39-year-old woman with ‘monthly’ headaches
DESCRIPTION
CLINICAL CASE. 39-year-old woman with ‘monthly’ headaches. Presented by: Anne MacGregor Barts Sexual Health Centre, St. Bartholomew’s Hospital, London, UK. IDENTIFICATION. 39-year-old woman with ‘monthly’ headaches The woman seeks help for disabling headaches associated with menstruation. - PowerPoint PPT PresentationTRANSCRIPT

39-year-old woman with ‘monthly’ headaches
Presented by:
Anne MacGregor
Barts Sexual Health Centre,
St. Bartholomew’s Hospital, London, UK
CLINICAL CASE

IDENTIFICATION
• 39-year-old woman with ‘monthly’ headaches
• The woman seeks help for disabling headaches associated with menstruation
CASE PRESENTATION (I)
• KG is 39-year-old accountant who presents with ‘sick’ headaches
• Attack frequency– Attack regularly with menstruation lasts three to four
days– One to two additional attacks per month lasting one
day

CASE PRESENTATION (II)
• Description of attacks– Nasal congestion on waking, which develops into
one-sided headache– Headache associated with nausea, light and sound
sensitivity
• Periods regular 5/27-29 days – Menstrual headaches disabling– No other menstrual problems
CASE PRESENTATION (III)
• Treatment– Paracetamol 1 g:
effective for non-menstrual headaches
not effective for menstrual headaches

PAST CLINICAL HISTORY (I)
• Headaches– Since teens– More frequent over last 10 years– Link with menstruation last 4 years– History of headaches in the pill-free week of
combined oral contraceptives

PAST CLINICAL HISTORY (II)
• Asthmatic, treated with inhalers• Avoids aspirin and NSAIDs• Otherwise healthy• Systems review normal

FAMILY HISTORY
• Parents– Mother well – past history of monthly headaches– Father being treated for high blood pressure
• Siblings– Two brothers both well with no medical complaints

PHYSICAL EXAMINATION
• On examination she looks in good health• Physical examination and neurological
assessments were unremarkable• BP 125/85 mmHg• BMI 23.2 kg/m2
DIAGNOSTIC PROCEDURES
• None indicated– No atypical features in the history– Physical and neurological examinations normal
http://tools.aan.com/professionals/practice/pdfs/gl0088.pdf
DIAGNOSIS (I)
• Is it migraine?– KG has had episodic headaches associated with
photophobia, nausea, and disability– She is free of symptoms between attacks– Normal physical and neurological examination
• This suggests a diagnosis of migraine without aura
Cephalalgia 2013;33: 629-808.

DIAGNOSIS (II)
• Is it menstrual migraine?– KG describes regular attacks of migraine with her
menstrual period and additional attacks at other times of the month
• This suggests a diagnosis of menstrually-related migraine without aura (Fig. 1)– Diary cards can confirm the diagnosis
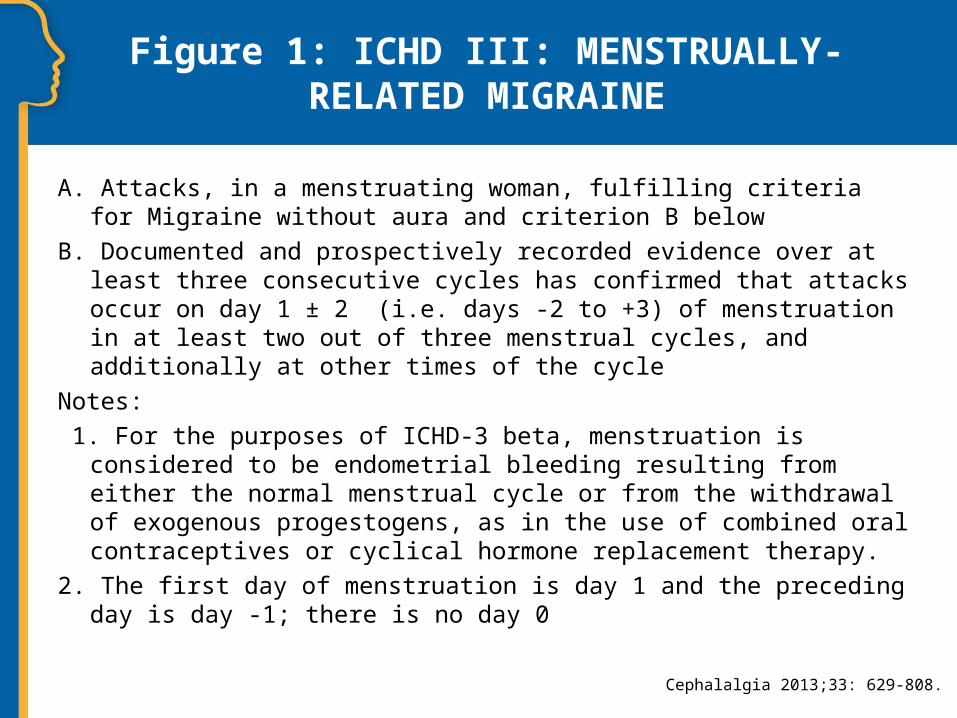
Figure 1: ICHD III: MENSTRUALLY-RELATED MIGRAINE
A. Attacks, in a menstruating woman, fulfilling criteria for Migraine without aura and criterion B below
B. Documented and prospectively recorded evidence over at least three consecutive cycles has confirmed that attacks occur on day 1 ± 2 (i.e. days -2 to +3) of menstruation in at least two out of three menstrual cycles, and additionally at other times of the cycle
Notes:
1. For the purposes of ICHD-3 beta, menstruation is considered to be endometrial bleeding resulting from either the normal menstrual cycle or from the withdrawal of exogenous progestogens, as in the use of combined oral contraceptives or cyclical hormone replacement therapy.
2. The first day of menstruation is day 1 and the preceding day is day -1; there is no day 0
Cephalalgia 2013;33: 629-808.

