6/9/2015f. atashzadeh1. fecal incontinence related to pregnancy, vaginal delivery, and cesarean...
TRANSCRIPT

04/18/23 F. Atashzadeh 1

Fecal incontinence related to pregnancy, vaginal delivery, and cesarean
Foroozan Atashzadeh ShoridehPhD nursing Candidate, Shahid Beheshti Medical University
04/18/23 F. Atashzadeh 2

Fecal incontinence has a significance impact on quality of life.
Vaginal delivery is the major risk factor for the development of pelvic organ prolapse and urinary and fecal incontinence, resulting from damage to the pelvic floor muscles, nerves and connective tissue.
04/18/23 F. Atashzadeh 3
Bortolini et al 2010

Definition Fecal incontinence refers to the
involuntary loss of solid or liquid stool.
Anal incontinence also includes involuntary release of flatus.
The consequences of AI can be detrimental to the psychological, social, and sexual wellbeing of the patient.
04/18/23 F. Atashzadeh 4
Tin et al , 2010
Prevalence
depending on the population studied,
the definition of type of stool loss, and
the frequency of episodes
04/18/23 F. Atashzadeh 5

Causes of Fecal Incontinence
04/18/23 6F. Atashzadeh

How does pregnancy affect pelvic floor dysfunction?
This is probably the result of the extra
weight of the uterus and baby on the pelvic
floor.
04/18/23 F. Atashzadeh 7

PREGNANCY AND FECAL INCONTINENCE
In studies of nulliparous women, the
prevalence of fecal incontinence increased
from 1% prior to pregnancy to 7% during
pregnancy.
04/18/23 F. Atashzadeh 8
Chaliha et al 1999, 2001

Labor and fecal incontinence
The risk of fecal incontinence associated
with second stage of labor appears to be
similar to the risk of vaginal delivery.
04/18/23 F. Atashzadeh 9
Liebling 2005, Bahl 2004

vaginal delivery and fecal incontinence
Controversial Anal incontinence was significantly
increased after spontaneous vaginal delivery compared to cesarean delivery (OR 1.32, 95% CI 1.04-1.68).
The risk of fecal incontinence alone was not significantly increased.
04/18/23 F. Atashzadeh 10
Pretlove et al 2008
Fecal incontinence after first
instrumental vaginal delivery
using Thierry’s spatulas
04/18/23 11F. Atashzadeh
Parant et al 2010
Fecal incontinence was assessed at 2 and 6
months
postpartum by a questionnaire (Wexner
score 5 was considered significant)
04/18/23 12F. Atashzadeh

Results
Episiotomy (odds ratio [OR]=5.0) and maternal age over 35 years (OR=4.1) were independently associated with fecal incontinence after adjustment.
04/18/23 13F. Atashzadeh

Role of anal sphincter laceration
In women with obstetric anal sphincter injuries
(OASIS), the risk of subsequent fecal
incontinence is estimated to be 9 to 28 percent.
04/18/23 F. Atashzadeh 14
Pollack et al 2004

Vaginal delivery or cesarean?
vaginal delivery (76%) was associated with
a greater risk of fecal incontinence
compared with cesarean delivery (24 %), if
the delivery conferred a laceration or
required instrumentation.
04/18/23 F. Atashzadeh 15
Guise et al 2009

Operative vaginal delivery
Operative vaginal delivery is a risk factor for anal sphincter laceration and other pelvic floor disorders.
This risk is further increased if the fetus is in the occipital posterior position.
The risk of OASIS appears to be higher in forceps deliveries than in vacuum-assisted delivery.
04/18/23 F. Atashzadeh 16

Type of episiotomy
Median
Mediolateral episiotomy
04/18/23 F. Atashzadeh 17
Birth weight
an odds ratio of 1.47 for a sphincter laceration with each 500 g increase in fetal birth weight
04/18/23 F. Atashzadeh 18
Prolonged second stage of labor
exceeds 60 minutes
04/18/23 F. Atashzadeh 19

