302 behavioralhealthpanel...participant guide 1 compliance in behavioral health for mcos and...
TRANSCRIPT

1/28/2014
Participant Guide 1
COMPLIANCE IN BEHAVIORAL
HEALT H FOR MCOS AND
PROVIDERS
Tuesday, February 11, 2014
2:45pm - 4:15pm
Gregory W. Moore
Peter J. Domas
Lesa Yawn
Mary Thornton
12
PANEL
D ISCUSSION
AGENDA
� Understanding current
environment and the implications
for MCOs and providers – 15 mins
� Assessing and determining risk for
MCOs and providers – 30-35 mins
� Implementing strategies to
mitigate and manage risk for MCOs
and providers – 30- 35 mins
� Questions and Answers – 10 mins
23
C O M P L I A N C E F R O N T A N D C E N T E R - R EQ U I R E M E N T S A N D E X P EC TAT I O N S
� MCO
– Compliance program, plan and activities in place
– Staffing and expertise of program in house
– Expectations for participating providers
� Providers
– Compliance program
– Reduction of Provider and MCO risk
– Expectations of guidance from MCOs and the government and on-going assessment of risk
3
1/28/2014
Participant Guide 2
T HE ENVIRONMENT
Constant Change Models
45
T H E E N V I R O N M E N T: A C A , PA R I T Y, C H R O N I C H E A LT H H O M E S ,
I N T E G R AT I O N , E T C .
� What does it mean for BH member/provider/services
management by MCO and Provider
– Inclusion
– Expectations of waste management
– Impact on MCO-provider relationship
6
ENVIRONMENTAL SCAN
� Compliance front and center - requirements and expectations
� Affordable Care Act - content and implications for both MCO and Provider
� Limited dollars - more for less
� Inclusion of eligible members with significant needs, lack of resources and barriers for engagement
� Inclusion of private and public sector providers with varying business and clinical models, resources and expertise
6

1/28/2014
Participant Guide 3
7
IMPACT OF
ELIGIBLE
MEMBERS ON
MCO AND
PROVIDERS
� Changes in eligibility due to
political climate and budgets -
moving target
� Increased penetration rates,
increased access and access
standards
� Changes in reimbursement
� More for less
7
Opportunit ies for
Behavioral Heal th Providers (and Payors) in
the Era of Heal thcare Reform
89
W H AT D O E S T H E G OV E R N M E N T S AY A B O U T T H E A C A
A N D B E H AV I O R A L H E A LT H?
� Fundamentally change what services will be available to individuals that have mental health and addiction disorders.
� Expand access to prevention services, including annual wellness visits, and include outreach and education campaigns. In addition, grants will be available to implement, evaluate, and disseminate community prevention activities.
� Create incentives to coordinate primary care, mental health, and addiction services, including the creation of health homes for individuals with chronic health conditions, including mental illness and substance use disorders.
� Enhance community-based service options for individuals with a mental health and/or substance use condition. Medicaid state plan changes and demonstration grants will expand these services for individuals who have long-term care needs (e.g., dual-eligibles, high-risk Medicare beneficiaries, 1915i changes, Money Follows the Person).
� Develop capacity to provide services in an effective and modern mental health and substance use system through various workforce initiatives, including education and training grants, loan repayment programs, and primary care residency training.
http://www.samhsa.gov/samhsanewsletter/Volume_18_Number_3/AffordableHealthCareAct.aspx

1/28/2014
Participant Guide 4
10
OPPORTUNITIES
AS A RESULT OF
THE ACA
� Opportunities unique to
behavioral health care providers,
MCOs and other third party
payors.
� Impact of Essential Health
Benefits on relationships
between providers and payors.
