900am dr feigenbaum strain echocardiography
TRANSCRIPT
A Practical Approach to Using Strain Echocardiography to Evaluate the Left Ventricle
Harvey Feigenbaum MD
No conflicts of interest to report
Echocardiography 2020: Opportunities and Challenges Alan S. Pearlman, MD, FASE, Editor JASE
JASE Volume 23, Issue 8, Pages 898-900, August 2010
• To me, an additional concern is that using only older “tried and true” technology is absolutely the antithesis of the exciting opportunities offered by the array of diagnostic tools available to the echocardiographer, as Dr. Zoghbi (ASE keynote address) so clearly demonstrated. If echocardiographers are to stand still, depend on standard 2D echo imaging using equipment produced a decade ago and not upgraded since, perform “ejectionfractionograms”, focus primarily on the left ventricle and simply “eyeball” the other chambers, and avoid new methods such as strain imaging and contrast echo because they are perceived as “a waste of time”, then I fear that echocardiography will be passed by. As the dinosaurs illustrated, we need to adapt and continue to evolve, or face the consequences.
Echo Assessment of Left Ventricle
• Linear dimensions: LVIDd LVIDs FS
• Areas: FAC
• Volumes: LVVd LVVs EF
• 2D Regional Wall Motion
• M-mode motion of walls, septum & valves
• Doppler measurements: Hemodynamics, MPI
• Tissue Doppler: Annular motion
• Strain and Strain Rate
Strain/Strain Rate
• The relationship between two points as if they were connected by a rubber band
• When the two points move away from each other (e.g. diastole) strain is increased (positive strain).
• When the two points move toward each other (e.g. systole) strain is decreased (negative strain).
Strain Rate
• Using tissue Doppler which is a form of pulsed Doppler, specific points in the myocardium can be identified
• Tracking these point permits the meassurement of strain
• Since Doppler is velocity or distance/time, the initial measurement is strain rate
• Integrating strain rate gives strain
L
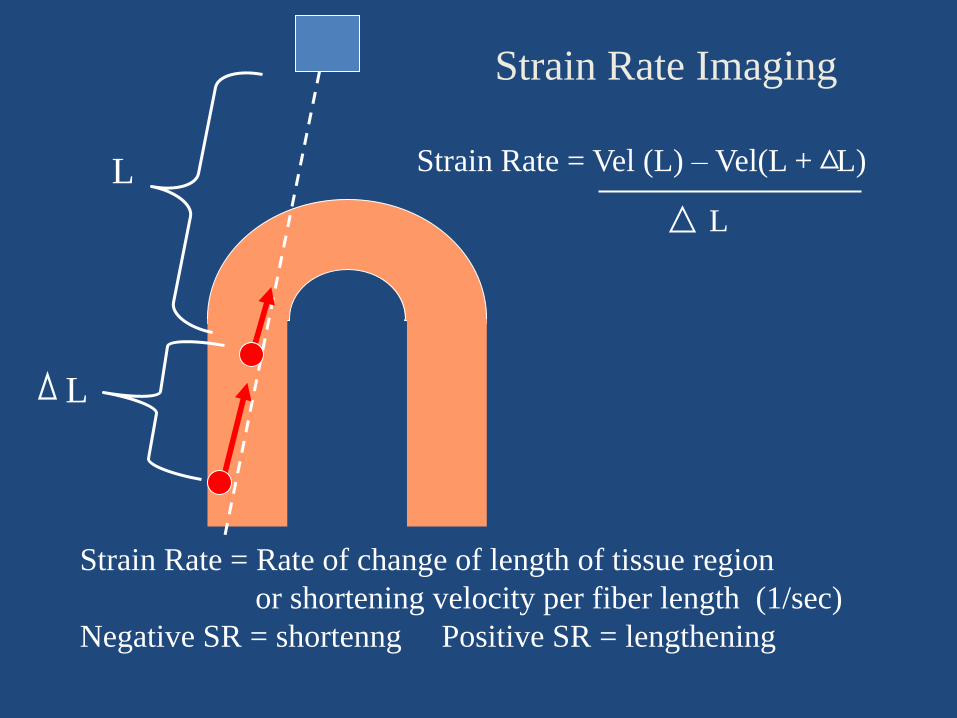
L Strain Rate = Vel (L) – Vel(L + L)
L
Strain Rate = Rate of change of length of tissue region
or shortening velocity per fiber length (1/sec)
Negative SR = shortenng Positive SR = lengthening
Strain Rate Imaging
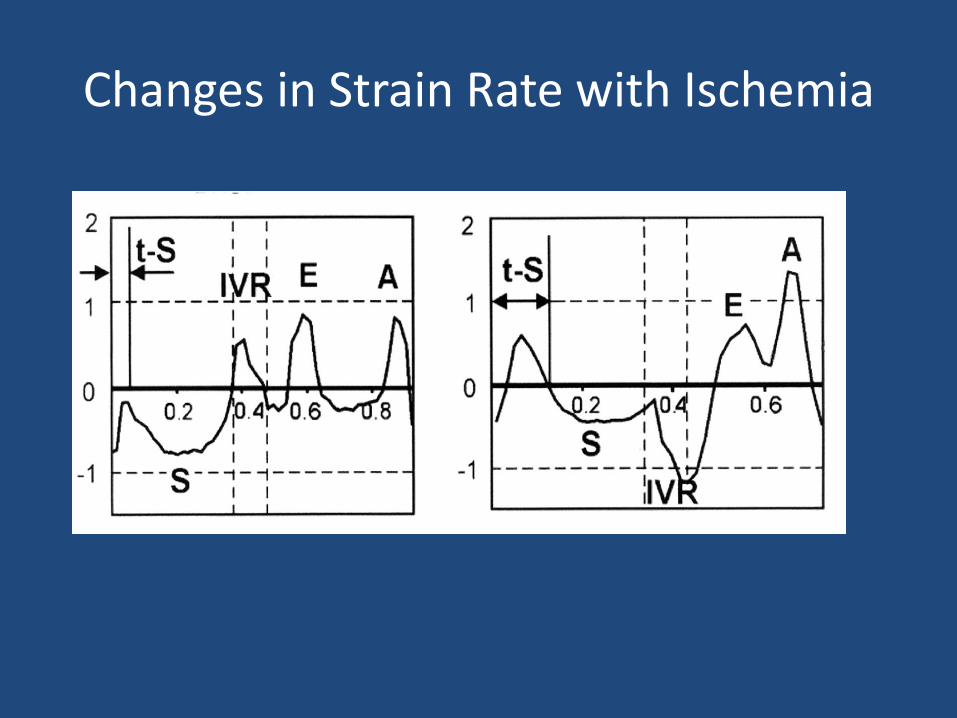
Changes in Strain Rate with Ischemia
Limitations With Doppler Based Strain Rate
• As with all Doppler applications, strain rate is angle dependent
• The Doppler strain rate sample volume is fixed while the myocardium is moving
• Strain rate is the derivative of strain and tends to be noisy
• The strain rate “curved M-mode” display is only semi quantitative, noisy, can be difficult to interpret and is not popular
Strain
2D and 3D Speckle Tracking
Speckle Tracking
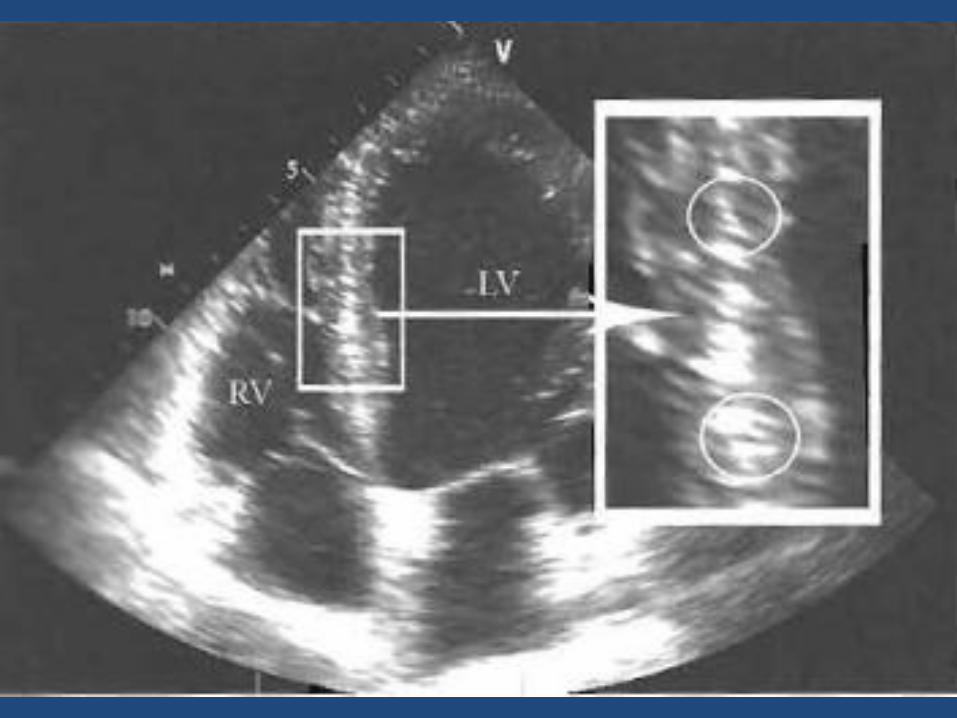
• The raw (radiofrequency or RF) ultrasonc image consists of numerous random speckles
• Any given point on an ultrasonic image can be identified by a unique speckle pattern
• Using these speckle patterns (speckle tracking) to identify specific points in the myocardium, strain can be recorded
• Since 2D echo is distance, the initial measurement is strain
• The derivative of strain will give strain rate
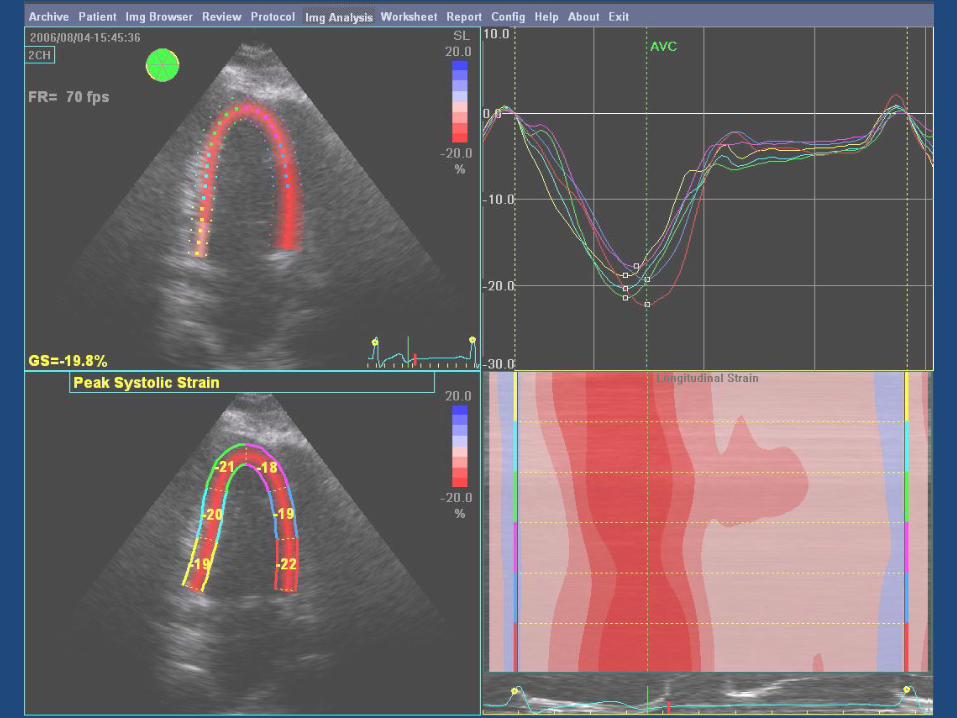
Normal Strain Displays
Quantitative Parametric Overlay
Wave Forms
Curved M-mode
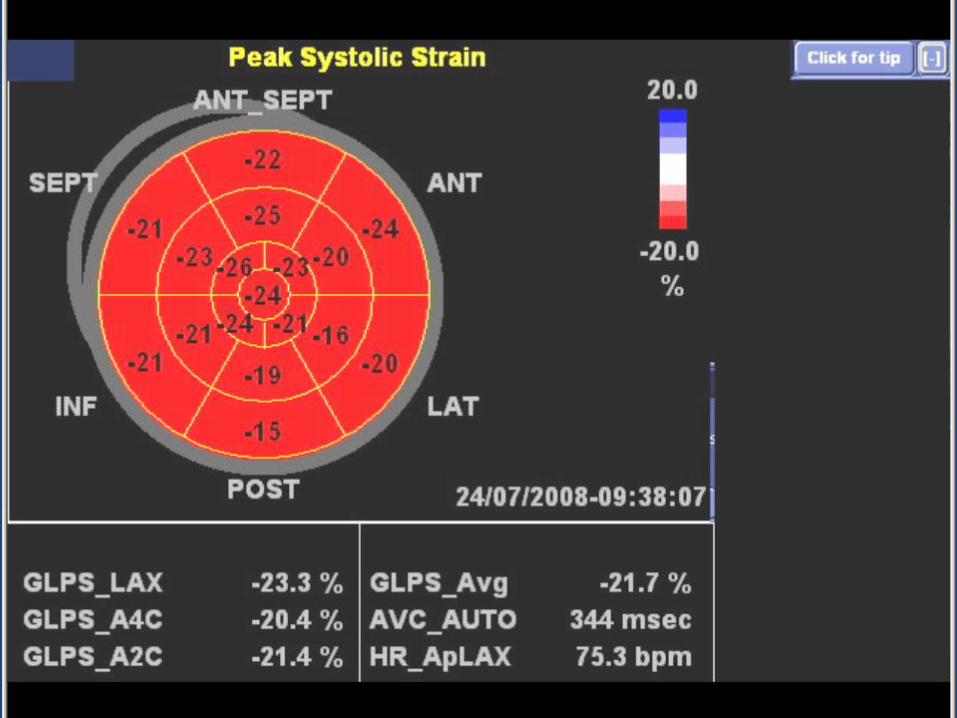
Normal Strain
Bullseye Presentation (base of LV outer ring, apex at center)
All segments red and all but one in upper teens or 20’s
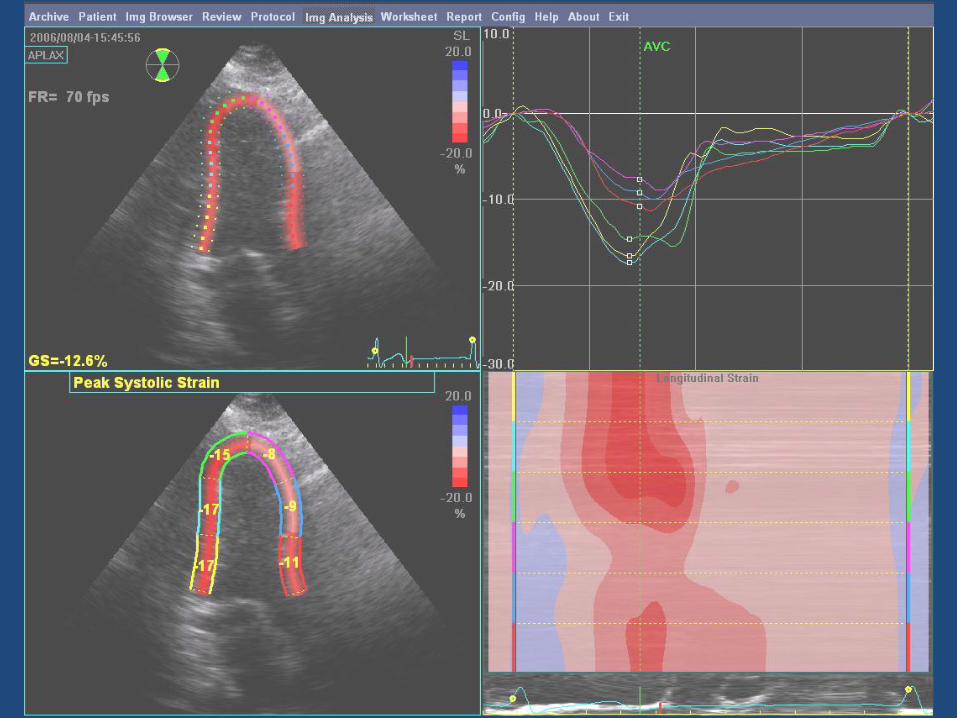
Abnormal Strain
Quantitative Parametric Overlay
Wave Forms
Curved M-mode
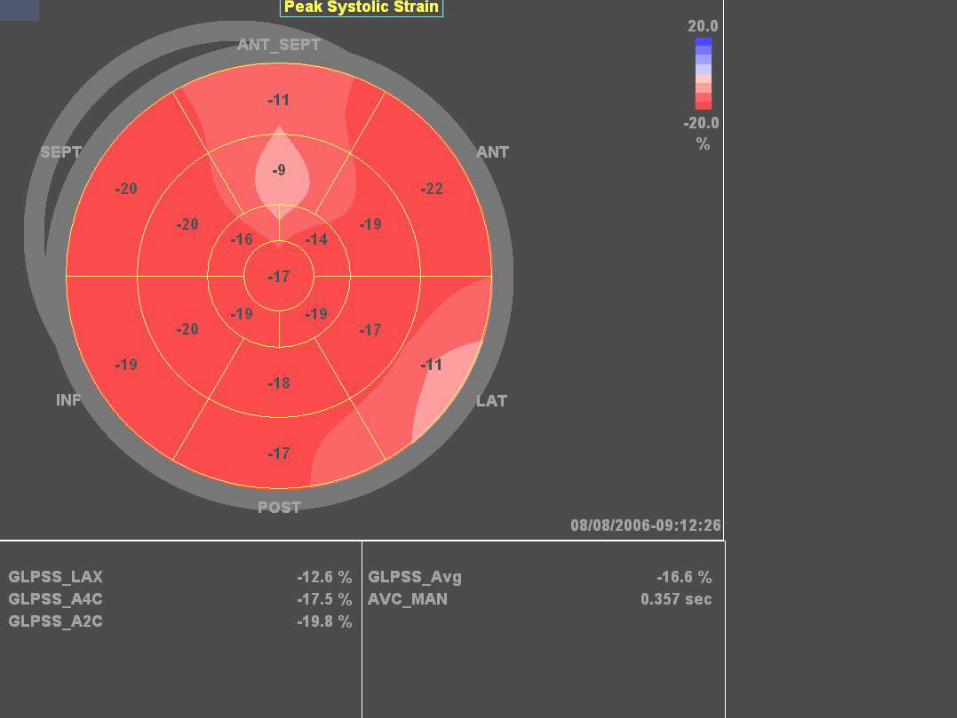
Abnormal Strain
Bullseye presentation
Several segments light red or pink and of lower values
Advantages of Strain/Strain Rate Imaging
• Avoids some of the limitations of wall motion analysis: tethering, off-axis false positive, subtle wall motion
• More sensitive in detecting myocardial dysfunction
• Quantitative
• Technically feasible with stress
• Closer to assessing true regional contraction than is wall motion or Tissue Doppler
• May assist in assessing viability with stress and at rest
• Represents an independent supplement to wall motion for LV mechanics
Longitudinal strain is a great tool to evaluate the real systolic function especially
in cases like HCM. This population appears to have a normal EF but the global
longitudinal strain is decreased (<-20%). I have to clarify that the strain is best
when is obtained by tissue tracking and not by the TDI. The speckle tissue
tracking is reproducible and has less intraobserver and interobserver variability.
Also the RV systolic function can be assess by longitudinal strain. This
information is important in pulmonary HTN, RV infarct, pulmonary embolism,
ARVD, systemic RV, TOF, etc.
Like every other emerging tool the secret is to put it in practice and master it!.
