9/7/20151 child psychiatry for medical students part i khalid bazaid, mb bs, frcpc assistant...
TRANSCRIPT

04/19/2304/19/23 11
Child Psychiatry for Child Psychiatry for Medical Students Part IMedical Students Part I
Khalid Bazaid, MB BS, FRCPCKhalid Bazaid, MB BS, FRCPCAssistant ProfessorAssistant Professor
Child & Adolescent PsychiatristChild & Adolescent PsychiatristDepartment of PsychiatryDepartment of Psychiatry
College of MedicineCollege of MedicineKing Saud UniversityKing Saud University

04/19/2304/19/23 22
OutlinesOutlines Introduction to Child & Adolescent psychiatryIntroduction to Child & Adolescent psychiatry
Review disorders first usually diagnosed in Infancy, Childhood and Review disorders first usually diagnosed in Infancy, Childhood and AdolescenceAdolescence– MR; PDDMR; PDD– LD; Motor Skills; S/L; TSLD; Motor Skills; S/L; TS– ADHD; Disruptive DisordersADHD; Disruptive Disorders
Review childhood presentation of general psychiatric disordersReview childhood presentation of general psychiatric disorders– Elimination disordersElimination disorders– MoodMood– AnxietyAnxiety– PsychosisPsychosis

04/19/2304/19/23 33
Remember: Children are not miniature adultsRemember: Children are not miniature adults

04/19/2304/19/23 44
5 Days5 Days 2 Months2 Months
1 Year1 Year 28 Years28 Years

04/19/2304/19/23 55
IMPROVING THE ODDS FOR IMPROVING THE ODDS FOR SUCCESSFUL DEVELOPMENTAL SUCCESSFUL DEVELOPMENTAL
OUTCOMESOUTCOMES
PROTECTIVE FACTORS:
Good parent-child relationship
Easy, outgoing temperament
Positive peer influence
Successful school experiences
Caring adult role models
Participation in pro-social groups
Access to needed services
e.g. healthcare, mental health, crisis intervention
04/19/2304/19/23 66
DISORDERS OF CHILDHOOD DISORDERS OF CHILDHOOD AND ADOLESCENCE - 1AND ADOLESCENCE - 1
DISORDERS OF CHILDHOOD DISORDERS OF CHILDHOOD AND ADOLESCENCE - 1AND ADOLESCENCE - 1
• MD of the conceptualization of the transitionsMD of the conceptualization of the transitions
• Unique clinical and academic skills that differentiate a child from Unique clinical and academic skills that differentiate a child from adultadult
• Specialty rather than subspecialtySpecialty rather than subspecialty
• Pediatric medicine 20Pediatric medicine 20thth century century
• Number of Child/Adolescent Psychiatrist per capita/populationNumber of Child/Adolescent Psychiatrist per capita/population
• It is fundamentally a team service rather than individualized It is fundamentally a team service rather than individualized
• Biopsychosocail modelBiopsychosocail model

04/19/2304/19/23 77
DISORDERS OF CHILDHOOD DISORDERS OF CHILDHOOD AND ADOLESCENCE - 2AND ADOLESCENCE - 2
DISORDERS OF CHILDHOOD DISORDERS OF CHILDHOOD AND ADOLESCENCE - 2AND ADOLESCENCE - 2
• Basically all adult Axis I disorders can occur in children and Basically all adult Axis I disorders can occur in children and adolescents (Depression, Bipolar, Schizophrenia, Anxiety, etc.)adolescents (Depression, Bipolar, Schizophrenia, Anxiety, etc.)
• Personality Disorders (Axis II) are usually not diagnosed (and Personality Disorders (Axis II) are usually not diagnosed (and ASPD can’t be), although personality ASPD can’t be), although personality traitstraits are often identified are often identified
• Specific disorders with childhood onset are listed separately in Specific disorders with childhood onset are listed separately in DSM-IV-TR (ADHD, Conduct Disorder, Learning Disorders, MR, etc). DSM-IV-TR (ADHD, Conduct Disorder, Learning Disorders, MR, etc). These may persist into adulthood.These may persist into adulthood.
• Comorbidity is commonComorbidity is common
• Epidemiology: 1 in 5 children involvedEpidemiology: 1 in 5 children involved

