501(r) tax exemption requirements for charitable hospitals presented by eddie phillips, principal...
TRANSCRIPT
501(r) Tax Exemption
Requirements for Charitable Hospitals
Presented byEddie Phillips, Principal
Draffin & Tucker, LLP

Patient Protection and Affordable Care Act
March 23, 2010

Two sets of Proposed Regulations – June 22, 2012 and April 5, 2013.
IRC Section 501(r)

IRS Releases Final 501(r) Regulations
The final IRS regulations were published in the Federal Register on December 31, 2014.
The effective date for the new regulations is for taxable years beginning after December 29, 2015.
For years beginning before the effective date, the final regulations provide that a hospital facility may rely upon a reasonable, good faith interpretation of section 501(r).

Financial Assistance
(FAP)
1. Eligibility criteria used to
determine qualificati
on for assistance
2. Basis for
calculating amounts
charged to patients
3. Method of
applying for
financial assistance
4. Collection
actions that may be taken
5. Measures to widely publicize policy in
community
Section 501(r)(4) requires a hospital facility to establish a written financial assistance policy that must include the following:

FAP Highlights
Final regulations require the FAP be widely publicized but the methods of publicizing the FAP no longer have to be disclosed in the FAP. Disclosure includes -• FAP, PLS* and Application on Website;• Paper copies of FAP, PLS and Application available
upon request both by mail and in public locations within the facility;
• Notify and inform members of the community about the FAP in a manner reasonably calculated to reach those most likely to require assistance.
*Plain Language Summary

FAP Highlights
• Notify and inform individuals receiving care from the facility about the FAP by offering a paper copy of the PLS; including a conspicuous written notice on billing statements about the availability of assistance (and including certain contact information); and setting up conspicuous displays in public locations (or other measures reasonably calculated to attract a patient’s attention) to notify and inform patients about the FAP.
• Public locations are defined to include at a minimum, the ER and admission areas.
• 10% limited English language proficiency translation requirement was changed. Now translations must be provided to LEP* groups that constitute the lesser of 1,000 individuals or 5% of the community. LEP groups must also be considered in the requirements to notify and inform members of the community and in setting up conspicuous displays in facility locations.
*Limited English Proficiency

FAP Highlights
LEP translations are also required to describe:
• The method used to determine the AGB amount, and
• A separate billing and collection policy (if a separate policy exists).

FAP Highlights
• The FAP must list all third party providers delivering emergency or medically necessary care in the hospital facility and identity those providers covered by the FAP (and which are not covered).
• Presumptive eligibility is permitted under the final regulations (at levels less than the most generous amount). Therefore, the FAP must describe any information obtained from sources other than the patient that the facility uses, and whether and under what circumstances it uses prior FAP eligibility determinations.

Others Comments
The final regulations state that a facility may grant financial assistance under its FAP notwithstanding an applicant’s failure to provide information or requested documentation. This clarification allows the facility to rely upon attestations or other evidence submitted by an applicant other than that which is specifically requested.A facility may use a definition of medically necessary using local standards (Medicaid or community/examining physician)

Emergency Care Policy
• Requires a hospital facility to provide care for emergency medical conditions without discrimination to all individuals regardless of whether they are FAP eligible; and
• Prohibits debt collection activities from occurring that may interfere with emergency medical treatment. The preamble to the final regulations indicate certain activities, such as the collection of co-payments upon discharge, checking for qualification for financial or public assistance, and asking for insurance information or co-pays after the patient is stabilized and waiting, are ordinary and unobjectionable activities.

12
Limitation on Charges
• Limit the amount charged for any emergency or other medically necessary care provided to a FAP-eligible individual to not more than the amounts generally billed to individuals with insurance covering that care (AGB).
• Limit the amount charged for any other medical care provided to a FAP-eligible individual to less than the gross charges for that care.

