapeutic Quality of the Hot Stones Hot Stone massage is generally thought of as a pampering Spa treatment, but it is actually very therapeutic.

7
Heat has always been used in various forms for therapeutic use. Sunlight, heated sand, and heated water were initially used as an effective means of therapy for ailments and pain. Early users of heat therapy also obtained heat from hot stones and coals, open fire, and irons. The earliest hot water containers consisted of hollow dried fruits and the bladder or skin of animals. Heat therapy, also called thermotherapy, is the application of heat to the body for pain relief and health. It can take the form of a hot cloth, hot water, ultrasound, heating pad, hydrocollator packs, whirlpool baths, and of course, Hot Stone massage. It can be beneficial to those with arthritis and stiff muscles and injuries to the deep tissue of the skin. Heat may be an effective self-care treatment for conditions like rheumatoid arthritis.1 Heat therapy accomplishes it’s therapeutic works by means of a physiological phenomenon known as vasodilatation (see below). These therapeutic effects include increasing the extensibility of collagen tissues; decreasing joint stiffness; reducing pain; relieving muscle spasms; reducing inflammation, edema, and aids in the post acute phase of healing; and increasing blood flow. The increased blood flow to the affected area provides proteins, nutrients, and oxygen for better healing.2 Heat therapy is useful for muscle spasms, myalgia, fibromyalgia, contracture, bursitis.3 Heat therapy can be used for the treatment of headaches and migraines. Many people who suffer from chronic headaches also suffer from tight muscles in their neck and upper back. The application of constant heat to the back/upper back area can help to release the tension associated with headache pain. The placement of stationary stones for a hot stone massage meets this need nicely. Applying hot stones on the body increases the temperature of the skin and muscle tissue to improve circulation and calm the nervous system. 1 Thermotherapy for treating rheumatoid arthritis, from Cochrane Library 2 Prentice, William E. Arnheim’s Principles of Athletic Training: a Competency Based Approach. New York. McGraw-Hill. 2008. 3 Raj, P. Pritvi, Practical Management of Pain. Mosby. 2.000. ISBN 978-0-8151-2569-3.
Israel, Beth. “Pain”. Stoppain.org. 2005. Date Assessed: 28 April 2009.

8
As a result, hot stone massages are deeply relaxing and act to rebalance the body and mind. As the superficial muscles relax, a therapist can also massage the deeper muscles. The heat of the basalt stones release muscle tension faster than a classic Swedish massage. Vasodilation Vasodilation refers to the widening of blood vessels.4 It results from relaxation of smooth muscle cells within the vessel walls, particularly in the large veins, large arteries, and smaller arterioles. The process is essentially the opposite of vasoconstriction, which is the narrowing of blood vessels. When blood vessels dilate, the flow of blood is increased due to a decrease in vascular resistance. Therefore, dilation of arterial blood vessels (mainly the arterioles) decreases blood pressure. The response may be intrinsic (due to local processes in the surrounding tissue) or extrinsic (due to hormones or the nervous system). Additionally, the response may be localized to a specific organ (depending on the metabolic needs of a particular tissue, as during strenuous exercise), or it may be systemic (seen throughout the entire systemic circulation). Contraindications Because heat is a vasodilator, it should be avoided in tissues with inadequate vascular supply, in case of acute injury, in bleeding disorders (because heat would increase bleeding), in tissues with a severe lack of sensitivity, in scars. Hot stone massages are not recommended for those who: � Are prone to blood clots
� Suffer a skin disease or rash
� Have an open wound
� Have just undergone surgery or chemotherapy
4 "Definition of Vasodilation". MedicineNet.com. 27 April 2011. Retrieved 13 January 2012.
9
� Hot stones should not be applied on bruises, open wounds, tumors, hernias, fractures and inflamed skin. Pregnant women should also seek advice from their doctor before having a hot stone massage.
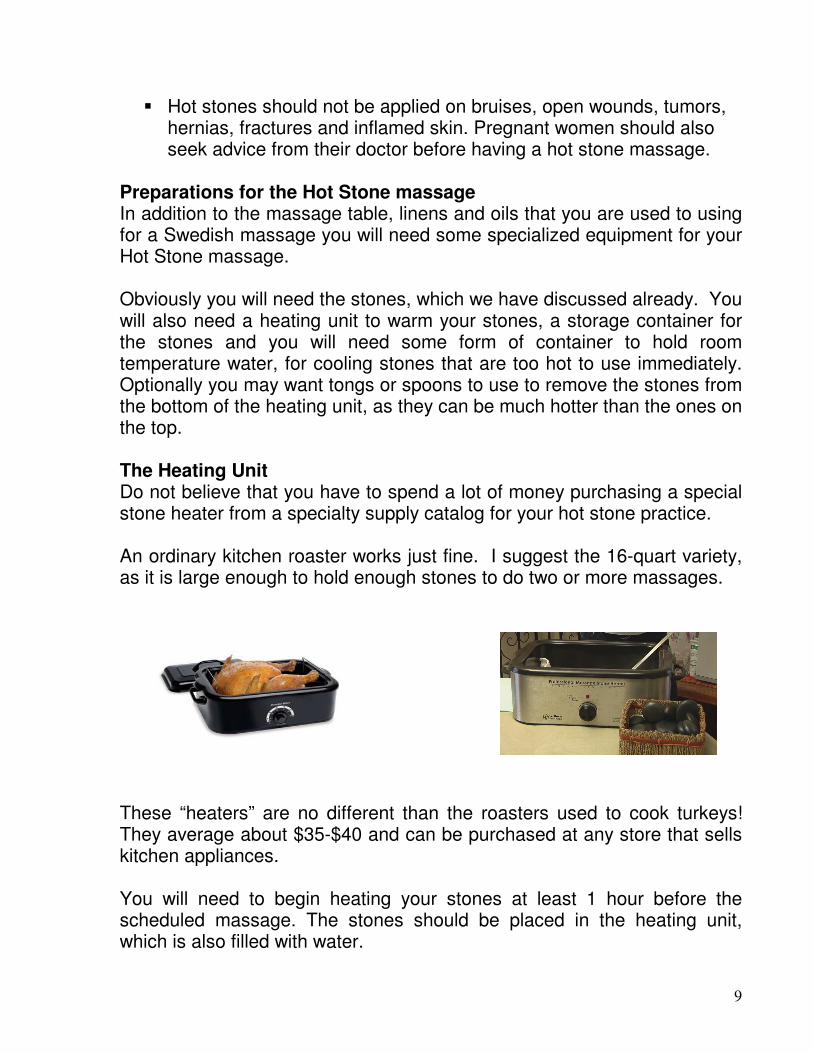
Preparations for the Hot Stone massage In addition to the massage table, linens and oils that you are used to using for a Swedish massage you will need some specialized equipment for your Hot Stone massage. Obviously you will need the stones, which we have discussed already. You will also need a heating unit to warm your stones, a storage container for the stones and you will need some form of container to hold room temperature water, for cooling stones that are too hot to use immediately. Optionally you may want tongs or spoons to use to remove the stones from the bottom of the heating unit, as they can be much hotter than the ones on the top. The Heating Unit Do not believe that you have to spend a lot of money purchasing a special stone heater from a specialty supply catalog for your hot stone practice. An ordinary kitchen roaster works just fine. I suggest the 16-quart variety, as it is large enough to hold enough stones to do two or more massages. These “heaters” are no different than the roasters used to cook turkeys! They average about $35-$40 and can be purchased at any store that sells kitchen appliances. You will need to begin heating your stones at least 1 hour before the scheduled massage. The stones should be placed in the heating unit, which is also filled with water.

10
You will find it is very helpful to place a small white towel in the bottom of the heater, so that you can see the stones. The inside of the heater is black and filled with water, and the stones are black, so placing a white towel inside makes it easier for you to find them. Temperatures vary by heating unit, but a safe range is 125-150 degrees Fahrenheit. While this seems very hot, they cool quickly, and if they are too hot you can douse them quickly in the container of room temperature water to cool them. Remember that anything over 100 degrees will feel warm to your client (that is warmer than normal human body temperature) so do not worry about the stones being too cool. An important rule is that if a stone is too hot to hold in your hand, it is too hot to use on your client. The palm of your hand has a great deal more temperature tolerance than a persons back, so keep that in mind. You can apply a stone to your forearm (like you would a baby bottle) to test it. Remember most of the stones you are using are going to be moving on the clients skin, so they are more tolerable than the stationary stones, which just sit on key areas. Stationary stones must be a little cooler or covered in an extra layer of linen. You should check in with your clients by asking them if the temperature is ok, just like you ask about pressure in a standard massage. Application of the Hot Stone massage Draping for the Hot Stone massage should be minimal. Diaper Draping is preferred. A good way to start your hot stone massage is by placing two warm palm sized stones in the clients hands. This establishes contact with them and keeps the contact going even when you leave their side to get more stones. As long as a stone is in contact with the client, you are in contact. Once you have placed the stones in the hand you can get two more and use them to effleurage any other area, like the back, the arms, the legs, etc.

11
Ensure that you have applied product to the skin of the area you are going to massage with the stone, and that you have applied product to the stones as well. They need to glide over the skin smoothly to be enjoyable to the client. This motion also allows you to use a stone that would be a little too

12
hot to rest on their skin, but will actually be very pleasant when gliding quickly over it. The direction of the gliding movements should be toward the heart, similar to an effleurage you would use during a Swedish massage. The direction of the gliding movements should be toward the heart, similar to an effleurage you would use during a Swedish massage.
No pressure or weight is needed when applying these gliding strokes-the heat does all the work. In this regard the hot stone massage can be a relaxing change of pace for you too.

13
The stones can be used to effleurage and to petrissage as well. Care should be taken when using the stones as tools for removing adhesions to not bruise the client. Stones penetrate tissue far more deeply than fingers and thumbs, and they are not yielding. After the stones have been used to perform effleurage and petrissage on the back the therapist can place stationary stones on the back to continue to work on the client while the arms and legs are attended to. Remember that stationary stones should be cooler than the ones used for gliding movements, especially if they are placed directly on the skin.

14
Care must be taken that the stones do not come loose and slide down to hit the clients neck or the back of the head. Keeping the stones further down on the back, like in the photo above or the diagram below, can prevent this. A large flat stone placed on the sacrum can feel very good to the client. The broad flat shape of the sacrum is very accommodating to weight and can take the stones comfortably. There are two basic patterns for placing the stationary stones on the back, and it really doesn’t matter which one you choose. You will notice that on both patterns there is one stone that is larger than the others on the sacrum and that there are no stones so high on the back that they might slip forward and fall onto the neck. The arms and the legs can be effleuraged with stones of the common variety, or if you are lucky enough to find some longer, flatter stones you can use them as shown below.

15
You can customize your hot stone massage by finding a variety of stones that can be used as different tools. You will want at least five or six large flat stones to use as stationary stones for the sacrum, sternum and back, and at least three or four tools to use for petrissage and flattening, like in these. Another option that is available is to place stones on the table, covered by linen, and then encourage your client to lie on top of them as you are working on their front. The idea here is to allow the stones to be stationary, and still working on the muscles of the back while laying on them. You must cover them with additional linens; the client will be laying on them and they are stones after all.
You can customize your hot stone massage by finding a variety of stones that can be used as different tools. You will want at least five or six large flat stones to use as stationary stones for the sacrum, sternum and back, and at least three or four tools to use for petrissage and flattening, like in the picture shown to the right.

16
A truly effective Hot Stone massage included a nice mixture of stationary stones and stones in motion, being used to effleurage and petrissage. Cold Stone Therapy Okay I know this course is entitled “Fundamentals of Hot Stone Massage” but I would be remiss if I didn’t introduce you to the other side of the stone-the Cold Stone Massage. Hot Stone therapy is built on the principle of vasodilatation, and as you would expect, Cold Stone therapy makes use of the opposite reaction-vasoconstriction. Vasoconstriction is the narrowing of the blood vessels resulting from contraction of the muscular wall of the vessels, particularly the large arteries and small arterioles. When blood vessels constrict, the flow of blood is restricted or decreased, thus, retaining body heat or increasing vascular resistance. On the surface this makes the skin turn paler because less blood reaches the surface, reducing the radiation of heat. On a larger
You will only want to try this if your massage table is sufficiently soft enough to allow the stones to “sink in” a bit. The table pictured has a memory foam pad, which allows the client to lie on the stones comfortably.

17
level, vasoconstriction is one mechanism by which the body regulates and maintains mean arterial pressure. Cold stones are primarily effective as a decongestant on various parts of the body. They help relieve swelling in the circulatory system, and this benefit makes cold stone massage a potential treatment for several ailments. In particular, the injuries related to sports are perfect examples. Most professional athletes have had to apply an icepack to some part of their body at least once in their career because of the swelling that goes hand in hand with pushing the body’s limits. The cold stones can help release the accumulation of blood in their tissues and muscles the same way that an icepack can. Because cold stones help relieve the congestion of body fluids, they can also be used on the sinuses to help alleviate pressure due to frequent colds or allergies. In any case where cold stones are used on the face, it's important that the therapist use a cloth under the stone to prevent discomfort from the stone being in direct contact with the skin. Other benefits of this type of massage include decreasing muscle spasms, stimulation of the nervous system and increased tissue metabolism. While the general the effect of hot stone massage is to create a feeling of relaxation, the cold stones are helpful for invigorating the tissues and blood vessels. Physiological benefits of cold stone massage One of the benefits of cold stone massage is that it can provide a deep state of relaxation, a release of tension, as well as, a reduction of swelling and inflammation due to scar tissue, trauma or injuries to muscles. Cold stones are critical in stone massage work as they decrease soreness when working on deeper muscles, and draws heat away from the body. Cold stone massages are also known for helping to alleviate: Anxiety/Depression-Stones that are cold help the mind to focus on the body and what it is experiencing rather than the mental/stress issues of life. PMS-Stones are placed on the abdomen and/or on the back to help alleviate pain, bloating and swelling associated with a menstruation

18
Sinusitis-Cold stones are placed on the face (or on a cloth that is on the face to prevent skin damage) to help reduce congestion and nasal swelling High Blood Pressure (with Increased Circulation)- When cold marble stones are placed in certain positions on the body, blood circulation increases and high blood pressure can decrease Fatigue-By relieving bloating, inflammation and swelling, and therefore increasing circulation, other benefits of this therapy is an increase energy levels and stamina Selection of the Cold Stones The important thermal quality that is best to look for in any type of massage stone, be it for hot or cold stone therapy, is its ability to resist thermal change. This is to say that if you are using a stone for cold stone therapy, it should have the ability to retain the cold for a long enough period of time to prove useful in a massage setting. Various stone can be used for cold stone therapy work. Sedimentary and basalt stone works but the industry favorite for cold stonework is marble. Marble retains cold very well but it is also the most expensive to purchase. The basalt stones we use for the hot stone massage are usually already round and perfectly smooth, but unfortunately marble doesn’t come so easily packaged. It must be shaped and polished so that it has a texture that is smooth enough to use against bare skin. This is why marble stone sets are typically more expensive than a basalt stone set. If you are going to be using cold stones you will want to keep in mind that, just as hot stones can burn, cold stones can desensitize the skin. While the cold stones will not desensitize the skin as quickly as ice does, it still can cause a massage client to loose enough feeling to the area that they wouldn't notice that soft tissue manipulations were too deep, and therefore would not let you know if you were actually causing damage. With this in mind, you would have to pay careful attention to the appearance of the skin. As with heat, cold can cause structural damage that may go unnoticed due to the anesthetic effect that cold as on a person's skin, but later it could be red and have “burned” look to it.

19
Alternating between hot and cold stones I am sure some of you reading this are already thinking, “Can I use both hot and cold stones in the same massage?” The answer is yes. Alternating between hot and cold stones can provide an exhilarating experience, but it is not one that everyone will enjoy or benefit from. Alternating between heat and cold will cause the blood vessels to alternate between dilation and constriction. The end result of this will be a dramatic increase in circulation to that area. For this reason this type of massage should not be used if the client has circulatory problems. Short and Long Hot Applications A short hot application on the skin, which lasts less than 5 minutes, produces a stimulatory response on circulation, as blood flow through the area is increased due to dilated blood vessels. In a long hot application, which is longer than 5 minutes, circulation is actually depressed as the movement of blood is decreased due to congestion produced by the first 5 minutes' exposure to heat. In the incident of the short hot application the reaction of the body is considered to be an "intrinsic" response, where the reaction is a direct result of the heat, which is transferred to the body. In the long hot application, the response of the body is a "reactive" one, where your body creates a reflex as a result of its protective reaction to the hot application. This reflex in the body occurs to prevent the observation we made in the above paragraph that the peripheral circulation although individually small, is collectively large enough in its capacity to hold the blood of central circulation if it is diverted away from the heart. Short and Long Cold Applications In a short cold application, which is less than 1 minute, the effect is stimulating to the circulation, though this would initially seem to be contradictory. On its initial contact with the skin, the effect is immediately depressive as the blood vessels instinctively constrict. This momentary and brief vasoconstriction is important, but insignificant, since it is quickly followed by a vasodilation that last for 20 to 60 seconds

20
The "reactive" response of the body occurs to prevent serious instant vasoconstriction, which occurs in disorders such as Raynaud's disease. Subsequent longer applications of cold greater than 1 minute result again in vasoconstriction. In long cold applications of greater than 1 minute, the effect on the circulation is thus depressive -- an "intrinsic" response of the body to cold. Effects on the Metabolism Thermotherapy and cryotherapy affects metabolism as a result of circulatory changes in the body or an area of the body. Even though thermotherapy and cryotherapy appears to be as simple as moving blood around, the effects on body tissues is profound. In the case of stimulatory effects of alternating thermotherapy and cryotherapy on metabolism, the following events take place in the body under a short cold or hot application. When the skin first encounters temperature changes, there is a temporary increase in blood pressure where the body responds by increasing circulation to the area. This increased superficial circulation results in increased blood supply to the muscles and tissues as the blood vessel widen to allow the blood to reach the capillaries on the skin. Subsequently, blood pressure drops. Heart rate, respiration rate, oxygen absorption, and carbon dioxide secretion all increase. Additional changes in metabolism occur under a short cold application. These include an increase in tissue tone, increase in peripheral white blood cell (WBC) counts, increase in peripheral red blood cell (RBC) counts, and a decrease in blood sugar levels. In addition, nitrogen absorption and excretion by the kidneys are also increased. For both short and long hot applications, the following changes in metabolism occur: decrease in tissue tone, decrease in peripheral WBC count, decrease in peripheral RBC count, and an increase in blood glucose levels. Introducing your clients to Hot or Cold Stones If you would like to introduce your current clients to the joy of Hot Stone massage an easy way to do it is to warm up the stones and ask them if they would like a free sample of the stones. You can add the use of hot stones to just one body part, like kneading the trapezius. This gives them an idea of how good it would feel, but leaves them wanting more.

21
Cleaning Your Stones The downside to incorporating hot stones in your massage practice is the amount of work it takes to clean up after the massage. Let’s get one thing perfectly clear-rubbing a warm stone covered with an organic carrier oil on a persons skin is like opening up a vacation resort for bacteria in your massage room. Sanitation measures have to be taken to keep your room free from disgusting pathogens. Hopefully you are already practicing good hygiene, but if you are going to be using hot stones you will have to take it up a notch. The massage stones must be cleaned after each client, without exception! While this may seem like a “no-brainer” you would be surprised how many day spas take the short cut of just putting them back in the heater, thinking, “Well it’s hot water, that kills germs, right?” Wrong. Very wrong. Ewwww. Not only do the stones have to be cleaned after being used on a client, the water in the heater must be changed between each client and the inside of the warmer has to be disinfected too. While this may sound extreme it makes perfect sense. You have to put your hands into the water of the heater to get the stones you use during the massage. Each and every time you put your hands in that water, you are contaminating it with the cooties of the person you are working on. Just because you don’t put the stones back in the heater after using them, it doesn’t mean you can skip the step of cleaning the heater. If this sounds like a lot of work, well, it is. The sad truth is that this is why we charge more money for a hot stone massage. It is more work for us. Not only do we have to pay way more attention while we are doing the massage (to avoid burning our clients) we have to do a lot more work after the session, so don’t feel bad charging and extra $20 or more in addition to your regular rate for the hour of hot stone work. Washing the stones in hot soapy water with antibacterial dish soap is sufficient for cleaning the hot stones. What I always did to save time was prepare a third container of hot soapy water before the massage, and I

22
would just drop the stones I used into it so they would be there waiting when I was done. The stones should then be rinsed in hot water, air-dried on a towel and if possible, wiped down with a disinfectant, Quats5 or even alcohol. The water in the heater should be changed after each use, and the water reservoir should be washed with antibacterial soap and water, rinsed and sprayed with disinfectant. The towel that is at the bottom of the heater must be replaced with a clean one. When it comes to cleaning the stones, light water soluble oil is easier to remove than a crème, gel or lotion. While these make great massage mediums, they become sticky messes when added to the water of the stone heater. When I worked at an upscale spa we were constantly pressured to get the client out of the room on time, since we only had a few minutes to wash our hands and change the linens before the next client arrived for their service. As you can imagine, this caused a great deal of grief when the service scheduled was a hot stone massage, and naturally, it led to cutting corners in the proper sanitation of the stones. We solved the problem by incorporating two things.
1. There was a large supply of stones available. We procured hundreds of stones for the massages from a local vendor of garden supplies and these stones were placed in tubs in a storeroom that was easily accessible by the three massage therapists that worked on any given day. We had enough stones so that we could easily wait until the end of the day to wash them so we didn’t have to worry about using the same ones twice.
2. Each massage room had two stone-heaters. When we looked at our schedule in the morning we could see what time we had hot stone massages. If there were ever two back to back (rare-but it happened) we would turn on both heaters, one for the massage we were doing and one for the following massage.
5 Quaternary ammonium compounds

23
These two simple steps made it possible for us to smoothly incorporate proper hygiene in a rapid paced business. Yes it cost the spa a little more initially to set up redundant heaters and excess stones, but it was worth it in the long run.
Demonstration Video If you feel like you need to see a demonstration you can see a very good one here. If you downloaded this course as a pdf document you can click this link here: http://www.sasionline.net/ems003_ems1227.html If you are reading it embedded in our website the link to the video page is below the embedded book.

