8th annual ntd conference · dr. stephen munga . director, cghr –kemri . 8 . message from the...
TRANSCRIPT

1
“NTDs: Successes, Challenges and Opportunities –From the Bench to the Field”
8TH ANNUAL NTD CONFERENCE 10-11 DEC, 2014 SOVEREIGN HOTEL –KISUMU
PROGRAM AND ABSTRACT BOOK

2
ACKNOWLEDGEMENTS
KASH Organizing Committee Dr. Pauline NM Mwinzi, Chair
Dr. Doris Njomo, Co-Chair
KASH Secretariat and Logistics Ms. Rosemary Musuva
Ms. Emmy Kavere Mrs. Apollonia Ayoo
NTD Scientific Sub-Committee
Dr. Maurice Odiere –Chair Mr. Erick Ndombi Mr. Martin Omedo
Ms. Elizabeth Ochola
Editorial
Dr. Pauline Mwinzi Dr. Maurice Odiere
Mr. Winston Mbanda Dr. Stephen Munga
Copyright © Kenya Medical Research Institute, 2014 The Kenya Medical Research Institute
P. O. Box 54840-00200 Nairobi, Kenya
ICT and Communications Mr. John Riaga
www.kemri.org

3
THE ORGANIZERS OF THE 8TH KEMRI NTD CONFERENCE
WOULD LIKE TO THANK OUR SPONSORS
4
5
6
MESSAGE FROM DIRECTOR, KEMRI
Recent years have witnessed increased global
momentum towards control and elimination of the so called Neglected Tropical Diseases (NTDs) –These are a group of infectious diseases which have shared a pandemic neglect in past decades, and affect mostly the poorest of poor communities mainly in developing countries. Children bear the brunt of NTDs leading to stigma, increased absenteeism and drop-out rates from school and affected adults suffer reduced economic activity due to poor health leading to a vicious cycle of poverty. f
The NTDs of priority in Africa include Lymphatic Filariasis (elephantiasis), Soil-Transmitted Helminthiasis
(STH), Schistosomiasis (bilharzia), Trachoma, Leishmaniasis (kala azar), Hydatidosis, Tungiasis (Jiggers), Buruli ulcer, Onchocerciasis (river blindness), and Guinea worm disease among others. They are the most common conditions affecting the poorest 500 million people living in sub-Saharan Africa (SSA), and together produce a burden of disease that may be equivalent to up to one-half of SSA's malaria disease burden and more than double that is caused by tuberculosis. NTDs can be eliminated using safe diagnostic tools, drugs, provision of safe water and sanitation facilities, health education among other intervention strategies.
KEMRI has over the years actively carried out research on infectious diseases which are now part of the WHO list of neglected tropical diseases targeted for elimination, and we’re happy to participate in this global urgent call to finally control and eliminate these scourges. In an effort to foster partnerships and collaborations in controlling and eventually eliminating the NTDs, KEMRI established the NTD conference as a forum that brings together NTD researchers, graduate students, policy makers, implementers, community members, patients as well as the private sector to share data, ideas, review progress made and to discuss research gaps and the way forward.
NTD control research in Africa and in Kenya has come a long way and grown tremendously over the years, contributing significantly to progress in NTD control in the region. To celebrate this journey, we will be honoring two most distinguished researchers who have and continue to be part of this journey; Prof. Simon Brooker of LSTMH, and Prof. Jefitha Karimurio of UoN, with a Distinguished NTD Researcher Award. Please join me in congratulating the two for this achievement.
I extend a warm welcome to you all to the 8th Annual Neglected Tropical Diseases meeting, which the Centre for Global Health is hosting for the eighth year running, and wish you fruitful deliberations.
Prof. Solomon Mpoke, PhD, MBS, IOD (K) DIRECTOR AND CEO, KEMRI
7
MESSAGE FROM THE DIRECTOR, KEMRI- CGHR
The Centre for Global Health Research, KEMRI,
based in Kisumu has participated in research on infectious diseases of poverty since its establishment in the early 80s, contributing significant wealth of knowledge for control and elimination of these diseases. Some of these diseases have now been listed by the global community and WHO as persisting scourges trapping their victims, mostly the poor in tropical settings, in a cycle of poverty and are earmarked for elimination by 2020. This is a huge task, but united in working closely and sharing progress, we can accomplish the goals we have set for ourselves.
It is therefore my great pleasure to welcome you to this year’s NTD Conference with its usual rich program of oral presentations, posters and side activities, which CGHR is proud to host for the 8th year running. We are honored by the presence of the Cabinet Secretary for Health, the Director KEMRI Dr. Solomon Mpoke, the Kisumu County Minister for Health, and the Kisumu County Director for Health. A special welcome to our Key Note speakers Dr. Simon Brooker, Prof. Jefitha Karimurio and Prof. Joyce Olenja. During the next two days, you will be able to hear from the presenters in four scientific sessions covering a wide range of topics, including operational research, public health and social studies, applied immunology, and basic research. This conference attracts both the experienced researchers, program managers, and the young scientists newly joining the field whom I wish to strongly encourage as this field of NTD research is in dire need of research capacity to match the international commitment towards elimination goals.
Our Neglected Tropical Disease Research Unit is focusing on providing the answers that schistosomiasis program managers would need in moving control and elimination efforts forward. We are delighted to present the progress from the SCORE projects at this conference, and to hear from others working on similar aspects and on other NTDs of significance in the region.
We are confident that this conference will present us with an opportunity to share excellent experiences from NTD research, control activities, to discuss new ideas and to make new friendships and collaborations. Please find time to visit a range of exhibitions from our partners and sponsors to whom we’re very grateful. While in Kisumu, please take a moment to pay us a visit at the Centre for Global Health Research Campus at Kisian and explore collaborative opportunities with our scientists.
Please enjoy the discussions at this conference, the company of all participants and the City of Kisumu!
Dr. Stephen Munga Director, CGHR –KEMRI
8
MESSAGE FROM THE CHAIR, KEMRI ANNUAL SCIENTIFIC AND HEALTH CONFERENCE (KASH), NTD CONFERENCE
We are delighted to present the 8th KEMRI NTD Conference. The Annual
KEMRI NTD Conference brings together health professionals including researchers, policy makers, implementers and other stakeholders, working on all aspects of Neglected Tropical Diseases (NTDs) to review progress and chart the way forward in the research and control of NTDs in the African region. This year’s conference is jointly organized and hosted by the Neglected Tropical Diseases Research Unit of the Centre for Global Health Research (CGHR), KEMRI, Kisumu and the Eastern and Southern Africa Centre for International Parasite Control (ESACIPAC), KEMRI, Nairobi. This annual meeting of NTD experts aims to foster networking among African NTDs researchers, policy makers and implementers and to disseminate research.’ This year’s Conference theme is NTD: Successes, Challenges and Opportunities –From the Bench to the Field and sub-themes include: Advances in applied Immunology and Diagnostics, Epidemiology and Operational Research, Health Behavioral and Social Sciences in all of the listed NTDs. This year, we have over 60 abstracts representing 12 of the NTDs, submitted by over 150 authors. Five nations in the African region are represented.
Our full program includes a key note address from a distinguished NTD researcher who has worked extensively in Africa, Prof. Simon Brooker of LSTMH. In addition two notable researchers in Kenya will give Key note addresses; Professors Jefitha Karimurio and Joyce Olenja, both leading researchers professors, and NTD control crusaders. A special welcome to both! In addition, several partners from the Ministry of Health, the Ministry of Education and NTD NGOs working in the country will have opportunities to address participants.
A good number of NTD program managers are in attendance and will give updates on control progress, and a special WASH symposium is organized in recognition of the much needed integrated approach to control of NTDs.
Pauline Mwinzi, PhD. CGHR. Doris Njomo, PhD. ESACIPAC
9
10
11
THE PROGRAM AT A GLANCE
WEDNESDAY, DECEMBER 10TH 2014 GUEST OF HONOR: CS, MINISTRY OF HEALTH, KENYA.
7.30 a.m. -9.00 a.m. ARRIVALS AND REGISTRATION 8.30 a.m. -9. 00 a.m.: The Year in Pictures Part I – Martin Omedo
Opening Session Session Chairs: Dr. Pauline Mwinzi; Dr. Doris Njomo
9.00 0a.m. - 11.00 a.m. 9.00 a.m. - 9:30 a.m. Introductions
Opening Plenary Session NTD Video –Fred Hollows Foundation
Dr. Maurice Odiere –Chief, KEMRI/CDC NTD Branch Dr. John Vulule – PI, KEMRI/CDC CoAg Dr. Martien Borgdorff Dr. Njenga –Director, ESACIPAC Dr. Munga-Director CGHR/KEMRI
9.30 a.m.- 9.40 a.m.
Welcome Speech
Dr. Solomon Mpoke-Director KEMRI
9.40 a.m. -9.50 a.m. Remarks Kisumu County Director of Health
9.50a.m. -10.00 a.m. Remarks Health Minister, Kisumu County
10.00 a.m. -10.15 a.m. Distinguished NTD Researcher Award
Dr. Solomon Mpoke-Director KEMRI
10.15 a.m. -10.45.a.m Opening address CS, MOH 11.00 a.m. - 11.30 p.m.
TEA BREAK MEDIA BRIEFING – Organizers: Winston Mbanda; James Wodera
Scientific session A: Immunology and Diagnostics 11.30 a.m. -1.00 p.m.
Session Chair: Dr. Bartholomew Ondigo, KEMRI Co-chair: Dr. Erick Muok, KEMRI
Rapporteur: Bernard Abudho
11.30 a.m. - 11.50 p.m. Plenary Dr. Mike Yaw Osei-Atweneboana

12
THURSDAY, DECEMBER 11TH DEC 2014
ARRIVALS AND REGISTRATION
8.00a.m. - 9.00 a.m. 8.30 a.m. -9. 00 a.m.: The year in Pictures Part II –Martin Omedo
NTD EPIDEMIOLOGY PLENARY
Chair: Dr. Maurice Odiere Rapporteur: Michael Ogutu
8.30a.m. - 9.00 a.m.
9.00 a.m. -9.10 a.m. NTD Video 9.20 a.m. - 9.30 a.m. Distinguished Scientist
Award Dr. Solomon Mpoke Dr. Stephen Munga
9.15 a.m. - 9.00 a.m. KEY NOTE ADDRESS Prof. Simon Brooker
11.50 a.m. - 1.00 p.m. Oral presentations Session Speakers
LUNCH 1.00 p.m. -2.00 p.m.
200 p.m. -4.30 p.m.
WASH SYMPOSIUM
Chair: Dr. Doris Njomo -KEMRI Co-chair: Mr. Martin Omedo –KEMRI/CDC
Rapporteur: Rosemary Musuva
2.00 p.m. - 2.30 p.m. KEY NOTE ADDRESS
Prof. Jefitha Karimurio
2.30 p.m. – 4.00 p.m. Oral Presentations 4.00 p.m. -4.30 p.m. Plenary Panelists:
Session speakers
4.15 p.m. – 5.30 p.m. TEA BREAK
POSTER SESSION [Immunology and Diagnostics;
WASH posters] SCIENTIFIC EXHIBITIONS
6. 00 p.m.-8.00 pm Student Reception
Session Organizers: Martin Omedo, Rosemary Musuva
13
Epidemiology and Operational Research: National Control Programs Chair: Dr. Doris Njomo
Rapporteur: Emmy Kavere 9.45 a.m. -10.30 am National programs updates Program managers
10.30a.m. - 11.00 a.m. Tea Break
11.00 a.m. – 1.00 p.m. Scientific Session B: Epidemiology and Operational Research
Session Chair: Dr. John Ayisi Mr. Martin Omedo
Rapporteur: Bridget Kimani 11.00 a.m. - 1.00 p.m.
11.00 a.m. - 11.20 a.m. Rabies update Dr. Mwangi Thumbi 11.20 a.m. - 12.45 p.m. Oral Presentations 12.45 p.m. - 1.00 p.m. Plenary Session Panelists:
1.00 p.m. -2.00 p.m. LUNCH BREAK
2.00 p.m. - 4.00 p.m. Scientific Session C: Health Behavioral Studies and Social Science
Chair: Dr. Jane Alaii Co-Chair Ms. Gladys Odhiambo
Rapporteur: Nipher Nyamogo
2.00 p.m. - 2.30 p.m. KEY NOTE ADDRESS Prof. Joyce Olenja 2.30 p.m. - 3.30 p.m. Oral presentations
4.00p.m -5.00 pm Closing Ceremony
Chair: Dr. Maurice Odiere Guest of Honor: Minister for Health Kisumu County
4.00 p.m. - 4.10 p.m. Chief Rapporteur Mr. Martin Omedo 4.10 p.m. – 4.15 p.m. NTD: Media Awards
Speech by Recipients Dr. Stephen Munga -Director, KEMRI-CGHR, Kisumu
4.15 p.m. - 4.30 p.m. Young Investigator Awards
Dr. Stephen Munga -Director, KEMRI-CGHR, Kisumu
4.30 p.m. Closing Remarks Minister Kisumu County
4.30 p.m. Coffee Break
PARTICIPANTS AND GUESTS LEAVE AT OWN PLEASURE
14
Simon Brooker is Professor of Epidemiology and a Wellcome Trust Senior Research Fellow at the London School of Hygiene & Tropical Medicine in the UK. His main research interests are the epidemiology, geography and control of infectious diseases, including neglected tropical diseases (NTDs) and malaria. He also has a keen interest in public engagement and the development of information and training resources and tools for NTD control, and developed the Global Atlas of Helminth Infection
(
KEYNOTE SPEAKER
www.thiswormyworld.org). Much of his research is conducted in close collaboration with national programmes and he has supported the work of national governments, international agencies and NGOs. Between 2008 and 2013 he was based full time at KEMRI-Wellcome Trust Research Programme in Nairobi and continues to collaborate with KEMRI on a range of research projects, including epidemiological support for the Kenya national school-based deworming programme.
15
Jefitha Karimurio is an Ophthalmologist, associate professor and expert in trachoma control working at the Department of Ophthalmology of the University of Nairobi since 1995. He is married with 2 adult children aged 26 and 29 years. Prof. Karimurio was educated at the University of Nairobi, for his Bachelor of Medicine and Bachelor of Surgery (1984), Master of medicine in Ophthalmology (1990) and later at the University of Melbourne, Australia for his PhD in Ophthalmology (2012). In his clinical career spanning several decades, he has worked in several places in Kenya as a Medical officer (MO), Medical Superintendent, Zonal Eye
Surgeon Acting Provincial Medical office for Central Province Head of the Kenya Ophthalmic Programme (KOP) Co-Chairman for the Eastern African Sub- Region, 1999-2004 International Agency for Prevention of Blindness (IAPB) World Health Organization prevention of blindness consultant to Eritrea, 2004 Prevention of blindness consultant to several NGOs and governments and has been the Lead consultant for Kenya trachoma mapping since 2004. He has published more than 30 articles in peer review journals Supervision of postgraduate research projects: 29 completed and 3 ongoing and facilitated many scientific conferences and workshops in his field of research.
KEYNOTE SPEAKER
16
Joyce Olenja is a Professor of Community Health in the School of Public Health, College of Health Sciences at the University of Nairobi. She has over 25 years of teaching and research experience. Trained as a Medical Anthropologist, she is engaged in teaching and supervision at both undergraduate and postgraduate levels. At postgraduate level supervision spans the broad areas of applied social
science and public health; specifically Primary health care and community partnerships. In addition she is engaged in population health research particularly the role of culture and how this interfaces with an emerging socio economic environment that influences care seeking behaviour. Some of the research conducted has contributed to policy change to meet the needs of the population as well as service delivery. She has several publications in peer reviewed journals.
KEYNOTE SPEAKER
17

18

19
PROGRAM
WEDNESDAY, DECEMBER 10TH 2014 GUEST OF HONOR: CS, MINISTRY OF HEALTH KENYA
7.30 a.m. -9.00 a.m. ARRIVALS AND REGISTRATION 8.30 a.m. -9. 00 a.m.: The year in pictures Part I –Martin Omedo
Opening Session Session Chair: Dr. Pauline Mwinzi
9.00 0a.m. - 11.00 a.m. 9.00a.m. - 9:30 a.m. Introductions
Opening Plenary Session NTD Video –Fred Hollows Foundation
Dr. Maurice Odiere –Chief, KEMRI/CDC NTD Branch Dr. John Vulule –PI, KEMRI/CDC CoAg Dr. Martien Borgdorff Dr. Njenga – Director, ESACIPAC Dr. Munga-Director CGHR/KEMRI
9.30 a.m. - 9.40 a.m.
Welcome Speech
Dr. Solomon Mpoke-Director KEMRI
9.40 a.m. - 9.50 a.m. Remarks Kisumu County Director of Health
9.50 a.m. - 10.00 a.m. Remarks Health Minister, Kisumu County
10.00 a.m. - 10.15 a.m. Distinguished NTD Researcher Award
Dr. Solomon Mpoke-Director KEMRI
10.15 a.m. - 10.45 a.m. Opening address CS MOH 11.00 a.m. - 11.30 p.m.
TEA BREAK MEDIA BRIEFING – Organizers: Winston Mbanda; James Wodera
Scientific session A: Immunology and Diagnostics 11.30 a.m. -1.00 p.m.
Session Chair: Dr. Bartholomew Ondigo, KEMRI Co-chair: Dr. Pauline Mwinzi, KEMRI