13
Limitation on Charges
Based on allowed claims.May be Medicare onlyMay be Medicare only OR Medicare plus private health insurersMay be Medicaid only, or Medicaid combined with either of the preceding options
Look Back Based on Medicare fee for service only or Medicaid only, or both in combination
Prospective
Methods to determine Amounts Generally Billed (AGB)
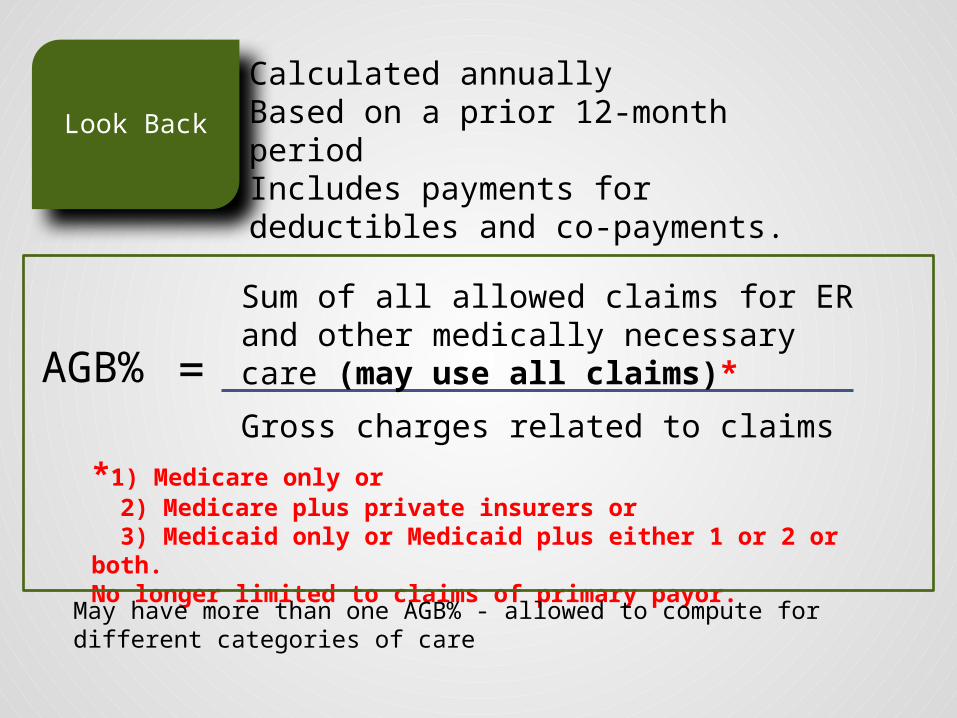
Look Back
Calculated annuallyBased on a prior 12-month periodIncludes payments for deductibles and co-payments.
Sum of all allowed claims for ER and other medically necessary care (may use all claims)*
Gross charges related to claims
*1) Medicare only or 2) Medicare plus private insurers or 3) Medicaid only or Medicaid plus either 1 or 2 or both.No longer limited to claims of primary payor.
AGB% =
May have more than one AGB% - allowed to compute for different categories of care

Limitation on Charges
Billing
Safe Harbor
May charge more than AGB if
1. The FAP-eligible individual has not submitted a complete FAP application as of time of charge;
2. Any excess charge was not made or requested as pre-condition of providing medically necessary care*; and
3. Once a completed FAP application is received and the individual is determined to be FAP-eligible, the facility refunds any amounts paid for care in excess of amount the individual is determined to be personally responsible for paying ($5 de minimis exception).
*prepayments should not exceed AGB

MUST forego extraordinary collection actions (ECA) before the hospital has made reasonable efforts to determine whether the individual is eligible for financial assistance.
16
Limitation on Charges
Billing
To have made a reasonable effort, a hospital facility should:• Refrain from initiating any ECAs for 120 days from
the date of the first post-discharge billing statement,
• Follow up with regard to incomplete applications in a prescribed manner, and
• Notify the individual before initiating any ECAs to obtain payment for care in a prescribed manner.
Notification of ECAs
The final regulations require a facility to do the following at least 30 days before initiating any ECAs:• Provide written notice that indicates assistance is
available, identifies the ECAs the facility intends to initiate to obtain payment, and states a deadline that is at least 30 days from the date the notice is provided.
• Provide a PLS of the FAP with the written notice.• Make reasonable efforts to orally notify the
individual of the FAP and how they the applicant can obtain assistance with the FAP process.

ECA Notification
• Multiple episodes of care may be aggregated for notification purposes, but the 120 day prohibition from initiating ECAs must run from the first post-discharge billing statement for the most recent episode of care.
• The notification period may be less that 30 days in situations involving the denial of care due to nonpayment for prior care if:o The individual is provided with an application form and
written notice of FAP availability which states a deadline on accepting and processing the application for the prior care and the deadline is no earlier than the later of 30 days from the date the written notice is provided or the 240 day application period for the prior care.
o The facility expedites the FAP application process if a timely submitted FAP application is received.