Strain analysis has opened the window to evaluate the myocardium inside out.
Start using it and be amazed.
Maria Alexandra Pernetz RDCS, RVT
Echo lab Technical Director
Emory University Hospital
ASE Open Forum
Current Status of Strain Echocardiography
• Hundreds of articles over the past 10 years have demonstrated the feasibility and potential clinical value of strain imaging
• Yet only a few academic centers have incorporated it into the everyday practice of echocardiography and even then only on a limited basis
•Noninvasive myocardial strain measurement by speckle tracking echocardiography:
• validation against sonomicrometry and tagged magnetic resonance imaging. •Amundsen BH, Helle-Valle T, Edvardsen T, Torp H, Crosby J, Lyseggen E et al.
•J Am Coll Cardiol 2006;47(4):789-93.
•The potential clinical role of strain and strain rate imaging in diagnosing
•acute rejection after heart transplantation. •Marciniak A, Eroglu E, Marciniak M. et al.
•Eur J Echocardiogr 2007;8(3):213-21.
Early detection of doxorubicin cardiomyopathy using two-dimensional strain
echocardiography. Migrino RQ, Aggarwal D, Konorev E et al.
Ultrasound Med Biol 2007;Oct 10;
•Myocardial strain imaging for early detection of cardiac involvement in patients
•with Duchenne’s progressive muscular dystrophy. •Mori K, Hayabuchi Y, Inoue M et al.
•Echocardiography 2007;24(6):598-608.
•Detection of subclinical cardiac involvement in systemic sclerosis
•by echocardiographic strain imaging. •Kepez A, Akdogan A, Sade LE et al.
•Echocardiography 2008;25:191-97.
•Association of myocardial strain with left ventricular
•geometry and progression of hypertensive heart disease.
•Hare JL, Brown JK, Marwick TH.
• Am J Cardiol 2008;102(1):87-91.
Partial List of References Demonstrating the Value of Echocardiographic Strain in Patients With Known or Suspected Heart Disease
Global 2-Dimensional Strain as a New Prognosticator in Patients With Heart Failure
• Goo-Yeong Cho, MD, PhD*,*, Thomas H. Marwick, MD, PhD, Hyun-Sook
Kim, MD, PhD, Min-Kyu Kim, MD, Kyung-Soon Hong, MD, PhD and Dong-Jin Oh, MD, PhD J Am Coll Cardiol, 2009; 54:618-624
• Conclusions: Strain is a powerful predictor of cardiac events and appears to be a better parameter than ejection fraction in patients with acute heart failure.

Global Longitudinal Strain as a Major
Predictor of Cardiac Events in Patients
with Depressed Left Ventricular
Function: A Multicenter Study
Erwan Donal, MD, PhDc, Amira Zaroui, MDa, Patricia Reant, MDa, Adrien Salem, MDb, Cecile Hamon, MDc, Severine Monzy, MDa, Raymond Roudaut, MD, PhDa, Gilbert Habib, MD, PhDb, Stéphane Lafitte, MD, PhDa
Lafitte, MD, PhDa
J Am Soc Echocardiogr Volume 23 Pages
1019-1024 October 2010
Strain assessment is highly feasible and
reliable in patients with LV dysfunction and
allows for cardiovascular risk stratification in
patients with heart failure with greater
accuracy than LV EF
Prediction of All-Cause Mortality From Global Longitudinal Speckle Strain Comparison With Ejection Fraction and Wall Motion Scoring
Stanton, Leano and Marwick Circulation Cardiovascular Imaging 2009;2:356-64
Of 546 consecutive individuals undergoing echocardiography for assessment of
resting left ventricular function, 91 died over a period of 5.2±1.5 years. In
addition to Simpson biplane EF, WMSI was determined by 2 experienced
readers and GLS was calculated from 3 standard apical views using 2D speckle
tracking. The incremental value of EF, WMSI, and GLS to significant clinical
variables was assessed in nested Cox models. Clinical factors associated with
outcome (model χ2=20.2) were age (hazard ratio [HR], 1.46; P<0.01), diabetes
(HR, 1.88; P=0.01), and hypertension (HR, 1.59; P<0.05). Although addition of
EF (HR, 1.23; P=0.03) or WMSI (HR, 1.28; P<0.01) added to the predictive
power of clinical variables, the addition of GLS (HR, 1.45; P<0.001) caused the
greatest increment in model power (χ2=34.9, P<0.001). GLS also provided
incremental value in subgroups with EF >35% and those with and without wall
motion abnormalities. A GLS ≥−12% was found to be equivalent to an EF ≤35%
for the prediction of prognosis. Intraobserver and interobserver variations for EF
and GLS were similar.
Conclusions— GLS is a superior predictor of outcome to either EF or WMSI
and may become the optimal method for assessment of global left ventricular
systolic function.
Why Isn’t Strain Echocardiography Being Used More Clinically
• Most articles in the literature use strain in time consuming and complicated ways
• There is longitudinal, radial, circumferential and twist all of which makes clinical use complicated
• “Deformation” may be scientifically accurate but is clinically confusing
• Analyzing multiple wave forms is not appealing • The fact that systolic strain or “contraction” is a
negative number is confusing e.g. is a strain of -10 more or less than a strain of -20?