20
11.30 a.m. - 11.50 p.m. NTD8-A1
Plenary: Phenotypic Response Profile Of Onchocerca volvulus To Ivermectin Treatment And Genetic Analysis Towards Development Of Genetic Markers For Monitoring Of Resistance
Dr. Mike Yaw Osei-Atweneboana
11.50 a.m. - 12.05 p.m. NTD8-A2 Impact of schistosomiasis and soil
transmitted helminths on vaccine-induced immune responses.
Diana K. Riner, Eric M. Ndombi, Barthlomew Ondigo et al.,
12.05 p.m. - 12.20 p.m. NTD8-A3
The reliability of the POC-CCA test makes it a suitable tool for use in schistosomiasis control programs
Elizabeth Ochola
12.20 p.m. - 12.35 p.m. NTD8-A4
Testing the diagnostic potential of in-house developed monoclonal antibodies against rift valley fever virus.
Salame Ashur
12.35 p.m. - 12.50 p.m. NTD8-A5
Performance of Kato-Katz, Mini-Parasep and Mini-FLOTAC techniques in detection of intestinal helminth ova in Mbita district, Homabay county, Kenya
Annette Ngetich
12.50 p.m. - 1.00 p.m. Plenary Session Panelists: Session speakers
LUNCH 1.00 p.m. -2.00 p.m.
WASH SYMPOSIUM
CHAIR: DR. DORIS NJOMO -KEMRI
Co-chair: Mr. Martin Omedo –KEMRI/CDC
2.00 p.m. - 2.30 p.m. KEY NOTE
KEY NOTE ADDRESS: Discrepancies in Trachoma control policies and practices in the last decade
Prof. Jefitha Karimurio
2.30 p.m. -2.45 p.m. NTD8-W1
Socio-cultural determinants to adoption of safe water, sanitation
Job Wasonga
21
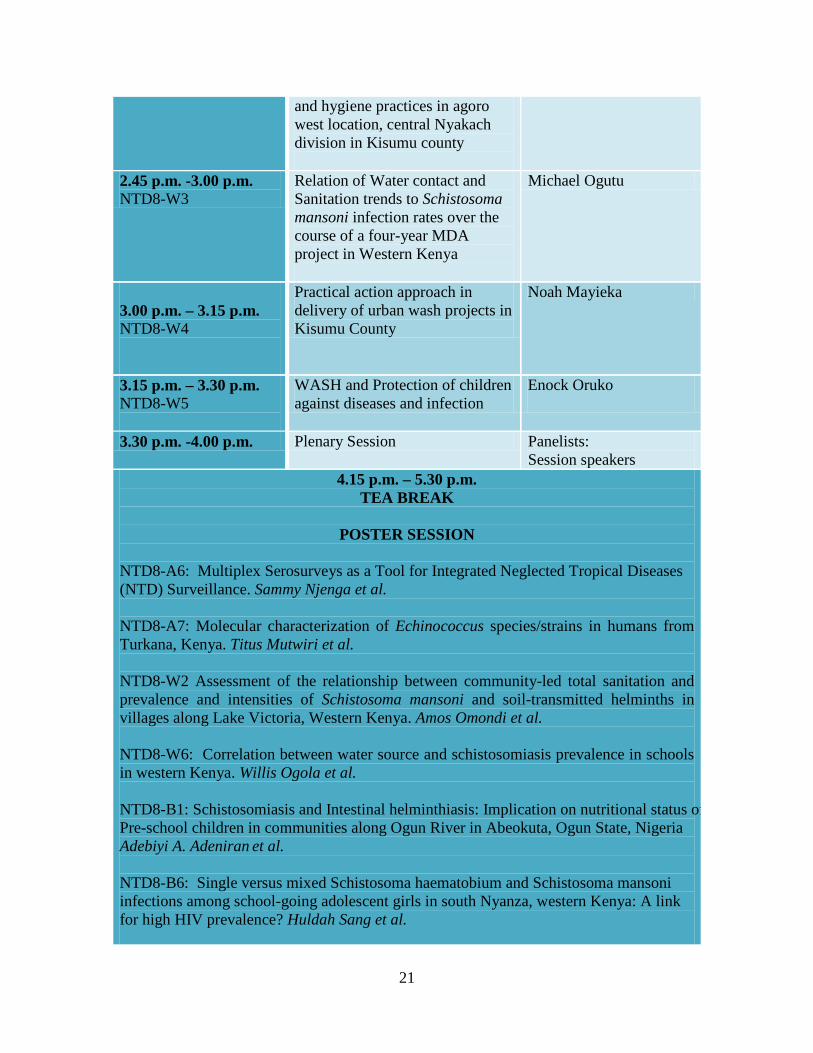
and hygiene practices in agoro west location, central Nyakach division in Kisumu county
2.45 p.m. -3.00 p.m. NTD8-W3
Relation of Water contact and Sanitation trends to Schistosoma mansoni infection rates over the course of a four-year MDA project in Western Kenya
Michael Ogutu
3.00 p.m. – 3.15 p.m. NTD8-W4
Practical action approach in delivery of urban wash projects in Kisumu County
Noah Mayieka
3.15 p.m. – 3.30 p.m. NTD8-W5
WASH and Protection of children against diseases and infection
Enock Oruko
3.30 p.m. -4.00 p.m. Plenary Session Panelists: Session speakers
4.15 p.m. – 5.30 p.m. TEA BREAK
POSTER SESSION
NTD8-A6: Multiplex Serosurveys as a Tool for Integrated Neglected Tropical Diseases (NTD) Surveillance. Sammy Njenga et al. NTD8-A7: Molecular characterization of Echinococcus species/strains in humans from Turkana, Kenya. Titus Mutwiri et al. NTD8-W2 Assessment of the relationship between community-led total sanitation and prevalence and intensities of Schistosoma mansoni and soil-transmitted helminths in villages along Lake Victoria, Western Kenya. Amos Omondi et al. NTD8-W6: Correlation between water source and schistosomiasis prevalence in schools in western Kenya. Willis Ogola et al. NTD8-B1: Schistosomiasis and Intestinal helminthiasis: Implication on nutritional status of Pre-school children in communities along Ogun River in Abeokuta, Ogun State, Nigeria Adebiyi A. Adeniran et al. NTD8-B6: Single versus mixed Schistosoma haematobium and Schistosoma mansoni infections among school-going adolescent girls in south Nyanza, western Kenya: A link for high HIV prevalence? Huldah Sang et al.
22
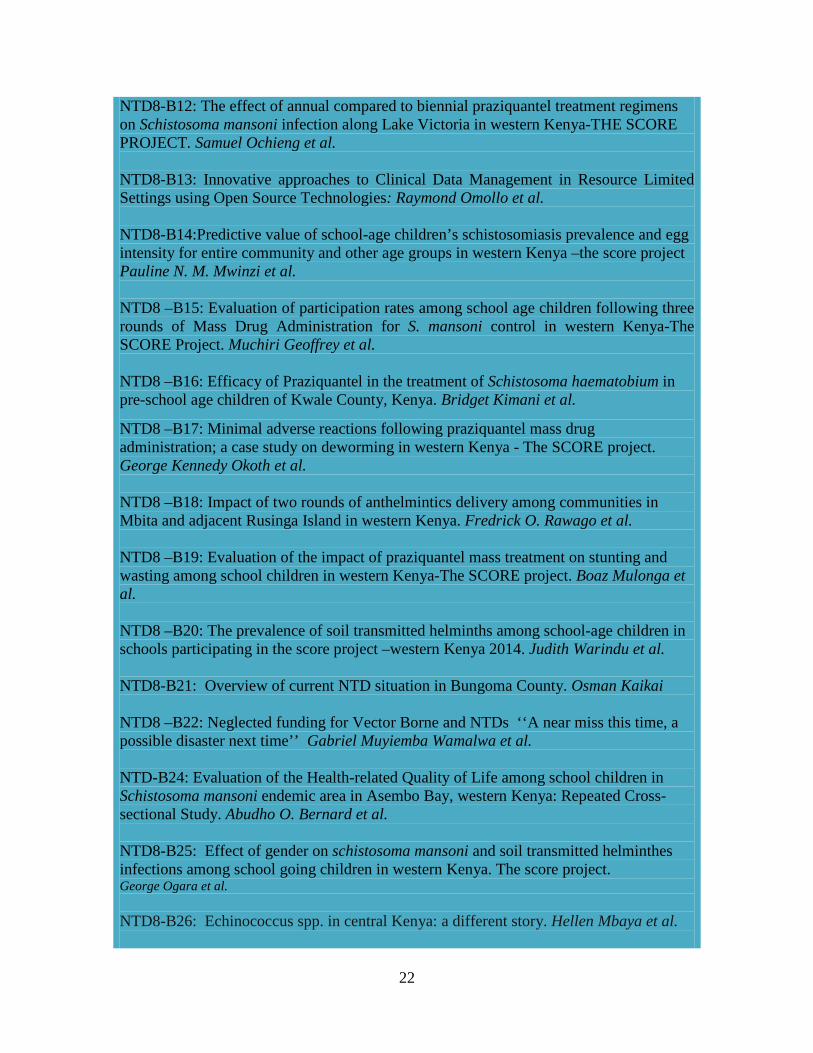
NTD8-B12: The effect of annual compared to biennial praziquantel treatment regimens on Schistosoma mansoni infection along Lake Victoria in western Kenya-THE SCORE PROJECT. Samuel Ochieng et al. NTD8-B13: Innovative approaches to Clinical Data Management in Resource Limited Settings using Open Source Technologies: Raymond Omollo et al.
NTD8-B14:Predictive value of school-age children’s schistosomiasis prevalence and egg intensity for entire community and other age groups in western Kenya –the score project Pauline N. M. Mwinzi et al. NTD8 –B15: Evaluation of participation rates among school age children following three rounds of Mass Drug Administration for S. mansoni control in western Kenya-The SCORE Project. Muchiri Geoffrey et al. NTD8 –B16: Efficacy of Praziquantel in the treatment of Schistosoma haematobium in pre-school age children of Kwale County, Kenya. Bridget Kimani et al.
NTD8 –B17: Minimal adverse reactions following praziquantel mass drug administration; a case study on deworming in western Kenya - The SCORE project. George Kennedy Okoth et al. NTD8 –B18: Impact of two rounds of anthelmintics delivery among communities in Mbita and adjacent Rusinga Island in western Kenya. Fredrick O. Rawago et al. NTD8 –B19: Evaluation of the impact of praziquantel mass treatment on stunting and wasting among school children in western Kenya-The SCORE project. Boaz Mulonga et al. NTD8 –B20: The prevalence of soil transmitted helminths among school-age children in schools participating in the score project –western Kenya 2014. Judith Warindu et al. NTD8-B21: Overview of current NTD situation in Bungoma County. Osman Kaikai NTD8 –B22: Neglected funding for Vector Borne and NTDs ‘‘A near miss this time, a possible disaster next time’’ Gabriel Muyiemba Wamalwa et al. NTD-B24: Evaluation of the Health-related Quality of Life among school children in Schistosoma mansoni endemic area in Asembo Bay, western Kenya: Repeated Cross-sectional Study. Abudho O. Bernard et al. NTD8-B25: Effect of gender on schistosoma mansoni and soil transmitted helminthes infections among school going children in western Kenya. The score project. George Ogara et al. NTD8-B26: Echinococcus spp. in central Kenya: a different story. Hellen Mbaya et al.
23
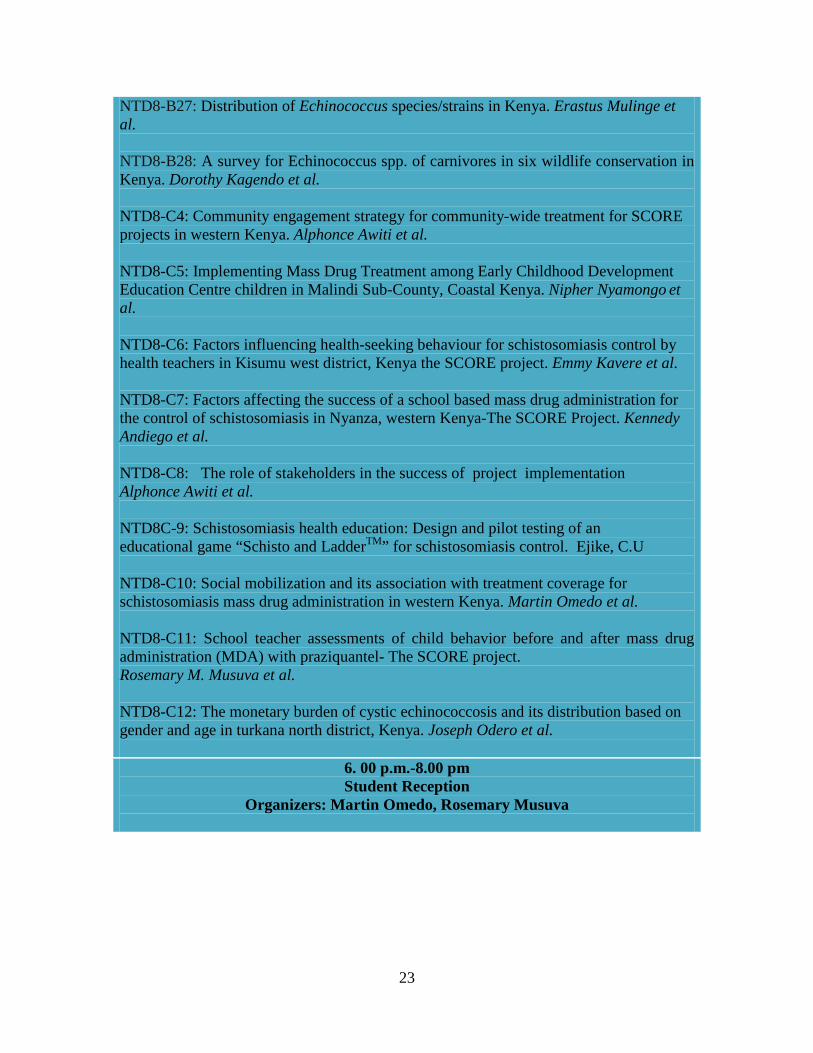
NTD8-B27: Distribution of Echinococcus species/strains in Kenya. Erastus Mulinge et al. NTD8-B28: A survey for Echinococcus spp. of carnivores in six wildlife conservation in Kenya. Dorothy Kagendo et al. NTD8-C4: Community engagement strategy for community-wide treatment for SCORE projects in western Kenya. Alphonce Awiti et al. NTD8-C5: Implementing Mass Drug Treatment among Early Childhood Development Education Centre children in Malindi Sub-County, Coastal Kenya. Nipher Nyamongo et al. NTD8-C6: Factors influencing health-seeking behaviour for schistosomiasis control by health teachers in Kisumu west district, Kenya the SCORE project. Emmy Kavere et al. NTD8-C7: Factors affecting the success of a school based mass drug administration for the control of schistosomiasis in Nyanza, western Kenya-The SCORE Project. Kennedy Andiego et al. NTD8-C8: The role of stakeholders in the success of project implementation Alphonce Awiti et al. NTD8C-9: Schistosomiasis health education: Design and pilot testing of an educational game “Schisto and LadderTM” for schistosomiasis control. Ejike, C.U NTD8-C10: Social mobilization and its association with treatment coverage for schistosomiasis mass drug administration in western Kenya. Martin Omedo et al. NTD8-C11: School teacher assessments of child behavior before and after mass drug administration (MDA) with praziquantel- The SCORE project. Rosemary M. Musuva et al. NTD8-C12: The monetary burden of cystic echinococcosis and its distribution based on gender and age in turkana north district, Kenya. Joseph Odero et al.
6. 00 p.m.-8.00 pm Student Reception
Organizers: Martin Omedo, Rosemary Musuva

24
THURSDAY, DECEMBER 11TH 2014
ARRIVALS AND REGISTRATION 8.00 a.m. - 9.00 a.m.
8.30 a.m. -9. 00 a.m.: The year in Pictures Part II –Martin Omedo
NTD EPIDEMIOLOGY PLENARY
Chair: Dr. Maurice Odiere 8.30 a.m. - 9.00 a.m.
9.00 a.m. - 9.10 a.m. NTD Video 9.00 a.m. - 9.15 a.m. Distinguished Scientist Award Dr. Solomon Mpoke
Dr. Stephen Munga 9.15 a.m. - 9.45 a.m. KEY NOTE ADDRESS:
Mapping, surveillance and control of neglected tropical diseases in Kenya and beyond
Prof. Simon Brooker
Epidemiology and Operational Research: National Control Programs
Chair: Dr. Doris Njomo 9.45 a.m. - 10.00 a.m. NTD8 –B7-P
Task shifting for eye care in Eastern Africa: General Nurses as trichiasis surgeons in Kenya, Malawi, and Tanzania
Michael Gichangi
10.00 a.m. - 10.15 a.m. NTD8 –B9-P
Countdown to Trachoma Elimination in Kenya
Ernest Barasa
10.15 a.m. - 10.30.a.m. NTD8 –B23-P
National School-Based Deworming Programme: successes, challenges, and lessons learnt from targeting and its impact on deworming coverage of school-age children.
Alex Mutua, Claire Gwayi-Chore et al.
10.30 a.m. - 11.00 a.m. Tea Break
11.00 a.m. – 1.00 p.m. Scientific Session B: Epidemiology and Operational Research
Session Chair: Dr. John Ayisi Co-Chair: Mr. Martin Omedo
11.00 a.m. - 11.15 a.m. NTD8 –B10-P
Eliminating human dog-mediated rabies in Kenya
Mwangi Thumbi

25
11.15 a.m. - 11.30 a.m. NTD8 –B2
Schistosoma mansoni and Biomphalaria pfeifferi compatibility studies and implications for schistosomiasis control in Kenya
Martin Mutuku
11.30 a.m. - 11.45 a.m. NTD8 –B3
Determination of prevalence and risk factors associated with intestinal schistosomiasis and helminth infections among adults living in Mwea West district, Kirinyaga County, Central Kenya.
Janet Masaku
11.45. a.m. - 12.00 p.m. NTD8 –B4
The evaluation of jigger infestations among populations of rural villages of Bumula and Kimilili sub counties, Bungoma County
Gabriel Muyiemba
12.00 p.m. - 12.15 p.m. NTD8 –B5
Exposures to chikungunya and dengue viruses in two coastal and western Kenyan sites
Bryson Ndenga
12.15 p.m. - 12.30 p.m. NTD8 –B8
The Economic Impact Of Visceral Leishmaniasis In Baringo, Kenya
Simon Bolo
12.30 p.m. - 12.45 p.m. NTD8 –B11
The impact of three rounds of Praziquantel Mass Drug Administration on Schistosoma mansoni infections: a comparison between Community Wide treatment and School-based treatment in western Kenya-The SCORE project.
Isaac Onkanga
12.45 p.m. -1.00 p.m.
Plenary Session Speakers
1.00 p.m. - 2.00 p.m. LUNCH BREAK
2.00 p.m. - 4.00 p.m. Scientific Session C: Health Behavioral Studies and Social Science
Chair: Dr. Jane Alaii Co-Chair Ms. Gladys Odhiambo
2.00 p.m. - 2.30 p.m. KEY NOTE
KEY NOTE ADDRESS: Applying a socio-ecological
Prof. Joyce Olenja
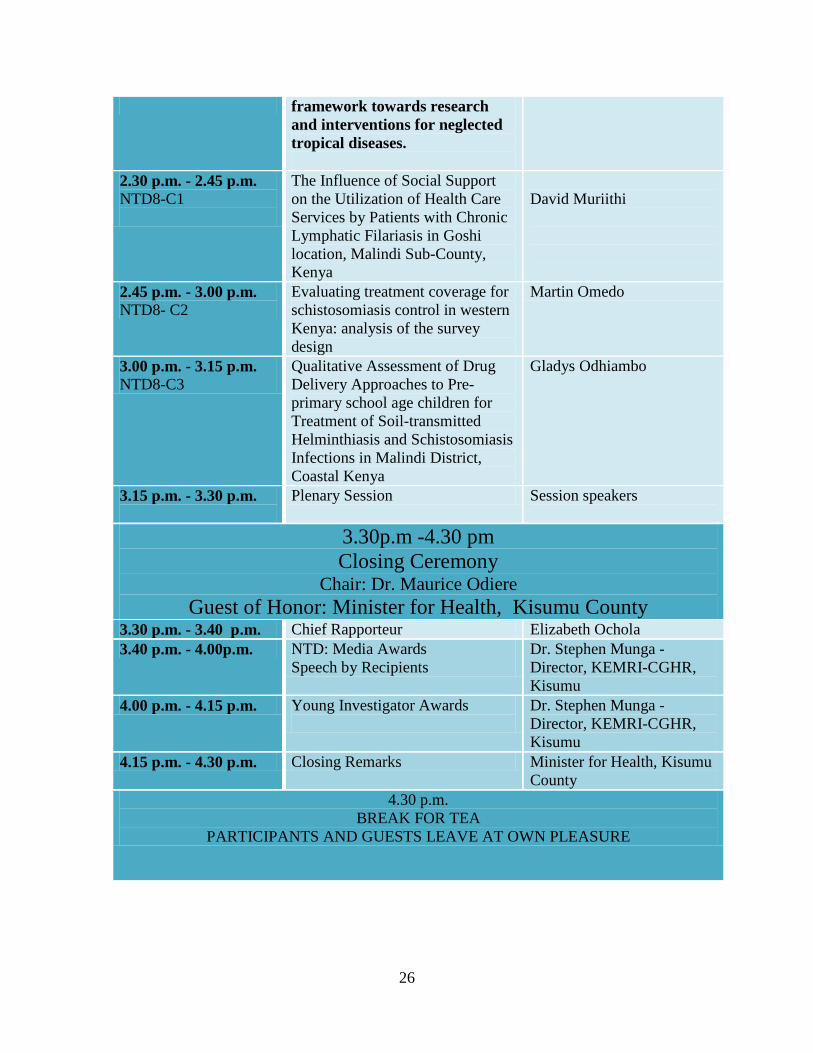
26
framework towards research and interventions for neglected tropical diseases.
2.30 p.m. - 2.45 p.m. NTD8-C1
The Influence of Social Support on the Utilization of Health Care Services by Patients with Chronic Lymphatic Filariasis in Goshi location, Malindi Sub-County, Kenya
David Muriithi
2.45 p.m. - 3.00 p.m. NTD8- C2
Evaluating treatment coverage for schistosomiasis control in western Kenya: analysis of the survey design
Martin Omedo
3.00 p.m. - 3.15 p.m. NTD8-C3
Qualitative Assessment of Drug Delivery Approaches to Pre-primary school age children for Treatment of Soil-transmitted Helminthiasis and Schistosomiasis Infections in Malindi District, Coastal Kenya
Gladys Odhiambo
3.15 p.m. - 3.30 p.m.
Plenary Session Session speakers
3.30p.m -4.30 pm Closing Ceremony
Chair: Dr. Maurice Odiere Guest of Honor: Minister for Health, Kisumu County
3.30 p.m. - 3.40 p.m. Chief Rapporteur Elizabeth Ochola 3.40 p.m. - 4.00p.m. NTD: Media Awards
Speech by Recipients Dr. Stephen Munga -Director, KEMRI-CGHR, Kisumu
4.00 p.m. - 4.15 p.m. Young Investigator Awards
Dr. Stephen Munga -Director, KEMRI-CGHR, Kisumu
4.15 p.m. - 4.30 p.m. Closing Remarks Minister for Health, Kisumu County
4.30 p.m. BREAK FOR TEA
PARTICIPANTS AND GUESTS LEAVE AT OWN PLEASURE