Reasonable efforts to determine eligibility for financial assistance
---------------- Minimum Application Period ------------
At least 30
days before
initiating any
ECAs - Notify
19
Begins on the date of 1st Post Discharge Bill
120 days after first
billing statement to
individual
240 days after first post discharge billing statement to individual
-----Period of Restraint-------
ECA may begin if no application is received but may have to be suspended.
Extraordinary collection efforts
ECAs that require a legal or judicial process include, but are not limited to, actions to—
o Place a lien on an individual's property;o Foreclose on an individual's real property;o Attach or seize an individual's bank account or any other
personal property;o Commence a civil action against an individual;o Cause an individual's arrest;o Cause an individual to be subject to a writ of body attachment;o Garnish an individual's wages;o Selling debt (with exception);o Reporting adverse information to credit reporting agencies;
ando Deferring, denying or requiring payment for medically
necessary care because of nonpayment of previous FAP covered care.
20

Extraordinary collection efforts
Sale of Debt Exception to ECA classification requires a binding written agreement with the purchaser that includes these requirements:
1. Purchaser is prohibited from engaging in ECAs to obtain payment;2. Purchaser is prohibited from charging interest in excess of the IRS
underpayment rate at the time the debt is sold;3. The debt is returnable or recallable to the hospital facility upon
determination of FAP-eligibility; and4. If the individual is determined to be FAP-eligible and the debt is
not returned or recalled, the purchaser is required to adhere to the procedures specified in the agreement that ensure the individual does not pay the purchaser and/or the hospital more than that person is responsible for paying under the FAP.
21

Referral to collection agency
• Debts may be referred to third parties to assist with collection actions at any time, including the initial 120-day period. The collection agent is subject to the same restrictions as the hospital.


Conducting CHNA
Final Regulations –Organization is still required to –
1. Define the community served,2. Assess the health needs of the community,3. Take into account input from the persons who
represent the broad interest of the community including those with special knowledge in public health,
4. Document the CHNA in a written report, and5. Make the CHNA widely available (current CHNA
and CHNA previous to current one should be available).

CHNA - Community Served
Final regulations -• Allow flexibility in allowing the organization to define the
community it serves.• Prohibit discrimination against medically underserved, low-
income or minority populations. For example, a facility may not define its community to exclude medically underserved, low-income or minority populations who live in geographic areas form which the facility draws its patients unless such populations are not part of the facility’s target patient populations.
• For a facility consisting of multiple buildings operating under a single license serving different geographic areas or populations, the community served is the aggregate of such areas.

CHNA – Assessing Needs
Final regulations require the facility to –o Identify significant health needs of
community,o Prioritize these needs, o Identify resources (both internal and
external) potentially available to address the health needs.
But do not require specific criteria for prioritizing the identified needs.

CHNA – Persons Representing the Broad Interest of the Community
Input must be taken into account from –
1. At least one state, local, tribal or regional governmental health department (the final regulations include a reference to the State Department of Rural Health as a public health option),
2. Members or representatives of the underserved, low-income and minority populations in the community,
3. Written comments received on the most recent CHNA (including the implementation strategies).

Broad Interest of the Community
• Final regulations do not require input from both a governmental public health department and someone with special knowledge or expertise in public health since the governmental department should have such expertise.
• Organizations are granted flexibility with regard to choosing the jurisdictional level of governmental public health department is most appropriate.
• Posting a draft copy of the CHNA on the facility’s website for public review and comment is an option for seeking input.

Medically Underserved
• Final regulations maintain the requirement to consider input from the medically underserved, low-income and minority populations.
• Medically underserved is defined to include populations experiencing health disparities or at risk of not receiving adequate care due to financial, geographic, language or other barriers.
• The facility may use direct input from such persons (surveys, focus groups, interviews, etc.) or from their representatives.

Documentation of the CHNA
CHNA report must include:
• Definition of the community served and a description of how the community was determined,
• Description of the process and methods used to conduct the CHNA (data and collection methods used in the assessment, methods of analyzing data, collaborative partners used to conduct the CHNA and those hired to assist in the process. The CHNA report may cite the source material in the case of data obtained from external sources.),
• Description of how input from those representing the broad interest of the community was solicited and taken into account,

Documentation of the CHNA
CHNA report must include:
• Prioritized description of the significant health needs identified (including a description of the process and criteria used to identify and prioritize such needs),
• Description of potential resources available, and
• An evaluation of the impact of any actions that were taken since the prior CHNA was conducted to address the significant health needs identified in the previous CHNA.

