4- cement ,,4
DESCRIPTION
NONETRANSCRIPT
1
Proper selection of luting Proper selection of luting cementscements
Dr.Salah abdel azimPHD Fixed Prosthodontics
2
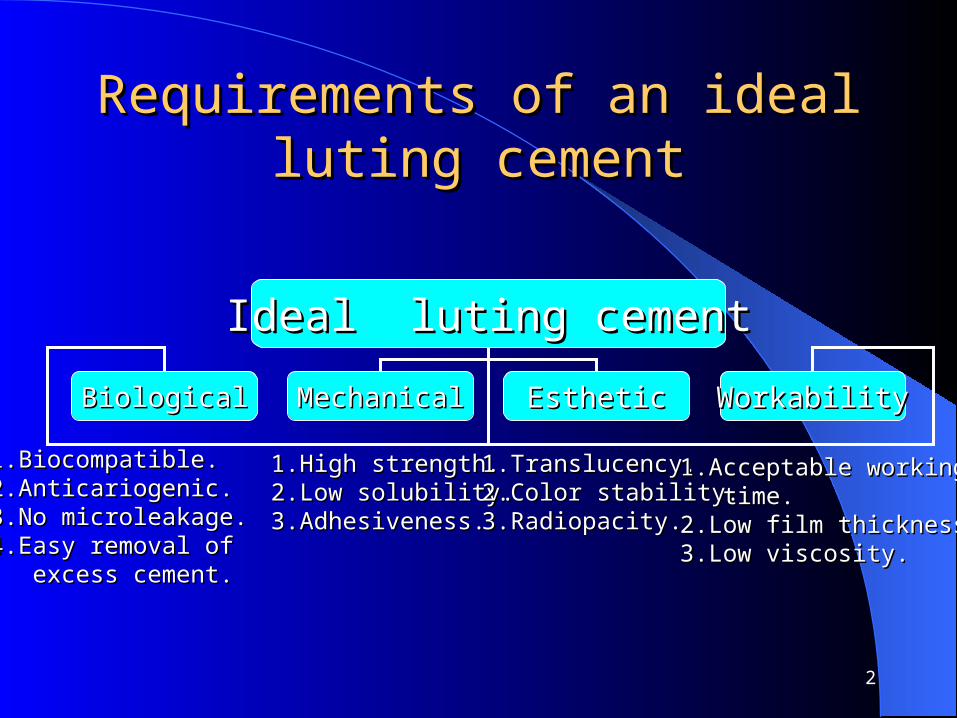
Requirements of an ideal Requirements of an ideal luting cementluting cement
Ideal luting cementIdeal luting cement
BiologicalBiological MechanicalMechanical EstheticEsthetic WorkabilityWorkability
1.Biocompatible.1.Biocompatible.2.Anticariogenic.2.Anticariogenic.3.No microleakage.3.No microleakage.4.Easy removal of4.Easy removal of excess cement.excess cement.
1.High strength.1.High strength.2.Low solubility.2.Low solubility.3.Adhesiveness.3.Adhesiveness.
1.Translucency.1.Translucency.2.Color stability.2.Color stability.3.Radiopacity.3.Radiopacity.
1.Acceptable working1.Acceptable working time.time.2.Low film thickness.2.Low film thickness.3.Low viscosity.3.Low viscosity.
