5. kavita orbit
TRANSCRIPT

8/11/2019 5. Kavita Orbit
http://slidepdf.com/reader/full/5-kavita-orbit 1/45
Diseases of Orbit
Dr. I Gede Suparta SpM
Bag. Mata FK UNRAM/SMF Ilmu Penyakit Mata RSU
Prop. NTB Mataram
8/11/2019 5. Kavita Orbit
http://slidepdf.com/reader/full/5-kavita-orbit 2/45
Anatomical considerations
• Walls
• Apex
•
Openings• Spaces
• Relations
• Blood vessels
9/20/2014 2
8/11/2019 5. Kavita Orbit
http://slidepdf.com/reader/full/5-kavita-orbit 3/45
Orbital Cavity
• Dimensions- conical in shape
• Depth- 40 mm
•
Height- 35 mm• Width- 40mm
9/20/2014 3
8/11/2019 5. Kavita Orbit
http://slidepdf.com/reader/full/5-kavita-orbit 4/45
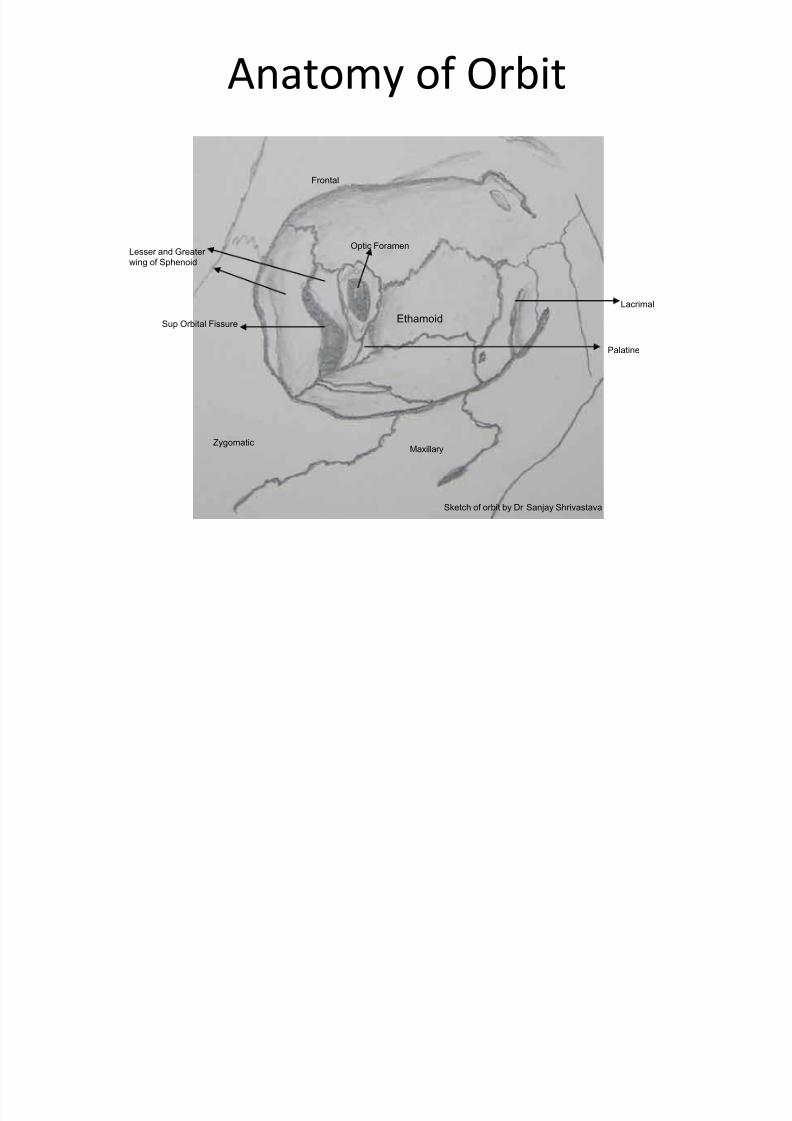
Anatomy of Orbit
Sketch of orbit by Dr Sanjay Shrivastava
Frontal
Ethamoid
Zygomatic
Lesser and Greater
wing of Sphenoid
Maxillary
Lacrimal
Palatine
Optic Foramen
Sup Orbital Fissure
8/11/2019 5. Kavita Orbit
http://slidepdf.com/reader/full/5-kavita-orbit 5/45
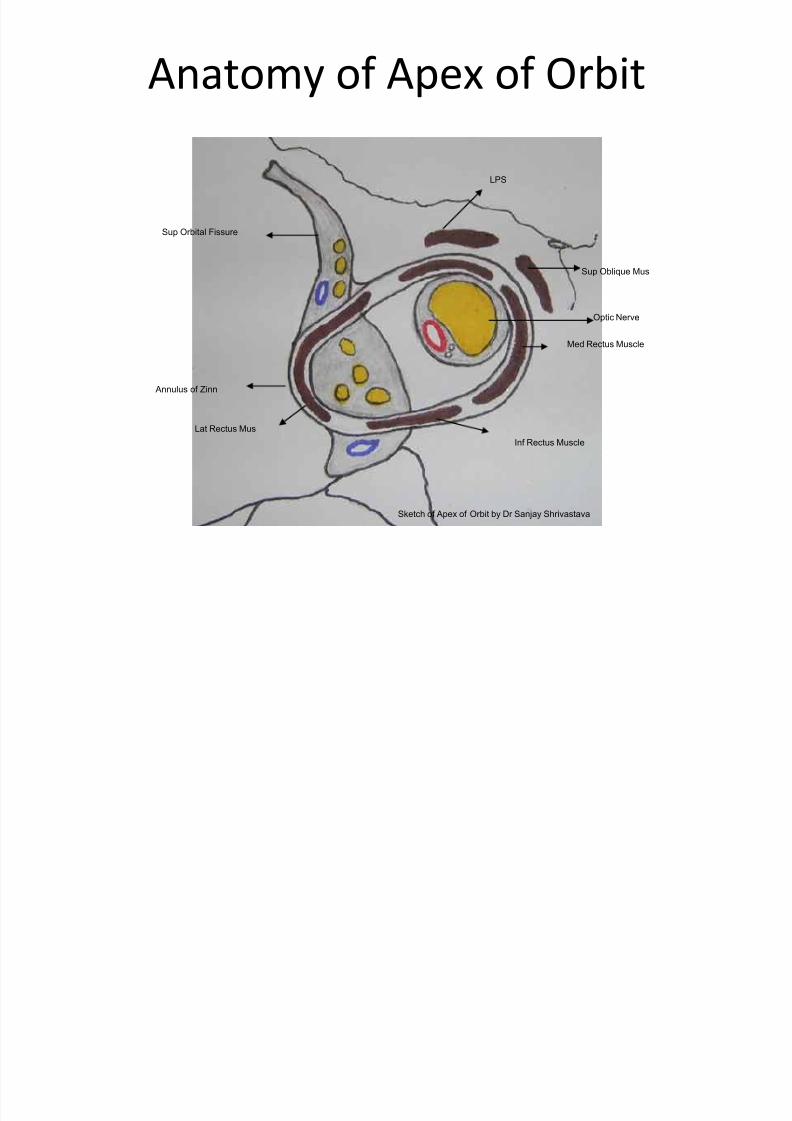
Anatomy of Apex of Orbit
Sketch of Apex of Orbit by Dr Sanjay Shrivastava
Sup Orbital Fissure
Annulus of Zinn
Med Rectus Muscle
Inf Rectus Muscle
Lat Rectus Mus
LPS
Sup Oblique Mus
Optic Nerve
8/11/2019 5. Kavita Orbit
http://slidepdf.com/reader/full/5-kavita-orbit 6/45
Walls
• Roof- is formed by the orbital plate of frontal boneand lesser wing of sphenoid
• Floor- is formed by the maxillary bone- orbital plate
and maxillary process of zygomatic bone and orbitalprocess of palatine bone
• Medial wall- is formed by the lacrimal andethamoidal bone, frontal process of maxillary bone
and body of sphenoid• Lateral wall- is formed by the greater wing of
sphenoid and zygomatic bone
9/20/2014 6
8/11/2019 5. Kavita Orbit
http://slidepdf.com/reader/full/5-kavita-orbit 7/45