04/19/2304/19/23 88

04/19/2304/19/23 99
EVALUATION STRATEGIESEVALUATION STRATEGIESEVALUATION STRATEGIESEVALUATION STRATEGIES
Patient InterviewPatient Interview
Testing Testing (IQ, Education, Projective,(IQ, Education, Projective, Personality, Neuropsychiatry,Personality, Neuropsychiatry, labs, EEG, MRI)labs, EEG, MRI)
ObservationObservation
Collateral InformationCollateral Information (Parents, School)(Parents, School)
04/19/2304/19/23 1010
TREATMENT MODALITIES*TREATMENT MODALITIES**(Usually 2 or more modalities are used *(Usually 2 or more modalities are used
simultaneously)simultaneously)
TREATMENT MODALITIES*TREATMENT MODALITIES**(Usually 2 or more modalities are used *(Usually 2 or more modalities are used
simultaneously)simultaneously)
• Individual Therapies (play, behavioral, cognitive, Individual Therapies (play, behavioral, cognitive, supportive, dynamic)supportive, dynamic)
• Family Therapy & Parent TrainingFamily Therapy & Parent Training
• Group Therapy - especially important for adolescentsGroup Therapy - especially important for adolescents
• Examples of Pharmacotherapy: Examples of Pharmacotherapy: ADHD: Stimulants (e.g., Ritalin, Concerta) andADHD: Stimulants (e.g., Ritalin, Concerta) and
Atomoxetine (Strattera)Atomoxetine (Strattera) MDD & Anxiety: SSRI's (recent Black Box warnings)MDD & Anxiety: SSRI's (recent Black Box warnings) Bipolar Disorders: Valproate, LithiumBipolar Disorders: Valproate, Lithium Psychosis: AntipsychoticsPsychosis: Antipsychotics

04/19/2304/19/23 1111
Mental RetardationMental Retardation• Epidemiology: 1-3% in USEpidemiology: 1-3% in US• IQ 70 or less on an individually IQ 70 or less on an individually
administered IQ testadministered IQ test• Onset before age 18Onset before age 18• Delays in two or more adaptive areas, Delays in two or more adaptive areas,
e.g., self care; communication; work; e.g., self care; communication; work; leisure; health; or safetyleisure; health; or safety
• Testing:Testing:• Intelligence testing - compares Intelligence testing - compares
individual test performance to individual test performance to normative of age group normative of age group • E.g., WISC-IV (6 to17y) or E.g., WISC-IV (6 to17y) or
Stanford-Binet V5 (2 to 85+y)Stanford-Binet V5 (2 to 85+y)• Vineland Adaptive Behavior Vineland Adaptive Behavior
Scales -measure of personal and Scales -measure of personal and social skillssocial skills

04/19/2304/19/23 1212

04/19/2304/19/23 1313
Mental RetardationMental Retardation
(~ 85%)(~ 85%)
(~ 10%)(~ 10%)
(~ 3%)(~ 3%)
(~ 1-2%)(~ 1-2%)

04/19/2304/19/23 1414
MILD MR: MILD MR: IQ 50/55 to 70 (~ 85%)IQ 50/55 to 70 (~ 85%)
• School: may acquire skills up to 6th grade level.School: may acquire skills up to 6th grade level.
• Social and Communication Skills: develop spontaneously.Social and Communication Skills: develop spontaneously.
• May first be detected in school.May first be detected in school.
• May acquire vocational skills and be self-supportive.May acquire vocational skills and be self-supportive.
• Social and Communication Skills: develop, but impaired.Social and Communication Skills: develop, but impaired.
• Early detection (i.e., before entering school).Early detection (i.e., before entering school).
• School: unlikely to progress past 2nd grade level.School: unlikely to progress past 2nd grade level.
• May work under close supervision (sheltered workshop).May work under close supervision (sheltered workshop).
• Social and Communication Skills: develop, but impaired.Social and Communication Skills: develop, but impaired.
• Early detection (i.e., before entering school).Early detection (i.e., before entering school).
• School: unlikely to progress past 2nd grade level.School: unlikely to progress past 2nd grade level.
• May work under close supervision (sheltered workshop).May work under close supervision (sheltered workshop).
MODERATE MR: MODERATE MR: IQ 35/40 to 50/55 (~ 10%)IQ 35/40 to 50/55 (~ 10%)
04/19/2304/19/23 1515
SEVERE MR:SEVERE MR: IQ 20/25 to 35/40 (~ 3%) IQ 20/25 to 35/40 (~ 3%)
• School: May learn to sight-read (survival School: May learn to sight-read (survival words)words)
• Social/Communication Skills: little or no Social/Communication Skills: little or no communicative speech. Often display poor communicative speech. Often display poor motor development.motor development.
• May acquire elementary hygiene skills and May acquire elementary hygiene skills and perform simple tasks; unable to benefit perform simple tasks; unable to benefit from vocational trainingfrom vocational training
• Social and Communication Skills: rarely have Social and Communication Skills: rarely have communicative speech efforts; minimal sensorimotor communicative speech efforts; minimal sensorimotor abilities.abilities.
• Require constant aid and supervision; nursing care.Require constant aid and supervision; nursing care.
• Social and Communication Skills: rarely have Social and Communication Skills: rarely have communicative speech efforts; minimal sensorimotor communicative speech efforts; minimal sensorimotor abilities.abilities.
• Require constant aid and supervision; nursing care.Require constant aid and supervision; nursing care.
PROFOUND MR:PROFOUND MR: IQ Below IQ Below 20/25 (~ 1-2%)20/25 (~ 1-2%)