3
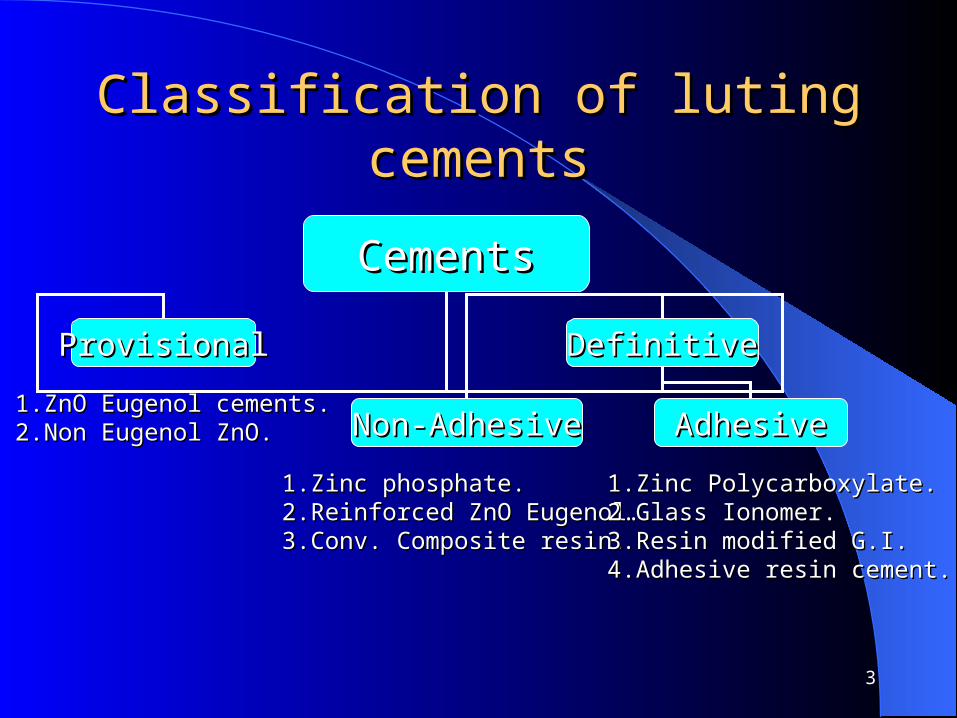
Classification of luting Classification of luting cementscements
CementsCements
ProvisionalProvisional DefinitiveDefinitive
Non-AdhesiveNon-Adhesive AdhesiveAdhesive1.ZnO Eugenol cements.1.ZnO Eugenol cements.2.Non Eugenol ZnO.2.Non Eugenol ZnO.
1.Zinc phosphate.1.Zinc phosphate.2.Reinforced ZnO Eugenol.2.Reinforced ZnO Eugenol.3.Conv. Composite resin.3.Conv. Composite resin.
1.Zinc Polycarboxylate.1.Zinc Polycarboxylate.2.Glass Ionomer.2.Glass Ionomer.3.Resin modified G.I.3.Resin modified G.I.4.Adhesive resin cement.4.Adhesive resin cement.
4
Zinc oxide eugenolZinc oxide eugenol Unmodified type used for provisional cementation. Biocompatible, have palliative and sedative effect. Low strength properties allowing non traumatic removal
of restorations. Soluble due to elution of eugenol. Not translucent, and no anticariogenc effect. Because eugenol acts as an inhibitor for free radical
polymerized materials, select other material for provisional restorations when bonding of the permanent restoration is anticipated.
Non eugenol ZnO cements are also available for provisional cementation, it contains ZnO and aromatic oil, these cements are also useful for eugenol sensitive patients. They are also used with acrylic provisional crowns because they do not soften the crown.
5
Reinforced Zinc oxide Reinforced Zinc oxide eugenoleugenol
Reinforced ZnO eugenol cements are used for definitive cementation either by the incorporation of a polymer or by the addition of alumina to the powder to the eugenol liquid..
However with these additives;1) Inferior mechanical properties.2) High film thickness.3) Difficult removal of excess.4) Difficult to manipulate in the oral cavity.
*For these reasons the use of ZnO eugenol as definitive cement has been confined to those situations in which it was anticipated that sensitivity might be a problem and good inherent retention is also available.
6
Zinc PhosphateZinc Phosphate Adequate compressive strength but low tensile. Early achievement of strength properties. Acceptable film thickness. Easy removal of excess. Moderate to high working time. Good flow, viscosity rises during setting.
Adhesion: Only mechanical. High acidity at time of placement. [Varnish application] No antibacterial effect. Soluble in oral fluids.
7
Special mixing method:
Zinc PhosphateZinc Phosphate
8
Frozen glass slab method: Higher strength properties.
More working time. Less pulp irritation. Greater resistance to
solubility.
*Slaking the fluid by incorporating small amount of powder into the liquid about 1minute before the main mixing is started will increase working and setting time.