11
AUTHORITY
� ACA gives states authority to work with providers and payers:
– To establish and fund alternative health care delivery models
– To develop innovative payment methods
– To promote federal, state and local collaboration by forming model of integrated care delivery for a better value
12
M ORE OF T HE M ANY C HANGES U NDER T HE AC A
� Integrated primary care and behavioral health models –treatment, case management, key service coordination
� Medicaid expansion
� Accountable Care Organization (ACO) model
� Community Health Centers (CHC)
� Patient Centered Medical Home Pilots
1/28/2014
Participant Guide 5
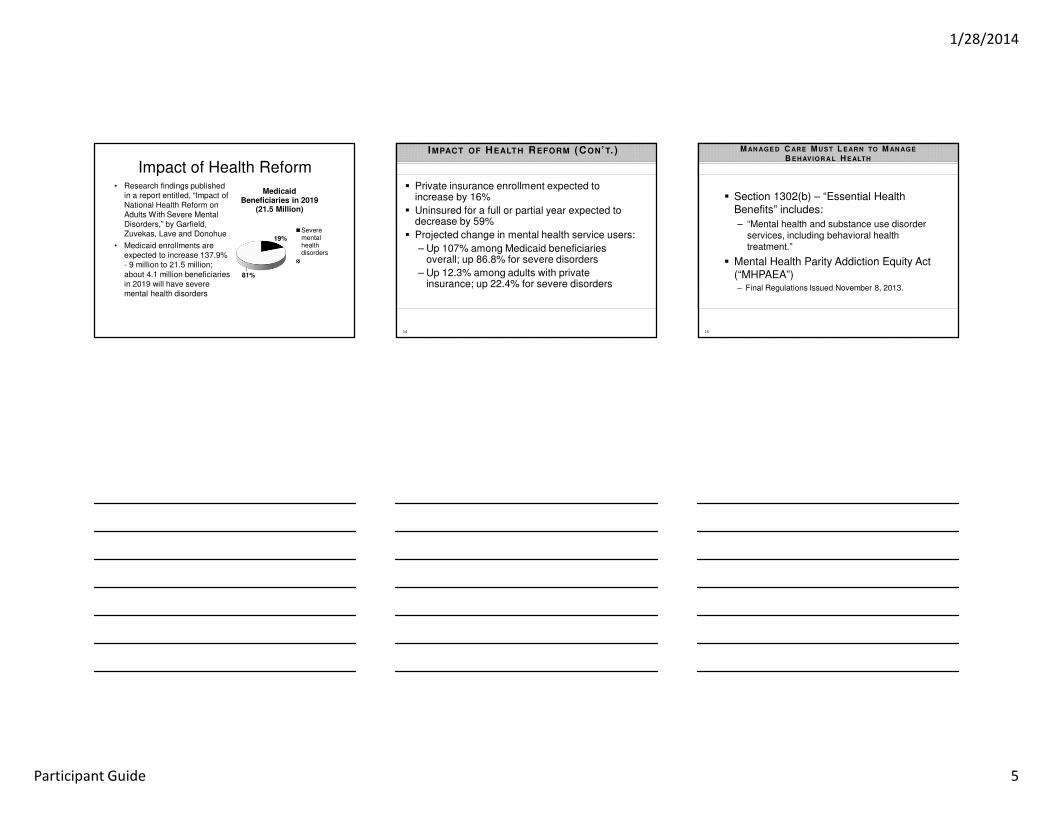
Impact of Health Reform• Research findings published
in a report entitled, “Impact of National Health Reform on Adults With Severe Mental Disorders,” by Garfield, Zuvekas, Lave and Donohue
• Medicaid enrollments are expected to increase 137.9% - 9 million to 21.5 million; about 4.1 million beneficiaries in 2019 will have severe mental health disorders
19%
81%
Medicaid Beneficiaries in 2019
(21.5 Million)
Severementalhealthdisorders
14
IMPACT OF HEALTH REFORM (CON’T. )
� Private insurance enrollment expected to increase by 16%
� Uninsured for a full or partial year expected to decrease by 59%
� Projected change in mental health service users:
– Up 107% among Medicaid beneficiaries overall; up 86.8% for severe disorders
– Up 12.3% among adults with private insurance; up 22.4% for severe disorders
15
M AN AGE D C ARE M UST L EARN TO M AN AGE
B EHAVIOR A L H EALTH
� Section 1302(b) – “Essential Health Benefits” includes:
– “Mental health and substance use disorder services, including behavioral health treatment.”
