6-2 ars final au edited final hiv 17 chi dr kolson build ... · hiv infiltrates the cns early...
TRANSCRIPT

1
Page 1
Dennis Kolson, MD, PhDProfessor of Neurology
University of PennsylvaniaPhiladelphia, Pennsylvania
Update on Neurologic Complications in Persons With HIV Infection: 2017
FORMATTED: MM/DD/YY
Chicago, Illinois: May 10, 2017
Slide 2 of 34
Financial Relationships With Commercial Entities
Dr Kolson has no relevant financial affiliations to disclose. (Updated 05/04/17)
Slide 3 of 34
Learning Objectives
Recognize and list the early neurologic manifestations of acute HIV infection
Describe the chronic neurologic manifestations and potential management options for neurologic complications of HIV infection in individuals on suppressive antiretroviral therapy
To describe the rationale for adjunctive neuroprotective strategies for cognitive impairment in individuals on suppressive antiretroviral therapy
After attending this presentation, learners will be able to:
Chicago, Illinois: May 10, 2017

2
Page 2
• HAND prevalence remains ~ 40%
BUT
• less severe HAND: encephalitis & dementia now ~2%
• neuropathy prevalence < 30% with newer ARTs
HAND
Post-ART eraneuropathy
Neurological complications of chronic HIV infection are less severe with use of antiretroviral therapy/ARTPre-ART era
HIV-encephalitis (HIVE)HIV-associated neurocognitive disorders (HAND)
• HIV-associated neurocognitive disorders (HAND) ~ 40%
• severe HAND: HIV encephalitis & dementia ~20%
• neuropathy prevalence ~ 30%
HIV encephalitisHAND
neuropathy
Slide 4 of 34
HIV infiltrates the CNS early (days-week) after systemic HIV Infection potential CNS reservoir
Adapted from Gill & Kolson, Crit. Rev. Immunol. (2013).
NEURON
ASTROCYTE
MACROPHAGE
proinflammatorycytokines/chemokines
ACTIVATEDMACROPHAGE/
MICROGLIA
viral replication
NMDA Receptor Excitotoxins
Glutamate Regulation
Neuronal Injury(loss of synapses
and dendrites
Endothelial Lumen
Blood Brain Barrier
HIV MONOCYTE
GlutamateQUIN, ROS,Ntox, PAF, TNF- , &
gp120, Tat
CD4+ T lymphocyteHIVHIV
Slide 5 of 34
CD4+ T lymphocyte
?
Slide 6 of 34
CNS compartmentalization in as early as 4 months & throughout course
Independent HIV replication in infiltrating lymphocyte population (pleocytosis)
Entering virus is exclusively R5, T lymphocyte-tropic
Little initial independent HIV replication in endogenous CNS cell population (macrophages), which begins to emerge during the first two years of infection, suggesting establishment of a macrophage reservoir)
Compartmentalization occurs in state of pleocytosis & higher viral loads
Presumably from replication in a CNS pool established by infiltrating T lymphocytes
Two ways to increase CSF viral load (early infection)
Influx of infected T lymphocytes carrying virus into the CNS
Replication in the CNS pool established by infiltrating T lymphocytes (compartmentalization)
Sturdevant, PLOS Path. (2015)
Chicago, Illinois: May 10, 2017
3
Page 3
Slide 7 of 34
What are the neurological complications of acuteHIV infection?
• meningitis • Acute Inflammatory Demyelinating Neuropathy (AIDP)
Early neurological complications of HIV infection prior to
initiation of antiretroviral therapy/ART
• IRIS
• meningitis• Acute IDP
• HAND (less severe) • Chronic IDP• DSPN • PML
Slide 7 of 34
HIV-associated neurocognitive disorders (HAND)Distal Symmetric Polyneuropathy (DSPN)
Early HIV infection (days 10-20) is associated with symptoms of meningitis in ~25% of individuals*
Meningitis (~25%)
McMichael AJ, Nat. Rev. Immunol. (2010)
*Typically HIV antibody ELISA negative at this time
Slide 8 of 34
Chicago, Illinois: May 10, 2017