Zinc PhosphateZinc Phosphate
9
Zinc PolycarboxylateZinc Polycarboxylate Excellent Biocompatibility. Adhesion to tooth structure through chelation of
calcium by the carboxyl grp. of polyacrylic acid. Lower adhesion to dentine compared to enamel due to lower inorganic content and presence of smear layer.
Adhesion to base metal alloys and amalgam. No adhesion to gold or porcelain. Tin plating of gold
alloys and sandblasting to improve it. Low film thickness despite their viscosity i.e pseudo
plastic. Increasing shear rate of mixing cause thinning.
Lower compressive strength but higher tensile strength and modulus of elasticity compared to Zinc Phosphate cements.
More difficult to remove excess than ZnPh. Decreased working time.
10
Zinc PolycarboxylateZinc Polycarboxylate Powder is added quickly, in large quantities. Mixing using plastic spatula is preferable. Mix should be used when still glossy to obtain proper
adhesion.
11
Zinc PolycarboxylateZinc Polycarboxylate
To achieve good adhesion tooth surface should be clean, a recommended method is to apply 10% Polyacrylic acid for 10 to 15 sec. then rinsing by water to remove smear layer.
Reducing powder liquid ratio will increase solubility dramatically. [by threefold]
A modification of the normal composition is the water based, where liquid is distilled water and the acid is dried and added to the powder. Longer working time is obtained.
12
Glass IonomerGlass Ionomer Anticariogenic effect due to fluoride release. Mechanical and Chemical adhesion to enamel and to a
lesser degree to dentine, strong bond to base metal alloys specially after sandblasting with 50 microns Alumina. Doesn’t adhere to porcelain or gold alloys.
Low film thickness. Easy removal because it develops brittle properties. Relative biocompatibility. [no effect on pulp if
remaining dentin thickness is at least 1mm] Somewhat translucent due to presence of glass.
Refractive index similar to enamel and dentine.
13
Glass IonomerGlass Ionomer High solubility initially. [Varnish application] Susceptible to moisture contamination. Should be
protected with a foil or resin coat or by leaving a band of cement undisturbed for 10min.
Very sensitive to desiccation as well which can lead to post cementation hypersensitivity.
Adequate compressive and tensile strength, low modulus of elasticity but reaches ultimate properties slowly.
Short working time. [increased by using cool glass slab technique or with water settable types]
Water settable types are available where the acid is dried and incorporated into the powder, the liquid is distilled water or dilute conc. of tartaric acid in water.
14
Glass IonomerGlass IonomerPost cementation hypersensitivityPost cementation hypersensitivity
Post cementation hypersensitivity thought to be due to desiccation or bacterial contamination rather than irritation from the cement itself.
How to decrease it?1) Slight hydration of the tooth before cementation by placing a drop of water on the tooth during mixing which is gently blown off just before restoration application.2) Allowing the cement to set hard to the touch plus one minute before excess removal.3) Placing a varnish on the margins of the restoration after excess removal.
15
Resin modified Glass IonomerResin modified Glass Ionomer R.M.G.I were introduced in an attempt to combine some
of the desirable properties of G.I [Fluoride release and adhesion] with the high strength and low solubility of resins.
Rapid development of mechanical properties, same compressive strength and tensile strength as G.I but increased fracture toughness.
Less susceptible to early moisture contamination than G.I. Fluoride release. [Anticariogenic] Early Ph acidic (3.5) and gradually rises. Minimal post operative sensitivity. High flow. Initial slow rise in viscosity with a subsequent
increase. Longer working time. Bond strength to dentin more than G.I. (17Mpa) No measured solubility in acids.
16
Composite resin cementComposite resin cement These types of filled resin cements replaced the unfilled
resin types due to their superior properties. Composite resin cements are classified according to their bonding mechanism to tooth structure into conventional and adhesive cements.
Conventional type do not form chemical bond to tooth structure or restoration, i.e mechanical bonding only.
Adhesive type contains a chemically active component which reacts with both the tooth and the restoration, i.e adhesion is mechanical as well as chemical.