Simplified More Practical Approach to Strain
Echocardiography
• We avoid manually adjusting the sampling of segments to quicken the analysis and enhance the reproducibility
• The “Bullseye “ presentation is the primary display for analysis
• Systolic strain is stated as a positive number
• Only longitudinal systolic strain is utilized
• Global strain is labeled “Global Systolic Strain (GSS)” instead of “Global Longitudinal Peak Systolic Strain (GLPSS)” or “Global Longitudinal Peak Strain Average (GLPS-A)”
• Basal Systolic strain (BSS), Mid Systolic Strain (MSS) and Apical Systolic Strain (APSS) are calculated
• The “Bullseye “ is analyzed by pattern recognition as well as quantitation
Current Status of Strain Echocardiography at IU/UH/WMH
• Over 3,000 studies done at the three institutions
• Success rate is still unclear but is at least approximately 80-85% (average patient >200 lb and many >250 lb)
• Takes 2-4 minutes to generate the strain data
• Intraobserver and interobserver reproducibility as good or better that EF
Strain Echocardiography
Bullseye Patterns
Concentric Hypertrophy
There is a Need to Identify People With Hypertension
Cardiac LVH indicates significant hypertension that is affecting the
heart
Nearly 20% Of Young Adults In US May Have High Blood Pressure.
ABC World News (5/25, story 6, 0:25, Sawyer) reported that research published online in Epidemiology indicates that nearly
one-fifth "of Americans who are 24 to 32 years old have high blood pressure."
USA Today (5/26, Marcus) reports, "For the National Longitudinal Study of Adolescent Health, dubbed Add Health, funded by
the National Institutes of Health, researchers from the University of North Carolina-Chapel Hill asked 14,000 men and women between
the ages of 24 and 32 about their high blood pressure history and then took blood pressure readings of participants." The investigators
"found that 19% of participants had high blood pressure." These "findings...are significantly higher than other recent research from another
large, ongoing health study, the National Health and Nutrition Examination Survey (NHANES), which found only 4% of adults 20 to 39 have high blood pressure."
The CNN (5/25) "The Chart" blog reported that lead study author Kathleen Mullan Harris said that "among those measured with high
blood pressure, only 25% had been told previously that they had high blood pressure."