4
Page 4
• IRIS
• meningitis• Acute IDP
• HAND (less severe) • Chronic IDP• DSPN • PML
Early neurologic complications of HIV-1 infection:Acute Inflammatory Demyelinating Polyneuropathy (AIDP)
Slide 10 of 34
HIV-associated neurocognitive disorders (HAND)Distal Symmetric Polyneuropathy (DSPN)
Early neurologic complications of HIV-1 infection:Acute inflammatory Demyelinating Polyneuropathy (AIDP)
http://emedicine.medscape
• CSF: < 50 cells/ul• elevated protein• indistinguishable from GBS
Symptoms & signs TreatmentNatural history
• weakness
• mild sensory sx.
• pain
• respiratory
• autonomic
• ankle reflexes absent
• plasmapheresis
• IVIG
• corticosteroids
• response rates probably similar to HIV-negative patients
• AIDP: (rare)
• most often at seroconversion (20-30d)
• progresses rapidly over days to < 4 weeks
Robinson-Papp, Muscle & Nerve. (2009)Kaku M, Curr Opin HIV AIDS. (2014)
Slide 11 of 34
Slide 13 of 34
Chronic neurological complications of HIV infection:• Chronic Inflammatory Demyelinating Neuropathy (CIDP)
• Distal Symmetric Polyneuropathy (DSPN)
• HIV-associated neurocognitive disorders (HAND)
Chicago, Illinois: May 10, 2017

5
Page 5
• IRIS
Later neurological complications of HIV infection after initiation of antiretroviral therapy/ART
• meningitis• Acute IDP
• HAND (less severe) • Chronic IDP• DSPN • PML
Slide 13 of 34
HIV-associated neurocognitive disorders (HAND)Distal Symmetric Polyneuropathy (DSPN)
• CSF: < 50 cells/ul• elevated protein• indistinguishable from idiopathic CIDP
Symptoms & signs TreatmentNatural history
• weakness
• mild sensory sx.
• pain
• respiratory
• autonomic
• ankle reflexes absent
• plasmapheresis
• IVIG
• response rates probably similar to HIV-negative patients
• CIDP: >1 year- later stages of HIV infection
• up to 30%of CIDP patients are HIV+*
• progresses over > 8 weeks
• relapses and remissions
Robinson-Papp, Muscle & Nerve. (2009)Kaku M, Curr Opin HIV AIDS. (2014)
Later neurological complications of HIV infection:Chronic inflammatory demyelinating polyneuropathy (CIDP)
Peripheral nerve onion-bulb in CIDP
Slide 14 of 34
*http://emedicine.medscape
• IRIS
Later neurological complications of HIV infection:Distal symmetric polyneuropathy (DSPN)
• meningitis• Acute IDP
• HAND (less severe) • Chronic IDP• DSPN • PML
• meningitis • HAND (less severe) • Chronic IDP
Slide 15 of 34
HIV-associated neurocognitive disorders (HAND)Distal Symmetric Polyneuropathy (DSPN)
Chicago, Illinois: May 10, 2017

6
Page 6
Robinson-Papp, Muscle & Nerve. (2009)Kaku M, Curr Opin HIV AIDS. (2014)
• Capsaicin (8% top.)‘proved’ effective gabapentin lamotrigine
(weak evidence)
• modify ART regimen
‘
Later neurological complications of HIV infection:Distal symmetric polyneuropathy (DSPN)
Symptoms & signs TreatmentNatural history
• Symmetric, distal, sensory (axonal +/- demyelinating)
Pain predominates• burning• hyperalgesia
• tightness• numbness• preserved proprioception
• prevalence ~ 30%• occurs with or without
ART use
• ART associated(d-drugs):
d4T (Stavudine)ddI (didanosine)ddC (zalcitabine)
‘
Stocking/glove distribution of pain in DSPN
Slide 16 of 34
http://emedicine.medscapeSimpson, Neurol. (2008),
Slide 18 of 34
Question #1
A 40 year old diabetic man presents to the ED with ascending weakness and mild numbness of the lower extremities (one week), and now he cannot walk. Two weeks prior he presented with a severe headache and neck stiffness; CSF showed a mild lymphocytosis. He had mentioned recent high-risk behavior, but was seronegative then. He is now seropositive for HIV infection. Among the following, which is most likely?
1. Diabetic Neuropathy
2. Distal Symmetric Polyneuropathy (DSPN)
3. Acute Inflammatory Demyelinating Polyneuropathy (AIDP)
4. Spinal cord infarction
Slide 19 of 34
Chicago, Illinois: May 10, 2017