� Mental Health Parity Addiction Equity Act (“MHPAEA”)– Final Regulations Issued November 8, 2013.

1/28/2014
Participant Guide 6
16
ESSENTIAL
HEALTH
BENEFITS
(CON’T.)
� Under the MHPAEA, cost-sharing (e.g., deductibles and copayments) and treatment limitations (e.g., visit or day limits) applicable to mental health or substance use disorder benefits can be no more restrictive than the cost-sharing and treatment limitations applicable to medical and surgical benefits covered by the plan
� the ACA will require all small group and individual market plans created after March 23, 2010 to comply with federal parity requirements.
MCO PROVIDER BH
NET WORKS
MCO Evaluations of Organizational Risk in their Provider Networks
1718
CONDUCTING
MCO R ISK
ASSESSMENT
� Tools: environmental scan
� Methodology
� Sources and Resources
� Results
1/28/2014
Participant Guide 7
19
MCOS� Opportunities for contracting with
managed care health plans
– Sophistication on the private side or “cash and carry only”
– Most public providers cannot exist with just SPMI models – but they are wary of MCO interference OR are unaware of MCO requirements
• Their “deficit funding” is going away
� New population of providers: “Medicaiding” mental health and substance abuse services
20
M C O C O N S I D E R AT I O N O F VA RY I N G B U S I N E S S A N D C L I N I C A L M O D E L S ,
R E S O U R C E S A N D E X P E R T I S E
� Who are the providers?
– Private
• CMHCs: big focus of OIG and other oversight
• Minimal experience with insurances – small private practices (most psychiatrists not participating)
• Experts – single case contracting
• Encouraged to not document
– Public
• Substance abuse and mental health may not be integrated –separate bureaucracies and regs
• Varying degree of management expertise
• Policy-based bureaus fighting for their existence
• Lots of regs and costs associated with licensing and accreditation
• Access to “quality” psychiatry
– Primary health – integration models
� What does this mean for the MCO?
– Contracting is complex
– Various levels of risk and hand-holding
21
MCO
CONSIDERATIONS
IN
IMPLEMENTATION
OF BEST OR EBPS
� Uneven
� Academic models
� Expense associated with fidelity
� MCO coverage:
– reluctance to choose for the
providers
– Incorporation into utilization
management
1/28/2014
Participant Guide 8
22
MCO
CONSIDERATIONS
IN INTEGRATION
� Regs have not caught up with
policy in many cases
� 4 quadrant model – accepted but
not easily implemented
23
MCO
CONSIDERATIONS
CARE
COORDINATION
� Usually called case management on provider side
– In some states no longer funded –MCO responsibility?
– In some cases still provided by state workers
� Community-based model is most prevalent
� Usually lower credentials
� National certification - not used
� High productivity models fight “recovery”
24
MCO
CONSIDERATIONS
IN
CREDENTIALING
� Private practitioners: licensed; varying degrees of experience; specialty providers
� Public providers: limited access to licensed practitioners – many are in supervisory, not practice positions
– Many MA level, no license
– BS and other BA providers –some allowed to do psychotherapy
– Below BA – case management; supports coordination; residential techs; rehab workers
– Peers: various credentials
1/28/2014
Participant Guide 9
25
CREDENTIALS
(CONT)
� Psychiatrists:
– Must be convinced to see insured individuals –payment issues primarily
– Child psychiatrists: rare and very expensive
– Public system: older; foreign; and difficult to find; patchwork of hours and coverage; medical directors given limited time to direct; quality issues can be overlooked because of replacement difficulty
� NPPs: CNS and nurse practitioners: difficult to find; do not want to just do medication management; PA’s often do not have appropriate credentials for psych
– State variation in how they may practice
� Primary care: will tolerate limited complexity –single meds; often (even with CM and other supports) will not take on the SPMI population even if stabilized.