24
Chapter 2: The Science Behind Hot and Cold Stone Therapy Thermotherapy Definition/Description Thermotherapy consists of application of heat or cold (cryotherapie) for the purpose of changing the cutaneous, intra-articular and core temperature of soft tissue with the intention of improving the symptoms of certain conditions. Cryotherapy and thermotherapy are useful adjuncts for the treatment of musculoskeletal injuries and soft tissue injuries. Using ice or heat as a therapeutic intervention decreases pain in joint and muscle as well as soft tissues and they have opposite effects on tissue metabolism, blood flow, inflammation, edema and connective tissue extensibility. Thermotherapy can be used in rehabilitation facilities or at home. Purpose The goal of thermotherapy is to alter tissue temperature in a targeted region over time for the purpose of inducing a desired biological response. The majority of thermotherapies are designed to deliver the thermal therapy to a target tissue volume with minimal impact on intervening or surrounding tissues. Heat: By increasing the temperature of the skin/soft tissue, the blood flow increases by vasodilatation. The metabolic rate and the tissue extensibility will also increase. Heat increases oxygen uptake and accelerates tissue healing, it also increases the activity of destructive enzymes, such as collagenase, and increases the catabolic rate. Cold: By decreasing the temperature of the skin/soft tissue, the blood flow decreases by vasoconstriction. It will be followed afterwards by a vasodilatation which will prevent against hypoxic damage (hunting reflex: If the cold pack is left on the skin for more than 10 minutes, the blood vessels will dilatate). The tissue metabolism will decrease just like the neuronal excitability, inflammation, conduction rate and tissue extensibility. At joint temperatures of 30°C or lower, the activity of cartilagedegrading enzymes, including collagenase, elastase, hyaluronidase, and protease, is inhibited. the decreased metabolic rate limits further injury and aids the tissue in surviving the cellular hypoxia that occurs after injury.

25
Both applications can reduce the pain, but when we need to use which application is still the question. Therefore, patient’s preference can be taken into consideration when deciding which thermotherapy tool to use. Application Heat: Heating of superficial tissues can be achieved using hot packs, wax baths, towels, sunlight, saunas, heat wraps, steam baths/rooms. We can also get the heat in the deeper tissues through electrotherapy (ultrasound, shockwave and infrared radiation). Cold: Cooling is achieved using ice packs, ice baths, cooling gel packs, cold air and sprays. In the literature, they describe cryotherapie (ice application) as an effective treatment for soft tissue injuries. It reduces the swelling, and it will improve the range of motion. However, there are still some doubts if it is actually effective for pain relief. So the application of ice may be useful for a variety of musculoskeletal pains, yet the evidence for its efficacy should be established more convincingly. Exercise in warm water, usually called hydrotherapy or balneotherapy, is a popular and effective treatment with a pain relief effect for many patients with painful neurologic or musculoskeletal conditions. The warmth of water may block nociception by acting on thermal receptors and mechanoreceptors, thus influencing spinal segmental mechanisms. It gives positive effects on cutaneous barrier homeostasis and a anti-inflammatory activity. In addition, the warmth may enhance blood flow and muscle relaxation. The hydrostatic effect may also relieve pain by reducing peripheral edema and by dampening sympathetic nervous system activity. Mechanism of Action Skin blood flow is controlled by two branches of the sympathetic nervous system: a noradrenergic vasoconstrictor system and a cholinergic active

26
vasodilator system. These dual sympathetic neural control mechanisms affect the major aspects of thermoregulatory responses over most of the human body’s surface. VC = vasocondtriction, VD = vasodilatation During periods of hypothermia, falling core and skin temperatures lead to reflexive increases in sympathetic active vasoconstrictor nerve activity to reduce skin blood flow and conserve body heat. During periods of heat stress, increasing core and skin temperatures lead to reflexive increases in sympathetic active vasodilator nerve activity to increase skin blood flow. The effect of heat on pain is mediated by heat sensitive calcium channels. These channels respond to heat by increasing intracellular calcium. This generates action potentials that increases stimulation of sensory nerves and causes the feeling of heat in the brain. These channels are part of a family of receptors called TRPV receptors. TRPV1 and TRPV2 channels are sensitive to noxious heat, while TRPV4 channels are sensitive to normal physiological heat. Their multiple binding sites allow a number of factors to activate these channels. Once activated, they can also inhibit the activity of purine pain receptors. These receptors, called P2X2 and P2Y2 receptors, are mediated pain receptors and are located in the peripheral

27
small nerve endings. For example, with peripheral pain, heat can directly inhibit pain. However, when pain is originating from deep tissue, heat stimulates peripheral pain receptors which can alter what has been termed gating in the spinal cord and reduce deep pain. Previous studies have suggested that temperature can affect the exchange between Ca2+ and Na+ in neural cells. They have documented an increase in both pain threshold (PTH) and pain tolerance (PTO) with the use of cooling. True or not true?Disadvantage: when you heat skin, vasodilatation (VD) distracts blood from soft tissue underneath and poor muscle circulation decreases metabolism in the muscles… Increased superficial tissue temperature results in the release of chemical mediators, such as histamine and prostaglandins, which result in vasodilation. These vasodilatory mechanisms do not significantly affect blood flow in skeletal muscle since skeletal muscle blood flow is heavily influenced by other physiologic and metabolic factors. Exercise is the best means to increase blood flow to skeletal muscle. Treatment The treatment depends on the type of application and the type of disease. There are 3 phases of the healing process: the inflammatory phase, the proliferation phase and the remodeling phase. The first phase, known as the inflammatory phase, protects the injured area from further injury while the body contains the damaged tissue. During this phase, cryotherapy can help to reduce swelling. Never use heat during this phase because heat increases the blood flow into the injured area and increases the amount of swelling. The inflammatory phase has a duration of 2 days. During the second phase, the proliferation phase, new tissue and scar tissue are formed. Heat can now be applied to the injured area to facilitate the healing process. The third and final phase, the remodeling phase, is the process of returning to health: the restoration of structure and function of injured or diseased tissues. The healing process includes blood clotting, tissue mending,

28
scarring and bone healing. Heat therapy can also be used during this phase. Physiological Effects Many of the local physiologic effects of heat and cold have been studied thoroughly. For instance, heat increases skin and joint temperature, improves blood circulation and muscle relaxation and decreases joint stiffness. Cold will numb the pain, decrease swelling, constrict blood vessels and block nerve impulses to the joint. Deep heating is thought to lessen nerve sensitivity, increase blood flow, increase tissue metabolism, decrease muscle spindle sensitivity to stretch, cause muscle relaxation, and increase flexibility. Heat stimulates the cutaneous thermo receptors that are connected to the cutaneous blood vessels, causing the release of bradykinin which relaxes the smooth muscle walls resulting in vasodilation. Muscle relaxation occurs as a result of a decreased firing rate of the gamma efferents, thus lowering the threshold of the muscle spindles and increasing afferent activity. There is also a decrease in firing of the alpha motorneuron to the extrafusal muscle fibre, resulting in muscle relaxation and decrease in muscle tone. Precautions A very important note that needs to be made is that thermotherapy is safe for people with a normal skin sensation. When a patient has problems with thermal sensitivity, it could be dangerous. They cannot feel if they are being burned due to the application. Effectiveness There are still a lot of contradictions if the use of thermotherapy is effective; however, worldwide it is used to reduce the pain. While there is good evidence that exercise relieves pain, improves function, and is cost-effective, evidence supporting the use of non-exercise physiotherapeutic interventions is much weaker. There is some support for the efficacy of thermotherapy, transcutaneous electrical neuromuscular stimulation (TENS), and massage. But there is little evidence to support the efficacy of electrotherapy, acupuncture or manual therapy. For knee osteoarthritis (OA), ice massage is reported to improve joint movement, pain and function; ice packs can reduce swelling and improve

29
movement but may not relieve pain. In rheumatoid arthritis (RA), heat or cold packs are reported to have no effect on edema, pain, movement, stre Despite conflicting evidence, the simple form of thermotherapy is widely recommended for many musculoskeletal conditions because it is a safe, effective, easy-to-apply and well-liked therapy based on anecdotal reports, expert opinion and patient preferences. Interventions that can be self-administered (thermotherapy, TENS, massage) are more likely to be cost-effective and less burdensome and hence much more attractive long-term management options. Complex thermal therapeutic modalities (heating deeper tissues) require special equipment, supervision and need to be delivered by a therapist, making them less accessible, more costly and higher risk. An example of Thermotherapy Osteoarthritis is a degenerative joint disease that affects mostly the weight-bearing joints in the knees and hips. As the affected joint degenerates pain and restriction of movement often occur. Inflammation can also occur sometimes resulting in edema of the joint with OA. Treatment focuses on decreasing pain and improving movement. To determine the effectiveness of thermotherapy in the treatment of OA of the knee. The outcomes of interest were relief of pain, reduction of edema, and improvement of flexion or range of motion (ROM) and function. Two independent reviewers selected randomized and controlled clinical trials with participants with clinical and/or radiological confirmation of OA of the knee; and interventions using heat or cold therapy compared with standard treatment and/or placebo. Trials comparing head to head therapies, such as two different types of diathermy, were excluded. Randomized and controlled clinical trials including participants with clinical or radiographical confirmation of OA of the knee and interventions using heat or cold compared to standard treatment or placebo were considered for inclusion. Study results were extracted by two independent reviewers. Outcomes were continuous in nature (pain, strength, improvement) and were analyzed by weighted mean difference using a fixed effects model. Graphical data were used when table data were not available.

30
Three randomized controlled trials, involving 179 patients, were included in this review. The included trials varied in terms of design, outcomes measured, cryotherapy or thermotherapy treatments and overall methodological quality. In one trial, administration of 20 minutes of ice massage, 5 days per week, for 3 weeks, compared to control demonstrated a clinically important benefit for knee OA on increasing quadriceps strength (29% relative difference). There was also a statistically significant improvement, but no clinical benefit in improving knee flexion ROM (8% relative difference) and functional status (11% relative difference). Another trial showed that cold packs decreased knee edema. Ice massage compared to control had a statistically beneficial effect on ROM, function and knee strength. Cold packs decreased swelling. Hot packs had no beneficial effect on edema compared with placebo or cold application. Ice packs did not affect pain significantly, compared to control, in patients with OA. More well designed studies with a standardized protocol and adequate number of participants are needed to evaluate the effects of thermotherapy in the treatment of OA of the knee. Thermotherapy (heat treatment) for treating osteoarthritis of the knee To answer this topic, scientists found and analyzed three studies. Over 170 people with osteoarthritis continue to take their medications but used hot, cold or ice packs/towels with or without massage or no treatment. The studies were not of high quality but this Cochrane review provides the best evidence we have today. What is thermotherapy and how might it help osteoarthritis of the knee? Osteoarthritis (OA) is the most common form of arthritis that can affect the hands, hips, shoulders and knees. In OA, the cartilage that protects the ends of the bones breaks down and causes pain and swelling. Thermotherapy involves applying heat or cold to joints to improve the symptoms of osteoarthritis and can be done with packs, towels, wax, etc. Heat may work by improving circulation and relaxing muscles, while cold may numb the pain, decrease swelling, constrict blood vessels and block nerve impulses to the joint. Thermotherapy can be used in rehabilitation programmes or at home.

31
One study showed that massaging with ice for 20 minutes, 5 days a week for 2 weeks, improved muscle strength in the leg, the range of motion in the knee and decreased time to walk 50 feet compared to no treatment. Another study showed that ice packs for 3 days a week for three weeks improved pain just as well as no treatment. Another study showed that cold packs for 20 minutes for 10 periods decreased swelling more than no treatment. Hot packs for the same amount of time had the same effect on swelling as no treatment. No side effects were reported in the studies, but in general, studies report that thermotherapy is safe when applied carefully. Since the studies were small and of low quality firm conclusions cannot be made. There is "silver" level evidence that ice massage could be used to improve range of motion and strength of the knee and function in people with osteoarthritis of the knee. Cold packs may be used to decrease swelling. Cryotherapy Definition/Description Cryotherapy, also known as ice application, is the simplest and oldest way to treat injuries. Its use is worldwide spread because of its effectiveness, convenience low cost and ease of transportation. Ice is believed to control pain by instigating local anesthesia. It also decreases edema, nerve conduction velocities, cellular metabolism and local blood flow. The effect of the cryotherapy depends on the method, the duration, the temperature of the ice and the depth of the subcutaneous fat. Application Methods The most common method of cryotherapy is the use of ice packs. There are different types of ice used in ice packs. The most common types are ice packs made with cubed, crushed and wetted ice. The study of Joseph H. Dykstra et al. sais that wetted ice is better to lower surface temperature during treatment and maintaining the lower temperature during recovery. It’s also more effective in lowering the intramuscular temperature during treatment. We may conclude that wetted ice is best for treating injuries and rapidly inducing local anesthesia.

32
Soft-Tissue Ice application is often used to treat soft tissue injuries. Yet, there is little evidence of the positive effects of cryotherapy. Therefore, many more high quality trials are needed to provide guidelines in the treatment of soft-tissue injuries. For more information, see APPENDIX II Ice Massage versus Conventional Icing: a comparison on the effectiveness of each in the inflammation phase of healing
Hydrotherapy-Balneotherapy Definition/Description Hydrotherapy is a definition for exercise in warm water and is a popular treatment for patients with neurologic and musculoskeletal conditions. The goals of this therapy are muscle relaxation, improving joint motion and reducing pain. This therapy is been used for thousands of years. (Level of evidence A1) Therapeutic effects 1) The warmth of water blocks nociception by acting on thermal receptors and mechanoreceptors, thus influencing spinal segmental mechanisms. 2) Warm water stimulates blood flow positively, which leads to muscle relaxation. 3) the hydrostatic effect may relieve pain by reducing peripheral edema and by dampening the sympatic nervous system activity. 4) Water exercises against resistance improves muscle strength. ( Levels of evidence A1,A2) Difference between aquatic exercise and balneotherapy Balneotherapy is hydrotherapy but without exercise and is also called “Spa therapy”. It is frequently used in alternative medicine as a disease cure and is very popular for treatment of all types of arthritis. There are not much studies that describe the difference in therapy effects between aquatic exercise and balneotherapy without exercise. Compared to balneotherapy, exercise in water is more effective for the treatment of musculoskeletal diseases than passive immersion. There are no long-term effects, so to keep the disease stable, it is necessary to frequently participate in water exercises.

33
It is not clear what exact the effect is of balneotherapy in musculoskeletal diseases because the studies involving this subject have poor methodological quality, which makes it difficult to determine the individual effect in this therapy. (Level of evidence A1) Hydrotherapy in patients with rheumatoid arthritis The study of A. Billberg confirms that temperate pool exercise has a significant effect on endurance and flexibility of the muscles, in upper and lower extremities in patients with RA. To gain this endurance and flexibility, exercises against resistance (Eccentric and concentric exercises) are necessary. Recent studies also indicate that patients with low muscle function can improve their muscle endurance with low impact exercises. The vitality of patients with Rheumatoid arthritis who participate in exercises in water is significantly improved after the hydrotherapy session. Two trials compared hydrotherapy to land-based exercise and failed to find any long term differences in quality of life, health status, pain or functional scores. When we compare aquatic exercises to no exercise at all, there is a significant improvement in reducing pain in patients who participated in aquatic exercises. Normal human body temperature Normal human body temperature, also known as normothermia or euthermia, depends upon the place in the body at which the measurement is made, the time of day, as well as the activity level of the person. Different parts of the body have different temperatures. Rectal and vaginal measurements, or measurements taken directly inside the body cavity, are typically slightly higher than oral measurements, and oral measurements are somewhat higher than skin temperature. The commonly accepted average core body temperature (taken internally) is 37.0 °C (98.6 °F). The typical oral (under the tongue) measurement is slightly cooler, at 36.8° ± 0.4 °C (98.2° ± 0.7 °F), and temperatures taken in other places (such as under the arm or in the ear) produce different typical numbers. Although some people think of these averages as representing the normal or ideal temperature, a wide range of temperatures has been found in healthy people.

34
The body temperature of a healthy person varies during the day by about 0.5 °C (0.9 °F) with lower temperatures in the morning and higher temperatures in the late afternoon and evening, as the body's needs and activities change. Other circumstances also affect the body's temperature. The core body temperature of an individual tends to have the lowest value in the second half of the sleep cycle; the lowest point, called the nadir, is one of the primary markers for circadian rhythms. The body temperature also changes when a person is hungry, sleepy, or cold. Temperature control (thermoregulation) is part of a homeostatic mechanism that keeps the organism at optimum operating temperature, as it affects the rate of chemical reactions. In humans the average internal temperature is 37.0 °C (98.6 °F), though it varies among individuals. However, no person always has exactly the same temperature at every moment of the day. Temperatures cycle regularly up and down through the day, as controlled by the person's circadian rhythm. The lowest temperature occurs about two hours before the person normally wakes up. Additionally, temperatures change according to activities and external factors. In addition to varying throughout the day, normal body temperature may also differ as much as 0.5 °C (0.9 °F) from one day to the next, so that the highest or lowest temperatures on one day will not always exactly match the highest or lowest temperatures on the next day. Normal human body temperature varies slightly from person to person and by the time of day. Consequently, each type of measurement has a range of normal temperatures. The range for normal human body temperatures, taken orally, is 36.8±0.5 °C (98.2±0.9 °F). This means that any oral temperature between 36.3 and 37.3 °C (97.3 and 99.1 °F) is likely to be normal. The normal human body temperature is often stated as 36.5–37.5 °C (97.7–99.5 °F). In adults a review of the literature has found a wider range of 33.2–38.2 °C (91.8–100.8 °F) for normal temperatures, depending on the gender and location measured. Natural rhythms

35
Body temperature normally fluctuates over the day, with the lowest levels around 4 a.m. and the highest in the late afternoon, between 4:00 and 6:00 p.m. (assuming the person sleeps at night and stays awake during the day). Therefore, an oral temperature of 37.3 °C (99.1 °F) would, strictly speaking, be a normal, healthy temperature in the afternoon but not in the early morning. An individual's body temperature typically changes by about 0.5 °C (0.9 °F) between its highest and lowest points each day. Body temperature is sensitive to many hormones, so women have a temperature rhythm that varies with the menstrual cycle, called a circamensal rhythm. A woman's basal body temperature rises sharply after ovulation, as estrogen production decreases and progesterone increases. Fertility awareness programs use this predictable change to identify when a woman can become pregnant. During the luteal phase of the menstrual cycle, both the lowest and the average temperatures are slightly higher than during other parts of the cycle. However, the amount that the temperature rises during each day is slightly lower than typical, so the highest temperature of the day is not very much higher than usual. Hormonal contraceptives both suppress the circamensal rhythm and raise the typical body temperature by about 0.6 °C (1.1 °F). Temperature also varies with the change of seasons during each year. This pattern is called a circannual rhythm. Studies of seasonal variations have produced inconsistent results. People living in different climates may have different seasonal patterns. Increased physical fitness increases the amount of daily variation in temperature. With increased age, both average body temperature and the amount of daily variability in the body temperature tend to decrease. Elderly patients may have a decreased ability to generate body heat during a fever, so even a somewhat elevated temperature can indicate a serious underlying cause in geriatrics. Measurement methods Different methods used for measuring temperature produce different results. The temperature reading depends on which part of the body is being measured. The typical daytime temperatures among healthy adults are as follows:

36
Temperature in the anus (rectum/rectal), vagina, or in the ear (otic) is about 37.5 °C (99.5 °F) Temperature in the mouth (oral) is about 36.8 °C (98.2 °F) Temperature under the arm (axillary) is about 36.5 °C (97.7 °F) Generally, oral, rectal, gut, and core body temperatures, although slightly different, are well-correlated, with oral temperature being the lowest of the four. Oral temperatures are generally about 0.4 °C (0.7 °F) lower than rectal temperatures. Oral temperatures are influenced by drinking, chewing, smoking, and breathing with the mouth open. Cold drinks or food reduce oral temperatures; hot drinks, hot food, chewing, and smoking raise oral temperatures. Axillary (armpit), tympanic (ear), and other skin-based temperatures correlate relatively poorly with core body temperature. Tympanic measurements run higher than rectal and core body measurements, and axillary temperatures run lower. The body uses the skin as a tool to increase or decrease core body temperature, which affects the temperature of the skin. Skin-based temperatures are more variable than other measurement sites. The peak daily temperature for axillary measurements lags about three hours behind the rest of the body. Skin temperatures are also more influenced by outside factors, such as clothing and air temperature. Variations due to outside factors Many outside factors affect the measured temperature as well. "Normal" values are generally given for an otherwise healthy, non-fasting adult, dressed comfortably, indoors, in a room that is kept at a normal room temperature (22.7 to 24.4 °C or 73 to 76 °F), during the morning, but not shortly after arising from sleep. Furthermore, for oral temperatures, the subject must not have eaten, drunk, or smoked anything in at least the previous fifteen to twenty minutes, as the temperature of the food, drink, or smoke can dramatically affect the reading.