04/19/2304/19/23 1616
Treatment ConsiderationsTreatment Considerations
• Family is coping with loss of “ideal” child:Family is coping with loss of “ideal” child: Grief and loss issuesGrief and loss issues
• Appropriate placement and support:Appropriate placement and support: School School setting, day care, group homes, sheltered workshop and relief setting, day care, group homes, sheltered workshop and relief carecare
• Specific problems responsive to medications:Specific problems responsive to medications:e.g. seizures; depression; hyperactivity ; aggressione.g. seizures; depression; hyperactivity ; aggression
• May experience “independent” psychiatric disorders: May experience “independent” psychiatric disorders:
e.g. schizophrenia, bipolar disorder, etc.e.g. schizophrenia, bipolar disorder, etc.
04/19/2304/19/23 1717
Pervasive Developmental DisordersPervasive Developmental Disorders
Disorders with severe and pervasive impairment in essential Disorders with severe and pervasive impairment in essential developmental areas:developmental areas:
Reciprocal social skillsReciprocal social skills Language developmentLanguage development Range of behavioral repertoire Range of behavioral repertoire
DSM-IV includes the following under PDD:DSM-IV includes the following under PDD:1.1. AutismAutism2.2. Rett’s DisorderRett’s Disorder3.3. Childhood Disintegrative DisorderChildhood Disintegrative Disorder4.4. Asperger’s DisorderAsperger’s Disorder5.5. PDD, not otherwise specifiedPDD, not otherwise specified
Language Disorders: Autism and Other Pervasive Developmental Disorders, Pediatr Clin N Am 54 (2007) 469–481
04/19/2304/19/23 1818
Autism Spectrum Disorders (ASD)Autism Spectrum Disorders (ASD)
ASD are increasingly common neurodevelopment disorderASD are increasingly common neurodevelopment disorder
Characterized by functional impairments in a triad of symptoms:Characterized by functional impairments in a triad of symptoms: (1)(1) limited reciprocal social interactionslimited reciprocal social interactions (2) disordered verbal and nonverbal communication(2) disordered verbal and nonverbal communication (3) restricted, repetitive behaviors or circumscribed interests(3) restricted, repetitive behaviors or circumscribed interests
These behaviors can vary in severity from mild to disablingThese behaviors can vary in severity from mild to disabling IQ:IQ: At least half of all children who have autism haveAt least half of all children who have autism have mentalmental retardation retardation Autism appears in early childhood, often as young as age 2 or 3Autism appears in early childhood, often as young as age 2 or 3 Prevalence rate for all ASDPrevalence rate for all ASD 0.6%0.6% (Am J Psychiatry 2005; 162(6): 1133-41)(Am J Psychiatry 2005; 162(6): 1133-41)
Up to 25% have grand-mal seizures and about 50% non-specific EEG Up to 25% have grand-mal seizures and about 50% non-specific EEG abnormalitiesabnormalities
boys to girls 4:1boys to girls 4:1 Asperger’s disorder 10:1 as many boys to girls Asperger’s disorder 10:1 as many boys to girls Genetic / environment Genetic / environment

04/19/2304/19/23 1919

04/19/2304/19/23 2020
Epidemiology of AutismEpidemiology of Autism
• Prevalence rate of Autism Spectrum Disorders is Prevalence rate of Autism Spectrum Disorders is about 1%about 1%
• Up to 25% have grand-mal seizures and about 50% Up to 25% have grand-mal seizures and about 50% non-specific EEG abnormalitiesnon-specific EEG abnormalities
• 50 to 70% have some degree of MR50 to 70% have some degree of MR
• Boys are effected 3 to 5 times more often than girlsBoys are effected 3 to 5 times more often than girls

04/19/2304/19/23 2121
Etiology of AutismEtiology of Autism
• Psychological theories have not been confirmed:Psychological theories have not been confirmed: Not caused by “refrigerator mother” or bad parentingNot caused by “refrigerator mother” or bad parenting
• Heritability over 90%Heritability over 90%
• Association with a variety of disorders: Association with a variety of disorders: Congenital rubella & Postnatal infectionCongenital rubella & Postnatal infection Genetic disorders, including Fragile XGenetic disorders, including Fragile X Metabolic disordersMetabolic disorders Tic disordersTic disorders OCDOCD