26
EXPERIENCE
WITH MCO’S
� What experience with managed
care? If any?
� Internal UM required? How
significant was this to operations?
� Use of level of care tools for
assignment
ROLE OF BEHAVIORAL HEALT H
PROVIDERS
Experiences Unique to Behavioral Health Providers Create a Significant Opportunity for Contracting
27
1/28/2014
Participant Guide 10
28
O PPOR TUNITIES BH – R EAD M ISSION P EN ALTY
S AGA
� If exceed 30 day readmit average for heart failure, heart attack or pneumonia
� In 2012, 2,217 hospitals penalized
� 307 cut full 1%
� In 2014, the penalty for readmission will increase to 2%
� In 2015, the penalties rise to 3%
29
MEDICARE
READMISSION
PENALTY
IMPACT
U.S. Total = $17.5 Billion a year
Source: Greene, Jay – Hospitals face reimbursement penalties over readmission rates
30
WHAT
HOSPITALS
SAY ABOUT
THE ISSUE
� “The process is out of our control”
� “We have found there is not a direct cause and effect as to why patients are readmitted”
� “There was no lack of coordination”

1/28/2014
Participant Guide 11
31
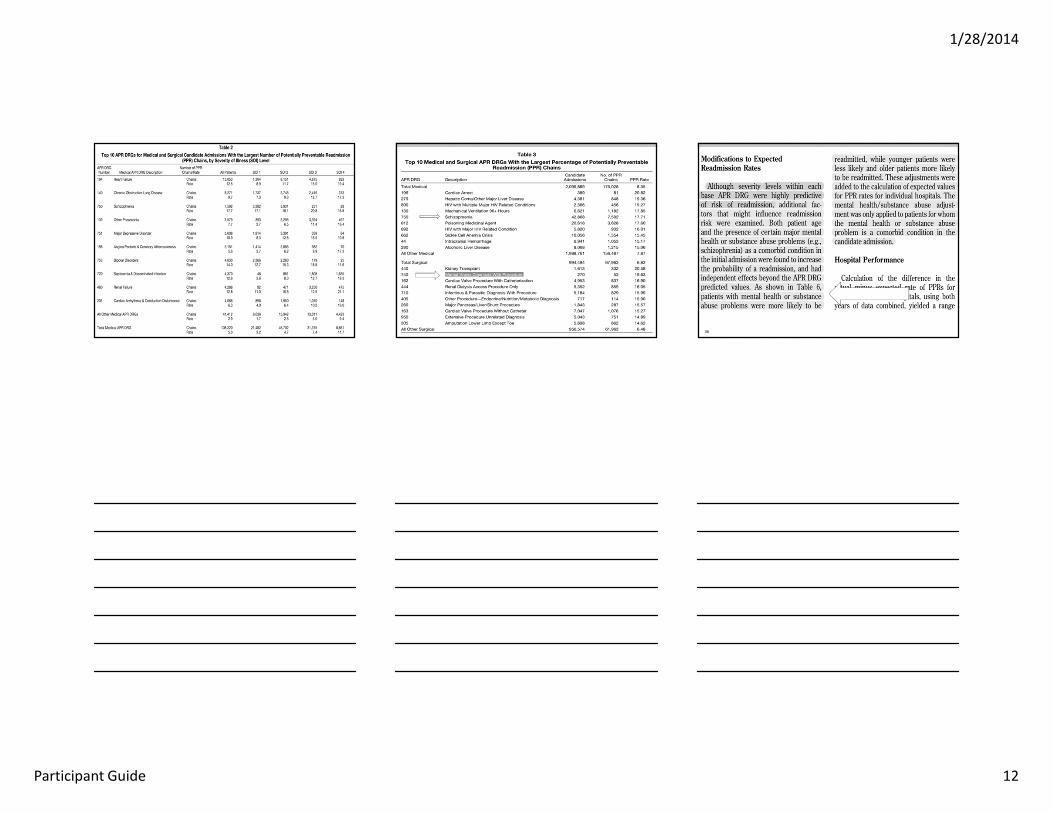
THE CASE FOR BH INVOLVEMENT
Identifying Potentially Preventable Readmissions, Norbert I. Goldfield, MD, et al, Health Care
Financing Review, Fall 2008.