37
Temperature is increased after eating or drinking anything with calories. Caloric restriction, as for a weight-loss diet, reduces overall body temperature. Drinking alcohol reduces the amount of daily change, slightly lowering daytime temperatures and noticeably raising nighttime temperatures. Exercise raises body temperatures. In adults, a noticeable increase usually requires strenuous exercise or exercise sustained over a significant time. Children develop higher temperatures with milder activities, like playing. Psychological factors also influence body temperature: a very excited person often has an elevated temperature. Wearing more clothing slows daily temperature changes and raises body temperature. Similarly, sleeping with an electric blanket raises the body temperature at night Sleep disturbances also affect temperatures. Normally, body temperature drops significantly at a person's normal bedtime and throughout the night. Short-term sleep deprivation produces a higher temperature at night than normal, but long-term sleep deprivation appears to reduce temperatures.Insomnia and poor sleep quality are associated with smaller and later drops in body temperature.Similarly, waking up unusually early, sleeping in, jet lag and changes to shift work schedules may affect body temperature. Thermoregulation explained Thermoregulation is the ability of the body to keep its temperature within certain boundaries, even when the surrounding temperature is very different. A thermoconforming organism, by contrast, simply adopts the surrounding temperature as its own body temperature, thus avoiding the need for internal thermoregulation. The internal thermoregulation process is one aspect of homeostasis: a state of dynamic stability in an organism's internal conditions, maintained far from equilibrium with its environment (the study of such processes in zoology has been called ecophysiology or physiological ecology). If the body is unable to maintain a normal temperature and it increases significantly above normal, a condition known as hyperthermia occurs. For humans, this occurs when the body is exposed to constant temperatures of approximately 55 °C (131 °F), and any prolonged exposure (longer than a few hours) at this temperature and

38
up to around 75 °C (167 °F) death is almost inevitable. Humans may also experience lethal hyperthermia when the wet bulb temperature is sustained above 35 °C (95 °F) for six hours. The opposite condition, when body temperature decreases below normal levels, is known as hypothermia. Whereas an organism that thermoregulates is one that keeps its core body temperature within certain limits, a thermoconformer is subject to changes in body temperature according to changes in the temperature outside of its body at a certain temperature. It was not until the introduction of thermometers that any exact data on the temperature of animals could be obtained. It was then found that local differences were present, since heat production and heat loss vary considerably in different parts of the body, although the circulation of the blood tends to bring about a mean temperature of the internal parts. Hence it is important to identify the parts of the body that most closely reflect the temperature of the internal organs. Also, for such results to be comparable, the measurements must be conducted under comparable conditions. The rectum has traditionally been considered to reflect most accurately the temperature of internal parts, or in some cases of sex or species, the vagina, uterus or bladder. Occasionally the temperature of the urine as it leaves the urethra may be of use in measuring body temperature. More often the temperature is taken in the mouth, axilla, ear or groin. As in other mammals, thermoregulation is an important aspect of human homeostasis. Most body heat is generated in the deep organs, especially the liver, brain, and heart, and in contraction of skeletal muscles. Humans have been able to adapt to a great diversity of climates, including hot humid and hot arid. High temperatures pose serious stresses for the human body, placing it in great danger of injury or even death. For humans, adaptation to varying climatic conditions includes both physiological mechanisms resulting from evolution and behavioural mechanisms resulting from conscious cultural adaptations. There are four avenues of heat loss: convection, conduction, radiation, and evaporation. If skin temperature is greater than that of the surroundings, the body can lose heat by radiation and conduction. But, if the temperature of the surroundings is greater than that of the skin, the body actually gains

39
heat by radiation and conduction. In such conditions, the only means by which the body can rid itself of heat is by evaporation. So, when the surrounding temperature is higher than the skin temperature, anything that prevents adequate evaporation will cause the internal body temperature to rise. During sports activities, evaporation becomes the main avenue of heat loss. Humidity affects thermoregulation by limiting sweat evaporation and thus heat loss. The skin assists in homeostasis (keeping different aspects of the body constant, e.g. temperature). It does this by reacting differently to hot and cold conditions so that the inner body temperature remains more or less constant. Vasodilation and sweating are the primary modes by which humans attempt to lose excess body heat. The brain creates much heat through the countless reactions which occur. Even the process of thought creates heat. The head has a complex system of blood vessels, which keeps the brain from overheating by bringing blood to the thin skin on the head, allowing heat to escape. The effectiveness of these methods is influenced by the character of the climate and the degree to which the individual is acclimatized. In hot conditions Eccrine sweat glands under the skin secrete sweat (a fluid containing mostly water with some dissolved ions), which travels up the sweat duct, through the sweat pore and onto the surface of the skin. This causes heat loss via evaporative cooling; however, a lot of essential water is lost. The hairs on the skin lie flat, preventing heat from being trapped by the layer of still air between the hairs. This is caused by tiny muscles under the surface of the skin called arrector pili muscles relaxing so that their attached hair follicles are not erect. These flat hairs increase the flow of air next to the skin increasing heat loss by convection. When environmental temperature is above core body temperature, sweating is the only physiological way for humans to lose heat. Arteriolar vasodilation occurs. The smooth muscle walls of the arterioles relax allowing increased blood flow through the artery. This redirects blood into the superficial capillaries in the skin increasing heat loss by convection and conduction.

40
Note: Most animals cannot sweat efficiently. Cats and dogs have sweat glands only on the pads of their feet. Horses and humans are two of the few animals capable of sweating. Many animals pant rather than sweat because the lungs have a large surface area and are highly vascularised. Air is inhaled, cooling the surface of the lungs and is then exhaled losing heat and some water vapour. In hot and humid conditions In general, humans appear physiologically well adapted to hot dry conditions. However, effective thermoregulation is reduced in hot, humid environments such as the Red Sea and Persian Gulf (where moderately hot summer temperatures are accompanied by unusually high vapor pressures), tropical environments, and deep mines where the atmosphere can be water-saturated. In hot-humid conditions, clothing can impede efficient evaporation. In such environments, it helps to wear light clothing such as cotton, that is pervious to sweat but impervious to radiant heat from the sun. This minimizes the gaining of radiant heat, while allowing as much evaporation to occur as the environment will allow. Clothing such as plastic fabrics that are impermeable to sweat and thus do not facilitate heat loss through evaporation can actually contribute to heat stress. In cold conditions The minute muscles under the surface of the skin called erector pili muscles (attached to an individual hair follicle) contract (piloerection), lifting the hair follicle upright. This makes the hairs stand on end, which acts as an insulating layer, trapping heat. This is what also causes goose bumps since humans do not have very much hair and the contracted muscles can easily be seen. Arterioles carrying blood to superficial capillaries under the surface of the skin can shrink (constrict), thereby rerouting blood away from the skin and towards the warmer core of the body. This prevents blood from losing heat to the surroundings and also prevents the core temperature dropping further. This process is called vasoconstriction. It is impossible to prevent all heat loss from the blood, only to reduce it. In extremely cold conditions, excessive vasoconstriction leads to numbness and pale skin. Frostbite occurs only when water within the cells begins to freeze. This destroys the cell causing damage.

41
Muscles can also receive messages from the thermo-regulatory center of the brain (the hypothalamus) to cause shivering. This increases heat production as respiration is an exothermic reaction in muscle cells. Shivering is more effective than exercise at producing heat because the animal remains still. This means that less heat is lost to the environment through convection. There are two types of shivering: low-intensity and high-intensity. During low-intensity shivering, animals shiver constantly at a low level for months during cold conditions. During high-intensity shivering, animals shiver violently for a relatively short time. Both processes consume energy, however high-intensity shivering uses glucose as a fuel source and low-intensity tends to use fats. This is a primary reason why animals store up food in the winter. Mitochondria can convert fat directly into heat energy, increasing the temperature of all cells in the body. Brown fat is specialized for this purpose, and is abundant in newborns and animals that hibernate. The process explained above, in which the skin regulates body temperature is a part of thermoregulation. This is one aspect of homeostasis — the process by which the body regulates itself to keep internal conditions constant.

42
Chapter 3: Unhealthy temperatures and injury treatment Unhealthy extremes in temperature Hot stone massage should be avoided if you suspect the client has a fever or another health issue that could be interfering with their thermoregulation. Fever A temperature setpoint is the level at which the body attempts to maintain its temperature. When the setpoint is raised, the result is a fever. Most fevers are caused by infectious disease and can be lowered, if desired, with antipyretic medications. An early morning temperature higher than 37.2 °C (> 98.9 °F) or a late afternoon temperature higher than 37.7 °C (> 99.9 °F) is normally considered a fever, assuming that the temperature is elevated due to a change in the hypothalamus's setpoint. Lower thresholds are sometimes appropriate for elderly people. The normal daily temperature variation is typically 0.5 °C (0.9 °F), but can be greater among people recovering from a fever. As a person's temperature increases, there is, in general, a feeling of cold despite an increase in body temperature. Once body temperature has increased to the new set-point temperature, there is a feeling of warmth. A fever can be caused by many medical conditions ranging from benign to potentially serious. Some studies suggest that fever is useful as a defense mechanism as the body's immune response can be strengthened at higher temperatures; however, there are arguments for and against the usefulness of fever, and the issue is controversial. With the exception of very high temperatures, treatment to reduce fever is often not necessary; however, antipyretic medications can be effective at lowering the temperature, which may improve the affected person's comfort. Fever differs from uncontrolled hyperthermia, in that hyperthermia is an increase in body temperature over the body's thermoregulatory set-point, due to excessive heat production or insufficient thermoregulation. A wide range for normal temperatures has been found. Fever is generally agreed to be present if the elevated temperature is caused by a raised set point and:

43
Temperature in the anus (rectum/rectal) is at or over 37.5–38.3 °C (99.5–100.9 °F) Temperature in the mouth (oral) is at or over 37.7 °C (99.9 °F) Temperature under the arm (axillary) or in the ear (otic) is at or over 37.2 °C (99.0 °F) In healthy adult men and women, the range of normal, healthy temperatures for oral temperature is 33.2–38.2 °C (91.8–100.8 °F), for rectal it is 34.4–37.8 °C (93.9–100.0 °F), for tympanic membrane (the ear drum) it is 35.4–37.8 °C (95.7–100.0 °F), and for axillary (the armpit) it is 35.5–37.0 °C (95.9–98.6 °F). Harrison's textbook of internal medicine defines a fever as a morning oral temperature of >37.2 °C (>98.9 °F) or an afternoon oral temperature of >37.7 °C (>99.9 °F) while the normal daily temperature variation is typically 0.5 °C (0.9 °F). Normal body temperatures vary depending on many factors, including age, sex, time of day, ambient temperature, activity level, and more. A raised temperature is not always a fever. For example, the temperature of a healthy person rises when he or she exercises, but this is not considered a fever, as the set-point is normal. On the other hand, a "normal" temperature may be a fever, if it is unusually high for that person. For example, medically frail elderly people have a decreased ability to generate body heat, so a "normal" temperature of 37.3 °C (99.1 °F) may represent a clinically significant fever. Febricula is an old term for a low-grade fever, especially if the cause is unknown, no other symptoms are present, and the patient recovers fully in less than a week. An organism at optimum temperature is considered afebrile or apyrexic, meaning "without fever". If temperature is raised, but the setpoint is not raised, then the result is hyperthermia. Hyperthermia Hyperthermia occurs when the body produces or absorbs more heat than it can dissipate. It is usually caused by prolonged exposure to high temperatures. The heat-regulating mechanisms of the body eventually

44
become overwhelmed and unable to deal effectively with the heat, causing the body temperature to climb uncontrollably. Hyperthermia at or above about 40 °C (104 °F) is a life-threatening medical emergency that requires immediate treatment. Common symptoms include headache, confusion, and fatigue. If sweating has resulted in dehydration, then the affected person may have dry, red skin. In a medical setting, mild hyperthermia is commonly called heat exhaustion or heat prostration; severe hyperthermia is called heat stroke. Heat stroke may come on suddenly, but it usually follows the untreated milder stages. Treatment involves cooling and rehydrating the body; fever-reducing drugs are useless for this condition. This may be done through moving out of direct sunlight to a cooler and shaded environment, drinking water, removing clothing that might keep heat close to the body, or sitting in front of a fan. Bathing in tepid or cool water, or even just washing the face and other exposed areas of the skin, can be helpful. With fever, the body's core temperature rises to a higher temperature through the action of the part of the brain that controls the body temperature; with hyperthermia, the body temperature is raised without the consent of the heat control centers. Hyperpyrexia Hyperpyrexia is a fever with an extreme elevation of body temperature greater than or equal to 41.5 °C (106.7 °F). Such a high temperature is considered a medical emergency as it may indicate a serious underlying condition or lead to significant side effects. The most common cause is an intracranial hemorrhage. Other possible causes include sepsis, Kawasaki syndrome, neuroleptic malignant syndrome, drug effects, serotonin syndrome, and thyroid storm. Infections are the most common cause of fevers, however as the temperature rises other causes become more common. Infections commonly associated with hyperpyrexia include: roseola, rubeola and enteroviral infections. Immediate aggressive cooling to less than 38.9 °C (102.0 °F) has been found to improve survival. Hyperpyrexia differs from hyperthermia in that in hyperpyrexia the body's temperature regulation mechanism sets the body temperature above the normal temperature, then generates heat to achieve this temperature, while in hyperthermia the body temperature rises above its set point due to an outside source.

45
Hypothermia Hypothermia is a condition in which the body's core temperature drops below that required for normal metabolism and body functions. This is generally considered to be less than 35.0 °C (95.0 °F). Characteristic symptoms depend on the temperature. In mild hypothermia there is shivering and mental confusion. In severe hypothermia there may be paradoxical undressing, where a person removes their clothing, as well as an increased risk of the heart stopping. Body temperature is usually maintained near a constant level of 36.5–37.5 °C (97.7–99.5 °F) through biologic homeostasis or thermoregulation. If a person is exposed to cold, and their internal mechanisms cannot replenish the heat that is being lost, the body's core temperature falls. This can occur due to excessive cold or health problems that decrease a person's ability to generate heat. The treatment of mild hypothermia involves: warm drinks, warm clothing and staying active. In those with moderate hypothermia minimizing movement is recommended along with heating blankets and warmed intravenous fluids. In severe hypothermia extracorporeal membrane oxygenation (ECMO) or cardiopulmonary bypass may be useful. In those without vitals signs cardiopulmonary resuscitation (CPR) is indicated along with the above measures. In those whose heart has stopped rewarming is typically continued until a persons temperature is greater than 32 °C (90 °F) before rewarming is deemed ineffective. It is the cause of at least 1500 deaths a year in the United States. One of the lowest documented body temperatures from which anyone has recovered was 13.0 °C (55.4 °F) in a near-drowning incident involving a 7-year-old girl in Sweden in December 2010. Hypothermia is the opposite of hyperthermia, which is present in heat exhaustion and heat stroke. Hypothermia is often defined as any body temperature below 35.0 °C (95.0 °F). With this method it is divided into degrees of severity based on the core temperature. Another classification system, the Swiss staging system, divides hypothermia based on the presenting symptoms which is preferred when it is not possible to determine an accurate core temperature.

46
Other cold-related injuries that can be present either alone or in combination with hypothermia include: Chilblains, superficial ulcers of the skin that occur when a predisposed individual is repeatedly exposed to cold. Frostbite, the freezing and destruction of tissue. Frostnip, a superficial cooling of tissues without cellular destruction. Trench foot or immersion foot, caused by to repetitive exposure to water at non-freezing temperatures. The normal human body temperature is often stated as 36.5–37.5 °C (97.7–99.5 °F).[6] Hyperthermia and fever, are defined as a temperature of greater than 37.5–38.3 °C (99.5–100.9 °F). Signs and symptoms vary depending on the degree of hypothermia, and may be divided by the three stages of severity. Infants with hypothermia may feel cold when touched, with bright red skin and unusual lack of energy. Symptoms of mild hypothermia may be vague, with sympathetic nervous system excitation (shivering, hypertension, tachycardia, tachypnea, and vasoconstriction). These are all physiological responses to preserve heat. Cold diuresis, mental confusion, and hepatic dysfunction may also be present. Hyperglycemia may be present, as glucose consumption by cells and insulin secretion both decrease, and tissue sensitivity to insulin may be blunted. Sympathetic activation also releases glucose from the liver. In many cases, however, especially in alcoholic patients, hypoglycemia appears to be a more common presentation. Hypoglycemia is also found in many hypothermic patients, because hypothermia may be a result of hypoglycemia. Moderate Low body temperature results in shivering becoming more violent. Muscle mis-coordination becomes apparent. Movements are slow and labored, accompanied by a stumbling pace and mild confusion, although the person may appear alert. Surface blood vessels contract further as the body focuses its remaining resources on keeping the vital organs warm. The subject becomes pale. Lips, ears, fingers, and toes may become blue.

47
Severe As the temperature decreases, further physiological systems falter and heart rate, respiratory rate, and blood pressure all decrease. This results in an expected heart rate in the 30s at a temperature of 28 °C (82 °F). Difficulty speaking, sluggish thinking, and amnesia start to appear; inability to use hands and stumbling are also usually present. Cellular metabolic processes shut down. Below 30 °C (86 °F), the exposed skin becomes blue and puffy, muscle coordination very poor, and walking almost impossible, and the person exhibits incoherent/irrational behavior, including terminal burrowing (see below) or even stupor. Pulse and respiration rates decrease significantly, but fast heart rates (ventricular tachycardia, atrial fibrillation) can also occur. Atrial fibrillation is not typically a concern in and of itself. Major organs fail. Clinical death occurs. Paradoxical undressing Twenty to fifty percent of hypothermia deaths are associated with paradoxical undressing. This typically occurs during moderate to severe hypothermia, as the person becomes disoriented, confused, and combative. They may begin discarding their clothing, which, in turn, increases the rate of heat loss. Rescuers who are trained in mountain survival techniques are taught to expect this; however, some may assume incorrectly that urban victims of hypothermia have been subjected to a sexual assault. One explanation for the effect is a cold-induced malfunction of the hypothalamus, the part of the brain that regulates body temperature. Another explanation is that the muscles contracting peripheral blood vessels become exhausted (known as a loss of vasomotor tone) and relax, leading to a sudden surge of blood (and heat) to the extremities, fooling the person into feeling overheated. Terminal burrowing An apparent self-protective behaviour known as terminal burrowing, or hide-and-die syndrome, occurs in the final stages of hypothermia. The afflicted will enter small, enclosed spaces, such as underneath beds or behind wardrobes. It is often associated with paradoxical undressing. Researchers in Germany claim this is "obviously an autonomous process of the brain stem, which is triggered in the final state of hypothermia and

48
produces a primitive and burrowing-like behavior of protection, as seen in hibernating animals." This happens mostly in cases where temperature drops slowly. Causes The rate of hypothermia is strongly related to age in the United States. Hypothermia usually occurs from exposure to low temperatures, and is frequently complicated by alcohol consumption. Any condition that decreases heat production, increases heat loss, or impairs thermoregulation, however, may contribute. Thus, hypothermia risk factors include: substance abuse (including alcohol abuse), homelessness, any condition that affects judgment (such as hypoglycemia), the extremes of age, poor clothing, chronic medical conditions (such as hypothyroidism and sepsis), and living in a cold environment. Hypothermia occurs frequently in major trauma, and is also observed in severe cases of anorexia nervosa. Alcohol Alcohol consumption increases the risk of hypothermia by its action as a vasodilator. It increases blood flow to the skin and extremities, making a person feel warm, while increasing heat loss. Between 33% and 73% of hypothermia cases are complicated by alcohol. Water immersion Hypothermia continues to be a major limitation to swimming or diving in cold water. The reduction in finger dexterity due to pain or numbness decreases general safety and work capacity, which consequently increases the risk of other injuries. Other factors predisposing to immersion hypothermia include dehydration, inadequate rewarming between repetitive dives, starting a dive while wearing cold, wet dry suit undergarments, sweating with work, inadequate thermal insulation (for example, thin dry suit undergarment), and poor physical conditioning. Heat is lost much more quickly in water than in air. Thus, water temperatures that would be quite reasonable as outdoor air temperatures can lead to hypothermia in survivors, although this is not usually the direct clinical cause of death for those who are not rescued. A water temperature of 10 °C (50 °F) can lead to death in as little as one hour, and water

49
temperatures near freezing can cause death in as little as 15 minutes. A notable example of this occurred during the sinking of the Titanic, when most people who entered the −2 °C (28 °F) water died within 15–30 minutes. The actual cause of death in cold water is usually the bodily reactions to heat loss and to freezing water, rather than hypothermia (loss of core temperature) itself. For example, plunged into freezing seas, around 20% of victims die within 2 minutes from cold shock, (uncontrolled rapid breathing, and gasping, causing water inhalation, massive increase in blood pressure and cardiac strain leading to cardiac arrest, and panic); another 50% die within 15–30 minutes from cold incapacitation (inability to use or control limbs and hands for swimming or gripping, as the body "protectively" shuts down the peripheral muscles of the limbs to protect its core), and exhaustion and unconsciousness cause drowning, claiming the rest within a similar time. Diagnosis Atrial fibrillation and Osborn J waves in a person with hypothermia. Note what could be mistaken for ST elevation. Accurate determination of core temperature often requires a special low temperature thermometer, as most clinical thermometers do not measure accurately below 34.4 °C (93.9 °F). A low temperature thermometer can be placed in the rectum, esophagus or the bladder. Esophageal measurements are the most accurate and are recommended once a person is intubated. Other methods of measurement such as in the mouth, under the arm, or using an infrared ear thermometer are often not accurate. As a hypothermic person's heart rate may be very slow, prolonged feeling for a pulse could be required before detecting. In 2005, the American Heart Association recommended at least 30–45 seconds to verify the absence of a pulse before initiating CPR.[45] Others recommend a 60 second check. The classical ECG finding of hypothermia is the Osborn J wave. Also, ventricular fibrillation frequently occurs below 28 °C (82 °F) and asystole below 20 °C (68 °F). The Osborn J may look very similar to those of an acute ST elevation myocardial infarction. Thrombolysis as a reaction to the presence of Osborn J waves is not indicated, as it would only worsen the underlying coagulopathy caused by hypothermia.