04/19/2304/19/23 2222
Asperger’s DisorderAsperger’s Disorder
• ““High functioning autism”High functioning autism”
• No delays in language and cognitive developmentNo delays in language and cognitive development
• Stereotypic, repetitive mannerismsStereotypic, repetitive mannerisms
• Lack of interactive play/communicationLack of interactive play/communication
• Impaired communication skillsImpaired communication skills

04/19/2304/19/23 2323
PDD NOSPDD NOS
When there is no severe and pervasive When there is no severe and pervasive impairment in the development of reciprocal impairment in the development of reciprocal
social interaction, or communication skills, or social interaction, or communication skills, or when stereotyped behaviors and activities are when stereotyped behaviors and activities are
present, but the criteria are not met for a present, but the criteria are not met for a specific pervasive developmental disorder.specific pervasive developmental disorder.

04/19/2304/19/23 2424
Interventions in PDD/AutismInterventions in PDD/Autism
Presently:Presently:
No curative treatmentNo curative treatment; early detection and symptomatic ; early detection and symptomatic approachesapproaches
Mainstay:Mainstay:
Structured behavioral and educational programs; speech and Structured behavioral and educational programs; speech and language serviceslanguage services
Medication:Medication:
To control seizures, hyperactivity, SIB, severe aggression, or To control seizures, hyperactivity, SIB, severe aggression, or mood disordersmood disorders

04/19/2304/19/23 2525
Rett’s DisorderRett’s Disorder
• One in every 10,000 to 15,000 live One in every 10,000 to 15,000 live female birthsfemale births• Normal growth for the first few months of lifeNormal growth for the first few months of life• Deceleration of head growth between 4-8 monthsDeceleration of head growth between 4-8 months• ““Hand washing” stereotypies, Loss of purposeful hand Hand washing” stereotypies, Loss of purposeful hand
movementsmovements• Truncal incoordination; gait problems; SeizuresTruncal incoordination; gait problems; Seizures• Most are in wheelchair by their late teens and die Most are in wheelchair by their late teens and die
before 30.before 30.• Disorder of femalesDisorder of females; in up to 80% due to mutation of ; in up to 80% due to mutation of
MECP2 gene on X chromosomeMECP2 gene on X chromosome

04/19/2304/19/23 2626
Childhood Disintegrative DisorderChildhood Disintegrative Disorder
• Normal development for at least the first two years of Normal development for at least the first two years of lifelife
• Clinically significant loss of previously acquired skills Clinically significant loss of previously acquired skills (before age 10 years) in 2 or more of the following (before age 10 years) in 2 or more of the following areasareas:: LanguageLanguage Social skills or adoptive behaviorSocial skills or adoptive behavior Motor skillsMotor skills Play Play Bowel or bladder controlBowel or bladder control

04/19/2304/19/23 2727
Questions after lecture?Questions after lecture?
Please e-mail ([email protected]) or call Please e-mail ([email protected]) or call (01 467 1717)(01 467 1717)
Interested in learning more about child and Interested in learning more about child and adolescent psychiatry?adolescent psychiatry?– Arrange to attend OPD Arrange to attend OPD – Consider an elective rotation during internship Consider an elective rotation during internship
or otherwiseor otherwise

04/19/2304/19/23 2828
Externalizing Disorders in Children Externalizing Disorders in Children (ADHD, CD, ODD)(ADHD, CD, ODD)

04/19/2304/19/23 2929
Attention Deficit/Hyperactivity Disorder Attention Deficit/Hyperactivity Disorder (ADHD)(ADHD)
• Present before age 7Present before age 7• Persist for at least 6 months and be more frequent and severe Persist for at least 6 months and be more frequent and severe than is typical for children at comparable developmental stagesthan is typical for children at comparable developmental stages• Symptoms in two or more settings• Boys to girls 3 : 1Boys to girls 3 : 1 • DSM-IV-TR distinguishes ADD WITH & WITHOUT hyperactivity, and recognizes a predominantly hyperactive subtype • Persists in some patients into adolescence and AdulthoodPersists in some patients into adolescence and Adulthood
• Normal IQNormal IQ

04/19/2304/19/23 3030
INATTENTIONINATTENTION
no attention to detailsno attention to details difficulty focusingdifficulty focusing not listeningnot listening easily distractedeasily distracted forgetful not forgetful not
following throughfollowing through difficulty organizingdifficulty organizing avoids effortful tasksavoids effortful tasks loses thingsloses things
HYPERACTIVITYHYPERACTIVITY
IMPULSIVITYIMPULSIVITY fidgetsfidgets leaves seatleaves seat runs/climbsruns/climbs loudloud on the goon the go excessive talkexcessive talk blurtsblurts can't wait turncan't wait turn interrupts/butts ininterrupts/butts in

