7 lip pits; orthodontic treatment,dentition and … inheritance in most cases of lip pits described...
TRANSCRIPT

7.1 Lip Pits
7.1.1 Pits of the Lower Lip in Cleft Lip and/or Palate – Genetic Considerations
Pits of the lower lip such as fistulas of lower lip, para-median sinuses of lower lip, humps of lower lip, orlabial cysts are a very rare congenital malformation,first described by Demarquay in 1845 [1].
This minimally deforming anomaly is remarkablechiefly for its association with facial clefts. The factthat clefts that occur with lip pits seem to run strongerin families than clefts without lip pits has attracted theattention of professionals dealing with cleft patients(Figs. 7.1–7.5).
7.1.2 Frequency
No survey of lip pits has been carried out among thegeneral population; hence the frequency of this rareanomaly has been only roughly estimated from its in-cidence in hospital records.
Assuming that 70% [2] to 80% [3] of patients withpits of the lower lip have associated cleft lip and/orpalate, and that the frequency of clefts is 1:650 (one inevery 650 births), it can be estimated that the frequen-cy of lip pits among the general population is about1:75,000–1:100,000 (one in every 75,000 to 100,000births).
Lip Pits; Orthodontic Treatment, Dentition and Occlusion;Associated Skeletal Structures
Samuel Berkowitz
7
Fig. 7.1. Lower lip pits in a child with abilateral cleft lip and palate. a Before lip sur-gery. b After lip surgery at 6 months
ba

7.1.3 Morphology
Fistulas of the lower lip usually appear as two pits orhumps on the vermilion portion of the lower lip, gen-erally equidistant from the midline. Various kinds ofasymmetry may be observed with regard to the mid-line, or one pit may be positioned more orally. Somepits are mere depressions; others are channels10–15 mm deep with openings at the top of nipple-likeelevations. Some secrete small amounts of viscoussaliva but most are asymptomatic.
In exceptional cases, only one pit is present, whichmay be located either centrally or on one side or theother of the midline of the lower lip. Some cases ofsingle lip pit have occurred in families with memberswith double lower-lip pits. It can be assumed that asingle pit is not a distinct entity but rather an incom-plete expression of the trait. On the other hand, therarely described fistulas of the upper lip [4,5] have notshown any inheritance pattern.
202 S. Berkowitz
Fig. 7.2. a Pits in the upper and lower lips in a 20-year-old with a bilateral cleft lip and palate. b Close-up view
a b
Fig. 7.3. Lip pits in the upper and lower lips in a bilateral cleft lip and palate
Fig. 7.4. Radiograph of a premaxilla show-ing two central and one lateral incisors (left)and twined lateral incisors and one mal-formed central incisor (right)
Commissural or angular lip pits – small, usuallyasymmetrical channels located at the lip angles – arealso distinct entities with a much higher incidenceand different embryology [2, 6–10].
7.1.4 Association with Other Malformations
In addition to their strikingly common associationwith cleft lip and/or palate, pits of the lower lip havebeen noted in association with other malformations.Gorlin and Pindborg [2] have found cases of lip pitsalong with anomalies of extremities, popliteal ptery-gia, and anomalies of the genitourinary system. Theassociation with cleft lip and/or palate may well forma distinct new syndrome.
A review of the literature suggests that a variety ofother anomalies may be associated with lip pits.Among them: syndactyly of the hands together withcleft lip and palate [4, 11]; mental retardation andcleft, type not specified [12]; ankyloglossia and cleftlip and palate [3]; polythelia [14]; symblepharon andcleft lip and palate [15]; and ankyloblepharon, adhe-sion between the maxilla and mandible, and cleft uvu-la [16]. In two cases of the orofacial digital syndrome,pits were observed by [17].
Chapter 7 Lip Pits 203
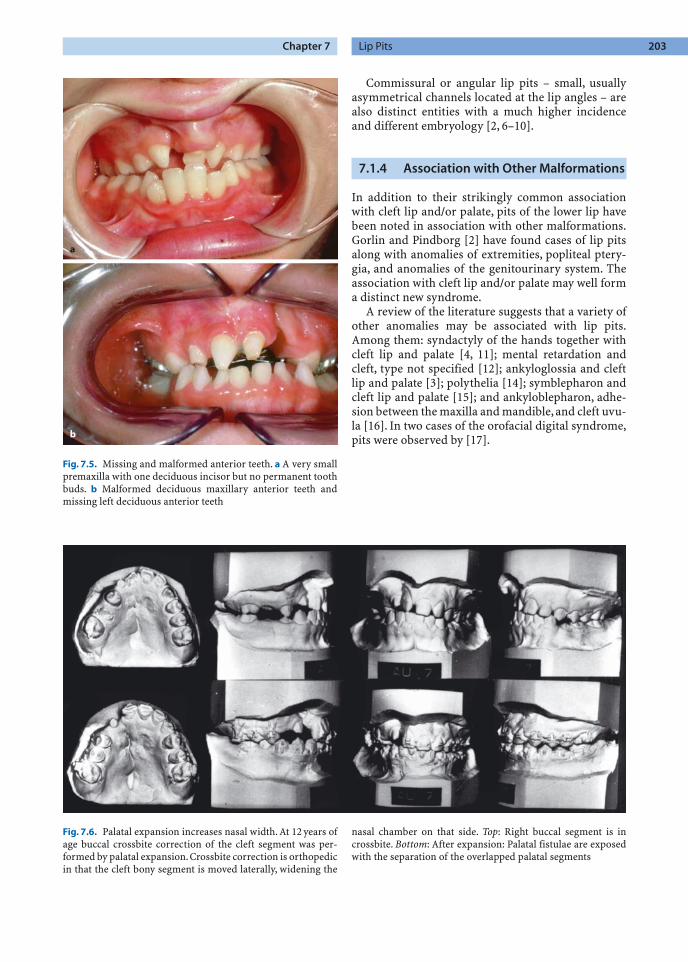
Fig. 7.5. Missing and malformed anterior teeth. a A very smallpremaxilla with one deciduous incisor but no permanent toothbuds. b Malformed deciduous maxillary anterior teeth andmissing left deciduous anterior teeth
a
b
Fig. 7.6. Palatal expansion increases nasal width. At 12 years ofage buccal crossbite correction of the cleft segment was per-formed by palatal expansion.Crossbite correction is orthopedicin that the cleft bony segment is moved laterally, widening the
nasal chamber on that side. Top: Right buccal segment is incrossbite. Bottom: After expansion: Palatal fistulae are exposedwith the separation of the overlapped palatal segments

7.1.5 Inheritance
In most cases of lip pits described during the last120 years, a marked hereditary pattern was observed.Although all authors have excluded autosomal reces-sive inheritance or X-linked inheritance, there is no uniform opinion concerning whether or not thecondition is due to a single autosomal dominantpleiotropic gene.