50
Prevention Appropriate clothing helps to prevent hypothermia. Synthetic and wool fabrics are superior to cotton as they provide better insulation when wet and dry. Some synthetic fabrics, such as polypropylene and polyester, are used in clothing designed to wick perspiration away from the body, such as liner socks and moisture-wicking undergarments. Clothing should be loose fitting, as tight clothing reduces the circulation of warm blood. In planning outdoor activity, prepare appropriately for possible cold weather. Those who drink alcohol before or during outdoor activity should ensure at least one sober person is present responsible for safety. Covering the head is effective, but no more effective than covering any other part of the body. While common folklore says that people lose most of their heat through their heads, heat loss from the head is no more significant than that from other uncovered parts of the body. However, heat loss from the head is significant in infants, whose head is larger relative to the rest of the body than in adults. Several studies have shown that for uncovered infants, lined hats significantly reduce heat loss and thermal stress. Children have a larger surface area per unit mass, and other things being equal should have one more layer of clothing than adults in similar conditions, and the time they spend in cold environments should be limited. However children are often more active than adults, and may generate more heat. In both adults and children, overexertion causes sweating and thus increases heat loss. Building a shelter can aid survival where there is danger of death from exposure. Shelters can be of many different types, metal can conduct heat away from the occupants and is sometimes best avoided. The shelter should not be too big so body warmth stays near the occupants. Good ventilation is essential especially if a fire will be lit in the shelter. Fires should be put out before the occupants sleep to prevent carbon monoxide poisoning. People caught in very cold, snowy conditions can build an igloo or snow cave to shelter. The United States Coast Guard promotes using life vests to protect against hypothermia through the 50/50/50 rule: If someone is in 50 °F (10 °C) water for 50 minutes, he/she has a 50 percent better chance of survival if wearing

51
a life jacket. A heat escape lessening position can be used to increase survival in cold water. Babies should sleep at 16-20 °C (61-68 °F) and housebound people should be checked regularly to make sure the temperature of the home is sufficient. Treatment ranges from noninvasive, passive external warming to active external rewarming, to active core rewarming.[10] In severe cases resuscitation begins with simultaneous removal from the cold environment and management of the airway, breathing, and circulation. Rapid rewarming is then commenced. Moving the person as little and as gently as possible is recommended as aggressive handling may increase risks of a dysrhythmia. Hypoglycemia is a frequent complication and needs to be tested for and treated. Intravenous thiamine and glucose is often recommended, as many causes of hypothermia are complicated by Wernicke's encephalopathy. The UK NHS advises the lay public against putting a person in a hot bath, massaging their arms and legs or using a heating pad. Rewarming Rewarming can be done with a number of different methods including passive external rewarming, active external rewarming, and active internal rewarming. Passive external rewarming involves the use of a person's own ability to generate heat by providing properly insulated dry clothing and moving to a warm environment. It is recommended for those with mild hypothermia. Active external rewarming involves applying warming devices externally, such as a heating blanket. These may function by warmed forced air (a Bair Hugger is a commonly used device), chemical reactions, or electricity. In wilderness environments, hypothermia may be helped by placing a hot water bottle in both armpits and groin. These methods are recommended for moderate hypothermia. Active core rewarming involves the use of intravenous warmed fluids, irrigation of body cavities with warmed fluids (the chest or abdomen), use of warm humidified inhaled air, or use of extracorporeal rewarming such as via a heart lung machine or extracorporeal membrane oxygenation. Extracorporeal rewarming is the fastest method for those with severe hypothermia. Survival rates with

52
normal mental functioning have been reported at around 50%. Chest irrigation is recommended if bypass or ECMO is not possible. Rewarming collapse (or rewarming shock) is a sudden drop in blood pressure in combination with a low cardiac output which may occur during active treatment of a severely hypothermic person. There was a theoretical concern that external rewarming rather than internal rewarming may increase the risk. These concerns were partly believed to be due to "after-drop", a situation detected during laboratory experiments where there is a continued decrease in core temperature after rewarming has been started. Recent studies have not supported these concerns, and problems are not found with active external rewarming. Fluids Warm sweetened liquids can be given provided the person is alert and can swallow. Many recommend that alcohol and drinks with lots of caffeine be avoided. As most people are moderately dehydrated due to cold-induced diuresis, warmed intravenous fluids to a temperature of 38–45 °C (100–113 °F) is often recommended. Dysrhythmias In those without signs of life cardiopulmonary resuscitation (CPR) should be continued during active rewarming. For ventricular fibrillation or ventricular tachycardia, a single defibrillation should be attempted. People with severe hypothermia however may not respond to pacing or defibrillation. It is not known if further defibrillation should be withheld until the core temperature reaches 30 °C (86 °F). In Europe epinephrine is not recommended until the temperature reaches 30 °C (86 °F) while the American Heart Association recommended up to three doses of epinephrine before 30 °C (86 °F) is reached. Once a temperature of 30 °C (86 °F) is reached, normal ACLS protocols should be followed. Prognosis It is usually recommended not to declare a person dead until their body is warmed to a near normal body temperature of greater than 32 °C (90 °F), since extreme hypothermia can suppress heart and brain function. Exceptions include if there is an obvious fatal injuries or the chest is frozen so that it cannot be compressed. If a person was buried in an avalanche for more than 35 minutes and is found with a mouth packed full of snow

53
without a pulse stopping early may also be reasonable. This is also the case if a persons blood potassium is greater than 12 mmol/l. Those who are stiff with pupils that do not move may survive if treated aggressively. Survival with good function also occasionally occurs even after the need for hours of CPR. Children who have a near-drowning accidents in water near 0 °C (32 °F) can occasionally be revived even over an hour after losing consciousness. The cold water lowers metabolism, allowing the brain to withstand a much longer period of hypoxia. While survival is possible, mortality from severe or profound hypothermia remains high despite optimal treatment. Studies estimate mortality at between 38% and 75%. In those who have hypothermia due to another underlying health problem, when death occurs it is frequently from that underlying health problem. Basal body temperature Basal body temperature is the lowest temperature attained by the body during rest (usually during sleep). It is generally measured immediately after awakening and before any physical activity has been undertaken, although the temperature measured at that time is somewhat higher than the true basal body temperature. In women, temperature differs at various points in the menstrual cycle, and this can be used in the long-term to track ovulation both for the purpose of aiding conception or avoiding pregnancy. This process is called fertility awareness. Core temperature Core temperature, also called core body temperature, is the operating temperature of an organism, specifically in deep structures of the body such as the liver, in comparison to temperatures of peripheral tissues. Core temperature is normally maintained within a narrow range so that essential enzymatic reactions can occur. Significant core temperature elevation (hyperthermia) or depression (hypothermia) that is prolonged for more than a brief period of time is incompatible with human life. Temperature examination in the rectum is the traditional gold standard measurement used to estimate core temperature (oral temperature is affected by hot or cold drinks and mouth-breathing). Rectal temperature is expected to be approximately one Fahrenheit degree higher than an oral temperature taken on the same person at the same time. Ear

54
thermometers measure eardrum temperature using infrared sensors. The blood supply to the tympanic membrane is shared with the brain. However, this method of measuring body temperature is not as accurate as rectal measurement and has a low sensitivity for fevers, missing three or four out of every ten fevers in children. Ear temperature measurement may be acceptable for observing trends in body temperature but is less useful in consistently identifying fevers. Until recently, direct measurement of core body temperature required surgical insertion of a probe, so a variety of indirect methods have commonly been used. The rectal or vaginal temperature is generally considered to give the most accurate assessment of core body temperature, particularly in hypothermia. In the early 2000s, ingestible thermistors in capsule form were produced, allowing the temperature inside the digestive tract to be transmitted to an external receiver; one study found that these were comparable in accuracy to rectal temperature measurement.
Chilblain, Frostnip and Frostbite Chilblain (aka pernio) is a medical condition that is often confused with frostbite and trench foot. Chilblain is the mildest form of cold injury and develops on the feet, hands, and face. Athletes participating in winter sports like skiing, snowboarding, and extreme snowball fighting are usually unaware of the injury, thinking it’s just normal tingling from the cold but later noticing a persistent burn and itching that can develop into blisters. The condition is caused by cold exposure damaging the capillary beds in the skin, which in turn causes redness, itching, blisters, and inflammation. This common cold weather sports injury can be avoided by keeping the hands and feet warm (duh) while participating in outdoor sports in winter. Frostbite is the medical condition where localized damage is caused to skin and other tissues due to freezing. Frostbite is most likely to happen in body parts farthest from the heart and those with large exposed areas. The initial stages of frostbite are sometimes called frostnip. At or below 0 °C (32 °F), blood vessels close to the skin start to constrict, and blood is shunted away from the extremities via the action of glomus bodies. The same response may also be a result of exposure to high winds. This constriction helps to preserve core body temperature. In

55
extreme cold, or when the body is exposed to cold for long periods, this protective strategy can reduce blood flow in some areas of the body to dangerously low levels. This lack of blood leads to the eventual freezing and death of skin tissue in the affected areas. There are four degrees of frostbite. Each of these degrees has varying degrees of pain. This is a severe stage of the condition and is unlikely to be encountered by cold weather athletes unless something seriously goes wrong, like they got stuck on the ski lift or got lost on the mountain and couldn’t get to the hot chocolate kiosk at the ski lodge before the sun went down. The first degree of Frostbite is frostnip and only affects the surface of the skin, which is frozen. On the onset, there is itching and pain, and then the skin develops white, red, and yellow patches and becomes numb. The area affected by frostnip usually does not become permanently damaged as only the skin's top layers are affected. Long-term insensitivity to both heat and cold can sometimes happen after suffering from frost nip. If freezing continues, the skin may freeze and harden, but the deep tissues are not affected and remain soft and normal. Second-degree injury usually blisters 1–2 days after becoming frozen. The blisters may become hard and blackened, but usually appear worse than they are. Most of the injuries heal in one month, but the area may become permanently insensitive to both heat and cold. Third and fourth degree frostbite occurs if the area freezes further. The muscles, tendons, blood vessels, and nerves all freeze. The skin is hard and feels waxy, and use of the area is lost temporarily, and in severe cases, permanently. The deep frostbite results in areas of purplish blisters which turn black and which are generally blood-filled. Nerve damage in the area can result in a loss of feeling. This extreme frostbite may result in fingers and toes being amputated if the area becomes infected with gangrene. If the frostbite has gone on untreated, they might just fall off on their own. The extent of the damage done to the area by the freezing process of the frostbite may take several months to assess, and this often delays surgery to remove the dead tissue. Massage therapy implications Massage is actually a great way to help prevent Chillblain, if the affected areas can be massaged in a safe warm environment when the symptoms

56
first begin. The increased circulation from the massage can greatly reduce the amount of discomfort that would be experienced later. If the Chillblain is in the acute stage (redness, itching, blisters, and inflammation) massage is contraindicated as it would only further agitate the skin. Frostnip and Frostite are both more serious conditions that contraindicate massage due to the presence of blistering and inflammation to the skin. Burns and Scalds A burn is a type of injury to flesh or skin caused by heat, electricity, chemicals, friction, or radiation. Burns that affect only the superficial skin are known as superficial or first-degree burns. When damage penetrates into some of the underlying layers, it is a partial-thickness or second-degree burn. In a full-thickness or third-degree burn, the injury extends to all layers of the skin. A fourth-degree burn additionally involves injury to deeper tissues, such as muscle or bone. The treatment required depends on the severity of the burn. Superficial burns may be managed with little more than simple pain relievers, while major burns may require prolonged treatment in specialized burn centers. Cooling with tap water may help relieve pain and decrease damage; however, prolonged exposure may result in low body temperature. Partial-thickness burns may require cleaning with soap and water, followed by dressings. It is not clear how to manage blisters, but it is probably reasonable to leave them intact. Full-thickness burns usually require surgical treatments, such as skin grafting. Extensive burns often require large amounts of intravenous fluid, because the subsequent inflammatory response causes significant capillary fluid leakage and edema. The most common complications of burns involve infection. While large burns can be fatal, modern treatments developed since 1960 have significantly improved the outcomes, especially in children and young adults. Globally, about 11 million people seek medical treatment, and 300,000 die from burns each year. In the United States, approximately 4% of those admitted to a burn center die from their injuries. The long-term outcome is primarily related to the size of burn and the age of the person affected.

57
The characteristics of a burn depend upon its depth. Superficial burns cause pain lasting two or three days, followed by peeling of the skin over the next few days. Individuals suffering from more severe burns may indicate discomfort or complain of feeling pressure rather than pain. Full-thickness burns may be entirely insensitive to light touch or puncture. While superficial burns are typically red in color, severe burns may be pink, white or black. Burns around the mouth or singed hair inside the nose may indicate that burns to the airways have occurred, but these findings are not definitive. More worrisome signs include: shortness of breath, hoarseness, and stridor or wheezing. Itchiness is common during the healing process, occurring in up to 90% of adults and nearly all children. Numbness or tingling may persist for a prolonged period of time after an electrical injury. Burns may also produce emotional and psychological distress. At temperatures greater than 44 °C (111 °F), proteins begin losing their three-dimensional shape and start breaking down. This results in cell and tissue damage. Many of the direct health effects of a burn are secondary to disruption in the normal functioning of the skin. They include disruption of the skin's sensation, ability to prevent water loss through evaporation, and ability to control body temperature. Disruption of cell membranes causes cells to lose potassium to the spaces outside the cell and to take up water and sodium. In large burns (over 30% of the total body surface area), there is a significant inflammatory response. This results in increased leakage of fluid from the capillaries, and subsequent tissue edema. This causes overall blood volume loss, with the remaining blood suffering significant plasma loss, making the blood more concentrated. Poor blood flow to organs such as the kidneys and gastrointestinal tract may result in renal failure and stomach ulcers. Increased levels of catecholamines and cortisol can cause a hypermetabolic state that can last for years. This is associated with increased cardiac output, metabolism, a fast heart rate, and poor immune function. Burns can be classified by depth, mechanism of injury, extent, and associated injuries. The most commonly used classification is based on the depth of injury. The depth of a burn is usually determined via examination, although a biopsy may also be used. It may be difficult to accurately

58
determine the depth of a burn on a single examination and repeated examinations over a few days may be necessary. In those who have a headache or are dizzy and have a fire-related burn, carbon monoxide poisoning should be considered. Cyanide poisoning should also be considered. The size of a burn is measured as a percentage of total body surface area (TBSA) affected by partial thickness or full thickness burns.[10] First-degree burns that are only red in color and are not blistering are not included in this estimation. Most burns (70%) involve less than 10% of the TBSA. There are a number of methods to determine the TBSA, including the "rule of nines", Lund and Browder charts, and estimations based on a person's palm size. The rule of nines is easy to remember but only accurate in people over 16 years of age. More accurate estimates can be made using Lund and Browder charts, which take into account the different proportions of body parts in adults and children. The size of a person's handprint (including the palm and fingers) is approximately 1% of their TBSA. To determine the need for referral to a specialized burn unit, the American Burn Association devised a classification system. Under this system, burns can be classified as major, moderate and minor. This is assessed based on a number of factors, including total body surface area affected, the involvement of specific anatomical zones, the age of the person, and associated injuries. Minor burns can typically be managed at home, moderate burns are often managed in hospital, and major burns are managed by a burn center. Scalding (from the Latin word calidus, meaning hot) is a form of burning from heated fluids such as boiling water or steam. Most scalds result from exposure to high-temperature water such as tap water in baths and showers or cooking water boiled for the preparation of foods. Another common cause of scalds is spilled hot drinks, such as coffee. Scalds are generally more common in children, especially from the accidental spilling of hot liquids. Most scalds are considered first or second degree burns, but third degree burns can result, especially with prolonged contact. Scalds are typically far more severe when caused by steam, because it has absorbed a great amount of latent heat, and is therefore far more effective at heating objects.

59
Applying first aid for scalds is the same as for burns. First, the site of the injury should be removed from the source of heat, to prevent further scalding. If the burn is at least second degree, remove any jewelry or clothing from the site, unless it is already stuck to the skin. Cool the scald for about 20 minutes with cool or lukewarm water, such as tap water from a faucet. Ice should be avoided, as it can do further damage to area around the injury, as should butter, toothpaste, and specialized creams. With second-degree burns, blisters will form, but should never be popped, as it only increases chances of infection. With third-degree burns, it is best to wrap the injury very loosely to keep it clean, and seek expert medical attention. First Aid for Burns and Scalds Appropriate first aid must be used to treat any burns or scalds as soon as possible. This will limit the amount of damage to your skin. You may need to apply the following first aid techniques to yourself or to another person who has been burnt. First aid for burns Follow the first aid advice below to treat burns and scalds: Stop the burning process as soon as possible. This may mean removing the person from the area, dousing flames with water or smothering flames with a blanket. Do not put yourself at risk of getting burnt as well. Remove any clothing or jewellery near the burnt area of skin. However, don't try to remove anything that is stuck to the burnt skin because this could cause more damage. Cool the burn with cool or lukewarm water for 10 to 30 minutes, ideally within 20 minutes of the injury occurring. Never use ice, iced water or any creams or greasy substances such as butter. Keep yourself or the person warm. Use a blanket or layers of clothing, but avoid putting them on the injured area. Keeping warm will prevent hypothermia, where a person's body temperature drops below 35ºC (95ºF). This is a risk if you are cooling a large burnt area, particularly in young children and elderly people.

60
Cover the burn with cling film. Put the cling film in a layer over the burn, rather than wrapping it around a limb. A clean clear plastic bag can be used for burns on your hand. Treat the pain from a burn with paracetamol or ibuprofen. Always check the manufacturer's instructions when using over-the-counter (OTC) medication. Children under 16 years of age should not be given aspirin. When to go to hospital Once you have taken these steps, you will need to decide whether further medical treatment is necessary. Go to a hospital accident and emergency (A&E) department for: � Large or deep burns – any burn bigger than the affected person's
hand � Full thickness burns of all sizes – these burns cause white or charred
skin � Partial thickness burns on the face, hands, arms, feet, legs or genitals
– these are burns that cause blisters � All chemical and electrical burns
Also get medical help straight away if the person with the burn: � Has other injuries that need treating � Is going into shock – signs include cold clammy skin, sweating, rapid
shallow breathing and weakness or dizziness � Is pregnant � Is over 60 years of age � Is under five years of age � Has a medical condition such as heart, lung or liver disease, or
diabetes � Has a weakened immune system (the body's defence system), for
example because of HIV or AIDS, or because they're having chemotherapy for cancer
If someone has breathed in smoke or fumes, they should also seek medical attention. Some symptoms may be delayed and can include coughing, a sore throat, difficulty breathing, singed nasal hair or facial burns. See recovering from burns and scalds for information on how serious burns are treated.

61
Summary of Fundamentals of Hot Stone Massage Hot Stone massage is a wonderful compliment to any massage practice. The techniques are easy to perform and to incorporate into an existing massage business. The equipment is inexpensive and easy to maintain and the therapeutic and financial benefits are substantial. I hope this overview of the fundamentals of Hot Stone massage will encourage you to explore this complimentary modality and to successfully include it in your catalog of services. Hot Stone massage began to become popular in America in 1993. We know Hot Stone massage is popular with Spa customers It is difficult to find a spa that does not offer it. A variety of different stones can be used for a Hot Stone massage, including Volcanic Basalt Stones, Mexican Pebble, and river smoothed stones. You can often get stones that are good to use in a Hot Stone massage at a rock quarry or landscape company. You need about 40-50 stones to do a good job, although you can get by with less if you have to. The majority of stones in your collection should be about as big as the palm of your hand. You can place stationary stones on the Charka points, along the spine or on the hands. You must take special precautions with stationary stones because they might burn the client if they are not moving. You can you keep stationary stones on the soles of the feet by wrapping a scarf or a a cloth bandage around the foot and the stone. Hot stone massage is effective because heat has many therapeutic properties; it relaxes muscles,increases blood circulation, and lowers the concentration of pain producing toxic metabolites. Pregnant women should seek a doctor’s advice before getting a Hot Stone massage, and you should never perform one on a client that you suspect has a temperature (fever) or difficulty regulating their internal temperature. You use a 16-Quart Roasterto heat your stones, and you should start warming them up at least an hour before your appointment. A safe temperature range for warming your stones is 125-150 degrees. You can

62
decide if a stone is too hot to use by testing it against your fore arm (like a baby bottle), and if it is too hot to hold in your hand it is definitely too hot to use. You do not have to worry about maintaining contact with your client during a Hot Stone massage because as long as a Stone is touching the client you are considered to be in contact. When efflueraging with a stone, you should move the stones towards the heart. Remember that when you are using a stone to remove an adhesion stones do not yield like flesh, they penetrate and can bruise. To clean your stones you should use an antibacterial soap.

63
Certificate of Completion and Transcript In order to receive your certificate of completion and an updated transcript for this course you must complete and pass the quiz. Once we have received your quiz we will generate your certificate and transcript and both will be emailed to you. If you completed the last quiz during our business hours (Monday-Friday 8:00 am-5:00 pm Pacific Standard Time) it should be emailed to you within a few minutes. If you complete the last quiz after business hours, or on a weekened it will still be emailed to you as quickly as possible. We check the system every hour until midnight most days so it should go out within an hour of you taking it. If you take the last quiz after midnight you will probably have to wait until the next morning, we do sleep. Please give us a full 24 hours before you call us if you have not received your certificate and transcript. We pride ourselves on being very fast, but if there is a condition beyond our control (the Internet Service Provider is down, etc) it may take us longer than usual. Also please be aware that many people wait until the last minute to do their courses. For this reason, the last few days of the month (28th, 29th, 30th, etc) are usually very, very busy times for us so our turn around time may be a little slower-but it should still be within 24 hours. If it has been more than 24 hours and you still have not received your emailed certificate, by all means call us! The number is (209) 777-6305. Lost Certificates and Transcripts If you need another copy of your documents emailed to you we will gladly do that for free at any time, just go to the contact page on our website and ask for it.

64
Course Evaluation We would like to hear some feedback form you. You can complete the evaluation online by clicking this link: http://www.sasionline.com/courseevaluation.html If you are using the “embedded” version of this course you will not be able to click the link above but there should be one you can access on the webpage itself. Thanks for taking our course; we really appreciate your business and we hope you come back to us next time you need continuing education hours. We would also love it if you would “Like us” on facebook, you can find us at www.facebook.com/beyondmassageschool. Errata If you found a typo PLEASE LET US KNOW what page it is on and the paragraph and we will fix it ASAP. This book has 45,000 words in the course content alone. Some of those are going to be misspelled. We’re not perfect, but we strive to be- so help us out. Help and Technical Support We have worked hard to make this course as easy to use as possible, but it does rely on technology and sometimes there are factors that are out of our control (like your local internet provider, your computer, your browser version, the device you are using etc). If for some reason you are not able to access the quiz you can call us and let us know, and we will problem solve it for you. We have office hours, Monday-Friday 8:00 am-5:00 pm PST but you can call or email for help at any time after hours, I monitor the system every hour until I go to sleep, so call if you need to and I will do my best to help you. The number is (209) 777-6305.