04/19/2304/19/23 3131
ADHD Low selfesteem
Academiclimitations
Relationships
Smoking andsubstance abuse
InjuriesMotor vehicle
accidents
Legaldifficulties
Occupational/vocational
ChildrenA
du
lts
Adolescents

04/19/2304/19/23 3232
ADHD DiagnosisADHD Diagnosis
• ADHD is more difficult to reliably diagnose in early childhood ADHD is more difficult to reliably diagnose in early childhood (age 4-6)(age 4-6)
• Obtain developmental and medical historyObtain developmental and medical history
• Get standardized questionnaires from parents and teachersGet standardized questionnaires from parents and teachers
• Observation in clinic setting may or may not show symptoms Observation in clinic setting may or may not show symptoms described by parentsdescribed by parents
• Psycho-educational testing useful if LD suspectedPsycho-educational testing useful if LD suspected

04/19/2304/19/23 3333
الطفل : المستشفى : ........................................ اسم ................العمر : ............................. رقم
:التعليماتالعبارات من واحده كل أمام الطفل وصف يناسب الذي الرقم حول دائرة وضع الرجاء
:التالية 0 كثيرا
جدا0كثير
ا0قليًال0
أبدا0
الطفل وصف تسلسل
3 2 1 0 مقعده . في يتحرك أو يتململ ما غالبا0 )1(
3 2 1 0 . 0 جالسا البقاء في صعوبة يجد )2(
3 2 1 0 انتباهه . تشتيت السهل من )3(
3 2 1 0وسط دوره انتظار في صعوبة يجد
أقرانه . )4(
3 2 1 0على االجابة في يندفع ما غالبا0
تفكير . دون األسئلة )5(

04/19/2304/19/23 3434
3 2 1 0 التعليمات . اتباع في صعوبة يجد )6(
3 2 1 0يطلب فيما انتباهه حصر في صعوبة يجد
عمله . منه )7(
3 2 1 0 ، إكماله قبل نشاط من ينتقل ما غالبا0
آخر . نشاط إلى )8(
3 2 1 0 بهدوء . اللعب في صعوبة يجد )9(
3 2 1 0 بافراط . يتكلم ما P0 غالبا )10(
3 2 1 0نفسه يقحم اآلخرين يقاطع ما غالبا0
عليهم .)11(
3 2 1 0 اإلنصات . عدم عليه يبدو ما غالبا0 )12(
3 2 1 0 ) األدوات الخاصة أشياءه يضيع ما غالبا0
( 0 مثًال المدرسية)13(
3 2 1 0دون بدنيا0 خطرة بأعمال يقوم ما غالبا0
ذلك . عن ينتج لما اكتراث)14(

04/19/2304/19/23 3535
ADHDADHD
EtiologyEtiology
NeuroanatomicalNeurochemical
Genetic
CNS insult
Environmental

04/19/2304/19/23 3636
NIMH Press Release November 12, 2007 NIMH Press Release November 12, 2007 Brain Matures a Few Years Late in ADHD, Brain Matures a Few Years Late in ADHD,
But Follows Normal PatternBut Follows Normal Pattern
http://www.nimh.nih.gov/science-news/2007/brain-matures-a-few-years-late-in-adhd-but-follows-normal-pattern.shtml

04/19/2304/19/23 3737
ADHD Child Home
Behavioural Therapy
MedicationSchool
Treatment