The Revolving Door: A report on U.S. Hospital
Readmissions, Robert Wood Johnson Foundation – An Analysis of Medicare Data by
the Dartmouth Atlas Project, February 2013
32
THE CASE
FOR BH
INVOLVEME
NT
33
THE CASE
FOR BH
INVOLVEMENT
1/28/2014
Participant Guide 12
34 35 36
1/28/2014
Participant Guide 13
37 38
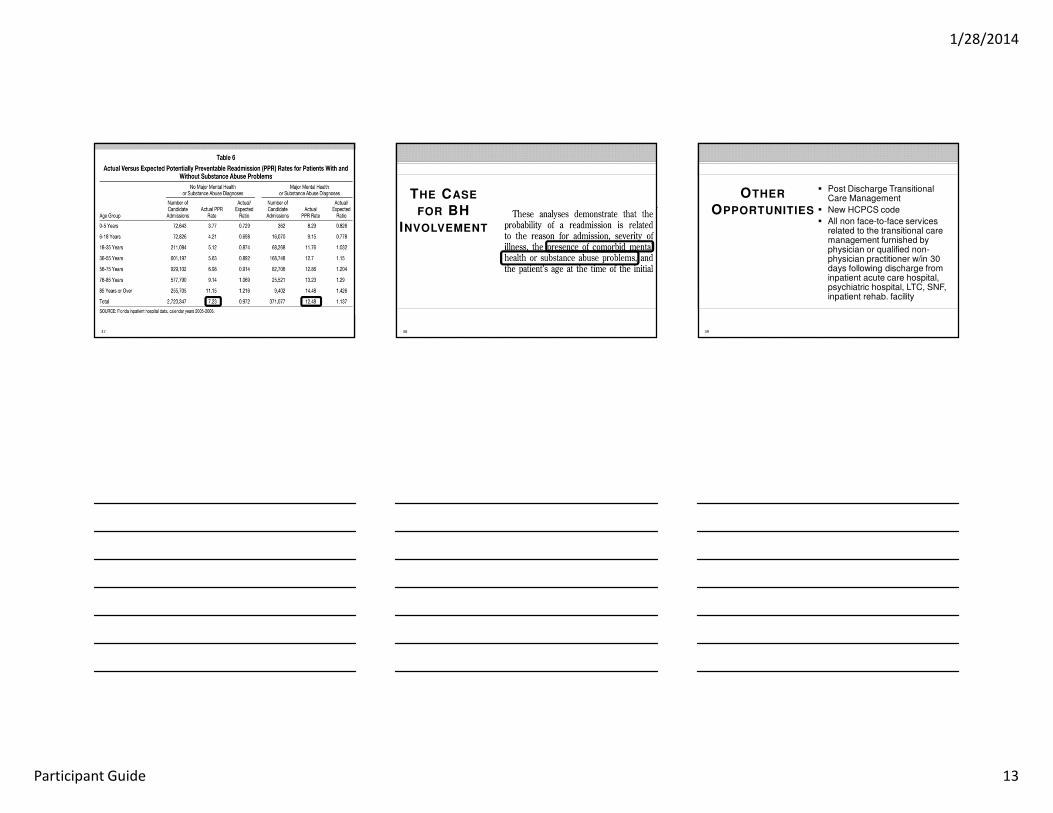
THE CASE
FOR BH
INVOLVEMENT
39
OTHER
OPPORTUNITIES
� Post Discharge Transitional Care Management
� New HCPCS code
� All non face-to-face services related to the transitional care management furnished by physician or qualified non-physician practitioner w/in 30 days following discharge from inpatient acute care hospital, psychiatric hospital, LTC, SNF, inpatient rehab. facility
1/28/2014
Participant Guide 14
BEHAVIORAL HEALT H
PROVIDERS
Risks Associated with Expanded Relationships with Behavioral Health Providers.
