3 togaviruses flaviviruses. togaviruses and flaviviruses (c63, p637) 1. structure (+ssrna,...
TRANSCRIPT
3 Togaviruses
Flaviviruses
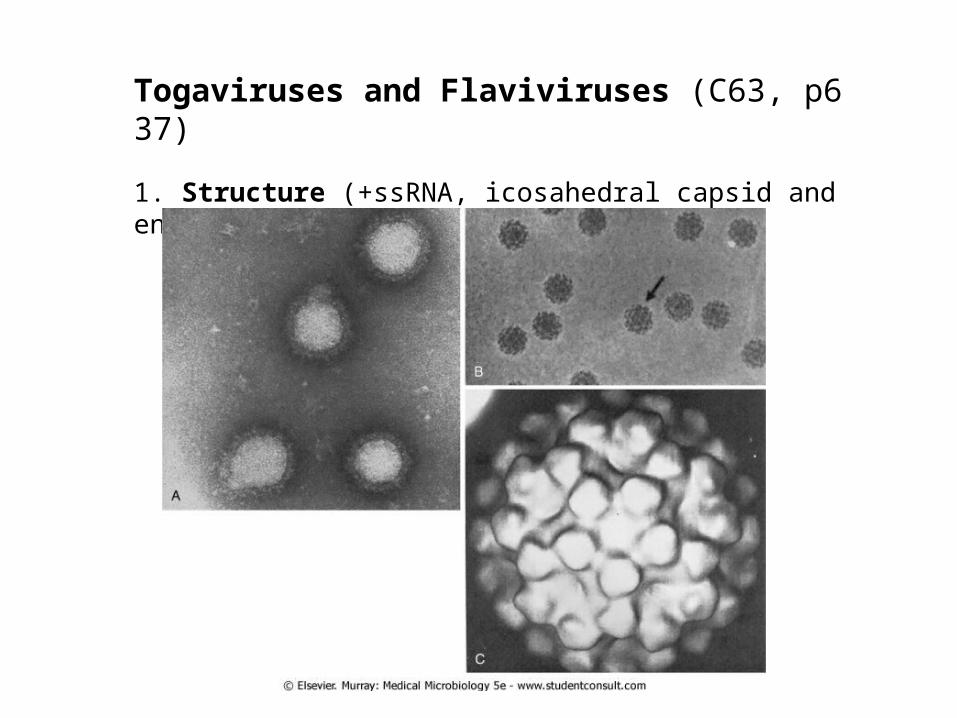
Togaviruses and Flaviviruses (C63, p637) 1. Structure (+ssRNA, icosahedral capsid and envelope)(Fig. 1)

2. Most members are arthropod-borne viruses (arboviruses, 節肢動物媒介病毒 ) Infect vertebrate hosts and induce viremia persistent productive infection of blood-feeding arthropod (broad host range including vertebrates and invertebrates; zoonoses) Exceptions: a. Rubella virus b. Hepatitis C virus Virus Group Human Pathogens
Togaviruses
Alphavirus Arboviruses
Rubivirus Rubella virus
Pestivirus None
Arterivirus None
Flaviviruses Arboviruses
Hepaciviridae Hepatitis C virus
Table 63-1. Togaviruses and Flaviviruses

The nomenclature of arboviruses are mostly based on endemic areas and symptoms induced by viruses, including fever, encephalitis and hemorrhagic fever (Table 2)
T2
EncephalitisNorth AmericaSmall mammalslxodes ticksPowassan encephalitis
EncephalitisRussiaBirdslxodes and Dermacentor ticks
Russian spring-summer encephalitis
EncephalitisNorth AmericaBirdsCulexSt. Louis encephalitis
Fever, encephalitis, hepatitis
Africa, Europe, central Asia, North America
BirdsCulexWest Nile encephalitis
EncephalitisAsiaPigs, birdsCulexJapanese encephalitis
Hepatitis, hemorrhagic fever
Africa, South AmericaHumans, monkeysAedesYellow fever*
Mild systemic; break-bone fever, dengue hemorrhagic fever, and dengue shock syndrome
Worldwide, especially tropics
Humans, monkeysAedesDengue*
Flaviviruses
Fever, arthralgia, arthritis
Africa, AsiaHumans, monkeysAedesChikungunya
Mild systemic; encephalitis
North and South America
BirdsCulex, CulisetaWestern equine encephalitis
Mild systemic; encephalitis
North and South America, Caribbean
BirdsAedes, CulisetaEastern equine encephalitis
Mild systemic; severe encephalitis
North, South, and Central America
Rodents, horsesAedes, CulexVenezuelan equine encephalitis
SubclinicalEast and West AfricaBirdsAedes and other mosquitoes
Semliki Forest*
SubclinicalAfrica, Australia, IndiaBirdsAedes and other mosquitoes
Sindbis*
Alphaviruses
DiseaseDistributionHostVectorDisease