65
Bibliography Beck, Mark F Theory and Practice of Therapeutic Massage. Milady 4 edition (2007) Alison Trulock Hot Stone Massage: The Essential Guide to Hot Stone and Aromatherapy Massage Sterling Publishing November 4, 2008
M. V. Hurley et al., Non-exercise physical therapies for musculoskeletal conditions, Best Practice & Research, Clinical Rheumatology, 2008.� 1C Brosseau L., Yonge K.A., Welch V. et al., Thermotherapy for treatment of osteoarthritis, the Cochrane library, 2003. 1A Petrofsky J., Berk L., Lee H., Moist heat or dry heat delayed onset muscle soreness, Journal of clinical medicine research, 2013. 2B Scott F. Nadler, DO, FACSM, Kurt Weingand, PhD, DVM, and Roger J. Kruse, MD; The Physiologic Basis and Clinical Applications of Cryotherapy and Thermotherapy for the Pain Practitioner, pain physician, 2004. 1A D. L. Kellogg Jr., In vivo mechanisms of cutaneous vasodilation and vasoconstriction in humans during thermoregulatory challenges, the American Physiological Society, 2006. 3A Hendee W.R., Physics of Thermal Therapy, Fundamentals and Clinical applications, By Taylor and Francis group, 2013. Heinrichs K., Textbook of medical physiology, Philadelphia, 1986. (chapter 16: superficial thermal modalities). Bleakley C.,McDonough S.,MacAuley D., The Use of Ice in the Treatment of Acute Soft-Tissue Injury: A Systematic Review of Randomized Controlled Trials, The American Journal of Sports Medicine; 2004. 1A Tricia J. Hubbard et al., Does Cryotherapy Improve Outcomes With Soft Tissue Injury? Journal of Athletic Training, 2004. 1A Ernst E., Fialka V., Ice freezes pain? A review of the clinical effectiveness of analgesic cold therapy, J pain symptoms manage, 1994. 5

66
11.0 11.1 Amin A. Algafly, Keith P. George, The effect of cryotherapy on nerve conduction velocity, pain threshold and pain tolerance, Br J Sports Med, 2007. 3B 12.0 12.1 Choi YJ et al. Therapeutic effects and immunomodulation of suanbo mineral water therapy in a murine model atopic dermatitis. 1B Hiroharu K., Kiichiro T., Effectiveness of Aquatic Exercise and Balneotherapy: A Summary of Systematic Reviews Based on Randomized Controlled Trials of Water Immersion Therapies, Journal of epidemiology, 2010. 1A Eversden L, Maggs F, Nightingale P, Jobanputra P., A pragmatic randomized controlled trial of hydrotherapy and land exercises on overall well-being and quality of life in rheumatoid arthritis, BMC Musculoskeletal Disorders, 2007. 2A Lacy A. Holowatz et al., Mechanisms of acetylcholine-mediated vasodilatation in young and aged human skin, The Physiological Society, 2005. 3B Swenson C et al. Cryotherapy in sports medicine. Scand J Med Sci Sports. 1996 Aug6(4) 1B 17.0 17.1 17.2 Kathleen A. Sluka, PhD, PT, Michelle R. Christy, MPT, Wendy L. Peterson, MPT, Staci L. Rudd, MPT, Stacie M. Troy, MPT, Reduction of pain-related behaviors with either cold or heat treatment in an animal model of acute arthritis, Archives of Physical Medicine and Rehabilitation, March 1999. 3B 18.0 18.1 Fahey T.D., Athletic training: principles and practice, Mayfield. 19.0 19.1 19.2 Oosterveld F.G.J., Rasker J.J., Effects of local heat and cold treatment on surface and articular temperature of arthritic knees, American college of rheumatology, 1994. 1B William E. Prentice, An Electromyographic Analysis of the Effectiveness of Heat or Cold and Stretching for Inducing Relaxation in Injured Muscle, The journal of orthopaedic and sports physical therapy, 1982. 1B
67
Steven E. Peres, David O. Draper, Kenneth L. Knight, Mark D. Ricard, Pulsed shortwave diathermy and prolonged long-duration stretching increase dorsiflexion range of motion more than identical stretching without diathermy, Journal of Athletic Training, 2003. 2B 22.0 22.1 22.2 Oosterveld F.G., Rasker J.J., Treating arthritis with locally applied heat or cold, semin Arthritis Rheum., 1994. 5 Chris Bleakley, Suzanne McDonough and Domhnall MacAuley; The Use of Ice in the TreatmentfckLRof Acute Soft-Tissue Injury: A Systematic Review of Randomized Controlled Trials; The American Journal of Sports Medicine; 2004; 32 (1); 251-261 [A1] Joseph H. Dykstra et al.; Comparisons of Cubed Ice, Crushed Ice, and Wetted Ice on Intramuscular and Surface Temperature Changes; Journal of Athletic Training; 2009;44(2); 136–141 [A2]

68
APPENDIX I Thermotherapy Study Thermotherapy. An alternative for the treatment of American cutaneous leishmaniasis. Liliana López1, Martha Robayo2, Margarita Vargas2 and Iván D Vélez1* * Corresponding author: Iván D Vélez [email protected] Author Affiliations 1 Program for the Study and Control of Tropical Disease, University of Antioquia, Carrera 53 #61-30, Medellín, Colombia 2 Dirección de Sanidad, DISAN, Colombia Army, Bogotá, Colombia
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Abstract Background Pentavalent antimonials (Sb5) and miltefosine are the first-line drugs for treating cutaneous leishmaniasis in Colombia; however, toxicity and treatment duration negatively impact compliance and cost, justifying an active search for better therapeutic options. We compared the efficacy and safety of thermotherapy and Meglumine antimoniate for the treatment of cutaneous leishmaniasis in Colombia. Method An open randomized Phase III clinical trial was performed in five military health centres. located in northwestern, central and southern Colombia. Volunteers with parasitological positive diagnosis (Giemsa-stained smears) of cutaneous leishmaniasis were included. A single thermotherapy session involving the application of 50°C at the center and active edge of each lesion. Meglumine antimoniate was administered intramuscularly at a dose of 20 mg Sb5/kg weight/day for 20 days. Results Both groups were comparable. The efficacy of thermotherapy was 64% (86/134 patients) by protocol and 58% (86/149) by intention-to-treat. For the Meglumine antimoniate group, efficacy by protocol was 85% (103/121 patients) and 72% (103/143) by intention-to-treat, The efficacy between the treatments was statistically significant (p 0.01 and <0.001) for analysis by intention to treat and by protocol, respectively. There was no difference

69
between the therapeutic response with either treatment regardless of the Leishmania species responsible for infection. The side effects of Meglumine antimoniate included myalgia, arthralgia, headache and fever. Regarding thermotherapy, the only side effect was pain at the lesion area four days after the initiation of treatment. Conclusion Although the efficacy rate of Meglumine antimoniate was greater than that of thermotherapy for the treatment of cutaneous leishmaniasis, the side effects were also greater. Those factors, added to the increased costs, the treatment adherence problems and the progressive lack of therapeutic response, make us consider thermotherapy as a first line treatment for cutaneous leishmaniasis. Registered ClinicalTrials.gov NCT00471705 Keywords: Thermotherapy; American cutaneous leishmaniasis; Meglumine antimoniate; treatment Background Leishmaniasis is a group of diseases caused by parasites from the Leishmania genus. It is transmitted by female insects from the Lutzomyia genus in America and Phlebotomus in the Old World, affecting humans and domestic and wild mammals [1,2]. It is endemic in more than 98 countries. There are 2 million new cases per year, of which 1.5 million present in the cutaneous form [3]. In Colombia, there has been a reappearance of leishmaniasis. During the years of 2005–2008, 61,120 new cases were diagnosed. Among these cases, 34,262 (56.1%) occurred in National Army soldiers Statistical data (Dirección de Sanidad del Ejército (DISAN)). Since the 1940s, the pentavalent antimonials (Sb5) (Meglumine antimoniate and sodium stibogluconate) have been considered first line medications for the treatment of leishmaniasis. In Colombia, health authorities recommend a 20 mg Sb5/kg/day dose for 20 days to treat cutaneous leishmaniasis and 28 days of therapy to treat mucosal leishmaniasis (ML) and visceral leishmaniasis (VL) [4]. However, the pentavalent antimonials are expensive (approximately $200 per patient), cardiotoxic (P wave prolongation, inverted T waves, ST elevation and QT prolongation), hepatotoxic (liver enzymes elevation),

70
nephrotoxic (BUN and creatinine elevation) and can also cause pancreatitis, leukopenia, thrombocytopenia, arthralgia and myalgia. These complications, in combination with the parenteral route and the duration of treatment, cause adherence problems. Antimonials are contraindicated during pregnancy and lactation, in very young children, in patients with hypersensitivity to the drug and in patients suffering from chronic conditions. Some reports have shown a decrease in the sensitivity of Leishmania parasites to antimonials [3-13]. In the Old World leishmaniasis caused by L. (L) tropica, the parasite resistance is the main problem for the use of antimony [14,15]. Therefore, all of the factors mentioned above reinforce the need for alternative therapies. Several oral medications have been tested for the treatment of CL, such as dapsone [16], ketoconazol [17,18], mefloquine [19], allopurinol [20], miltefosine [21-25] and others [4], none of which are completely effective. Comparisons of the efficacy of different drugs are complicated by the different protocols used in each study. According to a recent meta-analysis of clinical trials for CL, this lack of standardization of methodologies makes it impossible to obtain conclusive information [4,26,27]. Some studies have shown that it is possible to induce healing of lesions by treatment with local heat [28-30]. Ethnomedical studies have shown that, in rural communities of South America and Africa, the empiric application of caustic materials (powder, hot brown sugar, silver nitrate, oil, battery) or the cauterization of the lesions with hot metal objects (spoons, knifes) is very common [31-33]. Currently, we employ the local application of an instrument, maintained at 50°C, called Thermomed®. This equipment was used in this study [34]. In addition to the benefits of local treatment, the cost of thermotherapy is significantly lower than the pentavalent antimony. The antimony cost is approximately USD 37.2, which must be added on to the patients disability, medical test before, during and after treatment, and in cases where it is needed, the electrocardiogram. According to calculations by dermatologist of the study, the total cost of local heat therapy, does not exceed USD 20 [3].

71
The objective of this study was to evaluate the efficacy and safety of Thermotherspy compared with Meglumine antimoniate for the treatment of Cutaneous Leishmnaniosis in Colombia. Materials and methods Study design We conducted an open randomized, phase III clinical trial to compare the differences in efficacy and safety between thermotherapy and Meglumine antimoniate. Population and site of the study The study was conducted between June 2006 and April 2008. The subjects were adult males enlisted in the Colombian Army. The study took place in five military health clinics in the northeast, south and central regions of Colombia. Inclusion Criteria Patients included in this study met the following criteria: a) positive parasitologic diagnosis of leishmaniasis, b) no previous treatment for this parasitic infection, c) laboratory exams including renal, hepatic and hematologic testing and d) voluntary agreement to participate in the study. Exclusion criteria Patients with the following characteristics were excluded: a) chronic concomitant diseases, b) lesions compromising the mucosa, c) presence of 10 or more cutaneous lesions with a negative Montenegro test or d) cutaneous lesions located less than 2 cm from the nasal or oral mucosa, eyes or near the anal or urogenital orifices. Interventions Thermotherapy (Thermomed®, Thermosurgery Inc. Phoenix-USA). Following the aseptic preparation of the lesions and local anesthesia with 2% xylocaine, we applied a single session of thermotherapy to the center, active borders and peripheral area of the lesions. Each thermal application was at 50°C and lasted for 30 seconds; the number of applications depended on the size of the lesion. After the thermotherapy session and over the next 10 days, an antibiotic ointment (fusidic acid) was applied over the lesions, which were then covered with sterile gauze to prevent secondary infections. Meglumine antimoniate (Glucantime®, Aventis, Paris, France) was administered intramuscularly under medical supervision at a

72
dose of 20 mg Sb5/kg/day for 20 days. All patients of both groups remained within the military unit for the duration of the treatment. Data collection and samples After providing writing informed consent, all patients were given a medical chart with pertinent demographic information, lesion data and a review of inclusion/exclusion criteria. We subsequently photographed each lesion. Histologic samples were taken from all patients to confirm the diagnosis and to identify the type of Leishmania using PCR-RFLP, according to published guidelines [35]. Clinical samples were taken from all subjects for the parasitological confirmation of leishmaniasis by direct microscopic examination, lesion aspirate samples were taken from each of the patients and were processed as explained in other publications [35,36]. In brief, the aspirates were cultured in NNN culture medium, incubated at 26°C, and from the fourth day on they were observed weekly for one month, in the inverted microscope in search of promastigotes. The media cultures were labeled with the code of each participant and were stored on independent racks to avoid mixing. Each week positive cultures were mass cultured in 50 ml glass bottles with NNN modified medium, one part was frozen in liquid nitrogen and is now stored in the PECET Criobank, and the other was used for species identification; for the DNA extraction, Promastigotes cultures were centrifuged and washed three times for 5 min at 1000 g in PBS pH 7.6. Parasites were then re-suspended in 200 μl of lysis buffer (10 mM Tris–HCl, pH 8,5 mM EDTA, 0.5% SDS, 200 mM NaCl, 100 μg/ml proteinase K) for 90 min at 65°C with moderate agitation. DNA was precipitated by adding two volumes of absolute ethanol to the lysate and the solution was mixed by inversion, and centrifuged for 15 min at 10,000 g. To recover the DNA, the supernatant was discarded and the pellet was dried for 15 min at 65°C and then re-suspended in 200 μl of water or TE. Then for the PCR amplification of the Cpb gene. Due to the partial degree of variability of the Cpb sequence between the Viannia and Leishmania subgenus, Cpb-specific primers were designed using the primer3plus software (http://www.bioinformatics.nl/cgibin/primer3plus/primer3plus.cg webcite). A region of the Cpb gene in L. (V) panamensis, L. (V) braziliensis and L. (V) guyanensis were amplified with the primers FwNTerBra (5´-ATGACGGTGCCGAGGGTCCT-3´) and RvCTerBra (5’-CTACTTGAACGTGCAGAT-3’); while primers FwRGPS (5’-ATGGCGACGTCGAGGGCC-3’) and RvRGPS (5’-

73
CAGGTGTTCATGATCGAGCCC-3’) were used for L. (L) mexicana and L. (L) infantum; To amplify the Cpb region of L. (L) amazonensis the primers FwRPAMZ (5’-GGATCCATACACGTGGGCACGCCG-3’) and RvRPAMZ (5’-AAGCTTCTACGTGTAGTGACAGGT-3’) were used. These last pair of primers also amplify for L. (L)Mexicana. After each PCR round, 5 μl of the product were separated in a 1% agarose gel and stained with 0,5 μg/ml of ethidium bromide. DNA products were visualized using a Chemidoc image analyzer system (Bio-Rad, Hercules, California, USA). In order to identify the Leishmania species by RFLP, the NEBcutter V2.0 programme (New England Biolab, Ipswich, Massachusetts, USA) was used to generate species-specific restriction sites. To differentiate L. (V) panamensis from L. (V) braziliensis, 10 μl of the amplification product was digested with KpnI (Promega), the mix was incubated for 6 h at 37°C. To differentiate L. (V) panamensis from L. (V) guyanensis, 10 μl of the amplification product was digested with NsiI (New England Biolab), this mix was incubated for 16 h at 37°C. To differentiate L. (L) mexicana from L. (L) amazonensis, 10 μl of the amplification product was digested, with NarI (New England Biolab), and the mix was incubated for 6 h at 37°C. To differentiate L. (L) mexicana from L. (L) infantum, 10 μl of the amplification product was digested with KpnI (Promega). After digestion, products were separated in 1% or 2% agarose gel using the same conditions described above for visualizing the PCR-Cpb amplification products[37,38]. Assignment to the treatment group Subjects were assigned randomly to treatment groups using a generated list in blocks of eight (EpiInfo 3.1). Only the clinical coordinator of the study had access to the list and was in charge of allocating treatments. Follow-up and outcomes Subjects receiving Meglumine antimoniate were evaluated at the beginning and end of treatment, at 6 weeks and at 3 and 6 months after completing the treatment. Subjects receiving thermotherapy were evaluated on the same day they started the treatment, at days 10 and 20, at 6 weeks and at 3 and 6 months after the application of heat, although thermotherapy was applied in an only session the followup of the healing process of the lesions was carried out three weeks after application, coinciding with the visit of final treatment of the group that received Meglumine antimoniate. All patients underwent renal, hepatic, pancreatic and hematologic blood function tests before, during and after the completion of treatment. The

74
assessment of side effects was done according to the Common Terminology Criteria for Adverse Events v.3 (CTCAE)[39]. The treatment response was evaluated clinically. For each lesion, the following definitions were used: Initial healing Complete reepithelialization of all ulcers and complete loss of induration up to three months after the end of treatment. Definitive healing Initial healing criteria without any recurrence six months after the completion of treatment. Failure Increase in size of a lesion of more than 50% at the end of treatment or an absence of clinical response at 6 weeks (lesion size reduction less than 50% compared to the evaluation at the end of treatment), signs of lesion activity 3 months after the completion of treatment or recurrence or presence of mucosal leishmaniasis at any time 6 months after the end of treatment. Recurrence Lesion reactivation in the original site after cicatrization. Reinfection Presence of new lesions at an anatomic site different from the original lesions after the patient was considered healed and after returning to endemic areas. In all subjects that had a treatment failure, Meglumine antimoniate was provided as rescue therapy at a dose of 20 mg Sb5/kg/day for 20 days, according to the Colombian Ministry of Health guidelines [40]. Sample size calculation The sample size was calculated assuming a thermotherapy efficacy of 78%, Meglumine antimoniate efficacy of 90%, confidence interval (CI) of 95% and power of 80% (non-inferiority trial). To this sample size number, we added 20% to account for possible loss of subjects to follow-up. The total sample size was 144 subjects per group for a total of 288 participants.

75
Statistical analysis Data entry and data analysis were performed using ACCESS and SPSS v.15, respectively. The baseline characteristics of volunteers were categorized and analyzed by treatment group. The treatment efficacy was calculated by intention-to-treat and by protocol. The relative risk was calculated using 2x2 tables. For hypothesis tests in dichotomic variables, we used the Fisher's Test or X2 test. The student's t-test or the “U of Mann–Whitney” test was used to analyze continuous data. Potential confounding factors and interactions were controlled with analysis stratified by parasite species, number, location, type of lesions and geographic area where the infection occurred. Statistical survival analysis was performed using the Kaplan-Meier method and the log rank test to compare the healing time between both groups. A p value of <0.05 was considered as stastically significant and CI of 95% was used for data analysis. Results We included 292 subjects in the study and randomly assigned 149 to receive thermotherapy and 143 to receive Meglumine antimoniate. In the thermotherapy group, two subjects did not want to participate (1%), 13 (9%) did not complete the six month follow-up and a total of 134 (90%) completed the study. In the Meglumine antimoniate group, 18 (13%) did not complete the six month follow-up, 2 (1%) withdrew from the Army before completing the study, 2 (1%) died in combat and 121 (85%) completed the study, as shown in Figure 1. Recurrences Recurrence was reported in 6 (4.1%) and 4 (3%) patients for the thermotherapy and Meglumine antimoniate groups, respectively. All of these patients received Meglumine antimoniate as a rescue treatment, and only one patient, who was assigned to the Meglumine antimoniate group, required a third treatment with amphotericine B. All recurrences occurred within 3 months of treatment completion. Baseline analysis As shown in Table 1, both groups had similar demographic, clinical and parasitologic characteristics. Therapeutic response Initial healing

76
Three months after the end of treatment, 64% (95% IC 56–72) of the thermotherapy group and 78% (95% IC 71–85) of the Meglumine antimoniate group were healed. Definitive healing A total of 7 patients (4.8%) from the thermotherapy group and 7 (5%) from the Meglumine antimoniate group did not complete follow-up with the 3- and 6-month evaluations. By protocol, 64% (95% IC 55–73) of patients in the thermotherapy group and 85% (95% IC 64–80) of patients in the Meglumine antimoniate group showed definitive healing. By intention-to-treat, the definitive healing rate in the thermotherapy group was 58.5% (95% IC 49–66) and 72% (95% IC 78–92) in the Meglumine antimoniate group, as shown on Table 2. The efficacy analysis between both treatments showed a statistically significant difference, for the analysis by protocol the Meglumine antimoniate is 0.33 times more effective than thermotherapy (RR 1.33 (IC 95% 1.15 – 1.54) p <0.001), when analysis was carried out by intention to treat, the superiority of the Meglumine antimoniate maintained, being 0.25 more effective than thermotherapy (RR 1.25 (IC 95% 1.05 – 1.48) p <0.001). Group analysis We identified Leishmania species as agents of infection in 167 patients. In the group treated with Meglumine antimoniate, 32 patients (38%) had lesions caused by L. (V) panamensis and 52 (62%) by L. (V) brazililensis. In the thermotherapy group, 24 patients (29%) had lesions caused by L. (V) panamensis and 59 (71%) by L. (V) brazililensis. The healing response in the Meglumine antimoniate group, among patients with L. (V) panamensis and L. (V) braziliensis, was of 72% and 65%, respectively. In the thermotherapy group, the healing response was 58% for L. (V) panamensis and 53% for L. (V) braziliensis. There was no association found between the treatment (Meglumine antimoniate, p = 0.5, and thermotherapy, p = 0.6) and the Leishmania species identified. There was also no association between treatment and other variables such as number, location and lesion type or with the geographical area of Colombia where the infection occurred (Table 3). Safety

77
Table 4 shows the systemic and local side effects found in this study. Frequency and severity of side effects were greater in the Meglumine antimoniate group. These side effects occurred during and after treatment. These side effects included fever, myalgia, arthralgia and headache. In the group treated with thermotherapy, we found an association with local pain, especially four days after initiating treatment (p = <0.001). In all laboratory analysis conducted during and at the end of treatment with Meglumine antimoniate, there were alterations in renal, hepatic, pancreatic and hematologic tests. There was an association with increased amylase levels (p < 0.005), which reached grade 3 in some cases[39]. Severe side effects Three patients experienced serious adverse effects, none of which were related to medications (2 died in combat and 1 was wounded by a knife). These three patients were part of the Meglumine antimoniate group. Survival analysis The Meglumine antimoniate group experienced significantly fewer failures to treatment (15%) compared to the thermotherapy group (36%) (log rank = 9.6, p = <0.001). Discussion This study followed procedures delineated by the GCP. The sample size was adequate for the study. The follow-up rate was 88% at six months after treatment, which was higher than estimated when calculating the sample size. In the Meglumine antimoniate group, treatment efficacy by protocol and intention-to-treat were 85 and 72%, respectively. These results demonstrate a decrease in the rate of efficacy for this age group, which was reported as 93% during the 1990s [41-43]. This decrease in the efficacy of antimonials could be related, among other factors, to the administration of incomplete doses as a consequence of adherence problems, unavailability of a complete dose to all patients, black market of medications in rural areas and evidence that men also play a role in the transmission of American cutaneous leishmaniasis [29]. There was no statistically significant difference in terms of treatment efficacy with leishmania species.