Fogh-Andersen [18, 19] was the first to clearlypoint out that the inheritance of clefts in the familieswith a history of lip pits is of a different character thanin families where no lip pits occur.According to Fogh-Anderson [18, 19] the role of genetic factors in fami-lies with lip pits is much more pronounced, and bothgenetically different types of clefts (cleft lip or cleft lipand palate and isolated cleft palates) commonly arefound within a single family. Fogh-Andersen also stat-ed that, in families in which fistulae of lower lip occuras a dominant hereditary character, there are somecases of cleft lip and cleft palate alone. Possibly it maybe explained as the result of coupling of neighboringgenes.
Van der Woude [3], in a careful study of five pedi-grees with clefts and lip pits, found that the combina-tion of pits and clefts is based on a single dominantgene of variable expressivity. She agreed with otherauthors [12] that a mildly affected individual can passthe trait on in a very severe form, and a severely affect-ed individual can pass the trait on in mild form. Thesex of the individual is not a factor in passing on thisanomaly. No sex limitation or preference exists.
Patients with clefts but without lip pits (or theirparents) often ask for genetic advice. In most of thesecases, only a small risk of cleft lip (less than 10%) isindicated for the next child. But the counseling situa-tion is significantly changed when associated lip pitsare found. In this instance, all clefts in the family areconsidered part of the syndrome, and risk figures forclefts are remarkably higher.
7.1.6 Evidence of Heterogeneity
It is also clear that the risk of a cleft occurring in achild is significantly higher when the parent has lippits and a cleft than when the parent has lip pits only.Two alternative explanations for this heterogeneitybetween families can be considered: (1) The develop-ment of clefts in persons carrying a “lip pit” majorgene may be influenced by modifying genes at otherloci; and (2) in some families, a mutant allele may pro-duce lip pits with only occasional clefts; whereas inother families a different mutant allele (at the same ora different locus) may frequently lead to clefts in addi-tion to lip pits. Thus far, efforts to use the data to sup-port one or the other of these hypotheses have beenunsuccessful. Cervenka et al. [20] reported data from66 individuals with lip pits in his study and 446 caseswith lip pits from the literature with known sex to es-tablishing a 1:1 sex ratio. The frequency of the syn-drome was estimated as 1:75,000 to 1:100,000 in thewhite population.
Cervenka [20] further states that family historiescan be explained adequately on the basis of autosomaldominant inheritance with variable expressivity ofthe trait. Penetrance is high, estimated at 80%. Pitsshow up more frequently than clefts, and there is a sig-nificant association between the types of clefts in par-ents and their children. Possibly the development ofclefts in this syndrome is influenced by modifyinggenes or by different mutant alleles with a predilec-tion for the different types of cleft.
7.2 Orthodontic Treatment,Dentition and Occlusion
7.2.1 Crossbite Correction (Figs. 7.7–7.12)
Bergland and Sidhu [21] advocated postponing or-thodontic treatment until complete eruption of thepermanent anterior teeth. Segmental alignment canthen be corrected with simultaneous manipulation ofthe anterior teeth. We believe it is best to start maxil-
204 S. Berkowitz
Fig. 7.7. a Fixed palatal helix expander usedin deciduous dentition with or without ananterior finger spring. b Fixed “Arnold” ex-pander using a compressed open coil springto create an expansion force
a b

Chapter 7 Lip Pits 205
Fig. 7.8 a–c. Crossbite correction for bilateral cleft lip. a Age 2 years 8 months. Note the bilateral crossbite. b Arnold expander inplace. c Crossbite correction after 3 months brought on by the outward movement of the lateral palatal segments
a b c
Fig. 7.9 a–h. Correction of anterior andposterior crossbite in the deciduous andmixed dentition in a severely scarred palate.a Complete unilateral cleft lip and palate,unoperated. b Palatal segments in contact.c Palatal cleft closed at 6 months of age: vonLangenbeck procedure was used to close avery wide cleft space. d Bilateral buccal andanterior crossbite. e Arnold expander is inplace. f Crossbite is still present due to exces-sive scar tissue. g Expander is fully extendedin the early mixed dentition. h Anteriorcrossbite was corrected, but the buccalcrossbite is still present. Comments: The severely scarred palate prevents the lateralmovement of the medially positionedpalatal segments. Scars can only be stretcheda slight amount, and if that amount is ex-ceeded the bony segments will not move andinstead the teeth will respond to the ortho-dontic forces.Should the teeth be tipped out-wardly they will have to be permanentlyretained by a bridge or by teeth splinting
a b
c d
e f
g h

206 S. Berkowitz
Fig. 7.11. a Orthodontic correction ofan anterior and posterior crossbite in thepermanent dentition. Anterior dentalcrossbite does not necessarily mean thatthe maxilla is anteroposteriorly deficientin size and requires a LeFort I advance-ment. In this case the maxillary dentitionwas advanced orthodontically with themissing lateral incisor space opened toachieve interarch congruency. The expan-sion was maintained by complete archsplinting. b A severely ventroflexed pre-maxilla was uprighted during the decidu-ous dentition. In order to maintain thecorrection after the deciduous anteriorteeth are lost a fixed palatal retainer withan acrylic button is placed on the premax-illa’s palatal incline
a
b
Fig. 7.10 a, b. Anterior and buccal crossbite correction themixed dentition. a Anterior crossbite was due to palatally dis-placed deciduous teeth with premaxillary segment and not togrowth deficiency. The buccal teeth are in crossbite as a result ofthe lesser palated segment being palatally displaced. This picture has the maxillary anterior teeth in crossbite; the loweranterior teeth are shown while the upper teeth are hidden.