3. Replication -- Viral genome includes early (nonstructural) and late (structural) proteins. Genome arrangement is different between togaviruses and flaviviruses (Fig. 3).
-- Viral replication process includes the entry by receptor-mediated endocytosis, uncoating, protein (a single polyprotein ) synthesis, viral genome synthesis, assembly, and virus release by budding from plasma membrane or internal membrane (flaviviruses).

4. Pathogenesis and immunity
Transmission: viremic verterbrate hosts blood-feeding arthropod (female mosquito, persistently infected) infect another host and cause damage (death) of target cells
Disease development: viremia mild systemic disease might be due to interferon production after infection (fever, chills, headaches, backaches, etc., influenza-like symptoms) encephalitis, hepatitis, and arthrogentic (hemorrhage) disease.
Besides viral receptor, virus may attach to Fc receptor (macrophages and monocytes) via Ab to result in an increase of virus infection.
Antibody is produced to block infection. However, non-neutralizing Ab may have antibody dependent enhancement (ADE) effect to enhance virus replication by hundred folds.

BOX 63-2. Disease Mechanisms of Togaviruses and Flaviviruses
Viruses are cytolytic, except for rubella.
Viruses establish systemic infection and viremia.
Viruses are good inducers of interferon, which can account for the flulike symptoms of infection.
Viruses, except rubella and hepatitis C, are arboviruses.
Flaviviruses can infect cells of the monocyte-macrophage lineage. Non-neutralizing antibody can enhance flavivirus infection via Fc receptors on the macrophage.
Flulike Syndrome Encephalitis Hepatitis Hemorrhage Shock
Dengue + + + +
Yellow fever + + + +
St. Louis encephalitis + +
West Nile encephalitis + +
Venezuelan encephalitis + +
Western equine encephalitis + +
Eastern equine encephalitis + +
Japanese encephalitis + +

The nature of alphavirus and flavivirus disease is determined primarily by
• the specific tropisms of the individual virus type• the concentration of infecting virus, and • individual host response to the infection.

Page 642 Fig. 4

5. Epidemiology (1) Arboviruses are able to infect both vertebrates and invertebrates, initiate viremia in vertebrates, and initiate a persistent productive infection of the salivary gland of invertebrate. Humans are dead-end hosts.
(2) Death of infected no-human vertebrates, such as birds, occurs before human outbreak. (3) In winter, virus persist in arthropod eggs or migrate with birds. (4) Sylvatic (jungle) cycle (monkeys arthropods humans) urban cycle (humans arthropods humans)

BOX 63-3. Epidemiology of Togavirus and Flavivirus Infection
Disease/Viral Factors •Enveloped virus must stay wet and can be inactivated by drying, soap, and detergents. •Virus can infect mammals, birds, reptiles, and insects. •Asymptomatic or nonspecific (flulike fever or chills), encephalitis, hemorrhagic fever, or arthritis. Transmission •Specific arthropods characteristic of each virus (zoonosis: arbovirus). Who Is at Risk? •People who enter ecologic niche of arthropod: arboviruses. Geography/Season •Endemic regions for each arbovirus are determined by habitat of mosquito or other vector. •Aedes mosquito, which carries dengue and yellow fever, is found in urban areas and in pools of water. •Culex mosquito, which carries St. Louis encephalitis and West Nile encephalitis viruses, is found in forest and urban areas. •Disease is more common in summer. Modes of Control •Mosquito breeding sites and mosquitoes should be eliminated. •Live attenuated vaccines are available for yellow fever virus and Japanese encephalitis virus (killed).