7
Page 7
Slide 20 of 34
Question #1
A 40 year old diabetic man presents to the ED with ascending weakness and mild numbness of the lower extremities (one week), and now he cannot walk. Two weeks prior he presented with a severe headache and neck stiffness; CSF showed a mild lymphocytosis. He had mentioned recent high-risk behavior, but was seronegative then. He is now seropositive for HIV infection. Among the following, which is most likely?
1. Diabetic Neuropathy
2. Distal Symmetric Polyneuropathy (DSPN)
3. Acute Inflammatory Demyelinating Polyneuropathy (AIDP)
4. Spinal cord infarction
Later neurological complications of HIV infection: Immune Reconstitution Inflammatory Syndrome (IRIS)
• meningitis• Acute IDP
• HAND (less severe) • Chronic IDP• DSPN • PML
• meningitis • HAND (less severe) • Chronic IDP
• IRIS
Slide 17 of 34
HIV-associated neurocognitive disorders (HAND)Distal Symmetric Polyneuropathy (DSPN)
Initiation of cART (1-6 months): CNS syndrome (mild or severe) resulting from heightened immunologic and/or inflammatory response against opportunistic pathogens (or other antigens associated with HIV suppression by cART)
• robust inflammatory CNS infiltration (MRI detection)
• CNS IRIS in ~1-30% of pts. initiating cART
• rapid decline of viral load
- greatest risk with CD4 <50 and VL >100K
• most commonly associated with crypto meningitis, TB, PML
Johnson, Ann NY Acad Sci (2010)Johnson, Curr Opin HIV AIDS (2014)
Later neurological complications of HIV infection: Immune Reconstitution Inflammatory Syndrome (IRIS)
Slide 18 of 34
Chicago, Illinois: May 10, 2017

8
Page 8
Slide 23 of 34HIV-associated CNS IRIS
Zafiri et al. New Microbiologica. (2013)
57 yo HIV+ man, off ART x 3 years, then re-start:3 weeks right hemiparesis, slurred speech
CD4 T cells24 99/mm3
CSF:56 cells/ul64 mg/dl prot.
Admission: stroke 24 days post-ART: IRIS
31 days post-ART: IRIS
Slide 19 of 34
Slide 24 of 34HIV-associated CNS IRIS in PML patient Slide 20 of 34
Vendrely A, Acta Neuropathol. (2005)
52 yo HIV+ man, ART naïve x 16 years, admitted for sub-acute cognitive decline
cART started:CD4 T cells117 284/mm3
JC virus confirmed at autopsy
Before ART
1 mo. post-ART
• Supportive Care CSF drainage (Crypto), Abscess drainage (needle aspiration)
• Treatment for any underlying opportunistic infection• Anti-inflammatory treatment
NSAIDs Corticosteroids: severe cases
• 2-3wks, then taper • Investigational/Anecdotal treatments
None yet proven• Pausing HAART
reserved for severe, life-threatening symptoms risks of immunodeficiency & resistance
Later neurological complications of HIV infection: Immune Reconstitution Inflammatory Syndrome (IRIS)
Management:
Slide 21 of 34
Chicago, Illinois: May 10, 2017