Apex
• Annulus of zinn giving rise to origin to extra
ocular muscles
• Optic canal
• Part of superior orbital fissure
9/20/2014 7

8/11/2019 5. Kavita Orbit
http://slidepdf.com/reader/full/5-kavita-orbit 8/45
Openings
• Optic canal- optic nerve with meninges and
ophthalmic artery
• Superior orbital fissure-
Outside tendinous ring –
structures passing outsideare:
Lacrimal nerve –V1
Frontal nerve -V2Trochlear nerve
Superior and inferior veins
9/20/2014 8
8/11/2019 5. Kavita Orbit
http://slidepdf.com/reader/full/5-kavita-orbit 9/45
Opening
• Inside tendinous ring- structures passing
inside the ring are -
Oculomotor (3rd cranial nerve) upper division
Nasociliary nerve
Abducent nerve (6th cranial nerve)
Oculomotor lower division (3rd
cranial nerve)
Inferior orbital fissure-inferior ophthalmic vein
9/20/2014 9
8/11/2019 5. Kavita Orbit
http://slidepdf.com/reader/full/5-kavita-orbit 10/45
Opening
• Foramen rotandum - maxillary nerve
• Superior orbital notch-supraorbital nerve and
vessels
• Infra orbital foramen-infraorbital nerve and
artery
9/20/2014 10
8/11/2019 5. Kavita Orbit
http://slidepdf.com/reader/full/5-kavita-orbit 11/45
Spaces
• Subperiostial space
• Peripheral orbital space
•
Central space• Tenons space
9/20/2014 11
8/11/2019 5. Kavita Orbit
http://slidepdf.com/reader/full/5-kavita-orbit 12/45
Relations
• Frontal sinus
• Sphenoidal sinus
•
Maxillary sinus• Ethamoidal air cells
9/20/2014 12
8/11/2019 5. Kavita Orbit
http://slidepdf.com/reader/full/5-kavita-orbit 13/45
Common lesions
• Proptosis
• Exophthalmos- endrocrinal
•
Enophthalmos• Pseudoproptosis-slight prominence of eyes
like myopia, paralysis of extra ocular muscles,
obese people, mullers stimulation by cocain
9/20/2014 13