27
SCIENTIFIC SESSION A: IMMUNOLOGY AND DIAGNOSTICS
ABSTRACTS
NTD8-A1
Phenotypic Response Profile Of Onchocerca volvulus To Ivermectin Treatment And Genetic Analysis Towards Development Of Genetic Markers For Monitoring Of Resistance Mike Yaw Osei-Atweneboana Council for scientific and Industrial Research-Ghana Onchocerciasis control and elimination programmes worldwide are largely dependent on the sustained efficacy of ivermectin (IVM). However, recent reports on sub-optimal responses to IVM treatment has raised concerns about the possible emergence of IVM resistance. An epidemiological and genetic studies were carried out to assess the parasitological response profile of Onchocerca volvulus to IVM treatment and genetic analysis to select single nucleotide polymorphism (SNPs) for development of genetic markers. A total of 2,878 subjects from 30 onchocerciasis endemic communities were enrolled for a cross-sectional studies, this was followed by a fifteen month longitudinal study involving 538 subjects selected from 15 communities. The study involved repeated skin microfilariae (mf) assessment, semi-annual IVM treatments and nodulectomies at day 90 after the third study IVM treatment. Our results showed an average mf prevalence of 18.4% and nodule prevalene of 23.4% while 33.7% were microfilarial positive and/or nodule positive. For the longitudinal study, two out of 15 communities responded sub-optimally to IVM treatment, while three communities showed significantly faster (p<0.03) mf recovery rate of more than 50% of pre-treatment mf densities. Embryogramme analysis at 90 days after the third study IVM treatment showed the reproductive status of the adult female worms. About 37% of female worms were not reproductivly active at 90 days after IVM treatment, showing good response to IVM while 4% were found producing various embryonic stages including stretch mf, however, 63% of the females had both live and degenerate streteched mf. Genetic analyses carried out on 312 well-characterized female O. volvulus worms identified SNPs in β-tubulin genes that are associated with poor IVM response phenotypes. The genotype configuration, GG/CC/TT/GG occurring at four SNP sites, 1183 T/G, 1188 T/C, 1308 C/T and 1545 A/G was found to be strongly associated (p< 0.01) with poor IVM response phenotype worms. These SNPs have been selected as potential genetic marker for validation and marker development for monitoring IVM resistance.
NTD8- Impact of schistosomiasis and soil transmitted helminths on vaccine-
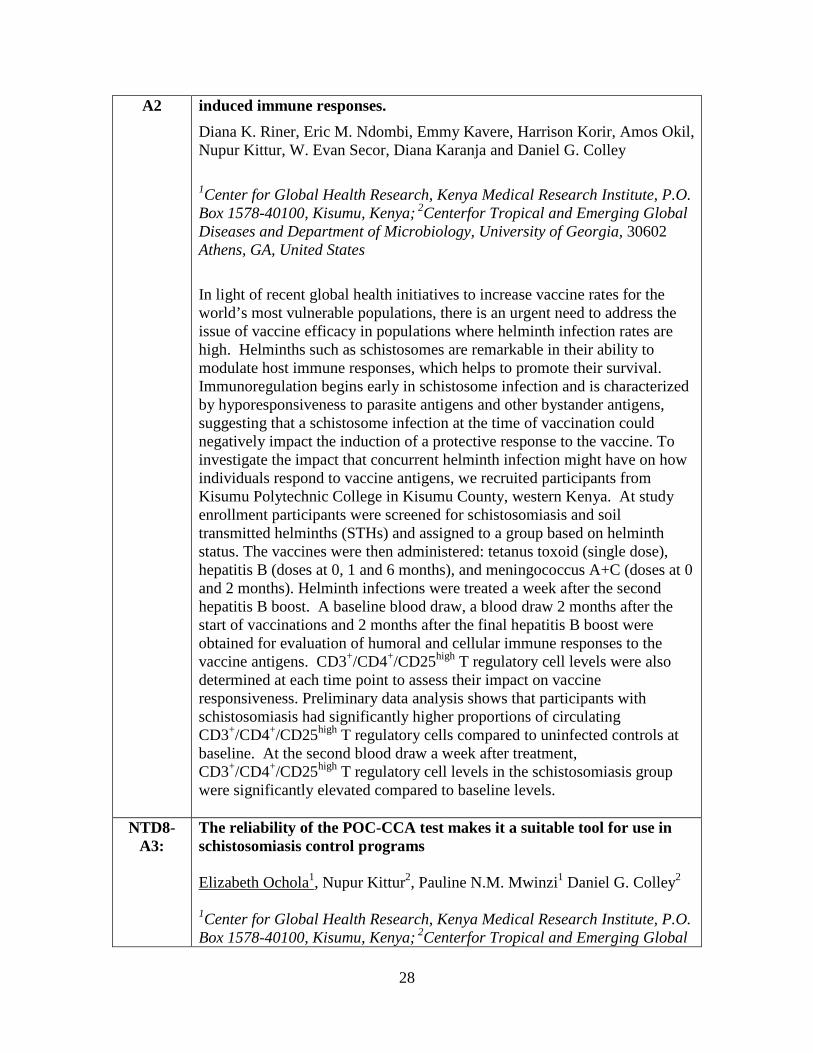
28
A2 induced immune responses. Diana K. Riner, Eric M. Ndombi, Emmy Kavere, Harrison Korir, Amos Okil, Nupur Kittur, W. Evan Secor, Diana Karanja and Daniel G. Colley
1Center for Global Health Research, Kenya Medical Research Institute, P.O. Box 1578-40100, Kisumu, Kenya; 2Centerfor Tropical and Emerging Global Diseases and Department of Microbiology, University of Georgia, 30602 Athens, GA, United States
In light of recent global health initiatives to increase vaccine rates for the world’s most vulnerable populations, there is an urgent need to address the issue of vaccine efficacy in populations where helminth infection rates are high. Helminths such as schistosomes are remarkable in their ability to modulate host immune responses, which helps to promote their survival. Immunoregulation begins early in schistosome infection and is characterized by hyporesponsiveness to parasite antigens and other bystander antigens, suggesting that a schistosome infection at the time of vaccination could negatively impact the induction of a protective response to the vaccine. To investigate the impact that concurrent helminth infection might have on how individuals respond to vaccine antigens, we recruited participants from Kisumu Polytechnic College in Kisumu County, western Kenya. At study enrollment participants were screened for schistosomiasis and soil transmitted helminths (STHs) and assigned to a group based on helminth status. The vaccines were then administered: tetanus toxoid (single dose), hepatitis B (doses at 0, 1 and 6 months), and meningococcus A+C (doses at 0 and 2 months). Helminth infections were treated a week after the second hepatitis B boost. A baseline blood draw, a blood draw 2 months after the start of vaccinations and 2 months after the final hepatitis B boost were obtained for evaluation of humoral and cellular immune responses to the vaccine antigens. CD3+/CD4+/CD25high T regulatory cell levels were also determined at each time point to assess their impact on vaccine responsiveness. Preliminary data analysis shows that participants with schistosomiasis had significantly higher proportions of circulating CD3+/CD4+/CD25high T regulatory cells compared to uninfected controls at baseline. At the second blood draw a week after treatment, CD3+/CD4+/CD25high T regulatory cell levels in the schistosomiasis group were significantly elevated compared to baseline levels.
NTD8-A3:
The reliability of the POC-CCA test makes it a suitable tool for use in schistosomiasis control programs Elizabeth Ochola1
1Center for Global Health Research, Kenya Medical Research Institute, P.O. Box 1578-40100, Kisumu, Kenya; 2Centerfor Tropical and Emerging Global
, Nupur Kittur2, Pauline N.M. Mwinzi1 Daniel G. Colley2
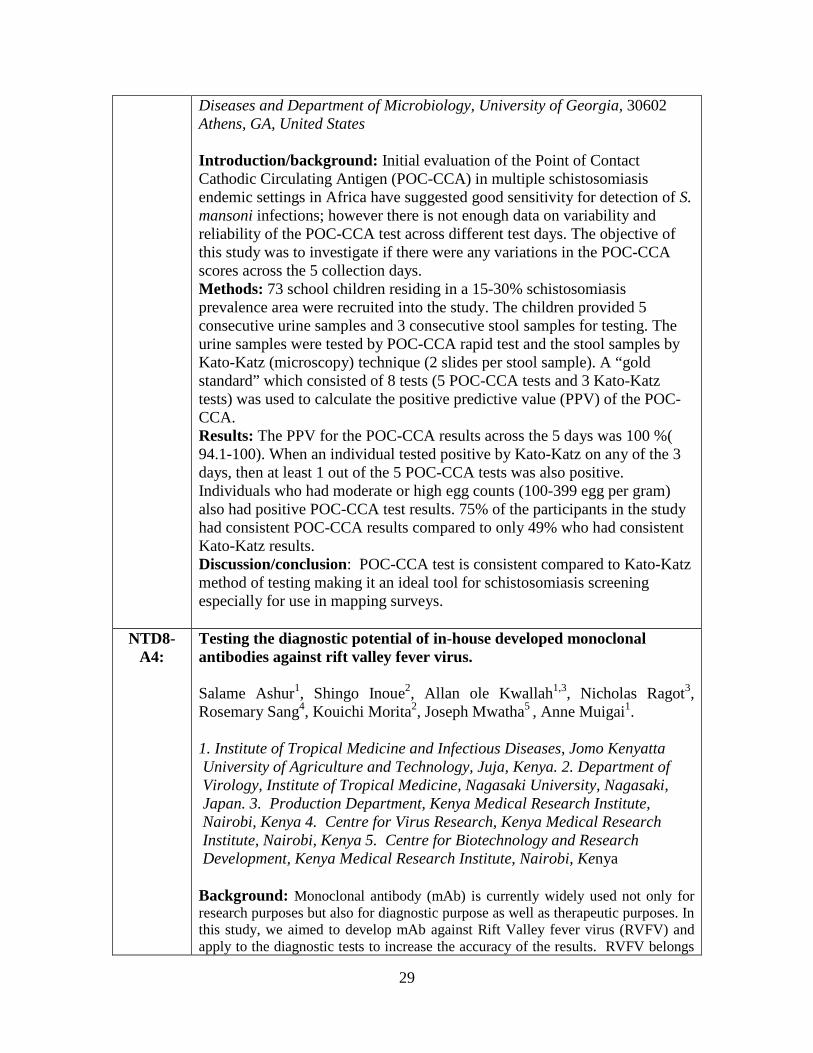
29
Diseases and Department of Microbiology, University of Georgia, 30602 Athens, GA, United States Introduction/background: Initial evaluation of the Point of Contact Cathodic Circulating Antigen (POC-CCA) in multiple schistosomiasis endemic settings in Africa have suggested good sensitivity for detection of S. mansoni infections; however there is not enough data on variability and reliability of the POC-CCA test across different test days. The objective of this study was to investigate if there were any variations in the POC-CCA scores across the 5 collection days. Methods: 73 school children residing in a 15-30% schistosomiasis prevalence area were recruited into the study. The children provided 5 consecutive urine samples and 3 consecutive stool samples for testing. The urine samples were tested by POC-CCA rapid test and the stool samples by Kato-Katz (microscopy) technique (2 slides per stool sample). A “gold standard” which consisted of 8 tests (5 POC-CCA tests and 3 Kato-Katz tests) was used to calculate the positive predictive value (PPV) of the POC-CCA. Results: The PPV for the POC-CCA results across the 5 days was 100 %( 94.1-100). When an individual tested positive by Kato-Katz on any of the 3 days, then at least 1 out of the 5 POC-CCA tests was also positive. Individuals who had moderate or high egg counts (100-399 egg per gram) also had positive POC-CCA test results. 75% of the participants in the study had consistent POC-CCA results compared to only 49% who had consistent Kato-Katz results. Discussion/conclusion: POC-CCA test is consistent compared to Kato-Katz method of testing making it an ideal tool for schistosomiasis screening especially for use in mapping surveys.
NTD8-A4:
Testing the diagnostic potential of in-house developed monoclonal antibodies against rift valley fever virus. Salame Ashur1, Shingo Inoue2, Allan ole Kwallah1,3, Nicholas Ragot3, Rosemary Sang4, Kouichi Morita2, Joseph Mwatha5 , Anne Muigai1. 1. Institute of Tropical Medicine and Infectious Diseases, Jomo Kenyatta University of Agriculture and Technology, Juja, Kenya. 2. Department of Virology, Institute of Tropical Medicine, Nagasaki University, Nagasaki, Japan. 3. Production Department, Kenya Medical Research Institute, Nairobi, Kenya 4. Centre for Virus Research, Kenya Medical Research Institute, Nairobi, Kenya 5. Centre for Biotechnology and Research Development, Kenya Medical Research Institute, Nairobi, Kenya Background: Monoclonal antibody (mAb) is currently widely used not only for research purposes but also for diagnostic purpose as well as therapeutic purposes. In this study, we aimed to develop mAb against Rift Valley fever virus (RVFV) and apply to the diagnostic tests to increase the accuracy of the results. RVFV belongs

30
to Family Bunyaviridae and it causes Rift Valley fever (RVF) which is one of the major viral hemorrhagic fevers in Kenya and African continent. RVFV is transmitted by Aedes and Culex mosquito bites and contact with infected body fluids including blood and milk. Due to the presence of other Bunya viruses (e.g. Crimean-Congo hemorrhagic fever virus and Nairobi sheep disease virus) in Kenya, RVFV specific mAb based diagnostic tests are highly needed. Methods: BALB/C mice were immunized with purified, inactivated RVFV (attenuated live vaccine strain: Smithburn) and when the IgG titers were high enough, the mouse spleen was harvested and splenocytes were fused with mouse myeloma SP2 cells. Four clones of anti-RVFV mAb were successfully established. Among them, Clone “P1E5” was further cultured in large scale and purified by protein G column. The purified mAb was applied for antigen detection ELISA, antigen-capture IgG indirect ELISA and western blot. Results: The mAb (P1E5) was applied for antigen detection ELISA and specifically detected only RVFV but not dengue virus serotypes 1-4, yellow fever virus, West Nile virus and chikungunya virus. Antigen capture IgG indirect ELISA could detect IgG from patient sera that were known to have anti-RVFV IgG. Western blot using this mAb could detect RVFV and it specifically reacted with L segment derived protein (250kDa). Conclusion: Although further analysis using other Bunya viruses is required, these three tests could detect RVFV and anti-RVFV IgG from clinical specimen. Keywords: Rift Valley fever virus, monoclonal antibody, Antigen capture IgG indirect ELISA, Western blot
NTD8-A5
Performance of Kato-Katz, Mini-Parasep and Mini-FLOTAC techniques in detection of intestinal helminth ova in Mbita district, Homabay county, Kenya Annette Ngetich1,3, Kimberley Won2, Walter GZO Jura3, Pauline NM Mwinzi1, Maurice R Odiere1
1Neglected Tropical Diseases Branch, Centre for Global Health Research, Kenya Medical Research Institute, P. O. Box 1578-40100, Kisumu, Kenya 2Centers for Disease Control and Prevention, Division of Parasitic Diseases and Malaria, Atlanta, GA, USA 3Department of Zoology, Maseno University, P. O. Box 333-40105, Maseno, Kenya. Background: Lack of knowledge about the true extent of multiparasitism is usually attributed to unavailability of a single diagnostic method which is able to combine robustness, simplicity, and good sensitivity in detecting all parasite species. Widely used diagnostic approaches such as the Kato-Katz technique lack sensitivity particularly in low endemicity areas, and hence reported prevalence rates considerably underestimate the true number of
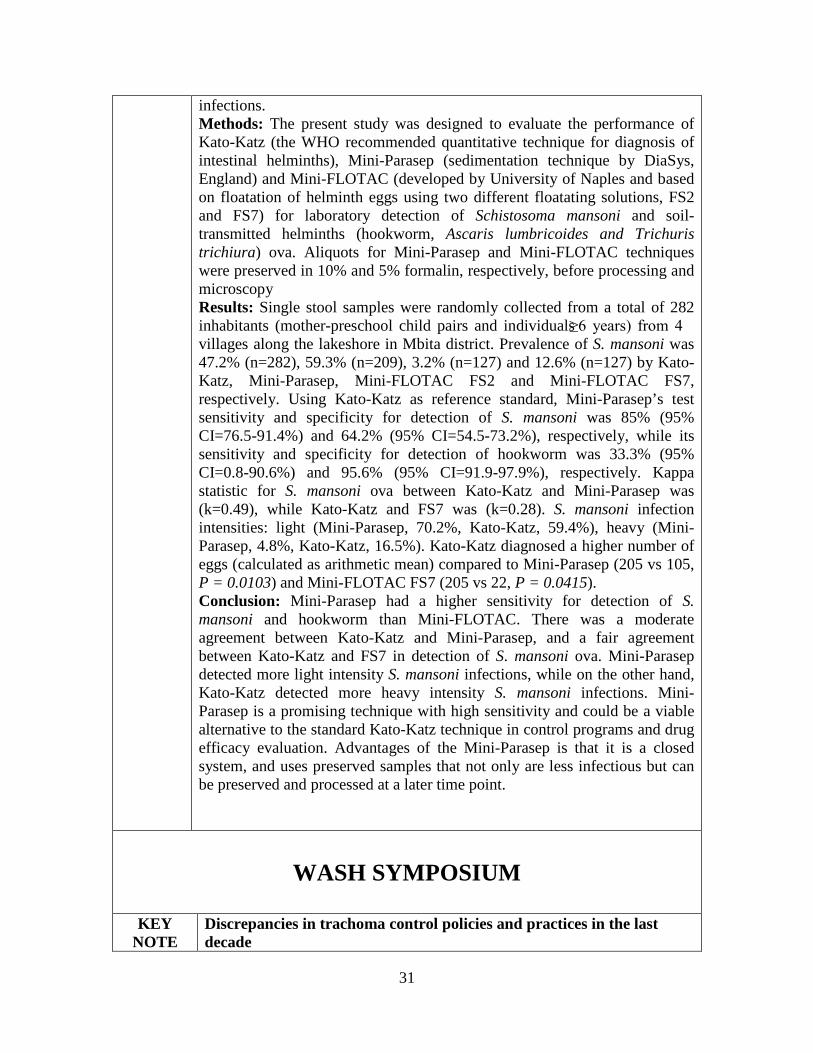
31
infections. Methods: The present study was designed to evaluate the performance of Kato-Katz (the WHO recommended quantitative technique for diagnosis of intestinal helminths), Mini-Parasep (sedimentation technique by DiaSys, England) and Mini-FLOTAC (developed by University of Naples and based on floatation of helminth eggs using two different floatating solutions, FS2 and FS7) for laboratory detection of Schistosoma mansoni and soil-transmitted helminths (hookworm, Ascaris lumbricoides and Trichuris trichiura) ova. Aliquots for Mini-Parasep and Mini-FLOTAC techniques were preserved in 10% and 5% formalin, respectively, before processing and microscopy Results: Single stool samples were randomly collected from a total of 282 inhabitants (mother-preschool child pairs and individuals ≥6 years) from 4 villages along the lakeshore in Mbita district. Prevalence of S. mansoni was 47.2% (n=282), 59.3% (n=209), 3.2% (n=127) and 12.6% (n=127) by Kato-Katz, Mini-Parasep, Mini-FLOTAC FS2 and Mini-FLOTAC FS7, respectively. Using Kato-Katz as reference standard, Mini-Parasep’s test sensitivity and specificity for detection of S. mansoni was 85% (95% CI=76.5-91.4%) and 64.2% (95% CI=54.5-73.2%), respectively, while its sensitivity and specificity for detection of hookworm was 33.3% (95% CI=0.8-90.6%) and 95.6% (95% CI=91.9-97.9%), respectively. Kappa statistic for S. mansoni ova between Kato-Katz and Mini-Parasep was (k=0.49), while Kato-Katz and FS7 was (k=0.28). S. mansoni infection intensities: light (Mini-Parasep, 70.2%, Kato-Katz, 59.4%), heavy (Mini-Parasep, 4.8%, Kato-Katz, 16.5%). Kato-Katz diagnosed a higher number of eggs (calculated as arithmetic mean) compared to Mini-Parasep (205 vs 105, P = 0.0103) and Mini-FLOTAC FS7 (205 vs 22, P = 0.0415). Conclusion: Mini-Parasep had a higher sensitivity for detection of S. mansoni and hookworm than Mini-FLOTAC. There was a moderate agreement between Kato-Katz and Mini-Parasep, and a fair agreement between Kato-Katz and FS7 in detection of S. mansoni ova. Mini-Parasep detected more light intensity S. mansoni infections, while on the other hand, Kato-Katz detected more heavy intensity S. mansoni infections. Mini-Parasep is a promising technique with high sensitivity and could be a viable alternative to the standard Kato-Katz technique in control programs and drug efficacy evaluation. Advantages of the Mini-Parasep is that it is a closed system, and uses preserved samples that not only are less infectious but can be preserved and processed at a later time point.
WASH SYMPOSIUM
KEY
NOTE Discrepancies in trachoma control policies and practices in the last decade

32
Author: Professor Jefitha Karimurio, PhD Department of Ophthalmology, University of Nairobi Email: [email protected] Purpose: To establish the discrepancies in trachoma control policies and practices since 2004 Introduction: The World Health Organisation (WHO) endorses clinical grading for trachoma surveys and SAFE strategy for control: Surgery for trachomatous trichiasis (TT), Antibiotics to treat infection and Facial cleanliness and Environmental changes to stop transmission. Method: Trachoma control guidelines and practices were reviewed. Between 2004 and 2010, interventions were conducted in administrative districts. In 2010, Kenya initiated surveys and interventions in areas (trachoma districts) with 100,000 – 200,000 people each to standardise the intervention units. Later, the WHO recommended impact assessments to be conducted in areas with 100,000-250,000 each. SAFE is implemented where baseline prevalence of active trachoma in children 1-9 years old is >10%. The lower age limit for surveys and monitoring of TT surgical services varies in different countries. Surgical services are justified where baseline prevalence of TT in persons aged 15+ years old is ≤1%. In 2014, the Global Trachoma Mapping Project (GTMP) introduced new guidelines where TT surveys participants are to be recruited exclusively in households sampled for active trachoma survey. Results: District-based project planning is convenient due to existing administrative structures but trachoma is more of a “community disease” than a “district level disease”. As a result, non-endemic communities in large meso-endemic districts (population >200,000 people) were included in mass drug administration (MDA). Also, “hot-spots” in large hypo-endemic districts missed due to widely scattered survey clusters. This triggered the adoption of a new in survey method in 2010. Microbiology tests to verify presence of chlamydial infection and assess drug resistance are not done due to cost and logistics. Prevalence of TT in persons aged 15+ years is usually low and survey sample sizes are big. Researchers adjust TT survey age limit and precision to suit available funds. The GTMP method is convenient but may under-estimate the prevalence since adults with children aged 1-9 years are relatively young while the prevalence increases with advancing age. Results from different surveys will not be directly comparable since the GTMP does not specify the sample size and precision for TT surveys. Moreover, GTM puts emphasis is on SA. Kenya prefers comprehensive surveys to assessment all the components of SAFE. In the last decade, FE components have been perpetually under-funded. Conclusions: Trachoma policy reviews are influenced by evidence, economic considerations and convenience. FE and trachoma microbiology are vital but ignored. Global trachoma policies should be adopted to

33
accommodate national programme needs.
NTD8-W1
Socio-cultural determinants to adoption of safe water, sanitation and hygiene practices in Agoro west location, central Nyakach division in Kisumu county Job Wasonga CARE International in Kenya, Project Manager-SWS Off ring road, P. O. Box 88-40100, Kisumu. www.care.or.ke<http://www.care.or.ke> +254 057 2020310 c: +254 722 901 434 | f: +254 057 2024474 Provision of safe water, adequate sanitation and hygiene (WASH) has been lauded as one way of preventing diarrhoeal infections, controlling helminthes infestation and improving health especially in developing countries. However, lack of safe water, inadequate sanitation and poor hygiene practices in most parts of rural Kenya, has continued to be a challenge contributing to high disease morbidity and mortality. In this regard, many Non-Governmental Organizations and governmental agencies have tried to provide water, sanitation and hygiene services. It is with this realization that the government of Kenya together with other Non-Governmental Organizations introduced sustaining and scaling school water, sanitation and hygiene plus community impact (SWASH+) programme as an intervention to mitigate diarrhoeal infections and deaths. However, such interventions often fail to achieve the intended results due to poor understanding of the socio-cultural environment where they are implemented. This study therefore endeavored to find out socio-cultural factor which determine WASH practices among the Luo of Nyakach. The study applied both qualitative and quantitative methodologies to gather information. The study found that factors such as gender roles, norms, religious and traditional belief systems were constraining adoption of safe water, sanitation and hygiene practices. In this case, there is need for agencies to take into consideration such factors when developing and implementing WASH interventions.
NTD8-
W3 Relation of Water contact and Sanitation trends to Schistosoma mansoni infection rates over the course of a four-year MDA project in Western Kenya Michael Ogutu1, Martin Omedo1, Isaac Onkanga1, Musuva Rosemary1, Awiti Alphonce1 Andiego Kennedy1, Diana Karanja1, Susan P. Montgomery2, W. Evan Secor2, Pauline N.Mwinzi1
1. Neglected Tropical Diseases Branch, Center for Global Health Research, Kenya Medical Research Institute (KEMRI), Kisumu, Kenya; 2.