41
COMPLIANCE IS
NOT OPTIONAL
–
CONTRACTUAL
OBLIGATIONS
Federal Government
State Government
Payors
Providers
I N T R O T O D E V E LO P I N G A N E F F E C T I V E C O M P L I A N C E P L A N
42
JUSTICE
NEWS
“Home Health Aide Sentenced to Prison for Medicaid Fraud Involving Time at Casinos, Resorts”
� Facts:
– Billed Medicaid as if she was working at several places at once
– Billed for working more than 24-hours in a day
– Claimed she was visiting patients’ homes, but was actually at casinos and resorts
– Medicaid recipients were also charged for taking kickbacks
� Penalty for Health Aide:
– Prison Time – 2 years
– Fines – $234,663.61 restitution
Source: http://www.ohioattorneygeneral.gov/Media/News-Releases/July-2013/Home-Health-Aide-Sentenced-to-Prison-for-Medicaid on
7/18/2013
I N T R O T O D E V E LO P I N G A N E F F E C T I V E C O M P L I A N C E P L A N

1/28/2014
Participant Guide 15
43
JUSTICE
NEWS
“Mental Health Counselor Gets 6-Year Prison Sentence”
� Facts:
– Falsely claimed that she was the clinician for services provided to Medicaid recipients when no services were provided
– “Rented out” Medicaid provider number in exchange for a percentage of fraudulent Medicaid reimbursements
– Fraudulently used Medicaid numbers of children whose parents thought they were enrolled in after school programs
� Penalty:
– Prison Time – 6 years
– Fines – $6,156,674.68 restitution
Source: http://www.fbi.gov/charlotte/press-releases/2013/mental-health-counselor-receives-six-year-prison-sentence-for-defrauding-medicaid-
of-6.1-million on 8/8/2013
I N T R O T O D E V E LO P I N G A N E F F E C T I V E C O M P L I A N C E P L A N
44
JUSTICE
NEWS
“Executives from Miami-Area Mental Health Care
Hospital Convicted for Participation in $70 Million
Medicare Fraud Scheme”
� Facts:
– Paying bribes to a network of patient recruiters
and falsifying documents
– Created the illusion of providing intensive
psychiatric care to qualifying patients when no care
of substance was provided
– Attempted to conceal payment of bribes and
kickbacks by creating false documents to make it
appear as if legitimate services were being
rendered
Source: http://www.justice.gov/opa/pr/2013/June/13-crm-744.html on 6/28/2013
45
JUSTICE
NEWS
“Long Island Health Care Provider Sentenced to 12 Years in Prison for $10 Million Medicare Fraud and HIPAA
Identity Theft”
� Facts:
– She used her position as a medical equipment company owner to enter nursing homes in order to access and steal patient records
– Falsely assumed a number of titles, including a doctor, nurse practitioner, and wound care expert
– Used the stolen records to create and submit false billings
– Violated the privacy of over 1000 patients
� Penalty:
– Prison Time – 12 years
– Fines – $10M restitution
Source: http://www.justice.gov/usao/nye/pr/2013/2013apr10.html on 4/10/2013
I N T R O T O D E V E LO P I N G A N E F F E C T I V E C O M P L I A N C E P L A N
1/28/2014
Participant Guide 16
46
JUSTICE
NEWS
“Health Care Clinic Director Sentenced for Role in $63 Million Health Care Fraud Scheme”
� Facts:
– Clinical director of community mental health center’s partial hospitalization program (“PHP”) conducted group therapy sessions without a therapist
– Paid illegal kickbacks to assisted living facilities (“ALFs”) in exchange for patient referral information, which was used to submit false claims
– Knew that main ALF referral patients were ineligible for partial hospitalization program services because many suffered from mental retardation, dementia, and Alzheimer’s