Excellent mechanical properties. CRC is the only insoluble cement in oral fluid. Translucent and has excellent esthetic.
17
Composite resin cementComposite resin cement Short working time (conv.), controlled (adhesive) e.g
Panivia. High film thickness (conv.), low (adhesive, 19microns) Viscosity: increases gradually. Easy removal of excess (adhesive), difficult (conventional). Conv. and adhesive types are both irritant to the pulp.
*Bonding of Adhesive CRC to restorations: It is adhesive to silanated porcelain, composites and the
oxide layer of metal surface. For non-precious alloys (NiCh and CoCh), they should be
sandblasted with 50microns oxide powder. For precious alloys, gold alloys should be sandblasted then
tin plated (0.2>>0.4 layer of tin). The cement bonds to tin oxide layer which develops on the tin plated surface.
18
Enamel bondingEnamel bonding
Bonding to enamel is achieved by acid etching which causes:1) Cleaning the enamel surface.2) Increasing the surface energy.3) Increasing the surface area by micro tags formation. (length 15>>>20microns, width 15microns)4) Mechanical interlocking through these micro tags.
N.B Recently enamel can be etched by Laser such as Carbon dioxide or Nd:YAG laser.
19
Dentine bondingDentine bonding Problems facing bonding to dentine:
1) Dentine is heterogeneous, even more than enamel.2) High protein content leading to low surface energy.3) Presence of smear layer.4) Presence of water film from dentinal tubules.5) Fear of pulp affection due to its proximity.
20
Cementation of long span bridgesCementation of long span bridges*Cement requirements:1)Long working time.2)High mechanical properties.3)Preferably to be adhesive.
*Cements of choice:1)Glass Ionomer. 2)R.M.G.I 3)Zinc Phosphate.4)Adhesive comp. resin. (Panavia with controlled setting
time)
N.B Zinc Polycarboxylate cements are not used due to its extremely short working time, ZnO eugenol cements are not used do to their low mechanical properties and short working time.
21
Cementation to deep Cementation to deep preparationspreparations
*Cement requirement:Should be non irritant and palliative to the pulp.
*Cement of choice:1)Zinc Polycarboxylate.2)Zinc oxide eugenol.
22
Cementation in caries active Cementation in caries active patientspatients
*Cement requirement:Must have anticariogenic effect by releasing fluoride ions and inhibiting secondary caries.
*Cements of choice:1)Glass Ionomer.2)Resin modified Glass Ionomer.3)Composite resin releasing fluoride. (e.g Panavia F)
23
Cementation to questionable Cementation to questionable preparationspreparations
*Cement requirements:1)Adhesive.2)Extremely high mechanical properties.3)Insoluble.
*Cement of choice:Adhesive composite resin cement with pulp protection over very deep dentinal tubules.
24
Cementation of Non-Precious Cementation of Non-Precious & Precious alloy restorations & Precious alloy restorations *Non-Precious alloys:
Adhesive resin cement, Glass Ionomer, R.M.G.I and Zinc Polycarboxylate provide good adhesion to non-precious alloys, especially after sandblasting. Zinc Phosphate is also used.
*Gold alloys:Zinc Polycarboxylate cements showed a bond strength 4 times greater than Zinc Phosphate and is directly proportional to copper present in the alloy.Surface should be blasted then tin plated before using the adhesive composite resin cement.
25
Post crowns cementationPost crowns cementation*Cement requirements:1)High flow.2)High strength properties.3)Preferable to be adhesive.
*Cements of choice:1)Resin modified Glass Ionomer.2)Glass Ionomer.3)Zinc Phosphate.4)Adhesive composite resin. (great care about
the working time)
26
Cementation to core based Cementation to core based materialsmaterials
*Cement requirements:Adhesion to the core material.
*Cements of choice: (According to core material type)1)Amalgam core: All currently used cements can be used.
It is recommended to use high copper amalgam core with high tin concentration with polycarboxylate cement since the high tin conc. enhances the bonding between amalgam cores and polycarboxylate cements.
2)Composite resin core: Composite resin cement.3)Glass Ionomer core: Glass Ionomer or R.M.G.I cement.