34
Division of Parasitic Diseases and Malaria, Centers for Disease Control and Prevention, Atlanta, Georgia.
Background: Schistosomiasis infection is linked to water contact and therefore to gain control of schistosomiasis, a successful control program should include safe water, sanitation and hygiene. Hence the aim of this study was to assess the village level water contact behavior and sanitation trends in 75 study villages and their impact on S.mansoni infection rates. Methods: A four-year village level longitudinal survey was conducted through the use of village heads/Community health workers and the village level water contact and sanitation practices collected. These practices were quantified in terms of their frequency (All the times, often, sometimes and never) of use and there after their relationship to infection intensity patterns determined. Results: Frequency of use of the open water sources for bathing and carrying out domestic chores all the times, had a strong positive relationship with the infection intensities over the years (r = 0.64 and 0.77 respectively). In terms of sanitation practices, the mean EPG values, were not linearly related to the respective sanitation practices (r = -0.09 and 0.03). Conclusion: The observed trend in water contact and sanitation practices over the four years suggest that schistosomiasis control programs should include water, sanitation and hygiene programs to effectively gain control of the disease.
NTD8-
W4 Practical action approach in delivery of urban wash projects in Kisumu County Noah Mayieka Partners: Kisumu Urban Apostolate Program (KUAP-Pandipieri), Kisumu County Public Health Office, Kisumu County Department of Environment Back ground: Practical Action is an international development agency working with the poor communities to help them choose and use technology to improve their lives for today and generations to come. Our program work is organized under four themes: Universal access to Energy,Urban services (Water, sanitation and waste management), Disaster risk reduction and food security, Climate change and market systems are two cross-cutting themes across our work. In Kisumu County oururban services programme aims to ensure that poor urban dwellers live in healthier and wealthier urban environments. We aim to improve their health, reduce women’s workload and enhance their safety and ultimately reduce morbidity and mortality especially amongst children below 5 years through improved access to safe water, sanitation and waste management. Methods: We work in conjunction with the dwellers of underserved urban

35
settlements with WASH services and their organisations and relevant stakeholders. We achieve this through: (i) Scale up of proven and tested community friendly technologies in safe WASH, Waste management and drainage services (with a special focus on women and children) (ii) support establishment and growth of viable Waste and WATSAN MSEs in informal urban settlements with access to technology and business opportunities (iii) contribute towards formulation and implementation of pro-poor policies in WATSAN and waste management sectors at county and national levels. Expected outcomes: Increased number of WASH and waste management facilities using modern technologies and are gender sensitive (in design and construction) managed by the communities themselves, functional networks of poor people’s Water and Waste organizations operational and influencing policy (Networking to improve policy and practice), increased number of women in MSEs exploiting opportunities in the WATSAN and waste management sector for productivity and incomes in the target regions, increased number of MFI’s providing affordable financing for WATSAN investments. Conclusion: Stronger linkages between local communities/their institutions with County government departments and utility service providers for accountability and increased investment in urban service delivery and market led approaches has great potential in closing the gaps in accessing WASH services by urban dwellers and reduction of costs associated with inadequate access to WASH amenities.
NTD8-W5 WASH and Protection of children against diseases and infection. Enock Oruko Regional WASH Officer World Vision Kenya - Lake Region Mobile No.0722303433
SCIENTIFIC SESSION B: EPIDEMIOLOGY AND OPERATIONAL
RESEARCH
NTD8-B1 KEY NOTE
Mapping, surveillance and control of neglected tropical diseases in Kenya and beyond Simon Brooker Professor of Epidemiology and Wellcome Trust Senior Research Fellow London School of Hygiene & Tropical Medicine The last decade has witnessed increasing commitment to the control and elimination of neglected tropical diseases (NTDs), with an increasing number of countries, including Kenya, launching national NTD control

36
programmes. Efforts to control NTDs reached a turning point in 2012, when WHO launched its NTD Roadmap and partners met in London and pledged to work together to control and eliminate 10 NTDs by 2020. As progress is made towards the goals, there is a need to obtain a detailed understanding of the geographical distributions of NTDs in order to target interventions and facilitate resource allocation. There is also a need to reliably track changes in levels of infection and identify areas where effective control is likely to be most difficult to achieve. These requirements necessitate detailed information on the geographical distribution of NTDs and reliable tools to monitor infection over time. In this talk, I will present work that seeks to define the distribution and burden of NTDs from country to global scales. Using the example of soil-transmitted helminths, I will present a framework that evaluates the feasibility of interrupting transmission and identifies the factors associated with effective STH control. Finally, I will evaluate the most cost-effective approach to the monitoring and surveillance of changes in NTD transmission. The work is conducted as part of the Global Atlas of Helminth Infection project (www.thiswormyworld.org).
NTD8-B23-P Successful targeting and cost effectiveness through school-based mass
drug administration
Alex Mutua, Claire Gware Chore
Evidence Action, NSBDP The mainstream development model proposes that, through targeting, resources are allocated to the poorest and neediest populations. Targeted mass drug administration (MDA) programmes have been successful in the control and elimination of various neglected tropical diseases (NTDs), including soil-transmitted helminths (STH) and schistosomiasis (SCH).
However, the invisibility of those affected by NTDs brought on by disease-associated stigma hinders them from receiving their allocation. Although advocates of targeting state that individuals in the lowest wealth bracket benefit from the greatest returns from targeted interventions, they battle against a dissenting school of thought promoting universalism, which emphasizes comprehensive and equitable availability of social services to all citizens.
Universalists argue that targeting is expensive, is inefficient at capturing the correct populations, can result in the stigmatization of beneficiaries leading to low uptake of interventions. Although there are a number of NTD
37
treatment programmes that administer MDA, few have been able to provide successful targeting, achieve high coverage, and remain cost-effective.
The National School-Based Deworming Programme (NSBDP) in Kenya is a successfully implemented, highly targeted, scaled MDA programme. Through careful parasitological surveying and analysis conducted in collaboration with the Kenya Medical Research Institute and the London School of Hygiene and Tropical Medicine, NSBDP ensures that all schools in eligible locations are targeted for treatment for STH (and SCH if necessary). In Years 1 and 2 of implementation, the programme dewormed 5.9 million children in over 10,000 schools and 6.4 million children in nearly 16,000 schools, respectively. Providing deworming tablets to children through schools not only results in high coverage because children are reached where they are – at schools – but also remains as a cost-effective strategy (less than $.50 per child) due to the readily available, extensive and sustained educational infrastructure.
The NSBDP therefore provides useful lessons for delivering impactful, targeted, cost-effective strategies that intend to contribute to the control and elimination of NTDs.
NTD8-B7 Task shifting for eye care in eastern Africa: General Nurses as trichiasis surgeons in Kenya, Malawi, and Tanzania Michael Gichangi1 Khumbo Kalua2-3 Ernest Barassa1 Edson Eliah4 Susan Lewallen4-5Paul Courtright4-5*
1 Ministry of Health, Kenya; 2 Departments of Ophthalmology, University
of Malawi, College of Medicine, Blantyre, Malawi 3 Blantyre Institute for Community Ophthalmology, Lions Sight First Eye
Hospital, Blantyre, Malawi; 4 Kilimanjaro Centre for Community Ophthalmology Tanzania, PO Box 2265, Moshi, Tanzania
5 Kilimanjaro Centre for Community Ophthalmology International, Division of Ophthalmology, University of Cape Town, South Africa
*Corresponding Author: Paul Courtright ([email protected]) Purpose: There are approximately 8 million people with trachomatous trichiasis globally; in the year 2009, less than 400,000 people had surgery. These numbers are too low in order to achieve the goal of elimination of blinding trachoma by the year 2020. Task shifting approaches have led to the training of general nurses in trichiasis surgery in eastern Africa. The overall aim of this study was to determine the attrition and productivity (and the factors associated with productivity) of trichiasis surgeons in Kenya, Tanzania and Malawi. Methods: A 3-year cohort study of trichiasis surgeons Results: The overall response rate was 86%. Defining high productivity as 50+ operations per year per surgeon, only 16.1% of the trichiasis surgeons

38
were highly productive. Among the surgeons, 27.9% were no longer at their site and ceased providing surgery (attrition) over the three years of study. High productivity was associated with having been trained by an experienced trainer, supervised by a clinical officer, having more than 3 surgical sets, and having an outreach programme. Conclusion: The attrition of general nurses trained in trichiasis surgery was high. Surgical productivity of trichiasis surgeons remains too low. It is likely that other approaches are needed to address the burden of trichiasis in the three countries. In terms of recommendations, training of trichiasis surgeons should be done in a “package”, including a plan for provision of surgical equipment, continuous support and supervision, and outreach.
NTD8-B9 Countdown to Trachoma Elimination in Kenya Ernest Barasa Wanyama National Trachoma Coordinator Email: [email protected] Ophthalmic Services Unit, Ministry of Health, P.O Box 43319-00100, Nairobi.
Introduction: Vision 2020: The Right to Sight is a global initiative to eliminate avoidable Blindness by the year 2020. The Alliance for the Global Elimination of Blinding Trachoma by 2020 (GET 2020) supports and collaborates with the World Health Organization (WHO) to carry out essential activities such as; Epidemiological assessment, including rapid assessment and mapping, project implementation, coordination, monitoring, disease surveillance, project evaluation and resource mobilization. As we count down towards the year 2020, Kenya is bracing herself in the last phase of Trachoma elimination. Purpose: The purpose of this presentation is to share on the milestones of the Kenya Trachoma elimination programme highlighting its achievements, challenges and forecast. Methods: A programme desk review for the last twelve years from 2002- 2014. Programme highlights: The National Trachoma Task Force suspected 18 out of 72 districts to be trachoma endemic in 2002 based on previous research, risk factors and desk review of eye care reports. The suspected districts were 39 sub-counties by 2009. All the 39 sub-counties had been surveyed by 2012. Four sub-counties of Garissa County have recently been suspected and will be surveyed in early 2015. Sub-district level surveys are planned in areas with TF prevalence of 5 to < 10% at baseline. A total 23,317, surgeries have been carried out between 2004 and October 2014 leaving a total backlog of 34,712 persons requiring

39
immediate surgery. Out of a target of 13,952,274 treatments with Zithromax and 1% TEO, 11, 083,382 treatments have been administered between 2007 and 2014 representing an overall National coverage of 79.44%. Construction of dams, sinking of boreholes, installation of water storage tanks, piping and protected springs have been carried out in endemic Counties. Construction of demonstration pit latrines and CLTS activities are and will be carried out in the next five years. Behaviour change Communication activities will be carried out by the MOH and a battery of partners including the Queen Elizabeth Diamond Jubilee Trust, Sight Savers, the Fred Hollows Foundation, Operation Eyesight, Christian Blind Mission, AMREF, Lions Clubs, Spanish Doctors and the WASH sector in Kenya. Conclusions: Coordinated partnerships for SAFE interventions will enable Kenya to achieve elimination of blinding Trachoma by the year 2020.
NTD8-B10
Eliminating human dog-mediated rabies in Kenya Thumbi SM1, 2, Ogola E2, Osoro E3, Bitek A3
1Paul G. Allen School for Global Animal Health, Washington State University 2Center for Global Health Research, Kenya Medical Research Institute 3Zoonotic Disease Unit, Ministry of Health & Ministry of Agriculture, Livestock and Fisheries Rabies has been endemic in Kenya since the first case was reported in a dog in 1912, and in human in 1928. Domestic dogs are the principal reservoir of the rabies virus and the source of infection for at least 98% of human rabies cases. To-date, rabies is estimated to cause up to 2000 deaths every year in Kenya, most of these occurring among poor rural communities and in children below 15 years of age. Here we provide data to dispel three misconceptions about rabies that have encouraged inaction; rabies is a low priority public health problem, stray dogs are the main drivers for rabies transmission, and rabies is impossible to control without controlling it in wildlife. Encouraged by success in dog rabies elimination in countries like Malaysia, Philippines, Kenya has launched a strategy for the elimination of human dog-mediated rabies by the year 2030. This strategy provides a guide for the systematic reduction of the risk of rabies through sustained mass dog vaccinations, pre and post-exposure prophylaxis and public education until the country is completely free of human dog-mediated rabies. The strategy is based on a six stage (stage 0 to 5) Stepwise Approach (SA) that proposes a graduated progression towards becoming a rabies-free country. Each stage has a set of activities and targets that must be reached and confirmed before moving to the next stage, and that build on each other to continuously reduce the risk of disease. The rabies elimination activities will be first conducted in pilot areas (Makueni-Machakos, Kitui, Kisumu and Siaya
40
counties) selected based on the current burden of rabies disease, availability of natural barriers to aid elimination efforts, before the elimination campaign is rolled-out to the rest of the country. The success of this elimination campaign is hoped to stir action in neighbouring countries, and the rest of Africa, and demonstrate the utility of the One-Health approach of close collaboration between human and animal health sectors in reducing the threat of zoonotic and emerging infectious diseases.
NTD8-B2 Schistosomamansoni and Biomphalariapfeiffericompatibility studies and implications for schistosomiasis control in Kenya Martin W Mutuku1, Celestine K Dweni1, Joseph M Kinuthia1, Moses Mwangi2, Ibrahim N Mwangi1, Geoffrey M Maina1, Lelo E Agola1, Si-Ming Zhang4, Rosebella Maranga3 , Eric S Loker4, Gerald M Mkoji1
1. Centre for Biotechnology Research and Development, Kenya Medical Research Institute, P.O Box 54840-00200, Nairobi, Kenya.
2. Centre for Public Health Research, Kenya Medical Research Institute, P.O Box 20752-00200, Nairobi, Kenya
3. Department of Zoology, Jomo Kenyatta University of Agriculture and Technology, P.O Box 62000-00200, Nairobi, Kenya
4. Center for Evolutionary and Theoretical Immunology, Department of Biology, and Parasitology Division, Museum of Southwestern Biology, University of New Mexico, Albuquerque U.S.A. 87131
Background: Schistosomamansoni is widely distributed in sub-Saharan Africa with Biomphalaria pfeifferi being its most widespread and important snail intermediate host. Few studies have examined the compatibility of field-derived B. pfeifferi snails with S. mansoni miracidia derived from human hosts. Compatibility of two isolates of S. mansoni from school children from Nyakach and Mweawith B. pfeifferi collected directly from Asao stream in Nyakach was investigated. Methods: Snails were exposed to four different doses of miracidia (1, 5, 10 and 25) from sympatric or allopatric S. mansoni, and maintained in a shaded, screened out-of-doors rearing facility. Both snail survival and the number of snails that became infected were monitored weekly. Results: Both sympatric and allopatric combinations of parasites and snails exhibited high compatibility (approximately 50% at a dose of one miracidium per snail), with an increase in infection rates as the miracidial dose was increased (P<0.002). Snail mortality increased significantly with dose of miracidia (P<0.05). Three percent of snails exposed to a low dose of sympatric miracidia (1 or 5) continued to shed cercariae for as long as 58 weeks post exposure. Conclusions: There were no significant local adaptation effects between schistosomes and snails. The existence of “super-survivor” snails is

41
noteworthy for its implications for current control initiatives that mostly rely on mass drug administration (MDA). Long-term shedders could provide an ongoing source of cercariae to initiate human infections for many months, suggesting care is required in considering how human MDA treatments are timed and how long MDA is sustained. Future control programs should incorporate means to eliminate infected snails This study was supported by NIH grant AI101438 and a Gates Grand Challenges Award.
NTD8-B3 Determination of prevalence and risk factors associated with intestinal schistosomiasis and helminth infections among adults living in Mwea West district, Kirinyaga County, Central Kenya. Masaku Janet 1
Conclusion/Discussion: There was high prevalence of S.mansoni among adults living in the area, with gender and education being the noted risk
*, Faith Mutungi1, Gichuki Paul1, Okoyo Collins1and Njenga
Sammy1
1Eastern and Southern Africa Centre of International Parasite Control (ESACIPAC) Kenya Medical Research Institute (KEMRI), P.O Box 54840 – 00200 Nairobi. Background: Schistosomiasis and soil-transmitted helminthiasis are common human parasitic diseases in many parts of the developing world. These infections are a major public health problem in Kenya as well as many other tropical countries. High and repeated exposure to parasite infections is as a result of multiple inter-related risk factors. Recently, much of research work on these parasitic infections in Kenya has focused on school going children. However, there is scanty information about adults living in the communities who could harbor the parasites and cause failure to the ongoing school control programmes. The current study determined prevalence and the risk factors associated with intestinal schistosomiasis and helminth infections among adults living in Mwea irrigation scheme, central Kenya, where rice farming is done through irrigation. Methods: The study was a descriptive cross-sectional study which utilized quantitative and qualitative methods of data collection. A total of 501 adults aged between 17-65 years, were recruited as study participants from four villages namely Mukou, Mianya A, Mianya B and Mbui Njeru. Results/Findings: There was very low infection of STHs species with Hookworm being the only species present, with a prevalence of 0.2% (95%CI: 0-1.4).The overall prevalence of S. mansoni was 33.1% (95%CI: 29.3-37.5) with mean intensity of 130 epg (95%CI: 88-192). Generally, there was suggestive evidence of association between gender and S. mansoni infection, p = 0.05. There was also significant association between level of education and S. mansoni infection, p = 0.012.
42
factors. STHs infections were found to be negligible. The study recommends the need to consider mass treatment of the community members as they could act as reservoirs of S. mansoni for the school going children and hinder the national control program. Key words: Schistostomiasis: S. mansoni: Prevalence: Intensity: Infection: Risk factors: Control. *Masaku Janet: [email protected]: 0721635554: +254.20.2731194
NTD8 –B4
The evaluation of jigger infestations among populations of rural villages of bumula and Kimilili sub counties, Bungoma county Gabriel W. Muyiemba Medical parasitologist Vector Diseases Control Unit (VBDCU) Kimilili Field Station Background: Jigger infestation is among the Neglected tropical diseases (NTDs) that are major public health problems in developing countries where they contribute to suffering of populations living in poor settings. As part of the research project in Bungoma County, a baseline cross sectional survey was conducted in 8 villages each for Bumula and Kimilili Sub Counties to provide information on the status of jigger infestations. This paper presents the result of a parasitological investigation among the populations in the study villages. Methods: A questionnaire was administered to understand the living conditions, with details on risk factors and other variables being captured. The population was assessed for the jigger infestations among 1607 households, 16 schools and 8 churches. Results: The study revealed high prevalence of jigger infestation 71.7% of those infested are school going children. 201 persons had high morbidity manifesting as inflammations, ulcerations, auto amputation of digits, deformation and loss of nails, formation of fissures and ulcers, gangrene, walking difficulties and secondary infections. 7.1% of school going children had dropped out of school due to the infestation. There were no policy mechanisms and guidelines or timelines that were in place to help eradicate the jigger menace. No monitoring and evaluation programmes were being implemented on the ground. Conclusion: In the current study jigger infestation has been identified as an important infestation among the population in the sub counties. Thus the population has been left untreated and remain an important potential reservoir for source of re-infestation. Therefore, we appeal to any interested partner to join and support our novel design strategies for preventive and chemotherapy interventions in an effort to reduce the force of infestation among the communities in the nine sub counties of Bungoma County.
43
NTD8 –B5
Exposures to chikungunya and dengue viruses in two coastal and western Kenyan sites Bryson Ndenga1, Francis Mutuku2, Sandra Musaki1, Emily Chinyavu2, Joan Shiroko1, Dunstan Mukoko2, John Vulule1, Charles King3, Angelle Desiree LaBeaud 1. Center for Global Health Research, Kenya Medical Research Institute, Kisumu, Kenya 2. Division of Vector Borne & Neglected Diseases, Ministry of Health, Nairobi, Kenya 3. Center for Global Health and Diseases, Case Western Reserve University, Cleveland, Ohio,USA 4. Center for Immunobiology and Vaccine Development, Children’s Hospital Oakland Research Institute, Oakland, California, USA Background: Febrile cases are common among children in western and coastal Kenya. In most instances, these febrile cases are assumed to be due to malaria infections. Rarely do medical service providers suspect chikungunya (CHIKV) and/or dengue (DENV) viruses to be the cause. An ongoing study aims to determine the burden of CHIKV and DENV transmission, infection and disease in Kenya. Methods: Healthy Community Cohort (HCC) and Acutely ill Cohort (AIC) studies on children aged between 2 – 17 years old are being conducted in rural and urban sites both in western and coastal Kenyan sites. Blood samples were collected and tested for IgG by ELISA to determine exposures to CHIKV and DENV and also for malaria parasites by microscopy. Results: Exposures to both CHIKV and DENV have been identified both in the western and coastal Kenyan sites. These exposures are either to chikungunya and dengue virus alone or to both and were found both in rural and urban sites. Malaria parasite prevalence in the communities was 15 - 38% and was mostly (86 - 96%) due to Plasmodium falciparum. 40 - 70% of febrile cases in the hospitals had malaria parasites. However, 30 - 60% of the fevers were due to other causes, which includes CHIKV and DENV. Conclusion: Exposures to CHIKV and DENV have been identified in western and coastal Kenyan sites. There is high possibility of on-going local transmission of these diseases; hence the need to suspect them especially in non-malaria fevers. Currently, vector control is the only method to prevent CHIKV and DENV transmission. Keyword: Exposures, chikungunya, dengue, malaria
NTD8 –B8
The Economic Impact Of Visceral Leishmaniasis In Baringo, Kenya Simon Bolo1, Hilda Omae2, Monique Wasunna1,3
1. Drugs for Neglected Diseases initiative (DNDi)