b A fixed palatal expander with finger springs is used to expandthe arch and advance the anterior teeth. In most instances it isunnecessary to disocclude the anterior teeth to move them for-ward. Buccal expansion depends on the ability of the lesserbony segment to move outward. Retention of the bony correc-tion is essential
a b

lary arch expansion when the deciduous dentition iscompletely erupted and when the children can be eas-ily managed. A three-phase treatment is followed: (1)Buccal crossbite is corrected at 4–6 years; (2) anteriorteeth are aligned at 8–9 years; and (3) final orthodon-tics is utilized at 11-plus years.
Crossbite correction by moving palatal segmentslaterally in the presence of extensive palatal scarringis difficult and often unsuccessful. Extensive mucope-riosteal undermining, leaving wide denuded palatalbone, was necessary to close the wide palatal cleft at6 months of age. Uniting the lip moved the palatal seg-ments together (molding action) into good arch ap-proximation. Palatal scar contracture moved the buc-cal segments farther medially, placing the buccal teethin crossbite. The anterior dental crossbite does notnecessarily reflect diminished anteroposterior maxil-lary growth but, rather, malposition of the premaxil-lary teeth of the greater segment.
7.2.1.1 Unilateral Cleft Lip and Palate
Deciduous and Mixed Dentition. When the smallersegment’s alveolar process is contained within thepremaxillary alveolar segment of the larger segment,a dental crossbite occurs between the maxillary andmandibular teeth. Dental dysplasia (eruption of atooth out of position) may or may not coexist withsegmental dislocation.A simple crossbite of one tooth
may be due to its malposition rather than to thepalatal segment’s collapse. The most frequent cross-bite is brought on by the mesioangular rotation of thelesser segment rather than by ectopic tooth eruption.Total buccal crossbite is seen less frequently but isgenerally present when the palatal tissue is scarred. Ineither case, the same helix type of palatal expandercan be utilized and correction achieved within 2 to4 months. Anterior movement of the deciduous cen-tral incisors often requires lingual undercuts either byorthodontic bands with lugs or by direct lingual shelfbonding to stabilize the anterior activated palatal fin-ger springs.
A fixed palatal retainer can hold the correction un-til the second stage of orthodontic therapy is initiated.There is no way to predict the return of a crossbite inthe absence of permanent retention. Bone graftingacross the alveolar cleft does not guarantee retentionof the corrected arch form.
Permanent Dentition. In Class I and Class III casesit is usually preferable to open the missing lateral in-cisor space with the expectation of utilizing a fixedbridge to stabilize the corrected arch form and replacethe missing tooth. In Class II cases it may be possibleto encourage the cuspid to erupt through the alveolarbone graft in the lateral incisor space, which elimi-nates the need for extensive orthodontics and bridge-work. The cuspid may need to be splinted to the cen-tral incisor in order to maintain the corrected archform.
Chapter 7 Lip Pits 207
Fig. 7.12 a, b. Repaired bilateral cleft lip and palate. An anteri-or openbite and retruded premaxilla resulting from inadequateorthodontic and surgical planning. a A slight anterior openbitewas present at 8 years of age at which time a secondary alveolarbone graft was performed. The orthodontist attempted to closethe lateral incisor spaces by bringing the cuspids mesially, whileretracting the central incisors. This created a more severe open-bite and an anterior crossbite. b The orthodontic mechanicswere reversed. The lateral incisor spaces were opened and the
central incisors were advanced into an ideal overbite and over-jet relationship. One of the bone grafts had to be redone. Com-ments: When the buccal occlusion is class I it is always better tokeep the lateral incisor space open in both bilateral and unilat-eral cleft cases. There are occasions when a mandibular centralincisor will need to be extracted in order to avoid flaring themaxillary central incisors and to obtain a proper occlusion. Ananterior fixed bridge will stabilize the arch and replace themissing maxillary lateral incisors
a b

7.2.1.2 Bilateral Cleft Lip and Palate
First Stage. Between the ages of 4 to 6 years, the pre-maxilla is usually ventroflexed and overlaps one orboth lateral palatal segments, which may be in partialor complete buccal crossbite. As in unilateral cases,treatment of bilateral cleft lip/palate necessitatesmoving bony segments into the surrounding musclering. If the premaxilla is to be moved forward, bandswith lingual lugs are placed on the deciduous centralincisors. A fixed helix-type palatal expander with an-terior-activated finger springs is cemented to the sec-ond deciduous molars. The finger springs are posi-tioned under the central incisor-banded lugs forretention. The premaxilla is uprighted prior to cor-recting the buccal crossbite. The anterior and buccalcrossbite correction can be completed within6 months. As the premaxilla and lateral palatal seg-ments are moved outward, the anterior cleft space isuncovered. A fixed palatal retainer with an acrylic an-terior extension to cover the anterior cleft space isplaced and kept in position until the alveolar cleft isbone-grafted and all fistulas are surgically closed. Per-manent complete palatal retention is necessary, evenafter alveolar bone grafting. A premaxillary retainermust be placed when the deciduous anterior teeth arelost.