78
Thermotherapy had an efficacy of 64 and 58% per protocol and intention-to-treat, respectively; these results are comparable to the findings reported by a study in Kabul, Afghanistan, (CL due to L. (L) tropica) in which the efficacy per protocol was 69% [44]. In other study made with patients from other Asian countries (Irán and Kuwait), following the same conditions of application of local heat and where the isolated specie was L. (L) major, the intent efficacy of thermotherapy to treat was 48%, two months after treatment ends[45]. With regard to efficiency, we found that Meglumine antimoniate is statistically superior to thermotherapy for the treatment of CL in Colombia (p < 0.001), but we also found that Meglumine antimoniate has been associated with severe side effects in the musculoskeletal system (myalgia and arthralgia), fever, headaches [4] and toxicity in organs such as the kidney, the pancreas and the hematologic and cardiovascular systems. These effects are not associated with thermotherapy, which only causes local pain four days after the initiation of treatment. Systemic treatment with pentavalent antimonials for cutaneous leishmaniasis caused by L. (V) panamensis and L. (V) braziliensis was recommended by the WHO in 1990 under the assumption that such treatment prevents the development of mucosal lesions[46]. However, subsequent studies conducted in Peru demonstrated that mucosal lesions may appear despite the use of these therapeutic schemes. In the case of Colombia, where the predominant parasite species are L. (V) braziliensis and L. (V) panamensis, the need for all patients to receive systemic treatment of 20 mg Sb5/kg/day for 20 days is even more controversial, especially because the incidence of mucosal leishmaniasis is less than 0.5% although it is estimated that, in rural areas far from health centers, only 10% of the population with CL receives complete treatment with antimonials [28-30]. Unpublished data (Dirección de Sanidad del Ejército (DISAN) and Programa de Estudio y Control de Enfermedades Tropicales (PECET)) documented 12 fatalities related to the use of this therapy, which is unacceptable for a form of the disease that is not fatal. Thermotherapy has been evaluated in several American and Old World countries with efficacy rates of more than 70%. In Colombia, only one report of thermotherapy used to treat CL was made in an epidemic area of L. (V) guyanensis. In this region, thermotherapy had an efficacy of 100 and 19% by protocol and intention-to-treat, respectively, although the lack of

79
follow-up in many patients (81%) decreased the efficacy of the study and limited the interpretation of results[47]. The facts mentioned previously led us to ponder the convenience of using local treatments (thermotherapy, paromomicine, cryotherapy, intra-lesion pentavalent antimony) in combination with patient education on how to detect early signs and symptoms of mucosal complications so they can be promptly reported to the physician and addressed with systemic treatment. The results of the present study show that thermotherapy could be considered a valid alternative treatment due to its efficacy (>60%) and safety as well as because it requires a single session and does not require laboratory monitoring. Although the equipment required for thermotherapy (ThermoMed) is very expensive and difficult to access in endemic countries due to its cost, the expenses related to conventional treatment overweigh the costs of Thermomed. With the goal of increasing its efficacy, we propose a subsequent clinical trial to evaluate new schemes of application of local treatment with thermotherapy; for example, patients may undergo 2–3 sessions or a combination of local treatments with a low systemic dose. Conclusions Although the efficacy rate of Meglumine antimoniate was greater than that of thermotherapy for the treatment of cutaneous leishmaniasis, the side effects were also greater. Those factors, added to the increased costs, the treatment adherence problems and the progressive lack of therapeutic response, make us consider thermotherapy as a first line treatment for cutaneous leishmaniasis. The thermotherapy is also a valid alternative in patients with renal, hepatic and cardiac illness who cannot receive systemic therapy. It is important to mention that thermotherapy should not be applied near mucosal areas. Ethical approval The protocol was approved by the Bioethics Committee for Human Research of “Sede de Investigacion Universitaria” (CBEIH-SIU) from the University of Antioquia and by the Ethics Committee of the General Health

80
Management of the Colombian Army and and carried out according to international norms of good clinical practice Consent informed Before deciding to participate in the research, All patients signed a informed consent form in the presence of two witnesses. Abbreviations CL, Cutaneous leishmaniasis; ML, Mucosal leishmaniasis; VL, Visceral leishmaniasis; CTCAE, Common Terminology Criteria for Adverse Events; CI, Confidence Interval; PECET, Programa de Estudio y Control de Enfermedades Tropicales; DISAN, Dirección de Sanidad del Ejército. Competing interest The authors declare that they have no competing interests. Authors' contributions LL coordinated and conducted the field work, participated in the design and reporting of the study; MR and MV carried out field work (inclusion and follow-up of volunteers); IV participated in the design, execution and reporting of the study. All authors read and approved the final manuscript. IV is guarantor of the paper. Authors' information LL MSc. Clinical Trials Coordinator PECET. MR Dermatologist, Colombia Army. MV Dermatologist, Colombia Army. IV MD MSc PhD. Director PECET, Professor University of Antioquia - Colombia, member of the "Data Management Team" TDR/WHO, Clinical Monitor TDR/WHO. Acknowledgements The authors express gratitude to the “Ministerio de Protección Social” and especially to Dr. Julio Cesar Padilla for his support and co-funding of this study. We also thank the personnel of the Colombian Army directed by General Mario Montoya Uribe, who supported and made the execution of this study possible. Thanks also to the staff from the “Direccion de Sanidad del Ejercito”, especially Colonels Erwin Solarte Rodríguez and Fernando Pineda, TC David Rojas Tirado, TC Gonzalo Godoy Mendez and the Army team of dermatologists (Coronel Ximena Sánchez, TC Alvaro Sandoval, TC

81
Gustavo Pérez and MY Claudia Cruz) for their support of the study. Thanks to the staff of Learning and Control of Tropical Diseases, Dra. Sara Robledo, Daniel Agudelo and Ronald and Eugenia Pelaez Cardona. Thanks to Dr. Piere Buffet (Hôpital Pitie Salpetriere in Paris) for reviewing this manuscript. We would also like to thank all of the patients for their willingness and commitment to the study. Funding Funding was provided by the Social Protection Ministry of the Republic of Colombia, which did not participate in the design, implementation, analysis or report of this project. References Bailey MS, Lockwood DN, 2: Cutaneous leishmaniasis. Clin Dermatol 2007, 25:203-211. Mar-Apr PubMed Abstract | Publisher Full Text OpenURL Bejarano EE, Sierra D, Perez-Doria A, Velez ID: First finding of Lutzomyia tihuiliensis (Diptera: Psychodidae) in the Valle de Aburra, Colombia. Biomedica 2006, 26(Suppl 1):228-231. PubMed Abstract OpenURL WHO (World Health Organization).Control of the leishmaniases. 2010. OpenURL Gonzalez U, Pinart M, Rengifo-Pardo M, Macaya A, Alvar J, Tweed JA: Interventions for American cutaneous and mucocutaneous leishmaniasis. Cochrane Database Syst Rev 2009, 2:CD004834. PubMed Abstract | Publisher Full Text OpenURL Arevalo I, Tulliano G, Quispe A, Spaeth G, Matlashewski G, Llanos-Cuentas A, et al.: Role of imiquimod and parenteral meglumine antimoniate in the initial treatment of cutaneous leishmaniasis. Clin Infect Dis 2007, 44(12):1549-1554. PubMed Abstract | Publisher Full Text OpenURL Berman JD: Treatment of New World cutaneous and mucosal leishmaniases. Clin Dermatol 1996, 14(5):519-522. Sep-Oct PubMed Abstract | Publisher Full Text OpenURL Kedzierski L, Sakthianandeswaren A, Curtis JM, Andrews PC, Junk PC, Kedzierska K: Leishmaniasis: current treatment and prospects for new drugs and vaccines. Curr Med Chem 2009, 16(5):599-614. PubMed Abstract | Publisher Full Text OpenURL Murray HW, Berman JD, Davies CR, Saravia NG: Advances in leishmaniasis. Lancet 2005, 366(9496):1561-1577. Oct 29-Nov 4 PubMed Abstract | Publisher Full Text OpenURL Ouellette M, Drummelsmith J, Papadopoulou B: Leishmaniasis: drugs in the clinic, resistance and new developments. Drug Resist Updat 2004, 7(4–5):257-266. Aug-Oct PubMed Abstract | Publisher Full Text OpenURL Palumbo E: Current treatment for cutaneous leishmaniasis: a review. Am J Ther 2009, 16(2):178-182. Mar-Apr PubMed Abstract | Publisher Full Text OpenURL Sampaio RN, de Paula CD, Sampaio JH, Furtado Rde S, Leal PP, Rosa TT, et al.: The evaluation of the tolerance and nephrotoxicity of pentavalent antimony administered in a dose of 40 mg Sb V/kg/day, 12/12 hr, for 30 days in the mucocutaneous form of leishmaniasis. Rev Soc Bras Med Trop 1997, 30(6):457-463. Nov-Dec PubMed Abstract | Publisher Full Text OpenURL Seaton RA, Morrison J, Man I, Watson J, Nathwani D: Out-patient parenteral antimicrobial therapy–a viable option for the management of cutaneous leishmaniasis. QJM 1999, 92(11):659-667. PubMed Abstract | Publisher Full Text OpenURL Soto J, Soto P: Current situation and future of antileishmanial therapy in Colombia. Biomedica 2006, 26(Suppl 1):194-206. PubMed Abstract OpenURL Hadighi R, Mohebali M, Boucher P, Hajjaran H, Khamesipour A, Ouellette M: Unresponsiveness to Glucantime treatment in Iranian cutaneous leishmaniasis due to drug-resistant Leishmania tropica parasites. PLoS Med 2006, 3(5):e162. PubMed Abstract | Publisher Full Text | PubMed Central Full Text OpenURL

82
Hadighi R, Boucher P, Khamesipour A, Meamar AR, Roy G, Ouellette M, et al.: Glucantime-resistant Leishmania tropica isolated from Iranian patients with cutaneous leishmaniasis are sensitive to alternative antileishmania drugs. Parasitol Res 2007, 101(5):1319-1322. PubMed Abstract | Publisher Full Text OpenURL Osorio LE, Palacios R, Chica ME, Ochoa MT: Treatment of cutaneous leishmaniasis in Colombia with dapsone. Lancet 1998, 351(9101):498-499. PubMed Abstract | Publisher Full Text OpenURL Momeni AZ, Aminjavaheri M, Omidghaemi MR: Treatment of cutaneous leishmaniasis with ketoconazole cream. J Dermatolog Treat 2003, 14(1):26-29. PubMed Abstract | Publisher Full Text OpenURL Singh S, Singh R, Sundar S: Failure of ketoconazole treatment in cutaneous leishmaniasis. Int J Dermatol 1995 Feb, 34(2):120-121. Publisher Full Text OpenURL Hendrickx EP, Agudelo SP, Munoz DL, Puerta JA, Velez Bernal ID: Lack of efficacy of mefloquine in the treatment of New World cutaneous leishmaniasis in Colombia. Am J Trop Med Hyg 1998 Dec, 59(6):889-892. OpenURL Velez I, Agudelo S, Hendrickx E, Puerta J, Grogl M, Modabber F, et al.: Inefficacy of allopurinol as monotherapy for Colombian cutaneous leishmaniasis. A randomized, controlled trial. Ann Intern Med 2010, 126(3):232-236. OpenURL Soto J, Berman J: Treatment of New World cutaneous leishmaniasis with miltefosine. Trans R Soc Trop Med Hyg 2006 Dec, 100(Suppl 1):S34-S40. OpenURL Soto J, Toledo JT: Oral miltefosine to treat new world cutaneous leishmaniasis. Lancet Infect Dis 2007 Jan, 7(1):7. OpenURL Velez I, Lopez L, Sanchez X, Mestra L, Rojas C, Rodriguez E: Efficacy of miltefosine for the treatment of American cutaneous leishmaniasis. Am J Trop Med Hyg 2010, 83(2):351-6. PubMed Abstract | Publisher Full Text | PubMed Central Full Text OpenURL Mohebali M, Fotouhi A, Hooshmand B, Zarei Z, Akhoundi B, Rahnema A, et al.: Comparison of miltefosine and meglumine antimoniate for the treatment of zoonotic cutaneous leishmaniasis (ZCL) by a randomized clinical trial in Iran. Acta Trop 2007 Jul, 103(1):33-40. Publisher Full Text OpenURL Esmaeili J, Mohebali M, Edrissian GH, Rezayat SM, Ghazi-Khansari M, et al.: Evaluation of miltefosine against Leishmania major (MRHO/IR/75/ER): in vitro and in vivo studies. Acta Med Iran 2008, 46(3):191-196. OpenURL Bari AU, Rahman SB: A Therapeutic update on Cutaneous leishmaniasis. J Coll Physicians Surg Pak 2003 Aug, 13(8):471-476. OpenURL Willard RJ, Jeffcoat AM, Benson PM, Walsh DS: Cutaneous leishmaniasis in soldiers from Fort Campbell, Kentucky returning from Operation Iraqi Freedom highlights diagnostic and therapeutic options. J Am Acad Dermatol 2005 Jun, 52(6):977-987. Publisher Full Text OpenURL Levine N: Cutaneous leishmaniasis treated with controlled localized heating. Arch Dermatol 1992 Jun, 128(6):759-761. Publisher Full Text OpenURL Navin TR, Arana BA, Arana FE, de Merida AM, Castillo AL, Pozuelos JL: Placebo-controlled clinical trial of meglumine antimonate (glucantime) vs. localized controlled heat in the treatment of cutaneous leishmaniasis in Guatemala. Am J Trop Med Hyg 1990 Jan, 42(1):43-50. OpenURL Velasco-Castrejon O, Walton BC, Rivas-Sanchez B, Garcia MF, Lazaro GJ, Hobart O, et al.: Treatment of cutaneous leishmaniasis with localized current field (radio frequency) in Tabasco, Mexico. Am J Trop Med Hyg 1997 Sep, 57(3):309-312. OpenURL Moreira Rda C, Rebelo JM, Gama ME, Costa JM: Knowledge level about of American tegumentary leishmaniasis (ATL) and use of alternative therapies in an endemic area in the Amazon Region in the State of Maranhao, Brazil. Cad Saude Publica 2002, 18(1):187-195. Jan-Feb PubMed Abstract | Publisher Full Text OpenURL Velez ID, Hendrickx E, Robledo SM, del Pilar Agudelo S: Gender and cutaneous leishmaniasis in Colombia. Cad Saude Publica 2001, 17(1):171-180. Jan-Feb PubMed Abstract | Publisher Full Text OpenURL Weigel MM, Armijos RX: The traditional and conventional medical treatment of cutaneous leishmaniasis in rural Ecuador. Rev Panam Salud Publica 2001, 10(6):395-404. PubMed Abstract | Publisher Full Text OpenURL Adams E: Thermosurgery in dermatology. Boston,. MA: Thecnology Assessment Program, Office of Patient Care Services 2008. OpenURL Ramirez JR, Agudelo S, Muskus C, Alzate JF, Berberich C, Barker D, et al.: Diagnosis of cutaneous leishmaniasis in Colombia: the sampling site within lesions influences the sensitivity of parasitologic diagnosis. J Clin Microbiol 2000, 38(10):3768-3773. PubMed Abstract | Publisher Full Text | PubMed Central Full Text OpenURL Robinson RJ, Agudelo S, Muskus C, Alzate JF, Berberich C, Barker DC, et al.: The method used to sample ulcers influences the diagnosis of cutaneous leishmaniasis. Trans R Soc Trop Med Hyg 2002, 96(Suppl 1):S169-S171. PubMed Abstract OpenURL Montalvo Alvarez AM, Nodarse JF, Goodridge IM, Fidalgo LM, Marin M, Van Der Auwera G, et al.: Differentiation of Leishmania (Viannia) panamensis and Leishmania (V.) guyanensis using BccI for hsp70 PCR-RFLP. Trans R Soc Trop Med Hyg 2010, 104(5):364-7. PubMed Abstract | Publisher Full Text OpenURL Montalvo AM, Monzote L, Fraga J, Montano I, Muskus C, Marin M, et al.: PCR-RFLP and RAPD for typing neotropical Leishmania. Biomedica 2008, 28(4):597-606. PubMed Abstract | Publisher Full Text OpenURL Trotti A, Colevas AD, Setser A, Rusch V, Jaques D, Budach V, et al.: CTCAE v3.0: development of a comprehensive grading system for the adverse effects of cancer treatment. Semin Radiat Oncol 2003 Jul, 13(3):176-181. Publisher Full Text OpenURL Guía de atención de la leishmaniasis. Ministerio de la Proteccion Social, Bogotá; 2007. PubMed Abstract OpenURL Soto JTJ, Vega J, Berman J: Short report: efficacy of pentavalent antimony for treatment of colombian cutaneous leishmaniasis.

83
Am J Trop Med Hyg 2005, 72(4):421-422. Apr PubMed Abstract | Publisher Full Text OpenURL Palacios R, Osorio LE, Grajalew LF, Ochoa MT: Treatment failure in children in a randomized clinical trial with 10 and 20 days of meglumine antimonate for cutaneous leishmaniasis due to Leishmania viannia species. Am J Trop Med Hyg 2001, 64(3–4):187-193. PubMed Abstract | Publisher Full Text OpenURL Vélez IDA, del Pilar Agudelo S, Hendrickx E, Puerta JA, Grogl M, Modabber F, et al.: Inefficacy of allopurinol as monotherapy for colombian cutaneus leishmaniasis. Ann Intern Med 1997, 126:232-236. PubMed Abstract | Publisher Full Text OpenURL Reithinger RMM, Wahid M, Bismullah M, Quinnell RJ, Davies CR, et al.: Efficacy of thermotherapy to treat cutaneous leishmaniasis caused by Leishmania tropica in Kabul, Afghanistan: a randomized, controlled trial. Clin Infect Dis 2005, 40(8):1148-1155. Apr 15 PubMed Abstract | Publisher Full Text OpenURL Aronson NE, Wortmann GW, Byrne WR, Howard RS, Bernstein WB, Marovich MA, et al.: A randomized controlled trial of local heat therapy versus intravenous sodium stibogluconate for the treatment of cutaneous Leishmania major infection. PLoS Negl Trop Dis 2010, 4(3):628. Publisher Full Text OpenURL Tuon FF, Amato VS, Graf ME, Siqueira AM, Nicodemo AC, Amato Neto V: Treatment of New World cutaneous leishmaniasis–a systematic review with a meta-analysis. Int J Dermatol 2008 Feb, 47(2):109-124. Publisher Full Text OpenURL Vega JC, Sanchez BF, Montero LM, Montana R, Mahecha Mdel P, Duenes B, et al.: The efficacy of thermotherapy to treat cutaneous leishmaniasis in Colombia: a comparative observational study in an operational setting. Trans R Soc Trop Med Hyg 2009 Jul, 103(7):703-706. Publisher Full Text OpenURL

84
APPENDIX II Ice Massage versus Conventional Icing: a comparison on the effectiveness of each in the inflammation phase of healing Chris Pantellere Therapeutic Modalities Dr Sterner 1 December 2008 Ice Massage versus Conventional Icing: a comparison on the effectiveness of each in the inflammation phase of healing A. Introduction Cryotherapy is the application of cold between the therapeutic temperatures of 32°F and 65°F. For ages, cryotherapy has been an acceptable modality of choice for acute soft tissue trauma.1 Cryotherapy has been used since the days of the ancient Greeks and its practice if evident in today’s health care providers. Cryotherapy is the easiest and most readily available modality, making cryotherapy one of the most widely used modalities in the athletic training setting. In previous studies cryotherapy techniques have shown to alter the effects of the acute inflammation phase in healing tissues.1,2 Many researchers in the past have studied the effect of icing techniques with little comparison between ice massage and conventional icing. The purpose of this paper is to examine these two different cryotherapy techniques and determine which would be more effective in treating acute injuries and injuries in the inflammation phase of the healing process. B. How does the body react to trauma? In order to fully understand the effect of cryotherapy on the body’s healing process, we must first investigate what happens when there is trauma to bodily tissues. The healing process is broken down into several different aspects; first the acute inflammatory phase, second the repair phase, and lastly the remodeling phase.3 For the purposes of this paper the investigator will focus on the acute inflammation phase. The acute inflammation phase is the first and one of the most important phases of healing. If something were to go wrong in the healing process in this phase, there could be serious setbacks.4 The inflammation phase is triggered by some sort mechanical trauma ranging from a cut to a fracture. This mechanical stimulus will cause a release of inflammatory mediators which will in turn cause a vascular, cellular, and immune responses which all occur simultaneously. Someone can tell that an