44
2. Strathmore Business School 3. Kenya Medical Research Institute
Introduction / Background: Visceral Leishmaniasis (VL) is a deadly parasitic disease transmitted by the bite of a female sandfly. According to the World Health Organization, VL is ranked as the third most important parasitic disease after malaria and lymphatic filariasis in terms of disease burden (Desjeux 2004; WHO 2009). The main objective of the study was to examine the economic impact of VL on households (HHs) in Baringo County, Kenya. Methods: A random sample of 84 out of 108 VL patients was calculated using the Creative Research Online sample calculator. Questionnaires were used to collect data from 30 HHs and analyzed using descriptive methods. Results/Findings: A single VL episode costs Kshs. 31,200 (USD.390, at exchange rate of 80) which is triple the average monthly income for the affected HHs or 1.6 times their annual per capita income. These costs are beyond the reach of majority poor HHs, 70% living in the first two poorest quintiles, and they are forced to employ a combination of coping strategies. In most cases, patients could still not meet the cost of treatment even after exhausting available coping strategies. Comparisons of cost lines indicate that short-term direct costs outweigh short-term indirect costs. We concluded that the economic burden of caring for VL patients and the subsequent stripping and compromise of coping mechanisms can institute a vicious cycle of poverty in a household and may undermine sustainable development of disease endemic communities Conclusions / Discussion: We recommended that VL disease control programmes need to adopt novel mechanisms to fast track VL patients’ diagnosis and treatment so as not to compromise livelihood and food security of their HHs. The support systems are necessary if the communities have to sustain good health, welfare and development in order to achieve the economic and health aspirations enshrined in the Vision 2030
NTD8-B11 The Impact of Three Rounds of Praziquantel Mass Drug Administration on SchistosomamansoniInfections: A Comparison Between Community Wide Treatment and School-Based Treatment in Western Kenya-The SCORE Project. Isaac Onkanga*, Pauline N. M. MwinziGeoffrey Muchiri, Ryan Wiegand, Kennedy Andiego, Alphonce Awiti, Michael Ogutu, Rosemary Musuva, Martin Omedo, W. Evan Secorand Susan P. Montgomery Center for Global Health Research, Kenya Medical Research Institute, Kisumu, Kenya; Division of Parasitic Diseases and Malaria, Centers for Disease Control and Prevention, Atlanta, Georgia
Abstract Introduction:Mass drug administration (MDA) is the cornerstone of

45
schistosomiasis control in highly endemic areas in sub-Saharan Africa. The World Health Organization (WHO) recommends either school-based treatment (SBT) or community-wide treatment (CWT)approachesbe employed in MDA delivery.However, in most endemic areas and particularly in Kenya, comparison studies of SBT and CWT approaches on parasitological outcomeshave not been performed. In an ongoing Schistosomiasis Consortium for Operational Research and Evaluation(SCORE) study covering 150 villages in western Kenya, we performed cross-sectional surveys to evaluateand compare the effect of CWT and SBTapproaches on Schistosomamansoniinfection prevalence and intensity levels among school-age children at baseline and after three rounds of MDA. Methods:In 75 villages, community health workers administered treatments using the CWT approach, while schoolteachersadministered treatment in 75 other villages using the SBT approach. In each survey, a total of 100 children aged 9-12 years old were surveyed in each CWT and SBT village, each providing three consecutive stool samples. Two slides per stool sample were screened for S. mansoni eggs using the Kato Katz method. All data analyses were performed using SPSS software. Results:Baseline S. mansoni prevalence and intensity levels in the SBT approach were 63% and 89.9eggs per gram (epg) and in the CWT approach were 60% and 88.5 epg. Following three rounds of treatment,respective prevalence and intensity levels in the SBT reduced to 33% and 33. 4 epg while in the CWT approach reduced to 38% and 46.5epg. Following treatment, both approaches recorded significant reductions in both prevalence and intensity levels, P<0.001. Comparisons of SBT and CWT prevalence and intensity levels at baseline and at three rounds of treatment did not show any significant differencesbetween the two approaches. Conclusion:In this study, the CWT approach was as effective as the SBT approach in reducing prevalence and intensity of schistosomiasis, suggesting that both approaches can be employed as alternative strategies in MDA delivery.
SCIENTIFIC SESSION C: HEALTH BEHAVIORAL STUDIES AND
SOCIAL SCIENCE
KEY NOTE
Applying a socio-ecological framework towards research and interventions for neglected tropical diseases. Prof Joyce Olenja School of Public Health, College of Health Sciences at the University of Nairobi

46
Neglected Tropical Diseases (NTDs) are a major burden to poor and marginalised populations in predominantly poor resource settings of the developing world. NTDs not only impair the physical and intellectual capacities of affected persons but also perpetuate the circle of poverty, negatively affect socio-economic development and health outcomes. Within the context of global health initiatives, there is a growing momentum to control and eliminate NTDs. In spite of the milestones achieved, there remain challenges that include limited understanding of the contextual factors underlying the disease burden. Research in NTDs is heavily guided by the biomedical paradigm and much less attention paid to the social context and vulnerability. Examining the role of the social environment and analysis of the political economy of health that reflects the realities of external influence is critical. NTDs elimination programmes tend to focus on short term treatment at the expense of prevention efforts and broader community engagement. Interventions in NTDs beg for trans-disciplinary approaches that are integrative and foster the understanding of social, ecological and environmental determinants of NTDs. This paper explores the relevance of the socio- ecological model with the aim of broadening the framework for understanding the contextual factors underlying the cause, prevention and spread of NTDs. In particular, the paper highlights key elements of vulnerability within the social environment of communities that invariably exacerbate the burden NTDs. It advocates for appropriate interventions for elimination of NTDs that are informed by implementation science research that takes into account the lived experience of communities affected by these diseases.
NTD7-C1
The Influence of Social Support on the Utilization of Health Care Services by Patients with Chronic Lymphatic Filariasis in Goshi location, Malindi Sub-County, Kenya Murithi David [1], Ng'ang'a Zipporah [1], Mukoko Dunstan [2], Njomo Doris W [3] [1] Jomo Kenyatta University of Agriculture and Technology [2] Ministry of Health, Division of Vector Borne Diseases, Kenya [3] Kenya Medical Research Institute (KEMRI), Background: Lymphatic filariasis (LF) caused by filarial worms and transmitted by mosquitoes is ranked as the second largest cause of disability in the world. Infection leads to clinical manifestations; lymphoedema of limbs and genitalia and elephantiasis. The disease causes considerable morbidity to affected individuals with consequent loss of income and social and psychological stress. To determine the influence of social support on the utilization of healthcare services by patients with chronic clinical signs of LF, a cross-sectional study was conducted in Goshi location, Malindi Sub-County, Kenya.
47
Methods: A total of 220 patients with chronic (LF) were purposively selected and interviewer-based questionnaires administered to them for quantitative data. Four focus group discussions with single sex adult and youth groups and 16 key informant interviews with purposively selected opinion leaders were conducted for qualitative data. The quantitative data was analyzed by SPSS version 16 and the qualitative data manually by study themes. Results: Encouragement received by patients from family and friends was significantly associated with health care services utilization (P<0.001). Most (68.2%) of patients who received such encouragement compared to 31.8% who did not, utilized health care services. Similarly, receiving encouragement from other patients with chronic LF was significantly associated with frequency of visiting health care facilities (P<0.001). Majority (81.8%) of respondents who received encouragement from fellow patients compared to 18.2% who did not, visited the health facility more frequently. Feeling of being a burden to the family was significantly associated with utilization of health care services (P<0.05). More than one half (57.1%) of those who felt that they were a burden to their family compared to 42.9% who did not, utilized health care services. Being affiliated to a support group was also significantly associated with utilization of health care services (P<0.001). Most (85.7%) of respondents who indicated that they were affiliated to a support group compared to 14.3% who were not, utilized health care services. Conclusion: Patients with chronic LF require encouragement from community members and fellow patients to remove the feeling of rejection and to seek health care services. Being a member of a support groups is an important contributor of increased health care services utilization and authorities should support patients to form such groups. Key words: social support, health care services, chronic lymphatic filariasis
NTD8-C2
Evaluating treatment coverage for schistosomiasis control in western Kenya: analysis of the survey design Omedo OM1, Ogutu M1, Onkanga I1, Musuva R1, Andiego K1, Awiti A1, Montgomery SP2, Secor WE2 and Mwinzi P1
1 Neglected Tropical Diseases Branch, Center for Global Health Research, Kenya Medical Research Institute, Kisumu, Kenya 2 Divisions of Parasitic Diseases and Malaria, Centers for Disease Control and Prevention, Atlanta, Georgia, USA Introduction: Monitoring mass drug administration (MDA) treatment coverage is very important for determining whether an interventionhas achieved the recommended optimal coverage. Currently, the commonly used tool to
48
monitor the coverage is household surveys (HHS), however, this method is very expensive and requires technical expertise in both design and data management.In contrast, the lot quality assurance sampling (LQAS) method, which is simpler and cheaper to conduct, has demonstrated efficacy in monitoring vaccine coveragein the expanded program for immunization (EPI).Nonetheless, little is known of its performance in determiningMDA coverage for schistosomiasis. Hence, this study compared performance of the LQAS method with HHS in identifying low performing areas that requireadditionaltreatment follow up to achieve the optimal coverage. Method: The LQAS and HHS methods were applied in eight and seven villages, respectively. These villages were areas where community health workers were working and were referred to as supervision areas. The performance of LQAS in identifying supervision areas with adequate and inadequate MDA coverage was compared with HHS. Ninety percent and 75% were used as the upper limit and lower limit respectively.Z statistics was used to compare proportions and a misclassification error of less than 10% was allowed. Results: LQAS method was able to identify 6/8 (75%) while HHS was able to identify 6/7 (85.7%) inadequately performing areas.The difference in the proportion of work-areas identified to be inadequately performing using the LQAS method and the HHS was not statistically significant (P Value=0.605). Conclusion:Both LQAS and HHS survey performed equally in identifying inadequately performing areas. LQAS could be used as a less expensive alternative to HHS to monitor MDA coverage.
NTD8-C3
Qualitative Assessment of Drug Delivery Approaches to Pre-primary school age children for Treatment of Soil-transmitted Helminthiasis and Schistosomiasis Infections in Malindi District, Coastal Kenya Gladys Odhiambo1
Introduction: In Kenya, the government through the National School-based deworming programme treats children in Early Childhood Development (ECD) Centres. However, the Programme does not consider the ECD Centres teachers as eligible for training to conduct deworming of the ECD Centre children. The programme therefore requires that ECD children whose centres are not within the primary schools be taken to the nearby primary schools to receive treatment from the trained primary school teachers. This type of ECD centre children therefore have to travel an average of 5km or more to receive
, Nipher Nyamogo3, Faith Mwende2 and Doris Njomo2. 1Center for Global Health Research, Kenya Medical Research Institute, P.O. Box 1578-40100, Kisumu, Kenya; 2Eastern and Southern Africa Centre of International Parasite Control (ESACIPAC) Kenya Medical Research Institute (KEMRI), P.O Box 54840 – 00200 Nairobi. 3Daystar University, P.O. Box 44400 – 00100 Nairobi

49
treatment. This may have negative implications in terms of accessing the nearest school and majority of the ECD Centre children are likely to miss the treatment. This study therefore aimed at developing and implementing an alternative drug delivery method in order to help maximize treatment coverage for this vulnerable age group. Methods: The study adopted a comparative cross-sectional study design. We conducted 64 Key Informant Interviews with Community Health Extension Workers (CHEWs) (16), Primary School Health teachers (12), Early Childhood Development Centre (ECD) Teachers (18) and Community Opinion leaders (18). Purposive sampling technique was used to identify participants and the sample was based on saturation model. Health teachers and CHEWs were trained to treat children in primary schools and standalone ECDs respectively. The data was collected by trained and experienced KEMRI staff, transcribed, coded and analyzed using ATLAS.ti version 6. Results: In our preliminary findings, majority of the participants displayed a strong preference for ECD centre treatment highlighting that the young children should not be subjected to walk long distances for treatment. Abdominal pain was reported as a major side effect among consumers of Praziquantel while no side effects were reported among those who took albendazole alone. ECD teachers were widely used during treatment with children being the main mobilization strategy. Discussion: ECD teachers have the capacity to treat children and all they need is training. To maximize treatment coverage, pre-school children should be treated at their centres and other mobilization techniques should be employed to enhance community participation.
POSTERS
NTD8-A6 Multiplex Serosurveys as a Tool for Integrated Neglected Tropical
Diseases (NTD) Surveillance Sammy Njenga1, Kimberly Won2, Fredrick Rawago3, Henry Kanyi1, Faith Mwende1, Ryan Wiegand2, E. Brook Goodhew2, Jeffrey Priest2, Vitaliano Cama2, Yeuk-Mui Lee2, W. Evan Secor2, Patrick Lammie2, Pauline Mwinzi3 and Maurice Odiere3
1 Kenya Medical Research Institute, ESACIPAC, Nairobi, Kenya, 2
Division of Parasitic Diseases and Malaria, Center for Global Health, Centers for Disease Control and Prevention, Atlanta, GA, USA, 3 Kenya Medical Research Institute, Centre for Global Health Research, Kisumu, Kenya A key strategy for control and elimination of five Neglected Tropical

50
Diseases (NTDs): lymphatic filariasis (LF), onchocerciasis, schistosomiasis, soil-transmitted helminthiasis (STH), and trachoma is preventive chemotherapy (PC) through mass drug administration (MDA). The impact of MDA is usually monitored by parasitological assessments or clinical examination. There is often geographic overlap of NTDs and other diseases, and populations in these areas are regularly exposed to a variety of other diseases. Disease control programs require routine monitoring and evaluation (M&E), but coordinated M&E is rarely conducted and can be a challenge. Antibody-based tests may facilitate integrated M&E. A multiplex bead assay (MBA) that detects antibody against multiple antigens using a single blood sample has been developed. A total of 935 serum samples collected from individuals (1-85 years) living in communities in Mbita district, western Kenya were tested for antibody responses to 36 antigens covering a variety of diseases including all five PC NTDs. This area in western Kenya is highly endemic for Schistosoma mansoni and at variable risk for STH, but is not believed to be at risk for LF, onchocerciasis or trachoma. It is also an area of intense malaria transmission. Antibody responses to two Schistosoma spp. antigens were significantly associated with intensity of S. mansoni infection assessed by stool examination (p<0.001). Although antibody responses to a Plasmodium falciparum antigen were not associated with blood film results, MBA results indicated high levels of infection or exposure to P. falciparum, but very low levels of antibody to P. vivax. Minimal levels of antibodies were detected for LF, trachoma and onchocerciasis. Additionally, antibody responses to tetanus toxoid were low, indicating insufficient coverage of routine vaccinations. Preliminary multiplex results are consistent with traditional measures such as stool examination and indicate the use of MBAs has the potential to provide an integrated platform for M&E in complex public health settings.
NTD8-A7 Molecular characterization of Echinococcus species/strains in humans from Turkana, Kenya Titus Mutwiri1, Japhet Magambo2, Eberhard Zeyhle3, Gerald Mkoji4, NjeriWamae4, Erastus Mulinge4, Cecilia Mbae4, Marion Wassermann5, Peter Kern6, Thomas Romig5
1Kenya Methodist University, School of Medicine and Health Sciences, Kenya 2Meru University of Science and Technology, Meru, Kenya 3Africa Medical Research Foundation, Nairobi, Kenya 4Kenya Medical Research Institute, Nairobi, Kenya 5Parasitology Unit, University of Hohenheim, Stuttgart, Germany 6Center for Internal Medicine, University Hospital, Ulm, Germany Background:Cystic echinococcosis (CE) is a neglected, economically important zoonotic disease affecting pastoralist communities of Turkana
51
and Masaai in Kenya. It is caused by a highly diverse complex “Echinococcus granulosus species”. The CE prevalence in the nomadic or semi-nomadic ethnic groups of the northern Kenya or southern Sudan stands at >5%. A number of well-characterized strains are now recognized and these are adapted to particular life cycle patterns and host assemblages. The E. granulosus spp present in humans in Kenya is not well characterized using molecular tools available. The present study sought to determine the genetic characteristics of Echinococcus taxa from Turkana in Kenya using PCR-RFLP targeting the nad 1 gene. Methodology:Fifty eight (58) archived samples of E. granulosus without biodata of the study subjects and eighty (80) prospective samples from twenty-six (26) subjects with biodata were analyzed by PCR-RFLP for molecular characterization of the E. granulosus. Results:Two strains, E. granulosus G1-G3 and E. canadensis G6/7 were identified with E. granulosus G1-G3 predominating. The liver was the most infected organ, and majority of cysts presented as CE1 and CE3 images according to WHO US classification. There was a positive association between age and cysts classification by ultrasound (p<0.001). All the E. canadensis G6/7 cases presented as single cysts in the infected persons. Conclusion:This study corroborates recent reports on the presence of E. granulosus G6/7 strain in Turkana, contrary to earlier findings that had reported E. granulosus G1-G3 as the only strain infecting human in Turkana. It is envisioned that the results of this study will serve as a model for African countries with similar settings and shed light on the emerging human CE, where the parasite presents a significant burden, as well as, shedding light on the geographical distribution of species that may later influence the control options.
NTD8-W2 Assessment of the relationship between community-led total sanitation and prevalence and intensities of Schistosoma mansoni and soil-transmitted helminths in villages along Lake Victoria, Western Kenya Amos Omondi1, Harrison Korir1, Elizabeth Ochola1, George Ogara1, John Oguso1, Diana M.S Karanja1. Centre for Global Health Research, Kenya Medical Research Institute 1578-40100 Kisumu1. Introduction: Schistosomiasis and soil-transmitted helminths remain major public health concerns in many developing countries. Schistosomiasis infects more than 207 million people worldwide while soil-transmitted helminths cause over two billion infections. Both diseases are often associated with poor sanitation. Kenya introduced Community-
52
led total sanitation and open defecation-free (CLTS/ODF) concepts for rural sanitation in 2007. In 2009, the Ministry of Public Health and Sanitation (MOPHS) formally approved and recommended CLTS as a potential approach for improving sanitation coverage in the country by including it in its national strategy. We assessed the impact of CLTS/ODF communities on prevalence and intensities of schistosomiasis and soil transmitted helminths in school age children in areas with a baseline schistosomiasis prevalence of 10-24% after two rounds of mass drug administration. Methodology: This study was conducted in 13 open defecation-free villages and 13 non-ODF villages along the shores of Lake Victoria within Kisumu West, Nyakach and Rarieda. The prevalence and intensities of schistosomiasis and soil-transmitted helminthes were determined using Kato-Katz on three consecutive stool samples among 9-12 year-old school-going children. The CLTS/ODF status of the villages was provided by public health officers of the Ministry of Public Health and Sanitation, who keeps a record of villages awarded the status. Results: The schistosomiasis prevalence for the non-ODF villages was 14.4% higher than ODF villages at 9.7%. Schistosomiasis intensity for ODF was lower (69 eggs per gram) as compared to non ODF (81 eggs per gram). A similar pattern was observed for two soil transmitted helminths. Prevalence for Trichuris trichiura was 7% in ODF and 8.4% in non ODF and was 3.3% in ODF and 6.8% in non ODF villages for Ascaris lumbricoides. Conclusion: Ending the practice of open defecation can lead to a reduction in the prevalence and intensities of Schistosomiasis and soil-transmitted helminthiases enhancing ongoing MDA control interventions.
NTD8–W6 Correlation between water source and schistosomiasis prevalence in schools in western Kenya Agollah W1, Musuva R1
, Ogutu M1, Onkanga I1, Omedo OM1 ,Andiego K1,
Awiti A1, Montgomery SP2, Evan SW2 and Mwinzi P1
1 Neglected Tropical Diseases Branch, Center for Global Health Research, Kenya Medical Research Institute, Kisumu, Kenya 2 Divisions of Parasitic Diseases and Malaria, Centers for Disease Control and Prevention, Atlanta, Georgia Introduction: Considerable studies have examined the effect of water, sanitary practices and hygiene (WASH) on reducing diarrhea prevalence and cholera in school-age children. However, limited research has been done to evaluate their link in controlling schistosomiasis. This study seeks to highlight the close relationship between water, sanitation and schistosomiasis prevalence in rural primary schools. Methods: A longitudinal survey was conducted in 75 schools along the