9
Page 9
Later neurological complications of HIV infection: Progressive Multifocal Leukoencephalopathy (PML)
• meningitis• Acute IDP
• HAND (less severe) • Chronic IDP• DSPN • PML
• meningitis • HAND (less severe) • Chronic IDP
• IRIS
Slide 22 of 34
HIV-associated neurocognitive disorders (HAND)Distal Symmetric Polyneuropathy (DSPN)
Later neurological complications of HIV infection: Progressive Multifocal Leukoencephalopathy (PML)
Symptoms & signs TreatmentNatural history
• papovavirus (JC virus) activation in the brain
• white matter (myelin) damage, early in occipital areas
• ~4% of all untreated patients
• ~1% in ART-treated patients
• Death within ~1 year in 90%
• hemiparesis
• memory loss
• slurred speech
• seizures
• visual sxs., blind spots
• sensory disturbances
up to 60%
~30-60%
~20-40%
~15-30%
~25%
~20%
• None effective
• ?inhibit JC virus
• ?reconstitute immune system
Slide 23 of 34
Later neurological complications of HIV infection: Progressive Multifocal Leukoencephalopathy (PML)
Note lesions restricted to white matter
Slide 24 of 34
Chicago, Illinois: May 10, 2017
10
Page 10
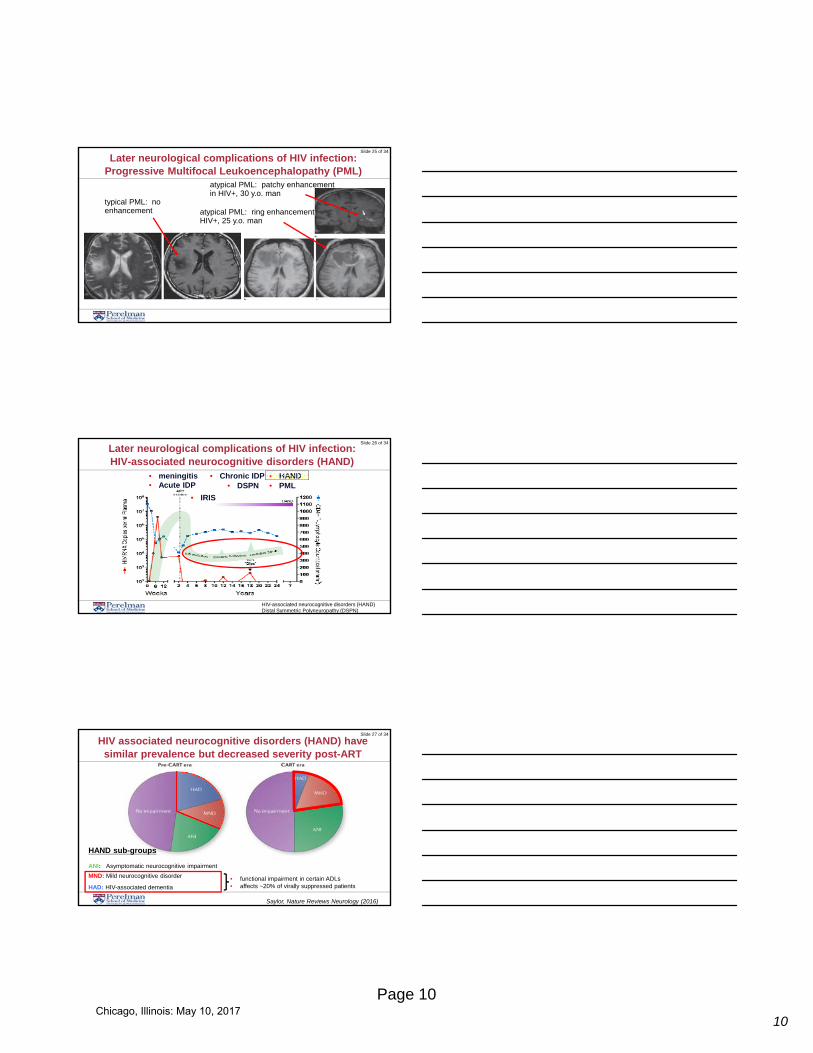
Later neurological complications of HIV infection: Progressive Multifocal Leukoencephalopathy (PML)
atypical PML: patchy enhancement in HIV+, 30 y.o. man
atypical PML: ring enhancementHIV+, 25 y.o. man
typical PML: no enhancement
Slide 25 of 34
• IRIS
• meningitis • HAND• DSPN • PML
Later neurological complications of HIV infection: HIV-associated neurocognitive disorders (HAND)
Slide 26 of 34
HIV-associated neurocognitive disorders (HAND)Distal Symmetric Polyneuropathy (DSPN)
• Acute IDP• Chronic IDP
HIV associated neurocognitive disorders (HAND) have similar prevalence but decreased severity post-ART
Saylor, Nature Reviews Neurology (2016)
HAND sub-groups
ANI: Asymptomatic neurocognitive impairment
MND: Mild neurocognitive disorder
HAD: HIV-associated dementia
• functional impairment in certain ADLs• affects ~20% of virally suppressed patients
Slide 27 of 34
Chicago, Illinois: May 10, 2017