Maternal birth position
standing, squatting or lithotomy positions
04/18/23 F. Atashzadeh 20
Maternal age
As an example, an observational study of
women reported an increase in odds ratio of
1.09 per year of maternal age (95% CI 1.06-
1.12).
04/18/23 F. Atashzadeh 21
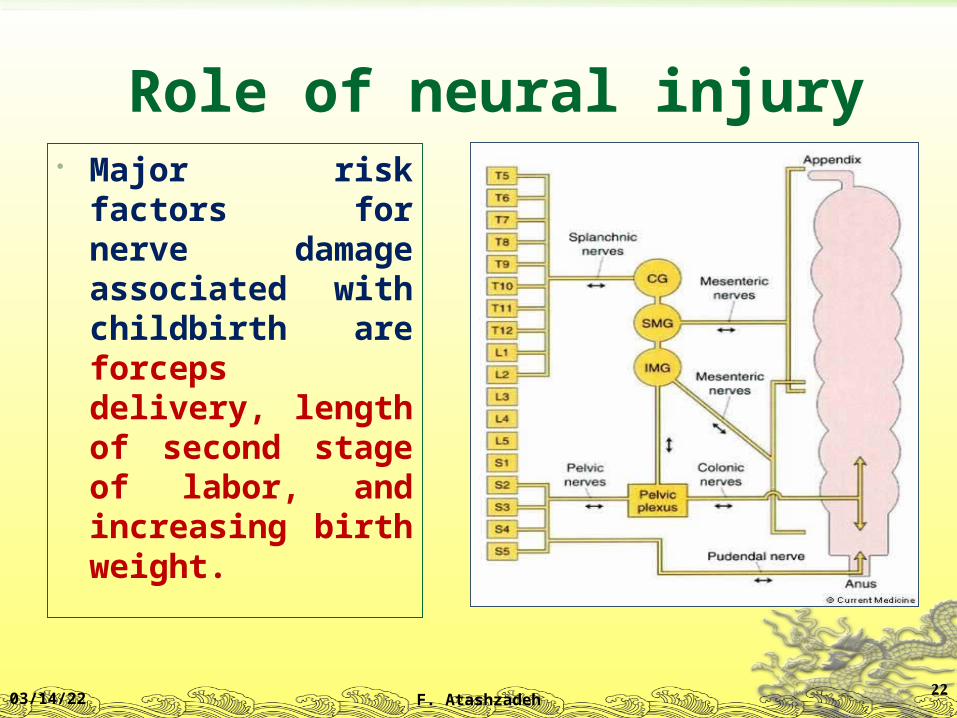
Role of neural injury Major risk factors
for nerve damage associated with childbirth are forceps delivery, length of second stage of labor, and increasing birth weight.
04/18/23 F. Atashzadeh 22

Role of time since delivery
04/18/23 F. Atashzadeh 23
5 years after vaginal delivery
6.4%
18 years after vaginal delivery
10%
Clinical manifestations and diagnosis
Fecal and anal incontinence Medical history Occult anal sphincter laceration (endoanal
ultrasound) Physical examination (inspection of the
perianal area and vagina and a digital rectal examination)
04/18/23 F. Atashzadeh 24

Diagnostic procedures
endoanal ultrasound anorectal manometry pudendal nerve terminal latency
measurement defecography electromyography
04/18/23 F. Atashzadeh 25

Function: Anorectal manometry in fecal incontinence
04/18/23 26F. Atashzadeh
Electrophysiologic tests
EMG – needle electrodes into the superficial portion of the external sphincter or puborectalis muscle – myoelectric activity
Pudendal nerve terminal motor latency – measures the delay between the application of an electrical stimulus and external sphincter muscle response. Prolonged – pudendal neuropathy

Defecography
Videodefecography – barium thickened to the consistency of stool is introduced into the rectum.
Evacuation is monitored with flouroscopy Assessment of the anorectal angle at rest and
during defecation Excessive perineal descent, failure of the
puborectalis muscle to relax, rectocele and internal intususception