53
shores of Lake Victoria over a period of 4 years. School level water and sanitation data was collected from the school heads annually. S. mansoni prevalence was determined by collecting three consecutive stool samples from the children. The relationship between these two aspects was then determined using pearson correlation. Results: There was a marked positive relationship between schistosomiasis prevalence and reliance on use of borehole water (r = 0.8). There was a strong negative correlation between prevalence and use of tap water (r = -0.8), the same direction relationship effect though moderate was observed with the use of rainwater (r = -0.5) while there was a weak positive association between use of Lake water and S. mansoni prevalence (r = 0.2). Conclusion: The strong association that exists between poor sanitation and increased S. mansoni prevalence necessitates the need for integrating WASH intervention into the control strategies for achieving sustained control, elimination, or eradication of schistosomiasis and other neglected tropical diseases (NTDs).
NTD8-B1 Schistosomiasis and Intestinal helminthiasis: Implication on nutritional status of Pre-school children in communities along Ogun River in Abeokuta, Ogun State, Nigeria Adebiyi A. Adeniran1*, Mogaji, Hammed.O.1, Oluwole, Akinola.S. 1, Abe, Eniola.M.2, Alabi, Oladimeji.M. 1, Olabinke, Dorcas.B.1, Aladesida, A.A.3, Olayiwola, I.O.4 and Ekpo, U.F.1
1 Spatial Parasitology and Health GIS Group, Department of Biological Sciences, Federal University of Agriculture, Abeokuta 2Department of Zoology, Federal University Lafia, Nassarawa 3Department of Biological Sciences, Federal University of Agriculture, Abeokuta 4Nutrition and Dietetics Department, Federal University of Agriculture, Abeokuta *Corresponding and presenting author: [email protected] , +2347061140496 Information on concurrent infections and effect on nutritional status of schistosomiasis and intestinal helminthiasis in preschool-aged children (PSAC) is scanty. A cross-sectional study was conducted in 5 randomly selected communities along Ogun River in Abeokuta. Ethical clearance was obtained from Ethical committee of Federal Medical Centre, Abeokuta. Urine and faecal samples were collected from 167 consented PSAC according to standard procedures. Urine samples were examined using sedimentation technique. Faecal samples were examined using sodium-acetate acetic-acid formalin ether concentration method. Nutritional status were assessed using anthropometry and computing height-for-age Z-scores (HAZ); weight-for-age Z-scores (WAZ); weight-for-height Z-scores (WHZ) and Body-mass-index-for-age Z-scores (BAZ) using 2006 WHO international growth standard. Data were analysed using
54
IBM SPSS version 20.0. Of the total 167 PSAC, 6(3.6%) and 8(4.8%) were infected with urinary and intestinal schistosomiasis, respectively. There was no significant difference across sex and age. Prevalence of Ascaris lumbricoides was 48.5%; hookworm 37.7%, Trichuris trichiura 5.4% and Taenia spp 50.3%. There was significant difference (p<0.05) in prevalence by age for T. trichiura and Taenia spp. There were no significant differences in infection by sex for all helminths infection. Prevalence of co-infection with schistosomiasis and intestinal helminths was 6%. Intensity of infection with A. lumbricoides was higher in males than females (1.66±0.15 versus 1.64±0.15epg). However, females had higher intensity of hookworm and Taenia spp infections than the males (1.44±0.11epg versus 1.28±0.14epg for hookworm) and (1.22±0.10epg versus 1.01±0.09epg for Taenia spp). Nutritional analysis revealed 46.7% of PSAC were malnourished with 39.5% stunted, 22.8% underweight, 12.3% wasted and 6.9% thin. No significant difference was observed in nutritional status between infected and uninfected PSAC. Although, effect on nutrition was not significant; association was established between infection and malnutrition and if not dealt with earlier, may eventually contribute to higher susceptibility to diseases and reduced school attendance.
NTD8-B6 Single versus mixed Schistosoma haematobium and Schistosoma mansoni
infections among school-going adolescent girls in south Nyanza, western Kenya: A link for high HIV prevalence?
Huldah C. Sang, Geoffrey Muchiri, Maurice R. Odiere and Pauline N.M. Mwinzi.
Neglected Tropical Diseases Unit, Center for Global Health Research, Kenya Medical Research Institute, P.O. Box 1578-40100, Kisumu Kenya
Abstract Background: Multiple parasite infections are believed to increase susceptibility to coinfection with other parasites, playing a vital role in the development of morbidity and clinical expression. In Kenya, one largely unexplored question is female genital schistosomiasis associated with chronic S. haematobium infection and its effects, partly due to paucity of information on schistosomiasis among females in the endemic regions. In western Kenya for instance, a region predominantly known for intestinal schistosomiasis, empirical evidence on urinary schistosomiasis has only began to emerge. Methods: This cross-sectional survey determined the prevalence and infection intensity of single versus mixed Schistosoma haematobium and Schistosoma mansoni infection among 1,614 school-going girls aged 7-17 years in 95 primary schools in south Nyanza, western Kenya. Prevalence of STHs (Ascaris lumbricoides and Trichuris trichiura) was also quantified. Hematuria was used as a proxy indicator for S. haematobium. Helminth eggs were analyzed from single urine (for S. haematobium) and stool (for S. mansoni and STHs) samples by centrifugation and Kato-Katz, respectively. Schistosome eggs were quantified whereas STH infection was noted as either presence or absence. Results: Overall infection prevalence of S. haematobium was 7.8% (95% CI = 6.6-9.2% and 20.9 eggs/10ml), S. mansoni 13.1% (95% CI = 11.5-14.8% and
55
164.9 epg), A. lumbricoides 5.3% (95% CI =4.3-6.5%) and T. trichiura 3% (95% CI =2.2-3.9%). Hematuria was associated with S. haematobium infection P<0.0001. Interestingly, out of the 126 S. haematobium-infected girls, the mean intensity was higher 25.6 epg (95% CI = 10.3-41 epg) in 12.7% girls who were co-infected with S. mansoni compared to a mean of 20.2 epg (95% CI = 13.45-26.95 epg) seen in 87.3% girls with only S. haematobium infection. These differences were however statistically insignificant. On the other hand, out of the 211 S. mansoni infected girls, mean infection intensity was lower 87.8 epg (95% CI = 48.6-127.1 epg) in 7.6% girls who were co-infected with S. haematobium compared to a mean of 171.3 epg (95% CI = 135.9-206.7 epg) in 92.4% girls with only S. mansoni infection. These differences were also insignificant. No association existed between S. haematobium and S. mansoni infection and vice versa. Conclusion: Mixed schistosomiasis depicts a higher S. haematobium relative to S. mansoni infection intensity in this setting, and may suggest significant genital morbidity. This is important in not only planning and implementing disease control programs, but also in exploring the contribution of schistosome infection in development of associated genital lesions and its predisposition to HIV infection among reproductive age women in Kenya, particularly in Nyanza region where there is not early sexual debut among adolescents but also where the HIV prevalence (15%) is double the National average. Key words: Schistosomiasis, single infection, mixed infection, south Nyanza, western Kenya
NTD8-B12 The effect of annual compared to biennial praziquantel treatment regimens on Schistosoma mansoni infection along Lake Victoria in western Kenya-THE SCORE PROJECT
Samuel Ochieng, Isaac Onkanga, Pauline N. M. Mwinzi, Geoffrey Muchiri, Judith Warindu, Willis Agolla, George Okoth, Kennedy Andiego, Martin Omedo, Ryan Wiegand, W. Evan Secor and Susan P. Montgomery. Center for Global Health Research, Kenya Medical Research Institute, Kisumu, Kenya; Division of Parasitic Diseases and Malaria, Centers for Disease Control and Prevention, Atlanta, Georgia
Introduction: The world health organization recommends a single annual dose of praziquantel treatment for schistosomiasis control in high risk areas, and once every two years in moderate risk areas but evidence for these proposed strategies is inadequate. In order to best inform strategies for current elimination targets, more studies on the most impactive and cost effective deworming treatment regimens are needed. This would be particularly important for sustainable implementation costs as many control programmes in underprivileged countries rely on external funding. To fill this information gap, we compared the effect of one and two rounds of praziquantel treatment on schistosomiasis infection over a period of two years in high risk prevalence communities (>25%) of western Kenya. Methods: The communities were randomized into treatment arms of 25

56
villages each and school based treatment was offered annually or biennially (every other year). Cross-sectional parasitological surveys using the Kato-Katz method were performed on children aged 9-12 years old in primary schools at baseline and after treatments. Analysis was performed using unpaired t test using SPSS. Results: The baseline S. mansoni infection prevalence and the arithmetic mean intensity in the arm treated every year were 60% and 87.3 eggs per gram of faeces respectively while those in the arm treated every other year were 63% and 95.13 epg respectively. At two years follow up, S. mansoni infection prevalence and the arithmetic mean intensity in the first arm were 34% and 31.8 epg respectively while those in the were 50% and 52.4 epg respectively. Both arms recorded significant reductions in both prevalence and intensity, P<0.001. Comparisons between the two arms revealed that both prevalence and intensity were insignificantly different at baseline but significantly lower in the than in arm 6 at follow up, P<0.001. Conclusion: Regardless of the number of treatment rounds, the two arms were shown to be effective in reducing S. mansoni infection levels. However, comparisons between the two arms revealed that two doses of praziquantel are superior to a single dose in a period of two years in high risk areas. This study supports the current treatment strategy of a single annual dose of praziquantel in the control of schistosomiasis infection, but that this is also not adequate to bring the prevalence to controlled levels in a two year period.
NTD8-B13 Innovative approaches to Clinical Data Management in Resource Limited Settings using Open Source Technologies: Raymond Omollo, Michael Ochieng, Brian Mutinda, Truphosa Omollo, Rhoda Owiti, Seth Okeyo1, Monique Wasunna and Tansy Edwards Introduction / Background: Clinical Data Management of clinical trials for Neglected Tropical Diseases in endemic countries can be difficult due to limited resources and expertise. There is a need to develop improved systems for data management which are efficient and affordable without violating the principles of Good Clinical Practice. Open source tools offer good alternatives when compared to proprietary systems but challenges in validation still abound. Results/Findings: We have developed an offline version of OpenClinica, making it possible to collect data in areas with limited internet infrastructure, together with an in-house system for query management which is a crucial component in data management. Both have been possible as a result of our experience in managing large multi-centre clinical trials in Africa on Neglected Tropical Diseases such as Visceral Leishmaniasis, with sites located in very remote areas.

57
Conclusions / Discussion: We demonstrate that innovative approaches to clinical data management are possible and that open source tools with good functionality are available and can be further developed to assure production of high quality and reliable data. It is also important to share knowledge on best practices, such as on systems validation and source code development, for better management of data from clinical trials in resource limited settings
NTD8-B14 Predictive value of school-age children’s schistosomiasis prevalence and egg intensity for entire community and other age groups in western Kenya –the score project Pauline N. M. Mwinzi, Geoffrey Muchiri, Ryan Wiegand, Martin Omedo, Diana M. S. Karanja, Susan P. Montgomery, W. Evan Secor Neglected Tropical Diseases Research Unit, Center for Global Health Research, Kenya Medical Research Institute, Kisumu, Kenya; Division of Parasitic Diseases and Malaria, Centers for Disease Control and Prevention, Atlanta, Georgia Depending on the prevalence of schistosomiasis in school children within a given community, the World Health Organization recommends that either school-based or community-wide mass drug administration (MDA) be employed. In a large study comparing MDA approaches for Schistosoma mansoni control, we evaluated whether infection and intensity of 9-12 year old students reflected infection levels in other children, adults, and the overall population in the same community. Cross-sectional surveys of pre-adolescents (9-12 years old) were compared to those of first year students (7-8 years old), and adults (20-55 years old) in 225 villages along the Kenyan shores of Lake Victoria. Village schistosomiasis prevalence and intensity for pre-adolescents strongly correlated (p<0.0001) with prevalence and infection intensity for all other age groups and the overall community. Our findings suggest that S. mansoni prevalence and intensity among 9-12 year olds is valid for sampling purposes in mapping for MDAs.
NTD8-B15 Evaluation of participation rates among school age children following three rounds of Mass Drug Administration for S. mansoni control in western Kenya-The SCORE Project. Muchiri Geoffrey1, R. Musuva1, M.Ogutu1,I.Onkanga1, W.Agollah1, G.Okoth1, J.Warindu1, S.Sawo1, M.Omedo1, D. Karanja1, S. Montegomery2, Evan.W.Secor2, P. Mwinzi1
1. Center for Global Health Research, Kenya Medical Research Institute,

58
P.O. Box 1578-40100,Kisumu Kenya; 2. Division of Parasitic Diseases, Center for Disease Control and Prevention, 1600 Clifton Rd, N.E. Atlanta ,GA 30329.\ Introduction: High study participation is a major hallmark of a ‘‘good’’ public health survey. Studies have reported steeper declines in recent years. However, little information is available on the trends of participation in most Neglected Tropical Diseases (NTDs) surveys. We sought to evaluate participation rates among school age children in an on-going five year-cross sectional survey for schistosomiasis control in western Kenya. Methodology: Participation rate was defined as the number of participants enrolled, and derived from calculating number of positive consent forms divided by the total number of eligible children to whom consent forms had been given. In 2013, 9562 consent documents were issued to all identified eligible school age children in the 100 participating schools while 7962 were issued to 75 schools participating in 2014. Two tailed unpaired and pairedT-testsand ANOVA were used for analysis withGraph Pad Prism 5. Results: In 2013, mean number of consent forms returned was 90.70 (95% CI: 86.27-95.13), while 4.92 (95% CI: 3.36-5.61) were not returned. Up to 86.54 (95% CI: 82.13-90.95) gave positive consent and 4.38 (95% CI: 3.15-5.61) declined the study. Participation rate was at 90.78% (95% CI: 88.77-92.78). In 2014, mean number returned was 102.6 (95% CI: 99.1-106.0), and 3.59 (95% CI: 2.45-4.7) were not returned. 99.1 (95% CI: 95.88-102.2) gave positive consent and 3.3 (95% CI: 2.41-4.17) gave negative consent. Participation rate was 93.64% (95% CI: 92.45-94.83). there were significant differences between number of consent forms returned or not returned and positive vs. negative consents between the two years (P<0.0001) with improvements in participation being noted in the second year for both unpaired and paired t-test analysis at P= 0.0262 and P= 0.0197 respectively. Conclusion:The results show significant increase in study enrollment and participation among the school-age children. These are attributable to health teachers training, health education, use of incentives to children, engagement of school health teachers and community health workers in sensitization, mobilization and consenting processes and additional follow-up schools that boostedschools withlow populations.Results also indicate contrast to the reported decline of participation byprevious studies.
NTD8-B16 Efficacy of Praziquantel in the treatment of Schistosoma haematobium in pre-school age children of Kwale County, Kenya
BW Kimani, A. Mbugua, JH Kihara, DW Njomo Authors: Bridget W. Kimani [1, 3], Amos Mbugua [1], Jimmy H. Kihara [2], Njomo Doris W [3] [1] Jomo Kenyatta University of Agriculture and Technology

59
[2] Ministry of Health, Division of Vector Borne Diseases, Kenya [3] Kenya Medical Research Institute (KEMRI), Background: Control of schistosome infections is through treatment with a single dose of the anti-helminth drug praziquantel (PZQ) which is safe, highly efficacious; cheap and can reverse schistosome-related morbidity particularly in the early stages of disease progression. Control Programmes emphasize treatment of school-aged children, but in high endemic areas, preschool-aged children are also at risk of infection. Since a pediatric formulation is not available outside of Egypt, crushed PZQ tablets mixed with water or fruit juice are used. The objective of this study was to determine the efficacy of PZQ in the treatment of Schistosoma haematobium in children attending Early Childhood Development Centers of Kwale County, Kenya. Methods: A semi-quasi experimental study design was used to systematically sample 10 pre-schools and all (353) preschool-aged (<6 years) children provided urine samples before and 5 weeks after treatment where S. haematobium eggs were detected and quantified using filtration techniques. Crushed PZQ tablets mixed with fruit juice were administered to all the children at the recommended dose of 40mg/kg. Results: Preliminary results of the ongoing study show that the prevalence of S. haematobium among the pre-school age children was 16.9% (95%CI). The cure rate was calculated as a ratio of the number of study participant who tested negative after treatment to those who tested positive before treatment 83.3%. The ratio of boys to girls who tested positive was 36:24 and 70% of these children were between 5-6 years of age. Conclusion: Crushed praziquantel administered to preschool-aged children at a dose of 40mg/kg is efficacious against S. haematobium and control programmes should consider administering PZQ to reverse morbidity in early stages.
NTD8-B17 Minimal adverse reactions following praziquantel mass drug administration; acase study on deworming in western kenya - the score project Okoth GK1,Musuva R1 , Awiti A1, Omedo M1,Onkanga I, Muchiri G1,Warindu J1, Sawo S1, Agolla W1,Secor WE2, Montgomery SP2, Mwinzi P1. 1Neglected Tropical Diseases Branch, Center for Global Health Research, Kenya Medical Research Institute (KEMRI), Kisumu, Kenya; 2Division of Parasitic Diseases and Malaria, Centers for Disease Control and Prevention, Atlanta, Georgia.