Also covering the story were the Raleigh News & Observer (5/26, Price), Reuters (5/26, Steenhuysen), WebMD (5/25, Mann), HealthDay (5/25, Dallas), and MedPage Today (5/25, Neale).
Masked Hypertension May Be Prevalent In 45% Of African Americans. HeartWire (5/25, O'Riordan) reported that research "presented this week" at the American Society of Hypertension 2011 Scientific Meeting “
confirm the high prevalence of masked hypertension in African Americans, with investigators reporting that masked hypertension is prevalent in
45% of African Americans during any single office visit." The findings "suggest that blood-pressure monitoring in the office might not be
sufficient to assess cardiovascular-risk exposure in this population and that out-of-office blood pressure monitoring might be
needed to expose underlying hypertension
Nearly 20% Of Young Adults In US May Have High Blood Pressure.
ABC World News (5/25, story 6, 0:25, Sawyer) reported that research published online
in Epidemiology indicates that nearly one-fifth "of Americans who are 24 to 32 years
old have high blood pressure."
USA Today (5/26, Marcus) reports, "For the National Longitudinal Study of
Adolescent Health, dubbed Add Health, funded by the National Institutes of Health,
researchers from the University of North Carolina-Chapel Hill asked 14,000 men and
women between the ages of 24 and 32 about their high blood pressure history and
then took blood pressure readings of participants." The investigators "found that 19%
of participants had high blood pressure." These "findings...are significantly higher than
other recent research from another large, ongoing health study, the National Health
and Nutrition Examination Survey (NHANES), which found only 4% of adults 20 to 39
have high blood pressure."
Masked Hypertension May Be Prevalent In 45% Of African Americans.
HeartWire (5/25, O'Riordan) reported that research "presented this week" at the
American Society of Hypertension 2011 Scientific Meeting "confirm the high
prevalence of masked hypertension in African Americans, with investigators reporting
that masked hypertension is prevalent in 45% of African Americans during any single
office visit." The findings "suggest that blood-pressure monitoring in the office might
not be sufficient to assess cardiovascular-risk exposure in this population and that out-
of-office blood pressure monitoring might be needed to expose underlying
hypertension."
Strain Presentation of LV Hypertrophy
• Basal strain segments decrease (become light red or pink)