04/18/23 29F. Atashzadeh

04/18/23 30F. Atashzadeh
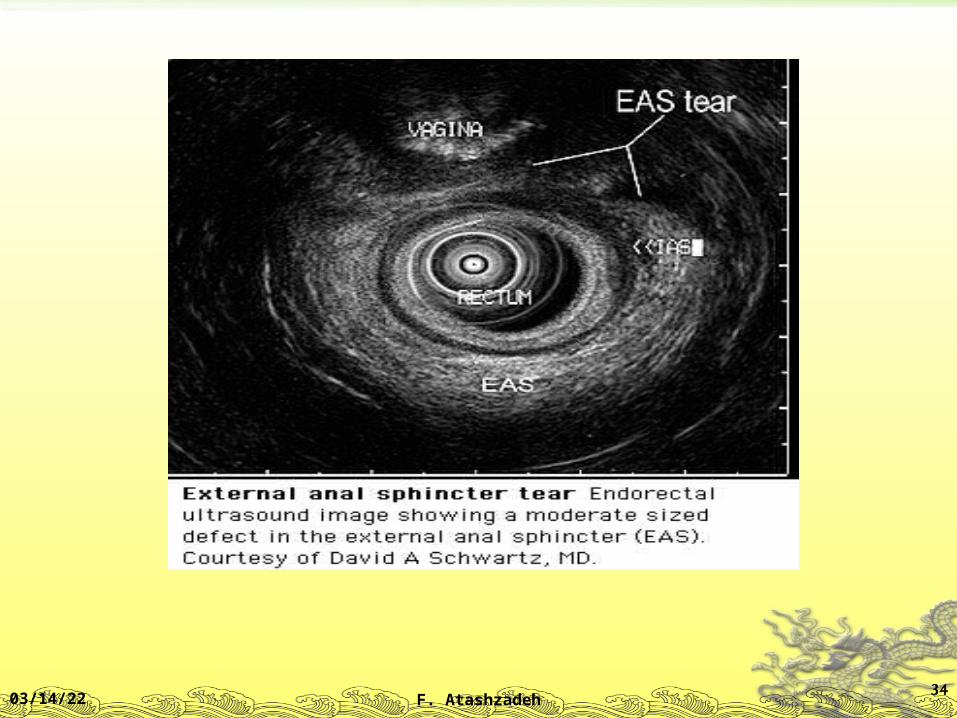
Anal Endosonography
An ultrasound probe is placed in the anal
canal or transvaginally to detect sphincter
injuries and to evaluate pelvic floor
structures.

Anatomy: Rectal Ultrasound
04/18/23 32F. Atashzadeh

04/18/23 33F. Atashzadeh
04/18/23 34F. Atashzadeh

Anatomy: Endoanal Coil MRI
04/18/23 35F. Atashzadeh

Treatment
Medical therapy Biofeedback Surgery
04/18/23 F. Atashzadeh 36

Treatment
Improving stool consistency
Increase intake of bulking agents – bran,
psyllium
Antidiarrheal agents – loperamide, lomotil,
cholestyramine
04/18/23 37F. Atashzadeh

Bowel management Fecal disimpaction
Scheduled toileting Glycerin suppositories daily, 30 min postprandial Attempt to defecate at the same time daily
Daily tap water enema
04/18/23 38F. Atashzadeh

Biofeedback
Biofeedback therapy inexpensive, quick and safe option
Success dependent on the expertise of the clinician and the motivation and the ability of the patient to understand and cooperate
Dementia, absent rectal sensation, inability to contract the external sphincter are the least likely to respond
04/18/23 39F. Atashzadeh

Biofeedback
70% restoring continence
90% reduction in incontinent episodes
Best outcome after anorectal surgery
Lowest success – spinal cored injury

04/18/23 41F. Atashzadeh

Is there a sound scientific basis
for the claim that having an
elective c-section protects the
pelvic floor?
04/18/23 F. Atashzadeh 42
Does perineal massage prevent
fecal incontinence?
04/18/23 F. Atashzadeh 43

What is the best mode of delivery
in women with a history of anal
sphincter laceration or fecal
incontinence ?
04/18/23 F. Atashzadeh 44
Will elective c-section prevent sexual
dissatisfaction during intercourse or uterine
prolapse?
04/18/23 F. Atashzadeh 45

Are there any circumstances when I might
wish to consider elective c-section?
04/18/23 F. Atashzadeh 46

04/18/23 F. Atashzadeh 47