8/11/2019 5. Kavita Orbit
http://slidepdf.com/reader/full/5-kavita-orbit 14/45
Proptosis and Exophthalmos
• Abnormal protrusion of eye ball is called
proptosis or exophthalmos.
• The term exophthalmos is reserved for
prominence of the eye secondary to thyroid
disease
9/20/2014 14
8/11/2019 5. Kavita Orbit
http://slidepdf.com/reader/full/5-kavita-orbit 15/45
Proptosis
• Abnormal protrusion of globe
• It may be Unilateral or Bilateral
• Unilateral – caused by orbital cellulitis, idiopathic
orbital inflammatory disease, thrombosis of orbitalvein, arterio-venous aneurysms, tumors of structuresof orbit , orbital haemorrahge , emphysema.
• Bilateral – endocrine exophthalmos , cavernous sinus
thrombosis , symmetrical orbital tumors, oxycephaly- diminished orbital volume
9/20/2014 15
8/11/2019 5. Kavita Orbit
http://slidepdf.com/reader/full/5-kavita-orbit 16/45
Proptosis
8/11/2019 5. Kavita Orbit
http://slidepdf.com/reader/full/5-kavita-orbit 17/45
Proptosis
8/11/2019 5. Kavita Orbit
http://slidepdf.com/reader/full/5-kavita-orbit 18/45
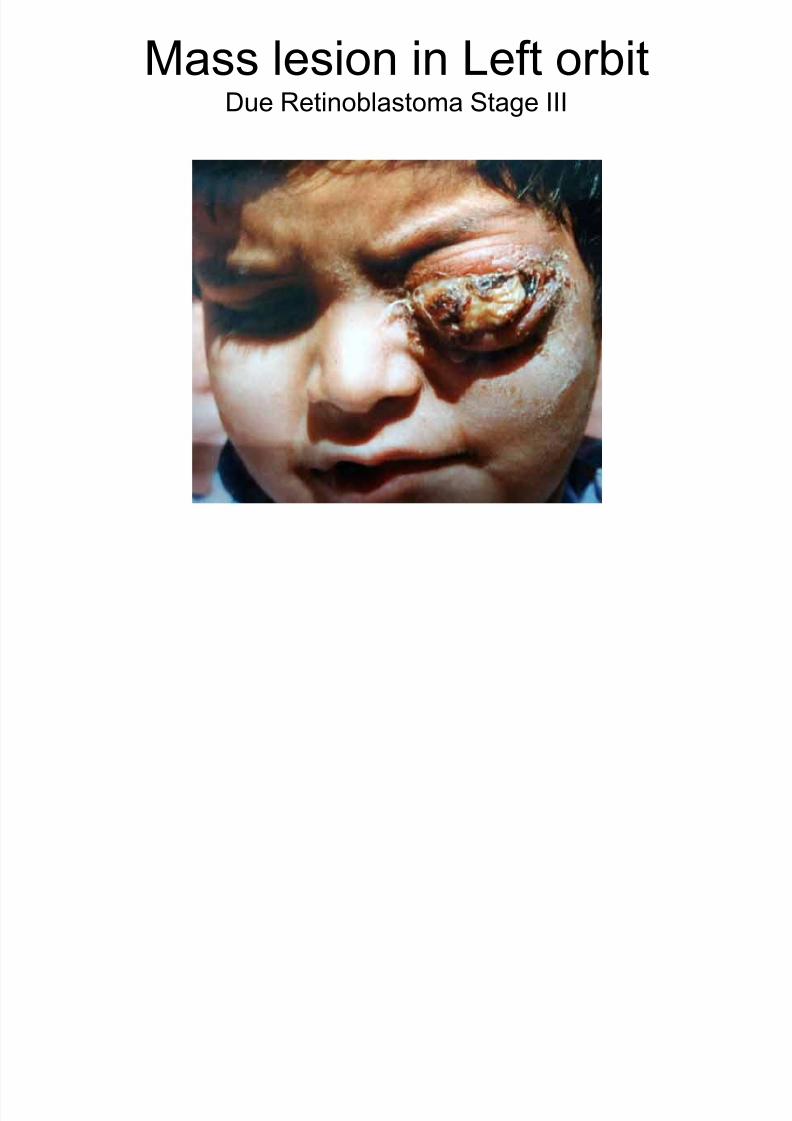
Proptosis in children
• Dermoid and epidermoid cyst
• Capillary haemangioma
• Optic nerve glioma
• Rhabdomyosarcoma
• Leukaemias
• Metastatic neuroblastoma
• Plexiform neurofibromatosis
• Lymphomas
9/20/2014 18
8/11/2019 5. Kavita Orbit
http://slidepdf.com/reader/full/5-kavita-orbit 19/45
Mass lesion in Left orbitDue Retinoblastoma Stage III
8/11/2019 5. Kavita Orbit
http://slidepdf.com/reader/full/5-kavita-orbit 20/45
Proptosis in adults
• Metastases – (of malignancy) from breast,
lung, GIT
• Cavernous haemangiomas
• Mucocele
• Lymphoid tumors
•
Meningiomas
9/20/2014 20

8/11/2019 5. Kavita Orbit
http://slidepdf.com/reader/full/5-kavita-orbit 21/45
Types of Proptosis