Source: http://www.justice.gov/opa/pr/2013/July/13-crm-844.html?goback=%2Egmr_5106478#%21 on 7/25/2013
I N T R O T O D E V E LO P I N G A N E F F E C T I V E C O M P L I A N C E P L A N
47
JUSTICE
NEWS
“Attorney General Masto Announces Sentencing of Las Vegas Behavioral Health Worker”
� Facts :
– Submitted progress notes and time attendance documents to a behavioral health company for incarcerated individuals who were unable to receive behavioral health services
– Did not call or visit the Medicaid recipients during times or for time periods that he claimed he had provided the behavioral health services
� Penalty:
– Jail: 150 days, suspended
– Community Service: 100 hours
– Fines: $23,946
– Probation: Up to 2 years
Source:
http://ag.nv.gov/News/PR/2013/Medicaid_Fraud/Attorney_General_Masto_Announces_Sentencing_of_Las_Vegas_Behavioral_Health_Worker/
on 10/7/2013
I N T R O T O D E V E LO P I N G A N E F F E C T I V E C O M P L I A N C E P L A N
48
PAYORS MAY
NEED TO
EQUIP CERTAIN
PROVIDERS
WITH TOOLS TO
ENSURE
COMPLIANCE
� Contracts with Behavioral Health Providers should provide for Compliance Program Requirements along with:
– Tools to implement Effective Compliance Programs
– Sources and Resources for Continuing Education.
– Expectations for Results
1/28/2014
Participant Guide 17
49
ELEMENT #1:
WRITE AND
D ISTRIBUTE
POLICIES AND
PROCEDURES
� Central component
� Could include:
– Conflict of Interest Policy
– Code of Conduct
– General policies and procedures
– Summary of key laws
and provisions
K E Y E L E M E N T S O F A C O M P L I A N C E P L A N
50
ELEMENT #2:
DESIGNATE A
COMPLIANCE
OFFICER OR
CONTACT
� Roles and responsibilities
� Communication channels
� Write a job description
K E Y E L E M E N T S O F A C O M P L I A N C E P L A N
51
ELEMENT #3:
CONDUCT
APPROPRIATE
TRAINING AND
EDUCATION
� Determine training needs
� Determine best-suited
delivery methods
� Consider:
– Frequency
– Metrics
– Accountability
– Organization-wide effort
K E Y E L E M E N T S O F A C O M P L I A N C E P L A N
1/28/2014
Participant Guide 18
52
ELEMENT #4: D EVELOP O PEN
L INES OF
C OMMUNICATION
� Ideas:
– Number/hotline
– Open Door Policy
– Complaints box
– Reporting form
� Establish policy and procedure
� Communicate importance of reporting
� No retaliation
K E Y E L E M E N T S O F A C O M P L I A N C E P L A N
53
ELEMENT #5:
CONDUCT
INTERNAL
MONITORING
AND AUDITING
� Various types of audits
� Set a baseline and regular intervals
for measurement
� Be proactive!
� Identify and resolve problems
K E Y E L E M E N T S O F A C O M P L I A N C E P L A N
54
ELEMENT #6:
ENFORCE
D ISCIPLINARY
STANDARDS
� Well-publicized guidelines
� Consistent and
appropriate consequences
� Procedures for disciplinary action
K E Y E L E M E N T S O F A C O M P L I A N C E P L A N
1/28/2014
Participant Guide 19
55
ELEMENT #7:
RESPOND
PROMPTLY AND
APPROPRIATELY
� Detecting offenses
– Warning indicators
� Investigating claims
� Documenting steps taken
� Developing an appropriate
response
K E Y E L E M E N T S O F A C O M P L I A N C E P L A N
56
OPERATING
AND
MAINTAINING
YOUR PLAN
� Keep policies and procedures
up-to-date and user-friendly
� Make training and education part
of the job/role
� Solicit feedback
� Maintain visibility
� Proactively audit
� Be consistent with enforcement
K E Y E L E M E N T S O F A C O M P L I A N C E P L A N
Source: HEAT and OIG
MCO: MIT IGAT ION OF RISK
Beyond the Compliance Program, What Can the MCOs Do?