• BSS below 17
• Apical segments remain normal
• Strain bullseye “donut”
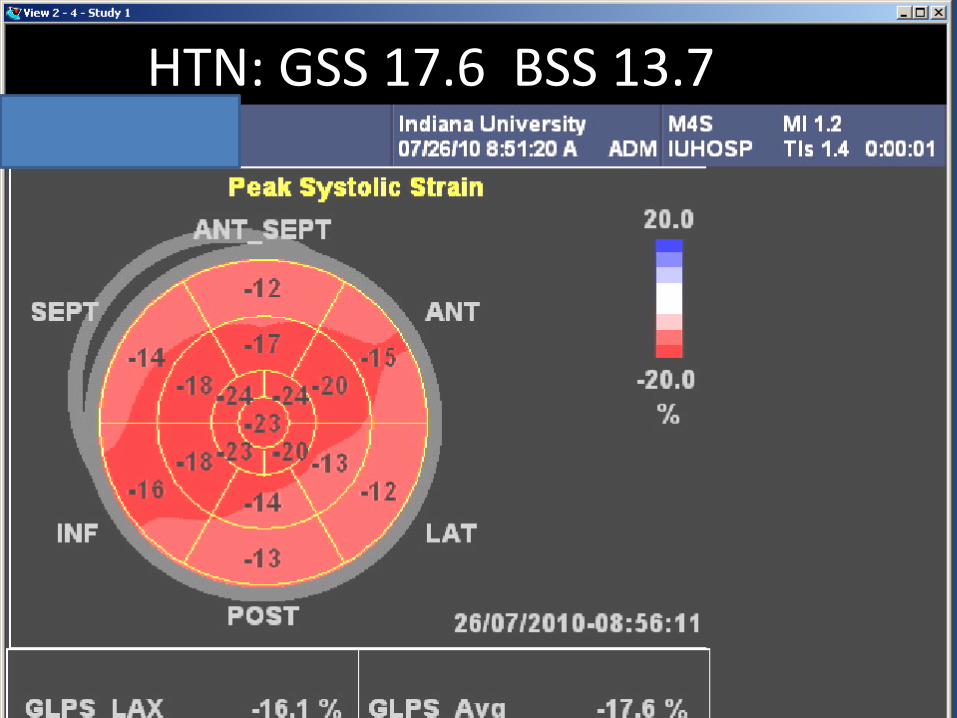
HTN: GSS 17.6 BSS 13.7
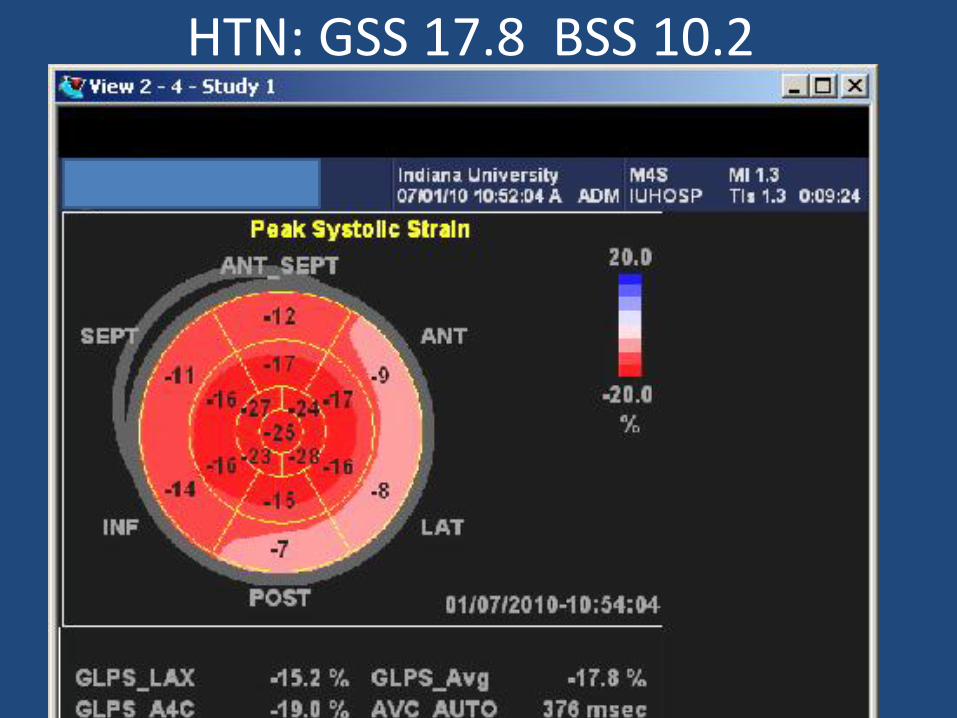
HTN: GSS 17.8 BSS 10.2
Hypertrophic Cardiomyopathy
Septal Strain Segments Decrease in Value (become pink)
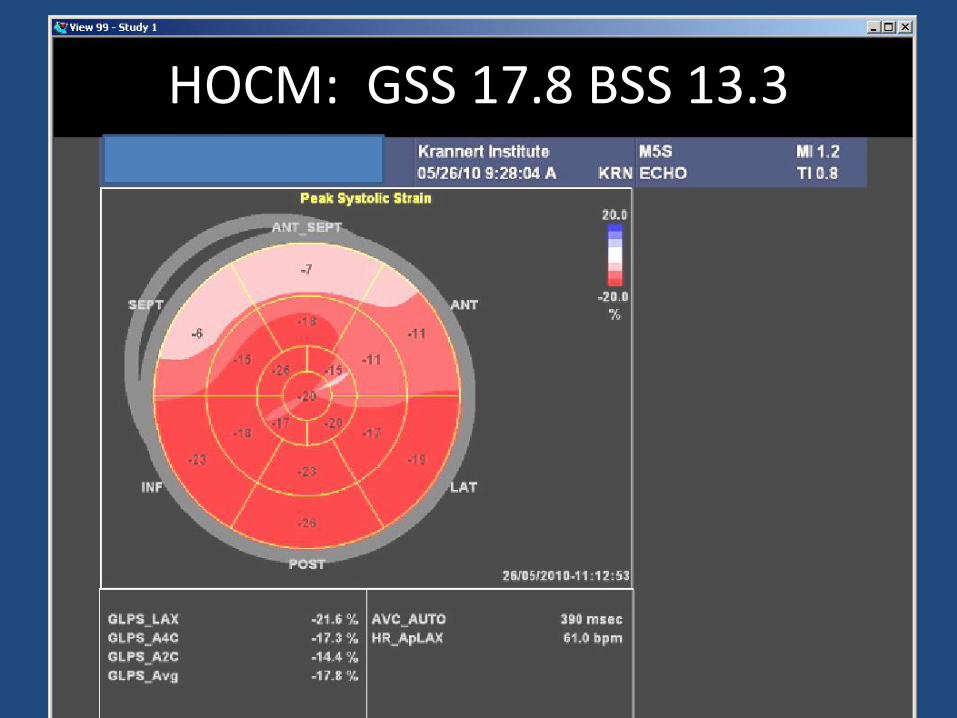
HOCM: GSS 17.8 BSS 13.3
Amyloidosis
Extreme Form of Strain LVH Pattern
Severe Amyloid Heart
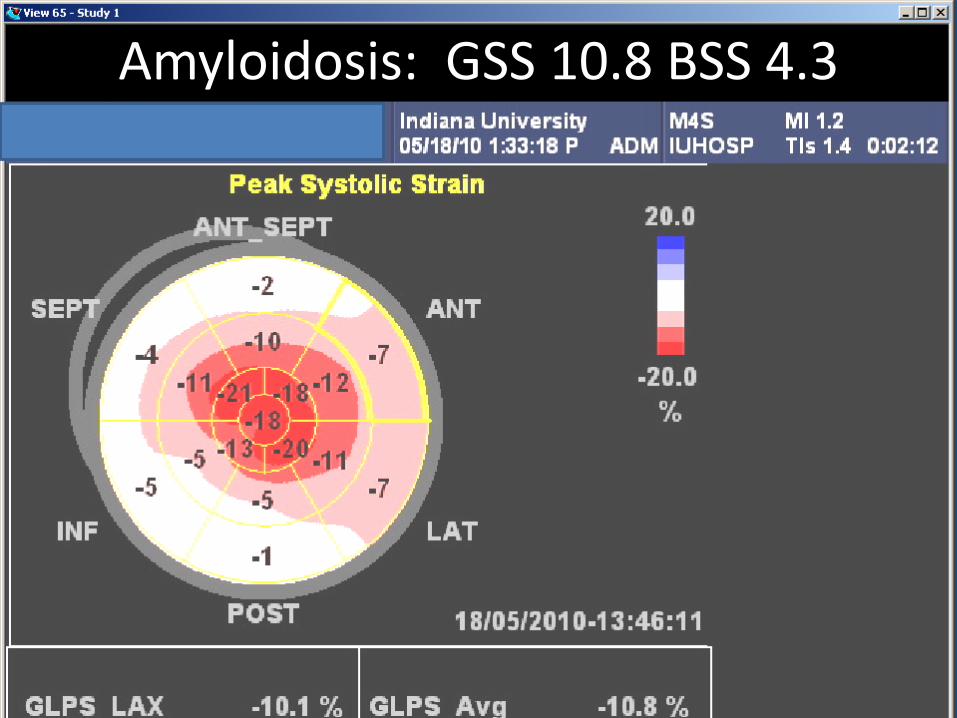
Amyloidosis: GSS 10.8 BSS 4.3
Less Severe Amyloid Heart
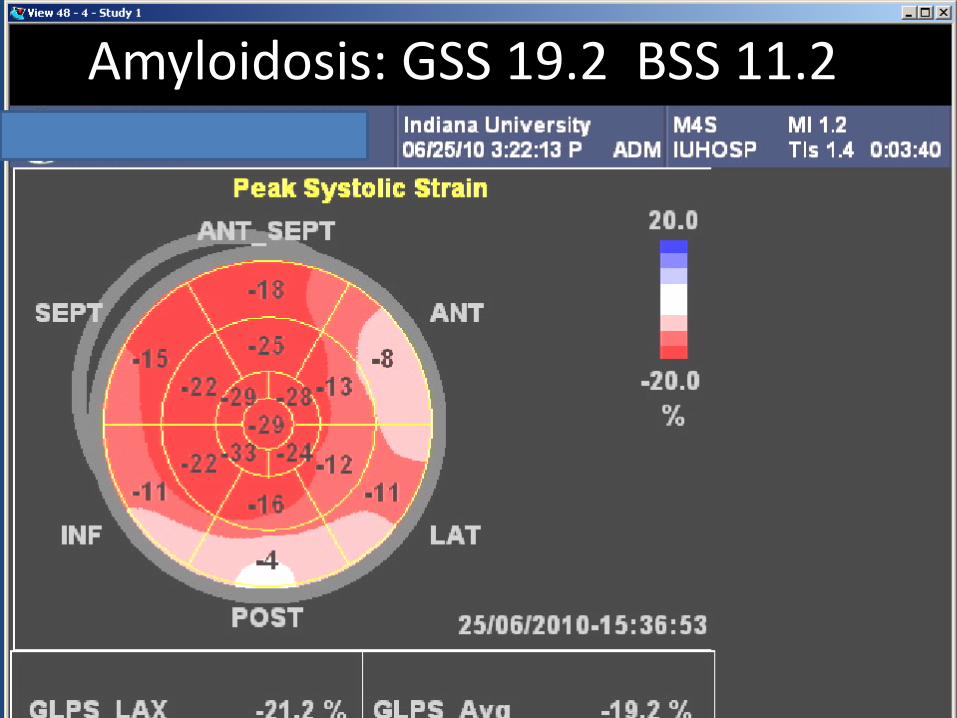
Amyloidosis: GSS 19.2 BSS 11.2
2D Images of Amyloid Heart
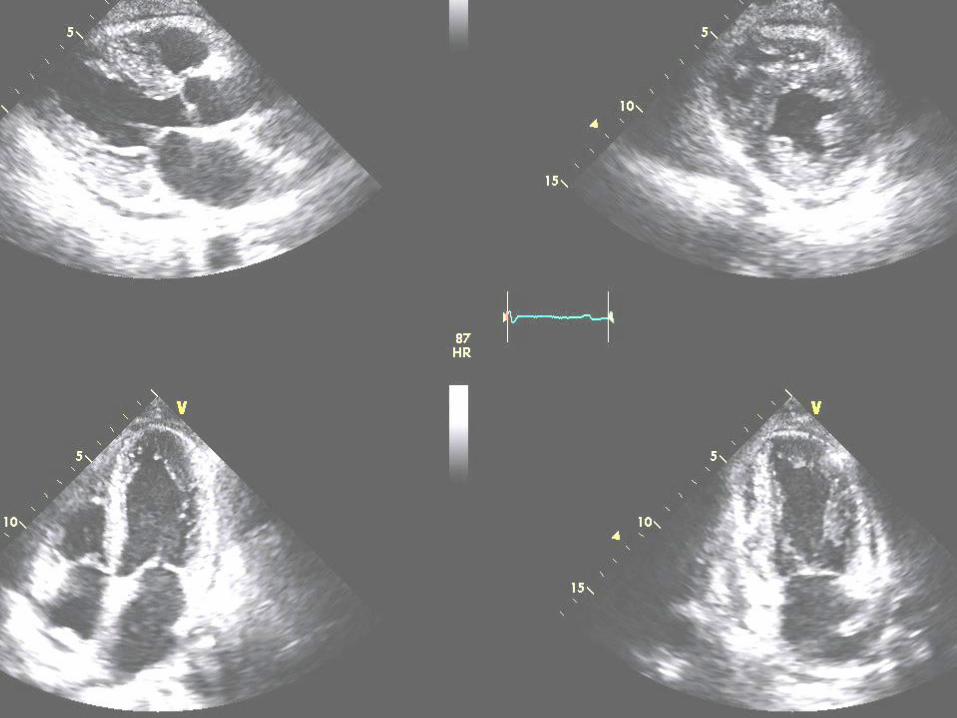
Same Patient One Year Later
Is there any change?
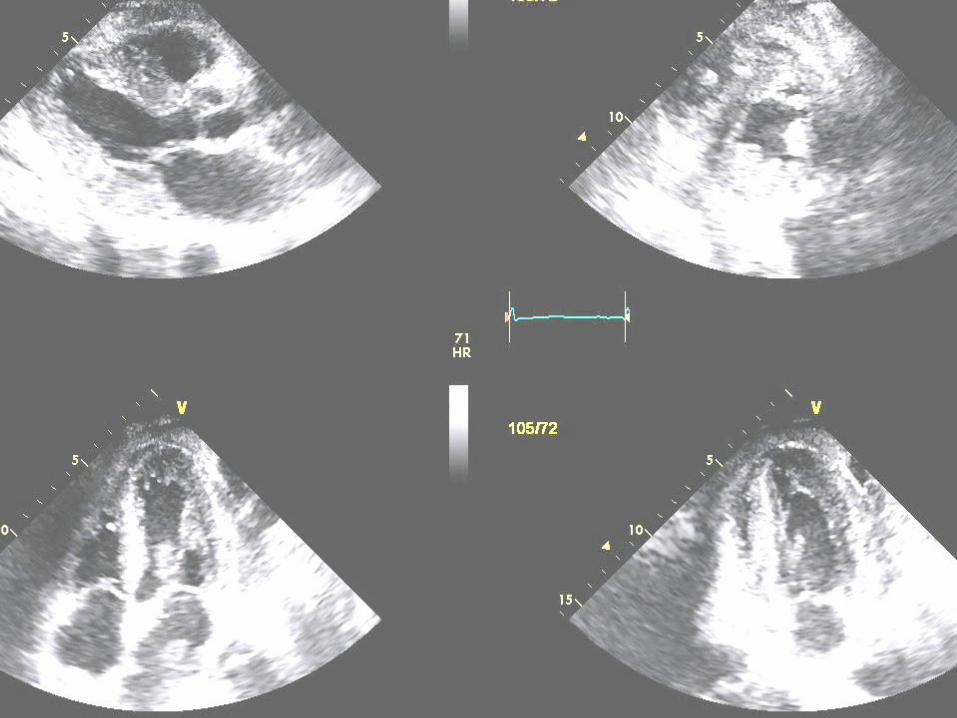
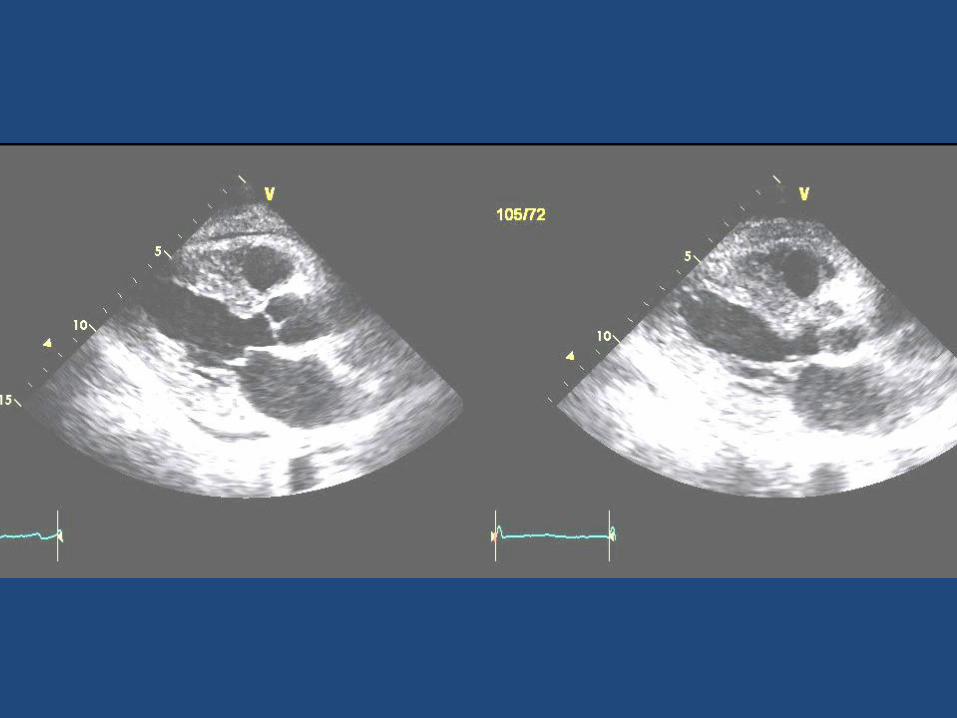
Strain Bullseye of the Same Amyloid Heart Images
The change in strain is not as subtle as the change in wall thickness
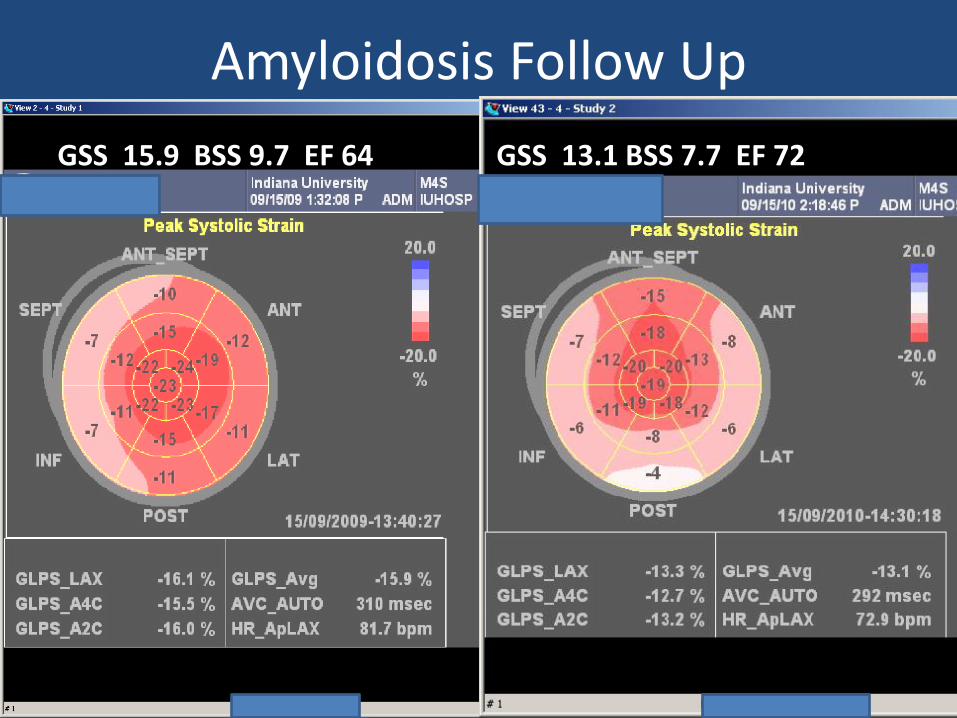
Amyloidosis Follow Up
GSS 15.9 BSS 9.7 EF 64
GSS 13.1 BSS 7.7 EF 72
Inferior Lateral Ischemia
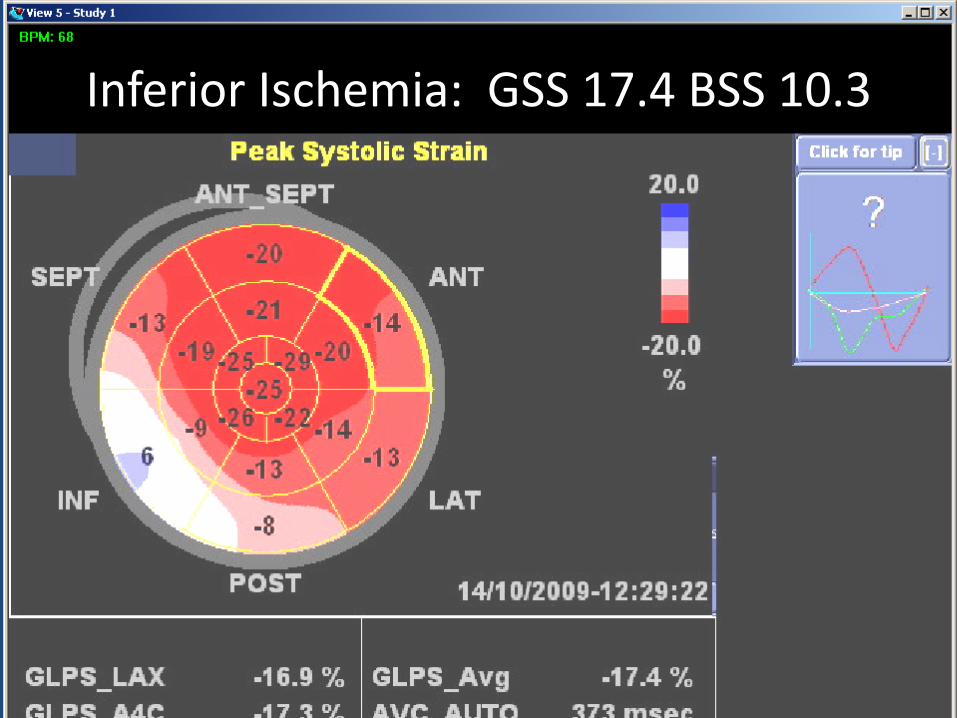
Inferior Ischemia: GSS 17.4 BSS 10.3
LAD Ischemia
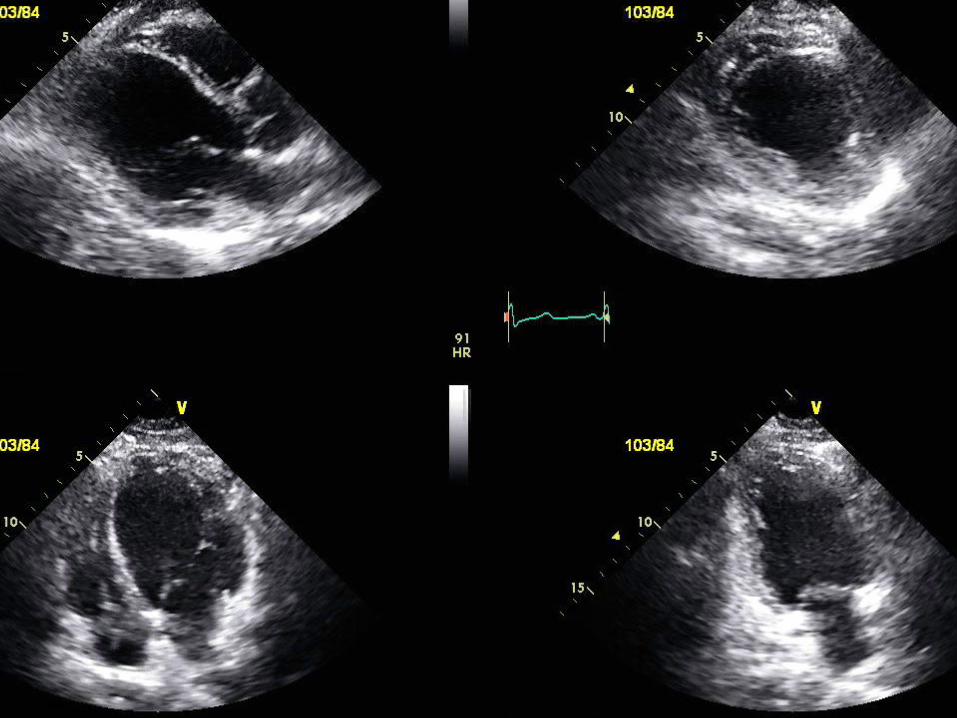
Strain of Same Patient
Numerous segments likely nonviable
(strain <10)
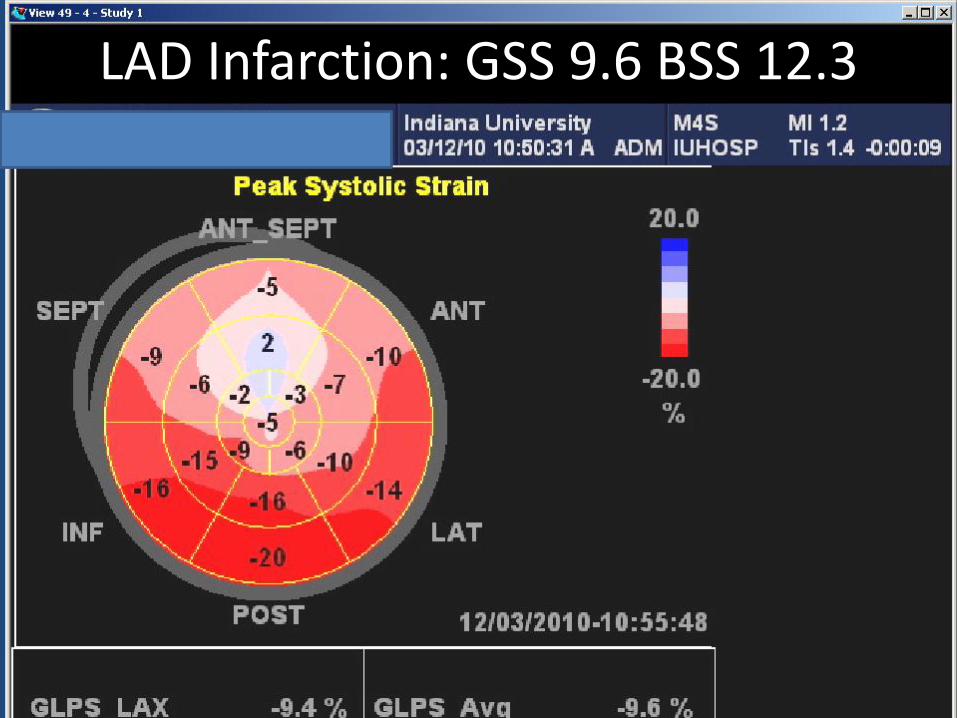
LAD Infarction: GSS 9.6 BSS 12.3
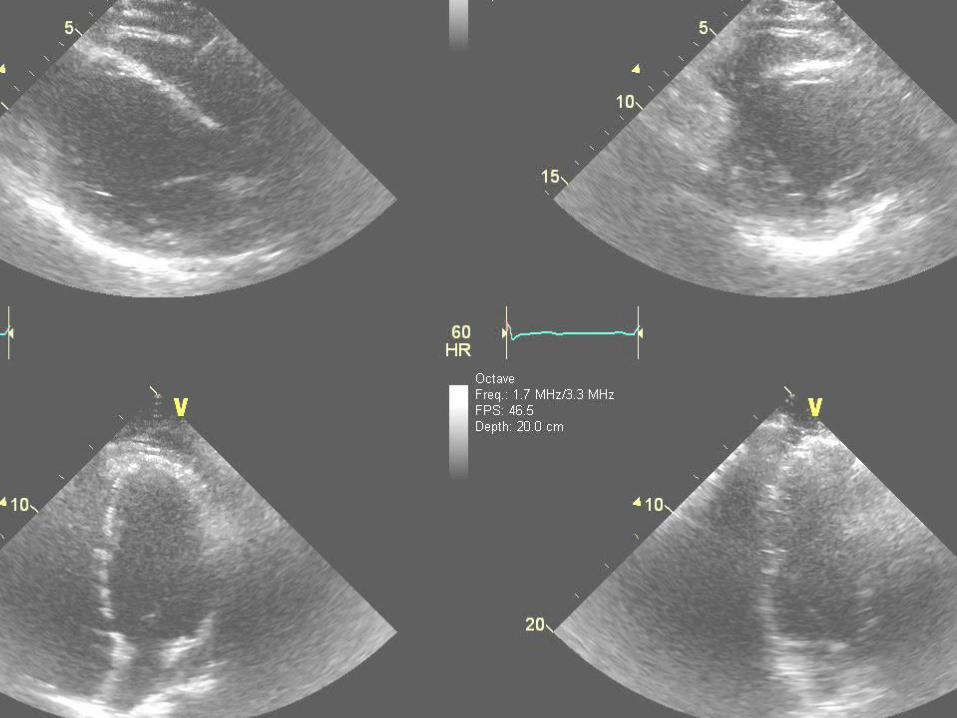
Another Patient with Anterior Myocardial Infarction
2D images very similar
Strain Abnormalities Not nearly as Severe or Extensive
Fewer segments likely nonviable (strain < 10)
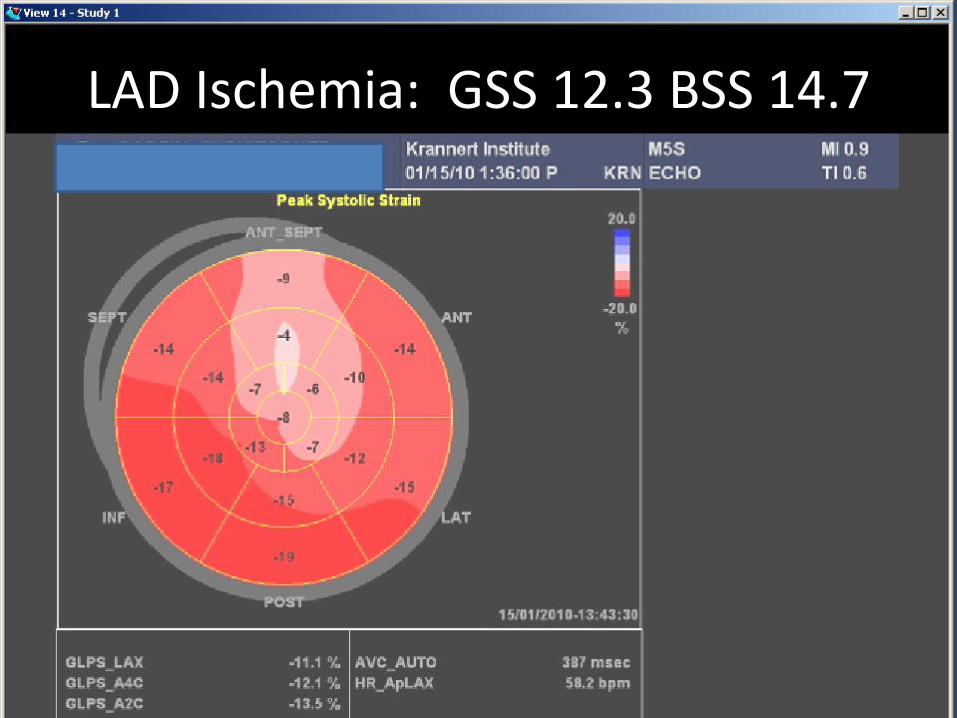
LAD Ischemia: GSS 12.3 BSS 14.7
Patient asymptomatic leading very active life
EF 38% but exercised over 10 mets on treadmill
Nonischemic Cardiomyopathy
Abnormal strain segments do not fit a coronary artery distribution
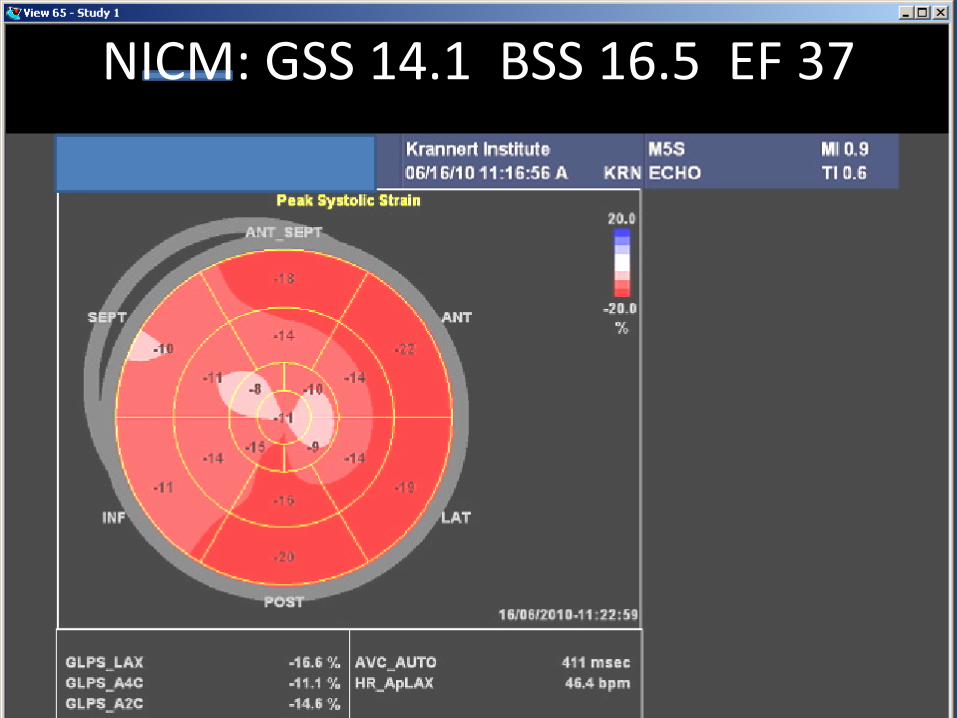
NICM: GSS 14.1 BSS 16.5 EF 37
Patient With More Severe Cardiomyopathy
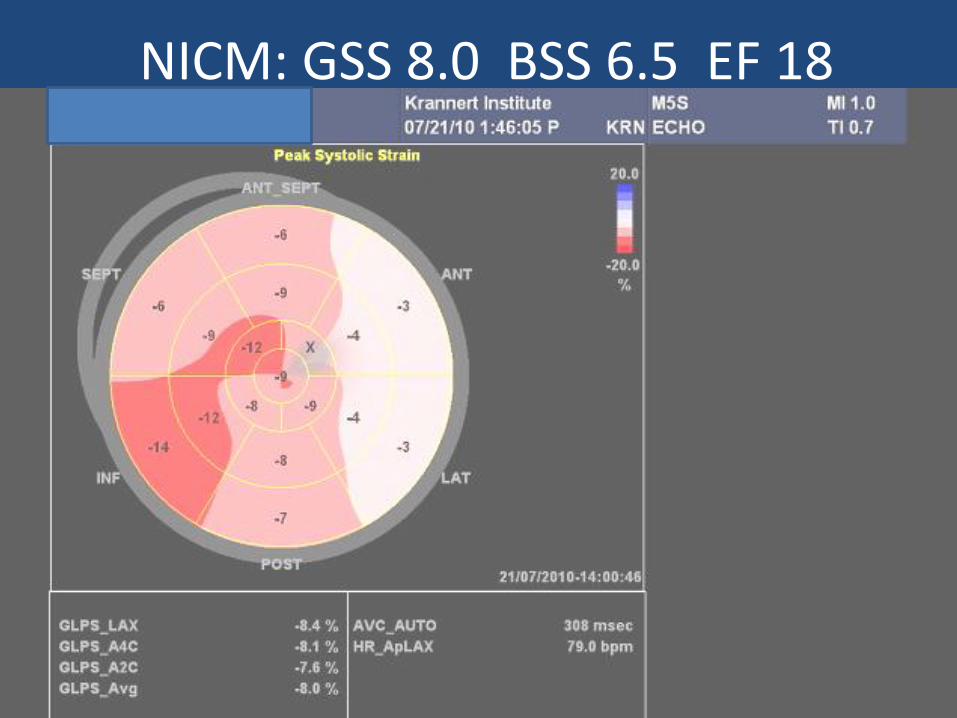
NICM: GSS 8.0 BSS 6.5 EF 18

Post Chemotherapy
Growing Awareness Of Cardiovascular Adverse Effects Of
Anticancer Drugs Spawns New Clinical Discipline.
Medscape (10/7, Chustecka) reported, "Growing awareness of the
cardiovascular adverse effects of anticancer drugs, plus the fact
that cancer patients are surviving and living longer, has given
birth to the new clinical discipline of cardioncology." According
to a paperrin Progress in Cardiovascular Disease, "patients with
early-stage breast cancer are now more likely to die from heart