DIAGNOSIS (III)
• Diary shows (Fig. 2)– Migraine starting on day -2 of menstruation; duration
4 days– 1 additional attack non-menstrual attack; duration 1
day

Figure 2: THE HEADACHE DIARY OF THE PATIENT

TREATMENT (I)
• What is her current treatment and is she taking it optimally?– Diary shows menstrual attack did not respond to
paracetamol– She delayed treatment for several hours after the
headache has started

TREATMENT (II)
• Are there any relevant non-hormonal triggers?

TREATMENT (III)
• Would she benefit from daily prophylaxis?– Depends on attack frequency and response to acute
treatment

TREATMENT (IV)
• Treatment management– NSAIDs contraindicated because of asthma– Recommend frovatriptan for treatment of long-
duration menstrual attacks– Diary records for three months– Consider non-hormonal triggers

FOLLOW-UP
• Review diary cards to confirm diagnosis of menstrually-related migraine (Fig. 3)
• Review efficacy of acute treatment and consider need for prophylaxis (Fig. 4)
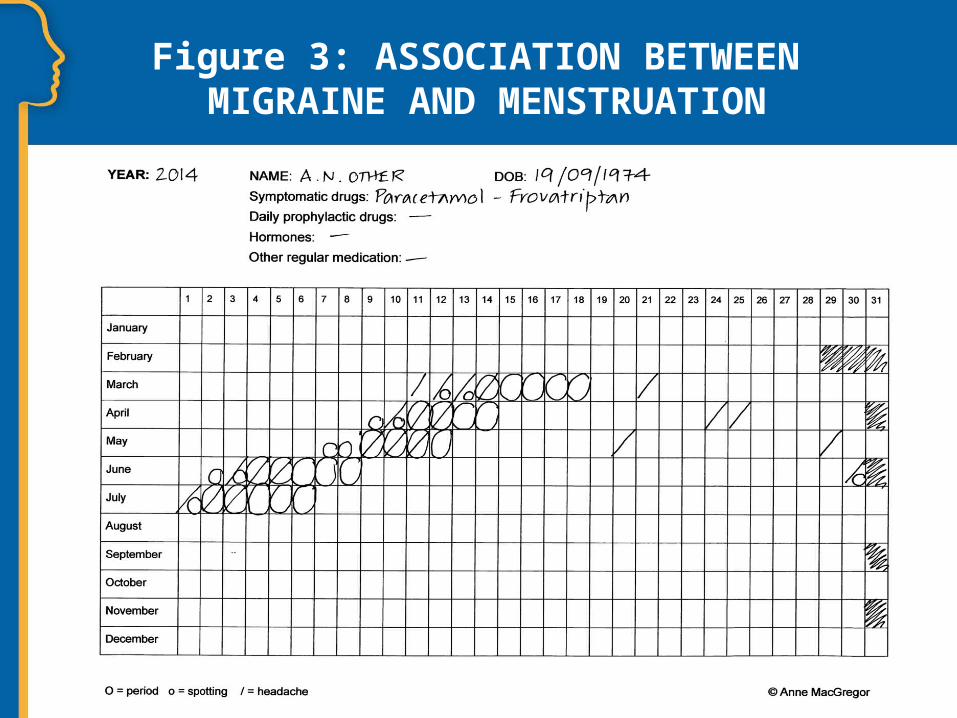
Figure 3: ASSOCIATION BETWEEN MIGRAINE AND MENSTRUATION

Figure 4: ACUTE TREATMENT WITH FROVATRIPTAN
TREATMENT EVALUATION
• Diary shows that menstrual attacks respond to frovatriptan and that she treats symptoms as soon as headache starts and repeats for relapse

CLINICAL EVALUATION
• She has reduced the frequency of non-menstrual migraine by avoiding lack of sleep and missed meals
• Daily prophylaxis is not indicated given her frequency of attacks and response to acute treatment

REMARKS (I)
• Late 30s/40s is the typical age for menstrual migraine to present
• Diary cards are essential to confirm the diagnosis and assess the effects of treatment
• Hormonal tests are not indicated
Sarchielli P, et al. J Headache Pain 2012;13 Suppl 2:S31-70;MacGregor EA, et al. Neurology 2006;67:2154-2158;MacGregor EA, et al. Neurology 2006;67:2159–2163.

REMARKS (II)
• Long-duration attacks, such as menstrual migraine, need treatments with a longer duration of action, such as frovatriptan
• Early treatment improves efficacy and reduces pain and functional disability
Sarchielli P, et al. J Headache Pain 2012;13(Suppl2):S31-70; Evers S, et al. Eur J Neurol 2009;16:968-981;
Bendtsen L, et al. Danish Headache Society, 2nd Edition, 2012. J Headache Pain 13 2012; Suppl1:S1-29;Geraud G, et al. Headache 2003;43:376-388;
Cady R, et al. Curr Med Res Opin 2004;20:1465-72.