60
Introduction: Praziquantel is universally accepted as the drug of choice for schistomiasis control. Praziquantel is generally considered a safe drug but may induce adverse reactions (ARs) that are transient and rapidly subside without treatment. The Schistosomiasis Consortium of Operational Research and Elimination(SCORE) carried out case studies on ARs experienced by the pupils and AE management during(how many?) mass drug administration(MDA) with praziquantel conducted in (year range?). Methodology: Each year, treatment was carried out by trained health teachers and community health workers. Any side effects noted within one hour of MDA were recorded in the treatment booklets. ARs were reported to community health technologist who then evaluated if a clinical evaluation and treatment was needed. A report was collected from the parent, pupil, health teacher and clinical officer. Results: Only one adverse reaction was reported in 2013 following MDA in 100 communities. A standard six pupil from X primary school developed rashes and skin peeling within a few hours) after treatment with praziquantel. This case was reported toa community health technologist, who observed the child but did not recommend any further clinical evaluation as the rashes were subsiding. According to health teacher records, the child had been treated with praziquantel the preceding year and there were no reported reactions. The child reported not taking lunch at home which may have contributed to the development of minor side effects. A similar case was reported within the same study in 2013 where a child from Y primary school was rushed to the health centre three days post Praziquantel treatment with the same symptoms. A clinical assessment was done after which the child was given an oral dose of cetricine 10mg OD for three days and within one week, the rashes had cleared. Conclusion: Although health teachers viewed the reactions as adverse, AE signs and symptoms subsided within a few days and could be attributed to taking the drug on an empty stomach. It is therefore imperative for programs carrying out mass distribution of praziquantel to ensure the children take a snack before treatment with praziquantel.
NTD8-B18 Impact of two rounds of anthelmintics delivery among communities in Mbita and adjacent Rusinga Island in western Kenya Fredrick O.Rawago1, Kimberly Y. Won2, Pauline N. Mwinzi1, Patrick J. Lammie2 and Maurice R. Odiere 1, 1Center for Global Health Research, Kenya Medical Research Institute, Kisumu, Kenya; 2 Centers for Disease Control & Prevention, Division of Parasitic Diseases and Malaria, Atlanta, GA, USA Background: Preventive chemotherapy against schistosomiasis and soil transmitted helminths (STH) has been implemented in other parts of the
61
world targeting school-age children and adults at high risk with plausible results. The evidence base for this policy needs to be established for regions not previously targeted to commit resources towards implementing similar programs. Methods: We conducted a cross-sectional study in Mbita District, Homa-Bay County, Kenya to evaluate the effect of co-administration of praziquantel and albendazole against intestinal schistosomiasis and STH infections after two rounds of single annual deworming. Besides effects of time, the study further compared the performance of the community-wide versus school based treatment strategies. Single stool sample was collected from each participant and presence and intensity of infection (EPG) for both Schistosoma mansoni and STH infection (hookworm, Ascaris lumbricoides and Trichuris trichiura) determined by duplicate slides by Kato-Katz technique among 6033 (Baseline), 6375 (Year 2) and 5710 (Year 3) participants in 30 study villages. Results: Overall prevalence of S. mansoni and STH marginally reduced to 29.8% and 3.0% post two rounds of annual deworming relative to the baselines’ 44.9% and 5.2% respectively (P = 0.0877 for S. mansoni). Moreover, heavy S. mansoni infection decreased from baseline to Year 3 post-MDA, 485(17.9%) and 160 (9.39%), respectively. Whereas, mean S. mansoni egg density significantly reduced by 40.5% compared to the baselines (266 versus 158 epg), stratification of egg density by study arm showed higher but not significant decrease in egg density in SBT arm (50.2% decrease) compared to CWT arm (44.2% decrease) post two rounds of annual treatment. Conclusion: Two rounds of anthelmintics delivery had significant impact on prevalence of intestinal schistosomiasis and STH among the targeted population. In-addition, treatment had substantial impact on S. mansoni infection intensity. However, no marked difference was noted between community-wide and school based treatment strategies.
NTD8-B19 Evaluation of the impact of praziquantel mass treatment on stunting and wasting among school children in western kenya-the SCORE project.
Boaz Mulonga,1Isaac Onkanga,1Geoffrey Muchiri,1Mike Ogutu1,Ken Andiego1, Martin Omedo,1Evan Secor,2Susan Montgomery2and Pauline Mwinzi.1
1. Center for Global Health Research (CGHR), Kenya Medical Research Institute Kisumu, Kenya, 2. Division Of Parasitic And Malaria, Center For Disease Control And Prevention, Atlanta, Georgia.
Background: Retardation of physical development remains an important public health problem associated with schistosomiasis in sub-Saharan Africa. However, the benefits associated with schistosomiasis treatment
62
remain scarce. We measured stunting and wasting levels at baseline and after three years to investigate the effect of annual praziquantel treatment. Methodology: A longitudinal survey was carried out among school children aged 7-8 years from 12 schools along the shores of Lake Victoria. Children from 6 of the schools (arm 6) received treatment once after baseline assessment while children from the other 6 schools (arm 1) received treatment once a year. Each child had three stool samples examined for Schistosoma mansoni eggs by microscopy. Additionally, children were tested for Plasmodium falciparum infection, and weight and height measurements were performed as a proxy for physical development. Height and weight data were entered into the WHOAnthro software, and Z-scores were calculated.Wasting was defined as a BMI-for-age Z-score of < −2, and stunting was defined as a height-for-age Z-score of < −2. Principal findings: The respective baseline prevalence of S. mansoni infection, P. falciparum infection, stunting and wasting were 77.8%, 7.7%, 11.5% and 32.9% for arm 1 schools (treated every year) and 60.1%, 8.5%, 6.9% and 16.0% for arm 6 schools (treated every other year). Following treatment, respective prevalence of S. mansoni infection, P. falciparum infection, stunting and wasting were 72.2%, 21.4%, 8.6% and 5.6% for arm 1 schools and 59.6%, 23.9%, 5.3% and 4.3% for arm 6 schools. After treatment, similar patterns were observed in the two arms whereby wasting levels significantly declined (P<0.001) while malaria levels significantly increased (P<0.001). Correlation analysis revealed that both wasting and stunting were not associated with S. mansoni and malaria infections. Conclusion: Although improved physical development was observed following treatment, our findings indicate that this could not be solely attributed to the PZQ treatment which did little in reducing S. mansoni infection. This indicates that more MDAs are required to realize any effect of PZQ on physical development, and that research is needed to evaluate integrated measures that improve the general development of the child.
NTD8-B20 The prevalence of soil transmitted helminths among school-age children in schoools participating in the score project –western Kenya 2014
Judith Warindu, Isaac Onkanga, Geoffrey Muchiri, Samuel Sawo, George Okoth,Willis Agolla, Ken Andiego, Martin Owino, Susan P. Montgomery, W. Evan Secor, Pauline NM Mwinzi.
Neglected Tropical Diseases Branch, Center for Global Health Research, Kenya Medical Research Institute (KEMRI), Kisumu, Kenya; Division of Parasitic Diseases and Malaria, Centers for Disease Control and Prevention, Atlanta, Georgia Introduction: Current mapping of the prevalence of soil transmitted helminths(STHs) infectionsis needed to more efficiently allocate control
63
interventions. In Kenya, the Ministry of Health uses this information to inform an annual national deworming programme to control helminth infections in primary school aged children.We carried out a cross-sectional survey to determine current prevalence of STHs infections among primary school children along the shores of Lake Victoria in western Kenya, within the Schistosomiasis Consortium for Operational Research and Evaluation (SCORE) project. Methods:A total of 75 schools was surveyed in this study. In each school, following informed consenta total of 100 children aged 9-12 years were recruited for participation. Each pupil provided three consecutive stool samples for three days. Two slides per stool sample were screened for AscarislumbricoidesandTrichuristrichiura using the Kato Katz method. Data summaries and comparisons using the t-statistic were carried out inSPSS software. Results: Respective prevalences for A. lumbricoidesand T. trichiura were 5.3% (95% CI: 4.8-5.8%) and 8.0% (95% CI: 7.4-8.7%). The prevalence ofT. trichiurawas significantly higher than that of A.lumbricoides, P<0.001. The prevalence ofA. lumbricoidesand T. trichiuracoinfection was 1.1% (95% CI: 0.8-1.3%) while the prevalence of those with any STH infection was 12.3% (95% CI: 11.5-13.0%). Conclusion:Compared to previous STHs infection reports in this setting, lower prevalence levels were recorded in our study.This could be attributed tobenefits gained from the national deworming programme that has been going on since 2009 in Kenya. However, prevalence levels of those with any STH infection indicates a need for continued deworming exercise in this area according to WHO guidelines.
NTD8-B21 Overview of current NTD stuation in Bungoma County Osman K. Kakai VBDCU Kimilili Field Station I/C The Vector Borne Diseases Control Unit (VBDCU) is a unit under preventive and promotive services department in the Ministry of Health. The Kimilili field station was opened in 1972 for the purposes of surveillance, monitoring and control of cutaneous leishmaniasis in Mt. Elgon region. However over the years its mandate has expanded to include other parasitic diseases namely Malaria, Jigger infestation, filariasis, Soil Transmitted Helminthes, onchocerciasis, Leptosipirosis and Trypanosomiasis which are endemic in the region, with burdens such as:
• Jigger infestations prevalence of 39.7% in the community • Re-emergence of cutaneous leishmaniasis cases in Mt. Elgon sub
county to a prevalence of up to 3.1% among the communities • Worm re-infestation among children and adults in the community • Re- emerging parasitic diseases and their vectors e.g. Filariasis,
64
trypanosomiasis Reasons for constraints:
• No resources allocated to implement efficient and effective jigger surveillance, monitoring and control
• Since the inception of the county system of government ,No resources have allocated to VBDCU for efficient and effective leishmaniasis surveillance, monitoring and control
• No resources allocated for efficient and effective soil transmitted helminthes (STH) surveillance, monitoring and control apart from the limited surveys conducted by National school deworming project
• No resources allocated for surveillance, monitoring and control of parasitic diseases
Recommendations: There is need to create linkages with interested partners to support collaborative NTD surveillance and control activities by the VBDCU Kimilili Research opportunities
• The VBDCU Kimilili station has infrastructure which if properly utilized for research in local NTDs can lead to new innovative control measures.
• Utilization of community strategy. VBDCU has established networks with 13 Community units in Kimilili Sub County on NTDs surveillance
NTD8-B24 Effect of gender on schistosoma mansoni and soil transmitted
helminthes infections among school going children in western kenya. The score project 1Centre for Global Health Research, Kenya Medical Research Institute 1578-40100 Kisumu, 2Division of Parasitic Diseases, Centers for disease Control and Prevention,4770 Buford Highway, N.E Mail Stop F-13,Atlanta G.A George Ogara1, Emmy Kavere1, Bernard Abudho1, Diana Karanja1, Maurice Odiere1, Susan P. Montgomery 2, Evan Secor2
Introduction: Schistosomiasis and soil-transmitted helminthes (Ascaris Lumbricoides, Trichuris trichuria) are some of the neglected debilitating infections in developing countries. They are usually associated with poverty, poor sanitation and lack of clean water. Studies have shown that boys are more infected than girls owing to their activities and time spent in infested water. As part of our program on evaluation of mass drug administration strategies in school children, we have analyzed the prevalence and intensities of S.mansoni, A. lumbricoides, and T. trichiura in boys and girls aged 9-12 years of age in a proportion of the schools. Materials and methods: 33 out of 50 schools were randomly selected,

65
with a total population of 2,722 children aged between 9-12 years (girls 1,356, boys 1,366). Three consecutive stool samples were collected from each participant and duplicate Kato-Katz (41.7mg) slides were prepared from each sample. 10% of the slides were randomly selected for quality control. Differences in proportions and relationships were done using Chi-square analysis and logistic regression. Intensity of S. mansoni was expressed in terms of epg. Statistical significance was tested at P≤0.05. Results: Out of the total 2722 participants examined, 10.2 % were infected with S. mansoni, 4.8% with A. Lumbricoides and 8.9% with T. trichuria. The prevalence of S. mansoni, A. Lumbricoides and T.trichuria in boys was 9.8%, 4.6% and 7.8% while infections in girls were 10.6%, 4.9% and 10.0% respectively. Girls posted higher infection than boys showing a significance difference for S. mansoni (P values 0.039) and T.trichuria (P value0.00) respectively. Intensity of S. mansoni was 178 epg for boys and371 for girls. Comparatively girls demonstrated a higher intensity than boys a cause that impacts morbidity. Conclusion: These findings indicate that a total of 649 (23.84%) were infected with different parasites or both,. Collectively it shows that helminthes infections are a significant public health problem among school-going children. These results differ with earlier studies’ finding that boys are more susceptible to S. mansoni and soil transmitted helminthes than girls. More studies with a bigger population are necessary to strengthen these findings.
NTD8-B25 Evaluation of the Health-related Quality of Life among school children in Schistosoma mansoni endemic area in Asembo Bay, western Kenya: Repeated Cross-sectional Study Abudho O. Bernard1, Eric M. Ndombi1, Nupur Kittur2, Diana M. S. Karanja1, W. Evan Secor3, and Daniel G. Colley2
1Centre for Global Health Research, Kenya Medical Research Institute, Kisumu, Kenya 2Center for Tropical and Emerging Global Diseases and Department of Microbiology, University of Georgia, Athens, GA 3Division of Parasitic Diseases, Centers for Disease Control and Prevention, Atlanta, GA Background: Schistosomiasis remains a global public health challenge in Africa where 90% of the disease burden is found. The infection is chronic in nature with few infected individuals exhibiting “severe” morbidity. However, less obvious morbidities such as anaemia, impaired growth, wasting, stunting, abdominal pain, poor school performance and reduced work capacity are commonly exhibited by most infected children. Omission of these subtle, but very real, morbidities when calculating schistosomiasis specific DALYs results in underestimation of the burden of

66
disease due to schistosomiasis. Methodology: In this study, we administered the Pediatric Quality of Life Inventory (PedsQoLTM, 4.0 questionnaires) tool, to assess heath-related quality of life (HrQoL) among 334 children aged 6-18 years in both primary and secondary schools at baseline before mass drug administration (MDA) and aged 7-13 years in primary schools one year after MDA. Results: At baseline, all the participants were S. mansoni positive by 3 Kato-Katz tests. Quality of life scores were not correlated with age, sex or S. mansoni intensity of the infection. One year after MDA, 56% of the participants tested positive for S. mansoni by the same tests. Statistically significant difference in HrQoL physical functioning score (p=0.033) was observed between S. mansoni positive and S. mansoni negative participants. There was no significant difference in HrQoL in psychological functioning score or total functioning score between S. mansoni positive and S. mansoni negative participants(p=0.603; p=0.306) respectively. The PedsQL reliabilities were generally high (Cronbach’s alphas ≥0.70) demonstrating adequate internal consistency, with no floor effects and acceptable levels of ceiling effects. Quality of life scores were not correlated with age, sex or S. mansoni intensity of the infection. Conclusion: We conclude that any level of S .mansoni infection correlates with physical morbidity. This finding is expected to be useful in longitudinal or clinical settings where patients are followed after treatments, and infection is defined based on sensitive parasitological diagnosis to improve the definition of HrQoL impact of S. mansoni infection among children. However, more studies are needed to replicate this observation in endemic areas with PedsQL as an effective tool in assessing the HrQoL in schistosomiasis infection and other neglected tropical diseases (NTDs) before and after treatments.
NTD8-B26 Echinococcus spp. in central Kenya: a different story Hellen Mbaya1,2, Japhet Magambo2,4, Sammy Njenga3, Eberhard Zeyhle5, Cecilia Mbae3, Erastus Mulinge3, Marion Wassermann6, Peter Kern7, Thomas Romig6. 1. National Biosafety Authority, Nairobi, Kenya 2. Jomo Kenyatta University of Agriculture and Technology, Nairobi, Kenya 3. Kenya Medical Research Institute, Nairobi, Kenya 4. Meru University of Science and Technology, Meru, Kenya 5. African Medical & Research Foundation, Nairobi, Kenya 6. Parasitology Unit, University of Hohenheim, Stuttgart, Germany e-mail: [email protected] 7. Comprehensive Infectious Diseases Center, University Hospitals, Ulm, Germany
67
Abstract Background:Research on cystic echinococcosis (CE) has a long history in Kenya, but has mainly concentrated on two discrete areas, Turkana and Maasailand, which are known to be foci of human CE in Africa. Here, we report on a survey for CE in livestock from central to northeastern Kenya, from where no previous data are available. Methodology: A total of 7,831 livestock carcasses were surveyed. CE prevalence was 1.92 % in cattle (n=4,595), 6.94 % in camels (n=216), 0.37 % in goats (n=2,955) and 4.62 % in sheep (n=65). Identification of the parasite was done using an RFLP-PCR of the mitochondrial nad1 gene, which had been validated before against the various Echinococcus taxa currently recognized as distinct species. Results:From a total of 284 recovered cysts, 258 could be identified as Echinococcus granulosus sensu stricto (n=160), E. ortleppi (n=51) and E.canadensis (n=47) by RFLP-PCR of nad1. In cattle, fertile cysts occurred mostly in the lungs and belonged to E. ortleppi (31 of 54), while the vast majority were sterile or calcified cysts of E.granulosus s.s. Most fertile cysts in camels belonged to E. canadensis (33 of 37); sterile or calcified cysts were rare. Goats harboured fertile cysts of E. ortleppi (n=3)—which is the first record in that host species—and E. canadensis (n=1),while all cysts of E. granulosus were sterile. Only sterile cysts were found in the three examined sheep. Typically, all cysts in animals with multiple infections belonged to the same species, while mixed infections were rare. Conclusion:Our data indicate that the epidemiological situation in central to northeastern Kenya is clearly different from the well-studied pastoral regions of Turkana and Maasailand, and the apparently low number of human CE cases correlates with the infrequent occurrence of E. granulosus s.s. Keywords:Echinococcus granulosus,Echinococcus canadensis, Echinococcus ortleppi, Cystic echinococcosis Sub-SaharanAfrica, Kenya
NTD8-B27 A survey for Echinococcus spp. of carnivores in six wildlife conservation in Kenya Dorothy Kagendo 1, 2, Japhet Magambo 1, 2, Eric Agola3, Sammy Njenga3, Eberhard Zeyhle4,Erastus Mulinge3, Peter Gitonga5, Cecilia Mbae3,Eric Muchiri2, Marion Wassermann6, Peter Kern7, Thomas Romig6.
1Jomo Kenyatta University of Agriculture and Technology, Nairobi, Kenya 2 Meru University of Science and Technology, Kenya. 3 Kenya Medical Research Institute, Nairobi, Kenya. 4African Medical and research Foundation, Nairobi, Kenya
68
5Kenya Wildlife services, Nairobi, Kenya 6Department of Parasitology, Hohenheim University, Stuttgart-Germany 7 Department of Infectiology, Ulm University, Germany Background: Echinococcus granulosus sensu lato the etiological agent of cystic echinococcosis (CE) has a worldwide distribution and is capable of adapting to a wide variety of domestic and wild intermediates and definitive hosts. In Kenya the role of wildlife in the transmission of CE and the genetic diversity of Echinococcus spp in wildlife is unknown. Methodology: A total of 832 faecal samples from wild carnivores (lions, leopards, spotted hyenas, wild dogs and silver-backed jackals) were collected in six different conservation areas of Kenya. Taeniid eggs were found in 120 samples (14.4%). In total, 1160 eggs were isolatedand further analysed using RFLP-PCR of the nad1 gene and sequencing. Results:38 of these samples contained eggs ofEchinococcus spp., which were identified as either Echinococcus felidis (n = 27) or Echinococcus granulosussensu stricto (n = 12); one sample contained eggs from both taxa. E. felidis was found in faeces from lions(n =20) and hyenas (n=5) while E. granulosus in faeces from lions (n=8), leopards (n=1) and hyenas(n = 3). The host species for two samples containing E. felidis could not be identified with certainty. Both taxa of Echinococcus were found in all conservationareas except Meru (only E. felidis) and Tsavo West (only E. granulosus). All samples with taeniideggs were subjected to a confirmatory host species RLFP-PCR of the cytochrome B gene. 60% had been correctlyidentified in the field. Frequently, hyena faeces weremistaken for lion and vice versa, and none of thesamples from jackals and wild dogs could be confirmed in the tested sub-sample. Conclusion: This is the first molecularstudy on the distribution of Echinococcus spp. in Kenyan wildlife. The presence of E. felidis is confirmed forlions and newly reported for spotted hyenas. Lions and hyenas are newly recognized hosts for E. granulosuss.s., while the role of leopards remains uncertain. These data provide the basis for further studies on thelifecycles and the possible link between wild and domestic cycles of cystic echinococcosis in eastern Africa.
NTD8-B28 Distribution of Echinococcus species/strains in Kenya Erastus Mulinge1,Cecilia Mbae1, Eberhard Zeyhle2,Titus Mutwiri3, Hellen Mbaya3, Dorothy Kagendo3, Joseph Odero3, Francis Addy3, Marion Wassermann4 Japhet Magambo5, Peter Kern6, Thomas Romig4
1Kenya Medical Research Institute, Nairobi, Kenya 2African Medical Research Foundation, Nairobi, Kenya 3Jomo Kenyatta University of Agriculture and Technology, Kenya 4Parasitology Unit, University of Hohenheim, Stuttgart, Germany 5Meru University of Science and Technology, Meru, Kenya

69
6Center for Internal Medicine, University Hospital, Ulm, Germany Background:Cystic Echinococcosis caused by the larval stage of the tapeworm Echinococcus granulosus sensu lato has a worldwide distribution. In Kenya it is endemic mainly in livestock rearing areas and pastoralist communities. Methodology: Cystic material from intermediate hosts (humans, livestock, wild herbivores) and faecal material from final hosts (wild canids and felids) were collected from various parts of Kenya. The samples were analyzed by PCR-RFLP and sequencing of the nad1 gene to identify the species and strains. Results:E.granulosus s.s was the most common strain infecting humans, cattle, sheep,goats & wildebeests but is also present in camels, lions & hyenas. This strainwas reported in all the study sites, while E. ortleppi was only found in Meru,Isiolo and from one cattle in Maasailand. E. canadensis G6/7 was frequent inIsiolo as this was the only study site where camels were examined, but alsoreported from other livestock species in Isiolo, Maasailand and Meru. E.felidis was widespread in Kenya and found frequently in lions and hyena as itwas reported from all the game parks/reserves. E. granulosus s.s wasdetected in either lions or/and hyenas from all the game reserves apart fromMeru National park. Additionally E. granulosus s.s was detected in faecalsamples from a leopard in Samburu. Conclusion: This study reports the presence of E. granulosus sensu stricto, E. ortleppi, E.canadensis G6/7 and E. felidis in Kenya confirming the existence of bothdomestic and wild cycles ofEchinococcus spp. Further the study has indicated that species and strains of E. granulosuss.l. are unevenly distributed in Kenya. Key words: Echinococcus granulosus sensu lato, genetic diversity, Kenya
NTD8-C4 Community engagement strategy for community-wide treatment for the SCORE project in western Kenya Alphonce Awiti, Rosemary Musuva, Martin Omedo, Michael Ogutu, Kennedy Andiego, W. Evan Secor, Susan P.Montgomery, Pauline Mwinzi. 1Centre for Global Health Research, Kenya Medical Research Institute, P.O. Box1578-40100,Kisumu Kenya; 2Division of Parasitic Diseases and Malaria, Centers for Disease Control and Prevention, 1600 Clifton Rd, N.E. Atlanta ,GA, USA 30329. Introduction: Control programs aimed at managing tropical diseases are much more likely to yield meaningful success if there iseffectivecommunity engagement. Nevertheless, little effort has been

70
made to assess the community engagement strategies that work best in health projects, particularly in the area of Neglected Tropical Diseases (NTDs). We explored and compared community engagement strategies used during project implementation. Methods: National, provincial and local stakeholders were involved through direct and indirect approaches. Written correspondences, meetings, public address systems and radio message highlights were employed in order to reach the target community members. A total of 10 stakeholder meetings were held with health, education, civic and political leaders from district to village levels to get feedback about the mobilization strategies. Forum discussions were audio-recorded and documented. A community engagement model was further used to explain the processes and levels of engagement adopted. Written correspondences and email were widely used in engaging health workers while direct engagement methods such as public address and trainings were employed at the community level. The discussions were audio recorded, transcribed, coded and thematically analyzed using Atlas TI software. Results: Better engagement strategies were realised on the basis of feedback meetings held in the second year of implementation which partly explained improved treatment coverage in that year and successive years. Proper coordination, inclusivity and cooperation among the key treatment implementing partners were highlighted as facilitative factors for effective community engagement activities. Inclusion of youth, women and other groups in planned future meetings was a cross-cutting recommendation during stakeholders’ forums. Conclusion: Community treatment activities can be better facilitated by adopting proper engagement of community leadership structures if success of any community-based initiative is to be realized. However, this must be layered both on correct entry processes and proper mobilization activities. We found that the word of mouth was the most effective for mobilizing villagers in western Kenya to participate in mass drug administration for schistosomiasis. Key words: Community, engagement, stakeholder, mobilization, Neglected tropical Diseases
NTD8-C5 Implementing Mass Drug Treatment among Early Childhood Development Education Centre children in Malindi Sub-County, Coastal Kenya, Nipher Nyamogo1, Gladys Odhiambo3, Faith Mwende2 and Doris Njomo2
1Dayster University, P.O. Box 44400 – 00100 Nairobi. 2Eastern and Southern Africa Centre of International Parasite Control (ESACIPAC) Kenya Medical Research Institute (KEMRI), P.O Box 54840 – 00200 Nairobi. 3Center for Global Health Research, Kenya Medical Research