disease than cancer, highlighting the need for a new discipline
that focuses on the treatment of cardiovascular disease in cancer
patients. The special issue of the journal celebrates the first year
of existence of the International Society of Cardioncology."
, has given birth to the new clinical discipline of cardioncology." According to a paper in Progress in Cardiovascular Disease, "patients with early-stage breast cancer are now more likely to die from heart disease than cancer, highlighting the need for a new discipline that focuses on the treatment of cardiovascular disease in cancer patients. The special issue of the journal celebrates the first year of existence of the International Society of Cardioncology."

Guidelines To Manage Heart Disease Risk In Cancer Patients Expected In 2012.
HeartWire (10/13, O'Riordan) reports, "The American Society of Echocardiography is
currently working on new guidelines to manage the risk of heart disease in cancer
patients." These "recommendations will guide clinicians in using strain echocardiography
in the early detection of cardiac toxicity resulting from therapies used to treat cancer,
such as doxorubicin and trastuzumab in breast-cancer patients with the HER2 genetic
mutation." HeartWire points out that "the new guidelines...expected in 2012, will be
written in collaboration with the European Association of Echocardiography and the
American Society of Clinical Oncology."
Reproducibility Study
• 43 year old breast cancer patient
• On continuous chemotherapy
• Echocardiograms with strain
• 2/17/2010
• 5/14/2010
• 3/14/2011
• 9/18/2011
All Strain Studies Essentially Normal and Unchanged

Frequent Effect of Chemotherapy on Strain
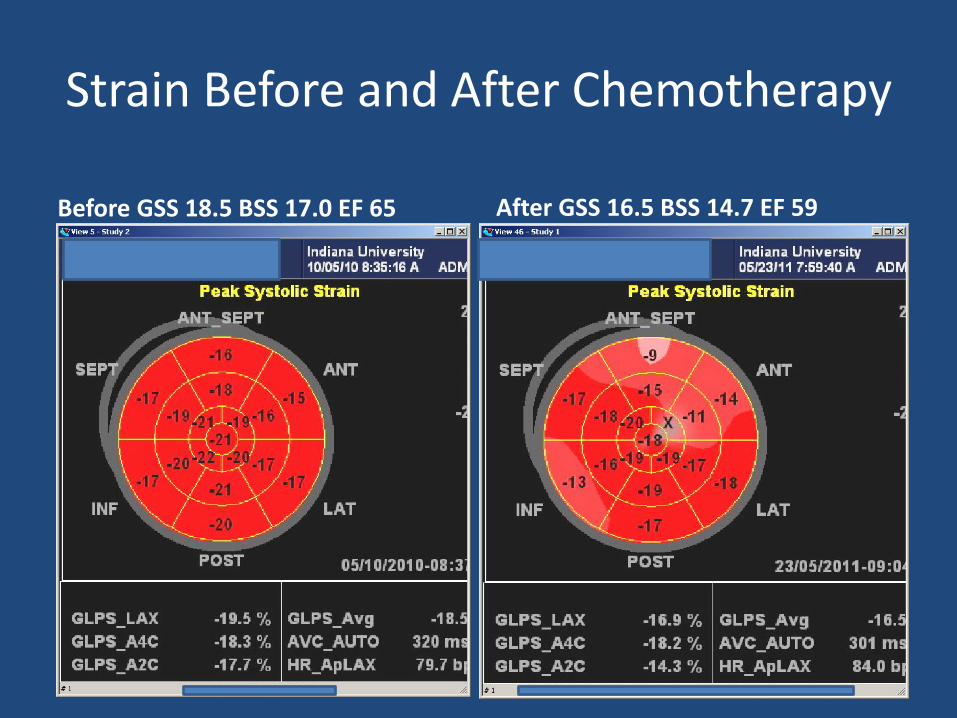
Strain Before and After Chemotherapy
Before GSS 18.5 BSS 17.0 EF 65 After GSS 16.5 BSS 14.7 EF 59
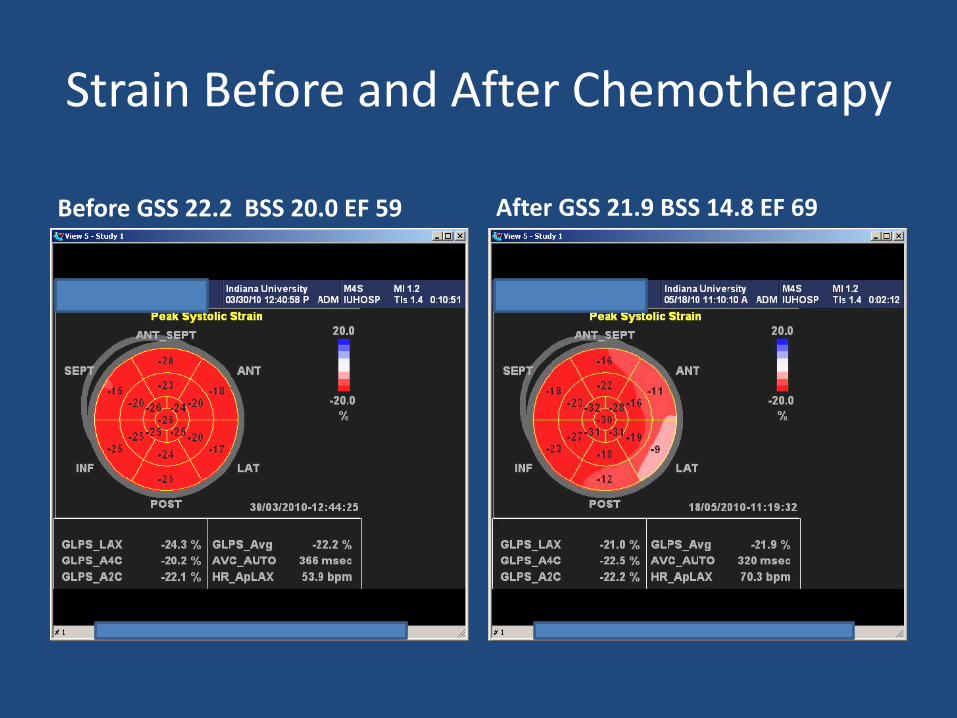
Strain Before and After Chemotherapy
Before GSS 22.2 BSS 20.0 EF 59 After GSS 21.9 BSS 14.8 EF 69
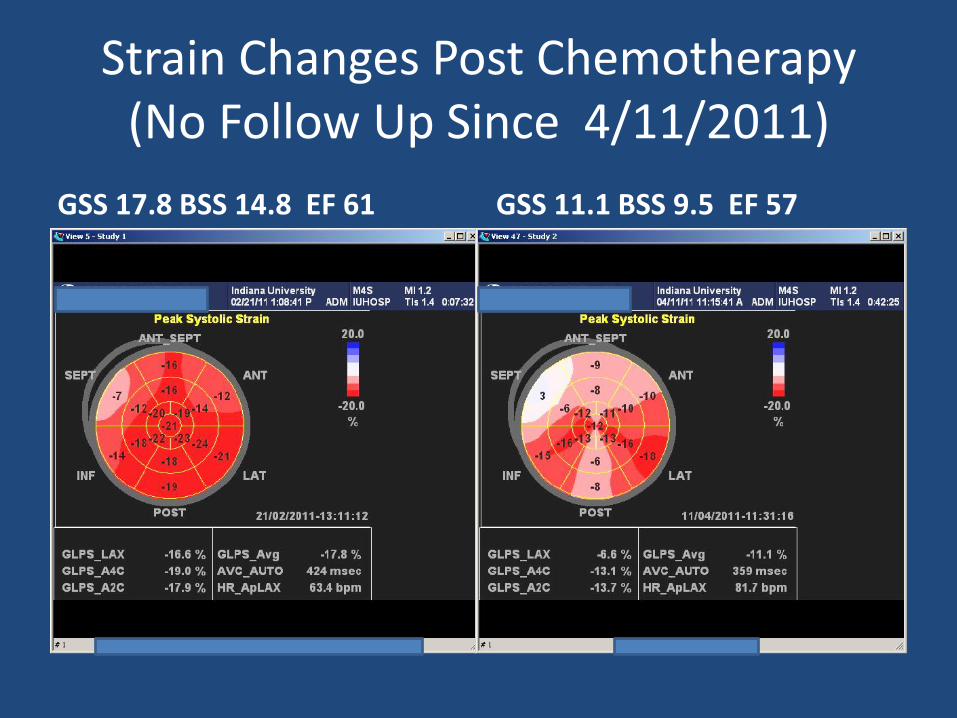
Strain Changes Post Chemotherapy (No Follow Up Since 4/11/2011)
GSS 17.8 BSS 14.8 EF 61 GSS 11.1 BSS 9.5 EF 57
Abnormal Strain is Reversible
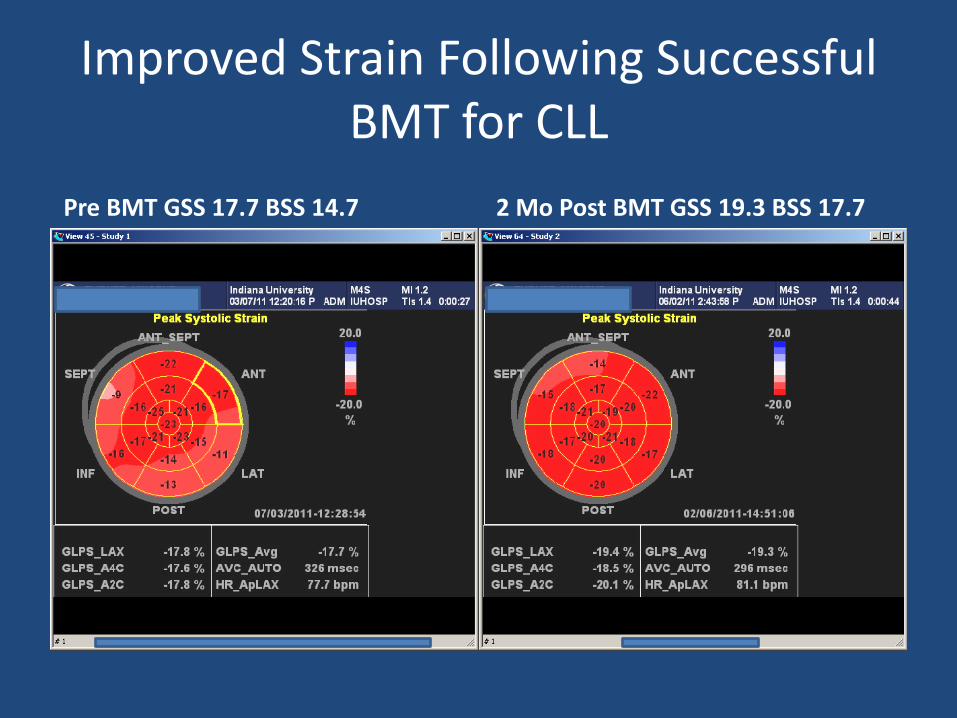
Improved Strain Following Successful BMT for CLL
Pre BMT GSS 17.7 BSS 14.7 2 Mo Post BMT GSS 19.3 BSS 17.7
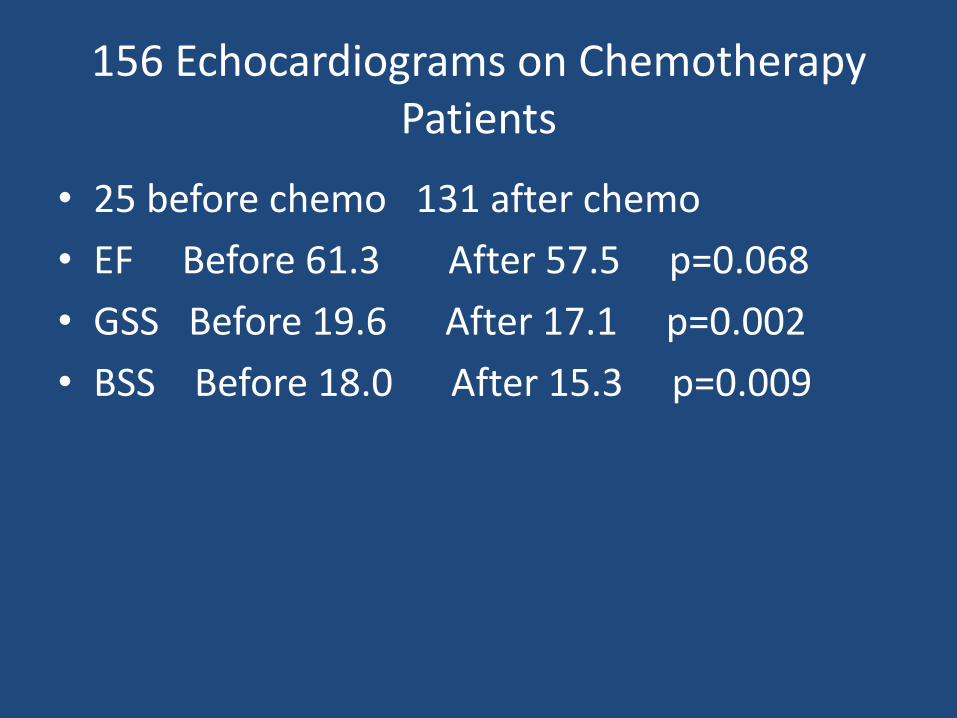
156 Echocardiograms on Chemotherapy Patients
• 25 before chemo 131 after chemo