27
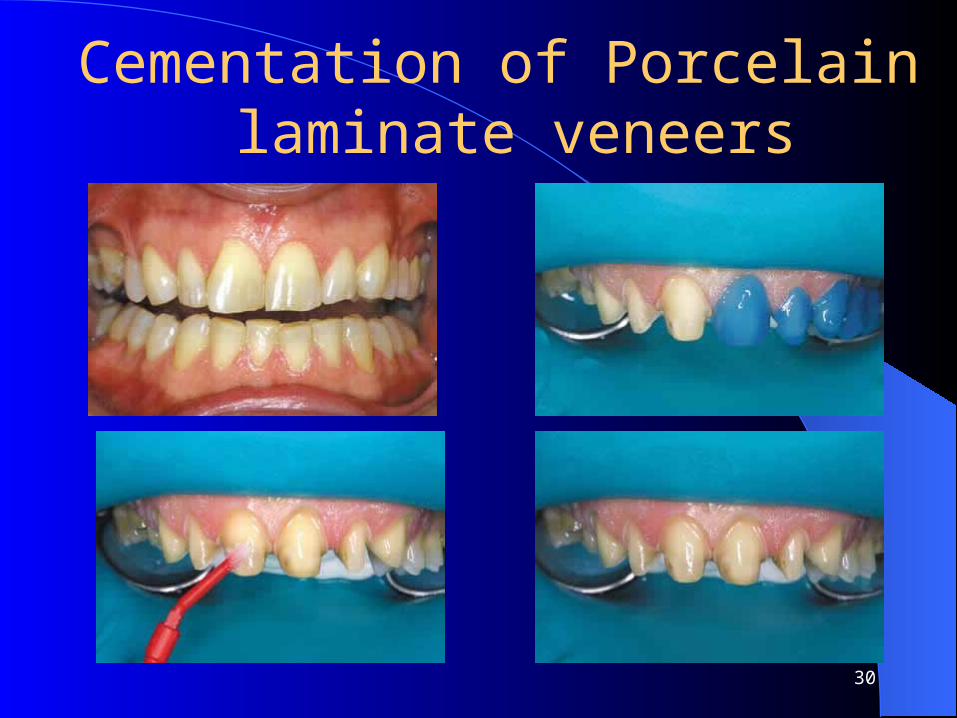
Cementation of Ceramic Laminate Cementation of Ceramic Laminate veneersveneers
*Cement requirements:1)Translucent. 2)Adhesive to tooth and porcelain.3)Early high mechanical strength and fracture toughness.
*Cements of choice: Composite resin cement.
N.B Glass Ionomer cement although it is translucent but has the disadvantage of slowness with which ultimate properties are developed. So when subjected to masticatory stress elastic deformation of the underlying cement could result in fracture of the brittle ceramic.
28
Cementation of Ceramic Laminate Cementation of Ceramic Laminate veneersveneers
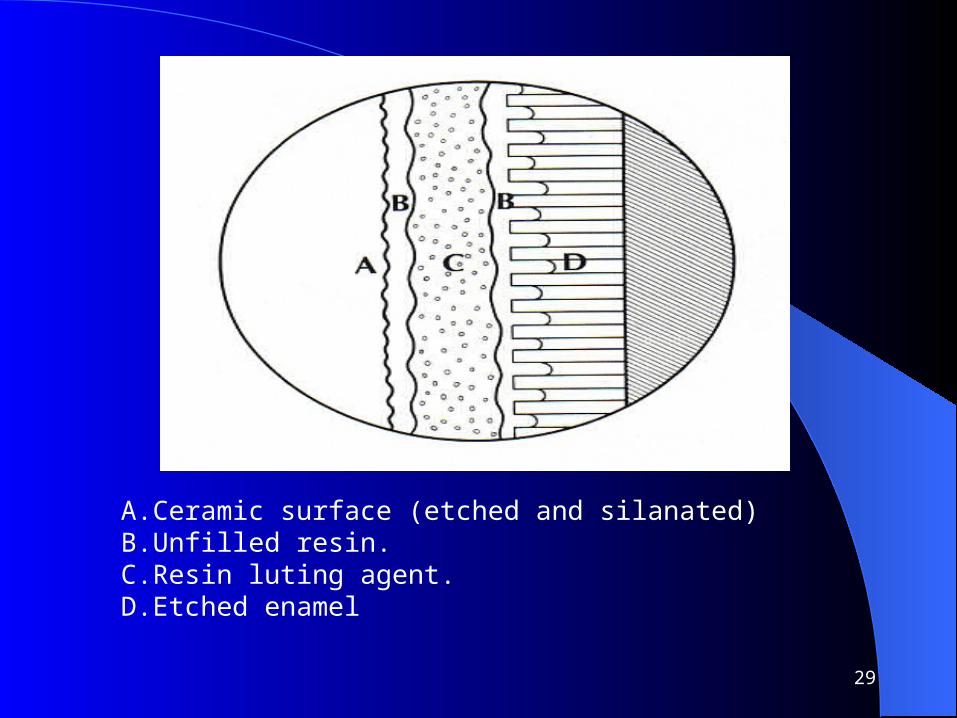