• Axial proptosis - eye is pushed directly
forwards – lesions situated in optic nerve
and central space
• Non axial- situated elsewhere in orbit
pushes eye in opposite direction
9/20/2014 21
8/11/2019 5. Kavita Orbit
http://slidepdf.com/reader/full/5-kavita-orbit 22/45
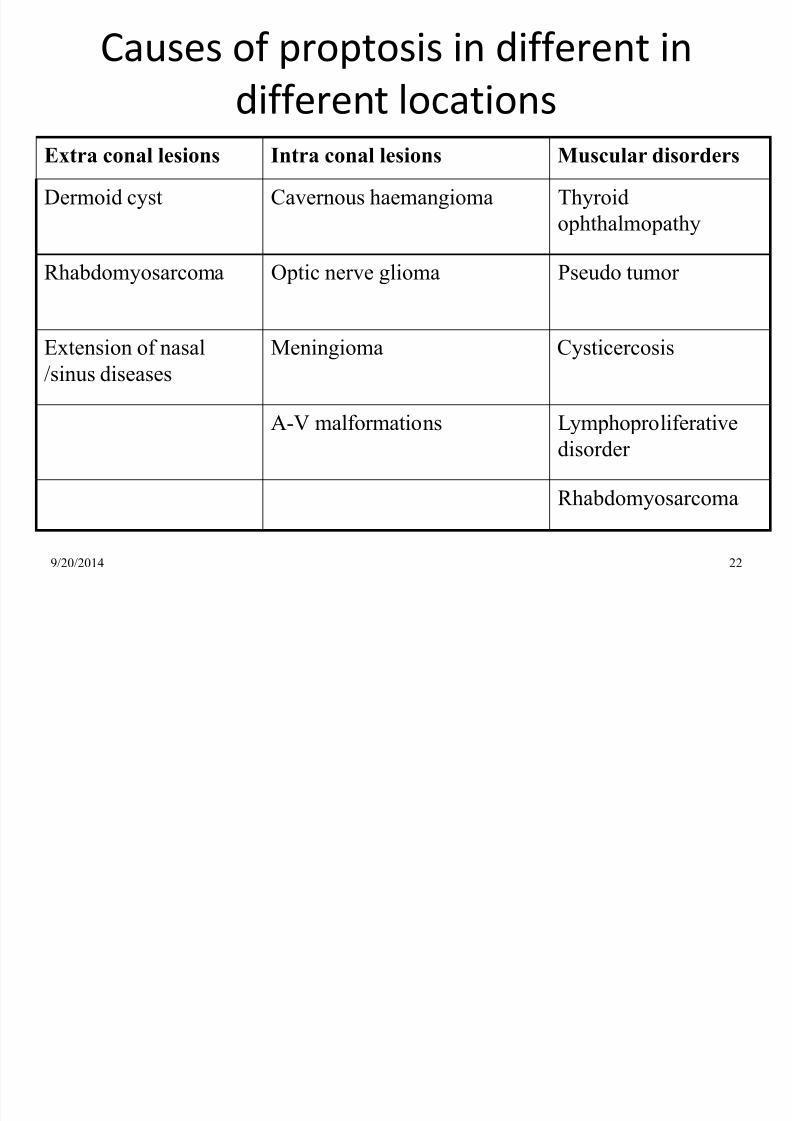
Causes of proptosis in different in
different locations
9/20/2014 22
Extra conal lesions Intra conal lesions Muscular disorders
Dermoid cyst Cavernous haemangioma Thyroid
ophthalmopathy
Rhabdomyosarcoma Optic nerve glioma Pseudo tumor
Extension of nasal
/sinus diseases
Meningioma Cysticercosis
A-V malformations Lymphoproliferativedisorder
Rhabdomyosarcoma
8/11/2019 5. Kavita Orbit
http://slidepdf.com/reader/full/5-kavita-orbit 23/45
Clinical presentation
• Static- as seen usually in congenital causes
• Increasing – fast- as in cases of
Rhabdomyosarcoma, neuroblastoma,
haemopoetic
• Gradual- as in cases of meningiomas
• Pulsatile- as in cases of carotid cavernous
fistula
• Intermittent- as in cases of orbital varicosity
9/20/2014 23
8/11/2019 5. Kavita Orbit
http://slidepdf.com/reader/full/5-kavita-orbit 24/45
Clinical signs
• Impaired mobility
• Diplopia
•
Papilloedema• Optic atrophy
• Hertel exophthalmometry – measures more
than 18 mm• Difference in two eyes of more than 2 mm is
considered positive
9/20/2014 24
8/11/2019 5. Kavita Orbit
http://slidepdf.com/reader/full/5-kavita-orbit 25/45
Investigations
• Careful history recording
• Systemic examination
• ENT examination
• Biochemical and haematological investigations
• Imaging of bony structures- plain x ray
• Imaging of soft tissues –CT scan, MRI
• Vascular study- orbital venography, carotidangiography, MR angiography, digital subtractionangiography