Second Stage. At 7–8 years of age, when the decidu-ous incisor teeth are replaced by permanent incisors,the anterior crossbite may have to be retreated. Theincisors may be rotated and malpositioned. Ortho-dontic brackets are placed in the upper arch to sup-port a labile arch wire, which will be utilized to repo-sition the incisor teeth and reduce the premaxillaryoverbite. A pontic tooth with band is placed on thearch wire to achieve a more pleasing aesthetic result.The premaxilla needs to be properly aligned with thelateral palatal segments prior to alveolar bone graft-ing; this procedure may be performed between 7 and9 years of age. A lateral incisor as well as a cuspid mayerupt through the area of new bone formation.
Third Stage. Children at 10+ years of age are treat-ed as any other child. The many malocclusion possi-bilities render it impossible to develop treatmentplans for each contingency; instead, basic treatmentproblems are discussed.1. Class I malocclusion (with anterior and/or buccal
crossbite): The crossbite generally is due to lingualbony displacement. The upper arch should be ad-vanced and expanded. If there is sufficient archlength, the missing lateral incisor area is left open.In arch shortage cases, it may be preferable to movethe cuspid adjoining the space into the lateral inci-sor area, rather than extract the first bicuspid onthat side.A number of variations of treatment existaccording to tooth size and location.
2. Class II malocclusion: The anterior overjet may becorrected by retraction of the premaxillary centralincisors in bilateral cleft lip and/or cleft palate cas-es. If one or both lateral incisors are missing, it maybe best to place the adjoining cuspid in that spaceand extract either the opposite lateral incisor or thefirst bicuspid.
3. Class III malocclusion: An anterior crossbite doesnot necessarily signify that a Class III malocclusionexists. In some cases the anterior teeth can be ad-vanced without excessively increasing their axialinclination. A true depressed midface with poorvertical and anteroposterior development requiresmidfacial lengthening and advancement. Segmen-tal surgery may have to be utilized to overcomepalatal width problems caused by excessive scar-ring.
7.2.1.3 Use of Orthopedic Forces to Correct Midfacial Recession
Developing anterior crossbites in either mixed or per-manent dentition can be corrected using orthopedicprotraction forces. These forces must average 800 gmper side and pull downward and forward off hooksplaced between the lateral incisor and cuspid. Theforce needs to be applied 12 h per day. With good co-operation, 5–10 mm of midfacial advancement can beaccomplished. The preferred facial mask is the Delairetype.
7.2.2 Supernumerary (Extra) Teeth,Missing Teeth, and Aplasia (Malformed Teeth)
This occurs more frequently in children with cleft lipand/or palate than in other figuration of the nasalfloor. (Figs. 7.5, 7.6, 7.13, 7.14). Bishara and coworkers[22] studied untreated adults in India who had cleftsof the lip and alveolus only, unilateral cleft lip andpalate, and bilateral cleft lip and palate. They observedthat the maxilla and cranial base were not differentfrom a matched normal population, but that the rela-tion of the maxilla and mandible to the cranial basevaried according to cleft type. Moss [23, 24] Blaine[25], Dahl [26], and Krogman et al. [27] have statedthat the cranial base in cleft palate patients differed inboth size and shape from noncleft individuals.
The incidence reported in different articles hasvaried because it is difficult to distinguish betweenvariations rooted in congenital causes and those relat-ed to surgery [30]. Recently, it has been observed thatsupernumerary teeth are more common in the decid-uous dentition. Moreover, the incidence of supernu-
208 S. Berkowitz

merary teeth is greatest in cases of cleft lip only anddecreases as the extent of the cleft increases. The rela-tionship is the opposite in cases of aplasia; the inci-dence of aplasia is lowest for cleft lip only and cleftpalate only and increases in proportion to the extentor complexity of the cleft [31–35].
In conditions of facial clefting, dental developmentis, except for the third molars, delayed for all teeth,both maxillary and mandibular [31, 32]. Asymmetri-cal development of tooth pairs, with delayed develop-ment on the cleft side, was recorded in approximatelyhalf of a group of children with congenital lip and/or palate clefts [33]. This supports other observa-tions that eruption is delayed in both dentitions[35–54].
Zilberman [55], from a study on clefts of the lip andalveolar structures, and Mirsa and colleagues [56], af-ter investigating clefts of the lip and palate, reportedthat unilateral clefts are more frequent on the left sideand are more common in males than in females.