04/19/2304/19/23 3838
ADHD TreatmentADHD Treatment
• Psychoeducation essential; medication alone is usually not Psychoeducation essential; medication alone is usually not sufficient for the treatment of ADHDsufficient for the treatment of ADHD
• Parent training in behavioral management and school-Parent training in behavioral management and school-based behavioral interventionsbased behavioral interventions
• FDA approved medications include FDA approved medications include stimulantsstimulants and and AtomoxetineAtomoxetine Note: Stimulant medications improve attention in Note: Stimulant medications improve attention in
normal individuals as well as children with ADHDnormal individuals as well as children with ADHD• Establish communication with teachers/school; potentially Establish communication with teachers/school; potentially
includes accommodations and IEPincludes accommodations and IEP
04/19/2304/19/23 3939
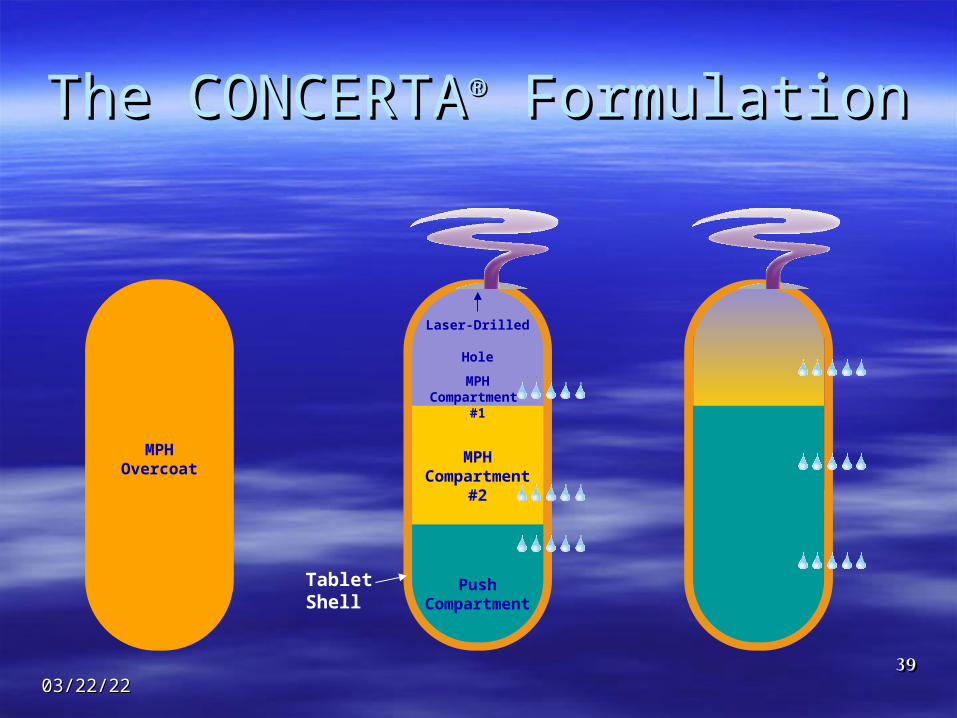
The CONCERTAThe CONCERTA®® Formulation Formulation
MPH Overcoat
Tablet Shell
Push Compartment
MPH Compartment
#2
Laser-Drilled Hole
MPH Compartment
#1

04/19/2304/19/23 4040

04/19/2304/19/23 4141
ADHD OutcomesADHD Outcomes
ADHD can be a lifetime disorder, with nearly 2/3 of children ADHD can be a lifetime disorder, with nearly 2/3 of children continuing with symptoms as adultscontinuing with symptoms as adults
Learning disabilities frequently comorbid in children with Learning disabilities frequently comorbid in children with ADHD and not responsive to medicationsADHD and not responsive to medications
Adult outcome studies show more relationship problems, Adult outcome studies show more relationship problems, lower educational and professional achievement, more traffic lower educational and professional achievement, more traffic violations and higher health care costs for cohort members violations and higher health care costs for cohort members with ADHD compared to unaffected controlswith ADHD compared to unaffected controls
Long term outcome strongly influenced by comorbid ODD, Long term outcome strongly influenced by comorbid ODD, CD, and substance abuseCD, and substance abuse

04/19/2304/19/23 4242

04/19/2304/19/23 4343
DepressionDepression
EpidemiologyEpidemiology
• 2.5% of children, up to 5% of adolescents
• Prepubertal-1:1/M:F; adolescence - 4:1/F:M
• Average length of untreated MDD - 7.2 months
• Recurrence rates - 40% within 2 years
• Most important risk factor for the development of depressive illness is having at least one parent with depression
04/19/2304/19/23 4444
DepressionDepressionDSM- IV-TR Modifications DSM- IV-TR Modifications
for children:for children: irritable mood (vs. irritable mood (vs.
depressive mood)depressive mood) observed apathy and observed apathy and
pervasive boredom (vs. pervasive boredom (vs. Anhedonia)Anhedonia)
failure to make expected failure to make expected weight gains (rather than weight gains (rather than significant weight loss)significant weight loss)
somatic complaintssomatic complaints social withdrawalsocial withdrawal declining school declining school
performanceperformance

04/19/2304/19/23 4545
Treatment of Depression
P sycho ed uca tio na l T he ra py
In te rpe rson a l C og n it ive / B eh av io ra l P lay
P sycho the ra py A n tid ep ressan ts
D e pressed Ch i ld
Treatment for Adolescents with Depression Study (TADS):Treatment for Adolescents with Depression Study (TADS):
• Multi-site (13 sites) clinical research study Multi-site (13 sites) clinical research study
• For adolescents aged 12 to 17For adolescents aged 12 to 17
• Compared short- and longer-term effectiveness of medication and Compared short- and longer-term effectiveness of medication and psychotherapy for depression psychotherapy for depression
• Flouxetine and cognitive-behavioral therapy combined produced the best success Flouxetine and cognitive-behavioral therapy combined produced the best success rate in treating depression in adolescents (71% responded)rate in treating depression in adolescents (71% responded)