85
individual is in the acute inflammatory phase by recognizing the cardinal signs of inflammation.3,4 1. Vascular response The vascular response is comprised of two segments. In the first response, which takes place immediately after an injury, there is a vasoconstriction at the arteriole and venule level which lasts five to ten minutes.1,3 This vasoconstriction’s purpose is an attempt to slow hemorrhaging and allow blood platelets to ‘patch up’ the damaged vessels. This process of the vascular repair is called the clotting cascade.1,3 The second response by the vascular system is triggered by a series of chemical reactions to cause vasodilation of the vessels. This vasodilation will bring in more blood to the area as well as, increase the permeability of the vessel.1 The chemical reaction that triggers this vasodilation attracts leukocytes which clean up the debris and toxins left behind after the injury. The increased permeability of the vessel is what allows these large leukocytes and blood to cross across to the injured area.1,3 This vascular permeability and influx of blood, proteins, and leukocytes is what causes edema. Although this edema brings aid to the injured tissue it can also cause severe trauma. A pressure buildup can occur on healthy tissues and cause a secondary hypoxic injury due to lack of oxygen. In addition these leukocytes can kill healthy cells.3 2. Cellular response The cellular response occurs simultaneously with the vascular response. Once trauma is detected chemical mediators trigger the vascular response. Other chemical mediators will also alert the body to send leukocytes which use phagocytosis to clean and repair the area.1 First to act are the neutrophils, followed by monocytes and macrophages.1,3 These cells play a large role in the repair of structures and are a cause of swelling and edema. 3. Immune response This segment of the inflammatory response is mediated by hormones and is complimented by the vascular system.1 The lymphatic and vascular systems are responsible for removing lymph and wastes throughout the body. In the inflammation phase it will help to remove these wastes and leukocytes that help clean the area of debris. C. The physical properties of ice 1. How does ice work? The common misconception with ice is the way people think it works. Many believe that ice directly cools the tissues it is in contact with, but in fact there is a constant reaction going on.3 As ice comes into contact with

86
the body, there is an obvious difference in body temperatures and the temperature of the ice. This difference in temperatures will cause the skin will give heat to the ice in an attempt to warm (melt) the ice.3,4,5 As the superficial tissue layers are brought to a lower temperature the superficial layers will draw heat from the deeper tissues in affect cooling the deeper tissues.4,5 This transfer of kinetic energy between two different temperatures is called the enthalpy of fusion.3 This energy transfer can be administered a number of different ways but the most common method is conduction. Conduction will transfer kinetic energy by coming in direct contact between the different temperatures, which we commonly see with cryotherapy.3,4,5 After the ice is removed from the area and if the individual remains sedentary the tissues will continue to cool.4 If an individual begins exercise or even to walk the tissues will begin to re-warm but if they remain still, five to ten more minutes of cooling will occur. This will result in a longer effect of the modality, making it more effective.3,5 2. Factors that affect kinetic energy transfer Thermal energy can be affected by a number of different variables. The size of the treatment area will have a huge affect on the effects of ice.4 The larger the treatment area the more energy transfer will occur and will cause a deeper penetration of the modality.3 The duration of the treatment time will also affect the rate of cooling. The longer the ice is left on, the greater the cooling rates of the tissue will occur. The temperature difference between the ice and tissue will also affect the cooling rates.2,4,5 The greater this temperature difference the faster cooling will take place. The body itself can also have adverse effects on cooling as well. The body’s natural insulator is adipose tissue. Adipose tissue retains body temperature which has affect on the rate of cooling as well as the rate of penetration.2,3,4,5 Higher levels of fat can prevent deep musculature from being cooled and requires longer treatment times in order to penetrate as deep as someone with less adipose tissue.2 D. Physiological responses to ice application 1. Effects of the vascular system If you recall when an injury occurs there can be a secondary hypoxic injury due to a vasodilation of the vessels. One of the first effects of ice application on the body’s systems is a vasoconstriction of the area where ice is being applied. This vasoconstriction can lower the healthy cells metabolic rate, therefore lowering the cells need for oxygen.1,2,3,4,5 For every 1.8°F decrease in tissue temperature metabolic rate will decrease thirteen percent.3 This vasoconstriction can also influence the amount of

87
edema formation by limiting the amount of hemorrhaging but it will not remove it.2,4,5 2. Effects on pain Pain perception can be altered by cryotherapy’s ability to alter nerve conduction velocity.6 All types of nerve fibers will be affected by cold application, particularly their synapses.3,6 One study said reported a decrease of 33% in nerve conduction velocity of sensory fibers after a 10 degree decrease in skin temperature.6 The same study said, the same decrease in skin temperature lowered motor nerve firing rates by 14%.6 The decreased sensory fibers will decrease the sensation of pain by the gate theory.3,6 A decrease in motor nerve fibers firing rates will reduce muscle spasm caused by injury, theoretically breaking the pain-spasm-pain cycle.2,4,5,6 Muscle spindle sensitivity will also be affected which will override the stretch reflex which will also affect spasm.6 The faster the skin is cooled and nerve conduction velocities are lowered, the faster analgesia will occur.4,5 3. Proprioception and muscular function Although sensory fibers are affected through ice application, proprioception is not altered.6 This is because propriocepive nerves have very low thresholds and are thickly myelinated, located deep in tissues.6 Since motor nerves and muscle spindles are altered by cold to reduce spasm and pain, we can expect to see a decrease in muscular function.5,6 One study indicated after a 20 minute cold application eccentric, concentric, and isokinetic contractions all decreased as did endurance and power.6 It has been theorized that short term icing can decrease the need for oxygen while maintaining full muscular ability.6 E. Ice Massage 1. What is ice massage? Ice massage is a cryotherapy technique that is usually administered in a manner so the clinician can keep the ice moving.3 Typically, water is frozen in a cup at 0-2°C then a portion of the cup is removed leaving some portion of the cup allowing the clinician to grip the modality.7,8 A tool in which a tongue depressor is frozen into the ice can be used as a grip, essentially making a round, flat popsicle.9 The ice is then moved in a circular or longitudinal manner over the affected area.3 Previous studies have shown that using a treatment area no larger than three times the surface of the ice so intramuscular temperatures can be lowered enough to cause metabolic rate.7,8,9,10 The limited amount of ice prevents clinicians from treating larger areas. 2. Cooling rates and depth of penetration

88
Almost immediately after ice massage is applied to the skin, the skin’s temperature begins to drop very rapidly.8 Waylonis reported that in the first five minutes of ice massage skin temperatures decreased 18.9°C on the gastrocnemius.8 Another study reported a 26.6°C decrease in skin temperature after a ten minute application.7 This same study by Bugaj stated that the rate of skin cooling is 2.7°C by ice massage.7 He also stated that re-warming took place at 1.9°C.7 However, it seems that ice massage has more difficulty affecting intramuscular temperatures.8 Waylonis reported the same five minute application of ice massage caused a 2.6°C decrease at a depth of 2.0cm.8 However, another study reported a 15.9°C decrease at 2.0cm deep for a similar five minute application.7 These studies also attempted ice massage for longer periods of time in an attempt to further decrease intramuscular temperatures.7,8,9,11 Lowdon and Moore reported after a ten minute ice massage application to the gastrocnemius caused a decrease in 18.4°C at 2.0 cm deep.11 They also said that a fifteen minute application caused a 20.4°C decrease at the same depth.11 Waylonis has much different results stating, a ten minute application lowered the temperature 5.2°C at the same depth of Lowdon and Moore.8 Waylonis also recorded the temperature change at 3 and 4cm deep.8 A ten minute application resulted in a decrease of 1.4°C at 3.0cm, and .1°C at 4.0cm deep.7,8 3. Effects on nerve conduction velocity and pain The circular or longitudinal movements produced on the skin can not only lower nerve conduction velocities of the pain sensing A-delta and C-fibers, but it can also stimulate the A-beta fibers.7,8 These large diameter fibers activate the gate theory, in sense beating the noxious stimuli to the spinal cord and modulating pain sensation.7,8,11 This decrease in pain will reduce the spasm caused by the injury.3 Cooling rates can be increased by applying more pressure with the icing implement.6,7,8,9 Studies have shown that a decrease in 7.4°C causes a decreased nerve conduction velocity of 33%.7,8 Ice massage has been shown to lower skin temperatures 26.6°C on the thigh after a tem minute ice massage application.8,9 Normal skin temperature is 33°C, a decrease of 26.6°C would bring skin temperature to 6.4°C. This is well below the 14.4°C which is when maximum analgesia occurs.7,9 F. Conventional icing 1. What is conventional icing? Conventional icing is providing cryotherapy through ice bag application to the injury site. In addition the area is compressed with an elastic wrap to enhance cooling effects as well as aid in venous and

89
lymphatic return.9,12,13 Ice can either be crushed or cubed produced by ice machines storing the ice just above 0°C.3 Before the ice bag is applied excess air must be taken out of the ice bag so the bag can conform to the injured area.9 Multiple ice bags can be used allowing larger treatment areas.12 These ice bags can be wrapped in moist towels.3,9,12 This provides insulation of the ice bag which helps the ice stay cooler for longer. This is not necessary for conventional icing but it can help transmission.12 2. Cooling rates and depth of penetration Ice bag application with compression has been shown to lower skin temperature 20.3°C after a 20 minute application.13 Another study showed a 13.1°C reduction after a 20 minute ice bag application without compression.12 It also seems that conventional icing can penetrate deeper and more effective than ice massage.9 Although one study states that after thirty-nine minutes of conventional icing without compression, lowered tissues 8°C at 2.0cm deep.9 The same study states, that when conventional icing is added with compression a thirty minute treatment time lowered intramuscular temperatures 13°C at the same depth.9 Another study has shown that conventional icing with compression caused a reduction in 12.7°C at 2.0cm deep.13 3. Effects on nerve conduction velocity and pain Dependent on adipose tissue levels maximum analgesia is usually produced within twenty minutes of conventional icing with compression. One study says conventional icing took nearly forty-five minutes to reach maximal analgesia.9 It could have been that this study had larger individuals who may have had more adipose tissue. Studies have shown that there is little difference between the rates at which nerve conduction velocities lower between conventional icing and ice massage.6,9 A-beta fibers are not stimulated as with ice massage application. G. Discussion 1. Pros/cons of ice massage and conventional icing Each application of cryotherapy surely has their place when it comes to management of the inflammation phase of healing.9 Each modality has positive and negative aspects that will lead a clinician to make a choice between each technique. With conventional icing, the fact that we can increase the rate of cooling and aid lymphatic return by adding compression is the biggest advantage.14 Although we can add compression to areas after ice massage, the combination of cold and compression is far more effective in reducing edema.14,15 Another positive point of conventional icing is that it allows clinicians to treat a larger area that is injured.3 The small amounts of ice used in ice massage limits us to

90
use a treatment size no larger than three times the diameter of the ice.7,8,9 Ice massage is a very effective modality in its own sense. Ice massage can help reduce spasm by activating A-beta fibers as well as lowering the conduction velocities.6,7,8,9 This is very helpful in treating flat even areas where there is spasm or pain.7 Ice massage can reduce skin temperatures faster than conventional icing, but it doesn’t penetrate as deep as deep.9 Even though some studies have shown the ability to cool intramuscular temperatures as much as 13°C results vary.6,7,8,9 For the most part, ice massage has shown little effect on intramuscular temperatures.8 This could be due to different methods of data collection or, differences in the amount of the subject’s adipose tissue. Certainly there is a need for a standard protocol to measure temperature changes, as well as an agreed upon amount adipose tissue levels of test subjects. Ice massage is inexpensive, easily accessible, and simple enough for a client to use. Patients can take several ice cups home after they have sustained and injury in practice if ice massage is preferred. Conventional icing also requires an ice machine which can be expensive and unreliable if not operating properly. 2. Clinical applications of injuries in the acute inflammation phase Ice massage although has its disadvantages certainly can be useful in the primary care of acute injuries. Instances in which ice massage can be used to manage acute inflammation conditions include: Acute bursitis of the elbow or the knee, acute strains to superficial tendons (i.e. biceps femoris, pes anserine muscle group, extensor carpi radialis/ulnaris, abductor pollicis brevis/longus, and extensor pollicis brevis/longus), volar plate and collateral ligament trauma of the phalanxes, strains to the trapezius, as well as the thenar and hypothenar eminences. In addition compression sleeves can be applied to bursitis conditions as well as, injuries to the digits of the hand.7,8,9 Conventional icing should be performed on larger areas of the body.13 Particularly where there are high levels of adipose tissue or where deep cooling is desired. If the athletic trainer does not have access to modalities such as electric stimulation, ice, compression, and elevation can be used immediately after the injury to reduce hemorrhaging and edema.13,14,15 We can also surround a joint with multiple ice bags in the case of severe knee injuries.12 The larger the area needed to be treated as well as, how deep penetration is needed will determine the modality the clinician uses.3 H. Conclusion Cryotherapy’s clinical use dates back to the days of the ancient Greeks when they discovered it can alleviate pain.3 All forms of

91
cryotherapy provide vasoconstriction, analgesia, altered nerve conduction velocities, and reduce the chance of secondary hypoxic injury by decreasing cell metabolism.1,2,3,4,5 Cryotherapy can be administered a number of different ways, but the therapeutic goals and phase of the healing process will determine the choice of application.1 Conventional icing can be used to treat larger, deeper areas, and entails compression which can help reduce edema.13 Ice massage has proven to cause analgesia faster than conventional icing but there is also less amount of penetration and no compression with the ice.9 Previous research has shown varied results for ice massage and there is a need for standardized measurements.7,8 Ice massage and conventional icing each have their own purposes in the inflammation phase of healing. In order to use each appropriately more research on these forms of cryotherapy must be administered with standardized methods in order to help clinicians determine the best course of treatment. Works Cited 1. Kellett, J. Acute soft tissue injuries-a review of the literature. Medicine & Science in Sports & Exercise. 1986;18(5):489-500. 2. Meeusen R, Lievens P. The Use of Cryotherapy in Sports Injuries. Sports Medicine. 1986;3(6):398-414. 3. Starkey C. Therapeutic Modalities. 3rd ed. Philadelphia, PA: FA Davis; 2004. 4. Swenson C, Sward L, Karlsson J. Cryotherapy in sports medicine. Scandinavian Journal of Medicine and Science in Sports. 1996;6:193-200. 5. Tepperman PS, Devlin M. Therapeutic heat and cold: a practitioner’s guide. Postgraduate Medicine. 1983;73(1):69-76. 6. Algafly AA, George KP. The effect of cryotherapy on nerve conduction velocity, pain threshold and pain tolerance. British Journal of Sports Medicine. 2007;41:365-369. 7. Bugaj R. The Cooling, Analgesic, and Rewarming Effects of Ice Massage on Localized Skin. Physical Therapy. 1975;55(1):11-19. 8. Waylonis G. The Physiologic Effects of Ice Massage. Archives of Physical Medicine and Rehabilitation. 1967;48(1):37-42. 9. Zemke JE, Anderson JC, Guion WK, McMillan J, Joyner AB. Intramuscular Temperature Responses in the Human Leg to Two Forms of Cryotherapy: Ice Massage and Ice Bag. Journal of Orthopaedics and Sports Physical Therapy.1998;27(4):301-307. 10. Borgmeyer JA, Scott BA, Mayhew JL. The effects of Ice massage on Maximum Isokinetic-Torque Production. Journal of Sport Rehabilitation. 2004;13:1-8. 11. Lowdon BJ, Moore RJ. Determinants and nature of intramuscular temperature changes during cold therapy. American Journal of Physical Medicine. 1975;54(5):223-233. 12. Kennet J, Hardaker N, Hobbs S, Selfe J. Cooling Efficiency of 4 Common Cryotherapeutic Agents. Journal of Athletic Training. 2007;42(3):343-348. 13. Merrick MA, Knight KL, Ingersoll CD, Potteiger JA. The Effects of Ice and Compression Wraps on Intramuscular Temperature at Various Depths. Journal of Athletic Training. 1993;29(3):236-245. 14. Bleakley CM, McDonough SM, MacAuley DC. Cryotherapy for Acute Ankle Sprains: A Randomized Controlled Study of Two Different Icing Protocols. British Journal of Sports Medicine. 2006;40:700-705. 15. Enwemeka CS, Allen C, Avila P, Bina J, Konrade J, Munns S. Soft Tissue Thermodynamics before, during, and after cold pack therapy. Medicine & Science in Sports & Exercise. January 2001;34(1):45-50.

92
APPENDIX III Human thermoregulation and the cardiovascular system Human thermoregulation and the cardiovascular system José González-Alonso Abstract A key but little understood function of the cardiovascular system is to exchange heat between the internal body tissues, organs and the skin to maintain internal temperature within a narrow range in a variety of conditions that produce vast changes in external (exogenous) and/or internal (endogenous) thermal loads. Heat transfer via the flowing blood (i.e. vascular convective heat transfer) is the most important heat-exchange pathway inside the body. This pathway is particularly important when metabolic heat production increases many-fold during exercise. During exercise typical of many recreational and Olympic events, heat is transferred from the heat-producing contracting muscles to the skin surrounding the exercising limbs and to the normally less mobile body trunk and head via the circulating blood. Strikingly, a significant amount of heat produced by the contracting muscles is liberated from the skin of the exercising limbs. The local and central mechanisms regulating tissue temperature in the exercising limbs, body trunk and head are essential to avoid the deleterious consequences on human performance of either hyperthermia or hypothermia. This brief review focuses on recent literature addressing the following topics: (i) the dynamics of heat production in contracting skeletal muscle; (ii) the influence of exercise and environmental heat and cold stress on limb and systemic haemodynamics; and (iii) the impact of changes in muscle blood flow on heat exchange in human limbs. The paper highlights the need to investigate the responses and mechanisms of vascular convective heat exchange in exercising limbs to advance our understanding of local tissue temperature regulation during exercise and environmental stress. Heat production in skeletal muscle Heat is produced in all body cells from the conversion of metabolic energy into mechanical and thermal energy. This process is very inefficient and thus approximately 30–70% of the energy liberated during muscle contraction appears as thermal energy (Edwards et al. 1975; González-Alonso et al. 2000b; Bangsbo et al. 2001; Krustrup et al. 2001, 2003). Heat production by dynamically contracting human skeletal muscle increases abruptly and markedly at the onset of dynamic exercise, increases further

93
at a lower rate during the early stages of exercise and eventually plateaus if exercise is of a steady-state nature. When exercise is intense, however, heat production does not level off, as illustrated in Fig. 1. A doubling in heat production is seen over 3 min of intense dynamic exercise, with half of the increase occurring during the first 38 s (González-Alonso et al. 2000b). Heat production in dynamically contracting muscle in conditions of unrestricted flow is estimated by measuring the amount of heat accumulated in the contracting muscles, the amount of heat removed by the blood to the body trunk and the amount of heat loss from the exercising limb skin. When looking at each subdivision (in conditions in which heat exchange with the surroundings of the thigh is minimized by a thermostatically isolated system and the circulation to the lower leg is arrested), heat storage in the active quadriceps muscles accounts for the immediate elevation in heat production, whereas heat removal to the body trunk via the blood is dominant at the end of exercise. Rates of total heat production and its subdivisions in terms of storage in the quadriceps muscle and removal by the blood to the body trunk are depicted for each 5 s of exercise. Note that heat storage in the quadriceps muscle accounts for the immediate increase in heat production, decreasing progressively thereafter. Conversely, heat removal by the blood is nil at the onset of exercise, increasing progressively thereafter to account for most of heat production at the end of the 180 s of exercise. (Modified from González-Alonso et al. 2000b.) The elevation of total heat production over time in contracting skeletal muscle is tightly coupled with changes in heat liberation during metabolic ATP production early in exercise (González-Alonso et al. 2000; Bangsbo et al. 2001; Krustrup et al. 2001, 2003). As depicted in Fig. 2, the contribution of anaerobic energy turnover to total energy turnover (i.e. the sum of total heat production and mechanical power output) is greatest at the onset of exercise, becoming smaller as the contribution of aerobic energy turnover increases. In vitro studies have shown that heat production during ATP utilization varies from 35 to 72 kJ (mol ATP)−1 depending upon whether creatine phosphate (PCr), glycolysis or oxidative phosphorylation provides the energy for ATP resynthesis (Wilkie, 1968; Curtin & Woledge, 1978). Hence, both in vitro and in vivo studies show that muscle heat production can increase during high-intensity dynamic exercise by a factor of two, with a shift in ATP resynthesis from primarily PCr catabolism to primarily oxidative phosphorylation.

94
image Figure 2. Total, anaerobic and aerobic energy turnover during intense dynamic knee-extensor exercise Rates of total and aerobic energy turnover and heat liberation for each 5 s period of intense dynamic knee-extensor exercise. Note that anaerobic heat liberation accounts for most of the total energy turnover at the onset of exercise, whereas aerobic heat liberation is dominant after some 45 s of exercise. (Modified from González-Alonso et al. 2000b.) Heat storage in body tissues depends upon the interplay among heat production, heat dissipation and, to a lesser extent, energy exchanged during mechanical work. Excessive heat accumulation or liberation compromises the physiological function of cellular and organ systems, which can lead to impaired human performance (González-Alonso et al. 2008a; Taylor et al. 2008). A well-developed control system is therefore required to regulate heat exchange within the body and between the skin and the environment. The two avenues of heat exchange inside the body are ‘intercellular conductive heat transfer’ and ‘vascular convective heat transfer’. Heat conductance through tissues in the human body is a slow process and, in limbs, is primarily dependent upon the temperature gradient between muscle and skin and the thermal conductivity of muscle. This avenue of heat exchange is particularly important in conditions of exercise in cold environments, which produces a large temperature gradient between deep muscle and neighbouring subcutaneous tissue and skin (Werner et al. 2008). Conversely, it plays no role when there is not a temperature gradient between muscle and surrounding skin, as during exposure to warm environments. In contrast, convective heat transfer (mass flow) from dynamically contracting limb muscles to the core of the body and to the surrounding subcutaneous limb tissues hinges upon tissue blood flow and arteriovenous blood temperature difference (according to the Fick principle; González-Alonso et al. 2000b). Hence, conditions that alter either limb tissue blood flow and/or arteriovenous blood temperature difference, such as exercise and/or environmental stress, are likely to induce profound changes in convective heat exchange within the exercising limbs and between the exercising limbs and the body torso. Conversely, when exercise is performed in ischaemic conditions (e.g. when limb circulation is arrested by inflation of a cuff), convective heat removal to the

95
body truck is nil and thus heat accumulates in the muscle (Edwards et al. 1975; Krustrup et al. 2003). The body of literature discussing the processes involved in heat liberation from the skin to the environment is very extensive. The reader is referred to two excellent reviews on the biophysics and physiology of heat exchange between the body and the environment (Gagge & Gonzalez, 1996; Werner et al. 2008). On the contrary, the number of studies directly investigating the processes involved in heat exchange inside the human body, particularly in contracting limb skeletal muscle, is relatively small due partly to the complexity of performing the necessary invasive measurements of tissue blood flow and blood and tissue temperature gradients. The focus of this paper is on the latter aspect of temperature regulation. Cardiovascular responses to exercise and environmental stress The circulatory adjustments to exercise and environmental stress are integrative responses to a vast collection of external and internal stimuli. Based on the external stimuli, the haemodynamic responses to environmental stress and exercise are determined by the magnitude of the environmental (heat or cold) load and the duration, intensity and type of exercise. The environmental conditions and the type and intensity of exercise determine the metabolic and thermal demands for local and systemic blood flow, whereas exercise duration defines the regulatory disturbances and constraints in cardiovascular function over time (Rowell et al. 1996; González-Alonso et al. 2008a; Mortensen et al. 2008). Depending upon the amount of muscle mass engaged, exercise can generally be classified as small or large muscle mass exercise. Single-limb exercise, such as forearm and isolated leg exercise, are examples of small muscle mass exercise, whereas whole-body exercise, such as cycling, running and rowing, are considered large muscle mass exercise. The effects of heat and cold stress during exercise on cardiovascular function are most likely to differ during small compared with large muscle mass exercise when exercise intensity is high (Mortensen et al. 2008). From a mechanistic physiology viewpoint, the combination of intense whole-body exercise and heat stress poses the greatest challenge to the regulation of temperature, mean arterial pressure and oxygen delivery to the working muscles, brain and heart, because in these conditions the cardiovascular system is pushed faster to the limit of its regulatory capacity (Rowell et al. 1996; González-Alonso et al. 2008).