• EF Before 61.3 After 57.5 p=0.068
• GSS Before 19.6 After 17.1 p=0.002
• BSS Before 18.0 After 15.3 p=0.009
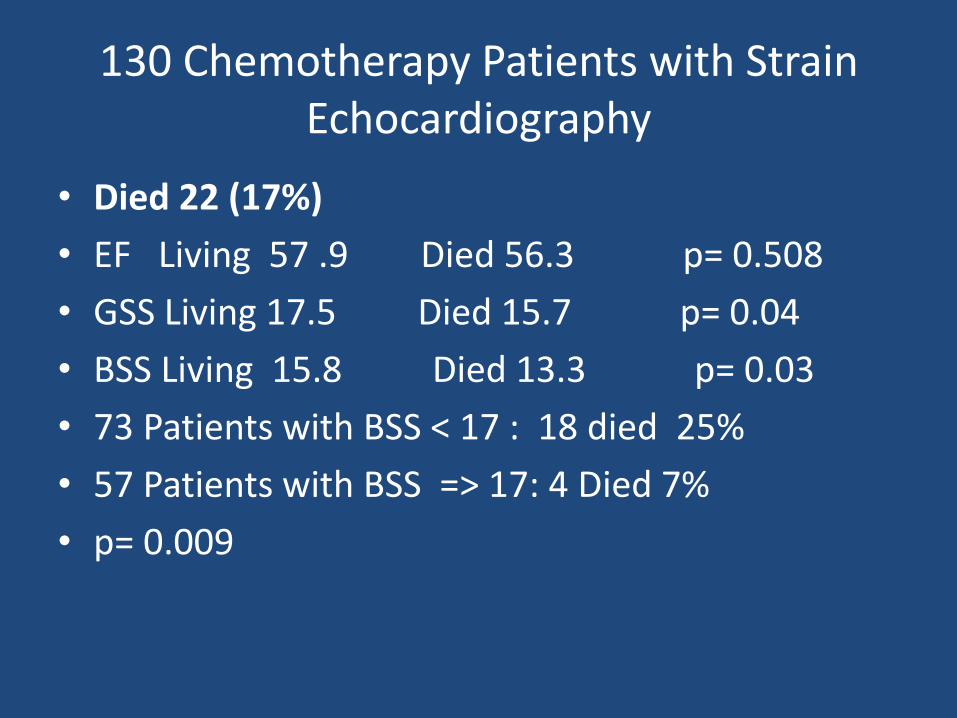
130 Chemotherapy Patients with Strain Echocardiography
• Died 22 (17%)
• EF Living 57 .9 Died 56.3 p= 0.508
• GSS Living 17.5 Died 15.7 p= 0.04
• BSS Living 15.8 Died 13.3 p= 0.03
• 73 Patients with BSS < 17 : 18 died 25%
• 57 Patients with BSS => 17: 4 Died 7%
• p= 0.009
49 YO Female
• Lymphoma
• Post chemotherapy
• Pre bone marrow transplant
• Ejection Fraction 60
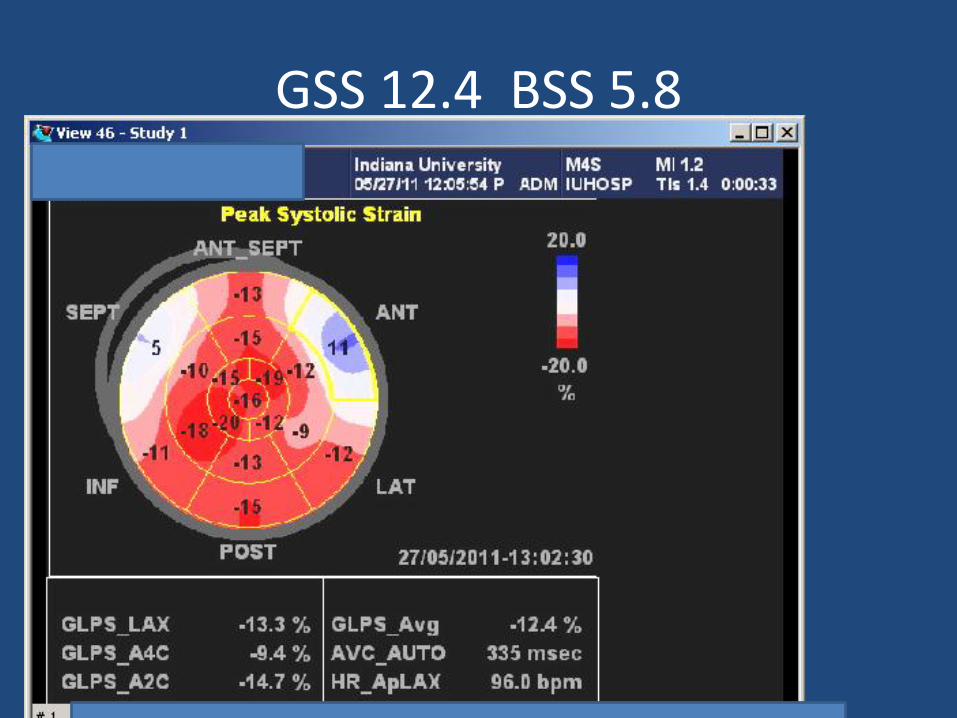
GSS 12.4 BSS 5.8
3 Months Later After BMT
Ejection Fraction 22
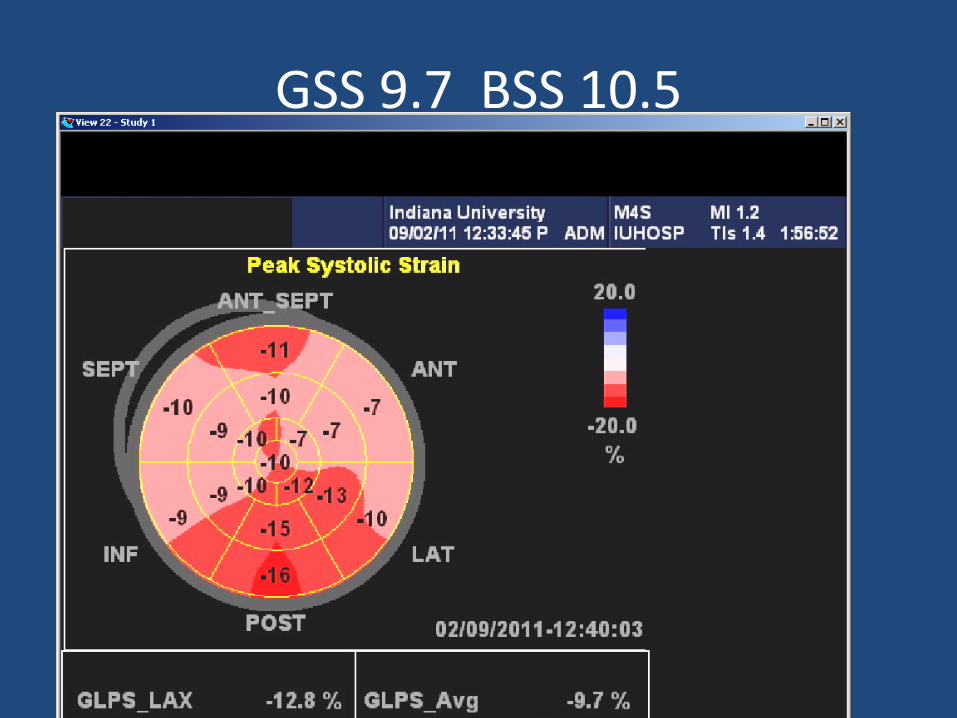
GSS 9.7 BSS 10.5
Patient died one week later
No Test is Perfect
Strain is not the first exception
False Positives
Isolated single abnormal segment surrounded by normal segments
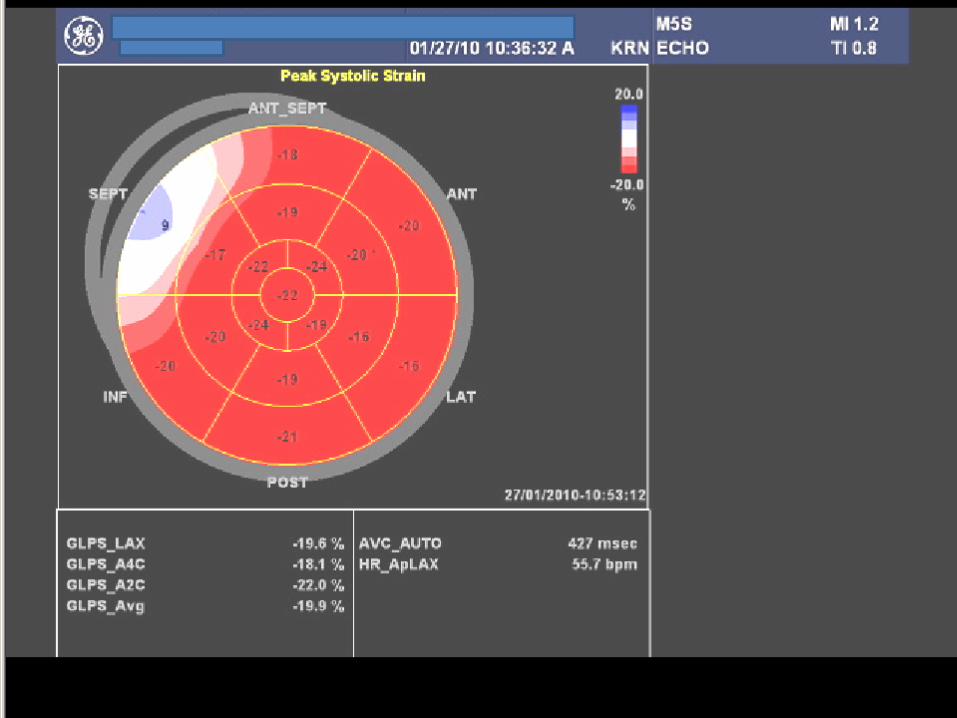
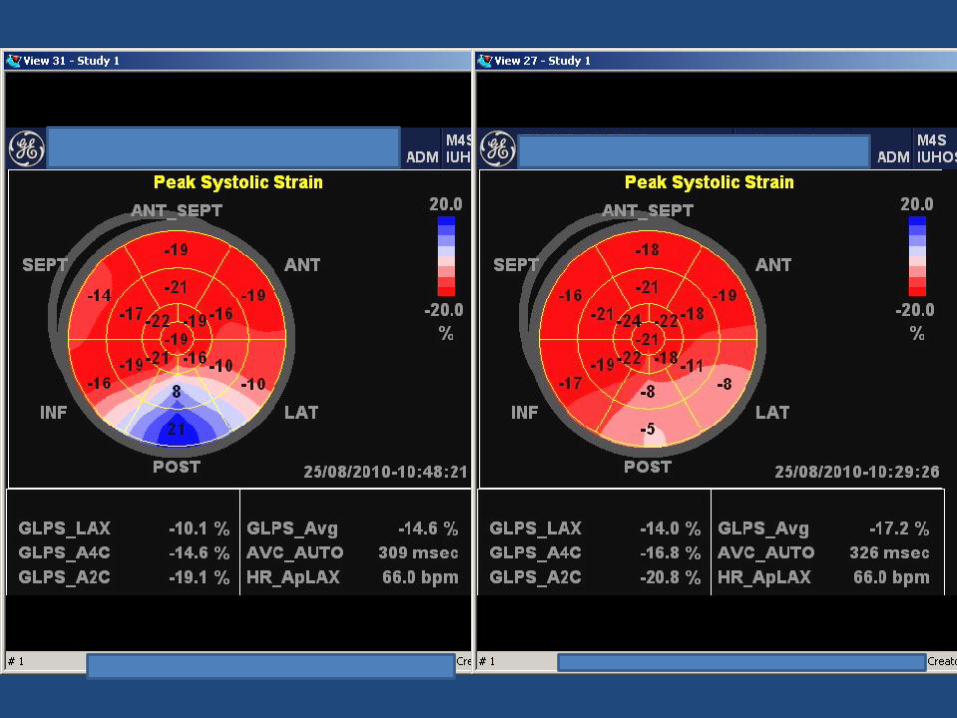
False Positive
Abnormal segment which has totally unphysiologic value
e.g. +21, repeat -5
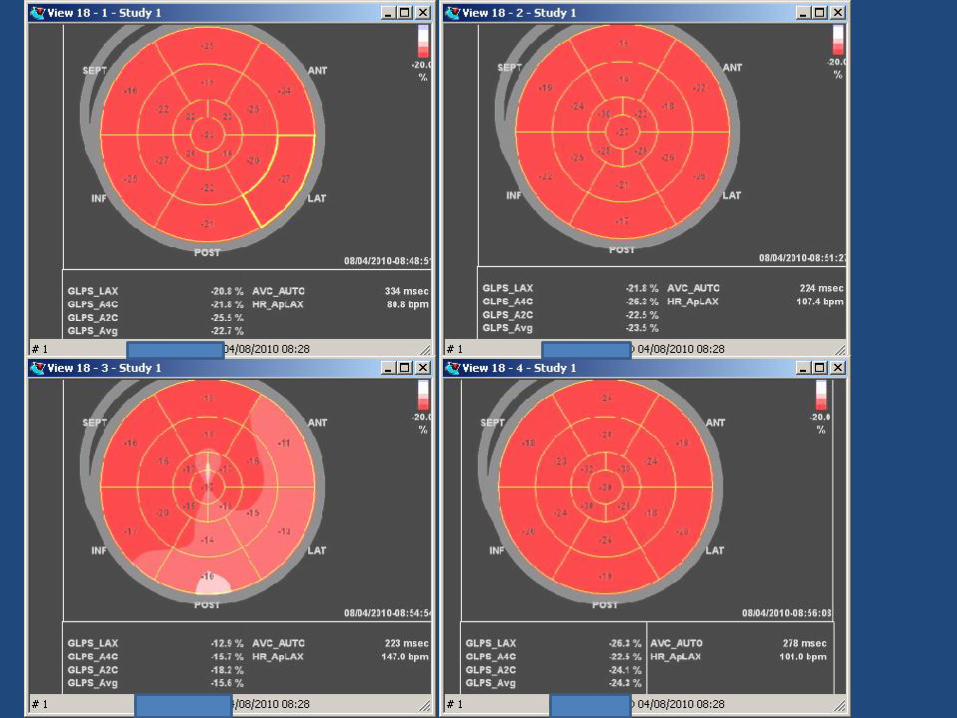
Current Speckle Strain Not Reliable with Rapid Heart Rates
e.g. Normal dobutamine echo with false positive segments at peak dose
with HR of 147
Strain Echocardiography: a sensitive indicator of myocardial dysfunction
• Ischemia
• Hypertrophy
• Infiltration
• Hypoxia
• Cardiotoxic drugs
• Myocardial rejection
• Severe systemic illness
Patients Benefiting From Strain Echocardiography
• Known or suspected CAD • Hypertension • Heart failure • Significant mitral or aortic regurgitation • Aortic stenosis • Any form of cardiomyopathy • Diabetes • Chemotherapy • Cardiac transplant
Strain as a Useful Supplement to Routine Transthoracic Echocardiography
• Wall motion analysis is subjective with high inter observer variability: Strain is quantitative with ease of interpretation
• Wall thickness measurements are difficult with high inter observer variability: Strain is an independent indicator of hypertrophy
• Ejection fraction has significant limitations: Strain overcomes many of them
• Speckle tracing strain is also possible with other cardiac chambers e.g. RV, LA
Limitations of Speckle Tracking 2D Strain Echocardiography
• Quality of 2D image is a factor
• Poor speckle tracking can lead to false positive results
• 2D strain limited by frame rate and HR
• If HR varies Bullseye not generated
• So far only one manufacturer supplying and displaying reliable strain data