9/20/2014 25
8/11/2019 5. Kavita Orbit
http://slidepdf.com/reader/full/5-kavita-orbit 26/45
Orbital cellulitis
• Definition: Purulent inflammation of the cellular
tissue of the orbit
• Causes of Orbital Cellulitis:
Spread of infection from neighbouring structureslike nasal sinuses, eyelids, eyeball (like in case
of panophthalmitis) facial erysiplas etc
Also due to deep penetrating injuries (speciallyin cases of retained Foreign body) and
metastatic infection in cases of pyaemia
9/20/2014 26
8/11/2019 5. Kavita Orbit
http://slidepdf.com/reader/full/5-kavita-orbit 27/45
Types of Orbital Cellulitis
• Two types- pre septal cellulitis and orbital
cellulitis
• Pre septal –structures anterior to orbital
septum, characterized by erythema,
chemosis, conjunctival discharge without
restriction of ocular movements and visual
impairment
9/20/2014 27
8/11/2019 5. Kavita Orbit
http://slidepdf.com/reader/full/5-kavita-orbit 28/45
Types of Orbital Cellulitis
• Orbital – behind orbital septum,
characterized severe pain, fever, diminution
of vision (due to retrobulbar neuritis or
compression of optic nerve and /or its bloodsupply), massive swelling of lids, chemosis,
proptosis, restriction of ocular movements,
diplopia, an abscess may form pointing
somewhere in the skin of the lid near theorbital margin or fornix
9/20/2014 28
8/11/2019 5. Kavita Orbit
http://slidepdf.com/reader/full/5-kavita-orbit 29/45
Complications
• Panophthalmitis
• Extension into brain through meninges , cavernoussinus thrombosis may develop
• In diabetic patients fungal superinfection maydevelop
9/20/2014 29
8/11/2019 5. Kavita Orbit
http://slidepdf.com/reader/full/5-kavita-orbit 30/45
Management
• Culture and sensitivity of pus, if present and ofblood