7. Clinical symptoms: a. togavirus encephalitides (mostly are not in Taiwan)
b. flaviviruses ex: Outbreak of West Nile virus has occurred in US since 1995
West Nile Encephalitis: During August, a 70-year-old man from a swampy area of Louisiana develops fever, headache, muscle weakness, nausea, and vomiting. He has difficulty answering questions. He progresses into a coma. Magnetic resonance imaging results show no specific localization of lesions (unlike in herpes simplex virus encephalitis). His disease progresses to respiratory failure and death. His 25-year-old niece, living next door, complains of sudden onset of fever (39°C [102.2°F]), headache, and myalgias, with nausea and vomiting lasting 4 days.
The West Nile virus infection in US is similar to the Japanese encephalitis virus in Taiw

ex. Japanese encephalitis virusa1. Transmission : pig, horse, cow, bird mosquito (三斑家蚊 ) → humans。
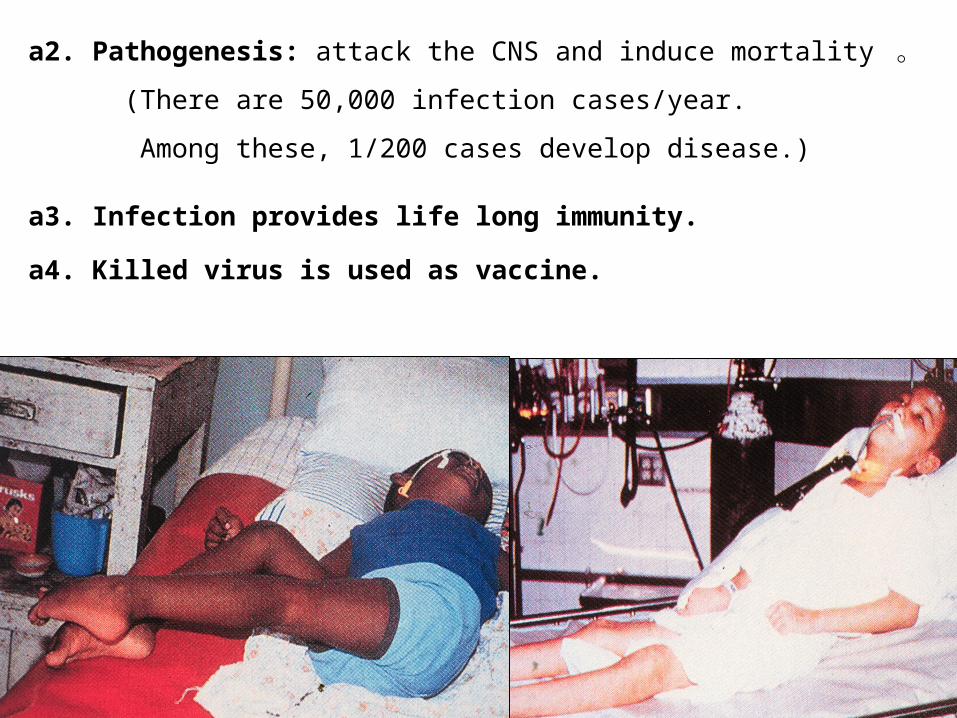
a2. Pathogenesis: attack the CNS and induce mortality 。
(There are 50,000 infection cases/year.
Among these, 1/200 cases develop disease.)
a3. Infection provides life long immunity.
a4. Killed virus is used as vaccine.

ex: dengue fever (caused by 4 serotypes of dengue virus)
Pathogenesis: 埃及或白線斑蚊→ humans →cause fever (DF), headache, rash, and back and bone pain for 6 to 7 days (break-bone fever) dengue hemorrhagic fever (DHF)
dengue shock syndrome (DSS)
Taiwan has all 4 serotypes, so the chance of Developing DHF/DSS is increasing.

b3. Epidemiology
•There are 100 million DF and 300,000 DHF/DSS cases per year.
• DHF and DSS are due to antibody dependent enhancement (ADE) induced by to infection with different serotypes of virus.