The incidence of dental malocclusion reported inpatients with cleft lip and/or palate varied widely instudies by Huddart and Bodenham [57], Hellquist etal. [58], Dahl et al. [59], Norden and associates [60],Bergland and Sidhu [21], Nylen and coworkers [61],Ranta and colleagues [62], and Hellquist and Skoog[63]. This may be because the patients had varyingtypes of clefts and their cases were recorded at differ-ent ages. Rehrman and coauthors [64] found the inci-dence of malocclusion in the mixed dentition to betwice that in the deciduous dentition.
In cases of cleft palate only, Ranta and colleagues[65] found only a slight increase in anterior crossbiteat the transition from the deciduous to the mixed den-tition. A noticeable increase in the incidence of ante-rior crossbite in the mixed dentition, in cases of com-plete unilateral clefts of the lip and/or palate, wasreported by Bergland and Sidhu [21]. This was irre-spective of the arch configuration in the deciduousdentition. They also reported that palatal segmentsstabilized early after lip repair and that further col-lapse was the exception. However, contrary to thefindings just cited,Nylen and coworkers [61] found noincrease in the frequency of anterior crossbite in theirmixed-dentition group.
7.2.3 Caries
Dahl et al. [66] reported the incidence of caries, gin-givitis,and dental abnormalities in preschool childrenwith cleft lip and/or palate in Stockholm, Sweden.Oral health was studied in 49 children 5–6 years oldwith clefts of the lip and/or palate (CL/P) and 49healthy children matched for sex and age. The resultsshowed a statistically significant increase in theprevalence and activity of caries among the CL/P chil-dren. The average number of decayed and filled toothsurfaces in the cleft group was 7.0 compared with 3.9in the control group (p <0.05).
The most evident difference between the twogroups was found in the number of decayed proximalsurfaces. The mean number of decayed proximal sur-faces in the CL/P group was 2.5, compared with 0.9 inthe control group (p <0.001). No significant differ-ences were found in the prevalence and activity ofcaries among children with isolated clefts of the lip orpalate.
The children with cleft lips/palates also exhibited asignificant increase (p >0.01) in the number of gingi-val units with gingivitis. Other dental abnormalities
Chapter 7 Lip Pits 209
Fig. 7.13. The left central and lateral incisor in the line of analveolar cleft areas reduced in size
Fig. 7.14. Tooth abnormalities. Coalescence of the right decid-uous central and lateral incisors in a right unilateral cleft of thelip and alveolus

included increased enamel hypomineralization(p <0.05), supernumerary teeth (p <0.001), unilateralcrossbite (p <0.001), and mesial terminal plane(p <0.01). These results clearly show that childrenwith CL/P as a group must be considered to have anincreased risk of caries and gum disease, and shouldtherefore have the benefit of additional preventiveprograms. (see Chap. 4, Facial and Palatal Growth)
7.3 The Relationship Between the Clefting Process and Contiguous Skeletal Structures
Some studies have indicated that clefting is not an iso-lated defect but may be a syndrome phenomenonwith ramifications in contiguous and often remotestructures.
In a study of Danish males, Dahl [26] suggestedthat the presence of cleft palate, with or without cleftlip, may have ramifications for distant craniofacialstructures and their development. Farkas and Lindsay[67] identified consistent variations in facial mor-phology in the cleft population and concluded thatthe cleft defect was not an isolated condition. They re-ported that what might otherwise be considered thenormal side of the face in cases of unilateral clefts wasnot completely normal, and that the anomaly influ-enced the development of the face equally on bothsides.
7.3.1 The Position of the Cleft Maxilla Within the Cranium and the Mandible
Berkowitz [68] undertook a mixed cross-sectionalstudy of CUCLP and CBCLP cases to determinewhether the maxillary complex relative to themandible is posteriorly positioned within the face bystudying the dental occlusion. None of the cases hadpresurgical orthopedics, and the hard palate cleftswere closed between 18 and 28 months of age using amodified von Langenbeck procedure with a vomerflap. This study was designed to test McNeil’s thesisthat the palatal segments, being detached from thenasal septum, are not only reduced in mass but alsohave not been brought forward with the developingnasal septum. This failure would lead to retrusivemidface with a Class III malocclusion.
Berkowitz [68] found that the occlusal relation-ships at 6 years of age did show Class I and Class II oc-clusions, but none of the cases had a Class III occlu-sion, which would have been present if McNeil’s [69,
70] hypothesis had been valid. Of the 29 bilateral cas-es, 5 cases had a crossbite on one side, 1 case had acomplete bilateral crossbite, and 6 cases had no cross-bites at all. It is quite evident that a buccal crossbite isnot, as stated by McNeil, a predictable outcome of thepresence of a palatal cleft.
Semb’s [71, 72] and Ross’s [73, 74] studies and thosealready acknowledged elsewhere established that inthe cleft population both the maxilla and mandibleare retropositioned within the face (see Chap. 9).However, if McNeil’s beliefs were accurate, the bilater-al cleft palatal segments would have been left behindin their growth, and a greater proportion of the caseswould have shown a Class III malocclusion on one orboth sides.
Chierici and associates [75] and Bishara [22, 76]found a relative retrusion of the maxilla and mandibleas well as increased steepness of the mandibular planein various cleft types. Krogman and his colleagues[27] reported significant differences in the cleft popu-lation in the size of the cranial base, its configuration,and direction of growth. They concluded that theclefting process has growth and/or development im-plications for the contiguous cranial base and facialstructures as well as for the maxilla.
Bishara [76] reported that the posterior position-ing of the maxilla and mandible relative to the anteri-or cranial base may result from the cleft’s influence on contiguous skeletal structures, and that clefting affects maxillary development and facial morphology.