• Treatment –
Broad spectrum Intravenousantibiotics , and anti inflammatory
• If abscess has formed – Incision and Drainage
under cover of antibiotics
9/20/2014 30
8/11/2019 5. Kavita Orbit
http://slidepdf.com/reader/full/5-kavita-orbit 31/45
Cavernous sinus thrombosis
• Due to extension of thrombosis from various feedingvessels
• Superior and inferior ophthalmic vein enter in front
•
Superior and inferior Petrosal sinus leave from behind• Cavernous sinus communicates with facial veins,
lateral sinus, jugular vein, Mastoid emmisary vein-
lateral sinus- superior petrosal sinus
9/20/2014side ssss 31
8/11/2019 5. Kavita Orbit
http://slidepdf.com/reader/full/5-kavita-orbit 32/45
Cavernous sinus thrombosis
• Cavernous sinus on one side communicates with
other side through transverse sinus
• Because of connection with mastoid through mastoid
emmisary vein, mastoid tenderness is diagnosticfeature of cavernous sinus thrombosis
8/11/2019 5. Kavita Orbit
http://slidepdf.com/reader/full/5-kavita-orbit 33/45
Source of infection
• Orbital veins - as in cases of eryiepelas, septic
lesion of face, orbital cellulitis , infective
condition of face, mouth, nose, sinuses
• Furuncle of upper lip –
dangerous area of face
• Metastatic infection or septic condition
9/20/2014 33
8/11/2019 5. Kavita Orbit
http://slidepdf.com/reader/full/5-kavita-orbit 34/45
Symptoms and Signs
• Patient may present with symptoms and signs of
Orbital cellulitis, there is sever supra-orbital pain
•Systemic features
– headache, fever ,altered
sensorium, vomiting and cerebral symptoms
• Transference of symptoms and signs to other
eye (bilateral orbital cellulitis with which it may
be confused is very rare clinical condition).Mastoid edema and tenderness is present.