Comparison between Different Speckle Tracking and Color Tissue Doppler Techniques to Measure Global and Regional Myocardial Deformation in Children
JASE , Volume23 Pages 919-928 (September 2010)
Laurens Koopman, et al
Some deformation measurements (e.g., longitudinal and circumferential ε) are comparable among different ultrasound machines and software packages, whereas others are significantly different (e.g., radial ε and strain rate). This study stresses the need for an industry standard for these techniques.
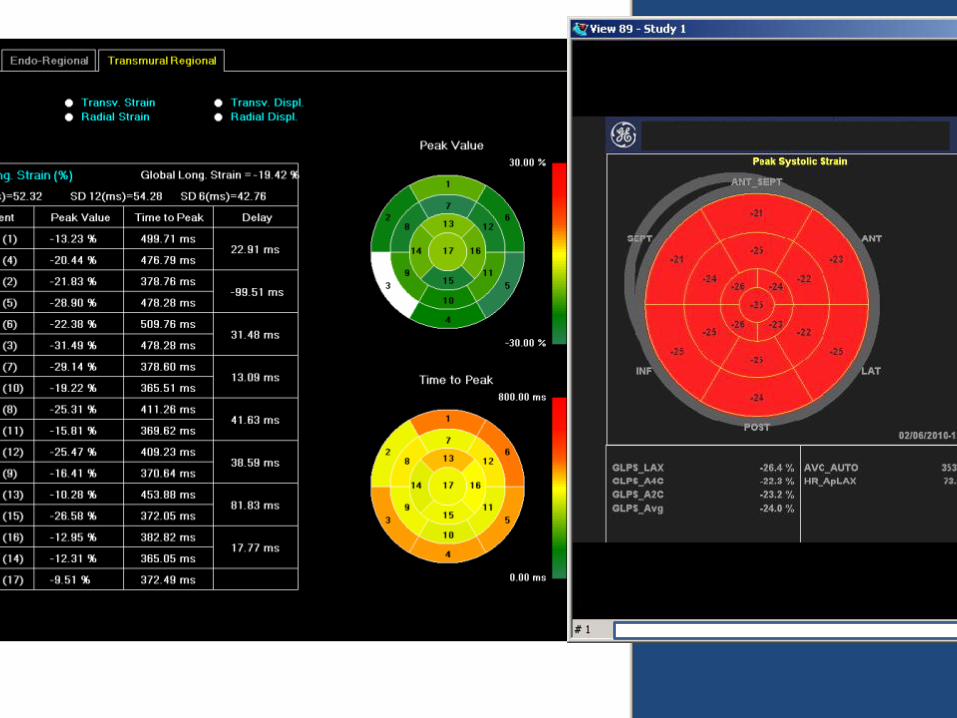
Strain From Different Instruments on Same Patient
Normal subject
Marked differences between green and red bullseye

Strain From Different Instruments on Same Patient
Abnormal patient
Marked differences between green and red bullseye

We have been attempting to do speckle tracking in our lab for the past couple of
years and have pretty much given up on it until recently. We have an iE33 with
version 7 QLAB software. Reproducibility of measurements has been poor, and I do
not feel very confident in the measurements we were obtaining
I have been told that the Vivid 7 software is better for this type of analysis
(and seems to be the machine of choice by the researchers publishing data
on this technique), but have no personal experience.
Russ Tonkovic MD, FASE,FACC
Barrington IL
ASE Open Forum
3D Speckle Strain
• Limited now by frame (volumes) rate
• As frame (volumes) rate increases, speckle strain should be simpler (only need to place two points on one view vs three points on three views) and will overcome some of current limitations of 2D speckle strain (basal twist, variations in heart rate of views e.g. atrial fibrillation)
• 3D speckle strain will probably be the preferred technique in the future, but 2D speckle is proving to be so valuable and relatively inexpensive, that it will be the practical approach for some time.
Role of Strain Echocardiography in Today’s Practice of Medicine
• Although it is possible that strain could be considered to be separate like Doppler, it is unlikely that there will be an added reimbursement for strain
• The major benefit will be to make echocardiograms more objective and quantitative thus producing a more accurate and complete cardiac evaluation
• Multiple “complimentary” imaging studies are very costly, “screening “examinations may be eliminated
• To be cost effective and competitive, echocardiography must be a definitive examination. Recording strain is a major step in this direction