7.3.2 The Cranial Base
Hayashi and colleagues [77] investigated cranialgrowth of a large sample of subjects from 4 to 18 yearsof age with complete unilateral clefts. The investiga-tors found that the cranial base angle was flatter, themaxilla was more retruded, and underdevelopment inboth the maxilla and the mandible was more pro-nounced in girls than in boys. They speculated thatupper face height in patients of both genders was lessthan normal as a result of cleft interference with nasalseptal and maxillary suture growth and changes in theconfiguration of the nasal floor. Bishara and cowork-ers [70] studied untreated adults in India who hadclefts of the lip and alveolus only, unilateral cleft lipand palate, and bilateral cleft lip and palate. They ob-served that the maxilla and cranial base were not dif-ferent from a matched normal population, but that therelation of the maxilla and mandible to the cranialbase varied according to cleft type.
210 S. Berkowitz

7.3.3 Relationship of the Nasal Cavity to Arch Form (Figs. 7.15, 7.16)
Aduss and Pruzansky [28] wrote that the anatomicdistortions common to all of their patients with cleftsincluded marked deviation of the nasal septum to-ward the noncleft side; flattening, particularly of theinferior turbinate on the cleft side; and an anterolater-
al displacement of the noncleft segment, with an out-ward and lateral rotation of the premaxillary area ad-joining the cleft.
These distortions are the result of unbridled septalgrowth, deviant maxillary growth, and aberrant vec-tors of muscle pull. Establishing a continuous muscleband across the cleft, by lip repair, can bring thepalatal shelves closer together and modify the config-
Chapter 7 Lip Pits 211
Fig. 7.15. a Frontal View. The septum is straight dividing the nasal chamber in two equal parts. b Lateral View. The componentswhich make up the nasal septum: the ethmoid bone. The nasal cartilage and the vomer
a b
Fig. 7.16. Serial frontal cephalometric radi-ographs illustrating geometric changes tothe nasal chamber in a CUCLP from birth to4 years of age before and after palatal expan-sion. Top: 0-2-8 At birth a widened nasalchamber is evident. 0-5-22 After lip surgerythe nasal chamber has narrowed. Bottom: 1-8-3 The inferior turbinate on the cleft side(R) makes contact with the vomer. 4-2-12 Af-ter palatal expansion the nasal width and theseptum to inferior turbinate distance has in-creased. Because the roof of the mouth isalso the floor of the nose, any disarrange-ment in the architecture of the roof of themouth is reflected in the nasal chamber.Prior to lip repair, the nasal septum is dis-placed to the noncleft side. After lip repairwith the medial movement of the cleft seg-ment, the septum bows toward the nasalchamber on the cleft side.After palate repairthere is continual palatal movement withseptal uprighting and decreased septal bow-ing. The turbinates on the cleft side are flat-ter, and the buccal teeth on the cleft side maybe in crossbite. The nasal chamber on thatside is narrowed. (Reprinted from [78])

uration of the palatal segments, as well as the config-uration of the internal nares.
Peyton and Ritchie [29], measuring the displace-ment of the soft tissues of the nose in complete unilat-eral cleft lip and palate, have shown that deviation ofthe external part of the nose toward the noncleft sideextends for the entire length of the nose, with thegreatest displacement at the tip. They further demon-strated that growth of the nasal structures is the samein noncleft children and children with complete uni-lateral cleft and that the early cleft deformity decreas-es with time. The natural tendency for self-correctionof the septal deviation was evident in the continualuprighting and medial movement of the end of theseptum observed in all cases.
References
1. Demarquay JN. Quelques considerations sur le bec-de-lievre. Gax Med Paris 1845; 13:52–53.
2. Gorlin RJ, Pindborg JJ. Syndromes of the head and neck.New York: McGraw-Hill; 1964. p. 117–125.
3. Van der Woude A. Fistula labii inferioris congenita and itsassociation with cleft lip and palate. Am J Hum Genet 1954;6:244–256.
4. Lannelongue O. Observation de division transversale con-genitale de la levre inferieure. Bull Mem Soc Chir Paris1879; 5:642.
5. Radcliff W. Rare congenital malformations of the upper lip.Brit J Surg 1940; 28:329–330.
6. Lemke G. Über Fisteln der Lippen inschliesslich der Mund-winkel. Derm Wchnschr 1959; 140:1085–1098.
7. Everett FG, Wescott WB. Commissural lip pits. Oral Surg1961; 14:202–209.
8. Witkop CJ. (ed.) Genetics and dental health. New York: Mc-Graw-Hill, 1964. p. 44.
9. Witkop CJ Jr, Barros I. Oral and genetic studies of Chileans1960. I. Oral anomalies. Am J Phys Anthropol 1963;21:15–24.
10. Schuermann H, Greither A, Hornstein O. Krankheiten derMündschleimhaut und der Lippen. Müchen: Urban &Schwarzenberg; 1966:23–25.
11. Bernauds. Discussion. Bull Soc Chir Gaz Hop 1861. Cited byStieda 1906;174.
12. Test AR, Falls HF. Dominant inheritance of cleft lip andpalate in five generations. J Oral Surg 1947; 5:292–297.
13. Sorricelli DA, Bell I, Alexander WA. Congenital fistulas ofthe lower lip. Oral Surg 1966; 21:511–516.
14. Baxter II. Congenital fistulas of the lower lip. Am J OrthodOral Surg 1939; 25:1002–1007.
15. Oberst. Über die angeborenen Unterlippenfisteln. Beitragez klin Chir 1910; 68:795–801.
16. Neuman Z, Shulman J. Congenital sinuses of the lower lip.Oral Surg 1961; 14;1415–1420.
17. Gorlin RJ, Psaume J. Orodigitofacial dysostosis: a new syn-drome. A study of 22 cases. J Pediat 1962; 61:520–530.
18. Fogh-Andersen P. Inheritance patterns for cleft lip andpalate. In: Pruzansky S (ed.) Congenital anomalies of theface and associated structures. Springfield, IL: CC Thomas;1961. p. 123–133.