Collaborative CHNA
Final regulations permit collaboration, but-1. Separate documentation for each facility’s CHNA is required
to be contained in a separate report (portions of CHNA may be identical where appropriate), or
2. Joint CHNA reports are allowed if community is defined the same and the joint CHNA clearly identifies each participating facility (and the authorized body of the facility adopts the joint report for each facility).

Implementation Strategies
• Describe how the facility plans to address a specific health need. Describe the actions to be taken, the anticipated impact of these actions and a plan to evaluate such impact. Must also identify the resources the facility plans to commit to addressing the health need and any planned collaboration.
• Identify the health need as one not intended to be addressed with an explanation as to why it is not being addressed (resource constraints, lack of experience or expertise, lack of effective interventions, other parties better suited to address the need, etc.).
• Must be adopted by the 15th day of the 5th month following the taxable year during which the CHNA is conducted.
• Adoption by an authorized body is mandatory.

Joint Implementation Strategies
If a joint CHNA is issued with collaborative partners, joint implementation strategies may also be adopted but the facility’s role and responsibilities in taking the actions identified must be stated clearly, and the programs and resources the facility plans to commit to such actions clearly identified.
A summary or other tool must be developed for each facility subject to the CHNA requirement.

New Facilities
If subject to the CHNA requirement, a new facility must meet the requirements by the end of the second taxable year beginning after the date the facility is acquired, licensed, registered or similarly recognized as a hospital.

Section 501(r) Failures
Loss of Exemption is Possible (1.501(r)-2)o IRS will consider:
• Previous failures, if any,• Size, scope, nature and significance of the failure,• Multiple facilities,• Reason for failure,• Prior to failure, compliance practices and policies,
and whether they were routinely followed,• Implementation of safeguards,• Correction of the failure by the organization, and• Safeguards and correction occur prior to discovery by
IRS.

Special Rule for Multiple Facilities
If an organization operates more than one facility, failure at one (or more) may result in–
• Income from the noncompliant facility being subject to taxation,
• The continued exemption of the organization, and
• No adverse impact on tax-exempt bonds.
If income from the facility is subject to taxation, such income may not be aggregated with other noncompliant facilities or other unrelated business income.

Section 501(r) Failures
The final regulations largely adopt the guidance offered in IRS Notice 2014-3 regarding failures and omissions. The regulations address failures by class:
• Minor omissions and errors that promptly corrected are not failures;
• Failures that are neither willful nor egregious if corrected and disclosed generally are not penalized (except for 4959 excise tax for CHNA failures);
• Failures that are willful or egregious will result in loss of tax exempt status.

Definitional Changes for Failures
• Correctible errors are minor and either inadvertent or due to reasonable cause.
• Multiple minor errors must be aggregated.
• Commission of a previously corrected minor error is a factor indicating the error is not inadvertent.
• Having established practices or procedures designed to promote compliance before an error is committed is a factor that indicates reasonable cause has been utilized.
• Correction and disclosure of an error is a factor that indicates a failure is not willful.
• Application of a facility level tax generally does not result in the facility being considered an unrelated trade or business.

Examples of Corrections*
• CHNA does not contain all of the elements required by 1.501(r)-3.
• FAP does not contain all of the elements required by 1.501(r)-4.
• Hospital charges FAP-eligible individuals more than a permitted amount under 1.501(r)-5.
• Hospital fails to widely publicize its FAP.
*from IRS Notice 2014-3

Recommended Actions
• Update the board on changes to section 501(r) and the role they must play in adopting the required policies.
• Review and update the methods used to publicize the FAP:
o Identify public locations in the facility that will need displays.
o Update billing statements for required communications.
o Review methods used to notify and inform members of the community served by the facility about the FAP.
o Revise patient intake and/or discharge procedures to ensure every patient is offered a PLS of the FAP.
• Assess document translation needs for the community under the lower LEP thresholds.

Recommended Actions
• Revise FAP to list third party service providers delivering emergency or medically necessary care in the facility. Identify which are and which are not covered by the FAP.
• Review FAP limitation on charges with regard to under insured patients .
• Review AGB calculation method. Consider impact of Medicaid alternative. Test prospective and look back method calculations (as well as multiple AGBs under the look back method).
• Review definition of medically necessary care and care covered by the FAP.
• Review all collection actions. • Review and update presumptive eligibility assistance.

Questions?
Contact Information:Eddie Phillips, PrincipalDraffin & Tucker, LLPAtlanta, [email protected](404) 719-4070