96
Prolonged whole-body exercise in the heat is associated with greater tachycardia, skin and core hyperthermia, but conflicting systemic and exercising limb blood flow responses compared with equivalent exercise in the cold (Claremont et al. 1975; McArdle et al. 1976; Nadel et al. 1979; Sawka et al. 1979; Montain & Coyle, 1992; González-Alonso et al. 1998, 2000a). The lack of control for subjects’ hydration status, randomization of the experimental trials and familiarization of the participants with the experimental conditions might explain, at least in part, the discrepancy in the blood flow responses in the literature. In this context, people lose more body water during exercise in the heat due to higher sweat rates and thus become more dehydrated than during exercise in the cold. The question then arises as to how distinct levels of dehydration impact upon the cardiovascular responses to exercise and environmental stress. Figure 3 depicts the results from a study investigating the influence of environmental temperature and hydration status on the cardiovascular responses to moderately intense leg cycling (González-Alonso et al. 2000a). Subjects were randomly tested at 35 and 8°C ambient temperatures when euhydrated and dehydrated by 1.5, 3.0 and 4.5% of their body weight. When subjects were euhydrated and core temperature and oxygen uptake (inline image) were the same during exercise in both environments, cardiac output was elevated by �1 l min−1 in the heat, accompanied by a higher heart rate but an unchanged stroke volume. This elevated systemic blood flow might have been a response to the threefold higher skin blood flow during exercise in the heat, as the metabolic and thermal demands for exercising muscle blood flow were apparently the same. Note that cardiac output was elevated in the heat in normal hydration conditions, but in contrast to exercise in the cold it declined significantly with increasing levels of dehydration owing to the greater decline in stroke volume (González-Alonso et al. 2000a). *Significantly different from the euhydrated control condition. †Significantly different from exercise in the cold at the same hydration level The circulatory responses to a given level of dehydration, however, vary in cold and hot environments. In contrast to the well-characterized cardiovascular strain evoked by dehydration during exercise in the heat (Sawka et al. 1979; Montain & Coyle, 1992; González-Alonso et al. 1998), graded dehydration up to 4% of body weight loss (i.e. 3 kg for a 70 kg person) does not reduce cardiac output, skin blood flow, arterial blood

97
pressure or systemic vascular conductance during exercise in the cold. Consequently, cardiac output, and possibly active muscle blood flow (González-Alonso et al. 1998), is lower during moderate intensity exercise in the heat compared with exercise in the cold when dehydrated by 4%, which is the opposite response to what occurs in the euhydrated state. Hydration status can therefore explain part of the discrepancy in the cardiac output responses to environmental stress and intense whole-body exercise reported in the literature. The literature directly comparing the effects of environmental heat and cold stress on the haemodynamic responses to small muscle mass exercise is sparse (e.g. Savard et al. 1988), yet evidence in resting limbs is extensive. Studies in resting limbs generally show that heat stress increases blood flow to the arms and legs, whereas cold stress reduces limb perfusion (e.g. Barcroft & Edholm, 1943). A highly controversial issue, however, is whether these differences in limb perfusion reflect changes only in skin blood flow or in both muscle and skin blood flow. With respect to heat stress, early investigations into the partition of limb perfusion between skin and skeletal muscle in the human forearm led to conflicting results, with some studies suggesting an elevation in muscle blood flow (Barcroft & Edholm, 1946; Barcroft et al. 1947), but others not (e.g. Rodie et al. 1956; Detry et al. 1972; Johnson et al. 1976). The negative findings together with the estimate of maximal skin blood flow of 6–8 l min−1, based on indirect measures of cardiac output and visceral blood flow during whole-body heat stress, promoted the idea that increases in skin blood flow with heat stress accounted fully for the rise in systemic hyperaemia and blood flow redistribution (Detry et al. 1972; Rowell 1974; Minson et al. 1998). Recent evidence in the human leg, however, challenges this widely held dogma. Using 133Xe washout or positron emission tomography techniques, Keller et al. (2010) and Heinomen et al. (2011) recently showed that passive leg heating increases calf blood flow by approximately 60–65%. In parallel, we have shown significant increases in leg tissue blood flow, deep femoral venous O2 content and muscle oxygenation and a parallel significant decline in leg arterial–deep venous O2 differences during whole-body heat stress, both at rest and during mild knee-extensor exercise, with a small effect or no effect on aerobic metabolism (Pearson et al. 2011). The enhanced muscle blood flow was closely associated with increases in arterial plasma ATP concentration and muscle temperature (Pearson et al. 2011), which is in turn coupled to a temperature-mediated release of ATP from erythrocytes (Kalsi & González-Alonso, 2012). On the other hand,

98
cold stress has repeatedly been shown to reduce limb blood flow in resting humans (e.g. Barcroft & Edholm, 1943; Gregson et al. 2011). For instance, the classic work of Barcroft & Edholm (1943) clearly showed lower forearm blood flows and deep muscle temperatures when the forearm was immersed in a water bath at 13, 20 and 25°C compared with higher water temperatures. Likewise, Gregson and co-workers recently reported a 35–40% decline in femoral artery blood flow and conductance following 10 min of cold and temperate water immersion (8 versus 22°C), which evoked drastic decreases in muscle and skin temperatures, but less cutaneous vasoconstriction at 8 than at 22°C water temperature, possibly reflecting a lower muscle blood flow (Gregson et al. 2011). Taken together, growing evidence from the human leg suggests that heat and cold stress not only alters blood flow to the skin, but also to the skeletal muscle. These circulatory adjustments might have important implications for heat transfer in resting and exercising human limbs. Muscle blood flow and limb heat liberation The flowing blood transports heat inside the body in relation to blood temperature and flow rate. Heat transfer in major arteries and veins supplying and draining the limbs is bidirectional. In normal resting conditions, limb muscle and venous blood temperatures are significantly lower than arterial and core temperature (González-Alonso et al. 1999; He et al. 2002; Fig. 4). In fact, blood temperature in the limb muscle microcirculation is normally several degrees lower than core temperature due to rapid thermal equilibration between tissues and vessels (He et al. 2002). At the level of the major supply vessels, the resulting negative arteriovenous temperature gradient indicates that more heat is being transferred from the upper body core to the extremities than vice versa (Fig. 4). This net body core-to-limbs heat transfer helps limbs to maintain tissue temperature when their metabolic heat production is low. For instance, leg inline image is normally about 25 ml min−1 in the resting state, corresponding to a total leg heat production of �0.5 kJ min−1 based on the heat equivalent of inline image (Bangsbo et al. 2000). This value is only half of the �1 kJ min−1 of heat being transferred from the body trunk to each leg when femoral venous temperature is �0.7°C lower than femoral arterial blood temperature, resting leg blood flow is �0.4 l min−1 and the blood specific heat is 3.61 kJ l−1°C−1 (Fig. 4). These simple estimates

99
demonstrate that more heat is transferred into the resting leg than produced locally in resting conditions. This implies that limb tissue temperature will drop if its circulation is arrested and heat dissipation to the surroundings of the limbs is kept constant. An example of this might occur during knee or elbow surgery. Note that muscle (Tm) and femoral venous temperatures (Tfv) are lower than core (Toes) and femoral arterial blood temperatures (Tfa) at the onset of submaximal leg cycling exercise (0–3 min for Tfa and 0–8 min for Tm), but increase very rapidly as exercise progresses. A net heat influx in the leg is observed at rest (0 min) and during the initial 5.5 min of exercise. A net heat efflux is seen thereafter. (Modified from González-Alonso et al. 1999.) The impact of alterations in limb perfusion on heat exchange between the body core and limbs can be exemplified from the findings of He et al. (2002) in the rat hindlimb. To the author's knowledge, comparable limb thermodynamic data are not available for humans. Femoral artery and vein blood flow was increased by infusion of the nitric oxide donor sodium nitroprusside (vasodilatation), normal (control) or reduced by infusion of noradrenaline (vasoconstriction; Fig. 5). Increases in blood flow were accompanied by parallel reductions in femoral arteriovenous temperature difference, thus net limb heat influx was the same. In contrast, when femoral artery blood flow was reduced, heat influx into the hindlimb was reduced, accompanying an essentially unchanged arteriovenous temperature gradient. Therefore, the findings of He and co-workers (2002) indicate that increasing limb blood flow in resting limbs does not necessarily increase the net amount of heat being transferred from the body trunk to the limbs because of compensatory tissue-to-blood thermal exchange adjustments within the leg tissues. However, reducing blood flow might have an impact on limb heat transfer. In the resting human leg, femoral venous blood temperature has been shown to decrease by up to 0.5°C with progressive increases in blood flow from 0.4 to 8 l min−1 evoked by intrafemoral artery infusion of ATP (González-Alonso et al. 2008b). Whether similar thermal adjustments to those described in the rat hindlimb occur in the human leg warrants detailed investigation. Note that increases in blood flow in the resting hindlimb do not change the net limb heat influx, because of compensatory changes in femoral

100
arteriovenous (a-v) temperature differences (drawn from data reported by He et al. 2002). *Significantly different from control. Exercise illustrates a different scenario, in which not only limb tissue perfusion and convective heat exchange, but also heat production increase. During the initial stages of leg exercise, the temperatures of the contracting muscle and the outflowing femoral venous blood increase at a faster rate than the temperatures of the inflowing femoral arterial blood and the upper body core (González-Alonso et al. 1999), yet a negative femoral arteriovenous blood temperature gradient prevails during the early stages of exercise, signifying that more heat is still transferred from the upper body core to the exercising limbs in normal environmental conditions (Fig. 4). After a few minutes of exercise (duration will depend on the initial temperatures and the rate of heat production or exercise intensity), muscle and venous blood temperature becomes higher than arterial blood and upper body core temperature. At this point in time, heat transferred from the exercising limbs to the body torso becomes positive, increasing thereafter to reach a plateau when exercise is of light-to-moderate intensity. To date, data on heat exchange in human limbs in different environmental and exercise conditions are very limited, thus the ideas discussed above require thorough scrutiny. Summary and future directions Our knowledge and understanding of human thermo-regulation and its interaction with cardiovascular regulation during exercise is largely based upon data from resting limbs. The observation that a significant amount of heat produced by the exercising muscles is liberated directly from the skin of the exercising limbs (González-Alonso et al. 1999) highlights the need to investigate the responses and mechanisms of vascular heat exchange in resting and exercising limbs. Quantification of heat production and convective heat exchange in human limbs is likely to shed new light onto the role of muscle blood flow in the control of tissue temperature during environmental stress and exercise. References Bangsbo J, Krustrup P, González-Alonso & Saltin B (2000). Muscle oxygen kinetics at onset of intense dynamic exercise in humans. Am J Physiol Regul Integr Comp Physiol 279, R899–R906. PubMed,CAS,Web of Science® Times Cited: 116 Bangsbo J, Krustrup P, González-Alonso J & Saltin B (2001). ATP production and efficiency of human skeletal muscle during intense exercise: effect of previous exercise. Am J Physiol Edocrinol Metab 280, E956–E964.

101
PubMed,CAS,Web of Science® Times Cited: 67 Barcroft H, Bonnar WM & Edholm OG (1947). Reflex vasodilatation in human skeletal muscle in response to heating the body. J Physiol 106, 271–278. PubMed,Web of Science® Times Cited: 46 Barcroft H & Edholm OG (1943). The effect of temperature on blood flow and deep temperature in the human forearm. J Physiol 102, 5–20. PubMed,CAS Barcroft H & Edholm OG (1946). Temperature and blood flow in the human forearm. J Physiol 104, 366–376. PubMed,Web of Science® Times Cited: 124 Claremont AD, Nagle F, Reddan WD & Brooks GA (1975). Comparison of metabolic, temperature, heart rate and ventilator responses to exercise at extreme ambient temperatures (0° and 35°C). Med Sci Sports 7, 150–154. CrossRef,PubMed,CAS,Web of Science® Times Cited: 37 Curtin NA & Woledge RC (1978). Energy changes and muscular contraction. Physiol Rev 58, 690–761. PubMed,CAS,Web of Science® Times Cited: 171 Detry JM, Brengelmann GL, Rowell LB & Wyss C (1972). Skin and muscle components of forearm blood flow in directly heated resting man. J Appl Physiol 32, 506–511. PubMed,CAS,Web of Science® Times Cited: 156 Edwards RH, Hill DK & Jones DA (1975). Heat production and chemical changes during isometric contractions of the human quadriceps muscle. J Physiol 251, 303–315. PubMed,CAS,Web of Science® Times Cited: 101 Gagge AP & Gonzalez RR (1996). Mechanisms of heat exchange: biophysics and physiology. In Handbook of Physiology, section 4, Environmental Physiology, ed. Fregly MJ & Blatteis CM, pp. 45–84. American Physiological Society, Bethesda , MD , USA . González-Alonso J, Calbet JAL & Nielsen B (1998). Muscle blood flow is reduced with dehydration during prolonged exercise in humans. J Physiol 513, 895–905. Direct Link: AbstractFull Article (HTML)PDF(356K)ReferencesWeb of Science® Times Cited: 100 González-Alonso J, Calbet JAL & Nielsen B (1999). Metabolic and thermodynamic responses to dehydration-induced reductions in muscle blood flow in exercising humans. J Physiol 520, 577–589. Direct Link: AbstractFull Article (HTML)PDF(292K)ReferencesWeb of Science® Times Cited: 65 González-Alonso J, Crandall CG & Johnson J (2008a). The cardiovascular challenge of exercising in the heat. J Physiol 586, 45–53. Direct Link: AbstractFull Article (HTML)PDF(400K)ReferencesWeb of Science® Times Cited: 32 González-Alonso J, Mora-Rodríguez R & Coyle EF (2000a). Stroke volume during exercise: interaction of environment and hydration. Am J Physiol Heart Circ Physiol 278, H321–H330. PubMed,Web of Science® Times Cited: 40 González-Alonso J, Mortensen SP, Jeppensen TD, Ali L, Barker H, Damsgaard R, Secher NH, Dawson EA & Dufour SP (2008b). Haemodynamic responses to exercise, ATP infusion and thigh compression in humans: insight into the role of muscle mechanisms on cardiovascular function. J Physiol 586, 2405–2417. Direct Link: AbstractFull Article (HTML)PDF(530K)ReferencesWeb of Science® Times Cited: 17
González-Alonso J, Quistorff B, Krustrup P, Bangsbo J & Saltin B (2000b). Heat production in human skeletal muscle at the onset of intense dynamic exercise. J Physiol 524, 603–615. Direct Link: AbstractFull Article (HTML)PDF(429K)ReferencesWeb of Science® Times Cited: 56 Gregson W, Black MA, Jones H, Minson J, Morton J, Dawson B, Atkinson G & Green DJ (2011). Influence of cold water immersion on limb and cutaneous blood flow at rest. Am J Sports Med 39, 1316–1323. CrossRef,PubMed,Web of Science® Times Cited: 3 He QLZ, Lemons DE & Weinbaum S (2002). Experimental measurements of the temperature variation along artery-vein pairs from 200 to 1000 microns diameter in rat hind limb. J Biomech Eng 124, 656–661. CrossRef,PubMed,Web of Science® Times Cited: 3 Heinonen I, Brothers RM, Kemppainen J, Knuuti J, Kalliokoski KK & Crandall CG (2011). Local heating, but not indirect whole-body heating, increases human skeletal muscle blood flow. J Appl Physiol 111, 818–824. CrossRef,PubMed,Web of Science® Times Cited: 2 Johnson JM, Brengelmann GL & Rowell LB (1976). Interactions between local and reflex influences on human forearm skin blood flow. J Appl Physiol 53, 744–749. Kalsi K & González-Alonso J (2012). Temperature-dependent release of ATP from human erythrocytes: Mechanism for the control of local tissue perfusion. Experimental Physiology, doi:10.1113/expphysiol.2011.064238 Direct Link: AbstractFull Article (HTML)PDF(414K)References Keller DM, Sander M, Stallknecht B & Crandall CG (2010). α-Adrenergic vasoconstrictor responsiveness is preserved in the heated human leg. J Physiol 588, 3799–3808. Direct Link: AbstractFull Article (HTML)PDF(296K)ReferencesWeb of Science® Times Cited: 6 Krustrup P, Ferguson RA, Kjaer M & Bangsbo J (2003). ATP and heat production in human skeletal muscle during dynamic exercise: higher efficiency of anaerobic than aerobic ATP resynthesis. J Physiol 549, 255–269. Direct Link: AbstractFull Article (HTML)PDF(452K)ReferencesWeb of Science® Times Cited: 35 Krustrup P, González-Alonso J, Quistoff B & Bangsbo J (2001). Muscle heat production and anaerobic energy turnover during repeated intense dynamic exercise in humans. J Physiol 536, 947–956.

102
Direct Link: AbstractFull Article (HTML)PDF(326K)ReferencesWeb of Science® Times Cited: 49 McArdle WD, Magel JR, Lesmes GR & Pechar GS (1976). Metabolic and cardiovascular adjustment to work in air and water at 18, 25 and 33°C. J Appl Physiol 40, 85–90. PubMed,CAS,Web of Science® Times Cited: 106 Minson CT, Wladkowski SL, Cardell AF, Pawelczyk JA & Kenney WL (1998). Age alters the cardiovascular response to direct passive heating. J Appl Physiol 84, 1323–1332. PubMed,CAS,Web of Science® Times Cited: 60 Montain SJ & Coyle EF (1992). Influences of graded dehydration on hyperthermia and cardiovascular drift during exercise. J Appl Physiol 73, 1340–1350. PubMed,CAS,Web of Science® Times Cited: 285 Mortensen SP, Damsgaard R, Dawson EA, Secher N & González-Alonso J (2008). Restrictions in systemic and locomotor skeletal muscle perfusion, oxygen supply and inline image during high-intensity whole-body exercise in humans. J Physiol 586, 2621–2635. Direct Link: AbstractFull Article (HTML)PDF(704K)ReferencesWeb of Science® Times Cited: 24 Nadel ER, Cafarelli E, Roberts MF & Wenger CB (1979). Circulatory regulation during exercise at different ambient temperatures. J Appl Physiol 49, 715–721. Web of Science® Times Cited: 258 Pearson J, Low DA, Stöhr EJ, Kalsi K, Ali L, Barker H & González-Alonso J (2011). Hemodynamic responses to heat stress in the resting and exercising human leg: insight into the effect of temperature on skeletal muscle blood flow. Am J Physiol Regul Integr Comp Physiol 300, R663–R673. CrossRef,PubMed,CAS,Web of Science® Times Cited: 1 Rodie IC, Shepherd JT & Whelan RF (1956). Evidence from venous oxygen saturation measurements that the increase in forearm blood flow during body heating is confined to the skin. J Physiol 134, 444–450. PubMed,Web of Science® Times Cited: 147 Rowell LB (1974). Human cardiovascular adjustments to exercise and thermal stress. Physiol Rev 54, 75–159. PubMed,CAS,Web of Science® Times Cited: 1136 Rowell LB, O’Leary DS & Kellogg DL Jr (1996). Integration of cardiovascular control systems in dynamic exercise. In Handbook of Physiology, section 12, Exercise: Regulation and Integration of Multiple Systems, ed. Rowell LB, Shepherd JT, chapter 17, pp. 770–838. Oxford University Press, New York . Savard GK, Nielsen B, Laszcynska J, Larsen BE & Saltin B (1988). Muscle blood flow is not reduced in humans during moderate exercise and heat stress. J Appl Physiol 64, 649–657. PubMed,CAS,Web of Science® Times Cited: 83 Sawka MN, Knowlton RG & Critz JB (1979). Thermal and circulatory responses to repeated bouts of prolonged running. Med Sci Sports 11, 177–180. PubMed,CAS,Web of Science® Times Cited: 57 Taylor NAS, Mekjavic IB & Tipton MJ (2008). The physiology of acute cold exposure, with particular reference to human performance in the cold. In Physiological Bases of Human Performance During Work and Exercise, ed. Taylor NAS & Groeller H, pp. 359–377. Churchill Livingstone Elsevier. Werner J, Mekjavic IB & Taylor NAS (2008). Concepts in physiological regulation: a thermoregulatory perspective. In Physiological Bases of Human Performance During Work and Exercise, ed. Taylor NAS & Groeller H, pp. 325–340. Churchill Livingstone Elsevier, New York. Wilkie DR (1968). Heat work and phosphorylcreatine break-down in muscle. J Physiol 195, 157–183. PubMed,CAS,Web of Science® Times Cited: 123