Please practice the case study of dengue infection in p. 648.

ex: Yellow fever virus induces yellow fever.
The disease is characterized by severe systemic disease, with generation of the liver, kidney, and heart, as well as hemorrhage.
Liver involvement causes the jaundice from which the disease gets its name, but massive gastrointestinal hemorrhages (black vomit).
The mortality rate is as high as 50%, but life long immunity.
8. Diagnosis:
Virus is identified by isolation, cytopathological studies, immunofluorescence, and RT-PCR. Serology is confirmed by the presence of virus specific IgM or a 4-fold increase in antibody titer. 10. No treatment exists for arbovirus diseases other than supportive care.11. Vector control is used to prevent virus spread.12. Vaccines are available for some viruses, such as JEV and yellow fever virus.
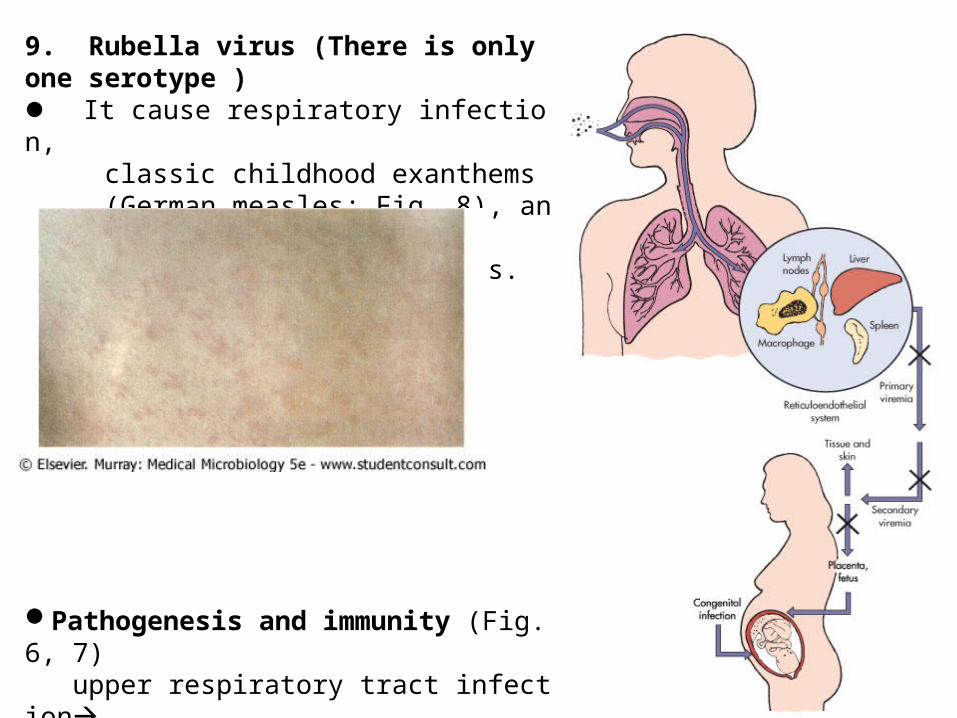
9. Rubella virus (There is only one serotype ) It cause respiratory infection, classic childhood exanthems (German measles; Fig. 8), and severe congenital defects.
Pathogenesis and immunity (Fig. 6, 7) upper respiratory tract infection local lymph nodes (lymphoadenopathy) viremia tissues rash.

• Immune response--Antibody production correlates with rash appearance, so immune complex causes rash. --Cell-mediated immunity helps to resolve infection. --Serum antibody provides life-long protection and prevents virus spread to fetus in pregnant women.
• Clinical syndromes
--Benign symptoms develop in children, but more severe problems (bone and joint pain, thrombocytopenia or encephalopathy) occur in adults (due to hypersensitivity or cell-mediated immunopathology).
Rubella: A 6-year-old girl from Romania developsa faint rash on her face and is accompanied by mild fever and lymphadenopathy. Over the next 3 days the rash progresses to other parts of the body.She has no history of rubella immunization.