71
Institute, P.O. Box 1578-40100, Kisumu, Kenya. Background: A number of countries especially in Africa are developing national plans for the control of neglected tropical diseases. A key component of such plans is school-based deworming (SBD) for the control of schistosomiasis and soil-transmitted helminths (STHs). In Kenya SBD is not conducted in standalone Early Childhood Development centers (ECD) which makes most of the children in these schools miss treatment and thus contribute towards continued transmission of the infections. This study therefore explored ways through which an ECD centre treatment could be employed to deliver treatment to this vulnerable and delicate group of children so as to maximize treatment coverage. Methods: The programme trained 36 Community Health Extension Workers (CHEWs) to deliver drugs to children at the stand alone ECD centers. Praziquantel was mixed with juice to enable easy swallowing during drug delivery. The study adopted a cross-sectional study design. We conducted 16 In-depth Interviews with CHEWs who had implemented the intervention. Purposive sampling technique was used to identify informants. The data was collected by trained and experienced KEMRI staff, transcribed, coded and analysed using ATLAS.ti version 6. Results: The study found out that the logistics of implementing ECD centre treatment were not complicated. All of the CHEWs reported being comfortable with drug administration and record keeping because of the training they had previously received. The research also brought out that the major motivation to participate in the study was the fact that the exercise was in their line of duty. High enrolment at the ECD centre and distance between the schools were the major challenges. Despite challenges that the CHEWs faced they reported having reached all the ECDs allocated to them and treated all the children present that day. All CHEWs interviewed said that they were willing to take part in the treatment of the ECD children in future. Discussion: Community Health Extension Workers can easily deliver mass treatment for schistosomiasis and soil transmitted helminths to pre-primary school children. However, the support of the ECD teachers cannot be ignored and we therefore recommend similar training and use of these teachers for drug delivery to pre- primary school children.
NTD8-C6 Factors influencing health-seeking behaviour for schistosomiasis control by health teachers in Kisumu west district, Kenya the SCORE project Emmy Kavere1, Brian Ogembo1, Martin Omedo1, Collins Ouma3, Diana Karanja1, Maurice Odiere1, Susan P. Montgomery 2, Evan Secor2
1Centre for Global Health Research, Kenya Medical Research Institute 1578-40100 Kisumu, 2Division of Parasitic Diseases, Centres for

72
Disease Control and Prevention,4770 Buford Highway, N.E Mail Stop F-13,Atlanta G.A 3. Maseno University Introduction: Schistosomiasis leads to chronic ill health and significant economic burden. 200,000 deaths are attributed to schistosomiasis annually. The disease is associated with poverty, limited access to safe water and poor sanitation. Initiatives for control and elimination include Mass Drug Administration (MDA), health education, access to safe water and good sanitation, and in limited situations, mullusciciding. Whereas World Health Organization (WHO) recommends MDA only for school age children as an appropriate intervention, schistosomiasis affects all populations. Schistosomiasis is a behavioural disease and health-seeking behaviour has been known to promote health. Health-seeking behaviour is not only a matter of knowledge about cause but also of perceived threat and severity. This study sought to explore factors influencing health-seeking behaviour for schistosomiasis control among health teachers who despite being key implementers, are excluded from the MDA program. Materilas and methods: This cross-sectional study was done in Kisumu West district in 41 schools undertaking mass drug administration for schistosomiasis control. Saturated sampling was used for participants’ selection and data collected using both qualitative and quantitative methods. Differences in proportions and relationships were done using Chi-square analysis and logistic regression but themes from qualitative data were analyzed by Atlas ti software. Results: Results demonstrated that source of information (p-value=0.003) and knowledge awareness for bilharzia control (p-value=0.010) were significant for health-seeking behaviour. Low perception of disease severity and cost of health care were perceived as major barriers to health-seeking behaviour for schistosomiasis control. Furthermore, mass drug administration was reported as having not influenced the teachers’ health-seeking behavior. Conclusion: This study reveals that health-seeking behavior is yet to be embraced as a control against schistosomiasis and there is need to strengthen teachers understanding of bilharzia as a public health concern in the fight towards bilharzia control in western Kenya.
NTD8-C7 Factors affecting the success of a school based mass drug administration for the control of schistosomiasis in Nyanza, western Kenya-The SCORE Project Andiego K1, Omedo M1, Awiti A1, Musuva R1, Secor WE2, Montgomery SP2, Mwinzi P1
1Neglected Tropical Diseases Branch, Centre for Global Health Research, Kenya Medical Research Institute, P. O. Box 1578-40100, Kisumu, Kenya;
73
2Centres for Disease Control and Prevention, Division of Parasitic Diseases and Malaria, 1600 Clifton Rd, N.E.; Mailstop-D65, Atlanta, GA 30329-4018, USA Introduction: School-based mass drug administration (MDA) with praziquantel to control schistosomiasis relies on school health teachers for drug distribution. Although coverage rates are generally high, low treatment coverage is reported in some schools. The aim of this study was to describe factors that affect MDA implementation in schools and to suggest strategies to improve uptake by pupils in low coverage schools. Methodology: This was a cross-sectional qualitative study in which group discussions were conducted a month after MDA. Treatment was administered in 75 schools by 75 trained health teachers. The group discussions were held with school health teachers during feedback meetings, discussions were recorded and later transcribed, and teachers’ views on the strategies they used to attain high treatment coverage (defined as: 90.0%-100.0%) were analysed. Results: The factors influencing the high uptake include collective responsibility between the teachers and the parents, communities’ positive attitude towards teacher-driven school health programs and well defined school health programs. Provision of snacks before treatment also played a key role in enticing the pupils to be in school during the treatment. Most of the health teachers in high coverage schools were happy to be involved in the MDA activity due to recognition and non- monetary incentives such as t-shirts. Mobilizing both parents and teachers’ was also a key factor to the success of the MDA. Conclusion: The study shows that the high uptake of praziquantel among school children is a result of a complex interplay between individual, interpersonal, institutional, community and public policy factors. School administrations should consider providing snacks prior to MDA as this helps in enticing pupils to be in school. In addition, facilitating health teachers helps boost their moral to participate in school based MDA. The success of a school based MDA should be a collective responsibility between the school administration, teachers, parents and the program implementers.
NTD8:C8 The role of stakeholders in the success of project implementation Alphonce Awiti1, Michael Ogutu1, Rosemary Musuva1, Martin Omedo1, Kennedy Andiego1, Evan Secor2, Sue Montgomery2, Pauline Mwinzi1. 1Centre for Global Health Research, Kenya Medical Research Institute, P.O. Box1578-40100,Kisumu Kenya; 2Division of Parasitic Diseases and Malaria, Centers for Disease Control and Prevention, 1600 Clifton Rd, N.E. Atlanta ,GA 30329. Introduction: There is a growing body of research suggesting that

74
stakeholder engagement in intervention delivery is a crucial factor for the growth and long-term sustainability of any program. However, there are very few reports of stakeholder engagement in public health interventions like mass drug administration (MDA) for neglected tropical diseases (NTDs).We performed a literature review to explore the importance and crucial role played by stakeholders including their identification and involvement criteria used in project planning and implementation of a schistosomiasis control project in Western Kenya. Methods: A literature search was conducted on published litereature using Google, Pubmed and Sociomed as the key search engines. Key words such as ‘engagement’, ‘stakeholder engagement’ and ‘stakeholder participation’ among others were highlighted and used to understand the previous insights and key tools used and engagement matrices. Stakeholder forum registration sheets were used to gather socio-demographic information about their diversity. This information was summarised tabularly using Microsoft Excel computer software and stakeholder categories were graphically compared. Treatment coverage data was further used to validate trends arising from different categories engaged over time. Finally, a comparative analysis was done across the time period for project implementation. Results: The role of the district health management teams and public administrators remained consistent as key implementers and overseers respectively. The inclusion of more community groups such as beach management units (BMU), women and youth groups was necessary in successive engagements to boost higher representation. The village elders were of critical importance in providing health education, security and crisis mediation. Conclusions: Principally, stakeholders should be involved from the planning phase of the project to its implementation and final evaluation if sustainability and post-implementation collaboration is to be achieved. Further research needs to be done to inform stakeholder participation and expansion of their engagement in health care, particularly regarding NTDs.
NTD8-C9 Schistosomiasis health education: Design and pilot testing of an educational game “Schisto and LadderTM for schistosomiasis control Ejike, C.U., Oluwole, A.S., Adeniran, A.A., Mogaji, H.O., Alabi, O.M., and *Ekpo, U.F. Department of Biological Sciences, Federal University of Agriculture, PMB 2240, Abeokuta 110001, Nigeria *Corresponding author email:[email protected] Schistosomiasis remains a public health problem in many rural and semi-urban communities in Africa. The current control strategy involves mass drug administration with Praziquantel. To complement on-going preventive

75
chemotherapy, a health educational game named “Schisto and Ladder™” was designed and tested for the control of schistosomiasis among primary school children in Imala-odo, an endemic community in Abeokuta, Nigeria. The school children were randomly divided through balloting into two groups (intervention and control group) after first screening for schistosomiasis. Their knowledge, attitudes and practices (KAP) were assessed using pre-test questionnaire. The health educational game “Schisto and Ladder™” was given to intervention group and the common game “Snake and Ladder” was given to the control group to play for two months under the supervision of their class teachers. Assessments of pupils KAP after two months were made using post-test questionnaires and Focus Group Discussions (FGDs). An overall prevalence of 89% was recorded for urinary schistosomiasis. Knowledge regarding risk behaviours, transmission, prevention and control of schistosomiasis were significantly improved (p=0.000) in intervention group (68.0%) compared to the control group (8.0%) after 2 months of playing the educational game. Focal group discussion shows that frequency of visits to river after games administration also reduced significantly (P=0.048) in intervention group (18.0%) compared to control the group (40.0%). This pilot study demonstrates the potential of the designed game “Schisto and Ladder™” for impacting the desired knowledge and behavioural changes among school children in endemic communities. Further testing through randomized control trials are required to fully evaluate this game.
NTD8-C10 Social mobilization and its association with treatment coverage for schistosomiasis mass drug administration in western Kenya Omedo om1, Ogutu M1, Onkanga I1, Musuva R1, Andiego K1, Awiti A1, Montgomery SP2, Evan SW2 and Mwinzi P1
1 Neglected Tropical Diseases Branch, Center for Global Health Research, Kenya Medical Research Institute, Kisumu, Kenya 2 Divisions of Parasitic Diseases and Malaria, Centers for Disease Control and Prevention, Atlanta, Georgia Introduction: Schistosomiasis remains endemic in western Kenya. Four rounds of mass drug administration (MDA) for the control have been conducted in this region by schistosomiasis consortium for operational research and evaluation (SCORE). However, achieving optimal coverage on a single round has been a great challenge and this necessitated the need for social mobilization to improve treatment coverage. While community health workers (CHWs) have always acknowledged the importance of social mobilization in improving treatment uptake, this has never been empirically evaluated from the community perspective. Hence, the aim of this study was to determine the association between social mobilization and treatment coverage following systematic social mobilization conducted before and during the intervention delivery.

76
Methods: We investigated the extent social mobilization had reached the people and the treatment uptake in a household survey by trained research assistants (RAs). Both bivariate and multivariate analysis was conducted in STATA V12 to determine the association. Statistical significance level was set at P value 0.05. Results: A total of 411 household heads (HHs) were recruited into the study of which 62.65% (n=265) took the medication. Over 95% of the HHs were aware of the MDA intervention. The main sources of information were, roadshows 44.7% (n=184), CHWs 20.68 (n=58), Radio19.22% (n=79) and village elders 15.33% (n=63). The odds of treatment uptake was significantly high amongst those who were aware of the MDA intervention odds ratio (OR) 3.1 95% CI [1.03-11.75]. There was no significant association between the source of information and treatment uptake. Over half of the respondents recommended community gatherings as future method of social mobilization while 10.64% (n=127) suggested the use of road shows. Conclusion: Treatment uptake showed significant positive association with awareness of the MDA intervention. Though there was no significance association between specific types of social mobilization methods employed with treatment uptake, roadshows had the highest reach.The future social mobilization should consider community gathering as another means of health information dissemination related to MDA and schistosomiasis.
NTD8-C11 School teacher assessments of child behavior before and after mass drug administration (MDA) with praziquantel- The SCORE project
Rosemary M. Musuva1, Martin Omedo1, Michael Ogutu1, Alphonce Awiti
Sue Binder2, Pauline N. M. Mwinzi1
1Neglected Tropical Diseases Branch, Centre for Global Health Research, Kenya Medical Research Institute, Kisumu, Kenya; 2Centers for Disease Control and Prevention, Division of Parasitic Diseases and Malaria, Atlanta, Georgia Introduction: Negative health outcomes such as impaired growth and poor cognition development among school going children are among the negative health outcomes caused by schistosomiasis. This may also be a route by which infection leads to impaired performance amongst this population because under nutrition has been shown to affect cognitive development and educational outcomes. The short-term impact of praziquantel treatment has not been evaluated systematically. The main objective was to use structured instruments to assess whether classroom behavior of school children with changes after praziquantel treatment. Methods: Six schools with the highest prevalence of schistosomiasis from the 2013 survey were recruited for the cross sectional study. Children with
77
=> 400 eggs per gram were selected with the control being children who tested negative for schistosomiasis. A total of 36 children participated in the study. (Three positive and three negative in every school). Class teachers were recruited and trained on the use of The BASC-2 tool. Baseline data (before treatment) was collected and the children observed for three weeks .The BASC-2 tool was then administered a second time Results: There was a marked difference between the baseline and after treatment data. 33% of the children showed signs of externalizing problems before treatment while only 21% tested positive after treatment. Both the intervention and control groups experienced somatization at 30% and 42% respectively, for before and after treatment. 39% of the children showed behavior problems with a majority manifesting withdrawal symptoms with 18% of them falling in the clinically significant range. After treatment this slightly improved to 24% with only 3% being clinically significant. Conclusion: It is evident that praziquantel has a positive effect on children after treatment; however, more tests that explore the parents perspectives as well as the child’s own, coupled with the socio economic status of the child’s parent need to be considered since there are many variables that can influence a child’s behavior. More follow- ups are needed to capture study and social skills
NTD8-C12 The monetary burden of cystic echinococcosis and its distribution based on gender and age in Turkana north district, Kenya Joseph Odero1, Japhet Magambo2, Eberhard Zeyhle3, Hellen Kutima1, Lynda Ndahi1, Francis Njonge1, Titus Mutwiri1, Hellen Mbaya1, Cecilia Mbae4, Erastus Mulinge4, Dorothy Kagendo1, Peter Kern5, Thomas Romig6
1. Jomo Kenyatta University of Agriculture and Technology, Nairobi, Kenya 2. Meru University of Science and Technology, Meru, Kenya 3. African Medical Research Foundation, Nairobi, Kenya 4. Kenya Medical Research Institute, Nairobi, Kenya 5. Ulm University Hospital, Ulm, Germany 6. University of Hohenheim, Stuttgart, Germany Background: Cystic Echinococcosis (CE) is caused by the larval stage of the tapeworm Echinococcus granulosus. The disease occurs worldwide, and is endemic in Turkana and Maasai areas, Kenya. The objective of the study was to assess the direct and indirect monetary burden of CE in Turkana North District, Kenya. Methodology:This study involved a retrospective review of CE patients’ medical records obtained from AMREF-Kenya (1991-2011), with patients originating from Turkana North district of Kenya. Data obtained were used to calculate CE- associated direct costs. Results:A total of 586 surgical cases treated at Kakuma Mission Hospital, Turkana, Kenya were evaluated. The ratio of infection in male to female was 1:2, with individuals in the 31-40 age groups being most prevalent.

78
The average direct cost of CE surgical treatment was US$ 703. Direct cost for 586 surgical patients, over the 20 year study period was US$ 453,154 with an average of US$ 22,658 per year. Annual indirect CE-associated monetary losses associated with lost economic opportunities amounted to US$ 4,414 for a herdsman and US$ 1,339 for a house wife. Turkana community is a nomadic pastoralist and the rural Turkana women lack formal education, their economic contribution to the family and community was evaluated on the basis of economic potential of a herdsman and a housewife. Conclusion: The results show that CE has a significant economic burden on individuals in this region. This requires immediate sustainable control measures at the definitive and intermediate hosts’ level to reduce the burden of the infection. Key words: Cystic echinococcosis, Echinococcus granulosus, Economic burden, Turkana North District-Kenya.
79
INDEX Name Abstract #
Name Abstract #
Abe, Eniola.M. B1
Kalua, Khumbo B7 Abudho, Bernard B24
Kanyi, Henry A6
Addy, Francis B28
Karanja, Diana M. S. A2;B14,15,24,25; C6; W2,3
Adebiyi A. Adeniran1 B1
Karimurio, Jefitha Key note: W
Agola, Eric B27
Kavere, Emmy A2; B24; C6
Agola, Lelo E B2
Kern, Peter A7; B16,26,27; C12
Agolla, Willis B12, B15, B17, W6
Kihara, Jimmy H. B16 Alabi, Oladimeji.M. B1
Kimani, Bridget W. B16
Aladesida, A.A. B1
King, Charles B5
Andiego, Kennedy B12, B20, C2, C4, C7, W3, W6
Kinuthia, Joseph M B2
Andiego, Kennedy C6
Kittur, Nupur A2,3; B25 Ashur, Salame A4
Korir, Harrison A2; W2
Awiti, Alphonce B17, C2, C4, C6, C7, C10, C11, W3, W6
Kutima, Hellen C12
Barassa, Ernest B7
LaBeaud, Angelle Desiree B5
Bernard, Abudho O B25
Lammie, Patrick J A6; B18 Binder, Sue C11
Lee, Yeuk-Mui A6
Bitek, A B10
Lewallen, Susan B7 Brooker, Simon Key note B
Loker, Eric S B2
Cama, Vitaliano A6
Magambo, Japhet A7; B26,27,28; C12
Chinyavu, Emily B5
Maina, Geoffrey M B2 Colley, Daniel G A2, A3, B25
Maranga, Rosebella B2
Courtright, Paul B7
Masaku, Janet B3 Dweni, Celestine K B2
Mayieka, Noah W4
Edwards, Tansy B13
Mbae, Cecilia A7; B26,27,28; C12
Eliah, Edson B7
Mbaya, Hellen B26, 28; C12 Gichangi, Michael B7
Mbugua, Amos B16
Gichuki, Paul B3
Mkoji, Gerald M A7; B2 Gitonga, Peter B27
Mogaji, Hammed.O. B1
Goodhew, E. Brook A6
Monique, Wasunna B8
Gware-Chore, Claire B23
Montegomery, Susan P
B,1214,15,1720,24; W6;C2,4,,6,7,10
Hilda, Omae B8
Morita, Kouichi A4 Jura, Walter GZO A5
Muchiri, Eric B27
Kagendo, Dorothy B27,28; C12
Muchiri, Geoffrey B6, 12,14,15, 17,20 Kakai, Osman K. B21 Muigai, Anne A4

80
Name Abstract #
Name Abstract # Mukoko, Dunstan B5,C1
Nyamogo, Nipher C3,5
Mulinge, Erastus A7, B26,27,28; C12
Ochieng, Michael B12,13 Mulonga, Boaz B19
Ochieng, Samuel B12
Murithi, David C1
Ochola, Elizabeth A3,W2 Musaki, Sandra B5
Odero, Joseph B28,C12
Musuva, Rosemary M.
C2, 4,6,7,10; B5,15,17; W3,6
Odhiambo, Gladys C3,5
Mutinda, Brian B13
Odiere, Maurice R A5,6;B6,18,24 Mutua, Alex B23
Ogara, George B24,W2
Mutuku, Francis B5
Ogembo, Brian C6 Mutuku, Martin W B2
Ogola E B10
Mutungi, Faith B3
Oguso, John W2
Mutwiri, Titus A7; B28; C12
Ogutu, Michael B15,20;C2,4,6,10,11; W3,6
Muyiemba, Gabriel W. B4
Okeyo, Seth B13
Mwangi, Ibrahim N B2
Okil , Amos A2
Mwangi, Moses B2
Okoth George K B12,15,17 Mwatha, Joseph A4
Okoyo, Collins B3
Mwende, Faith A6; C3,5
Olabinke, Dorcas.B. B1
Mwinzi, Pauline N. M.
A3,5,6; B6,12,14,15,17,18,20;W3,6; C2,4,6,7,10,11
Olayiwola, I.O. B1
Ndahi, Lynda C12
Ole Kwallah, Allan A4 Ndenga, Bryson B5
Olenja, Joyce Key Note: C
Ndombi, Eric M B25
Oluwole, Akinola.S. B1
Ndombi, Eric M. A2
Omedo, Martin B12,14,15,17,20; C2,4,6,7;10,11;W3,6
Ng'ang'a, Zipporah C1
Omollo, Raymond B13 Ngetich, Annette A5
Omollo, Truphosa B13
Njenga, Sammy A6,B3,26,27
Omondi, Amos W2
Njomo, Doris B16;C1,3,5,12
Onkanga Isaac B12,15,17,20; C2,6;W3,5,6
Njonge, Francis C12
Oruko, Enock W5
81
Name Abstract #
Name Abstract # Osei-Atweneboana, Mike Yaw Pleanary: A
Shingo, Inoue A4
Osoro E B10
Shiroko, Joan B5
Simon, Bolo B8
Owiti, Rhoda B13
Thumbi, Mwangi B10 Peter Kern B28
Vulule, John B5
Priest, Jeffrey A6
Wamae, Njeri A7
Ragot, Nicholas A4
Wanyama, Ernest Barasa B9
Rawago, Fredrick O A6, B18
Warindu J B12,15,17,20 Rinerm, Diana K. A2
Wasonga, Job W1
Romig, Thomas A7; B26,27,28; C12
Wassermann, Marion A7; B26,27,28 Sang, Huldah C. B6
Wasunna, Monique B13
Sang, Rosemary A4
Wiegand, Ryan A6;B12,14 Sawo S B15,17
Won, Kimberley A5,6; B18
Sawo, S. B15
Zeyhle, Eberhard A7; B26,27,28; C12
Secor, W. Evan
A2,6; B12,14,15,17,20,24,25; C2,4,6,7; W3,6,10
Zhang, Si-Ming B2

82
83
Congratulations to the 2013 Young Investigator Award winners
Martin Omedo
Lucy Wankuru
Nipher Nyamongo
Isaac Onkanga
Geoffrey Muchiri
Annette Imali
Copyright © Kenya Medical Research Institute, 2014
The Kenya Medical Research Institute, P. O. Box 54840-00200 Nairobi, Kenya www.kemri.org