*Porcelain surface treatment:1)Acid etching 2 to 10% Hydrofluoric acid gel. (Glass
ceramics by 10% ammonium difluoride gel). Acid etching produces surface layer micromechanical retentive surface due to preferential dissolution of the crystalline portion of the ceramic.
2)Silane coupling agent (adhesion promoter) is used to enhance the chemical adhesion of the resin cement to ceramic material. Silane is bifunctional material, with one end of the molecule capable of reacting with an inorganic surface (ceramic) and other end with an organic surface (resin).
29
A.Ceramic surface (etched and silanated)B.Unfilled resin.C.Resin luting agent.D.Etched enamel
30
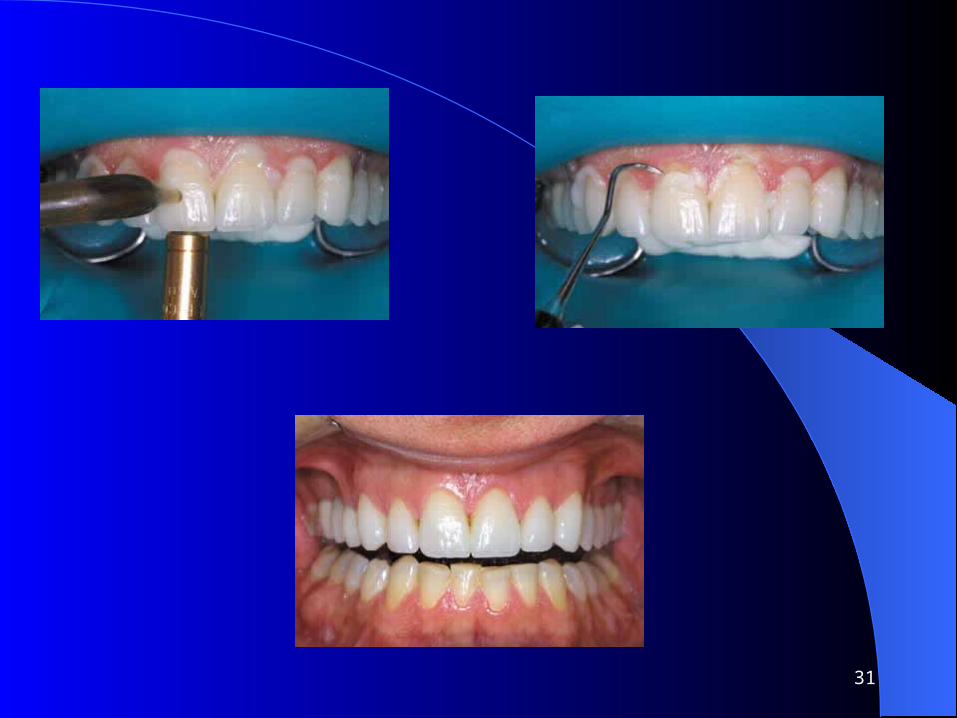
Cementation of Porcelain laminate veneers
31

32
Thank you….