19. Fogh-Andersen P. Inheritance of harelip and cleft palate.Nyt Copenhagen: Nordisk Forlag, Arnold Busck; 1942.
20. Cervenka J, Gorlin RJ, Anderson VE. The syndrome of pitsof the lower lip and cleft lip and or palate, genetic consider-ations. Am J Hum Gen 1967; 19:416–430.
21. Bergland O, Sidhu SS. Occlusal changes from the deciduousto the early mixed dentition in unilateral complete clefts.Cleft Palate J 1974; 11:317–326.
22. Bishara SE, de Arrendondo RSM, Vales HP, Jakobsen JR.Dentofacial relationships in persons with unoperatedclefts: comparisons between three cleft types. Am J Orthod1985; 88:481–507.
23. Moss ML. The primary role of functional matrices in facialgrowth. Am J Orthod 1969; 55:566.
24. Moss ML, Bromberg BE, Song IC, Eisenmann G. The passiverole of nasal septal cartilage in midfacial growth. Plast Re-constr Surg 1968; 41:536–542.
25. Blaine HL. Differential analysis of cleft palate anomalies.J Dent Res 1969; 48:1042–1048.
26. Dahl E. Craniofacial morphology in congenital clefts of thelip and palate – An x-ray cephalometric study of youngadult males. Acta Odontol Scand 1970; 28(Suppl.):57.
27. Krogman WM, Mazaheri M, Harding RL, et al. A longitudi-nal study of the craniofacial growth pattern in childrenwith clefts as compared to normal birth to six years. CleftPalate J 1975; 12:59–84.
28. Aduss H, Pruzansky S. The nasal cavity in complete unilat-eral cleft lip and palate. Arch Otolaryngol 1967; 85:53–61.
29. Peyton WT, Ritchie HP. Quantitative studies on congenitalclefts of the lip. Arch Surg 1936; 33:1046–1053.
30. Bohn A. Dental anomalies in hare lip and cleft palate. ActaOdontol Scand 1963; 21(Suppl.):38.
31. Brook AH. A unifying aetiological explanation for anom-alies of human tooth number and size. Arch Oral Biol 1984;29:373–378.
32. Garn SM, Lewis AB, Polacheck DL. Variability of tooth for-mation. J Dent Res 1959; 38:135–148.
33. Brabant H. Comparison of the characteristics and anom-alies of the deciduous and permanent dentition. J Dent Res1967; 46:897–902.
34. Garn SM, Lewis AB, Blizzard RM. Endocrine factors in den-tal development. J Dent Res 1965; 44(Suppl. to No. 1):243–258.
35. Garn SM, Lewis AB, Polacheck DL. Interrelations in dentaldevelopment. I. Interrelationships within the dentition. JDent Res 1960; 39:1049–1055.
36. Garn SM, Burdi AR, Nagy JM. Distance gradient in prenataldental development. J Dent Res I 1971; 40:785.
37. Ranta R. The development of the permanent teeth in chil-dren with complete cleft and palate. Proc Finn Den Soc1972; 68(Suppl. 3).
38. Ranta R. Asymmetric tooth formation in a permanent den-tition of cleft-affected children: an orthopantomographicstudy. Scand J Plast Reconstr Surg 1973; 7:59–63.
39. Ranta R. Development of asymmetric tooth pairs in thepermanent dentition of cleft-affected children. Proc FinnDent Soc 1973; 69:71–75.
40. Garn SM, Cole PE, Wainright RL. Dimensional communali-ties of the deciduous teeth. J Dent Res 1977; 56:1208.
41. Ranta R. Eruption of the premolars and canines and factorsaffecting it in unilateral cleft lip and palate cases: an or-thopantomographic study. Suom Hammaslaak Toim 1971;67:350–355.
212 S. Berkowitz

42. Fanning EA. A longitudinal study of tooth formation androot resorption. NZ Dent J 1961; 57:202–217.
43. Garn SM, Cole PE, Wainright RL. Dimensional correspon-dences between deciduous and permanent teeth. J Dent Res1977; 56:1214.
44. Dixon DA. Defects of structure and formation of teeth inpersons with cleft palate and the effect of reparative sur-gery on the dental tissues. Oral Surg 1968; 25:435–446.
45. Falkner F. Deciduous tooth eruption. Arch Dis Child 1957;32:386–391.
46. Delgado H, Habicht J-P, Yarbrough C, Lechtig A, MartorellR, Malina RM, Klein RE. Nutritional status and the timingof deciduous tooth eruption. Am J Clin Nutr 1975;28:216–224.
47. Demirjian A. Dentition. In: Falkner F, Tanner JM (eds.) Hu-man Growth – a comprehensive treatise.Vol. 2, 2nd ed. NewYork: Plenum Press; 1986. p. 269–298.
48. Fishman LS. Factors related to tooth number, eruptiontime, and tooth position in cleft palate individuals. J DentChild 1970; 37:31–34.