Congenital rubella syndromes
3-13
BOX 63-5. Prominent Clinical Findings in Congenital Rubella Syndrome
•Cataracts and other ocular defects •Heart defects •Deafness •Intrauterine growth retardation •Failure to thrive •Mortality within the first year •Microcephaly •Mental retardation

Clinical Events Number Affected
Rubella cases 12,500,000
Arthritis-arthralgia 159,375
Encephalitis 2,084
Deaths
Excess neonatal deaths 2,100
Other deaths 60
Total deaths 2160
Excess fetal wastage 6250
Congenital rubella syndrome
Deaf children 8055
Deaf/blind children 3580
Mentally retarded children 1790
Other congenital rubella syndrome symptoms
6575
Total congenital rubella syndrome
20,000
Therapeutic abortions 5000
Table 63-3. Estimated Morbidity Associated with the 1964-1965 U.S. Rubella Epidemic

BOX 63-4. Epidemiology of Rubella Virus
Disease/Viral Factors •Rubella infects only humans. •Virus causes asymptomatic disease. •There is one serotype. Transmission •Respiratory route. Who Is at Risk? •Children: Mild exanthematous disease. •Adults: More severe disease with arthritis or arthralgia. •Neonates younger than 20 weeks: Congenital defects. Modes of Control •Live attenuated vaccine is administered as part of measles, mumps, and rubella (MMR) vaccine.
*
*
*
*

Before vaccination, congenital infection causes 1 % neonatal abnormality. (Vaccination reduces congenital infection to <1 to 0.1 per 100,000 pregnancies) Lab. Diagnosis
--It is difficult to isolate virus. --Virus is detected by RT-PCR. --Serology
Please practice the case study of rebella infection in p. 648.
CASE STUDY AND QUESTIONS
A 27-year-old businessman experienced a high fever, serious retroorbital headache, and severe joint and back pain 5 days after he and his family returned from a trip to Malaysia. The symptoms lasted for 4 days, and then a rash appeared on his palms and soles that lasted for 2 days.
At the same time the man's 5-year-old son experienced mild flulike symptoms and then collapsed after 2 to 5 days. The boy's hands were cold and clammy, his face was flushed, and his body was warm. There were petechiae on his forehead and ecchymoses elsewhere. He bruised very easily. He was breathing rapidly and had a weak rapid pulse. He then rapidly recovered after 24 hours.
1. What features of these cases pointed to the diagnosis of dengue virus infection? 2. Of what significance was the trip to Malaysia? 3. What was the source of infection in the father and son? 4. What were the significance of and the pathogenic basis for the petechiae and ecchymoses in the child?

The diagnosis of dengue virus infection is indicated by the disease signs of high fever, severe headache, and joint and back pain. The patient's trip to Malaysia would have increased his risk of exposure to Aedes mosquitoes carrying the virus.
The Aedes mosquito is endemic in Malaysia and is a carrier of dengue virus, which is prevalent in Malaysia.
The virus was transmitted independently by different mosquitoes to the father and son.
Petechiae and ecchymoses are indicators of hemorrhagic disease.

Two weeks after returning from a trip to Mexico, a 25-year-old man had arthralgia (joint aches) and a mild rash that started on his face and spread to his body. He recalled that he had felt as if he had the flu a few days before the onset of the rash. The rash disappeared in 4 days.
1. What features of this case pointed to the diagnosis of rubella infection? 2. Why is it significant that the symptoms started after a trip outside the United States? 3. What precaution could the man have taken to prevent this infection? 4. How was this infection transmitted? 5. Who was at risk for a serious outcome of this infection? 6. If this disease is normally mild in children, why is their immunization so important?
1. The diagnosis of rubella infection is suggested by the arthralgia and especially the mild rash. These immune-mediated responses occur after the virus replication and viremic spread, which induces interferon, causing the influenza-like syndrome.
2. Exposure to rubella in the United States is unlikely because of the U.S.'s effective vaccine program.
3. If the man had been immunized with the MMR (measles, mumps, rubella) vaccine and received his booster immunization at 15 years of age, he should have been protected against rubella disease.
4. Rubella is the only togavirus that is transmitted by aerosols as a respiratory virus.
5. All unimmunized individuals are at risk for this infection. However, the most serious outcomes occur to the fetus of women who are infected prior to the 20th week of pregnancy. Rubella causes severe congenital defects.
6. Immunization of the populace (especially children) for rubella prevents congenital defects in babies.