04/19/2304/19/23 4646
SuicideSuicide Publicity regarding suicide may prompt other adolescents to Publicity regarding suicide may prompt other adolescents to
attempt suicideattempt suicide
Attempts- 3:1/F:M, Completions- 4:1/M:FAttempts- 3:1/F:M, Completions- 4:1/M:F
Most common means of completed suicide: FIREARMSMost common means of completed suicide: FIREARMS
Most often associated with depressive disorder. Also Most often associated with depressive disorder. Also consider schizophrenia and substance abuse.consider schizophrenia and substance abuse.
Risk factors: Age, sex, presence of psychiatric illness, family Risk factors: Age, sex, presence of psychiatric illness, family history, isolation from friends, substance abusehistory, isolation from friends, substance abuse

04/19/2304/19/23 4747
Adolescents and SuicideAdolescents and Suicide
In 1998, In 1998, 4,153 young people4,153 young people, ages 15-24, committed , ages 15-24, committed suicide in the United States, an average of 11.3 per day.suicide in the United States, an average of 11.3 per day.11
Suicide accounts for Suicide accounts for 13.5%13.5% of all deaths in this age- of all deaths in this age-groupgroup11
Suicide is the Suicide is the third leading causethird leading cause of death in this age of death in this age group following unintentional injury and homicidegroup following unintentional injury and homicide22
1 Murphy, SL, 1998
2 The Surgeon General’s Call to Action to Prevent Suicide, 1999

04/19/2304/19/23 4848
Suicide-Related Fatalities by Suicide-Related Fatalities by CauseCause
393 320
34
1211
41 47 490
200400600800
100012001400

04/19/2304/19/23 4949
Suicide PreventionSuicide Prevention
Don’t dismiss suicidal ideation, depression, runaway, Don’t dismiss suicidal ideation, depression, runaway, substance abuse as just “normal” for age.substance abuse as just “normal” for age.
Educate families to control access to potentially lethal Educate families to control access to potentially lethal methods of self-harm.methods of self-harm.
Provide crisis hotline information.Provide crisis hotline information.

04/19/2304/19/23 5050
Bipolar DisorderBipolar DisorderADULTSADULTS
At least one At least one manic/mixed episode manic/mixed episode
MANIA includes MANIA includes expansive, irritable or expansive, irritable or euphoric mood plus euphoric mood plus (3/7) grandiosity, (3/7) grandiosity, decreased need for decreased need for sleep, pressured speech, sleep, pressured speech, racing thoughts, racing thoughts, distractibility, distractibility, psychomotor agitation, psychomotor agitation, increase in high risk increase in high risk activitiesactivities
CHILDREN & ADOLESCENTSCHILDREN & ADOLESCENTS
More likely to present with More likely to present with aggressiveness, irritability, aggressiveness, irritability, and emotional labilityand emotional lability
Harder to delineate specific Harder to delineate specific episodesepisodes
Prone to chronic mixed or Prone to chronic mixed or rapid cycling with agitated rapid cycling with agitated affect and explosive angeraffect and explosive anger

04/19/2304/19/23 5151
Diagnosing Diagnosing Bipolar DisorderBipolar Disorder
Not to be confused with normal development coupled with Not to be confused with normal development coupled with parenting issuesparenting issues
Symptoms may include the full range of child psychiatric Symptoms may include the full range of child psychiatric symptoms of childhoodsymptoms of childhood
Expansive or irritable moodExpansive or irritable mood Rapid cycling of mood for little or no reasonRapid cycling of mood for little or no reason Explosive ragesExplosive rages Non specific aggressionNon specific aggression Defiance of authorityDefiance of authority Inappropriate sexual behaviorInappropriate sexual behavior Impaired judgment, impulsivity, dare devil behaviorImpaired judgment, impulsivity, dare devil behavior GrandiosityGrandiosity

04/19/2304/19/23 5252
Treatment of Bipolar DisorderTreatment of Bipolar Disorder
Limited data is available on the efficacy and safety of mood Limited data is available on the efficacy and safety of mood stabilizing medications in youth.stabilizing medications in youth.
The essential treatment for this disorder in adults involves The essential treatment for this disorder in adults involves the use of appropriate doses of mood stabilizers, most the use of appropriate doses of mood stabilizers, most typically lithium and/or valproate, often combined with typically lithium and/or valproate, often combined with atypical antipsychotic medications.atypical antipsychotic medications.
Research on the effectiveness of these and other medications Research on the effectiveness of these and other medications in children and adolescents with bipolar disorder is ongoing. in children and adolescents with bipolar disorder is ongoing.
In addition, studies are investigating various forms of In addition, studies are investigating various forms of psychotherapy, including cognitive-behavioral therapy and psychotherapy, including cognitive-behavioral therapy and well-being therapy, to complement medication treatment for well-being therapy, to complement medication treatment for this illness in young people. this illness in young people.