49. Foster TD, Lavelle CLB. The size of the dentition in com-plete cleft lip and palate. Cleft Palate J 1971; 8:177–184.
50. Galili G, Rosenzweig KA, Klein H. Eruption of primaryteeth and general pathologic conditions. J Dent Child 1969;36:51–54.
51. Haring FN. Dental development in cleft and non-cleft sub-jects. Angle Orthod 1976; 46:47–50.
52. Hatton ME. A measure of the effects of heredity and envi-ronment on eruption on the deciduous teeth. J Dent Res1955; 34:397–401.
53. Haavikko K. Development of the dentition. In: Thilander B,Ronning O (eds.) Introduction to ort#hodontics. 5th ed.Stockholm: Tandlakarforetaget; 1985. p. 45–62.
54. Haataja J, Rintala A, Ranta R. On asymmetric developmentof the first and second permanent molars in children withcraniofacial anomalies. An orthopantomographic study.Proc Finn Dent Soc 1972; 68:15–19.
55. Zilberman Y. Observations on the dentition and face inclefts of the alveolar process.Cleft Palate J 1973; 10:230–238.
56. Mirsa FM, Ray RK, Kapoor DN. Dental abnormalities incases of cleft lip and palate. J Indiana Dent Assoc 1972;44:1–9.
57. Huddart AG, Bodenham RS. The evaluation of arch formand occlusion in unilateral cleft palate subjects. Cleft PalateJ 1972; 9:194–209.
58. Hellquist R, Linder-Aronson S, Norling M, Ponten B, Sten-berg T. Dental abnormalities in patients with alveolar clefts,operated upon with or without primary periosteoplasty.Eur J Orthod 1979; 1:169–180.
59. Dahl E, Hanusardottir B, Bergland O. A comparison ofocclusions in two groups of children whose clefts wererepaired by three different surgical procedures. Cleft PalateJ 1981; 18:122–127.
60. Norden E,Aronson SL, Stenberg T. The deciduous dentitionafter only primary surgical operations for clefts of the lip,jaw and palate. Am J Orthod 1973; 63:229–236.
61. Nylen B, Korlor B, Arnander C, Leandersson R, Barr B,Nordin KK. Primary, early bone grafting in complete cleftsof the lip and palate. Scand J Plast Reconstr Surg 1974;8:79–87.
62. Ranta R, Oikari T, Haataja J. Prevalence of crossbite in de-ciduous and mixed dentition in Finnish children with oper-ated cleft palate. Proc Finn Dent Soc 1974; 70:20–24.
63. Hellquist R, Skoog T. The influence of primary periosteo-plasty on maxillary growth and deciduous occlusion in cas-es of complete unilateral cleft lip and palate: a longitudinalstudy from infancy to the age of 5 yrs. Scand J Plast Recon-str Surg 1976; 10:197–208.
64. Rehrman A, Koberg W, Koch H. Die Auswirkungen derOsteoplastik auf das Wachstum des Oberkiefers-Erhebun-gen der Ergebnisse mit Hilfe der Elektronischen Datenver-arbeitung Fortschr, Kiefer Gesichtschir 1973; 16/17:102–108.
65. Ranta R, Oikari T, Rintala A, Haataja J. Effect of the pe-riosteal flap technique on cleft width and the formation ofalveolar ridge in relation to the bite level in surgery for cleftlip and palate. Scand J Plast Reconstr Surg 1974; 8:62–66.
66. Dahl G, Ussisoo-Joandi R, Ideberg M, Modeer T. Caries, gin-givitis, and dental abnormalities in preschool children withcleft lip and/or palate. Cleft Palate J 1989; 26:238–238.
67. Farkas LG, Lindsay WK. Morphology of adult face after re-pair of isolated cleft palate in childhood. Cleft Palate J 1972;9:132–142.
68. Berkowitz S. Timing cleft palate closure – age should not bethe sole determinant. J Craniofac Gen and Devel Biol 1985;1(Suppl.):69–83.
69. McNeil CK. Orthodontic procedures in the treatment ofcongenital cleft palate. Dent Rec 1950; 70:126–132.
70. McNeil CK. Oral and facial deformity. London: Sir Isaac Pit-man and Sons; 1954.
71. Semb G. A study of facial growth in patients with unilateralcleft lip and palate treated by the Oslo CLP team. CleftPalate Craniofac J 1991: 28:1–47.
72. Semb G. A study of facial growth in patients with bilateralcleft lip and palate treated by the Oslo team. Cleft PalateCraniofac J 1991; 28:22–39.
73. Ross RB. Treatment variables affecting facial growth incomplete unilateral cleft lip and palate. Parts I, V, VII. CleftPalate J 1987; 24:5.
74. Ross RB. Treatment variables affecting facial growth incomplete unilateral cleft lip and palate. Part VII: Anoverview of treatment and facial growth. Cleft Palate J 1987;24:71–77.
75. Chierice G, Harvold EP,Vargevik K. Morphogenetic experi-ments in cleft palate: Mandibular response. Cleft Palate J1973; 10:51–61.
76. Bishara SE, Iversen WW. Cephalometric comparisons onthe cranial base and face in persons with isolated clefts ofthe palate. Cleft Palate J 1974; 11:162–175.
77. Hayashi Il, Sakuda M, Takimoto K, Miyazaki T. Craniofacialgrowth in complete unilateral cleft lip and palate: a roent-gencephalometric study. Cleft Palate J 1976; 13:215–237.
78. Aduss H, Pruzansky S. Nasal cavity in complete unilateralcleft lip and palate. Arch Otolaryngol 1967; 85:53–58
Chapter 7 Lip Pits 213