11
Page 11
HIV-associated neurocognitive disorders (HAND)
Later neurological complications of HIV infection: HIV-associated neurocognitive disorders (HAND)
• 1/3 have MRI evidence of white matter abnormality, with or without brain atrophy
46 year old man, HIV+ for ~20 years, CD4 nadir 50+ cells/ulbegan ART after severe immunosuppresion; white matter lesions + brain atrophy
Slide 28 of 34
• Using ART regimens with higher CNS penetration?
multiple (conflicting) reports suggest no benefit
ART drugs may directly induce oxidative stress and neuronal damage
• Intensification of ART regimens with additional classes of antivirals?
* recent studies of Maraviroc (CCR5 blocker) suggest possible benefit
additional studies underway
• Adjunctive therapies in addition to ART?
focus on controlling neuroinflammation & oxidative stress
How to reduce residual HAND impairment in ART- treated individuals?
Slide 29 of 34
* Gates, AIDS (2016)
HAND Diagnosis
NCNNeurocognitively Normal
HANDHIV-associated neurocognitive disorders
HIVEHIV-encephalitis
Gill et al. J Clin Invest (2014)
Heme oxygenase-1 protein reduction in the prefrontal cortex correlates with clinical dysfunction (HAND)
Chicago, Illinois: May 10, 2017

12
Page 12
HIV-associated neurocognitive disorders (HAND)Distal Symmetric Polyneuropathy (DSPN)
• IRIS
• meningitis• Acute IDP
• HAND (less severe) • Chronic IDP• DSPN • PML
• meningitis • Chronic IDP
Neuropathy (less severe)
HAND
Neurological complications of HIV can persist in ART-treated individuals and require adjunctive therapies to limit morbidity
Slide 30 of 34
Slide 36 of 34
Question #2
A 34 year old woman came to the ED with a 3-4 day history of confusion & disorientation, which were worsening. She stated that she was diagnosed with HIV infection more than 3 years ago, when she was diagnosed with a brain infection (she was unclear what type). She started, then discontinued ART and re-started it only ~2 months ago. Her physical examination confirmed altered mental status. Her MRI showed a gadolinium-enhancing lesion of the parietal lobe, no meningeal enhancement. Cryptococcal antigen was negative.
1. HIV-associated neurocognitive disorders (HAND)
2. Immune Reconstitution Inflammatory Syndrome (IRIS)
3. HIV meningitis
Slide 37 of 34
Chicago, Illinois: May 10, 2017

13
Page 13
Slide 38 of 34
Question #2
A 34 year old woman came to the ED with a 3-4 day history of confusion & disorientation, which were worsening. She stated that she was diagnosed with HIV infection more than 3 years ago, when she was diagnosed with a brain infection (she was unclear what type). She started, then discontinued ART and re-started it only ~2 months ago. Her physical examination confirmed altered mental status. Her MRI showed a gadolinium-enhancing lesion of the parietal lobe, no meningeal enhancement. Cryptococcal antigen was negative.
1. HIV-associated neurocognitive disorders (HAND)
2. Immune Reconstitution Inflammatory Syndrome (IRIS)
3. HIV meningitis
Slide 39 of 34
Thank you!
Kolson Lab: Univ. of Pennsylvania
• Alexander Gill, MD, PhD student
• Colleen Kovacsics, PhD student• Yoelvis Garcia-Mesa, PhD
• Rolando Garza, BS• Patricia Vance, BS
Penn Center for AIDS Research
• Ron Collman, MD (Director)
University of Texas Medical Branch
• Ben Gelman, MD, PhD
University of North Carolina, Chapel Hill
• Kevin Robertson, PhD
AcknowledgementsSlide 32 of 34
Chicago, Illinois: May 10, 2017

14
Page 14
Dennis Kolson, MD, PhDProfessor of Neurology
University of PennsylvaniaPhiladelphia, Pennsylvania
Update on Neurologic Complications in Persons With HIV Infection: 2017
FORMATTED: MM/DD/YY
Chicago, Illinois: May 10, 2017
Chicago, Illinois: May 10, 2017