04/19/2304/19/23 5353
School Refusal: Symptom, not disorder – may School Refusal: Symptom, not disorder – may accompany different anxiety disordersaccompany different anxiety disorders
esp. separation anxiety disorderesp. separation anxiety disorder
Recurrent vague, Recurrent vague, mysterious physical mysterious physical complaintscomplaints
No physical cause found on No physical cause found on initial and F/U exams. initial and F/U exams. Labs when necessary.Labs when necessary.
Symptoms predominate in Symptoms predominate in the AM then disappear. the AM then disappear.
Child has missed five or Child has missed five or more days of school for more days of school for same symptom(s).same symptom(s).
Average pediatrician Average pediatrician should diagnose 2 cases should diagnose 2 cases a montha month
5% of elementary 5% of elementary school students, 2% of school students, 2% of middle school studentsmiddle school students
Most common somatic Most common somatic symptom linked to symptom linked to school refusal / anxiety - school refusal / anxiety - ABDOMINAL PAINABDOMINAL PAIN

04/19/2304/19/23 5454
Specific PhobiasSpecific Phobias Marked and persistent fear of Marked and persistent fear of
a specific object or situation a specific object or situation with exposure causing an with exposure causing an immediate anxiety responseimmediate anxiety response
Must interfere with normal Must interfere with normal activities or relationshipsactivities or relationships
0ne-year community 0ne-year community prevalence estimated at 11%prevalence estimated at 11% In general, decreases with In general, decreases with
ageage About 2 - 3% of About 2 - 3% of
adolescents have adolescents have significant fearssignificant fears

04/19/2304/19/23 5555
Specific PhobiasSpecific Phobias
Animal phobias most Animal phobias most common childhood phobiacommon childhood phobia
Also frequently afraid of Also frequently afraid of the dark and imaginary the dark and imaginary creaturescreatures
In older children, fears are In older children, fears are more focused on health, more focused on health, social and school problemssocial and school problems

04/19/2304/19/23 5656
Selective MutismSelective Mutism Failure to speak in specific Failure to speak in specific
social situations despite social situations despite speaking in other speaking in other situationssituations
Classified as an anxiety Classified as an anxiety disorderdisorder
High association with High association with depressiondepression

04/19/2304/19/23 5757
Generalized Anxiety DisorderGeneralized Anxiety Disorder
Excessive anxiety and worry for Excessive anxiety and worry for at least 6 monthsat least 6 months
Worry about performance at Worry about performance at school and sportsschool and sports
DSM IV-TR criteria less DSM IV-TR criteria less stringent for childrenstringent for children Need only one criteria Need only one criteria
instead of three of sixinstead of three of six

04/19/2304/19/23 5858
Obsessive Compulsive DisorderObsessive Compulsive Disorder Presence of obsessions (thoughts) Presence of obsessions (thoughts)
and/or compulsions (behaviors)and/or compulsions (behaviors)
Although adults with OCD Although adults with OCD should have insight, kids may notshould have insight, kids may not
Interferes with life or causes Interferes with life or causes distressdistress
0.3-1.0% of pediatric population0.3-1.0% of pediatric population
One-third to one-half of all adult One-third to one-half of all adult patients report onset in childhood patients report onset in childhood or adolescenceor adolescence
04/19/2304/19/23 5959
SchizophreniaSchizophrenia• Need two of the following five symptoms over six months:Need two of the following five symptoms over six months:
DelusionsDelusions HallucinationsHallucinations Disorganized speechDisorganized speech Disorganized behaviorDisorganized behavior Negative symptomsNegative symptoms
• Onset in childhood is rare (1 in 10,000 children)Onset in childhood is rare (1 in 10,000 children)
• Genetic, organic, and environmental risk factorsGenetic, organic, and environmental risk factors
• Prodromal symptoms may include attention deficits and Prodromal symptoms may include attention deficits and poor executive functioning – may look like ADHDpoor executive functioning – may look like ADHD
04/19/2304/19/23 6060
Questions after lecture?Questions after lecture?
Please e-mail ([email protected]) or call Please e-mail ([email protected]) or call (01 467 1717)(01 467 1717)
Interested in learning more about child and Interested in learning more about child and adolescent psychiatry?adolescent psychiatry?– Arrange to attend OPD Arrange to attend OPD – Consider an elective rotation during internship Consider an elective rotation during internship
or otherwiseor otherwise