1/28/2014
Participant Guide 20
58
ASSESSING AND DETERMINING RISK FOR MCOS
� Implications for MCO & Providers - new language & new
concepts to understand
– “QA, QI and QM”;
– “Regulatory Compliance”;
– “Risk Management”;
59
MCOS NEED TO THINK “OUTSIDE THE BOX”
1. Stretching “healthcare” for the SPMI Population
A. Housing first
B. Peer Services: credentialing and supervision
C. Supported Employment
D. ACT
2. Integration requires movement away from routine office visits –telehealth, self-management, phone based therapy, etc.
A. Who gets treated where?
B. Value added for somatizers
3. Co-occurring models: where can capacity be built?
A. Who does it well?
4. What if the state stands in the way?
60
CARE COORDINATION
� Who should provide? Who must provide?
� What credentials if provider-based?
– Medical competency – how can that be taught?
� Separate from or integrated into UM?
� Community vs. phone-based CM
� Public sector: transportation issue
1/28/2014
Participant Guide 21
61
ACCESS TO
MEDICATIONS
� Management of pharmacy benefit or not?
� Integration:
– Medical protocol/formulary implementation – must have behavioral health expertise
• Cocktails
• Children: risk based management
• Black box
• Off-label
� Non-integrated: medical protocols, especially focused on high risk individuals
62
CORRECT
LEVEL OF
CARE
ASSIGNMENT
� Utilization Management:
– Protocols for UM that are publicized and that educate providers using objective criteria
• E.g. LOCUS/CALOCUS or other tools
– Trainers need to be experts in provision of services not just management
• Watch out for tools like CANS/ANSA that are being used or promoted by states and courts that were not developed to be level of care criteria
• MCO needs to take lead and designate tools that must be used
63
OUTCOME
BASED
PAYMENTS
� Behavioral health: it would be very
difficult to develop outcomes
based payment at this time
� If MCO decided to move in this
direction, it would require
considerable amounts of expertise
and oversight

1/28/2014
Participant Guide 22
64
I M P L E M E N T I N G S T R AT EGI E S T O M I T I GAT E A N D M A N A G E R I S K
F O R M C O S
� Stretch compliance dollars in behavioral healthcare: audit claims or monitor compliance programming
– The better they are, the less risk you have
� Forge Provider Partnerships to support compliance especially with community based providers who have very few resources to dedicate to compliance
– They need access to information; to new regulatory requirements being contemplated; to new audit information, etc.
– Unless dealing with very large business entities, then the Compliance Officer has 3 or 4 other jobs
65
D E T E R M I N E S T R U C T U R E F O R C O M P L I A N C E P R O G R A M A N D P L A N F O R
M C O
� Use shared template to include seven/eight
components of compliance program
� Identify key areas of a compliance program
necessary to mitigate the risk associated with:
– expanding relationships with managed care
health plans, or
– developing integration strategies with physical
medicine
66
I M P L E M E N T I N G S T R AT EGI E S T O M I T I GAT E A N D M A N A G E R I S K
F O R M C O S
� Use and incorporate other findings - from DHHS,
accreditation, EQRO, individual and aggregate audit
results, current “hot buttons”
– Many providers have multiple
regulatory/licensing agencies involved – don’t
duplicate
� Evaluate which provider-types pose most risk
– An example: private providers –fraud vs. public
providers - waste

1/28/2014
Participant Guide 23
67
QUESTIONS AND ANSWERS
68
THANK YOU FOR YOUR TIME
Gregory W. Moore
248.988.5842
Clark Hill PLC
Lesa Yawn, PhD, JD757.343.8620
[email protected] Consulting Inc.
Peter J. Domas
248.988-5870
Clark Hill PLC
Mary Thornton BSRN, MBA, CHC, CHPC617.730.5800
[email protected] Mary Thornton & Associates,
Inc.