9/20/2014 34
8/11/2019 5. Kavita Orbit
http://slidepdf.com/reader/full/5-kavita-orbit 35/45
Symptoms and Signs
• In case of infection spreading to other eye,
the first sign is involvement of lateralrectus of other eye
• Papilloedema
8/11/2019 5. Kavita Orbit
http://slidepdf.com/reader/full/5-kavita-orbit 36/45
Treatment
• Emergency
• Broad spectrum Intra Venous antibiotics
• Anti coagulants
• Neurophysicians to be consulted
9/20/2014 36

8/11/2019 5. Kavita Orbit
http://slidepdf.com/reader/full/5-kavita-orbit 37/45
Exophthalmos
• Endocrine exophthalmos : Graves
Ophthalmopathy (dysthyroid eye disease) is
the commonest cause of uniocular or bilateral
proptosis in age groups between 25 and 50years
9/20/2014 37
8/11/2019 5. Kavita Orbit
http://slidepdf.com/reader/full/5-kavita-orbit 38/45
Graves Disease
• Consists of Exophthalmos, and all signs of
thyrotoxicosis (i.e. tachycardia, muscular
tremors and raised BMR)
• In early stage the presentation may be
unilateral, becomes bilateral. Palpabral
aperture is wide open due to lid retraction
(Dalrymple sign). Upper lid fail to followdownward movement of eye (von Graefe
sign)
9/20/2014 38

8/11/2019 5. Kavita Orbit
http://slidepdf.com/reader/full/5-kavita-orbit 39/45
Summary of signs in Graves disease
• Lid retraction
• Lid lag (upper and lower
• Infrequent blinking and incomplete closure of lids (Stellwag sign)
•
Lid edema• Exophthalmos
• Conjunctival congestion over the insertion of recti muscles and
chemosis
•Convergence insufficiency (Mobius sign) and Diplopia
• Raised intraocular tension may be present
• Superior limbic keratopathy
9/20/2014 39
8/11/2019 5. Kavita Orbit
http://slidepdf.com/reader/full/5-kavita-orbit 40/45
Werner classification of signs (NO SPECS)
• Grade 0 – No signs or symptom
• Grade 1 – Only sign (lid retraction)
• Grade 2 – Soft tissue involvement (Chemosis)
• Grade 3 – Proptosis (which may be minimum
<23, moderate , marked >28)
•
Grade 4 –
Extraocular muscle involvement• Grade 5 – Corneal involvement
• Grade 6 – Sight loss
9/20/2014 40
8/11/2019 5. Kavita Orbit
http://slidepdf.com/reader/full/5-kavita-orbit 41/45
Exophthalmic Ophthalmoplegia
• Is proptosis with external ophthalmoplegia
• Usually seen in middle aged people , it is of
insidious onset, typically assymetrical limiting
upward movement and abduction due to
swollen, pale edematous, infiltrated ocular
muscles . There is irreducible exophthalmos
with risk of exposure keratitis , globedislocation mechanical compression of optic
nerve and ophthalmic vessels
9/20/2014 41
8/11/2019 5. Kavita Orbit
http://slidepdf.com/reader/full/5-kavita-orbit 42/45
Exophthalmic Ophthalmoplegia
• Disease is self limiting with intermissions and
relapses, usually not affected by any
treatment . Spontaneous resolution may take
place which rarely is complete
9/20/2014 42
8/11/2019 5. Kavita Orbit
http://slidepdf.com/reader/full/5-kavita-orbit 43/45
Treatment of Exophthalmic Ophthalmoplegia
• Short term oral steroid therapy (with dose of 40-60
mg) with radiotherapy (1000 rad ) are effective in
controlling soft tissue inflammation
•Exposed cornea should be protected by doingtarsorrhaphy in less severe cases , by orbital
decompression in more severe cases. Lateral
tarsorrhaphy may also be needed.
• Residual muscle palsy is dealt with muscle
adjustment surgery.
9/20/2014 43
8/11/2019 5. Kavita Orbit
http://slidepdf.com/reader/full/5-kavita-orbit 44/45
Types
• Type –
I : Characterized by symmetrical mildproptosis with lid retraction usually associatedwith thyrotoxicosis
• Type –
II : Characterized by extremeexophthalmos, compressive neuropathy andextraocular muscle involvement. This formmay be associated with any state of thyroid
function, but usually with hypothyroidism,seen after thyroidectomy.
9/20/2014 44
8/11/2019 5. Kavita Orbit
http://slidepdf.com/reader/full/5-kavita-orbit 45/45
Cause of exophthalmos
• Due to edema, lymphocytic infiltration anf
fibrosis of orbital contents and extra-ocular
muscles
• Lid retraction is due to contraction of Muller
muscle